Back to Journals » Nature and Science of Sleep » Volume 17

Reduced Slow Wave Sleep Is Associated with Increased Risk of Short Stature in Children: A Cross-Sectional Study
Authors Chen Z ![]() , Shi Y, Lei F, Feng X, Tan L, Li T, Zhou J
, Shi Y, Lei F, Feng X, Tan L, Li T, Zhou J ![]() , Sun Y, Liao J, Li Y
, Sun Y, Liao J, Li Y ![]() , Yu Z, Jiao J, Wang Y, Sanford LD, Vitiello MV
, Yu Z, Jiao J, Wang Y, Sanford LD, Vitiello MV ![]() , Zhang Y
, Zhang Y ![]() , Ren R, Tang X
, Ren R, Tang X ![]()
Received 28 August 2025
Accepted for publication 13 November 2025
Published 18 November 2025 Volume 2025:17 Pages 2957—2967
DOI https://doi.org/10.2147/NSS.S475390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Valentina Alfonsi
Zhaohua Chen,1,2,* Yuan Shi,1,2,* Fei Lei,1,2 Xujun Feng,1– 3 Lu Tan,1,2 Taomei Li,1,2 Junying Zhou,1,2 Yuanfeng Sun,1,2 Jiamin Liao,1,2 Yun Li,4– 6 Zhoulong Yu,7 Jian Jiao,1,2 Yanyan Wang,8 Larry D Sanford,9 Michael V Vitiello,10 Ye Zhang,1,2 Rong Ren,1,2 Xiangdong Tang1,2
1Sleep Medicine Center, Mental Health Center, Department of Respiratory and Critical Care Medicine, Department of Otolaryngology Head & Neck Surgery, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 2State Key Laboratory of Biotherapy, Sichuan University, Chengdu, People’s Republic of China; 3Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, People’s Republic of China; 4Department of Sleep Medicine, Mental Health Center of Shantou University, Shantou, People’s Republic of China; 5Sleep Medicine Center, Shantou University Medical College, Shantou, People’s Republic of China; 6Shantou University Medical College-Faculty of Medicine of University of Manitoba Joint Laboratory of Biological Psychiatry, Shantou, People’s Republic of China; 7National Institute on Drug Dependence and Beijing Key Laboratory of Drug Dependence, Peking University, Beijing, People’s Republic of China; 8Healthcare Innovation Research Laboratory, West China School of Nursing, National Clinical Research Center for Geriatrics, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 9Sleep Research Laboratory, Center for Integrative Neuroscience and Inflammatory Diseases, Biomedical and Translational Sciences, Eastern Virginia Medical School, Macon & Joan Brock Virginia Health Sciences at Old Dominion University, Norfolk, VA, USA; 10Department of Psychiatry and Behavioral Sciences, University of Washington, Seattle, WA, USA
*These authors contributed equally to this work
Correspondence: Yuan Shi, Sleep Medicine Center, Mental Health Center, Department of Respiratory and Critical Care Medicine, Department of Otolaryngology Head & Neck Surgery, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China, Tel +86 18582450627, Email [email protected] Xiangdong Tang, Sleep Medicine Center, Mental Health Center, Department of Respiratory and Critical Care Medicine, Department of Otolaryngology Head & Neck Surgery, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China, Tel +86 18980602059, Email [email protected]
Objective: Although growth hormone was shown to be specifically released during slow wave sleep (SWS), no population-based evidence has demonstrated the association between sleep quality and childhood height. To address this gap, our study aims to investigate the relationship between SWS and height of children.
Methods: We analyzed polysomnography data and z-scores for height in 2527 suspected obstructive sleep apnea (OSA) children (537 non-OSA children and 1990 OSA children) collected over the past 16 years. Different grades of z-scores for height and SWS were classified by the quartile method, and the lowest z-scores for height quartile defined short stature as the main outcome. Logistic regression models were used to assess the relationship between SWS and short stature.
Results: 1990 OSA children and 537 non-OSA children were included in analyses. The mean value of z-score for height from high to low were 0.80, 0.34, 0.23 and − 0.19 in non-OSA children, and 0.47, 0.10, 0.14 and 0.05 in OSA children. Fully adjusted logistic regression models showed that, compared to the highest SWS quartile, the lowest quartile had 4.85-fold higher odds (95% CI, 2.4– 9.4) of short stature in non-OSA children and 2.15-fold higher odds (95% CI, 1.5– 3.0) in OSA children. Subgroup analyses demonstrated that in both non-OSA and OSA children, the reduction of SWS was significantly related to short stature in prepubertal children. Linear regression models confirmed positive correlations between SWS and z-score for height.
Conclusion: Our findings emphasize the crucial role of adequate sleep quality in childhood growth and development, supporting the inclusion of sleep assessments and improvements in pediatric growth monitoring programs.
Keywords: sleep, slow wave sleep, sleep quality, height, short stature, pediatric
Introduction
It is widely claimed that adequate amounts and qualities of sleep are necessary for height growth in children. This assertion is evidenced by a plethora of cultural records from around the world, including those of the Greek, Indian, and Chinese civilizations. The close relationship between sleep and growth was mentioned in the ancient Chinese medical classic Huangdi Neijing in 26 BCE, which suggests that sleep initiation during the Zi Shi period (11:00 PM to 1:00 AM) is beneficial for enhancing metabolic vitality and promoting the growth and development process of children.1
The earliest evidence related to the physiological mechanism of height development originated in the 1920s, when scientists removed the pituitary glands of animals, causing growth arrest, with resumed growth after supplementing with pituitary extract.2,3 The key role of the pituitary gland in growth regulation was confirmed, and it was speculated that a growth-promoting hormone exists.4 Subsequently, in 1957, Morris Raben successfully extracted growth hormone (GH) from the pituitary gland of human corpses and used the extract for treating dwarfism, marking the beginning of the clinical application of GH and clarifying the effect of GH on the development of bone structure.5 To date, GH remains the first-line treatment for growth hormone deficiency (GHD), with approved indications extending to a spectrum of pediatric growth disorders, including Turner syndrome and Prader-Willi syndrome.6,7
Polysomnography (PSG) is the gold standard tool for assessing the quantity and quality of sleep.8 In PSG-determined sleep stages, slow wave sleep (SWS) is considered a deep sleep state and reflects the quality of sleep under homeostatic regulation. In 1968, it was first revealed that the peak of GH secretion was closely related to SWS.9 Numerous studies have confirmed this finding and demonstrated that GH secretion remains strongly linked to SWS regardless of altered circadian rhythms or sleep deprivation.10–13 After two decades of whole-organism physiological research, recent work by Dan et al, for the first time, comprehensively demonstrated the neuroendocrine circuits regulating GH secretion across separate behavioral states of rapid eye movement (REM) sleep, non-rapid eye movement (NREM) sleep, and wakefulness.14
Nowadays, many textbooks, guidelines, and public education for childcare emphasize that good sleep is the basis for maintaining normal growth and development. However, population-based studies have yet to demonstrate an immediate relationship between sleep and linear growth. One significant challenge in addressing this gap has been the difficulty in obtaining a sufficiently large sample of polysomnographically measured sleep data in children. Our study addresses this gap by analyzing PSG-measured SWS and physical examinations of children in a large opportunistic clinical sample over a 16-year period. In addition, previous studies on SWS and GH have been exclusively conducted in adult humans and rodent models, which cannot directly demonstrate GH’s role in longitudinal growth. In contrast, our study focusing on a pediatric population offers unique insights into the physiological mechanisms underlying height development during childhood.
Elucidating the direct relationship between SWS and child height carries significant clinical implications. The findings are expected to: (1) offer a scientific basic for clinical practices aimed at promoting linear growth and mitigating growth faltering through sleep quality interventions; (2) advocate for the standardization of sleep quality assessment in routine child healthcare, shifting public health strategies from merely “ensuring adequate sleep duration” to “optimizing sleep architecture”; and (3) ultimately lay the groundwork for developing personalized sleep-health guidance programs to maximize children’s growth potential.
Materials and Methods
Subjects
This cross-sectional study included subjects from the Sleep Medicine Center, West China Hospital. This study complies with the Declaration of Helsinki and the Sichuan University Review Board approved the study procedure (NO. 1119). Before undergoing PSG monitoring, well-trained researchers verbally informed each child and their guardian about the study using a standardized script. The script includes a unified greeting, an explanation of the research purpose, and the potential use of their de-identified clinical data. Only participants and guardians who provide agreement are formally enrolled in the study, as documented by the researcher using a unified checklist and signed consent form. Subsequent analysis exclusively utilizes data from these consented individuals.
All subjects were Chinese children (aged 2–18 years) evaluated at the Sleep Medicine Center because of clinical suspicion of obstructive sleep apnea (OSA, primary symptoms including snoring, mouth breathing, hypertrophy of tonsils, etc). All potential research subjects were interviewed with a comprehensive questionnaire to collect information on general health, medication use, and history of sleep complaints.
To quantify for the present study, subjects were classified as OSA children if they meet an apnea-hypopnea index (AHI) criterion of ≥2 events/hour, whereas individuals with an AHI<2 events/hour were classified as the non-OSA children. We excluded subjects who had (1) duplicate data; (2) incomplete height or weight information; (3) other sleep disorders (eg, central disorder of hypersomnia, parasomnias, insomnia, sleep movement disorders and others); or (4) severe neuropsychiatric disorders (eg, epilepsy, depression, anxiety, schizophrenia, Tourette’s syndrome, and others). Additional information on screening criteria for the subjects is provided in Figure S1.
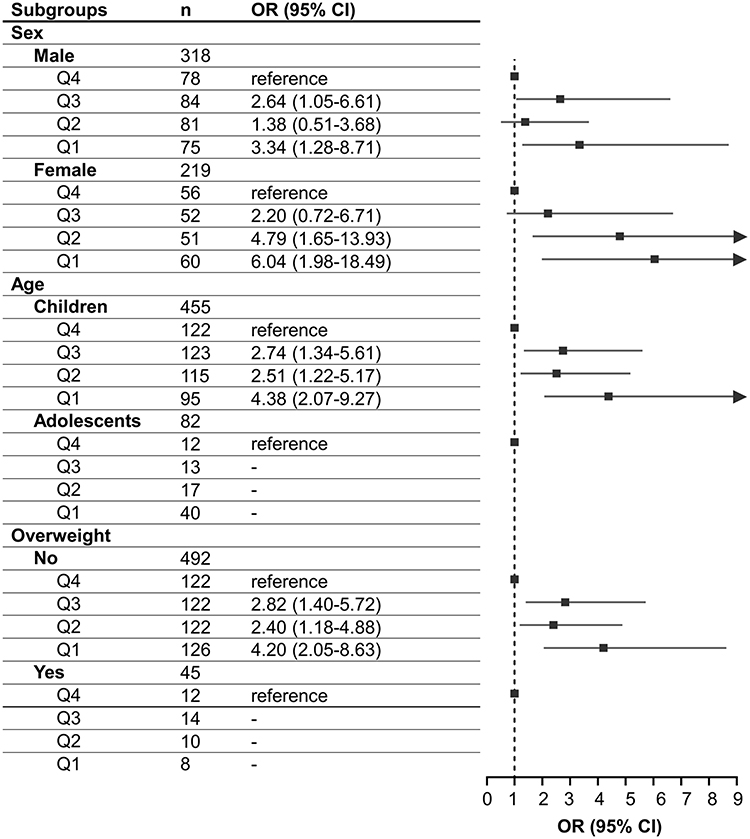 |
Figure 1 Subgroup analysis of the association between SWS and short stature in non-OSA children. Children were defined as those aged 2–9 years; adolescents were defined as those aged 10–18 years. Overweight was defined as≥2 SD of weight-for-height by sex in children aged 2–4 years, and ≥1 SD z-score for BMI for age and sex in children between 5–18 years. Q1, SWS≤21.4; Q2, 21.4<SWS≤26.6; Q3, 26.6<SWS≤32.2; Q4, SWS>32.2. The sex-stratified models were adjusted for age, z-score for BMI; age-stratified models were adjusted for sex, z-score for BMI; weight-stratified models were adjusted for age and sex. All models were additionally adjusted for sleep onset latency, total sleep time, sleep efficiency, wake after sleep onset, arousal index, AHI, and mean SpO2. Abbreviations: SWS, slow wave sleep; OSA, obstructive sleep apnea; BMI, body mass index; AHI, apnea-hypopnea index; SpO2, oxygen saturation during sleep. |
Physical Examination
The height and weight measurements of each subject were obtained by a trained physician on the PSG night. To standardize height and weight and increase the comparability of height and weight across different ages, z-scores for height and body mass index (BMI) were calculated using the World Health Organization (WHO) 2006 growth standard15 and Cole’s LMS method.16 Subjects were divided into quartiles by z-score for height, and the lowest quartile of z-score for height was considered as short stature (for non-OSA children: z-score for height<-0.507, for OSA children: z-score for height<-0.509).
Polysomnography (PSG)
All subjects completed a full-night PSG in sleep laboratories (using Alice 5 Diagnostic Sleep System prior to 2016 and the Alice 6 thereafter; Philips Respironics Bend, OR). During the sleep study, subjects were allowed to sleep ad libitum based on their routine sleep time, with the recording time ranging from 21:00–22:00 to 06:00–07:00. Sleep recordings were scored according to the latest version of the American Academy of Sleep Medicine (AASM) Manual for the Scoring of Sleep and Associated Events applicable in the corresponding year.17 SWS was expressed as the percentage of total sleep time and categorized into quartiles (for non-OSA children: Q4 (SWS>32.20), Q3 (26.60<SWS≤32.20), Q2 (21.40<SWS≤26.60), and Q1 (SWS≤21.40); for OSA children: Q4 (SWS>29.10), Q3 (24.70<SWS≤29.10), Q2 (20.20<SWS≤24.70), and Q1 (SWS≤20.20)). The highest quartile of percent SWS for each group was considered as their reference.
The AHI was determined by counting the total number of apneas and hypopneas per hour during sleep. An apnea was defined as a reduction in airflow of 90% or more, lasting at least 10 seconds. According to the prevailing AASM definitions, two different criteria were used to define hypopnea. From 2009–2012, a hypopnea was defined as a reduction in airflow of 50% or more for at least 10 seconds, accompanied by a decrease in blood oxygen saturation of 4% or more, or a reduction in airflow of 30% or more for at least 10 seconds, accompanied by a respiratory effort-related arousal (RERA). From 2013–2025, a hypopnea was defined as a reduction in airflow of 30% or more for at least 10 seconds, accompanied by a decrease in blood oxygen saturation of 3% or more, or resulting in a RERA.18,19
Statistical Analysis
Differences in sample characteristics according to OSA status and amount of SWS were assessed using ANOVA, independent-sample t-tests, or Mann–Whitney U-tests for normally distributed and skewed continuous variables, respectively. Chi-square tests were applied for categorical variables.
Independent associations of OSA and SWS with short stature, as well as their interaction effect, were assessed by logistic regression models. After observing a significant OSA×SWS interaction (P<0.001), we first examined the association of short stature with SWS in OSA and non-OSA children separately. Then, the joint effects of OSA and SWS on short stature were assessed by using non-OSA children as a reference group. We further investigated the relation between the presence/absence of OSA and short stature in stratified analysis across different SWS quartiles. Previous studies found that disturbed objective sleep structure and OSA severity negatively impacts the release of GH, indirectly influencing the growth of children.20,21 Therefore, covariates included age, sex, z-score for BMI, sleep onset latency (SOL), total sleep time (TST), sleep efficiency (SE), wake after sleep onset (WASO), arousal index (AI), AHI, and mean blood oxygen saturation (SpO2). Collinearity correlation indicators were excluded, including percentage of non-rapid eye movement sleep stage 1 (N1%), non-rapid eye movement sleep stage 2 (N2%) and rapid eye movement sleep stage (REM%). Results are presented as unadjusted and adjusted odds ratios (ORs) and 95% Confidence Intervals (CIs).
The same logistical regression models were used to measure the independent associations of SWS with short stature in different age, sex, and weight subgroups. In the age-stratified subgroups, subjects were categorized as children (2–9 years) and adolescents (10–18 years).22 In the weight-stratified subgroups, overweight was defined as≥2 standard deviation (SD) of weight-for-height by sex in children aged 2–4 years, and ≥1 SD z-score for BMI for age and sex in children between 5–18 years according to the WHO standard.23 Additionally, among children with OSA, we performed subgroup analyses based on OSA severity and arousal levels. OSA severity subgroups were classified as follows: mild (AHI ≥2events/hour), moderate (AHI ≥5events/hour), and severe (AHI ≥10 events/hour).24 Arousal level subgroups were dichotomized using the mean AI value of 11.30 as the cutoff, resulting in high-arousal (AI ≥11.30) and low-arousal (AI <11.30) subgroups.
We also used linear regression models to explore the association between z-score for height values and percent SWS among non-OSA children and across different degrees of OSA severity. Age, sex, z-score for BMI, SOL, TST, SE, WASO, AI, AHI, and mean SpO2 were included as covariates.
Statistical analyses were performed with SPSS version 29.0. All statistical tests were 2-sided, and P values of equal or less than 0.05 were considered statistically significant.
Results
The sample comprised 2527 subjects, of whom 1990 were patients with OSA. Among all the participants, 66.24% were male. The mean age was 6.55±3.25 years, the mean z-score of BMI was 0.30±1.49, and the mean z-score for height was 0.21±1.21. Demographic and sleep characteristics of this sample of non-OSA children and subjects with OSA are provided in Table S1. Compared with non-OSA children, OSA subjects had a higher percentage of male children, higher BMI, arousal index, and AHI, and lower SWS. Non-OSA children and OSA children showed comparable age, z-score for height, SOL, TST, SE, WASO, N1%, N2%, REM%, and mean SpO2%. The demographic and sleep characteristics of non-OSA children and OSA children stratified according to percent SWS are exhibited in Tables S2 and S3, respectively. Children with lower percentage of SWS were older, had lower z-scores for height and WASO, higher SE, AI, N1%, N2% and REM%, longer TST. Histograms were employed to illustrate the distribution of z-score for height across SWS% quartiles (Figures S2 and S3). OSA children in lower SWS quartiles had higher AHI.
As shown in Table 1, SWS presented a significant, dose-dependent association with short stature in both non-OSA and OSA children. From unadjusted and adjusted models, compared with Q4 group (subjects with the highest quartile of percent SWS), Q3, Q2 and Q1 groups were all more likely to have short stature, in both non-OSA and OSA children. Given that the criteria for interpreting hypopnea changed in 2012, we conducted a separate analysis of the data from January 2013 onward to explore the stability of the results. As shown Table S4, findings after 2013 are comparable with those from 2009 to 2025.
 |
Table 1 Adjusted ORs and 95% CIs for the Association Between SWS and Short Stature |
In Table 2, we present the joint effect of OSA and SWS on height. OSA children with less SWS (Q3, Q2, Q1) were more likely to show short stature compared with non-OSA children. However, OSA children with highest SWS (Q4) had decreased odds of short stature compared with non-OSA children.
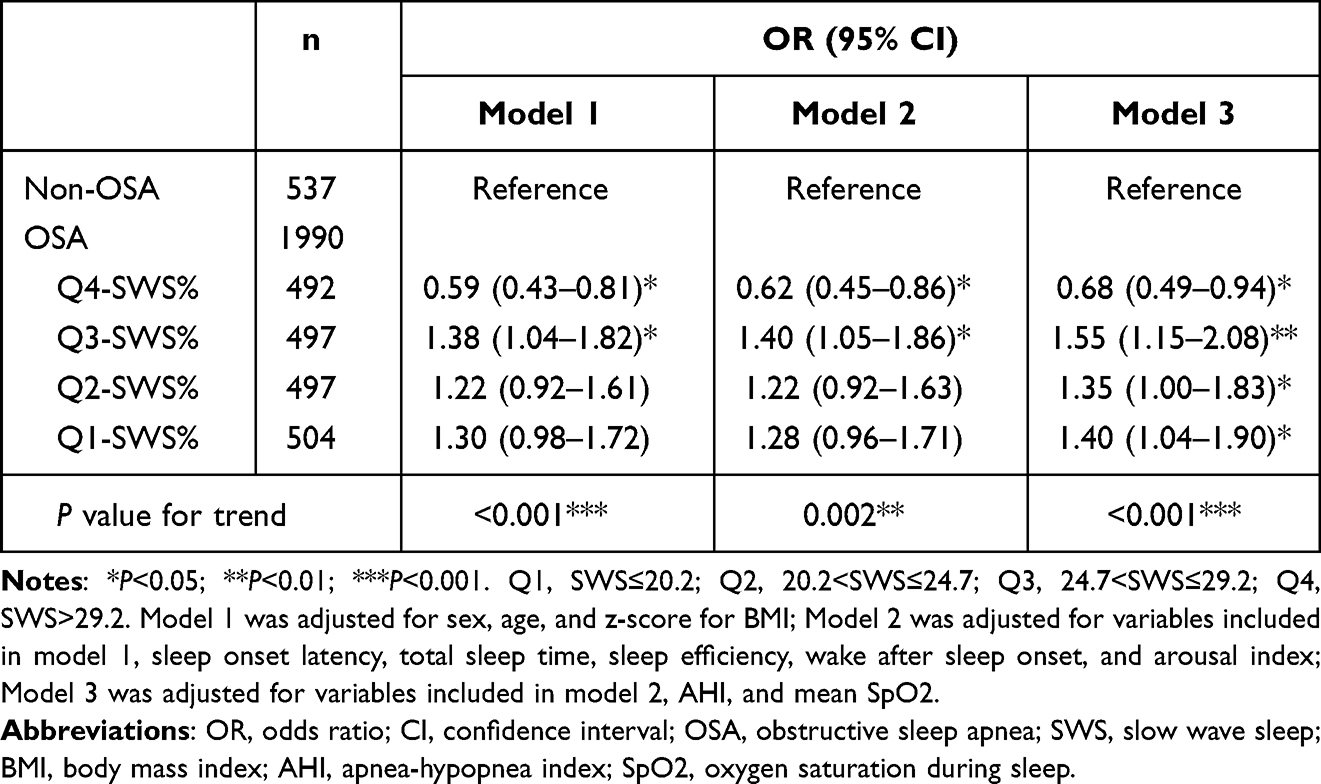 |
Table 2 Adjusted ORs and 95% CIs for the Joint Effects of OSA and SWS on Short Stature |
We further performed subgroup analyses separately for children without OSA and those with OSA, stratified by sex, age group, and overweight status (Figures 1 and 2). Additional subgroup analyses based on OSA severity and arousal levels were conducted specifically in those with OSA (Tables S5 and S6). In non-OSA children, males in Q1 group showed 3.34-fold higher odds of short stature versus in Q4, while females exhibited even greater risk (OR, 6.04). Children aged 2–9 years and non-overweight individuals displayed similar dose-response patterns (OR, 4.38 and 4.20, respectively). Among OSA children, lower SWS quartiles were associated with increased odds, particularly in males (OR, 2.05) and children aged 2–9 years (OR, 2.07). Non-overweight OSA children showed more solid associations than overweight peers. In children with OSA, a significant association between SWS and short stature was observed primarily in those with moderate to severe OSA. Moreover, among all children with OSA, those in the lower SWS quartiles exhibited a consistently elevated risk of short stature, regardless of arousal levels.
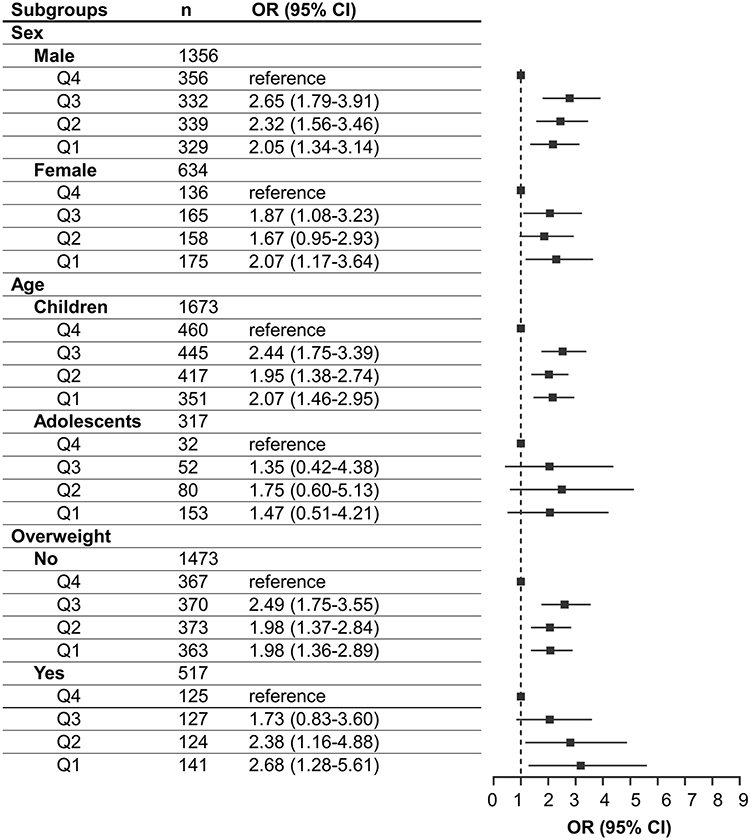 |
Figure 2 Subgroup analysis of the association between SWS and short stature in OSA children. Children were defined as those aged 2–9 years; adolescents were defined as those aged 10–18 years. Overweight was defined as≥2 SD of weight-for-height by sex in children aged 2–4 years, and ≥1 SD z-score for BMI for age and sex in children between 5–18 years. Q1, SWS≤20.2; Q2, 20.2<SWS≤24.7; Q3, 24.7<SWS≤29.2; Q4, SWS>29.2. The sex-stratified models were adjusted for age, z-score for BMI; age-stratified models were adjusted for sex, z-score for BMI; weight-stratified models were adjusted for age and sex. All models were additionally adjusted for sleep onset latency, total sleep time, sleep efficiency, wake after sleep onset, arousal index, AHI, and mean SpO2. Abbreviations: SWS, slow wave sleep; OSA, obstructive sleep apnea; BMI, body mass index; AHI, apnea-hypopnea index; SpO2, oxygen saturation during sleep. |
Additionally, height and SWS were considered as continuous variables to explore the linear relationship. In Table S7, SWS and z-score for height showed a significantly positive correlation in both non-OSA (β=0.028) and OSA children (β=0.019). In OSA subgroups, a significant positive relationship between SWS and z-score for height existed in moderate (β=0.022) and severe (β=0.026) OSA subgroups.
Discussion
Our study provides the first large population-based evidence showing an association between reduced SWS and a higher risk of short stature in children under real-world conditions. Our findings reveal that children in the lowest SWS quartile had 4.85-fold higher odds of short stature in non-OSA children and 2.15-fold higher odds in OSA children relative to those in the matching highest quartile, even after comprehensive adjustment for potential confounders. Similar and stable results were obtained for sex, age, and weight subgroups. These results substantiate historical observations linking sleep quality to growth while providing novel evidence that SWS deficiency may represent an independent risk factor for impaired height development across pediatric populations.
The link between reduced SWS and increased risk of short stature in both non-OSA and OSA children provides evidence that SWS deficiency contributes to height impairment. The underlying physiological mechanism is rooted in the GH-insulin-like growth factor-1 (IGF-1)-1 axis, which is a critical mediator of bone growth. Specifically, GH promotes the production of IGF-1 in the liver, which supports bone growth by stimulating chondrocyte proliferation in the epiphyseal plates.25,26 We speculate that reduction of SWS leads to a shortened release time window of GH, resulting in a decrease in GH level, thereby directly stunting linear growth in children.27–29 While SWS deficiency appears to be a primary driver of GH deficiency and short stature in non-OSA children, pathophysiology in children with OSA is more multifactorial and complex. Therefore, we also preliminarily explored the joint effects of SWS and OSA on height, considering that majority of our research sample consisted of subjects with OSA (78.75% of the total sample). Unexpectedly, in children with OSA, increased risk of short stature was only observed in those with deficient SWS, not in those with preserved SWS, suggesting that SWS play a protective role against growth impairment in children affected by OSA and further supports the apparent effect of OSA on the height of children.
OSA-related pathophysiological alterations might also affect the height of children, which can be explained by the fact that, in the fully adjusted models, the OR of non-OSA children was twice as high as that of OSA (4.85 vs 2.15). Non-OSA children with low SWS experience GH deficiency, making the reduction in SWS a primary factor in height impairment and indicating that the influence of SWS on height is higher in non-OSA children than in OSA children, which further supports the independent correlation between SWS and height. In contrast, the main pathophysiological hypotheses for OSA, chronic intermittent hypoxia and sleep fragmentation is that they independently affect bone metabolism by increasing inflammatory cytokines (eg, IL-6, TNF -α) and oxidative stress, which is supported by studies showing that OSA-related growth impairment often results from complex interactions between hypoxia-inducible factors (HIF), inflammatory cytokines, and metabolic changes, which may alter the GH - IGF −1 axis independently of SWS effects.30,31 The impact of OSA-related characteristics on the height of children will be further explored in our subsequent studies.
The association between SWS deficiency and short stature is more significant in prepubertal children, which can be explained by the following reasons. First, epidemiological investigations show that the age range of onset of OSA in children is generally 4–6 years old,30 such that the age at which children first visit the doctor and complete a PSG is concentrated before puberty. In our sample, the proportions of adolescents among non-OSA and OSA children are 15.27% and 15.93%, respectively, suggesting that smaller sample sizes may lead to less robust findings in the adolescent subgroups. Second, the factors influencing the height of adolescents are complex and diverse. In addition to GH, sex hormones also affect the growth and development of adolescents.32,33 The age-related decrease in SWS proportion may represent an additional modulatory mechanism.34 We speculate that the diversity of factors influencing height during adolescence and the phenomenon that SWS decreases with age may mask the impact of SWS on height in adolescents. However, this speculation requires further verification in future studies with sufficient sample sizes to adequately address the issue.
Infancy (from birth to 1 year old) and adolescence (10–12 years old for females and 12–14 years old for males) are two peaks of height growth in children.35 In the present sample, children aged 2–9 years constituted up to 84.21% of the subjects, indicating that most subjects were in a period of steady height growth. Exploring the relationship between SWS and height during such a period may facilitate the reduction of confounding factors, such as the peak of sex hormone secretion. Thus, our results are likely to be reliable and stable among the group of children before puberty. In other subgroup analyses, independent correlations between the reduction of SWS and the increased risk of short stature were obtained in different sex and weight subgroups. Subgroup analyses based on OSA severity and arousal level in children with OSA also confirmed this association consistently (See Tables S5 and S6). These results demonstrate the stability of the finding that SWS is related to children’s height. Meanwhile, the relationship between SWS and short stature has not been obtained in some subgroups, such as overweight and adolescents, which could be attributed to insufficient sample size for robust comparisons. Further studies with sufficient sample sizes and adequate follow-up duration are expected to better investigate this issue.
Our findings support important clinical considerations. During children’s critical growth period, especially before puberty, the influence of sleep quality on height development should be considered, with PSG recommended for objective assessment when necessary. Reduced SWS was shown to be a risk for short stature in both non-OSA and OSA children. This suggests that sufficient SWS is of importance for all children, particularly for those with already compromised sleep. For children with OSA, clinicians should attach importance to the negative impact of sleep fragmentation and associated reductions in SWS on height. Notably, in children with conditions that impair sleep quality, such as attention-deficit hyperactivity disorder, autism spectrum disorder, or epilepsy, clinical management should extend beyond treating the primary disease to address potential growth impairments associated with disrupted sleep. For children with growth-impairing conditions (eg, GHD, Prader-Willi syndrome, etc)., sleep quality optimization may represent a novel therapeutic target in addition to growth hormone therapy. Future research should investigate the efficacy of behavioral interventions (eg, sleep hygiene education, regulated daylight exposure, and moderate exercise) and pharmacologic options on growth promotion in those children.36
This is the first study to report direct evidence of an association between sleep quality and height of children. A strength of this study is its large sample size. However, the study has limitations. First, given the study’s observational design, it did not establish a causal link between reduced SWS and impaired height. While follow-up data might provide further evidence of a relationship between SWS and children’s height, it will still be insufficient to demonstrate a causal link. Even an optimal study design examining this relationship that would employ concurrent measurement of PSG-based SWS%, GH levels, and height in a large sample of children, which would be logistically and fiscally prohibitive, would still yield only correlational data. Second, although night-to-night variations and the first-night effects on sleep quality and SWS cannot be ruled out by the one-night PSG recording employed by the current study, previous research has demonstrated that SWS exhibits high night-to-night reproducibility,37,38 largely attributable to its heritable nature.39 Third, although we adjusted for numerous potential confounders, unmeasured factors such as nutritional status, physical activity, parental height, and genetic predisposition may still influence our study results. Finally, the generalizability of these results is constrained by the clinically derived nature of the study cohort. Meanwhile, the sample included in our study was predominantly composed of subjects with OSA, and high proportion of patients with OSA means the findings may not be easily generalizable to the general pediatric population without sleep disorders. Future studies should further validate our results in longitudinal and population-based cohorts.
Conclusion
This study presents evidence that reduced SWS is linked to increased risk of short stature in both non-OSA children and those with OSA, with especially pronounced effects seen in prepubertal children. Our findings highlight the vital role of sufficient sleep quality in childhood growth and development, advocating for the inclusion of sleep evaluation and improvement in pediatric growth monitoring programs.
Abbreviations
GH, Growth Hormone; GHD, Growth Hormone Deficiency; PSG, Polysomnography; SWS, Slow Wave Sleep; REM, Rapid Eye Movement; NREM, Non-Rapid Eye Movement; OSA, Obstructive Sleep Apnea; AHI, Apnea-Hypopnea Index; BMI, Body Mass Index; WHO, World Health Organization; AASM, American Academy of Sleep Medicine; RERA, Respiratory Effort-Related Arousal; SOL, Sleep Onset Latency; TST, Total Sleep Time; SE, Sleep Efficiency; WASO, Wake After Sleep Onset; AI, Arousal Index; Spo2, Mean Blood Oxygen Saturation; N1%, Non-Rapid Eye Movement Sleep Stage 1; N2%, Non-Rapid Eye Movement Sleep Stage 2; REM%, Rapid Eye Movement Sleep Stage; OR, Odds Ratio; CI, Confidence Interval; SD, Standard Deviation; IGF-1, Insulin-Like Growth Factor-1; HIF, Hypoxia-Inducible Factors.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki and informed consent was obtained for each child and their guardian. The West China Hospital Research Ethics Board has approved the study (NO. 1119).
Acknowledgments
The authors sincerely thank all the patients who participated in this study. We are deeply grateful to the technical staff for conducting and scoring the overnight sleep recordings, as well as to the research support specialists for their invaluable contributions.
Author Contributions
Zhaohua Chen: Conceptualization, Writing - original draft, Visualization, Writing – review & editing, Formal analysis, Software, Investigation. Yuan Shi: Conceptualization, Writing - original draft, Writing - review & editing, Methodology, Software, Formal analysis, Investigation. Fei Lei: Data curation, Software, Writing - review & editing. Xujun Feng: Writing - original draft, Writing - review & editing, Methodology, Formal analysis, Investigation. Lu Tan: Investigation, Writing - review & editing, Supervision. Taomei Li: Investigation, Writing - review & editing, Supervision. Junying Zhou: Conceptualization, Writing - review & editing, Supervision. Yuanfeng Sun: Investigation, Writing - review & editing, Supervision. Investigation, Jiamin Liao: Investigation, Writing - review & editing, Supervision. Yun Li: Conceptualization, Writing - review & editing, Supervision. Zhoulong Yu: Conceptualization, Writing - review & editing, Supervision. Jian Jiao: Investigation, Writing - review & editing, Supervision. Ye Zhang: Investigation, Writing - review & editing, Supervision. Rong Ren: Investigation, Writing - review & editing, Supervision. Yanyan Wang: Investigation, Writing - review & editing, Project administration, Supervision. Larry D Sanford: Conceptualization, Writing - review & editing, Supervision. Michael V Vitiello: Conceptualization, Writing - review & editing, Supervision. Xiangdong Tang: Writing - review & editing, Conceptualization, Funding acquisition, Resources, Validation.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting or writing, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for the contents of this article.
Funding
This work was supported by the Ministry of Science and Technology of the People’s Republic of China (2021ZD0201900), National Natural Science Foundation of China (82120108002 and U21A20335).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Cavalieri S, Rotoli M. Huangdi Neijing: a classic book of traditional Chinese medicine. Recenti Prog Med. 1997;88(11):541–546.
2. Evans HM, Long JA. Characteristic effects upon growth, oestrus and ovulation induced by the intraperitoneal administration of fresh anterior hypophyseal substance. Proc Natl Acad Sci U S A. 1922;8(3):38–39. doi:10.1073/pnas.8.3.38
3. Smith PE. The disabilities caused by hypophysectomy and their repair: the tuberal (hypothalamic) syndrome in the rat. J Am Med Assoc. 1927;88(3):158–161. doi:10.1001/jama.1927.02680290020005
4. Ling N, Esch F, Böhlen P, Brazeau P, Wehrenberg WB, Guillemin R. Isolation, primary structure, and synthesis of human hypothalamic somatocrinin: growth hormone-releasing factor. Proc Natl Acad Sci U S A. 1984;81(14):4302–4306. doi:10.1073/pnas.81.14.4302
5. Raben MS. Preparation of growth hormone from pituitaries of man and monkey. Science. 1957;125(3253):883–884. doi:10.1126/science.125.3253.883
6. Hage C, Gan HW, Ibba A, et al. Advances in differential diagnosis and management of growth hormone deficiency in children. Nat Rev Endocrinol. 2021;17(10):608–624. doi:10.1038/s41574-021-00539-5
7. Hindmarsh PC, Dattani MT. Use of growth hormone in children. Nat Clin Pract Endoc. 2006;2(5):260–268. doi:10.1038/ncpendmet0169
8. Marino M, Li Y, Rueschman MN, et al. Measuring sleep: accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep. 2013;36(11):1747–1755. doi:10.5665/sleep.3142
9. Takahashi Y, Kipnis DM, Daughaday WH. Growth hormone secretion during sleep. J Clin Invest. 1968;47(9):2079–2090. doi:10.1172/jci105893
10. Honda Y, Takahashi K, Takahashi S, et al. Growth hormone secretion during nocturnal sleep in normal subjects. J Clin Endocrinol Metab. 1969;29(1):20–29. doi:10.1210/jcem-29-1-20
11. Holl RW, Hartman ML, Veldhuis JD, Taylor WM, Thorner MO. Thirty-second sampling of plasma growth hormone in man: correlation with sleep stages. J Clin Endocrinol Metab. 1991;72(4):854–861. doi:10.1210/jcem-72-4-854
12. Davidson JR, Moldofsky H, Lue FA. Growth hormone and cortisol secretion in relation to sleep and wakefulness. J Psychiatry Neurosci. 1991;16(2):96–102.
13. Brandenberger G, Gronfier C, Chapotot F, Simon C, Piquard F. Effect of sleep deprivation on overall 24 h growth-hormone secretion. Lancet. 2000;356(9239):1408. doi:10.1016/s0140-6736(00)02847-6
14. Ding X, Hwang FJ, Silverman D, et al. Neuroendocrine circuit for sleep-dependent growth hormone release. Cell. 2025;20:
15. World Health Organization Multicentre Growth Reference Study. WHO child growth standards: length/height-for-age, weight-for-age, weight-for length, weight-for-height and body mass index-for-age. Available from: https://www.who.int/tools/child-growth-standards/who-multicentre-growth-reference-study.
16. Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med. 1992;11(10):1305–1319. doi:10.1002/sim.4780111005
17. American Academy of Sleep Medicine. The AASM manual for the scoring of sleep and associated events. Available from: https://aasm.org/clinical-resources/scoring-manual/.
18. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. deliberations of the sleep apnea definitions task force of the American academy of sleep medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
19. Ruehland WR, Rochford PD, O’Donoghue FJ, Pierce RJ, Singh P, Thornton AT. The new AASM criteria for scoring hypopneas: impact on the apnea hypopnea index. Sleep. 2009;32(2):150–157. doi:10.1093/sleep/32.2.150
20. Katz ES, Moore RH, Rosen CL, et al. Growth after adenotonsillectomy for obstructive sleep apnea: an RCT. Pediatrics. 2014;134(2):282–289. doi:10.1542/peds.2014-0591
21. Chennaoui M, Léger D, Gomez-Merino D. Sleep and the GH/IGF-1 axis: consequences and countermeasures of sleep loss/disorders. Sleep Med Rev. 2020;49:101223. doi:10.1016/j.smrv.2019.101223
22. World Health Organization. Maternal, newborn, child and adolescent health and ageing. Available from: https://platform.who.int/data/maternal-newborn-child-adolescent-ageing/adolescent-data.
23. World Health Organization. Obesity and Overweight. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.Accessed.
24. Bixler EO, Fernandez-Mendoza J, Liao D, et al. Natural history of sleep disordered breathing in prepubertal children transitioning to adolescence. Eur Respir J. 2016;47(5):1402–1409. doi:10.1183/13993003.01771-2015
25. Mathews LS, Norstedt G, Palmiter RD. Regulation of insulin-like growth factor I gene expression by growth hormone. Proc Natl Acad Sci U S A. 1986;83(24):9343–9347. doi:10.1073/pnas.83.24.9343
26. Wang Y, Cheng Z, Elalieh HZ, et al. IGF-1R signaling in chondrocytes modulates growth plate development by interacting with the PTHrP/Ihh pathway. J Bone Miner Res. 2011;26(7):1437–1446. doi:10.1002/jbmr.359
27. Ranke MB, Wit JM. Growth hormone - past, present and future. Nat Rev Endocrinol. 2018;14(5):285–300. doi:10.1038/nrendo.2018.22
28. Van Cauter E, Plat L, Copinschi G. Interrelations between sleep and the somatotropic axis. Sleep. 1998;21(6):553–566.
29. Hindmarsh PC, Brook CGD. Final height of short normal children treated with growth hormone. Lancet. 1996;348(9019):13–16. doi:10.1016/S0140-6736(96)01038-0
30. Lévy P, Kohler M, McNicholas WT, et al. Obstructive sleep apnoea syndrome. Nat Rev Dis Primers. 2015;1:15015. doi:10.1038/nrdp.2015.15
31. Bhatt A, St-Laurent A, Graham ME. Pediatric obstructive sleep apnea. CMAJ. 2024;196(7):E241. doi:10.1503/cmaj.230897
32. Mauras N. Growth hormone and sex steroids. Endocrinol Metab Clin North Am. 2001;30(3):529–544. doi:10.1016/S0889-8529(05)70200-0
33. Kerstin A-W, Rosberg S. Analyses of 24-hour growth hormone profiles in children: relation to growth. J Clin Endocr Metab. 1988;67(3):493–500. doi:10.1210/jcem-67-3-493
34. Van Cauter E, Leproult R, Plat L. Age-related changes in slow wave sleep and REM sleep and relationship with growth hormone and cortisol levels in healthy men. JAMA. 2000;284(7):861–868. doi:10.1001/jama.284.7.861
35. Boas F. Observations on the growth of children. Science. 1930;72(1854):44–48. doi:10.1126/science.72.1854.44
36. De Bruin EJ, van Steensel FJ, Meijer AM. Cost-effectiveness of group and internet cognitive behavioral therapy for insomnia in adolescents: results from a randomized controlled trial. Sleep. 2016;39(8):1571–1581. doi:10.5665/sleep.6024
37. Iber C, Redline S, Gilpin AMK, et al. Polysomnography performed in the unattended home versus the attended laboratory setting—sleep heart health study methodology. Sleep. 2004;27(3):536–540. doi:10.1093/sleep/27.3.536
38. Ren R, Zhang Y, Feng X, et al. Association between slow wave sleep and blood pressure in insomnia. Sleep. 2024;48(1):zsae257. doi:10.1093/sleep/zsae257
39. Tang X, Yang L, Sanford LD. Individual variation in sleep and motor activity in rats. Behav Brain Res. 2007;180(1):62–68. doi:10.1016/j.bbr.2007.02.022
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
To Evaluate the Effect of Pediatric Massage Combined with Comprehensive Management on Growth Parameters and Biochemical Indicators in Children with Short Stature

Yang Q, Wu J, Deng X, Chen L, Chen Y
International Journal of General Medicine 2025, 18:4987-5000
Published Date: 31 August 2025
The Complex Interplay Between Sleep and Healthy Aging: A Scoping Review
Bragazzi NL, Mutti C, Ratti PL, Sardella A, Quattropani MC, Lodi R, Pizza F, Biscarini F, Bottignole D, Salvi M, Maggio M, Parrino L, Plazzi G, Franceschini C
Nature and Science of Sleep 2025, 17:3085-3100
Published Date: 29 November 2025