Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
The Association Between Cognitive Functions and Psychological Factors in Patients with Severe COPD
Authors Hansen KK ![]() , Hilberg O
, Hilberg O ![]() , Jensen HI
, Jensen HI ![]() , Løkke A
, Løkke A ![]() , Farver-Vestergaard I
, Farver-Vestergaard I
Received 20 June 2023
Accepted for publication 6 September 2023
Published 19 September 2023 Volume 2023:18 Pages 2065—2078
DOI https://doi.org/10.2147/COPD.S426897
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Kristina Kock Hansen,1,2 Ole Hilberg,1,2 Hanne Irene Jensen,2,3 Anders Løkke,1,2 Ingeborg Farver-Vestergaard2,4
1Department of Respiratory Diseases, Lillebaelt Hospital, Vejle, University Hospital of Southern Denmark, Denmark; 2Department of Regional Health Research, University of Southern Denmark, Odense, Denmark; 3Department of Anaesthesiology and Intensive Care, Lillebaelt Hospital, Vejle, University Hospital of Southern Denmark, Denmark; 4Department of Medicine, Lillebaelt Hospital, Vejle, University Hospital of Southern Denmark, Denmark
Correspondence: Kristina Kock Hansen, Department of Respiratory Diseases, Lillebaelt Hospital, Vejle, University Hospital of Southern Denmark, Beriderbakken 4, Vejle, 7100, Denmark, Tel +45 20189828, Email [email protected]
Purpose: Patients with COPD experience anxiety, depression, and stress more frequently than in the age and gender-matched general population. This cross-sectional study aimed to examine the relationship between cognitive functions and the psychological factors of anxiety, depression and stress among patients with COPD.
Patients and Methods: Between January 2021 and January 2023, patients with severe COPD were recruited, along with age-matched controls. Participants completed the Hospital Anxiety and Depression Scale (HADS) and the Perceived Stress Scale (PSS). The Montreal Cognitive Assessment (MoCA), a continuous reaction time test (CRT), and a driving simulator were used to assess cognitive impairment. Hierarchical multiple linear regression analyses were used to explain the variance of the correlations.
Results: In total, 80 patients (mean age = 64yrs) and 22 controls (mean age = 61yrs) participated in the study. Patients reported significantly higher levels of psychological symptoms compared to the controls (p ≤ 0.001). We found no differences in anxiety (p = 0.31), depression (p = 0.66) and stress (p = 0.37) between patients with and without cognitive impairment. However, stress showed to be a significant predictor of decreased attention (higher stress score resulted in decreasing CRT-index, indication a reduced stability in reaction time) (p = 0.02). Psychological factors did not explain additional variance in cognitive functions beyond sociodemographic factors such as age and sex.
Conclusion: Psychological symptom levels are higher in COPD than controls and perceived stress among patients with COPD appears to be associated with decreased attention. However, psychological factors in general did not appear to contribute to the variance in cognitive functions beyond sociodemographic, physical, and self-perceived symptoms.
Keywords: chronic obstructive pulmonary disease, cognitive impairment, Montreal Cognitive Assessment, anxiety, depression, stress
Corrigendum for this paper has been published.
Introduction
COPD is a complex and multifactorial disease and comorbidities are more common in patients with COPD than in the age and gender-matched general population.1,2 To fully characterize the clinical spectrum of COPD, identification, comprehension, and assessment of all comorbidities in COPD are required.3 Some of the prevalent comorbidities include cardiovascular disease,4 osteoporosis,5 lung cancer,6 type 2 diabetes7 and cognitive impairment (CI)8 as well as obstructive sleep apnea (OSA), which is linked to CI.9
Cognitive functions such as memory and learning, word finding, perception, attention, executive function, and motor function and can all be negatively impacted in people with COPD.1 Neuropsychological tests are used to examine cognitive functions, for example generic tests like Montreal Cognitive Assessment (MoCA) and Mini Mental State Examination (MMSE) as well as more domain-specific tests such as Stroop Color-Word Test or Wechsler Memory Scale.10,11 CI is associated with age and appears in some studies to be more common in male sex.12,13 Some studies11,14 show an association between hypoxemia and cognitive functions. Alcohol consumption and deterioration of vision and hearing also affects the cognitive functions.12,15,16
In patients with COPD, CI reduces the level of function in everyday life and can lead to poor adherence with both medication and oxygen therapy.17,18 Lack of adherence with inhalation therapy in patients with COPD increases the risk of acute exacerbations.19 Studies have looked into the prevalence estimates of CI in COPD, with conflicting results ranging from 10.4% to 77%.20,21 Furthermore, several studies11,22 have examined and found an association between the forced expiratory volume in 1 s (FEV1) and CI, while other studies13,23 show no correlation between FEV1 and CI.
However, a connection between COPD-related symptoms and CI may be explained by FEV1 or FVC, but not exclusively so. A study by von Siemens et al,24 using the screening instrument DemTect for evaluation of CI, demonstrated that it was not solely FVC but instead self-perceived disease-specific quality of life measured by St George’s respiratory questionnaire (SGRQ) that was associated with CI. Patients with a similar degree of FEV1 reduction may experience breathlessness and other COPD-related symptoms differently, and as the Nishimura et al study demonstrated,25 lung function does not accurately predict the perceived severity of dyspnea and other COPD-related symptoms.
The patients’ mental health may have an impact on self-reported COPD-related symptoms or vice versa; COPD-related symptoms may have an impact on the patients’ mental health, which may then have an impact on their cognitive functions. It is known that patients with COPD experience anxiety, depression, and stress more frequently than in the age and gender matched general population,26 as well as more frequently than in patients with conditions such as ischemic heart disease, diabetes, cerebral infarctions, and cancer.27 Smoking, which is the primary risk factor for developing COPD, at least in the Western World, is associated with depression28 and CI.29 Psychological factors can also affect the treatment, compliance and outcome in patients with COPD.2
It is difficult to assess whether sociodemographic factors, physical or self-perceived disease-related symptoms, or a generalized state of poor health are more likely to contribute to CI than COPD itself. Furthermore, CI might primarily be carried forward due to poor mental health. Therefore, we aimed to study the relationship between cognitive functions and the psychological factors of anxiety, depression and stress among patients with COPD.
Materials and Methods
In a cross-sectional study conducted between January 2021 and January 2023, patients with COPD were enrolled from the Outpatient Clinic of Respiratory Diseases at a Danish University Hospital. Age-matched controls were chosen as a reference group.
Study Population
Patients were eligible to participate in the study if they had severe or very severe COPD (forced expiratory volume in one second (FEV1) <50% of predicted) according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2019 classification.30 According to some research,31 CI is associated with disease severity and we were interested in learning more about the factors that contribute to CI in severe COPD. We chose this group to be sure there was some prevalence of CI. Due to the magnitude of the test battery, we could only test a limited number of patients while still trying to test as homogeneous a group as feasible.
Eligible patients had to be within the age span of 40 to 75 years, possess a valid driver’s license, and be without COPD exacerbations in the previous three weeks. Previous studies32–34 using driving simulators have applied the exclusion criteria of not holding a valid driver’s license, due to minimization of training bias in the results. The non-COPD reference group included volunteers from the general public who reacted to adverts on social media as well as family members or friends of the included patients with COPD.
Participants were excluded from the study if they met at least one of the following criteria: 1) were physically unable to operate the driving simulator; 2) needed oxygen therapy; 3) had a history of obstructive sleep apnea; 4) consumed a large amount of alcohol (>21 units per week for men; >14 units per week for women); 5) had uncorrected vision or hearing loss; 6) had serious uncontrolled comorbidities; 7) did not read or understand Danish.
We decided to exclude participants in oxygen therapy, as their oxygen levels were “artificially” (medically) ameliorated. Participants with OSA were excluded because we aimed to explore the treatment effect of undiagnosed OSA on cognitive functions over time. We excluded participants with high alcohol consumption and poor vision/hearing abilities as it may compromise the validity of the cognitive tests.
Prior to data collection, informed consent was obtained from each participant. The Southern Denmark Regional Committee on Health Research Ethics (S-20190082) and the Danish Data Protection Agency both accepted the study. The study was registered with the Open Patient Data Explorative Network (OPEN), Odense University Hospital (OP_1159), and www.clinicaltrials.gov (NCT04458038) in compliance with the Declaration of Helsinki.
Data Collection
KKH, who had received training in using the cognitive assessment battery, collected the data. Patients were examined in a quiet room free from disturbance. It took between two and three hours to complete the examination and involved answering questionnaires, clinical evaluation, and cognitive assessment. To minimize the influence of exhaustion on the performance during cognitive assessment, we performed the cognitive tests first, followed by the clinical evaluation and questionnaires. We finished with a collection of record data.
Questionnaires
Participants completed the COPD Assessment Test (CAT)35 and the modified Medical Research Council (mMRC-scale) dyspnea scale,36 and provided information about their age, sex, cohabitation, education level (International Standard Classification of Education 2011),37 employment status and smoking history. Medical records were used to gather data on the comorbidities including Charlson Comorbidity Index Score and exacerbation history of the patients. Participants completed the Epworth Sleepiness Scale (ESS)38 and their mental health was examined using the Hospital Anxiety and Depression Scale (HADS)39,40 and the Perceived Stress Scale (PSS).41
Clinical Assessment
Data on forced vital capacity (FVC) (L), FVC% predicted, FEV1(L), FEV1% predicted, and FEV1/FVC were collected. A CardioRespiratory Monitor (CRM), NOX T3TM (ResMed, Denmark) is handed out to the participant, along with instructions on how to use it at home the same night and return it the next day. The CRM is used to assess respiratory effort, nasal airflow, pulse, and oxygen saturation during sleep.42
Cognitive Assessment
A battery of neuropsychological tests, including the Montreal Cognitive Assessment test (MoCA),43,44 was used to evaluate cognitive functions. All participants were divided into groups based on their overall MoCA score, with a score of <26 indicating CI and a score of ≥26 indicating no CI. According to Nasreddine et al, the cut-off value of 26 yields the best balance between sensitivity and specificity.43 Visuospatial ability, executive functioning, attention, language, and short-term memory through delayed recall are the five selected MoCA domains that were evaluated.
A 20-minute driving simulator test was also conducted.45 The standard deviation (SD) of the car’s distance from the center of the road and the ability to press a button on the steering wheel when the number “2” appeared on the screen (average response time in seconds) were used to assess participants’ perception and attention.11 Additionally, participants completed the Continuous Reaction Times (CRT) test,46 which is created to assess sustained attention and attention stability, as well as reaction time, in cirrhosis patients. CRT-index >1.9 is considered normal.46
Statistics
Continuous data were checked for normal distribution and descriptive analyses were made. To compare the mean value of the results that were normally distributed between the COPD and control group and the CI group and the group without CI, parametric unpaired t-tests were utilized. Chi2 was used for categorical data and non-parametric Mann Whitney U-tests were used for not normally distributed continuous data.
Whether psychological factors (anxiety, depression and stress) predicted cognitive function better than sociodemographic (age, sex and years of education), and physical factors (FEV1, sleep apnea and smoking), or self-perceived COPD symptom burden (CAT score) were examined using hierarchical multiple linear regression analysis. Independent variables that were not normally distributed were converted into logarithmic before regression analyses were conducted. The hierarchical regression analyses consisted of four steps and in each step, unadjusted and ΔR2 estimates were reported (including Likelihood-ratio test).
A 5% significance level was in all cases used to determine statistical significance. An estimated range with a 95% confidence level was provided. The sample size calculation based on MoCA scores (values from relevant studies),31,47 with a mean of 26, power 0.9, difference 2, SD 2, alpha 0.05 and a patient–control ratio of 5:1, showed a need for a minimum of 65 patients and 13 controls. Data was entered into Research Electronic Data Capture (REDCap), a secure web application that is designed to handle both online and offline data collection for research studies and operations. Statistical analysis was performed using Stata version 17.0.
Results
Out of 177 eligible patients with severe COPD, 80 (53% male) were included in this study. The impact of COPD symptoms on physical functioning, too frequent hospital visits and lack of motivation were most commonly stated as reasons for not participating. Twenty-two age-matched controls (32% male) were also included. The inclusion process is illustrated in the study flowchart (Figure 1). Fifty-eight (73%) and twenty-two (27%) patients were spirometrically categorized as GOLD 3 and GOLD 4, respectively. There were several statistically significant differences in covariates between patients and controls, including sociodemographic, physical and psychological factors (Table 1). We found 56 patients (70%) with undiagnosed OSA and/or ND at the time of recruitment. These patients were not excluded but instead we adjusted for OSA and/or ND in the analysis.
 |
Table 1 Baseline Characteristics of Patients with COPD and Age-Matched Controls |
 |
Figure 1 Study flowchart of the inclusion process. Abbreviations: FEV1, Forced Expiratory Volume in 1 second, % of predicted; OSA, Obstructive Sleep Apnea. |
Characteristics of Patients with and without CI on Psychological Factors
As shown in Table 2, we did not find any statistically significant differences in anxiety, depression and stress between patients with CI and without CI.
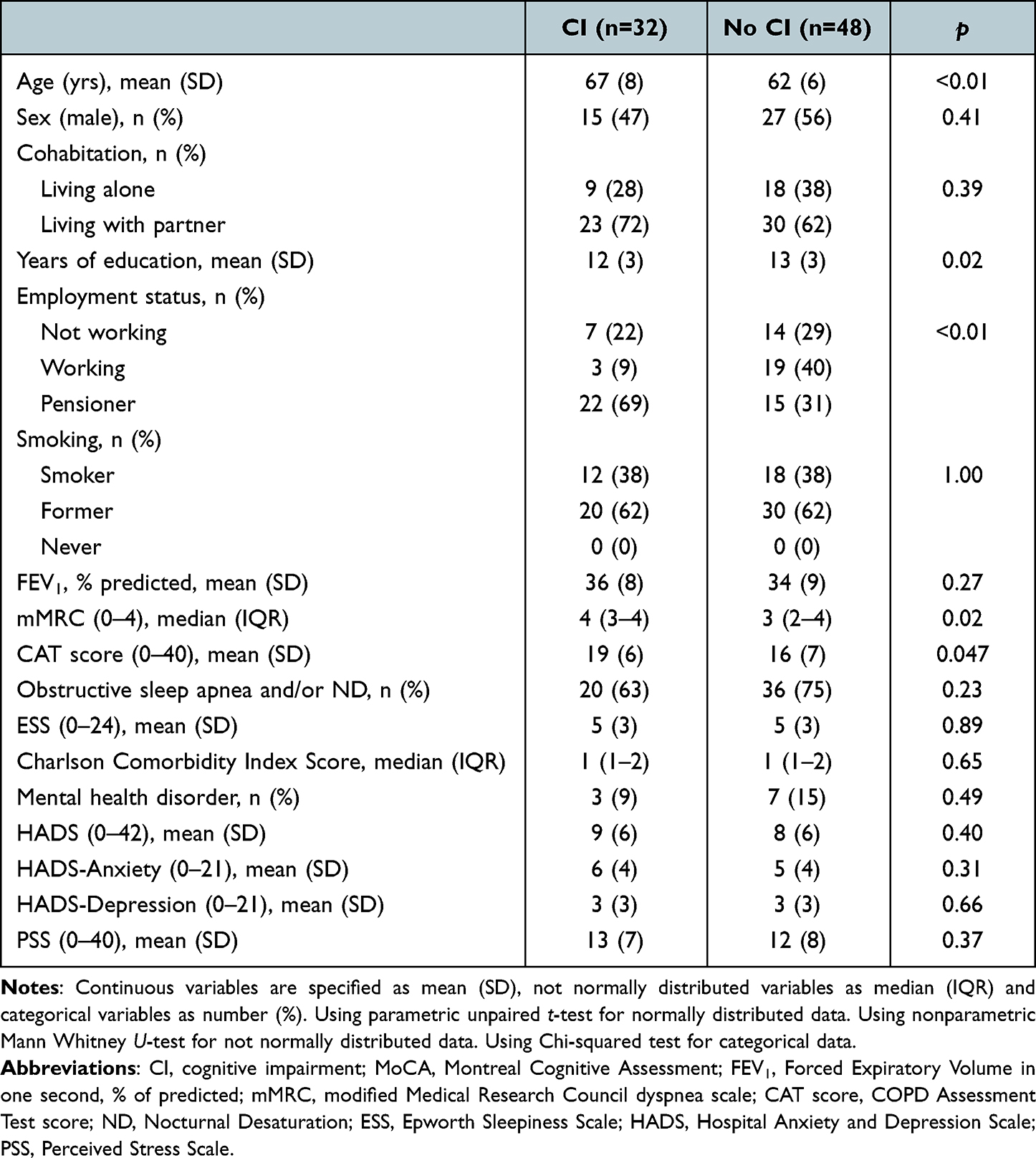 |
Table 2 Characteristics of Patients with COPD with CI (MoCA Score <26) and without CI (MoCA Score 26–30) |
Hierarchical Regression Analyses
The hierarchical multiple-regression analysis is displayed in Table 3.
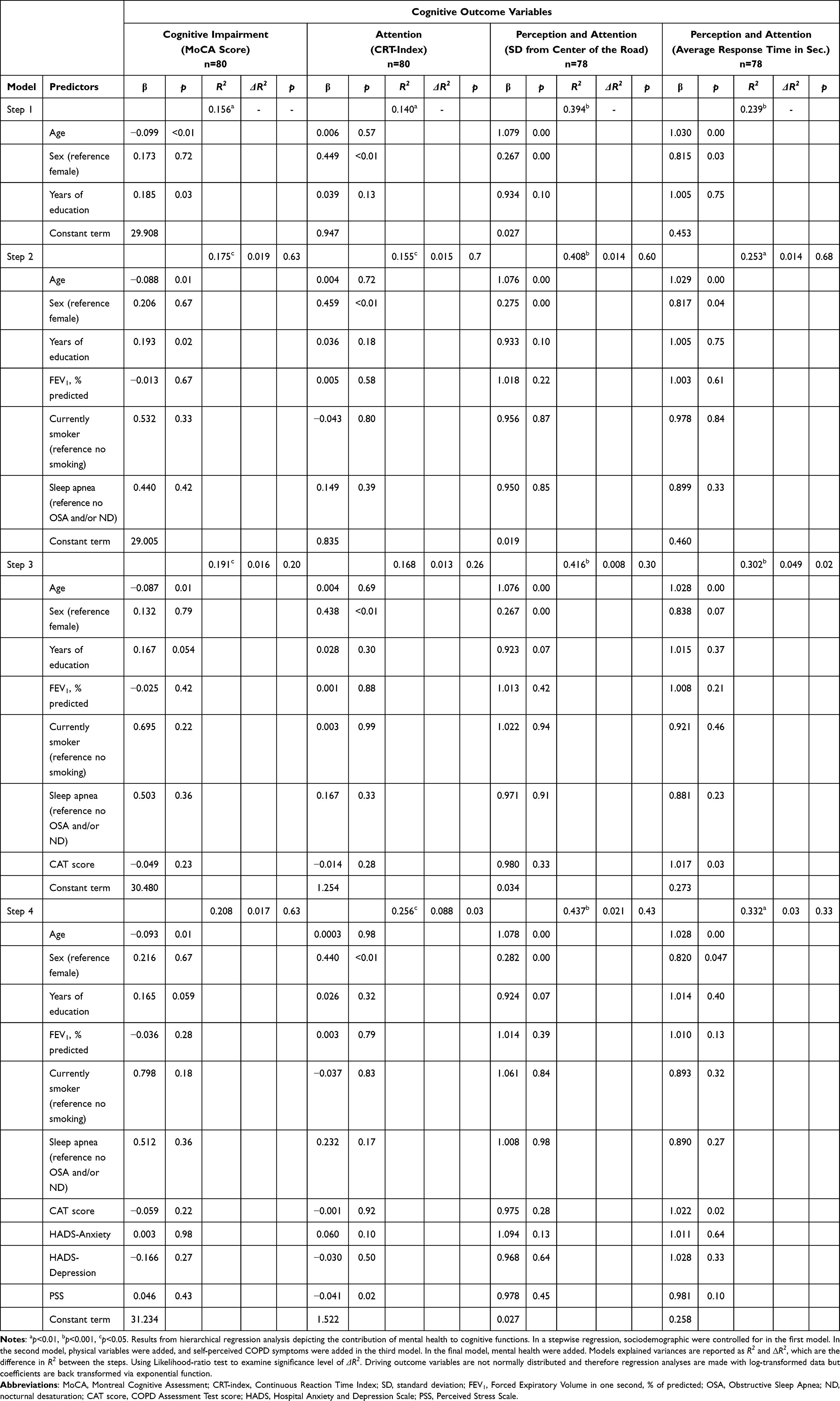 |
Table 3 Hierarchical Multiple Regression Analyses – Associations of Sociodemographic, Physical and Self-Perceived COPD Symptoms as Well as Psychological Factors and Cognitive Functions in Patients with COPD |
Cognitive Impairment Based on MoCA Score
Results from the analyses showed that in the first and second step of the model, the sociodemographic factors, age and years of education, were the only significant predictors of CI, explaining 17.5% of the variance in outcome. Higher age and less years of education were associated with more CI. Only age continued being statistically significant through all four steps, adding another 3.3% to the variance. Neither physical factors, self-perceived COPD-symptom burden nor psychological factors explained any additional variance of CI based on MoCA score.
Sustained Attention and Attention Stability Based on CRT-Index
The first three steps of the model explained 16.8% of the variance in attention and attention stability based on CRT-index, with sex as the only statistically significant predictor. Being a man was associated with better attention (higher CRT-index score indicating higher stability in reaction time) compared to being a woman. Adding psychological factors to the model in step four explained additionally 8.8% (p = 0.03) of the variance in CRT-index score, with stress as the only significant predictor. A one-point increase in PSS score resulted in decreasing CRT-index, indication a reduced stability in reaction time.
Perception and Attention Based on Driving Data
The first step of the model, including sociodemographic information, explained 39.4% of the variance in perception and attention measured by SD from center of the road in the driving test. Age and sex were statistically significant predictors and remained the only significant predictors through all subsequent steps in the model. Higher age and being a woman were associated with higher SD from center of the road and thereby worse perception and attention. No additional variance in SD from center of the road could be explained by physical factors (step 2), self-perceived COPD symptom burden (step 3), or psychological factors (step 4).
Concerning the outcome of average response time, sociodemographic information and physical factors accounted for 25.3% of the variance (steps 1 and 2), with age and sex as statistically significant predictors. Higher age and being a woman were associated with higher average response time indicating longer reaction time. Adding self-perceived COPD symptom burden in step three explained an additional 4.9% of the variance (p = 0.02), with CAT score as a significant predictor. Adding psychological factors to the model in step four did not result in a significant change in the model.
Supplementary Subgroup Analysis
In a subgroup analysis dividing the patients into three groups of driving time (<10, 10–19.99 and 20 minutes), we did not find any statistically significant differences in anxiety, depression and stress between the groups (Table S1).
Discussion
The results of the present study showed that patients with severe COPD reported statistically significantly higher levels of anxiety, depression and stress symptoms compared to their age-matched non-COPD controls, which concurs with findings from multiple other studies.26,48 However, when comparing patients with CI to patients without CI, there were no statistically significant differences in psychological symptoms between groups. Furthermore, measures of psychological factors did not contribute to the variance to a greater extent than sociodemographic and physical factors as well as self-perceived COPD symptom burden. Contrarily, sociodemographic factors like age and sex appeared to be significantly better to explain the variance of cognitive functions compared to psychological factors. However, based on the CRT test, stress showed to be a statistically significant predictor of decreased attention, because a one-point increase in PSS score resulted in decreasing CRT-index, indicating a reduced stability in reaction time.
Anxiety and Depression in Patients with CI
Several studies49–54 examining patients with COPD and cognitive functions based on MoCA have reported results on psychological factors like anxiety and depression. However, some of these studies49,51,54 are using other psychological tests than HADS or use a MoCA cut-off value of 21 to identify CI.52 We found only one study,53 with a HADS mean anxiety (HADS-A) and depression (HADS-D) score and with diagnosed CI (based on a MoCA cut off value of 26), that showed no statistically significant differences in mean anxiety (HADS-A) or depression (HADS-D) score between patients with CI and without CI, similarly to the findings in our study. Compared to our study, the study by Andrianopoulos et al53 had a lower sample size (52 patients vs 80 patients) and a higher average age (68 vs 64 years), but a similar prevalence of CI (40%) and a nearly identical mean MoCA score (25.3 vs 26.0). None of the studies49–54 examined stress.
It is possible that patients with severe COPD may already have such low levels of functioning and are so affected by psychological factors that the cognitive decline is “drowning” because of dire circumstances of living with COPD. This may explain why there was no statistically significant difference in anxiety and depression between those with and without CI. Furthermore, if we had used more COPD-specific measures of anxiety and depression such as The COPD-Anxiety-Questionnaire,55,56 we may have seen a greater association between psychological factors and cognitive function. Additionally, patients with COPD who have the resources to take part in comprehensive studies may receive more support from their partners and/or network or are better to cope with CI and psychological symptoms, which means that they have less of an impact on one another.
The Association Between Stress and Attention Based on CRT
Our hierarchical multiple-regression analyses showed that when we added psychological factors to the model, stress was the strongest and only statistically significant predictor. A study by Phibbs et al57 has examined the influence of perceived stress on response time (inconsistent), and similarly to our study, this study57 also found a positive, statistically significant association between perceived stress and response time. Research suggests that response time potentially serve as an indicator of CI,58 and because stress affects response time, we must include stress when researching cognitive processes. Therefore, it would be preferable to adjust for stress when using neuropsychological testing. Similar to some studies,12,13,59 our results also showed that age and sex are strong predictors of CI, with older age and being a woman linked to a decline in cognitive functions.
Clinical Implications
In our present study, we did not find that patients with CI were at risk of psychological problems compared to patients without CI. Therefore, CI may not necessarily indicate the need for psychological testing. On the other hand, psychological symptoms do not automatically warrant a neuropsychological test. However, because both psychological and cognitive symptoms are often highly prevalent in patients with severe COPD,26,49 screening for both should be included in routine standard care. If using CRT as a neuropsychological test, the individual level of stress should be addressed when interpreting test results.
As no consensus exists regarding which neuropsychological tests are most clinically relevant, reliable and feasible to use, future studies of cognitive functions in patients with COPD should focus on examining these aspects.
Strength and Limitations
The relatively low rate of missing data across a broad test battery, which included data on cognitive assessment, physical and mental health in our study is a strength. The internal validity was increased by the first author (KKH), carrying out all examinations and maintaining and evaluating the data.
The patient inclusion rate of 45% is a limitation of the study. Although the cognitive functions of those who declined to participate in the study are unknown, their age and FEV1 were similar to those of the patients who were included (Table S2). Dyspnea, lack of physical strength, lack of motivation, and too frequent hospital visits were given as reasons for declining participation. Patients with mental excess may be more likely to take part in a two- to three-hour examination. Therefore, we cannot rule out the risk that our study contained selection bias. Furthermore, we are aware of the risk that the exclusion of individuals without a driver’s license might have resulted in biased selection of patients with better cognitive function.
Conclusions
In our study, patients with severe COPD reported statistically significantly higher levels of anxiety, depression, and perceived stress symptoms compared to non-COPD controls of comparable age. However, when looking only at patients with COPD, there were no statistically significant differences in psychological symptoms between individuals with and without CI. While stress appeared to be a statistically significant predictor of diminished attention measured by CRT, psychological factors in general did not contribute to the variance in cognitive functions beyond sociodemographic, physical, and self-perceived symptoms in COPD.
Abbreviations
CAT, COPD Assessment Test; CI, Cognitive Impairment; COPD, Chronic Obstructive Pulmonary Disease; CRM, CardioRespiratory Monitor; CRT, Continuous Reaction Time test; ESS, Epworth Sleepiness Scale; FEV1, Forced expiratory volume in 1 second; FVC, Forced vital capacity; GOLD, Global initiative for chronic Obstructive Lung Disease; HADS, Hospital Anxiety and Depression Scale; IQR, Interquartile Range; mMRC, Modified Medical Research Council dyspnea scale; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; OPEN, Open Patient data Explorative Network; OSA, Obstructive Sleep Apnea; PSS, Perceived Stress Scale; SD, Standard deviation.
Data Sharing Statement
If interested, data can be shared upon request with the corresponding author.
Acknowledgments
KKH thanks all the participants in the study. KKH thanks colleagues in the Outpatient Clinic and Research Unit for helping with practical assignments and patient recruitment. Also acknowledged are statistician Sören Möller from Open Patient data Explorative Network (OPEN), Odense University Hospital, for providing statistical support, and ResMed Denmark A/S for lending CardioRespiratory Monitors.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agreed to be accountable for all aspects of the work.
Funding
This research was funded by the Research Council Lillebaelt Hospital, The Danish Lung Association, Eva Merete Falck Crone´s Foundation, Wonge´s Foundation and supported by a Chiesi Foundation research grant. The sponsors had no role in any of the stages from study design to submission.
Disclosure
The authors report no conflicts of interest in the present work.
References
1. Dodd JW, Getov SV, Jones PW. Cognitive function in COPD. Eur Respir J. 2010;35(4):913–922. doi:10.1183/09031936.00125109
2. Smith MC, Wrobel JP. Epidemiology and clinical impact of major comorbidities in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2014;9:871–888. doi:10.2147/COPD.S49621
3. Jones PW, Agusti AG. Outcomes and markers in the assessment of chronic obstructive pulmonary disease. Eur Respir J. 2006;27(4):822–832. doi:10.1183/09031936.06.00145104
4. Sin DD, Man SF. Why are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? The potential role of systemic inflammation in chronic obstructive pulmonary disease. Circulation. 2003;107(11):1514–1519. doi:10.1161/01.CIR.0000056767.69054.B3
5. Bolton CE, Ionescu AA, Shiels KM, et al. Associated loss of fat-free mass and bone mineral density in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;170(12):1286–1293. doi:10.1164/rccm.200406-754OC
6. Wasswa-Kintu S, Gan WQ, Man SF, Pare PD, Sin DD. Relationship between reduced forced expiratory volume in one second and the risk of lung cancer: a systematic review and meta-analysis. Thorax. 2005;60(7):570–575. doi:10.1136/thx.2004.037135
7. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32(4):962–969. doi:10.1183/09031936.00012408
8. Villeneuve S, Pepin V, Rahayel S, et al. Mild cognitive impairment in moderate to severe COPD: a preliminary study. Chest. 2012;142(6):1516–1523. doi:10.1378/chest.11-3035
9. Wang Y, Li B, Li P, et al. Severe obstructive sleep apnea in patients with chronic obstructive pulmonary disease is associated with an increased prevalence of mild cognitive impairment. Sleep Med. 2020;75:522–530. doi:10.1016/j.sleep.2020.05.002
10. Schou L, Østergaard B, Rasmussen LS, Rydahl-Hansen S, Phanareth K. Cognitive dysfunction in patients with chronic obstructive pulmonary disease--a systematic review. Respir Med. 2012;106(8):1071–1081. doi:10.1016/j.rmed.2012.03.013
11. Torres-Sánchez I, Rodríguez-Alzueta E, Cabrera-Martos I, López-Torres I, Moreno-Ramírez MP, Valenza MC. Cognitive impairment in COPD: a systematic review. J Bras Pneumol. 2015;41(2):182–190. doi:10.1590/S1806-37132015000004424
12. Lal C, Strange C, Bachman D. Neurocognitive impairment in obstructive sleep apnea. Chest. 2012;141(6):1601–1610. doi:10.1378/chest.11-2214
13. Tudorache E, Fildan AP, Frandes M, Dantes E, Tofolean DE. Aging and extrapulmonary effects of chronic obstructive pulmonary disease. Clin Interv Aging. 2017;12:1281–1287. doi:10.2147/CIA.S145002
14. Thakur N, Blanc PD, Julian L, et al. COPD and cognitive impairment: the role of hypoxemia and oxygen therapy. Am J Respir Critical Care Med Conference. 2010;181(1):263.
15. Martini A, Castiglione A, Bovo R, Vallesi A, Gabelli C. Aging, cognitive load, dementia and hearing loss. Audiol Neurootol. 2014;19 Suppl 1:2–5. doi:10.1159/000371593
16. Humes LE, Young LA. Sensory-Cognitive Interactions in Older Adults. Ear Hear. 2016;37 Suppl 1(Suppl 1):52s–61s. doi:10.1097/AUD.0000000000000303
17. Antonelli-Incalzi R, Corsonello A, Trojano L, et al. Correlation between cognitive impairment and dependence in hypoxemic COPD. J Clin Exp Neuropsychol. 2008;30(2):141–150. doi:10.1080/13803390701287390
18. Incalzi RA, Gemma A, Marra C, Capparella O, Fuso L, Carbonin P. Verbal memory impairment in COPD: its mechanisms and clinical relevance. Chest. 1997;112(6):1506–1513. doi:10.1378/chest.112.6.1506
19. Suh HS, Chang MS, Yu I, et al. Adherence to Long-Acting Inhaler Use for Initial Treatment and Acute Exacerbation of Chronic Obstructive Pulmonary Disease: a Retrospective Cohort Study. J Pers Med. 2022;12(12):2073. doi:10.3390/jpm12122073
20. Grant I, Heaton RK, McSweeny AJ, Adams KM, Timms RM. Neuropsychologic findings in hypoxemic chronic obstructive pulmonary disease. Arch Intern Med. 1982;142(8):1470–1476. doi:10.1001/archinte.1982.00340210062015
21. Antonelli-Incalzi R, Corsonello A, Pedone C, et al. Drawing impairment predicts mortality in severe COPD. Chest. 2006;130(6):1687–1694. doi:10.1378/chest.130.6.1687
22. Crişan AF, Oancea C, Timar B, Fira-Mladinescu O, Crişan A, Tudorache V. Cognitive impairment in chronic obstructive pulmonary disease. PLoS One. 2014;9(7):e102468. doi:10.1371/journal.pone.0102468
23. Liesker JJ, Postma DS, Beukema RJ, et al. Cognitive performance in patients with COPD. Respir Med. 2004;98(4):351–356. doi:10.1016/j.rmed.2003.11.004
24. von Siemens SM, Perneczky R, Vogelmeier CF, et al. The association of cognitive functioning as measured by the DemTect with functional and clinical characteristics of COPD: results from the COSYCONET cohort. Respir Res. 2019;20(1):257. doi:10.1186/s12931-019-1217-5
25. Nishimura K, Izumi T, Tsukino M, Oga T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest. 2002;121(5):1434–1440. doi:10.1378/chest.121.5.1434
26. Di Marco F, Verga M, Reggente M, et al. Anxiety and depression in COPD patients: the roles of gender and disease severity. Respir Med. 2006;100(10):1767–1774. doi:10.1016/j.rmed.2006.01.026
27. Schane RE, Walter LC, Dinno A, Covinsky KE, Woodruff PG. Prevalence and risk factors for depressive symptoms in persons with chronic obstructive pulmonary disease. J Gen Intern Med. 2008;23(11):1757–1762. doi:10.1007/s11606-008-0749-z
28. Mendelsohn C. Smoking and depression--a review. Aust Fam Physician. 2012;41(5):304–307.
29. Jia L, Du Y, Chu L, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. 2020;5(12):e661–e671. doi:10.1016/S2468-2667(20)30185-7
30. Singh D, Agusti A, Anzueto A, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
31. Yin M, Wang H, Hu X, Li X, Fei G, Yu Y. Patterns of brain structural alteration in COPD with different levels of pulmonary function impairment and its association with cognitive deficits. BMC Pulm Med. 2019;19(1):203. doi:10.1186/s12890-019-0955-y
32. Beratis IN, Andronas N, Kontaxopoulou D, et al. Driving in mild cognitive impairment: the role of depressive symptoms. Traffic Inj Prev. 2017;18(5):470–476. doi:10.1080/15389588.2016.1265648
33. George CF, Boudreau AC, Smiley A. Effects of nasal CPAP on simulated driving performance in patients with obstructive sleep apnoea. Thorax. 1997;52(7):648–653. doi:10.1136/thx.52.7.648
34. Prior TS, Troelsen T, Hilberg O. Driving performance in patients with chronic obstructive lung disease, interstitial lung disease and healthy controls: a crossover intervention study. BMJ Open Respiratory Research. 2015;2(1):1–6.
35. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
36. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
37. United Nations Educational, Scientific and Cultural Organization. International Standard Classification of Education ISCED 2011. United Nations Educational, Scientific and Cultural Organization (UNESCO); 2011.
38. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
39. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
40. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002;52(2):69–77. doi:10.1016/S0022-3999(01)00296-3
41. Eskildsen A, Dalgaard VL, Nielsen KJ, et al. Cross-cultural adaptation and validation of the Danish consensus version of the 10-item Perceived Stress Scale. Scand J Work Environ Health. 2015;41(5):486–490. doi:10.5271/sjweh.3510
42. Cairns A, Wickwire E, Schaefer E, Nyanjom D. A pilot validation study for the NOX T3(TM) portable monitor for the detection of OSA. Sleep Breath. 2014;18(3):609–614. doi:10.1007/s11325-013-0924-2
43. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
44. Ciesielska N, Sokołowski R, Mazur E, Podhorecka M, Polak-Szabela A, Kędziora-Kornatowska K. Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatr Pol. 2016;50(5):1039–1052. doi:10.12740/PP/45368
45. Land M, Horwood J. Which parts of the road guide steering? Nature. 1995;377(6547):339–340. doi:10.1038/377339a0
46. Lauridsen MM, Thiele M, Kimer N, Vilstrup H. The continuous reaction times method for diagnosing, grading, and monitoring minimal/covert hepatic encephalopathy. Metab Brain Dis. 2013;28(2):231–234. doi:10.1007/s11011-012-9373-z
47. Wong GKC, Mak JSY, Wong A, et al. Minimum Clinically Important Difference of Montreal Cognitive Assessment in aneurysmal subarachnoid hemorrhage patients. J Clin Neurosci. 2017;46:41–44. doi:10.1016/j.jocn.2017.08.039
48. Willgoss TG, Yohannes AM. Anxiety disorders in patients with COPD: a systematic review. Respir Care. 2013;58(5):858–866. doi:10.4187/respcare.01862
49. Dulohery MM, Schroeder DR, Benzo RP. Cognitive function and living situation in COPD: is there a relationship with self-management and quality of life? Int J Chron Obstruct Pulmon Dis. 2015;10:1883–1889. doi:10.2147/COPD.S88035
50. Yohannes AM, Eakin M, Holbrook JT, et al. Association of mild cognitive impairment and characteristic of COPD and overall health status in a cohort study. Expert Rev Respir Med. 2021;15(1):153–159. doi:10.1080/17476348.2021.1838278
51. Pierobon A, Bottelli ES, Ranzini L, et al. COPD patients’ self-reported adherence, psychosocial factors and mild cognitive impairment in pulmonary rehabilitation. International Journal of COPD. 2017;12:2059–2067. doi:10.2147/COPD.S133586
52. Ozturk HM, Ogan N, Erdogan M, Akpinar EE, Ilgar C, Ozturk S. The association between total cholesterol and cognitive impairment in chronic obstructive pulmonary disease patients. Prostaglandins Other Lipid Mediat. 2023;164:106697. doi:10.1016/j.prostaglandins.2022.106697
53. Andrianopoulos V, Gloeckl R, Scheeberger T, et al. Changes in cognitive function of cognitively impaired patients with COPD after pulmonary rehabilitation and 1-year follow-up. Eur Respir J Conference. 2018;52(62):PA3649.
54. Lv Z, Hu P, Jiang Y, et al. Changes in Spatial Working Memory in Stable Chronic Obstructive Pulmonary Disease: a Retrospective Study. Biomed Res Int. 2020;2020:7363712. doi:10.1155/2020/7363712
55. Farver-Vestergaard I, Rubio-Rask S, Timm S, Christiansen CF, Hilberg O, Løkke A. Disease-Specific Anxiety in Chronic Obstructive Pulmonary Disease: translation and Initial Validation of a Questionnaire. Front Psychol. 2022;13:907939. doi:10.3389/fpsyg.2022.907939
56. Kühl K, Kuhn C, Kenn K, Rief W. The COPD-Anxiety-Questionnaire (CAF): a new instrument to assess illness specific anxiety in COPD patients. Psychother Psychosom Med Psychol. 2011;61(1):e1–9. doi:10.1055/s-0030-1248281
57. Phibbs S, Stawski RS, MacDonald SWS, Munoz E, Smyth JM, Sliwinski MJ. The influence of social support and perceived stress on response time inconsistency. Aging Ment Health. 2019;23(2):214–221. doi:10.1080/13607863.2017.1399339
58. MacDonald SW, Nyberg L, Bäckman L. Intra-individual variability in behavior: links to brain structure, neurotransmission and neuronal activity. Trends Neurosci. 2006;29(8):474–480. doi:10.1016/j.tins.2006.06.011
59. Au B, Dale-McGrath S, Tierney MC. Sex differences in the prevalence and incidence of mild cognitive impairment: a meta-analysis. Ageing Res Rev. 2017;35:176–199. doi:10.1016/j.arr.2016.09.005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
A Narrative Review of Research on Adjustment to Spinal Cord Injury and Mental Health: Gaps, Future Directions, and Practice Recommendations
Sandalic D, Arora M, Pozzato I, Simpson G, Middleton J, Craig A
Psychology Research and Behavior Management 2022, 15:1997-2010
Published Date: 5 August 2022
Spiritual Well-Being, Depression, Anxiety, and Stress in Indonesian Muslim Communities During COVID-19
Hamka, Suen MW, Ramadhan YA, Yusuf M, Wang JH
Psychology Research and Behavior Management 2022, 15:3013-3025
Published Date: 17 October 2022
Dietary Supplement Consumption and Mental Health in Indonesian Adults During Second Wave of COVID-19 Pandemic
Yusof J, d'Arqom A, Andriani AP, Nasution MZ, Fatimah N, Mustika A, Handayani S, Syed Abdul Kadir SZ
Patient Preference and Adherence 2023, 17:1799-1811
Published Date: 24 July 2023
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024