Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
The CO-MIND Study: Chronic Obstructive Pulmonary Disease Management in Daily Practice and Its Implications for Improved Outcomes According to GOLD 2019 Perspective
Authors Gunen H, Kokturk N ![]() , Naycı S
, Naycı S ![]() , Ozkaya S
, Ozkaya S ![]() , Yıldız BP
, Yıldız BP ![]() , Turan O
, Turan O ![]() , Gumus A, Akgun M
, Gumus A, Akgun M ![]() , Gurgun A, Ogus C, Mirici A, Sen E, Bayram N, Eken V
, Gurgun A, Ogus C, Mirici A, Sen E, Bayram N, Eken V ![]() , Erkus H
, Erkus H
Received 27 April 2022
Accepted for publication 2 August 2022
Published 18 August 2022 Volume 2022:17 Pages 1883—1895
DOI https://doi.org/10.2147/COPD.S372439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Hakan Gunen,1 Nurdan Kokturk,2 Sibel Naycı,3 Sevket Ozkaya,4 Birsen Pınar Yıldız,5 Onur Turan,6 Aziz Gumus,7 Metin Akgun,8 Alev Gurgun,9 Candan Ogus,10 Arzu Mirici,11 Elif Sen,12 Nazan Bayram,13 Volkan Eken,14 Hakan Erkus14
1Department of Pulmonary Medicine, Sureyyapasa Training and Research Centre for Chest Diseases and Thoracic Surgery, Istanbul, Turkey; 2Department of Pulmonary Medicine, Faculty of Medicine, Gazi University, Ankara, Turkey; 3Department of Pulmonary Medicine, Mersin University School of Medicine, Mersin, Turkey; 4Department of Pulmonary Medicine, VM Medical Park Samsun Hospital, Samsun, Turkey; 5University of Health Sciences, Yedikule Chest Disease and Surgery Training and Research Hospital, Pulmonology, Istanbul, Turkey; 6Department of Pulmonary Medicine, Izmir Katip Çelebi University, İzmir, Turkey; 7Department of Pulmonary Medicine, Recep Tayyip Erdogan University, Faculty of Medicine, Rize, Turkey; 8Department of Pulmonary Medicine, Atatürk University School of Medicine, Erzurum, Turkey; 9Department of Pulmonary Medicine, Ege University School of Medicine, İzmir, Turkey; 10Department of Pulmonary Medicine, Akdeniz University Medical Faculty, Antalya, Turkey; 11Department of Pulmonary Medicine, Canakkale 18 Mart University, Canakkale, Turkey; 12Department of Pulmonary Medicine, Ankara University School of Medicine, Ankara, Turkey; 13Department of Pulmonary Medicine, Gaziantep University, Sahinbey Research Hospital, Gaziantep, Turkey; 14GlaxoSmithKline, Istanbul, Turkey
Correspondence: Hakan Gunen, Department of Pulmonary Medicine, Sureyyapasa Training and Research Centre for Chest Diseases and Thoracic Surgery, Istanbul, Turkey, Tel +90 532 621 16 99, Fax +90 216 421 41 10, Email [email protected] Nurdan Kokturk, Department of Pulmonary Medicine, Faculty of Medicine, Gazi University, Ankara, Turkey, Tel +90 532 627 91 11, Fax +90 312 212 90 19, Email [email protected]; [email protected]
Purpose: GOLD 2019 proposed a novel treatment decision tool for follow-up based on the predominant trait (exacerbation or dyspnea) of patients, alongside treatment escalation and de-escalation strategies. This study was designed to provide an up-to-date snapshot of patient and disease characteristics, treatment pathways, and healthcare resource use (HRU) in COPD in real life, and comprehensively examine patients considering GOLD 2019 recommendations.
Patients and Methods: This mixed design, observational, multicenter (14 pulmonology clinics) study included all patients with a documented COPD diagnosis (excluding asthma-COPD overlap [ACO]) for ≥ 12 months, aged ≥ 40 years at diagnosis who had a COPD-related hospital visit, spirometry test and blood eosinophil count (BEC) measurement under stable conditions within the 12 months before enrollment between February and December 2020. Data were collected cross-sectionally from patients and retrospectively from hospital medical records.
Results: This study included 522 patients (GOLD group A: 17.2%, B: 46.4%, C: 3.3%, D: 33.1%), of whom 79.5% were highly symptomatic and 36.2% had high risk of exacerbation. Exacerbations (n = 832; 46.6% moderate, 25.5% severe) were experienced by 57.5% of patients in the previous 12 months. Inter-rater agreement between investigators and patients regarding the reason for visit was low (κ coefficient: 0.338, p = 0.001). Inhaled treatment was modified in 88 patients at index, mainly due to symptomatic state (31.8%) and exacerbations (27.3%); treatment was escalated (57.9%, mainly switched to LABA+LAMA+ICS), inhaler device and/or active ingredient was changed (36.4%) or treatment was de-escalated (5.7%). 27% had ≥ 1 hospital overnight stay over 12 months. Emergency department visits and days with limitation of daily activities were higher in group D (p < 0.001).
Conclusion: Despite being on-treatment, many patients with COPD experience persistent symptoms and exacerbations requiring hospital-related HRU. A treatable trait approach and holistic disease management may improve outcomes by deciding the right treatment for the right patient at the right time.
Keywords: COPD, GOLD, exacerbation, COPD treatment, eosinophilia
Introduction
Chronic obstructive pulmonary disease (COPD) is a global health concern associated with significant morbidity and mortality. In 2019, COPD affected 212 million people worldwide and was the third leading cause of mortality, resulting in 3.28 million deaths.1 Furthermore, COPD was among the top-ranked causes of disability-adjusted life-years (DALYs): the sixth in all ages and the fourth in adults aged 50–74 years.2 In Turkey, the prevalence of COPD is high, as shown by estimates in adults aged ≥40 years, which ranged from 9.1% to 19.1% for fixed airway obstruction.3–6 In addition, COPD accounted for 5% of all deaths in Turkey in 2019.7,8 With the increasingly aging population and high smoking rates in Turkey,7,8 the prevalence of COPD is expected to rise over the coming decades.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) works extensively to increase awareness of COPD and improve its prevention, diagnosis, and treatment worldwide.9 Since the release of the first GOLD strategy document for COPD in 2001, there have been significant changes to recommendations for evaluating the disease. Until 2011, a forced expiratory volume in one second (FEV1)-based classification was exclusively recommended, but the GOLD panelists have since proposed an additional “ABCD” tool that includes the Modified Medical Research Council (mMRC) Dyspnea Scale, the COPD assessment test (CAT) and exacerbation history from that year, thus considering the impact of symptoms and exacerbations on disease progression. The GOLD 2019 revision proposed, for the first time, a new treatment decision tool for follow-up based on the predominant trait (exacerbation or dyspnea) of patients, alongside treatment escalation and de-escalation strategies. Furthermore, blood eosinophil count (BEC) was suggested as a biomarker to predict the potential efficacy of inhaled corticosteroids (ICS) in preventing exacerbations.10
To the best of our knowledge, there have been no data published following comprehensive investigation of the distribution of patients with COPD according to GOLD 2019 guideline recommendations. This real-life study was designed to provide an up-to-date snapshot of patient and disease characteristics, treatment pathways, and healthcare resource use, in order to give health-care professionals managing COPD a broader perspective that may aid daily clinical practice.
Materials and Methods
Study Design
The CO-MIND (COPD Management IN Daily Practice) study was an observational, multicenter study conducted by pulmonologists from February–December 2020 in 14 hospitals across Turkey. The study had a mixed method, where data were collected from patients with COPD both cross-sectionally and retrospectively. COPD patients who naturally present at the hospital were invited to participate in the study and data were collected from these face-to-face patient visits. Retrospective data of the patients who were included into the study covered a 12-month period and were obtained from paper-based or electronic hospital medical records.
The study was conducted in accordance with the Declaration of Helsinki 2008, the Guidelines for Good Pharmacoepidemiology Practices, The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use Good Clinical Practice guidelines, and applicable local regulations. It was approved by the University of Health Sciences Turkey, Ethics Committee of Sureyyapasa Research Center for Chest Diseases and Thoracic Surgery. Signed informed consent forms were obtained from study participants.
Study Population
All patients with COPD who attended the investigator site during the patient recruitment period were invited to participate in the study. Those who fulfilled the following eligibility criteria were enrolled: patients ≥40 years of age at the time of COPD diagnosis, a documented COPD diagnosis according to the GOLD definition at least one year before enrolment (the index date), current or former tobacco smoking history of ≥10 pack-years, no current diagnosis of asthma, a prior visit for COPD-related medical care in the 12 months before the index date, spirometry and BEC measured under stable conditions (no COPD exacerbation in the four weeks prior to measuring spirometry and no parasitic infestation or COPD exacerbation in the four weeks prior to measuring BEC) within the 12 months prior to the index date.
Patients with the following history were excluded: participated in a clinical/interventional study that might influence medical treatment during the study observation period, diagnosed with asthma-COPD overlap (ACO) by a physician, or severe psychiatric illness or other diseases that impaired cognitive ability and/or the patient’s routine COPD treatment.
Assessments
Retrospectively collected data included BEC, spirometry (FEV1, forced vital capacity [FVC], and FEV1/FVC), current COPD inhaled treatment on the day of study visit, exacerbations within the 12 months prior to enrolment, and physician-diagnosed comorbidities. Additionally, patients provided information on the number of nights spent in hospital, emergency department (ED) visits, missed workdays and days with limitation of daily activities in the past 12 months.
The following data were obtained cross-sectionally at a single face-to-face hospital visit: demographics (age, gender, body mass index (BMI)), smoking history (active/former smokers and smoking load), level of education (< or ≥ high school graduate), monthly household income (equal to or higher than the national minimum wage), COPD history, inhaled treatment modification on visit day (escalation or de-escalation) and reason for visit (routine follow-up, dyspnea, exacerbations or other) according to both patient and investigator. Additionally, scores for the mMRC Dyspnea Scale (0–4 stage breathlessness scale ranging from 0 [I only get breathless with strenuous exercise] to 4 [I am too breathless to leave the house]) and CAT (the 8-item, 5-point COPD specific assessment scale ranging from 0 to 40, corresponding to the best and worst health status, respectively) were collected.
The study assessed the distribution of participants by degree of airflow limitation, as per GOLD grading: mild, post bronchodilator (PB) FEV1 ≥80%; moderate, PB FEV1 <80% to ≥50%; severe, PB FEV1 <50% to ≥30% and very severe, PB FEV1 <30%. Considering the descriptive nature of the study, patients were classified according to the GOLD 2019 ABCD group definitions for exacerbation risk and symptom levels, even though they were receiving treatment on the day of the study visit: Group A (low risk, less symptoms: mMRC 0–1 or CAT <10, and 0 or 1 moderate exacerbations not leading to hospital admission in the last 12 months); Group B (low risk, more symptoms: mMRC ≥2 or CAT ≥10, and 0 or 1 moderate exacerbations not leading to hospital admission); Group C (high risk, less symptoms: mMRC 0–1 or CAT <10, and ≥2 moderate exacerbations or ≥1 leading to hospitalization); Group D (high risk, more symptoms: mMRC ≥2 or CAT ≥10, and ≥2 moderate exacerbations or ≥1 leading to hospitalization). Mild and moderate exacerbations were defined according to GOLD descriptions: mild, treated with short-acting bronchodilators (SABDs) only; moderate, treated with SABDs plus antibiotics and/or oral corticosteroids. However, a slightly modified definition (hospitalization or staying at the ED for ≥24 hours) was used in the study for severe exacerbation due to the high frequency of emergency unit attendance for non-urgent outpatient visits in clinical practice in Turkey. Patients were split into three groups based on BEC, as proposed by GOLD guidelines: <100 cells/μL, ≥100 to ≤300 cells/μL, and >300 cells/μL. Demographics, clinical and laboratory characteristics, and healthcare resource use in the past 12 months were described for each GOLD group. The concordance between investigator- and patient-reported reasons for visiting the hospital on the index date was evaluated based on the percent agreement of these groups.
Statistical Analysis
Statistical analysis was conducted using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY). The suitability of the variables to the normal distribution was examined by visual and analytical methods (Kolmogorov–Smirnov/Shapiro–Wilk tests).
Demographic features and clinical parameters were tabulated for descriptive statistical analyses. The Chi-square (χ2) test was used to compare categorical data, while numerical data were analyzed using the Friedman test. Post-hoc processes were applied to determine the group that made the difference for the p values found to be significant in Chi-square (χ2) comparisons. Change over time was evaluated by Wilcoxon test. Data were expressed as mean (standard deviation), median (minimum–maximum) and percent (%), where appropriate, and p < 0.05 was considered statistically significant. Kappa analyses were used to examine the conformity of patient and physician evaluations in terms of the reasons for visiting hospital. Comparisons of parameters and ordinal variables that do not distribute normally were made using Mann–Whitney U-test, Wilcoxon test and Kruskal–Wallis test. Pairwise comparisons were made using Mann–Whitney U-test and interpreted using Bonferroni Correction for cases where the differences were significant.
Results
Patient Characteristics
A total of 522 patients (92.9% male) with a mean (SD) age of 65.90 (8.66) were included in the study. Key demographics of the study population are summarized in Table 1.
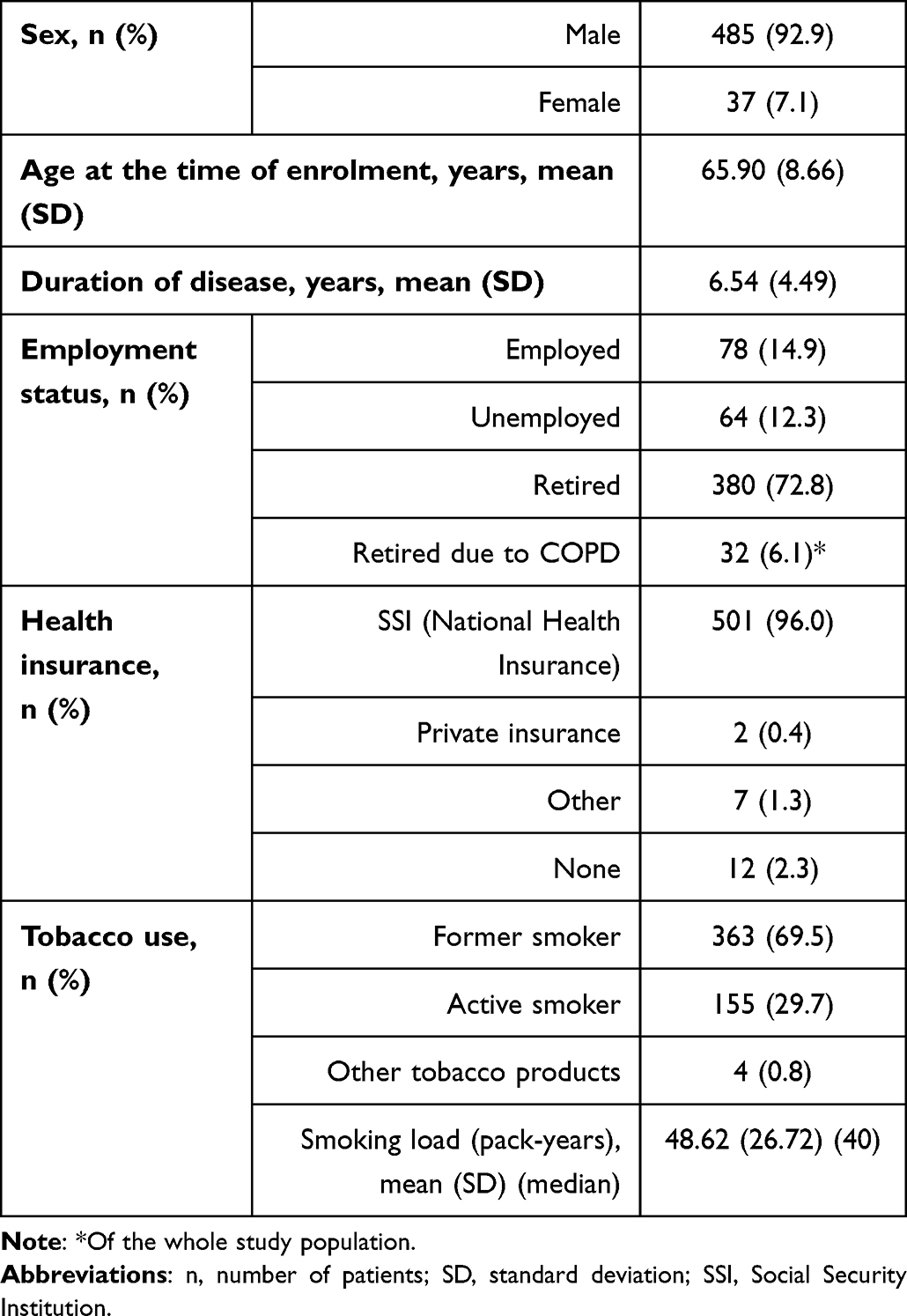 |
Table 1 Patients’ Demographics (n = 522) |
Burden of Symptoms and Risk of Exacerbation (ABCD Groups)
Overall, 79.5% (n = 415) of patients were highly symptomatic based on mMRC or CAT scores, and 36.2% (n = 189) had high risk of exacerbation. The most frequently observed group was B (n = 242; 46.4%), followed by D (n = 173; 33.1%), A (n = 90; 17.2%), and C (n = 17; 3.3%).
Patient demographics by ABCD group are presented in Table 2. The distribution of patients by level of education was statistically significantly different across the groups due to the low percentage of high school or university graduates in group D (21.4%) (p < 0.001). The groups also differed in terms of employment status; the percentage of retired or unemployed patients was 93.6% in group D, compared to 75.6–81.8% in the other groups (p = 0.004). The percentage of patients with a monthly household income equal to or below the minimum wage was highest in group D (78.8%) and lowest in group A (53.3%) (p < 0.001). Patients in group D were less educated (p < 0.001), had a lower employment rate (p = 0.004), and a lower monthly household income (p < 0.001). The groups were similar regarding current or former tobacco use but smoked pack-years were significantly highest in group C (p < 0.001).
 |
Table 2 Demographic Characteristics by Patient Groups |
Table 3 reports patients’ clinical and laboratory characteristics by ABCD group.
 |
Table 3 Distribution of Patients According to Clinical and Laboratory Characteristics |
Airflow Limitation
Patients most frequently had GOLD grade 2 (moderate; 42.3%) airflow limitation. As shown in Table 3, there were significant differences across the ABCD groups regarding FEV1, FVC and FEV1/FVC values. Airflow limitation was less severe in groups A and B than in groups C and D. Group B patients had better spirometry results compared to group D (FEV1: 56% vs 44%; FVC: 70.5% vs 62%; FEV1/FVC: 63% vs 56%; p < 0.001 for all).
Dyspnea Assessment
As shown in Table 3, CAT and mMRC scores, and oxygen saturation varied among the ABCD groups. As expected, CAT and mMRC scores were significantly higher in groups B and D, whereas oxygen saturation was highest in group A (p < 0.001 for all). CAT and mMRC scores were significantly higher in group D than in group B (p < 0.001).
Exacerbations
Overall, 300 patients (57.5%) had 832 exacerbations in the 12 months prior to the index date, of which 388 (46.6%) were moderate and 212 (25.5%) were severe. Of these patients, 44.7% (n = 134), 53% (n = 159) and 40.3% (n = 121) experienced mild, moderate, and severe exacerbations, respectively. As shown in Table 3, the mean number of mild exacerbations did not differ across the ABCD groups.
Figure 1 presents the distribution of patients with moderate and/or severe exacerbations in the 12 months before index. Around one quarter of the study population (n = 121; 23.2%) had at least one severe exacerbation, whereas the frequencies of those who experienced 1 and ≥2 moderate exacerbations were 15.7% (n = 82) and 14.8% (n = 77), respectively. In total, 219 patients (42%) had at least one moderate or severe exacerbation.
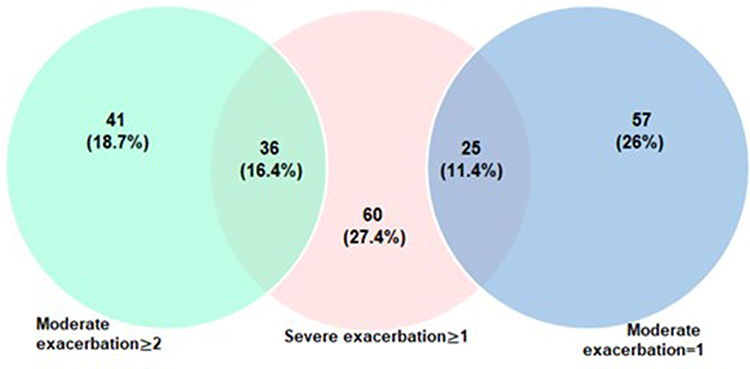 |
Figure 1 Distribution of moderate and severe exacerbations across patients (n = 219). |
Patients who experienced an exacerbation in the past year reported that they most frequently attended the ED for treatment (149 of 291 patients [51.2%], data were missing for nine patients).
Blood Eosinophil Count (BEC)
Overall, the BEC (mean (SD)) of the study population was 199.3 (189.9) cells/μL (median: 160). Almost half (48.7%) of patients had a BEC of ≥100 cells/μL to ≤300 cells/μL, while 162 (31%) patients had BEC <100 cells/μL and 106 (20.3%) patients had BEC >300 cells/μL. The percentages of ICS users in different BEC categories were as follows: 80.2% (BEC <100 cells/μL), 66.5% (100 cells/μL≤ BEC ≤300 cells/μL), and 67.9% (BEC >300 cells/μL).
Comorbidities
Hospital records revealed that 57.5% of patients had comorbidities, most commonly involving the cardiovascular system (42.1%), followed by the endocrine (14.4%) and renal (10%) systems. The ABCD groups differed regarding the distribution of cardiovascular (p = 0.039) and renal comorbidities (p = 0.016) (Table 3).
Reasons for Visit
According to the patients, the most common reason for attending a hospital on the index day was a routine follow-up visit (61.9%), whereas investigators noted that the principal cause of hospital visits was dyspnea (42.2%) (Table 4). The study population and investigators reported that exacerbations led to hospital visits in 5.6% and 15.7% of cases, respectively. There was low inter-rater agreement regarding the reason for visit between the investigators and patients (κ coefficient: 0.338, p = 0.001). The distribution of patients according to reason for visit differed across the ABCD groups; routine follow-up was the main reason for visit in group A, dyspnea was more common in groups B, C and D, and exacerbations were more frequently reported in groups C and D.
 |
Table 4 Inter-Rater Agreement About Reason for Visit |
COPD Treatment at Index
Overall, 71.1% of study participants were on ICS-containing regimens. The frequency of ICS use in the A, B, C and D groups was 42.8%, 72.7%, 68.8% and 83.8%, respectively. Most patients (51.9%) were on inhaled triple therapy (long-acting beta agonist [LABA]+ long-acting muscarinic antagonist [LAMA]+ICS), either in the form of single inhaler triple therapy (SITT; 13.2%) or multiple inhaler triple therapy (MITT; 86.8%). Other treatments included LABA+ICS (16%), LAMA (14%) and LABA+LAMA (11%).
Of the 82 patients who visited hospital on the index date due to exacerbations (according to the physicians), 72 (87.8%) were on ICS-containing regimens: two (2.4%) were on ICS, 18 (21.9%) were on LABA+ICS, and 52 (63.4%) were on LABA+LAMA+ICS.
Oral medications and bi-level/continuous positive airway pressure machines were used, in addition to inhaled medications, by 42 (8%) and 17 (3.2%) patients, respectively. Most of the inhaler devices used by the study participants for maintenance treatment were dry powder inhalers (707 devices; 74%) followed by metered dose inhalers (156 devices; 16.3%) and nebulizers (93 devices: 9.7%).
Treatment Modification on the Index Date
As shown in Table 5, the inhaled COPD medications of 88 patients were modified on the index date. The ABCD groups differed regarding the percentage of patients in whom the inhaled treatment was changed: 5.5% in A, 19.4% in B, 18.7% in C, and 19.1% in D (p < 0.038). The most common treatment modification was treatment escalation, which occurred in 51 patients (57.9%), of whom 42 switched to LABA+LAMA+ICS. Inhaler device and/or active ingredient was changed in 32 patients (36.4%) without escalation or de-escalation of treatment. In total, treatment was de-escalated in five (5.7%) patients, all of whom had been receiving triple therapy prior to modification. Following treatment modification, ICS-containing regimen use increased from 71.1% (n = 371) to 74.3% (n = 388) in total.
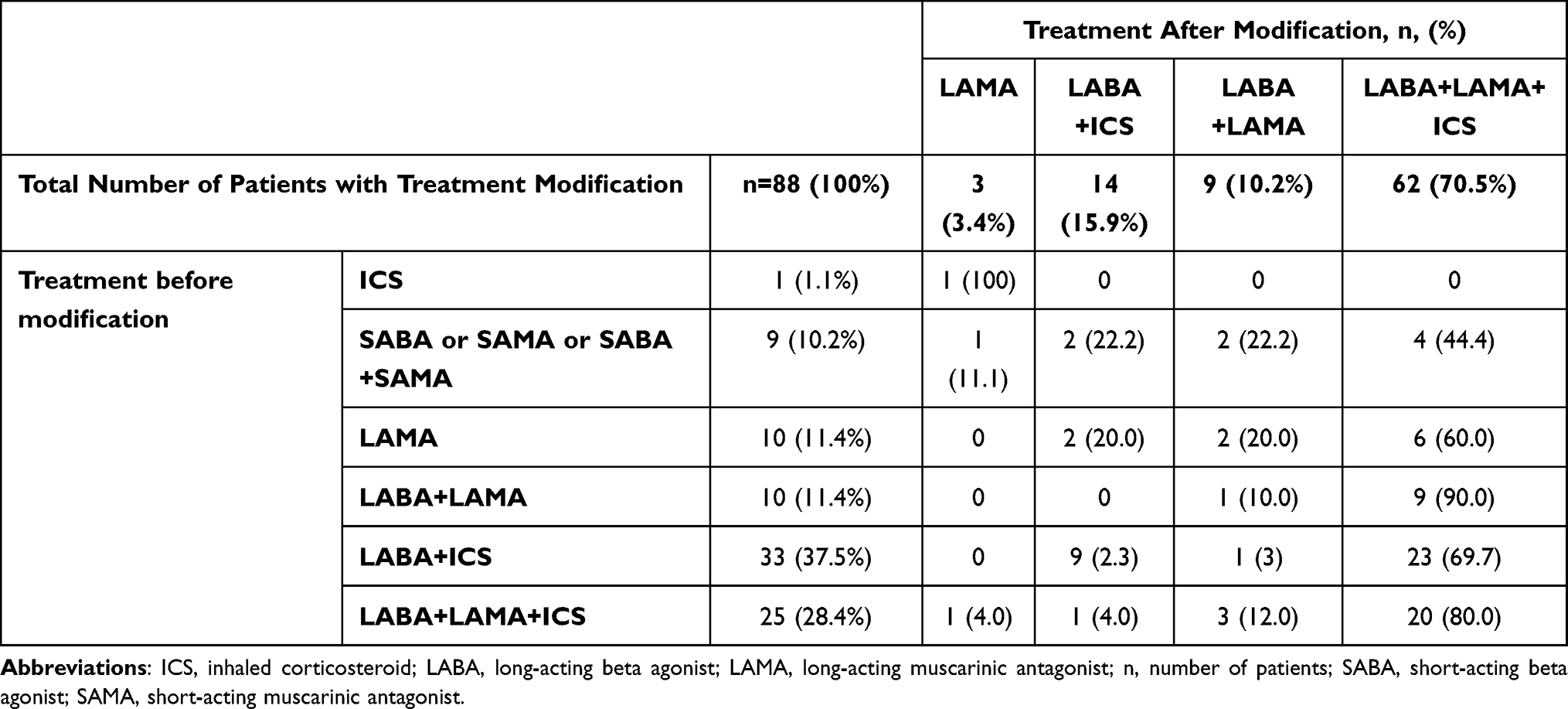 |
Table 5 Treatment Modifications on the Index Date |
Among patients whose inhaled maintenance treatments were changed on the index date, 44 had experienced moderate to severe exacerbations in the 12 months prior to the study visit. Treatment was escalated in 61.4% of these patients, with most switched to triple combination therapy.
The reasons for treatment change were reported in 35 of 88 patients and were usually multifactorial. Symptomatic state was the most frequent reason for treatment switch (n = 28; 31.8%) and led to treatment modification mainly in group B (n = 13) and group D (n = 12). Treatment was modified due to exacerbations in 24 patients (27.3%), most frequently in group B (n = 13) and group D (n = 8).
Healthcare Resource Use and Limitation of Daily Activities
Table 6 presents data on healthcare resource use and limitation of daily activities due to COPD in the 12 months prior to the study visit. A total of 141 patients (27%) had at least one hospital overnight stay over the 12 months; the number of nights spent in hospitals (mean (SD)) was 12.6 (10.5) and did not differ across the ABCD groups. ED visits were highest in group D and constituted 80.1% (507 of 633) all ED visits. The ABCD groups were comparable regarding the number of missed workdays, but the number of days with limitation of daily activities was higher in group D (p < 0.001) (Table 6).
 |
Table 6 Healthcare Resource Use and Limitation of Daily Activities Due to COPD in the Previous 12 Months by ABCD Group |
Discussion
To our knowledge, this is the first study to perform a comprehensive examination of patients with COPD considering the GOLD 2019 recommendations for patient assessments. We report a low rate of physician-patient agreement regarding the reasons for hospital visits (59%), and a low percentage of treatment modification (17%) in a COPD patient population with high symptomatic burden (80%) and an elevated risk of exacerbation (36%). These findings reveal the obvious need for improvement in clinical management of patients with COPD in daily practice.
Excluding severity of airflow limitation from the combined assessment tool as of 2017 and considering only moderate and severe exacerbations for categorization significantly affected the distribution of patients across ABCD groups, resulting in a transition from groups C and D to groups A and B, respectively. Therefore, the distribution of patients across ABCD groups in the current study was markedly different from the cross-sectional ALPHABET study conducted in Turkey that analyzed the group allocation of patients with COPD according to GOLD 2013 recommendations, which classified all patients with severe or very severe airflow limitation in high-risk exacerbation groups (group C or D).11 Comparatively, 22.2% and 40.1% of patients in groups A and B, respectively, had severe or very severe airflow limitation in the present study. While most patients were in group A (41.1%), followed by group D (25%), B (20.8%) and C (13.2%) in the ALPHABET study,11 we observed that more patients fulfilled group B criteria (46.4%) compared to groups D (33.1%), A (13.2%) and C (3.3%) in the present study. A similar distribution was reported in the UNLOCK real-life study from Greece, which used GOLD 2018 categorization.12
It is noteworthy to mention that, in the current study, 8.7% of patients had mild airflow limitation in group D who, by definition, have high exacerbation risk and symptomatic burden. These observations highlight how complex patient presentations in a single group can be and demonstrate the benefits of using a simpler tool at follow-up to “review-assess-adjust” pharmacological treatment based on the patient’s predominant trait, allowing a more personalized management of COPD in clinical practice.10
The current GOLD strategy document strongly supports adding ICS to long-acting bronchodilators in case of high risk of exacerbations, high BEC (>300 cells/µL) or in those with a history of asthma. Furthermore, it is recommended to consider ICS use in patients with a history of one moderate exacerbation or BECs between 100 and 300 cells/µL.13 In this study, the percentage of ICS users was high across all BEC ranges. This can be attributed to insufficient implementation of GOLD recommendations regarding the use of ICS within the short time elapsed since publication of the 2019 strategy document. Additionally, the fact that 57.5% of the cohort had COPD exacerbations within the previous 12 months, and the main reasons for attending the clinics on the study visit day were dyspnea (42.2%) and exacerbation (15.7%) as per investigators’ judgement, might at least partly explain the high preference for ICS-containing regimens in this study. At this point, we need to emphasize the low concordance we observed between investigators and patients regarding the reason for visit (κ coefficient 0.338, p = 0.001). In contrast to the investigators, patients mostly reported that they attended the clinics for routine follow-up (61.9%). This discordance deserves attention, and its underlying causes need clarification to improve the effectiveness of patient management. On the other hand, the high rates of persistent symptoms and exacerbations despite being on-treatment draw attention to the importance of choosing the right treatment for the right patient at the right time.
Evidence shows that combining ICS with one or more long-acting bronchodilators improves lung function, health status and symptoms, and reduces COPD exacerbations.14–18 This study reports that 71.1% of patients were using ICS on the study visit date, which further increased to 74.3% following treatment change. ICS-containing regimens were mostly prescribed to patients with higher symptom burden and/or risk of exacerbations. LABA+LAMA+ICS combination was the most prescribed regimen. This is in line with GOLD recommendations on the use of triple therapy in symptomatic and exacerbating patients with COPD despite being on dual therapy, as evidenced by Phase III studies14–18 which showed the superiority of LABA+LAMA+ICS over dual therapy (LABA-ICS or LABA-LAMA) regarding several outcomes, including moderate and severe exacerbations, symptoms, airflow limitation, and quality of life. In the present study, escalation was the predominant type of treatment modification (57.9%), while de-escalation was only observed in 5.7% of treatment modification. The high rates of clinic attendance due to exacerbations or dyspnea according to physicians’ judgements might have had an impact on this finding. Treatment modification was limited to device and/or active substance change in approximately one-third of patients, confirming that the GOLD recommendation to review these factors in case of treatment ineffectiveness was considered in daily practice. However, the wide range of available inhaler devices increases therapeutic options but renders treatment more complex. In this study, incorrect use of inhaler devices and adherence issues were the reasons for treatment modification in 17% of patients whose medications were switched on the study visit date and were mainly observed in group D patients who had the most burdensome disease.
Another important aspect of COPD management is the economic burden it places on patients and health-care systems. In this study, we observed impaired productivity, which was most burdensome in group D, among patients who were the most symptomatic and had a higher exacerbation risk. This was not translated into days of work lost, as more than two-thirds of the study population (approximately 80% in group D) had already retired. ED visits were also more common in group D. Since only hospitalizations due to COPD exacerbations were considered, no patients from groups A and B had been hospitalized in line with the definition of ABCD groups. These findings are in line with other real-world studies19–24 and confirm the economic burden of COPD.
The main limitation of the study is its retrospective design, which restricted access to information on several outcomes due to unrecorded data in hospital records. Another limitation was that we did not assess adherence, which is an important factor that may impact the effectiveness of inhaled medications. Additionally, the study population consisted of patients who attended tertiary clinics, who therefore may represent a patient population with more severe disease. However, inhaled maintenance treatments can only be initiated by pulmonologists and referral from primary care is not required to attend secondary and tertiary hospitals. It should be emphasized that the healthcare resource utilization data are restricted to hospitalizations and ED visits but do not cover interventions, non-pharmacological management, and treatment-related costs. Additionally, we ascertained which values were responsible for statistical significance by using multiple pairwise comparisons between the groups, but that type I error was controlled using Bonferroni correction, as mentioned in the statistical analysis section.
Conclusions
It was shown in this study that 79.5% (n = 415) of COPD patients were highly symptomatic and 36.2% (n = 189) of patients had a high risk of exacerbation despite being on treatment, treatment adjustments were done largely in the direction of escalation (57.9%), as well as the physician-patient agreement regarding the reasons for hospital visits was low. All of these important points about COPD management reveal the obvious need for improvement in the clinical approach and management of patients with COPD in daily practice. Besides, the higher hospital-related healthcare resource use in patients with high symptomatic burden and exacerbation risk indicates that patients with COPD deserve a treatable trait approach and holistic disease management, which aim to improve outcomes by deciding the right treatment for the right patient at the right time.
Acknowledgments
The authors thank Dr. Idilhan Baloglu Ar for organizing and presenting the data by compiling their comments, citing references, and providing language support. We also would like to thank Evrim Koseoglu, Sinan Ozgur Aydin and their team from CRM CRO (Ankara, Turkey) for their support and follow-up during the execution of the study.
Disclosure
This study was funded by GlaxoSmithKline (GSK study 208435). Volkan Eken and Hakan Erkus are GlaxoSmithKline Pharmaceuticals employees and shareholders. The other authors report no other conflicts of interest in this study.
References
1. GBD 2019 cause and risk summaries. Chronic obstructive pulmonary disease - level 3 cause. Available from: https://www.healthdata.org/results/gbd_summaries/2019/chronic-obstructive-pulmonary-disease-level-3-cause.
2. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019 [published correction appears in Lancet. 2020 Nov 14;396(10262):1562]. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
3. Kocabas A, Hancioglu A, Turkyilmaz S, et al. Prevalence of COPD in Adana, Turkey (BOLD-Turkey Study). Proc Am Thorac Soc. 2006;3(Suppl):A543.
4. Gunen H, Hacievliyagil SS, Yetkin O, Gulbas G, Mutlu LC, Pehlivan E. Prevalence of COPD: first epidemiological study of a large region in Turkey. Eur J Intern Med. 2008;19(7):499–504. doi:10.1016/j.ejim.2007.06.028
5. Arslan Z, Ilgazlı A, Etiler N, Hamzaoğlu O. Prevalence of chronic obstructive pulmonary disease in Kocaeli: an industrialised city in Turkey. Balkan Med J. 2013;30(4):387–393. doi:10.5152/balkanmedj.2013.8042
6. Örnek T, Tor M, Kıran S, Atalay F. Prevalence of chronic obstructive pulmonary disease in Zonguldak province of Turkey. Tuberk Toraks. 2015;63(3):170–177. doi:10.5578/tt.9582
7. Türkiye İstatistik Kurumu (TÜİK), Ölüm ve Ölüm Nedeni İstatistikleri 2019, Turkish [Turkish Statistical Institute (TUIK), Death and Cause of Death Statistics 2019, Turkish]. Available from: https://data.tuik.gov.tr/Bulten/Index?p=Olum-ve-Olum-Nedeni-Istatistikleri-2019-33710.
8. Başara BB, Çağlar İS, Aygün A, et al. Sağlık Bilgi Sistemleri Genel Müdürlüğü, Sağlık Bakanlığı, Ankara, 2019, Turkish [General Directorate of Health Information Systems, Ministry of Health, Ankara, 2019, Turkish]. Available from: https://sbsgm.saglik.gov.tr/Eklenti/40564/0/saglik-istatistikleri-yilligi-2019pdf.pdfistatistikleri-yilligi-2019pdf.
9. Global initiative for chronic obstructive lung disease. Available from: https://goldcopd.org/.
10. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2019 report. Available from:https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf.
11. Gunen H, Yilmaz M, Aktas O, et al. Categorization of COPD patients in Turkey via GOLD 2013 strategy document: ALPHABET study. Int J Chron Obstruct Pulmon Dis. 2015;10:2485–2494. doi:10.2147/COPD.S87464
12. Tsiligianni I, Kampouraki M, Ierodiakonou D, Poulonirakis I, Papadokostakis P. COPD patients’ characteristics, usual care, and adherence to guidelines: the Greek UNLOCK study. Int J Chron Obstruct Pulmon Dis. 2019;14:547–556. doi:10.2147/COPD.S185362
13. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2022 report. Available from: https://goldcopd.org/2022-gold-reports-2.
14. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
15. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
16. Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, Phase 3 randomised controlled trial [published correction appears in Lancet Respir Med. 2018 Oct 4; [published correction appears in Lancet Respir Med. 2019 Feb;7(2):e9]. Lancet Respir Med. 2018;6(10):747–758. doi:10.1016/S2213-2600(18)30327-8
17. Singh D, Papi A, Corradi M, et al. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group, randomised controlled trial. Lancet. 2016;388(10048):963–973. doi:10.1016/S0140-6736(16)31354-X
18. Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial [published correction appears in Lancet. 2018 Feb 26]. Lancet. 2018;391(10125):1076–1084. doi:10.1016/S0140-6736(18)30206-X
19. Foo J, Landis SH, Maskell J, et al. Continuing to confront COPD international patient survey: economic impact of COPD in 12 countries. PLoS One. 2016;11(4):e0152618. doi:10.1371/journal.pone.0152618
20. Patel JG, Coutinho AD, Lunacsek OE, Dalal AA. COPD affects worker productivity and health care costs. Int J Chron Obstruct Pulmon Dis. 2018;13:2301–2311. doi:10.2147/COPD.S163795
21. Souliotis K, Kousoulakou H, Hillas G, Tzanakis N, Toumbis M, Vassilakopoulos T. The direct and indirect costs of managing chronic obstructive pulmonary disease in Greece. Int J Chron Obstruct Pulmon Dis. 2017;12:1395–1400. doi:10.2147/COPD.S132825
22. Wacker ME, Jörres RA, Schulz H, et al. Direct and indirect costs of COPD and its comorbidities: results from the German COSYCONET study. Respir Med. 2016;111:39–46. doi:10.1016/j.rmed.2015.12.001
23. Rehman AU, Hassali MAA, Muhammad SA, Harun SN, Shah S, Abbas S. The economic burden of chronic obstructive pulmonary disease (COPD) in Europe: results from a systematic review of the literature. Eur J Health Econ. 2020;21(2):181–194. doi:10.1007/s10198-019-01119-1
24. Gutiérrez Villegas C, Paz-Zulueta M, Herrero-Montes M, Parás-Bravo P, Madrazo Pérez M. Cost analysis of chronic obstructive pulmonary disease (COPD): a systematic review. Health Econ Rev. 2021;11(1):31. doi:10.1186/s13561-021-00329-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Antibiotic Prescriptions in Hospitalized Patients with an Exacerbation COPD and a Proven Influenza or RS Virus Infection
van Brummelen S, Tramper-Stranders G, Jonkman K, de Boer G, in 't Veen J, Braunstahl GJ
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1261-1267
Published Date: 1 June 2022
Pulmonologists’ Opinion on the Use of Inhaled Corticosteroids in Chronic Obstructive Pulmonary Disease Patients in Spain: A Cross-Sectional Survey
Miravitlles M, González-Torralba F, Represas-Represas C, Pomares X, Márquez-Martín E, González C, Amado C, Forné C, Alonso S, Alcázar B, Barrecheguren M, Jurado Mirete JM, Naval E
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1577-1587
Published Date: 12 July 2022
Lack of COPD-Related Follow-Up Visits and Pharmacological Treatment in Swedish Primary and Secondary Care
Sandelowsky H, Janson C, Wiklund F, Telg G, de Fine Licht S, Ställberg B
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1769-1780
Published Date: 9 August 2022
The Effect of Maintenance Treatment with Erdosteine on Exacerbation Treatment and Health Status in Patients with COPD: A Post-Hoc Analysis of the RESTORE Dataset

Calverley PMA, Papi A, Page C, Rogliani P, Dal Negro RW, Cazzola M, Cicero AF, Wedzicha JA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1909-1920
Published Date: 22 August 2022
Cost-Effectiveness Analysis of Triple Therapy with Budesonide/ Glycopyrronium/ Formoterol Fumarate versus Dual Therapy in Patients with Chronic Obstructive Pulmonary Disease in Spain
Trigueros JA, Garin N, Baloira A, Aceituno S, Calvo A, Prades M, Touron C, Martínez A, Torres C
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2905-2917
Published Date: 15 November 2022