Back to Journals » Nature and Science of Sleep » Volume 17

The Complex Interplay Between Sleep and Healthy Aging: A Scoping Review
Authors Bragazzi NL, Mutti C, Ratti PL, Sardella A, Quattropani MC ![]() , Lodi R, Pizza F, Biscarini F, Bottignole D
, Lodi R, Pizza F, Biscarini F, Bottignole D ![]() , Salvi M
, Salvi M ![]() , Maggio M, Parrino L, Plazzi G, Franceschini C
, Maggio M, Parrino L, Plazzi G, Franceschini C ![]()
Received 12 August 2025
Accepted for publication 18 October 2025
Published 29 November 2025 Volume 2025:17 Pages 3085—3100
DOI https://doi.org/10.2147/NSS.S555177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Nicola Luigi Bragazzi,1 Carlotta Mutti,2,3 Pietro Luca Ratti,4,5 Alberto Sardella,6 Maria C Quattropani,6 Raffaele Lodi,7,8 Fabio Pizza,9,10 Francesco Biscarini,9,10 Dario Bottignole,2,3 Marco Salvi,3,11 Marcello Maggio,3,11 Liborio Parrino,2,3 Giuseppe Plazzi,9,12 Christian Franceschini2,3
1Human Nutrition Unit (HNU), Department of Food and Drugs University of Parma, Parma, Italy; 2Department of Medicine and Surgery, Sleep Disorders Center, Parma University Hospital, Parma, Italy; 3Mario Giovanni Terzano Interdepartmental Center for Sleep Medicine, University of Parma, Parma, Italy; 4Neurocenter of Southern Switzerland, Regional Hospital of Lugano, Bellinzona, Switzerland; 5Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, UK; 6Department of Educational Science, University of Catania, Catania, Italy; 7Department of Biomedical and Neuromotor Sciences, University of Bologna, Bologna, Italy; 8Functional and Molecular Neuroimaging Unit, IRCCS Istituto delle Scienze Neurologiche Di Bologna, Bologna, Italy; 9Department of Biomedical and Neuromotor Sciences (DIBINEM), Alma Mater Studiorum, University of Bologna, Bologna, Italy; 10Center for Sleep Studies, IRCCS Istituto Delle Scienze Neurologiche Di Bologna (ISNB), Bologna, Italy; 11Geriatric Clinic Unit, University Hospital of Parma, Parma, Italy; 12Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Modena, Italy
Correspondence: Christian Franceschini, Bio Technological Pole, School of Medicine, Clinical Psychology Unit, University of Parma, Volturno Street 39, Parma, 43126, Italy, Email [email protected]
Background: The relationship between sleep and healthy aging is complex, involving changes in sleep patterns, architecture, and disturbances. Recognizing these changes is crucial for maintaining physical, cognitive, social, and psychological well-being in older adults. However, links between sleep parameters and aging outcomes remain unclear.
Objective: This review synthesizes current knowledge on associations between sleep parameters (duration, continuity, architecture, quality) and healthy aging outcomes, including physical health, cognitive function, psychological well-being, and social engagement.
Methods: Following the Arksey and O’Malley framework and Joanna Briggs Institute guidelines, this scoping review analyzed observational studies on healthy older adults. Sleep-related measures were examined without confounders from mental or physical illnesses.
Results: Twenty studies were included. Across cohorts, older adults consistently exhibited advanced sleep phases (bedtime ≈39 minutes earlier, wake time ≈76 minutes earlier) and reduced total sleep time (by approximately 2.4 hours vs younger adults). Both short and long sleep durations were associated with poorer aging outcomes, supporting a U-shaped relationship between sleep length and healthy aging. Sleep efficiency decreased by 13% and wake after sleep onset increased fourfold with age, particularly among women. Age-related reductions in slow-wave and REM sleep were linked to lower cognitive performance and altered mood regulation. Moderate daytime napping (< 60 min/day) was generally associated with better sleep quality, whereas excessive napping correlated with reduced odds of “successful aging”. Discrepancies between subjective and objective sleep assessments emerged, indicating that older adults may underreport sleep disturbances.
Conclusion: Gaps in understanding longitudinal sleep data, the mechanisms of sleep’s impact on aging, and napping’s role need further exploration. Future research could inform interventions for promoting healthy aging.
Keywords: sleep, objective sleep, subjective sleep, sleep quality, healthy aging, scoping review
Introduction
Sleep plays a fundamental role in maintaining overall health and well-being throughout the lifespan,1 with its importance becoming increasingly pronounced as individuals age.2,3 Healthy aging, often referred to as “resilient” or “successful” aging, is a multidimensional concept characterized by the maintenance of physical, cognitive, and social functioning, along with the preservation of psychological well-being in older adults.4,5 Active aging, a complementary concept to healthy aging, emphasizes the continued participation of older individuals in social, economic, cultural, spiritual, and civic activities, regardless of physical capacity. Active aging constitutes one of the three core components of the Rowe and Kahn model of “successful aging”,6,7 which conceptualizes “better-than-average” aging as the confluence of three elements: i) avoidance of disease and disability, ii) maintenance of high physical and cognitive functioning, and iii) sustained engagement with life. Despite its popularity and widespread influence, this model has been criticized for its overly individualistic and biomedical orientation, which places limited emphasis on social and environmental determinants of aging.8,9 This has led health institutions and organizations such as the World Health Organization (WHO) to broaden and expand the definition of aging. For instance, the WHO has defined active aging as the process of optimizing opportunities for health, participation, and security to enhance quality of life as people age. This aligns with the broader framework of healthy aging, which the WHO defines as the process of maintaining functional ability to enable well-being in older age. In recognition of the growing importance of this issue, the WHO has declared 2020–2030 the Decade of Healthy Ageing, focusing on fostering environments that promote both active and healthy aging.5,10
While aging is inevitably associated with changes in sleep patterns and architecture,11 the extent to which these changes impact healthy aging outcomes remains a topic of ongoing research and debate.10,12 Several key factors underscore the importance of examining the relationship between sleep and healthy aging. Firstly, advancing age is often accompanied by alterations in sleep duration, continuity, and quality, including a tendency towards more fragmented sleep, decreased total sleep time (TST), and alterations in sleep architecture characterized by reduced slow-wave sleep (SWS) and diminished rapid eye movement (REM) sleep.13 These changes in sleep patterns are influenced by a myriad of factors, including physiological, psychological, and environmental variables,14–16 and might also reflect the progressive modifications in the brain structure that para-physiologically accompany the aging process, which can have implications for the physical and cognitive health of older adults.17–20 For instance, emerging evidence indicates that insufficient or disrupted sleep can adversely affect cognitive function through multiple converging biological pathways. These include altered prefrontal cortex activation leading to impaired executive control and attention, activation of systemic inflammatory and oxidative stress cascades, and disturbances in neuronal plasticity and cellular homeostasis.21,22 Both population-based investigations and experimental animal models have demonstrated that these mechanisms may accelerate neurocognitive decline, highlighting sleep as a potential modifiable target for preserving brain health and functional aging.
Furthermore, an increasing body of scholarly literature suggests that the association between sleep and aging is not linear. For instance, a recent large-scale investigation on 13,569 participants in the US focusing on the concept of “phenotypic aging” (ie, the biological and functional decline reflected in physiological markers rather than just the passage of time captured by chronological age) provided compelling evidence that sleep duration exerts a strong influence on healthy aging, showing that both short and long sleep durations are associated with accelerated aging.23 The potential influence of several endogenous (such as sex/gender) and external factors (including, above all, physical activity and exercise) can lead to a U-shaped relationship between sleep duration and phenotypic aging, as recently described in seminal population-based studies,23,24 increasing the complexity of such an intricated interplay.
Moreover, sleep disturbances are prevalent among older adults, with conditions such as insomnia, sleep apnea, restless legs syndrome, REM sleep parasomnias, and periodic limb movement disorder becoming more common with aging.25,26 These sleep disorders not only contribute to subjective complaints of poor sleep quality but may also exacerbate age-related declines in cognitive function, increase the risk of chronic medical conditions such as arterial hypertension, metabolic disorders, and diabetes, and impair the quality of life and well-being in older individuals.27–29 Despite the recognition of the interplay between sleep and healthy aging, the complex relationships between sleep parameters and various domains of healthy aging outcomes are still largely poorly understood. Specifically considering the increasing burden of neurodegenerative diseases in the overall general population and its societal and economic impacts,30 understanding the complex role that sleep may play as a protective factor is crucial in contemporary society.
Existing reviews have predominantly focused on pathological sleep conditions in relation to aging, thereby overlooking the complex spectrum of physiological sleep changes that accompany the aging process.31–37 When addressing healthy older populations, these reviews have typically examined only a restricted set of sleep parameters (most often sleep duration or self-reported quality) and a narrow range of health outcomes, with particular emphasis on cognitive function. As a result, other key domains of healthy aging and the interplay between objective and subjective sleep measures have remained largely underexplored.
Given the breadth and complexity of the research question, a scoping review of the literature represents the most appropriate methodological approach, unlike a systematic review, which typically focuses on narrowly defined questions suitable for quantitative synthesis or meta-analysis. A scoping review can, indeed, offer a rigorous and systematic approach to collating and evaluating the available body of scholarly evidence, thereby providing valuable insights to elucidate the associations between sleep and healthy aging across various populations and settings, identifying gaps in knowledge, and informing future research directions and clinical interventions aimed at promoting optimal aging trajectories. This review aims to examine the current state of knowledge regarding the associations between sleep parameters, including sleep duration, continuity, architecture, and quality, and multiple dimensions of healthy aging, such as physical health, cognitive function, psychological well-being, and social engagement, by synthesizing findings from diverse epidemiological studies to provide a comprehensive understanding of how sleep influences healthy aging outcomes and to identify future research and clinical practice avenues for optimizing sleep and promoting successful aging in older adults.
Materials and Methods
Details concerning the methodology are reported in Table 1 as well as in the next sections.
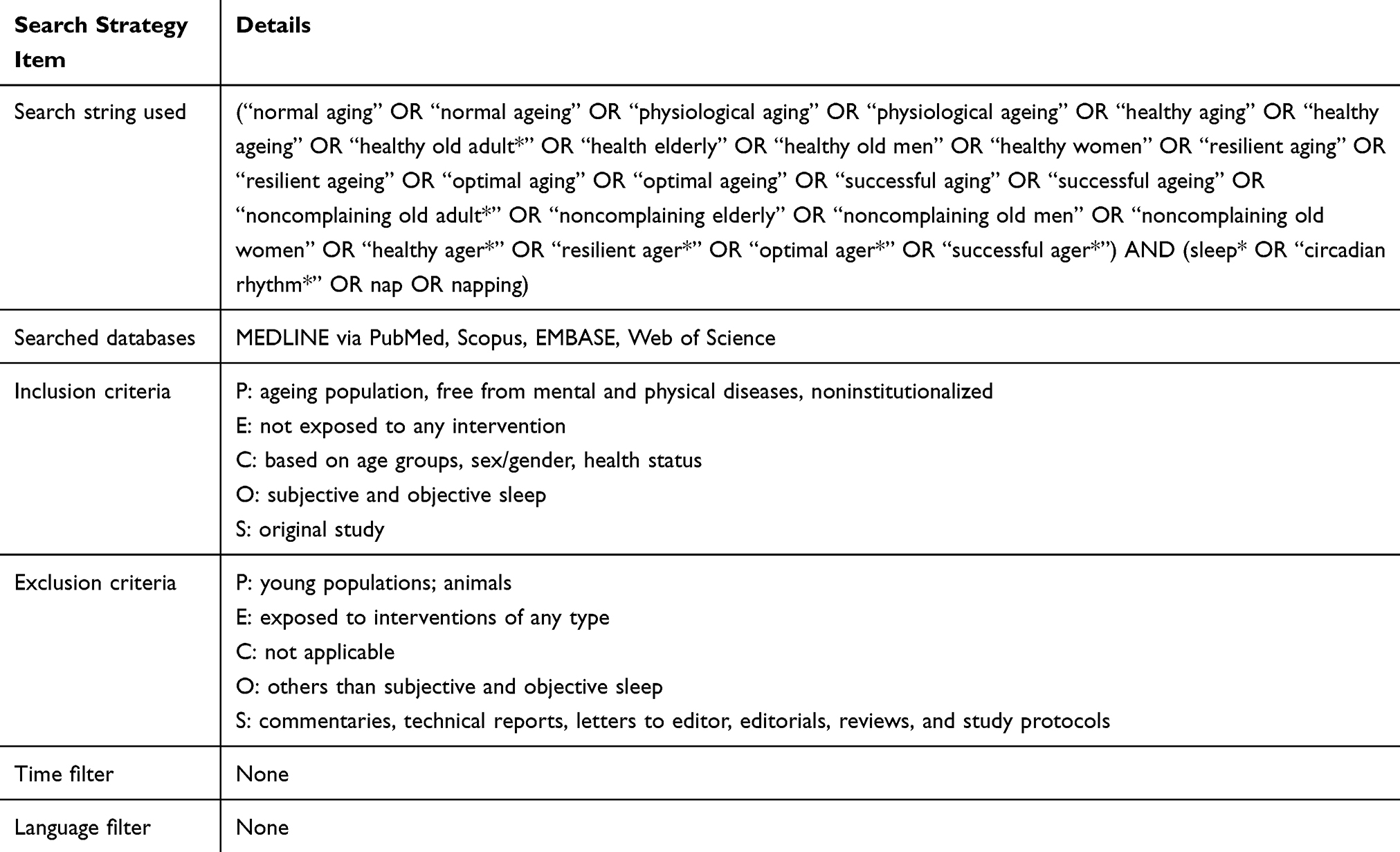 |
Table 1 Search Strategy Adopted in the Present Review |
Study Protocol
An a priori study protocol was devised following the “Joanna Briggs Institute” (JBI) recommendations.38
Methodological Framework
The Arksey and O’Malley framework,39 a widely recognized methodological tool for conducting scoping reviews, designed to map the key concepts underpinning a research area and the main sources and types of evidence available, was leveraged. This framework involves several stages, including identifying the research question, identifying relevant studies, study selection, charting the data, and summarizing and reporting the results. As such, using this structured approach enabled the identification and analysis of the breadth of literature on sleep and healthy aging, as well as the identification of gaps in knowledge, understudied areas or areas with mixed findings, and future research directions.
Literature Search
The search string utilized focused on various terms related to the process of aging and its association with sleep. The precise search string used is reported in Table 1. Four major scholarly electronic databases were searched, namely, MEDLINE via PubMed, Scopus, EMBASE, and ISI/Web of Science (WoS).
Moreover, target journals related to sleep, gerontology, aging, and the psychology of aging were hand-searched to ensure the inclusion of relevant studies and high coverage of the topic under study. Specifically, leading sleep science journals such as Sleep, Journal of Sleep Research, Sleep Medicine, and Nature and Science of Sleep were manually screened, given their centrality in publishing original research on sleep parameters, architecture, and quality across the lifespan. To capture the gerontology and aging perspective, we hand-searched Journal of Frailty & Aging, BMC Geriatrics, Maturitas, Journal of the American Geriatrics Society, and American Journal of Geriatric Psychiatry, which regularly feature studies on health, well-being, and aging trajectories. We also hand-searched journals related to the psychological/psychiatric correlates of sleep in aging (Biological Psychiatry, Journal of Psychiatric Research, Psychology and Aging, Journal of Psychosomatic Research, and Brain Research Bulletin). Finally, extensive cross-referencing was applied. The search was conducted from inception until September 26, 2024.
Inclusion and Exclusion Criteria
Inclusion/exclusion criteria were devised according to the PECOS mnemonic.40 Only original observational studies involving non-institutionalized old individuals, aged sixty years and older, free from mental and physical diseases, meeting the criteria of healthy aging, were considered. Comparisons of any type (based on age groups, sex/gender, healthy versus diseased states) were considered. Outcomes were either objective or subjective sleep-related measures. Studies using animal models or focusing on middle-aged individuals were discarded. Investigations focusing on sleep disturbances and abnormalities were excluded if not including healthy controls. Interventional trials, including those administering central nervous system (CNS)-acting drugs, were not considered. Finally, commentaries, technical reports, letters to the editor, editorials, reviews, and study protocols were not deemed eligible for inclusion (Table 1).
Data Extraction
The following data were extracted independently by two authors (N.L.B. and D.B).: study, study country, study design, sample size, the definition of healthy aging employed in the study, tools for studying sleep, sleep-related parameters studied, sleep timing, sleep duration, sleep continuity and efficiency, sleep architecture, chronotype and circadian rhythms, subjective sleep (ie, sleep quality), comparison between objective and subjective measures, and key findings. A customized Excel spreadsheet was utilized.
Finding Reporting
The findings were reported in accordance with the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) Extension for Scoping Reviews (PRISMA-ScR) checklist.41
Results
The initial literature search yielded a pool of 7,694 items (2,587 from Embase, 1,766 from Scopus, 1,758 from PubMed/MEDLINE, and 1,583 from the ISI/WOS). After removing duplicates, 3,832 items were screened. After discarding irrelevant items based on the title and/or abstract, 107 results were analyzed in-depth. From the full-text assessment, 87 studies were excluded with reasons: 39 studies were excluded due to the study population, involving community-dwelling persons with comorbidities or other health issues, hospital-based patients, or institutionalized elderly not free from diseases, therefore not meeting the inclusion criterion of healthy participants. Eleven studies were excluded because they were methodological in nature, 22 studies were classified as interventional and thus excluded, and 15 studies were excluded as they explored outcome measures not of interest. Twenty studies42–61 were finally included in the present review (Table 2). The study selection process is depicted in Figure 1.
 |
Table 2 Major Features of the Studies Included in the Present Scoping Review |
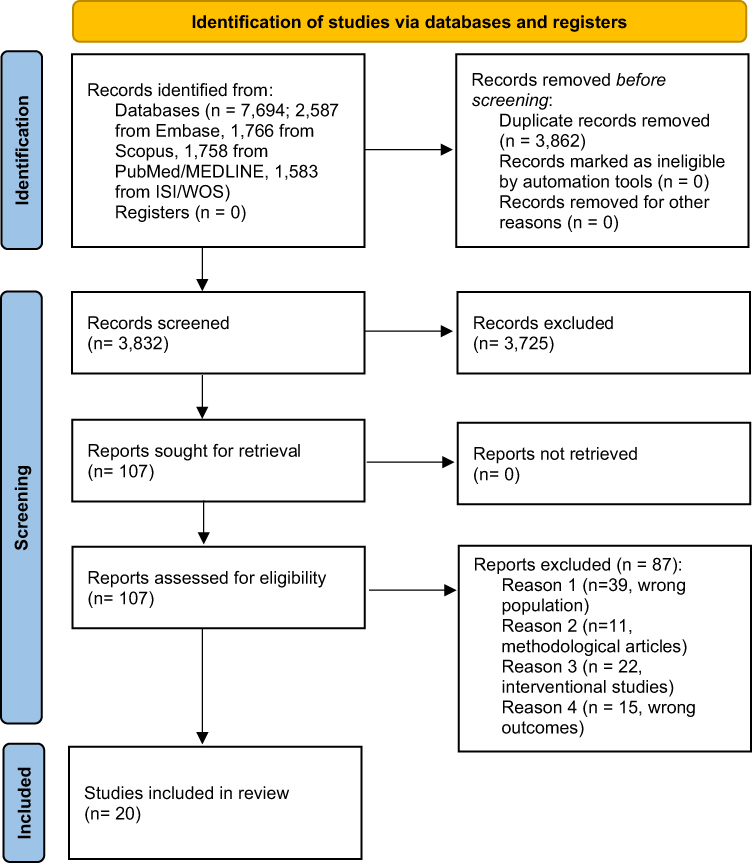 |
Figure 1 PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) flow diagram depicting the selection process. Notes: PRISMA figure adapted from Tricco AC, Lillie E, Zarin W et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–473.41 |
Demographic Features
The average participant age in these studies ranged from 60 to 85 years, enabling us to examine the structure of sleep across a wide age range. In terms of gender distribution, both males and females were well represented. A few studies focused exclusively on women, while most studies featured mixed-gender samples. The sample sizes across the studies varied significantly, from small investigations involving as few as seven participants to large cohort studies including more than 7,000 participants. Altogether, the studies included more than 20,000 individuals from different geographic locations.
One study was conducted in Japan,48 focusing on sleep timing and body temperature rhythms in healthy older (aged 63.7±8.0 years, 50–73 years) versus younger adults (aged 21.1±2.3 years, 18–24 years). Two studies were conducted in Germany,46,51 exploring sleep architecture in healthy elderly, Alzheimer’s, and depression patients, as well as HPA axis activity and sleep in the elderly, with a third59 investigating perceived sleep quality and its temporal stability in the elderly.
Multiple studies originated from the USA, 44(p24),47,53–56,61 including one53 comparing sleep architecture in elderly, Alzheimer’s, and depression patients, another47 as part of the Nurses’ Health Study focusing on sleep duration and healthy aging, while the others examine circadian rhythms, sleep quality, and gender differences in older adults.
Two studies were conducted in China50,52 using data from the China Health and Retirement Longitudinal Study (CHARLS), investigating sleep patterns and successful aging, as well as the impact of daytime napping on healthy aging in the elderly. Two Italian studies focused on the role of stress hormones49 and body movements during sleep in the elderly.58 Australian researchers60 assessed sleep quality and health in elderly men and women. Additionally, an investigation from Belgium42 explored napping, circadian rhythms, and perceived sleep quality among seniors aged 69 years, as well as its temporal stability. Another study from Switzerland45 examined REM sleep characteristics and their long-term impact on cognitive functions and aging. Finally, one study from Greece43 focused on sleep quality and healthy aging trajectories in older adults.
Tools for Investigating and Measuring Sleep
Nine studies employed objective sleep assessment through polysomnography (PSG),44–46,51,53,54,56–58 providing detailed information on sleep architecture, efficiency, latency, and stages. One study relied exclusively on subjective measures, using validated sleep-related questionnaires and patient-reported outcomes to capture perceived sleep quality and disturbances.55 Three studies complemented objective assessments with sleep diaries,44,48,56 allowing for the evaluation of daily sleep patterns, timing, and variability. The remaining investigations adopted multimodal approaches, integrating different assessment tools, such as PSG, sleep diaries, self-reported questionnaires, and/or actigraphy, to obtain a more comprehensive characterization of sleep behavior and quality in older adults.42,52,60
Sleep Timing
Six studies provided data on sleep timing.44,48,51,54–56 All of these studies consistently reported an advanced sleep phase in older adults, characterized by earlier bedtimes and wake-up times compared to younger adults. This pattern was found to be consistent across various countries and cultures, including Japan, the USA, and Germany, regardless of study design. More specifically, negative correlations were observed between sleep onset time and age, with less pronounced but still notable correlations between final awakening time and age.48
In one study,44 elderly participants went to bed approximately 39 minutes earlier and woke up around 76 minutes earlier than their younger counterparts. Gender-specific differences were also observed: despite similar bedtimes, women tended to wake up earlier than men (mean difference of 30 minutes), with the timing of peak body temperature closely linked to both bedtime and wake-up time.55 Additionally, in a subset of older women, a relationship between perceived sleep quality and sleep onset was suggested, with poor sleepers tending to have a longer sleep latency compared to good sleepers.54
Sleep Duration
Nine studies provided data on sleep duration in the elderly.47,48,50–52,54,55,57,61 One study61 found that healthy older subjects sleep 2.4 hours less per 24 hours compared to younger individuals, suggesting that sleep duration decreases with age but stabilizes after the age of 60. Sleep quality is closely associated with TST, with poorer sleepers having shorter sleep durations compared to good sleepers,54 though this trend was confirmed primarily in older women. A study comparing body temperature and circadian rhythm in a small sample of healthy 70-year-old individuals reported that women tended to sleep less than age-matched men (7.3 vs 7.8 hours), showing earlier sleep onset associated with a phase advance in the acrophase of body temperature, and a concomitant reduction in sleep quality.55 Conversely, the study by Vitiello et al,57 which analyzed both PSQI and PSG data in a larger cohort of older adults (late 60s), found longer total sleep time (TST) among women compared to men. It is noteworthy that the first study was conducted in 1994, whereas the latter was performed about a decade later and reported an overall reduction of approximately one hour of sleep in both sexes (6.4 hours in women and 6.1 hours in men).
Moreover, interesting relationships between sleep duration and aging trajectories were analyzed by a few studies,47,50,52 which found that both shorter and longer sleep durations were associated with unhealthy aging, highlighting a non-linear (inverse U-shaped) relationship between sleep duration and aging. From a gender perspective, contrasting findings have been reported. One study revealed that women had longer TST,57 while another observed that women had shorter sleep durations than men.55
Sleep Continuity and Efficiency
In the aging population, sleep is characterized by less continuity and efficiency, as confirmed by several studies,44,54,57 which consistently found that older subjects spent more time awake during the night, with this effect being more pronounced in women.54,56 Notably, these changes do not necessarily correlate with subjective complaint about sleep quality: one study57 examining a cohort of 150 healthy older adults (mean age 67.5±0.5 years) using both objective (PSG) and subjective (PSQI) assessments confirmed a marked reduction in sleep efficiency (mean 82.2±0.7% vs 94.8±0.5%) and sleep continuity (WASO 64.3±3.1 min vs 15±2.9 min) in both sexes. Notably, women exhibited a greater discrepancy between objective and subjective measures, suggesting that conventional self-reported tools such as the PSQI may have limited predictive accuracy in detecting subclinical or latent sleep disturbances in this population.
Sleep Architecture
Several studies reported data on sleep architecture,45,46,51,53,54,56,57,61 collectively highlighting the age-related effects and showing a general trend for a reduction of SWS and alterations in REM sleep among the elderly, with more fragmented patterns. Specifically, whilst SWS anomalies do not allow for a specific characterization of pathological aging, REM-related parameters and in particular REM density appear more specifically indicating unhealthy sleep, with REM density being a strong predictor of cognitive decline.62 One study51 found that aged subjects spent more time in stage 1 sleep, while time spent in stage 2 or SWS and in REM was reduced. From a gender perspective, aged men tended to spend more time in REM sleep than aged women, with shortened REM sleep latency observed in elderly men but not women. Another study61 observed no differences in SWS between older and younger subjects but noted fewer REM sleep minutes in older subjects.
These changes in sleep architecture are paralleled by age-related changes in hormonal status. The increase of stress hormones, including cortisol, is paralleled by the profound decline of anabolic hormones dehydroepiandrosterone and its sulfate derivative (DHEA and DHEAS), testosterone, estradiol, growth hormone (GH), and insulin growth factor-1 (IGF-1) concentrations, resulting in a net increase of catabolic/anabolic ratio.51 The main change of this hormonal imbalance affects the HPA axis activity and includes an altered function of hippocampal corticosteroid receptors. There is a profound relationship between these changes in HPA activity and the individual circadian rhythm.51 Besides hormonal changes, other factors that might be involved in these profound changes in the sleep architecture include progressive cortical thinning, neurodegenerative processes, age-related retinal changes with subsequent limited exposure to light signals, progressive accumulation of waste materials within the brain parenchyma, and other processes.
Of note, changes in sleep architecture correlate with cognitive function, as reported by a longitudinal study with 14 years of follow-up,45 which found that healthy old subjects with successful aging and good cognitive performances had longer REM latencies, higher REM density, and spent less time in REM sleep. Curiously, the authors also found that a greater number of NREM shifts were associated with healthy aging.45
Finally, gender differences also emerged as significant factors in understanding sleep architecture-related changes with age, with less SWS observed in healthy old men compared to women.57
Daytime Sleep and Napping
The frequency of diurnal naps significantly increases in later life, with 10% of adults and 25% older subjects reporting the occurrence of daytime naps.63 Of note, across older age groups, roughly half of these naps are unplanned, suggesting an important link between napping and excessive daytime sleepiness.
Among the included studies, four reported data on daytime sleep and napping in the elderly.42,44,50,52 One study42 found no differences in daytime rest timing between nappers and non-nappers, with no differences in overall locomotor activity, although, as expected, nappers reported a higher daily nap frequency and had longer daytime rest periods. Nappers also exhibited higher sleep efficiencies and a greater proportion of REM sleep during daytime naps compared to nighttime naps, suggesting that napping may have a beneficial effect on sleep quality and efficiency. However, nappers also presented a decrease in the melatonin peak compared to non-nappers, suggesting that napping might influence an altered circadian regulation. Interestingly, napping does not seem to have an impact on the timing of melatonin peak onset in the investigated subjects.42
Whereas significant changes in the sleep onset and duration were observed in the elderly, with a general tendency towards an advanced circadian rhythm, no differences in the timing of daily naps among age groups could be found.42 As such, while the 24-hour sleep duration may decrease with age, the propensity or preference for napping does not significantly change.
Finally, one study51 suggested that longer daytime naps (over 60 minutes/day) were linked to reduced odds of achieving successful aging, suggesting a negative impact of excessive daytime napping on sleep quality and overall health.
Chronotype and Circadian Rhythms
Two studies42,61 addressed chronotype and circadian rhythms in the aging population, offering insights into the patterns and implications of circadian preferences and biological rhythms in older adults. One study61 consistently found that circadian sleep propensity was phase-advanced in older adults, with peak sleep tendency occurring 2–3 hours earlier. This study highlights the shift in circadian rhythms that accompanies aging, leading to earlier sleep and wake times. Another study comparing older subjects with and without daytime napping42 observed no differences in Morningness-Eveningness Questionnaire scores between nappers and non-nappers, nor in the timing of melatonin peak between the two groups.
Sleep Quality
Several studies have explored sleep quality in the elderly.44–46,48,51,53,56–58,60 Older subjects tend to report poorer sleep quality than younger individuals, with sleep quality correlating with the odds of successful aging. Elderly people reporting poor sleep at least five days per week have a lower likelihood of experiencing healthy aging.
Furthermore, subjective sleep quality, as seen by increased variability in Pittsburgh Sleep Quality Index (PSQI) scores, is comparable to objective sleep measurements: the elderly with poorer sleep quality are more likely to have a greater number of short arousals and a higher mean Apnea-Hypopnea Index.
Also, of note, sleep quality, as measured through the PSQI, exhibits satisfactory stability over time, with only minimal variations with time (around 0.1±2.5 points of variation after 16±5 months of follow-up), according to a longitudinal study analyzing 91 non-complaining subjects with a 16±5-month follow-up.59 Notably, a high percentage of aged patients (26% of males and 34.5% of females) did not complain about any sleep disturbances, although they presented abnormal PSQI results (>5), probably reflecting an adaptation in the perception of disturbed sleep.
Finally, from the gender standpoint, one study55 revealed gender differences in sleep satisfaction linked with the acrophase of peak body temperature, with women being phase-advanced by 1.25 h (mean value) compared to men, reporting a lower satisfaction rate, which suggests a close relationship between circadian changes and perceived sleep quality. In a study based on a sample of old women only,54 it was noted that poor sleepers had later bedtimes, longer sleep onset times, and reported more psychological symptoms, such as anxiety and depression, highlighting the impact of psychological factors on sleep quality.
Comparison Between Sleep-Related Objective and Subjective Measures
Only three studies54,56,57 performed a comparison between sleep-related objective and subjective measures, reporting contrasting findings. While one study56 failed to compute significant correlations between objective and subjective features in the elderly, other studies57 detect significant correlations between the subjectively perceived sleep quality, assessed through PSQI, and time in bed, TST, WASO, SE, and sleep latency.54
Discussion
The present scoping review systematically investigated the intricate, non-linear relationship between sleep and healthy aging, highlighting the multifaceted nature of sleep changes and their implications on aging trajectories and outcomes (pictorially depicted in Figure 2 and summarized in Table 1, fully reported in Supplementary Table 1).On the one hand, the synthesis of findings from diverse geographical regions, populations, and study designs emphasizes the universal relevance of sleep in the context of aging, underscoring, on the other hand, the need for a nuanced understanding of sleep in older adults. This is the first step to contextualize the findings related to sleep patterns, duration, continuity, architecture, and quality.
 |
Figure 2 The relationship between sleep patterns, chronotype, circadian rhythms, and their impact on healthy aging, with specific insights into gender differences. |
The review reveals consistent findings of an advanced sleep phase in older adults across different cultures, with earlier bedtimes and wake-up times. This pattern is linked to various factors, including gender, with women tending to wake up earlier. A reciprocal relationship between sleep duration and sleep quality was also suggested, where poor sleepers presented with later sleep-onset. Noteworthy, the relationship between sleep duration and healthy aging outcomes indicates a U-shaped association, where both shorter and longer sleep durations can be detrimental, suggesting an optimal range conducive to healthy aging.
Sleep continuity and efficiency are found to decrease with age, with more pronounced effects in women, although findings on gender differences remain fuzzy. The impact of aging on sleep architecture is evident in the reduction of SWS and alterations in REM sleep, with potential implications for cognitive functions. The role of gender in these changes is also highlighted, with differences in REM sleep patterns and SWS between men and women.
Daytime sleep and napping emerge as significant aspects of sleep in older adults. Findings suggest that napping may improve sleep quality and efficiency. Additionally, napping has concomitant circadian implications. Furthermore, excessive daytime napping is linked to reduced odds of successful aging. Chronotype and circadian rhythms also shift with age, leading to earlier sleep and wake times, with implications for sleep propensity and circadian preferences, but also towards perceived sleep quality.
Finally, subjective sleep quality is a critical factor in healthy aging, with older adults often reporting poorer sleep quality compared to younger individuals. A higher tolerability for disturbed sleep with aging was also suggested, with an elevated percentage of non-complaining old subjects, especially women, with above-threshold PSQI results. This might also suggest the poor applicability of this screening tool among the elderly. The relationship between sleep quality and successful aging is underscored, with poor sleepers having lower odds of experiencing healthy aging. Gender differences in sleep satisfaction and the impact of psychological factors on sleep quality are also notable, pointing to the complex interplay between psychological well-being and sleep in older adults. The comparison between objective and subjective sleep measures reveals contrasting findings, indicating the need for careful consideration of both types of measures in sleep research among older adults, as previously mentioned. The lack of significant correlations in some studies suggests potential discrepancies between perceived and actual sleep quality, highlighting the complexity of assessing sleep in aging populations.
Knowledge Gaps and Future Research Directions
The present scoping review on the relationship between sleep and healthy aging reveals several critical gaps in the current literature, pointing to key areas for future research. These gaps not only highlight the need for a deeper understanding of specific aspects of sleep in the context of aging but also underscore the potential for developing targeted interventions aimed at enhancing sleep quality and, by extension, promoting healthy aging outcomes.
A first limitation encountered in summarizing the reviewed evidence is the heterogeneity of the older population samples studied and the definition of healthy aging, which spans from the use of disease-centered aging models, often focused on the presence of neurological disorders, to multidimensional ones. This means, considering such a wide age range, that the aging trajectories of the subjects included in these studies can be extremely variable, influenced by multiple interfering factors of a bio-psycho-social nature, and therefore, not so easy to study in relation to the effect of sleep and its properties.
Another relevant gap concerns longitudinal data on sleep patterns: there is, indeed, a notable scarcity of studies tracking sleep patterns over time in the same individuals. Such data would be of paramount importance to understand the trajectory of sleep changes with aging and their long-term impact on health outcomes. The underlying biological mechanisms linking sleep changes with aging processes also remain inadequately explored. Future research should aim to elucidate the pathways through which alterations in sleep architecture, duration, and quality impact physical, cognitive, and psychological mental health in older adults. Furthermore, the impact of daytime napping and its role in healthy aging is still not fully understood, with conflicting findings on its benefits versus potential drawbacks. Research clarifying the optimal duration and timing of naps could inform guidelines for healthy sleep practices in older adults.
Moreover, mixed findings on gender differences in sleep patterns, continuity, and architecture indicate a gap in gender-specific research. Detailed studies focusing on the distinct sleep needs and challenges faced by older men and women are needed to tailor interventions appropriately.
Another important limitation of our study relates to age heterogeneity among the included participants. Although it is plausible that differences in sleep quality and/or quantity may vary across age groups (for instance, between individuals in their 60s and those over 80), most of the included studies did not report sufficiently detailed age-specific data to enable such stratified analyses.
In terms of cultural and ethnic considerations, while the present review includes studies from diverse geographic locations, there is a need for more comprehensive research exploring societal and cross-cultural differences in sleep patterns and their implications for healthy aging, since the confounding effect of other determinants of healthy aging is not well addressed in the included studies.
Furthermore, several of the included studies were conducted many years ago, with key investigations dating back to the 1990s and early 2000s. Given the profound societal and technological transformations that have occurred since then, such as changes in lifestyle patterns, work schedules, exposure to artificial light and screens, and the pervasive influence of electronic devices, the sleep behaviors and environmental exposures of contemporary older adults may differ considerably from those observed in earlier cohorts. Consequently, the generalizability and current relevance of some of these findings should be interpreted with caution.
Additionally, we limited our observations to subjective findings and macrostructural changes in sleep architecture, although we acknowledge that aging is also accompanied by numerous and central alterations at the microstructural level. These include variations in cyclic alternating patterns (CAPs), SWS amplitude, and other electrophysiological features, which may play a pivotal role in shaping the cognitive and psychological consequences of disrupted or altered sleep in this population.
Finally, the discrepancies between subjective reports and objective measures of sleep among older subjects highlight a gap in understanding the factors contributing to these differences and potentially suggest the need for the development and validation of more sensitive and contemporary assessment tools capable of accurately capturing sleep quality and related changes in advanced age. Further research could explore the reasons behind these discrepancies and their implications for sleep assessment and intervention.
Considering these evidence limitations and gaps found in the literature, the use of older population samples that are homogeneous in terms of age and aging trajectories, with stratification based on multidimensional models, could contribute to improving the methodological consistency of future studies aimed at investigating the role of sleep as a determinant of aging.
Clinical and Practical Implications
The findings of this scoping review hold significant implications for clinicians, public health stakeholders, and older individuals themselves. For healthcare providers, awareness of the physiological yet heterogeneous nature of sleep changes in aging is essential for distinguishing normal variations from early signs of pathological decline, particularly in cognitive and affective domains. Integrating objective assessments such as PSG or actigraphy with validated subjective tools could enhance diagnostic precision and guide individualized sleep management plans. Beyond descriptive observation, these results should be interpreted in light of the growing body of evidence on interventions for sleep improvement in older adults.64 Behavioral and lifestyle-based strategies, mindfulness and relaxation practices, structured exercise programs, music therapy, and manual approaches like massage or acupuncture have shown measurable benefits on sleep onset latency, sleep efficiency, and WASO, while also enhancing psychological and functional outcomes.
For public health professionals, promoting these approaches through education, prevention, and accessibility programs could represent a sustainable and cost-effective strategy. Community-based initiatives encouraging regular sleep–wake schedules, exposure to natural light, and moderate physical activity may help maintain circadian stability and overall well-being. Furthermore, embedding sleep optimization within broader multimodal interventions, targeting mental health, cognitive preservation, and chronic disease prevention, could foster a comprehensive framework for active and functional aging.
Finally, for aging individuals, increasing self-awareness of sleep behaviors and adopting lifestyle modifications, including daily exercise, cognitive stimulation, and structured relaxation routines, can mitigate age-related sleep disruptions and preserve well-being. Digital self-monitoring tools and technology-assisted feedback may further improve adherence and empower older adults to actively manage their sleep health. Collectively, these insights underscore the necessity of translating emerging scientific knowledge into actionable, person-centered interventions that combine clinical assessment, behavioral therapy, and community engagement to support restorative sleep and healthier aging trajectories. To this end, a multidisciplinary approach based on the collaboration between sleep medicine experts and geriatricians could provide the decisive impetus for an increasingly comprehensive evaluation of sleep health in older individuals.
Conclusion
Overall, this review underscores the critical importance of sleep in the context of healthy aging, calling for a comprehensive approach to understanding and addressing sleep-related issues in older adults. Future high-quality, community-based research, leveraging longitudinal frameworks and employing multidisciplinary approaches that coherently combine and integrate insights from sleep science, gerontology, psychology, and technology, is needed to eventually develop comprehensive assessments and holistic interventions that address the multifaceted nature of sleep in aging.
This would pave the way for personalized sleep management in the aging population, investigating the potential for strategies that consider individual differences in sleep patterns, preferences, and responses to interventions. Data from studies could inform policy and public health initiatives aimed at promoting healthy sleep habits among older adults, considering the broader socio-economic and environmental factors influencing sleep.
By addressing these gaps and pursuing the suggested future directions, research can significantly advance our understanding of the complex relationship between sleep and healthy aging, ultimately leading to more effective strategies for promoting optimal sleep and aging outcomes.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Author Contributions
NLB: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Software; Validation; Visualization; Writing - original draft, Writing - review & editing; CM: Formal analysis; Writing - original draft; Writing - review & editing; PLR: Writing - original draft; Formal analysis; Writing - review & editing; AS: Formal analysis; Writing - review & editing; MCQ: Formal Analysis; Writing - review & editing; RL: Formal analysis; Writing - review & editing; FP: Conceptualization; Writing - review & editing; FB: Conceptualization; Writing - review & editing; DB: Formal analysis; Writing – review & editing; MS: Conceptualization; Writing - review & editing; MM: Conceptualization; Writing - review & editing; LP: Conceptualization; Writing - review & editing; GP: Conceptualization; Writing - review & editing; CF: Conceptualization; Validation; Writing - original draft, Writing - review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Francesco Biscarini reports support from Bioprojet for attending congresses. The author(s) report no conflicts of interest in this work.
References
1. Ramar K, Malhotra RK, Carden KA, et al. Sleep is essential to health: an American Academy of Sleep Medicine position statement. J Clin Sleep Med. 2021;17(10):2115–2119. doi:10.5664/jcsm.9476
2. Li J, Vitiello MV, Gooneratne NS. Sleep in normal aging. Sleep Med Clin. 2018;13(1):1–11. doi:10.1016/j.jsmc.2017.09.001
3. Li J, Vitiello MV, Gooneratne NS. Sleep in normal aging. Sleep Med Clin. 2022;17(2):161–171. doi:10.1016/j.jsmc.2022.02.007
4. Decade of healthy ageing: baseline report. ed. World Health Organization; 2021.
5. Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 2020;139:6–11. doi:10.1016/j.maturitas.2020.05.018
6. Rowe JW, Kahn RL. Human aging: usual and successful. Science. 1987;237(4811):143–149. doi:10.1126/science.3299702
7. Rowe JW, Kahn RL. Successful Aging. Gerontologist. 1997;37(4):433–440. doi:10.1093/geront/37.4.433
8. Stowe JD, Cooney TM. Examining Rowe and Kahn’s concept of successful aging: importance of taking a life course perspective. Gerontologist. 2015;55(1):43–50. doi:10.1093/geront/gnu055
9. Martinson M, Berridge C. successful aging and its discontents: a systematic review of the social gerontology literature. Gerontologist. 2015;55(1):58–69. doi:10.1093/geront/gnu037
10. Menassa M, Stronks K, Khatami F, et al. Concepts and definitions of healthy ageing: a systematic review and synthesis of theoretical models. eClinicalMedicine. 2023;56:101821. doi:10.1016/j.eclinm.2022.101821
11. Lavoie CJ, Zeidler MR, Martin JL. Sleep and aging. Sleep Sci Pract. 2018;2(1):3. doi:10.1186/s41606-018-0021-3
12. Mander BA, Winer JR, Walker MP. Sleep and Human Aging. Neuron. 2017;94(1):19–36. doi:10.1016/j.neuron.2017.02.004
13. Ravyts SG, Dzierzewski JM. Sleep and healthy aging: a systematic review and path forward. Clin Gerontol. 2024;47(3):367–379. doi:10.1080/07317115.2022.2064789
14. Ohayon MM, Carskadon MA, Guilleminault C, Vitiello MV. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep. 2004;27(7):1255–1273. doi:10.1093/sleep/27.7.1255
15. Crowley K. The effects of normal aging on sleep spindle and K-complex production. Clin Neurophysiol. 2002;113(10):1615–1622. doi:10.1016/S1388-2457(02)00237-7
16. Godfrey S, Iversen HK, West AS. Melatonin profile in healthy, elderly subjects - A systematic literature review. Chronobiol Int. 2022;39(4):476–492. doi:10.1080/07420528.2021.2016794
17. Taillard J, Gronfier C, Bioulac S, Philip P, Sagaspe P. Sleep in normal aging, homeostatic and circadian regulation and vulnerability to sleep deprivation. Brain Sci. 2021;11(8):1003. doi:10.3390/brainsci11081003
18. Muehlroth BE, Rasch B, Werkle-Bergner M. Episodic memory consolidation during sleep in healthy aging. Sleep Med Rev. 2020;52:101304. doi:10.1016/j.smrv.2020.101304
19. Kroeger D, Vetrivelan R. To sleep or not to sleep – effects on memory in normal aging and disease. Aging Brain. 2023;3:100068. doi:10.1016/j.nbas.2023.100068
20. Pace-Schott EF, Spencer RMC. Sleep-dependent memory consolidation in healthy aging and mild cognitive impairment. In: Meerlo P, Benca RM, Abel T, editors. Sleep, Neuronal Plasticity and Brain Function. Vol 25. Current Topics in Behavioral Neurosciences. Berlin Heidelberg: Springer; 2014:307–330. doi:10.1007/7854_2014_300
21. You Y, Liu J, Li X, Wang P, Liu R, Ma X. Relationship between accelerometer-measured sleep duration and Stroop performance: a functional near-infrared spectroscopy study among young adults. PeerJ. 2024;12:e17057. doi:10.7717/peerj.17057
22. You Y, Li J, Zhang Y, Li X, Li X, Ma X. Exploring the potential relationship between short sleep risks and cognitive function from the perspective of inflammatory biomarkers and cellular pathways: insights from population‐based and mice studies. CNS Neurosci Ther. 2024;30(5):e14783. doi:10.1111/cns.14783
23. You Y, Chen Y, Liu R, et al. Inverted U-shaped relationship between sleep duration and phenotypic age in US adults: a population-based study. Sci Rep. 2024;14(1):6247. doi:10.1038/s41598-024-56316-7
24. Taporoski TP, Beijamini F, Alexandria S, et al. Gender differences in the relationship between sleep and age in a Brazilian cohort: the baependi heart study. J Sleep Res. 2025;34(4):e14154. doi:10.1111/jsr.14154
25. Scullin MK, Sleep BDL. Cognition, and normal aging: integrating a half century of multidisciplinary research. Perspect Psychol Sci. 2015;10(1):97–137. doi:10.1177/1745691614556680
26. Penalba-Sánchez L, Silva G, Crook-Rumsey M, et al. Classification of sleep quality and aging as a function of brain complexity: a multiband non-linear EEG analysis. Sensors. 2024;24(9):2811. doi:10.3390/s24092811
27. Kay DB, Dzierzewski JM. Sleep in the context of healthy aging and psychiatric syndromes. Sleep Med Clin. 2015;10(1):11–15. doi:10.1016/j.jsmc.2014.11.012
28. Siddarth P, Thana-udom K, Ojha R, et al. Sleep quality, neurocognitive performance, and memory self-appraisal in middle-aged and older adults with memory complaints. Int Psychogeriatr. 2021;33(7):703–713. doi:10.1017/S1041610220003324
29. Altena E, Ramautar JR, Yd VDW, Van Someren EJW. Do sleep complaints contribute to age-related cognitive decline? In: Progress in Brain Research. Vol. 185. Elsevier;2010:181–205. doi:10.1016/B978-0-444-53702-7.00011-7
30. Wang S, Jiang Y, Yang A, Meng F, Zhang J. The expanding burden of neurodegenerative diseases: an unmet medical and social need. Aging Dis. 2024;16(5):293doi:10.14336/AD.2024.1071.
31. Liu HM, Xue YJ, Tang KW, et al. Association between sleep duration and frailty in older adults: systematic review and meta-analysis of observational studies. Arch Gerontol Geriatr. 2025;137:105949. doi:10.1016/j.archger.2025.105949
32. Kavousi P, Mali E, Seifhashemi N, Souri M, Pakravan L, Khalili F. Worldwide prevalence of poor sleep quality in older adults: a systematic review and meta-analysis. Iran J Psychiatry. 2025;20:265–280. doi:10.18502/ijps.v20i2.18207
33. Ma X, Yao G, Wan X, et al. Relationship between sleep and cognitive frailty in older adults: a systematic review and meta‐analysis. J Adv Nurs. doi:10.1111/jan.17081
34. Wai JL, Yu DS. The relationship between sleep–wake disturbances and frailty among older adults: a systematic review. J Adv Nurs. 2020;76(1):96–108. doi:10.1111/jan.14231
35. Sella E, Miola L, Toffalini E, Borella E. The relationship between sleep quality and quality of life in aging: a systematic review and meta-analysis. Health Psychol Rev. 2023;17(1):169–191. doi:10.1080/17437199.2021.1974309
36. Sun R, Xie Y, Jiang W, Wang E, Li X. Effects of different sleep disorders on frailty in the elderly: a systematic review and meta-analysis of observational studies. Sleep Breath. 2023;27(1):91–101. doi:10.1007/s11325-022-02610-5
37. Casagrande M, Forte G, Favieri F, Corbo I. Sleep quality and aging: a systematic review on healthy older people, mild cognitive impairment and alzheimer’s disease. Int J Environ Res Public Health. 2022;19(14):8457. doi:10.3390/ijerph19148457
38. Peters MDJ, Godfrey C, McInerney P, et al. Best practice guidance and reporting items for the development of scoping review protocols. JBI Evid Synth. 2022;20(4):953–968. doi:10.11124/JBIES-21-00242
39. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
40. Craig JV, Smyth RL. The Evidence-Based Practice Manual for Nurses.
41. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
42. Deantoni M, Reyt M, Baillet M, et al. Napping and circadian sleep–wake regulation during healthy aging. Sleep. 2024;47(5):zsad287. doi:10.1093/sleep/zsad287
43. Gkotzamanis V, Panagiotakos DB, Yannakoulia M, et al. Sleep quality and duration as determinants of healthy aging trajectories: the HELIAD study. J Frailty Aging. 2023;12(1):16–23. doi:10.14283/jfa.2022.37
44. Buysse DJ, Browman KE, Monk TH, Reynolds CF, Fasiczka AL, Kupfer DJ. Napping and 24‐hour sleep/wake patterns in healthy elderly and young adults. J Am Geriatr Soc. 1992;40(8):779–786. doi:10.1111/j.1532-5415.1992.tb01849.x
45. Spiegel R, Herzog A, Köberle S. Polygraphic sleep criteria as predictors of successful aging: an exploratory longitudinal study. Biol Psychiatry. 1999;45(4):435–442. doi:10.1016/S0006-3223(98)00042-0
46. Dykierek P, Stadtmüller G, Schramma P, et al. The value of REM sleep parameters in differentiating Alzheimer’s disease from old-age depression and normal aging. J Psychiatr Res. 1998;32(1):1–9. doi:10.1016/S0022-3956(97)00049-6
47. Shi H, Huang T, Ma Y, Eliassen AH, Sun Q, Wang M. Sleep duration and snoring at midlife in relation to healthy aging in women 70 years of age or older. Nat Sci Sleep. 2021;13:411–422. doi:10.2147/NSS.S302452
48. Nakazawa Y, Nonaka K, Nishida N, et al. Comparison of body temperature rhythms between healthy elderly and healthy young adults. Psychiatry Clin Neurosci. 1991;45(1):37–43. doi:10.1111/j.1440-1819.1991.tb00503.x
49. Maggio M, Colizzi E, Fisichella A, et al. Stress hormones, sleep deprivation and cognition in older adults. Maturitas. 2013;76(1):22–44. doi:10.1016/j.maturitas.2013.06.006
50. Xin C, Zhang B, Fang S, Zhou J. Daytime napping and successful aging among older adults in China: a cross-sectional study. BMC Geriatr. 2020;20(1):2. doi:10.1186/s12877-019-1408-4
51. Dodt C, Theine KJ, Uthgenannt D, Born J, Fehm HL. Basal secretory activity of the hypothalamo–pituitary–adrenocortical axis is enhanced in healthy elderly. An assessment during undisturbed night-time sleep. Eur J Endocrinol. 1994;131(5):443–450. doi:10.1530/eje.0.1310443
52. Liu H, Byles JE, Xu X, Zhang M, Wu X, Hall JJ. Association between nighttime sleep and successful aging among older Chinese people. Sleep Med. 2016;22:18–24. doi:10.1016/j.sleep.2016.04.016
53. Hoch CC, Reynolds CF, Houck PR, Verran JA, Wolanin MO. Sleep patterns in alzheimer, depressed, and healthy elderly. West J Nurs Res. 1988;10(3):239–256. doi:10.1177/019394598801000302
54. Bliwise NG. Factors related to sleep quality in healthy elderly women. Psychol Aging. 1992;7(1):83–88. doi:10.1037/0882-7974.7.1.83
55. Campbell SS, Gillin JC, Kripke DF, Erikson P, Clopton P. Gender differences in the circadian temperature rhythms of healthy elderly subjects: relationships to sleep quality. Sleep. 1989;12(6):529–536.
56. Buysse DJ, Reynolds CF, Monk TH, Hoch CC, Yeager AL, Kupfer DJ. Quantification of subjective sleep quality in healthy elderly men and women using the Pittsburgh Sleep Quality Index (PSQI). Sleep. 1991;14(4):331–338.
57. Vitiello MV, Larsen LH, Moe KE. Age-related sleep change. J Psychosom Res. 2004;56(5):503–510. doi:10.1016/S0022-3999(04)00023-6
58. Gori S, Ficca G, Giganti F, Nasso ID, Murri L, Salzarulo P. Body movements during night sleep in healthy elderly subjects and their relationships with sleep stages. Brain Res Bull. 2004;63(5):393–397. doi:10.1016/j.brainresbull.2003.12.012
59. Danker-Hopfe H, Hornung O, Regen F, Hansen ML, Albrecht N, Heuser I. Subjective sleep quality in noncomplaining elderly subjects: results of a follow-up study. Anthropol Anz Ber Uber Biol-Anthropol Lit. 2006;64(4):369–376.
60. Driscoll HC, Serody L, Patrick S, et al. Sleeping well, aging well: a descriptive and cross-sectional study of sleep in “successful agers” 75 and older. Am J Geriatr Psychiatry. 2008;16(1):74–82. doi:10.1097/JGP.0b013e3181557b69
61. Campbell SS, Murphy PJ. The nature of spontaneous sleep across adulthood. J Sleep Res. 2007;16(1):24–32. doi:10.1111/j.1365-2869.2007.00567.x
62. Scullin MK, Bliwise DL. Is cognitive aging associated with levels of REM sleep or slow wave sleep? Sleep. 2015;38(3):335–336. doi:10.5665/sleep.4482
63. Foley DJ, Vitiello MV, Bliwise DL, Ancoli-Israel S, Monjan AA, Walsh JK. Frequent napping is associated with excessive daytime sleepiness, depression, pain, and nocturia in older adults: findings from the national sleep foundation ‘2003 sleep in america’ poll. Am J Geriatr Psychiatry. 2007;15(4):344–350. doi:10.1097/01.JGP.0000249385.50101.67
64. Yu Y, Wang H, Li W, Guo H, Chen Y. Non-pharmacological interventions for sleep in older adults: an umbrella review and evidence map of randomized controlled trials. Front Neurol. 2025;16:1655192. doi:10.3389/fneur.2025.1655192
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Examining Physical Wellness as the Fundamental Element for Achieving Holistic Well-Being in Older Persons: Review of Literature and Practical Application in Daily Life
Hung ST, Cheng YC, Wu CC, Su CH
Journal of Multidisciplinary Healthcare 2023, 16:1889-1904
Published Date: 5 July 2023
Reduced Slow Wave Sleep Is Associated with Increased Risk of Short Stature in Children: A Cross-Sectional Study
Chen Z, Shi Y, Lei F, Feng X, Tan L, Li T, Zhou J, Sun Y, Liao J, Li Y, Yu Z, Jiao J, Wang Y, Sanford LD, Vitiello MV, Zhang Y, Ren R, Tang X
Nature and Science of Sleep 2025, 17:2957-2967
Published Date: 18 November 2025
Factors Influencing Successful Aging in Community-Dwelling Older Women: A SOC Model Approach
Han EK, Son HK
International Journal of Women's Health 2026, 18:594173
Published Date: 21 April 2026