Back to Journals » Clinical Ophthalmology » Volume 20
The Acute Effects of Caffeine on OCT and OCTA Parameters: A Systematic Review and Meta-Analysis
Authors Veiga DM ![]() , Ivanov YA
, Ivanov YA ![]() , Júnior AYF, Rebolho MEF
, Júnior AYF, Rebolho MEF ![]() , Gerente BGDSM, Amaral DC
, Gerente BGDSM, Amaral DC ![]() , Jacometti R, Guedes J
, Jacometti R, Guedes J ![]() , Monteiro ML, Louzada RN
, Monteiro ML, Louzada RN ![]()
Received 20 October 2025
Accepted for publication 12 March 2026
Published 11 April 2026 Volume 2026:20 568498
DOI https://doi.org/10.2147/OPTH.S568498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Davi Marçola Veiga,1 Yuri Aleksander Ivanov,2 Alexandre Yamada Fujimura Júnior,1 Maria Eduarda Figueiredo Rebolho,1 Beatriz Gonçalves da Silva Miroski Gerente,3 Dillan Cunha Amaral,4 Raíza Jacometti,5 Jaime Guedes,6 Mário Luiz Ribeiro Monteiro,5 Ricardo Noguera Louzada4,5
1Faculty of Medicine, Marilia Medical School, Marília, SP, Brazil; 2Faculty of Medicine, University of the Extreme South of Santa Catarina, Criciúma, SC, Brazil; 3Faculty of Medicine, University of Southern Santa Catarina, Florianópolis, SC, Brazil; 4Department of Ophthalmology and Otorhinolaryngology, Faculty of Medicine, Federal University of Rio de Janeiro, Rio de Janeiro, RJ, Brazil; 5Division of Ophthalmology and the Laboratory for Investigation in Ophthalmology (LIM-33), Faculty of Medicine, Universidade de São Paulo, São Paulo, SP, Brazil; 6Aran Eye Associates, Coral Gables, FL, USA
Correspondence: Jaime Guedes, Aran Eye Associates, 1097 S Lejeune Road, Coral Gables, FL, 33134, USA, Email [email protected]
Purpose: This systematic review and meta-analysis aimed to comprehensively assess the acute effects of caffeine and caffeinated beverages on ocular microvasculature measured by optical coherence tomography (OCT) and optical coherence tomography angiography (OCTA) parameters, explicitly focusing on subfoveal choroidal thickness (SFCT) and superficial capillary vessel density (SVD), and deep capillary vessel density (DVD).
Methods: A systematic search was conducted across PubMed, the Cochrane Database, and Embase for trials evaluating the acute effects of caffeine or caffeinated beverages on SFCT, SVD, and DVD, as measured by OCTA. Pooled mean differences (MD) were calculated using random-effects models, with heterogeneity assessed by I2 statistics. Subgroup analyses were performed by study design, intervention type, and refractive status. The protocol was prospectively registered in PROSPERO (CRD420251091123). Statistical analyses were performed using RStudio 2025.05.1+513.
Results: 18 studies comprising 630 patients were included. Pooled analysis demonstrated a significant reduction in SFCT after caffeine intake (– 23.79 μm; 95% CI: – 31.43 to – 16.15; p < 0.001), particularly with coffee and caffeine capsules, whereas no effect was observed with energy drinks or in highly myopic eyes. Regarding SVD, caffeine was associated with significant reductions across foveal, parafoveal, and perifoveal regions, mainly driven by coffee and capsule interventions. In DVD analyses, no overall significant effect was found; however, subgroup analyses indicated significant reductions with caffeine capsules and coffee, while energy drinks showed opposite trends.
Conclusion: Acute caffeine intake, primarily from capsules or coffee, induces significant SFCT reduction and modest reductions in SVD, while changes in DVD were confined mainly to the caffeine-capsule subgroup, suggesting that energy drink ingredients may counteract caffeine-induced vasoconstriction. These findings offer valuable insights into the acute effects of caffeine on ocular microvasculature; however, the modest effect sizes necessitate caution regarding inherent physiological, measurement, and bioactive components variability. This study establishes a foundation for future investigations into the clinical significance of acute ocular microvascular fluctuations following caffeine intake.
Keywords: caffeine, coffee, subfoveal choroidal thickness, optical coherence tomography, optical coherence tomography angiography, systematic review
Introduction
Caffeine is the most widely consumed psychoactive substance worldwide, with approximately 80% of the Western population consuming it regularly.1 Its popularity is due to its wide availability, legal status, and rapid absorption in the gastrointestinal tract, reaching peak plasma levels in approximately 30 minutes.2,3 The primary dietary sources of caffeine include coffee, tea, energy drinks, and cola-based soft drinks.1,4 Once ingested, caffeine stimulates the central nervous system, increasing blood pressure and heart rate through antagonism of adenosine receptors, particularly A1 and A2A.5–7
Caffeine’s vasoconstrictive effects are well documented. However, its impact on ocular blood flow has been less extensively investigated and has been associated with transient choroidal vasoconstriction and reduction in subfoveal choroidal thickness (SFCT).8 Studies assessing retinal vessel caliber have reported decreases in both arteriolar and venular diameters following caffeine intake, with corresponding changes in ocular hemodynamic parameters.9,10
These findings support the hemodynamic influence of caffeine on ocular circulation and provide a physiological framework for interpreting structural and vascular changes detected by Optical Coherence Tomography (OCT) and optical coherence tomography angiography (OCTA).11
More recently, OCT and OCTA have been employed to further evaluate these vascular effects, reporting reductions in SFCT following caffeine consumption.12 SFCT is defined as the vertical distance between Bruch’s membrane and the inner scleral boundary beneath the fovea.13 These noninvasive imaging modalities allow detailed structural and microvascular assessment of the retina and choroid and have facilitated investigation of the relationship between caffeine intake and SFCT.14
These changes typically begin between 5 and 30 minutes after the intake of approximately 200 mg of caffeine and may persist for up to 4 hours, peaking around 1 hour post-ingestion.15 Choroidal thinning has been attributed to reduced ocular blood flow associated with the vasoconstrictive effect of caffeine.8,12,16 However, ocular autoregulatory mechanisms are thought to maintain overall perfusion within physiological limits.15
The choroid is one of the most highly vascularized tissues in the human body and plays a fundamental role in supplying oxygen and nutrients to the outer retina, particularly the photoreceptors and the retinal pigment epithelium (RPE).17,18 Owing to its rich vascular supply, the choroid is sensitive to hemodynamic changes induced by vasoactive substances.17,19 OCT and OCTA imaging have also been used to evaluate the vascular and structural effects of other substances on the retina and choroid. For instance, nicotine has been reported to exert ischemic effects on retinochoroidal and vascular structures.20 Conversely, specific agents have been associated with increased choroidal thickness, including intraocular pressure–lowering medications, topical atropine, and the systemic administration of β-blockers and ethanol.21
Accordingly, several studies have investigated the effects of caffeine on choroidal circulation, reporting reductions in ocular blood flow and choroidal thickness. Changes in SFCT, macular flow area, and macular vessel density have also been described following caffeine intake, and investigations assessing superficial, deep, and choriocapillaris vessel density using OCTA have yielded variable findings.16
Given these observations, variations in choroidal thickness should be interpreted within the context of physiological and methodological variability.16,22,23 Epidemiological investigations have also explored associations between caffeine intake and ocular conditions, although findings remain heterogeneous.24
Therefore, a systematic evaluation of the available evidence is warranted to quantify the acute effects of caffeine and caffeinated beverages on structural and microvascular parameters assessed by OCT and OCTA.
Methods
Protocol and Registration
This study was conducted and reported according to the guidelines of the Cochrane Collaboration Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement.25 The protocol was prospectively registered in the International Prospective of Systematic Reviews (PROSPERO) under protocol number CRD420251091123.
Data Source and Search Strategy
We systematically searched PubMed, Embase, and Cochrane databases. References of eligible papers and systematic reviews were also searched for additional studies of interest. Our search was last updated in June 2025. Two authors independently assessed all records, and decisions on full-text retrieval were reached by consensus. Full texts were retrieved from all databases, and inclusion and exclusion criteria were discussed. The full search strategy for all databases was (caffeine OR energy drink OR coffee OR tea OR cola) AND (“Optical Coherence Tomography” OR OCT[Title/Abstract] OR “Optical Coherence Tomography Angiography” OR “OCTA” OR “vessel density” OR “foveal avascular zone” OR “FD-300” OR “optic nerve head” OR “retinal nerve fiber layer thickness” OR “retinal vessel” OR “choroidal thickness”). Conference abstracts and prospective trials were also searched. Data were collected independently by two authors. Following data collection, the extracted information was cross-checked, and any discrepancies were discussed until consensus was reached. No automation tools were used at any stage of the data extraction process.
Eligibility Criteria
There were no restrictions on the publication date or language. We considered studies eligible for inclusion if they (1) assessed OCT or OCTA at baseline and after caffeine or caffeinated beverages ingestion (2) reported on outcomes of interest. The exclusion criteria were as follows: (1) in vitro studies; (2) case reports, abstracts, editorials, letters, and conference proceedings without sufficient data.
Endpoints and Subanalyses
The clinical outcomes of interest in our study were: (1) SFCT; (2) Foveal DVD;
(3) Parafoveal DVD; (4) Perifoveal DVD; (5) Foveal SVD; (6) Parafoveal SVD; (7) Perifoveal SVD. Additionally, baseline characteristics of included studies and participants were also collected and summarized in Table 1. The variables collected included reported outcomes, intervention type, number of participants, and number of eyes analyzed. Participant-level characteristics included age, sex, refractive error, spherical equivalent, eye axial length, body mass index, and systolic and diastolic blood pressure.
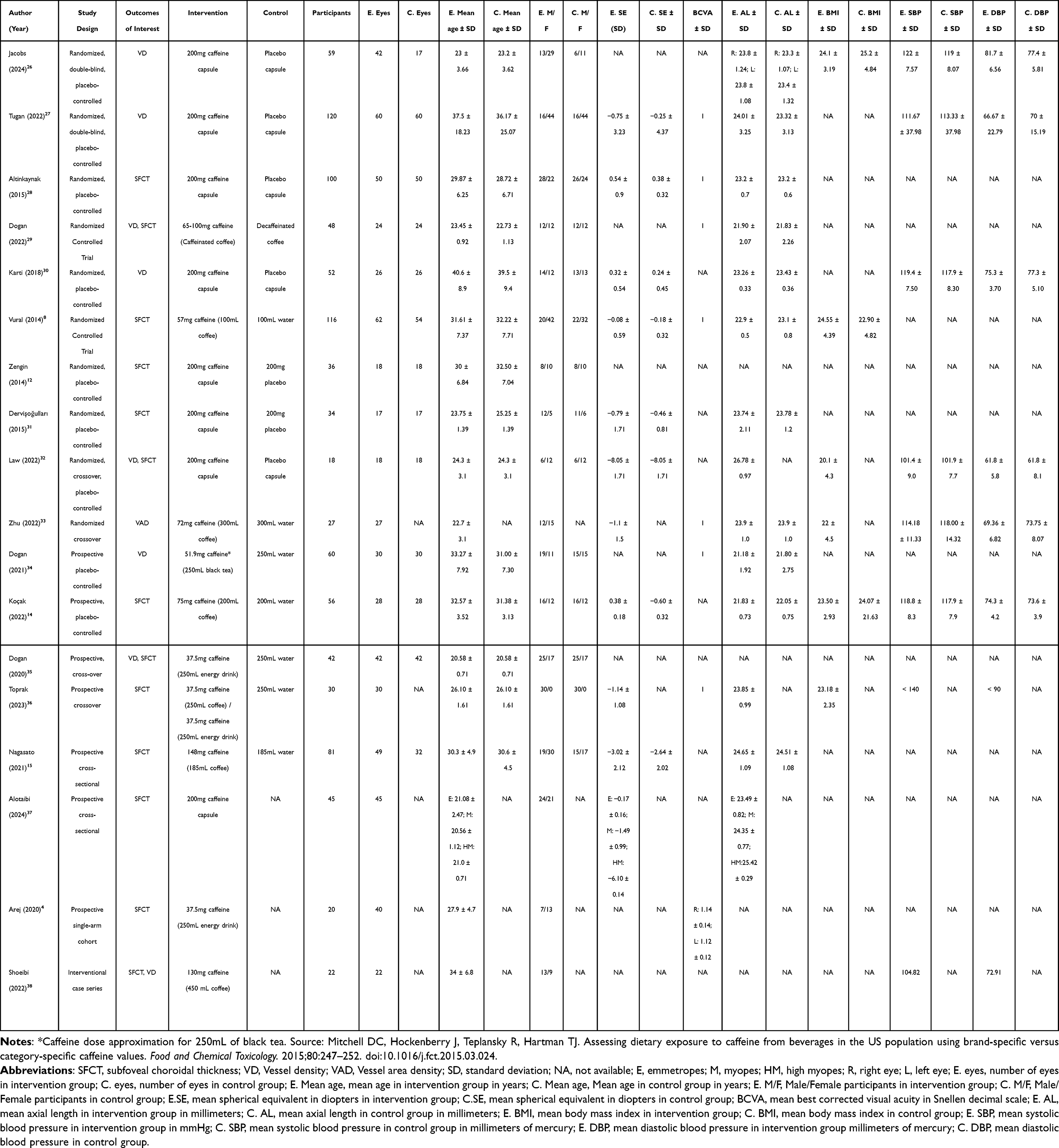 |
Table 1 Baseline Characteristics of the Studies Included |
Quality Assessment
Risk of bias was assessed independently by two authors using the Cochrane Risk of Bias tool for randomized controlled trials (RoB 2),39 and the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool.40 Any discrepancies were resolved through discussion until consensus was reached. Visual representations of the assessments were generated using the RobVis tool.
Statistical Analysis
All statistical analyses were performed using R (RStudio version 2025.05.1+513) with the meta package. Study characteristics were tabulated to decide which studies were eligible for each synthesis. For continuous outcomes, mean and standard deviation (SD) values were extracted from the intervention groups’ baseline and post-intervention data. When studies reported medians and interquartile ranges (IQR), these values were converted to means and SDs using the method proposed by Wan et al (2014) via the Meta-Analysis Accelerator tool.41,42 When standard deviations (SDs) were not reported, they were imputed using the P-value to SD in 2 Groups conversion method. When no conversion was feasible, SDs were assumed from studies with similar methodology and comparable populations, in accordance with recommendations from the Cochrane Handbook for Systematic Reviews of Intervention.43
All meta-analyses were conducted under a random-effects model, using the inverse-variance method with the restricted maximum likelihood (REML) estimator for the between-study variance (τ2). Pooled MD and their corresponding 95% confidence intervals (CI) were calculated for each continuous outcome. A two-sided p-value of < 0.05 was considered statistically significant. Between-study heterogeneity was assessed using Cochrane’s Q test (Chi2) and quantified with the I2 statistic; p ≤ 0.10 indicated significant heterogeneity. To explore possible causes of heterogeneity among study results, subgroup meta-analyses according to intervention type, refractive status, and study design were conducted when sufficient data were available.
Results
Study Selection
As shown in Figure 1, the search strategy initially identified 770 studies. After removing 155 duplicates, 615 records remained for title and abstract screening. Of these, 39 were selected for full text, resulting in 18 studies being included.4,8,12,14,15,26–38 Altogether, these studies involved 630 participants with a mean age of 28.8 years. Among them, 276 received caffeine in capsule form, 212 consumed coffee, 30 consumed black tea, and 82 consumed an energy drink. One study with 30 participants used a mixed intervention, in which the same individuals ingested coffee, followed by an energy drink.36 Regarding refractive status, 76 patients were classified as myopes, 23 as high myopes, and the remainder as emmetropes. The detailed baseline characteristics of the included studies are presented in Table 1.
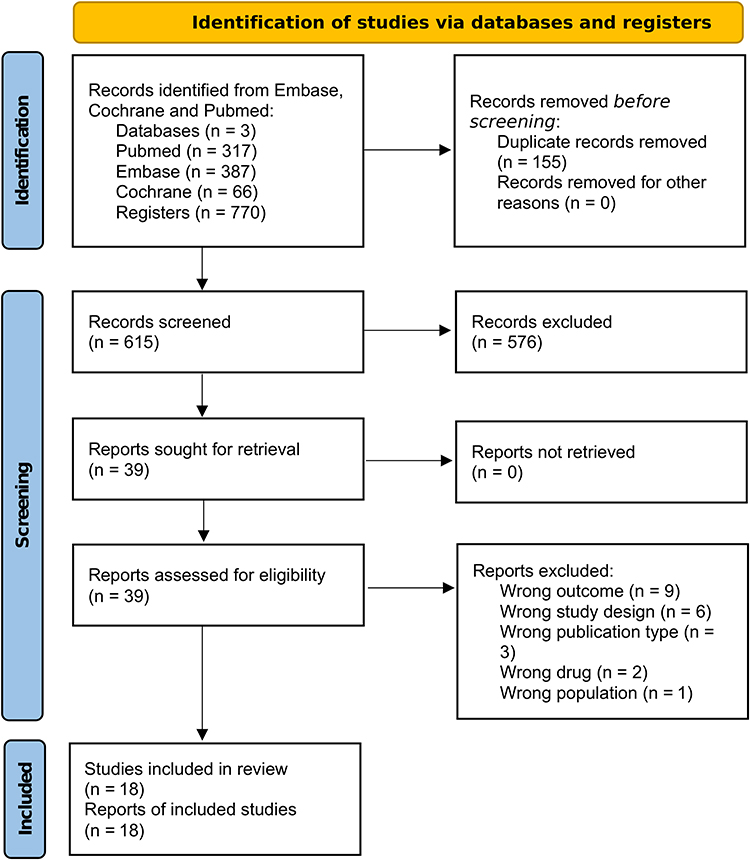 |
Figure 1 PRISMA flow diagram. |
Subfoveal Choroidal Thickness
Regarding the SFCT outcome, a pooled analysis of 13 studies demonstrated a significant reduction in SFCT following caffeine intake compared with baseline. The overall MD was –23.79 micrometers (95% confidence interval [CI]: –31.43 to –16.15; p < 0.001), indicating a consistent thinning of the subfoveal choroid after caffeine administration.
In the subgroup analysis by type of intervention, distinct effects were identified (Figure 2). Among the 238 participants who ingested coffee, a marked and significant reduction in SFCT was observed one hour after intake, with a MD of –29.48 micrometers (95% CI: –40.11 to –18.86; p < 0.001). In the subgroup of 103 participants who received caffeine capsules, a significant reduction was also demonstrated, with a MD of –20.24 micrometers (95% CI: –39.92 to –3.56; p = 0.018). Conversely, in the subgroup of participants who consumed energy drinks, no significant effect was observed, with an MD of –9.49 micrometers (95% CI: –28.64 to 9.72; p = 0.33).
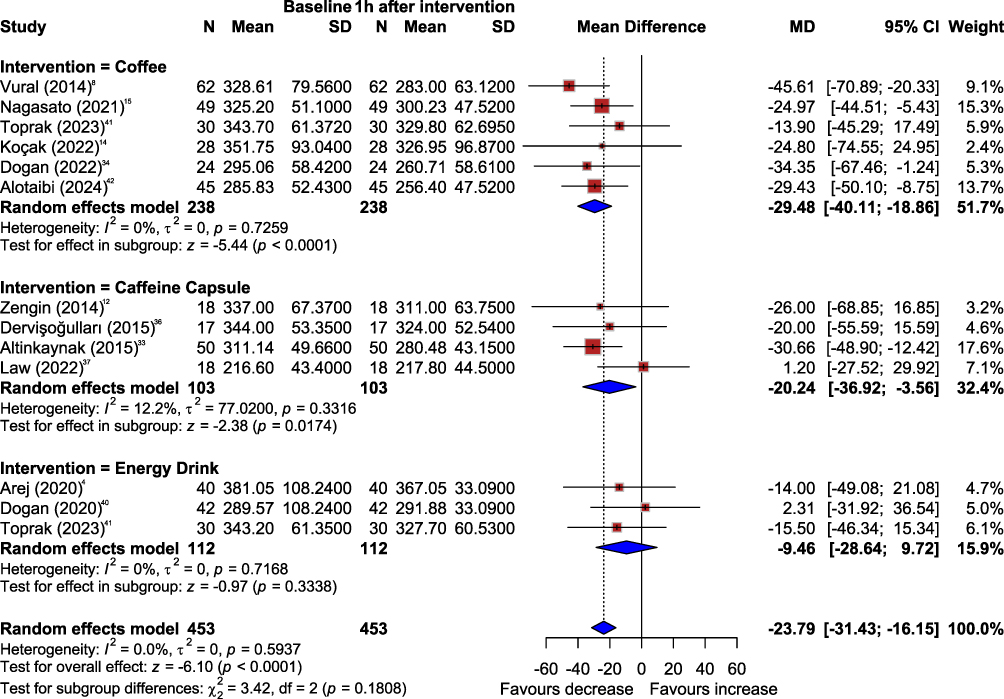 |
Figure 2 SFCT subgroup analysis, according to type of intervention. Abbreviations: SFCT, subfoveal choroidal thickness; Baseline, before intervention; 1h after intervention, 1 hour after intervention; N, number of participants; Mean, Mean SFCT (µm); MD, mean difference; SD, standard deviation; 95% CI, 95% Confidence Interval; I2, heterogeneity; p, p-value. |
This outcome was further analyzed by refractive status (Figure 3). In the emmetropic group (324 participants), caffeine intake was associated with a significant reduction of –28.47 micrometers (95% CI: –38.03 to –18.90; p < 0.001). A similar effect was observed among myopic patients, with a reduction of –32.86 micrometers (95% CI: –53.14 to –12.58; p = 0.002). However, in the subgroup of high myopes, caffeine intake did not demonstrate effectiveness, with a non-significant MD of –0.13 micrometers (95% CI: –27.82 to 27.56; p = 0.99).
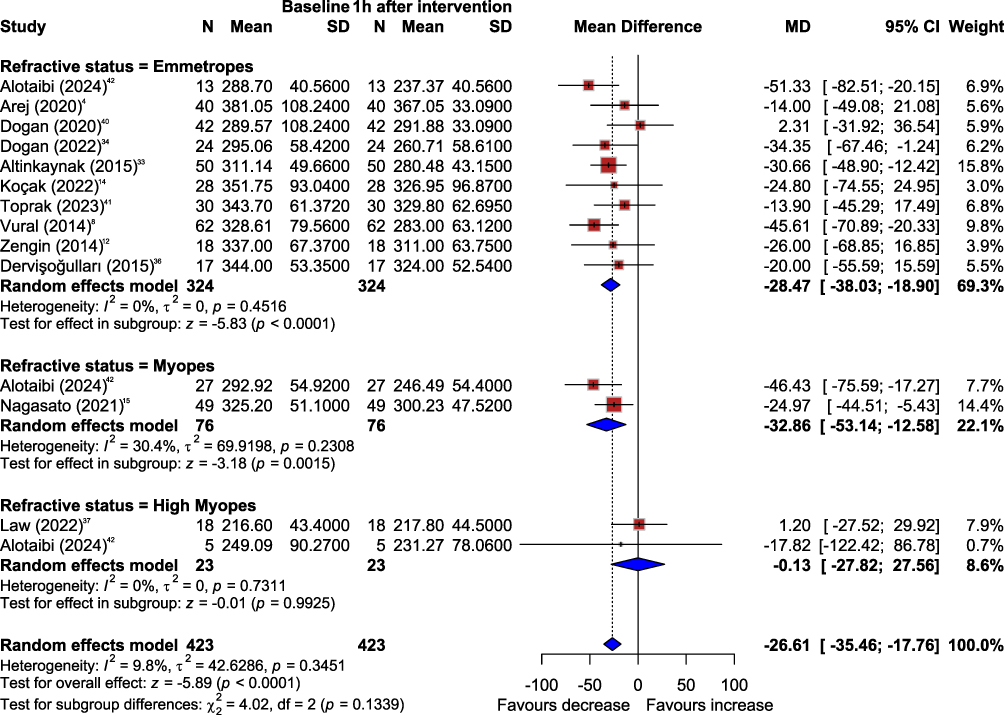 |
Figure 3 SFCT subgroup analysis, according to refractive status. Abbreviations: SFCT, subfoveal choroidal thickness; Baseline, before intervention; 1h after intervention, 1 hour after intervention; N, number of participants; Mean, Mean SFCT (µm); MD, mean difference; SD, standard deviation; 95% CI, 95% Confidence Interval; I2, heterogeneity; p, p-value. |
Additionally, subgroup analysis by study design was conducted (Supplementary Figure 1), encompassing 423 eyes (224 in the non-randomized subgroup and 199 in the randomized subgroup). For both subgroups, a significant reduction in SFCT at 1 h post-ingestion was observed. Nevertheless, this trend was greater in the randomized subgroup (MD = –32.52; 95% CI: –44.29 to –20.75; p < 0.0001) compared to the non-randomized subgroup (MD = –17.33; 95% CI: –28.40 to –6.25; p = 0.002).
Deep Capillary Vessel Density
The evaluation of DVD was performed across three retinal regions: foveal, parafoveal, and perifoveal. Thus, the study by Jacobs et al (2024)26 was not included in the meta-analysis, as DVD was reported only for 3×3 mm and 6×6 mm scans centered on the fovea. In that study, no significant differences in DVD at 1 hour post-intervention were observed between the caffeine and placebo groups for either the 3×3 mm (p = 0.760) or the 6×6 mm (p = 0.242) scans.
A total of 204 participants were included in the foveal region. No statistically significant alteration in DVD was observed, with a pooled MD of –0.94% (95% CI: –2.26 to 0.38; p = 0.16). The analysis further revealed a substantial heterogeneity of 59.2%, indicating variability among the included studies. A subgroup analysis was performed to identify potential factors contributing to heterogeneity and to provide a more specific assessment (Figure 4). The use of caffeine capsules demonstrated a statistically significant reduction in foveal DVD, with a pooled MD of –2.23% (95% CI: –3.70 to –0.76; p = 0.003) and no heterogeneity (I2 = 0%). In contrast, other types of interventions, including coffee, energy drinks, or black tea, did not show statistically significant effects on this outcome. These subgroup differences were statistically significant (p = 0.007).
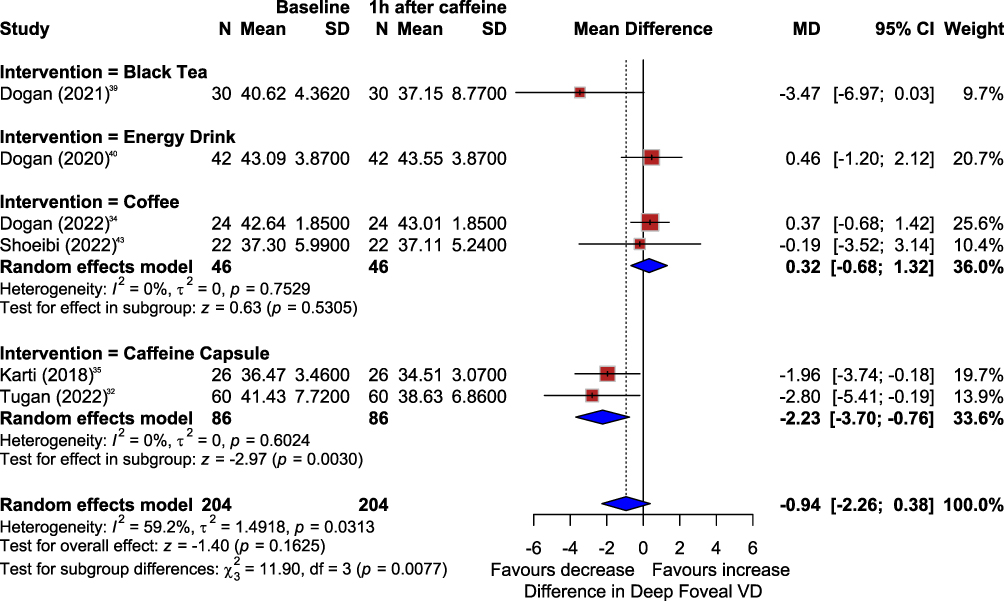 |
Figure 4 Foveal DVD subgroup analysis, according to intervention. Abbreviations: VD, vessel density; Baseline, before intervention; 1h after caffeine, 1 hour after intervention; N, number of participants; Mean, mean VD (%); MD, mean difference; SD, standard deviation; 95% CI, 95% Confidence Interval; I2, heterogeneity; p, p-value. |
In the parafoveal region, a total of 204 participants were evaluated. No statistically significant overall difference was observed, with a pooled MD of –0.39% (95% CI: –2.45 to 1.66; p = 0.71) and a substantial heterogeneity of 84.9%, suggesting considerable variability across studies. In the subgroup, participants who ingested caffeine capsules demonstrated a statistically significant reduction in parafoveal DVD (Figure 5), with a pooled MD of –2.18% (95% CI: –3.13 to –1.24; p < 0.001) and no heterogeneity (I2 = 0%). Similarly, in the subgroup of patients who consumed caffeinated coffee, a significant reduction of –1.83% (95% CI: –3.17 to –0.50; p = 0.007) was also observed. In contrast, studies evaluating energy drinks and black tea showed an increase in parafoveal DVD.
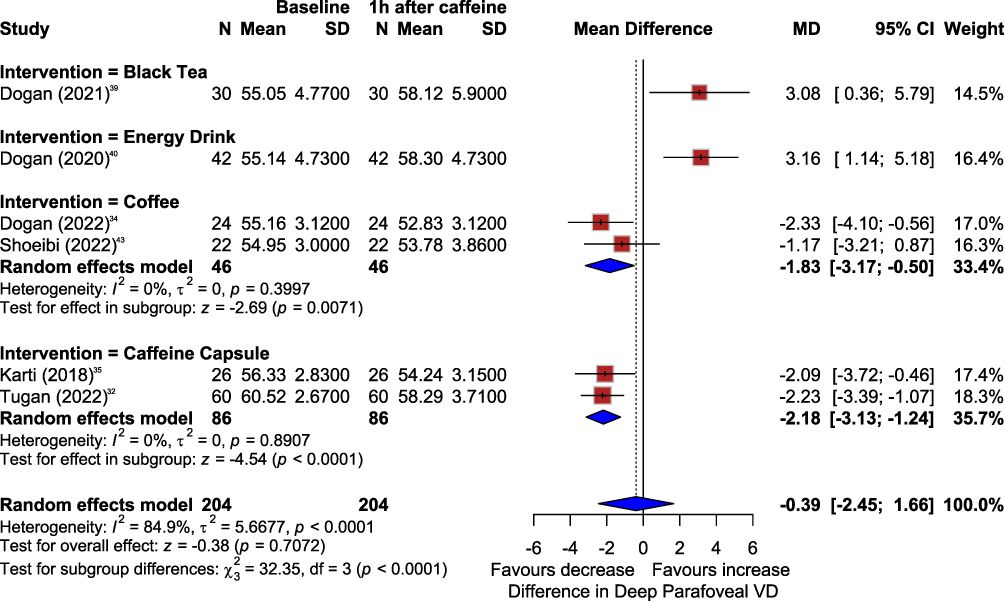 |
Figure 5 Parafoveal DVD subgroup analysis by intervention. Abbreviations: VD, vessel density; Baseline, before intervention; 1h after caffeine, 1 hour after intervention; N, number of participants; Mean, mean VD (%); MD, mean difference; SD, standard deviation; 95% CI, 95% Confidence Interval; I2, heterogeneity; p, p-value. |
A total of 178 participants were evaluated in the perifoveal region. The combined analysis did not reveal a statistically significant change in DVD, with a pooled MD of –1.18% (95% CI: –4.08 to 1.71%; p = 0.42). In the subgroup analysis, distinct patterns emerged (Supplementary Figure 2). The study assessing caffeine capsules demonstrated a statistically significant reduction in perifoveal DVD (95% CI: –6.84 to –3.00), whereas interventions with coffee (95% CI: –3.93 to 0.74) and black tea (95% CI: –4.39; 1.68) did not show statistically significant results. Conversely, the study evaluating energy drinks observed a substantial increase in perifoveal DVD (MD = 3.41%; 95% CI: 1.09 to 5.73). Consequently, subgroup differences were statistically significant (p < 0.0001).
Superficial Capillary Vessel Density
SVD was analyzed across the same retinal regions as in the DVD assessment. The study by Jacobs et al (2024)26 was again excluded from the meta-analysis due to the previously referred difference in measurement reporting. Consistently, this study found no statistically significant differences SVD at 1 hour post-ingestion between the caffeine and control groups for either the 3×3 mm (p = 0.460) or 6×6 mm (p = 0.175) scans.
In the foveal region, a total of 222 participants were analyzed. The combined analysis of studies evaluating caffeine intake through different forms, including coffee, caffeine capsules, black tea, and energy drinks, demonstrated a statistically significant reduction in SVD, with a pooled MD of –0.87% (95% CI: –1.60 to –0.14; p = 0.02). The analysis revealed no heterogeneity (I2 = 0%), indicating highly consistent results across the included interventions (Figure 6). In the subgroup analysis, both specific interventions showed reductions in foveal SVD; however, these reductions did not reach statistical significance individually and became significant only when the studies were pooled.
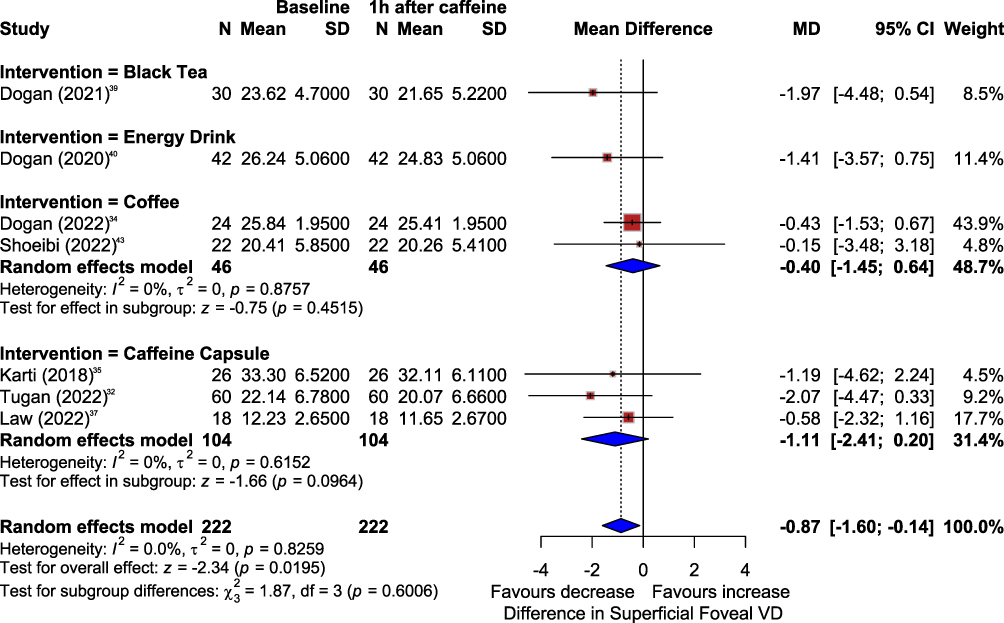 |
Figure 6 SVD subgroup analysis, according to intervention. Abbreviations: VD, vessel density; Baseline, before intervention; 1h after caffeine, 1 hour after intervention; N, number of participants; Mean, mean VD (%); MD, mean difference; SD, standard deviation; 95% CI, 95% Confidence Interval; I2, heterogeneity; p, p-value. |
In the parafoveal region, the pooled analysis demonstrated a statistically significant reduction in SVD, with a MD of –1.39% (95% CI: –2.36 to –0.43; p = 0.005) and a substantial heterogeneity of 79.4%. In the subgroup analysis, studies evaluating caffeine capsules and coffee maintained the same pattern (Figure 7), showing statistically significant reductions in parafoveal SVD (MD = –1.80% and –1.74%; 95% CI: –2.36% to –0.31 and –3.18 to –0.31, respectively). In contrast, studies that investigated black tea and energy drinks did not report significant alterations in this parameter within the parafoveal region.
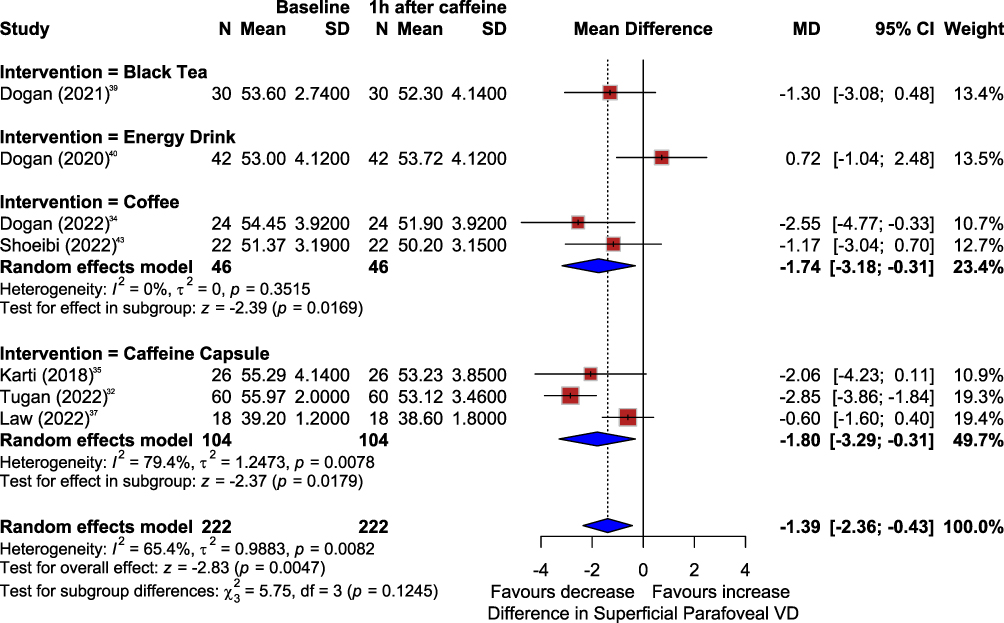 |
Figure 7 Parafoveal SVD subgroup analysis, according to intervention. Abbreviations: VD, vessel density; Baseline, before intervention; 1h after caffeine, 1 hour after intervention; N, number of participants; Mean, mean VD (%); MD, mean difference; SD, standard deviation; 95% CI, 95% Confidence Interval; I2, heterogeneity; p, p-value. |
In the perifoveal region, the results were consistent with the observations in the parafoveal areas. The pooled analysis revealed a statistically significant reduction in SVD, with a MD of –1.04% (95% CI: –1.90 to –0.19; p = 0.017) and moderate heterogeneity (I2 = 52.8%). Subgroup analysis (Supplementary Figure 3A) indicated that the reduction was significant for the caffeine capsule intervention (MD = –1.84%; 95% CI: –2.55 to –1.13), but not for the coffee intervention alone (MD = –1.48%; 95% CI: –3.23 to 0.28; p = 0.1). However, when coffee and caffeine capsule subgroups were combined (Supplementary Figure 3B), significance was reached (MD = –1.79%; 95% CI: –2.45 to –1.13; p < 0.0001). In contrast, interventions with energy drinks and black tea did not demonstrate significant reductions in this region (MD: –0.45%, 95% CI: –1.29 to 0.39; and MD: –0.05%, 95% CI: –1.67 to 1.57, respectively).
Risk of Bias
Figure 8A and 8B (RoB-2 and ROBINS-I, respectively) illustrate the risk of bias assessment for each study. Among the randomized studies, four were well-designed and classified as low risk of bias, while another four raised some concerns due to issues with randomization and population selection. For ROBINS-I, two studies were judged to have a critical overall risk of bias: Shoeibi et al, as it was a case series with inherent methodological limitations, and Nagasato et al, which introduced critical bias by selecting both study groups. Studies by Aloitabi et al (2024), Altinkaynak et al (2015), Dogan et al (2021), and Toprak Sr et al (2023) were rated as having a serious risk of bias due to lack of randomization or failure to account for important confounders such as habitual caffeine consumption. The remaining studies (Arej et al 2021; Dervişoğullari et al 2015; Dogan et al 2020, Dogan et al 2022) were classified as having a moderate overall risk of bias, primarily due to concerns related to randomization, missing data, and misclassification of interventions.
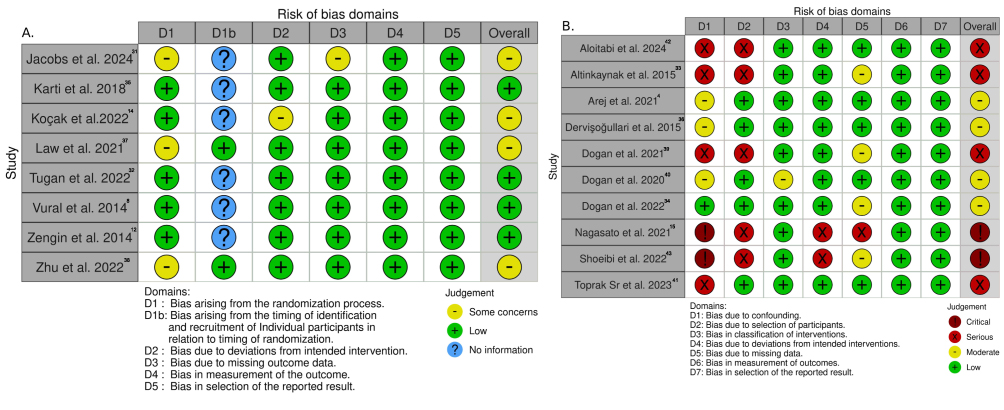 |
Figure 8 (A) RoB-2 risk of bias. (B) ROBINS-I risk of bias. |
Discussion
In this systematic review and meta-analysis of 18 studies involving 966 patients, we evaluated the acute impact of caffeine on ocular microvasculature using OCT and OCTA imaging. Our analysis identifies a significant and consistent thinning of the subfoveal choroid following caffeine ingestion, regardless of whether it was administered via capsules or energy drinks. In the retinal circulation, we observed a general reduction in SVD across the foveal and extrafoveal regions. However, the response of the deep capillary plexus was markedly more heterogeneous, appearing sensitive to the specific source of caffeine. While caffeine capsules and coffee tended to reduce DVD, energy drinks and tea often showed negligible or even opposing effects. These findings suggest that while caffeine generally promotes ocular vasoconstriction, the net vascular response is influenced by the delivery vehicle and the specific retinal layer being measured.
The consistent thinning of the choroid identified in this meta-analysis reinforces the physiological role of caffeine as a potent adenosine receptor antagonist.1,44 By blocking adenosine receptors, caffeine inhibits the vasodilation typically maintained by endogenous adenosine, thereby promoting vasoconstriction within the highly vascularized choroidal tissue.1,7 To ensure accuracy in these measurements, several included studies employed Enhanced Depth Imaging (EDI), which provides improved visualization of the choroidal layers and allows for more precise demarcation of the chorioretinal interface.13,45 These findings quantitatively corroborate numerous observational studies reporting reduced thickness following caffeine ingestion.8,12,14,15 While this vasoconstrictive effect extends to the retinal circulation, the response in the deep capillary plexus remains more variable.20,27 This discrepancy may be influenced by the type of OCT technology used; for instance, Jacobs et al observed significant effects using swept-source OCTA (SS-OCTA), which offers faster acquisition and reduced susceptibility to motion artifacts compared to the spectral-domain platforms (SD-OCTA) used by Tugan et al26,27 Such technical differences may partly explain the variations in reported effect sizes across the literature. Compared with Tugan et al, who used SD-OCT, Jacobs et al observed a significant effect, although of lesser magnitude. A clinically relevant finding from our subgroup analysis is the differential impact of caffeine source on ocular hemodynamics. Coffee elicited a stronger reduction in SFCT (–29.48 µm) compared with pure caffeine capsules (–20.24 µm), suggesting that additional bioactive compounds in coffee may exert synergistic vasoconstrictive effects.46 In contrast, energy drinks did not produce significant changes in SFCT, despite containing higher caffeine concentrations. This divergence from the consistent effects observed with coffee and caffeine capsules8,12,14,15 supports the hypothesis that other ingredients commonly present in energy drinks, such as taurine or L-carnitine, may exert vasodilatory effects,47,48 that counteract the primary vasoconstrictive action of caffeine. This complex interaction suggests that caffeine may not be the sole causal factor in the hemodynamic response to these specific formulations. Furthermore, given the modest magnitude of the observed changes, it is possible that a portion of the report effects reflects inherent physiological variability or measurement noise rather than a definitive pharmacological event. Acknowledging these confounding factors is fundamental to the conceptual validity of the findings, as it characterizes the retinal and choroidal response to a multifactorial process.
Caffeine, a methylxanthine-class central nervous system stimulant, influences both cerebral and ocular blood flow.1,49 Its primary mechanism of action involves antagonism of adenosine receptor subtypes and the indirect release of catecholamines, which inhibit adenosine-mediated vasodilation and promote vasoconstriction.1 OCT and OCTA enable detailed assessment of these effects using markers such as vessel length, perfusion density, the foveal avascular zone, and choroidal thickness.50 However, interpreting these changes requires caution, as the choroid is a highly dynamic tissue. Its thickness is influenced by a wide array of confounding factors, including age, refractive error, diurnal variation, and perfusion pressure.45,50–58 Therefore, studies assessing this outcome should thoroughly specify patient characteristics to account for heterogeneous populations, particularly concerning these confounding factors. However, several of the included studies did not adequately address these variables, limiting the ability to determine whether observed differences in choroidal thickness were attributable to caffeine itself or to underlying individual variation.
The transient vasoconstrictive effect of caffeine, though generally benign in healthy individuals, may become clinically relevant in the presence of ocular pathologies such as degenerative myopia, age-related macular degeneration (AMD), and diabetic retinopathy (DR).45,59–63 While our findings of reduced SFCT in emmetropic and myopic eyes are consistent with prior,4,8,14,15 the absence of this effect in high myopia is a novel observation. In highly myopic eyes, where choroidal thinning is a well-established predictor of visual acuity loss,49–51 unique anatomical alterations could plausibly blunt the vascular response to caffeine.45,59,62 However, given the limited sample sizes in these subgroups, the lack of significance may equally reflect insufficient statistical power rather than a true physiological resistance to caffeine. In DR, reductions in vessel and perfusion density and enlargement of the foveal avascular zone correlate with disease severity.64 Thus, additional vasoconstrictive stress from caffeine may further reduce perfusion, exacerbating ischemic risk. Similarly, in dry AMD, caffeine-induced microvascular constriction could aggravate ischemic compromise, consistent with the ischemic hypothesis of pathogenesis.63,65,66
This study has important limitations. First, the inclusion of both randomized and non-randomized studies introduces heterogeneity in study design, quality, caffeine dosage, and the timing of post-ingestion measurements, which may affect the reliability of pooled estimates. Second, the patient populations differed in their physiological adaptation to caffeine, with some regular coffee/caffeine drinkers and others not, which could influence choroidal thickness measurements and limit the generalizability of the findings. Finally, although OCT and OCTA are established methods for measuring choroidal thickness and vessel density, differences in imaging modality, device, algorithm, and acquisition protocols across studies may have contributed to measurement variability. Random effects, quality assessment, and sensitivity analysis were used to try to mitigate these limitations.
Conclusion
This meta-analysis found consistent evidence that caffeine intake induces measurable, acute changes in the posterior eye segment, specifically through a temporary decrease in SFCT and SVD, but not DVD. These alterations are short-term, with most parameters returning to baseline within hours of ingestion. The subgroup analyses reveal that this effect is complex and is significantly modulated by the delivery vehicle and refractive status of the eyes. These findings underscore the importance of controlling caffeine intake in both clinical and research settings to ensure the accurate interpretation of advanced ocular imaging.
Data Sharing Statement
All relevant data are within the manuscript and Supplementary Data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare that they have no affiliations with or involvement in any organization or entity with any interest in the subject matter or materials discussed in this manuscript.
References
1. Justin E, John RR, Amanda SB. Caffeine. Vol. 2. Treasure Island (FL): StatPearls Publishing; 2025. doi:10.1016/B978-0-12-824315-2.00372-9
2. Grzegorzewski J, Bartsch F, Köller A, König M. Pharmacokinetics of caffeine: a systematic analysis of reported data for application in metabolic phenotyping and liver function testing. Front Pharmacol. 2022;12. doi:10.3389/FPHAR.2021.752826
3. Blanchard J, Sawers SJA. The absolute bioavailability of caffeine in man. Eur J Clin Pharmacol. 1983;24(1):93–16. doi:10.1007/BF00613933
4. Arej N, Azar G, Salviat F, et al. Study of choroidal thickness variations after ingestion of a taurine and caffeine-containing energy drink. Clin Nutr ESPEN. 2021;43:245–249. doi:10.1016/j.clnesp.2021.04.007
5. Mort JR, Kruse HR. Timing of blood pressure measurement related to caffeine consumption. Ann Pharmacother. 2008;42(1):105–110. doi:10.1345/APH.1K337
6. Gahr M. Caffeine, the most frequently consumed psychostimulant: a narrative review article. Fortschritte der Neurologie Psychiatrie. 2020;88(5):318–330. doi:10.1055/A-0985-4236
7. Fisone G, Borgkvist A, Usiello A. Caffeine as a psychomotor stimulant: mechanism of action. Cell Mol Life Sci. 2004;61(7–8):857–872. doi:10.1007/S00018-003-3269-3
8. Vural AD, Kara N, Sayin N, Pirhan D, Ersan HBA. Choroidal thickness changes after a single administration of coffee in healthy subjects. Retina. 2014;34(6):1223–1228. doi:10.1097/IAE.0000000000000043
9. Terai N, Spoerl E, Pillunat LE, Stodtmeister R. The effect of caffeine on retinal vessel diameter in young healthy subjects. Acta Ophthalmol. 2012;90(7). doi:10.1111/J.1755-3768.2012.02486.X
10. Özkan B, Yüksel N, Anik Y, Altintaş Ö, Demirci A, Çaǧlar Y. The effect of caffeine on retrobulbar hemodynamics. Curr Eye Res. 2008;33(9):804–809. doi:10.1080/02713680802344708
11. Cole ED, Moult EM, Dang S, et al. The definition, rationale, and effects of thresholding in OCT angiography. Ophthalmol Retina. 2017;1(5):435–447. doi:10.1016/J.ORET.2017.01.019
12. Zengin MO, Cinar E, Karahan E, Tuncer I, Kucukerdonmez C. The effect of caffeine on choroidal thickness in young healthy subjects. Cutan Ocul Toxicol. 2015;34(2):112–116. doi:10.3109/15569527.2014.912659
13. Branchini LA, Adhi M, Regatieri CV, et al. Analysis of choroidal morphologic features and vasculature in healthy eyes using spectral-domain optical coherence tomography. Ophthalmology. 2013;120(9):1901–1908. doi:10.1016/j.ophtha.2013.01.066
14. Koçak N, Beldağlı C, Yeter V. Acute effects of coffee on peripapillary and subfoveal choroidal parameters in young healthy subjects. Eur J Ophthalmol. 2022;32(6):3584–3591. doi:10.1177/11206721221078660
15. Nagasato D, Mitamura Y, Egawa M, et al. Changes in choroidal component ratio and circulation after coffee intake in healthy subjects. Invest Ophthalmol Vis Sci. 2021;62(3):27. doi:10.1167/IOVS.62.3.27
16. Yan A, La Rosa A, Chhablani PP, Chhablani J. Caffeine and vision: effects on the eye. Turk J Ophthalmol. 2024;54(5):291–300. doi:10.4274/TJO.GALENOS.2024.43895
17. Motamed Shariati M, Khazaei S, Yaghoobi M. Choroidal vascularity index in health and systemic diseases: a systematic review. Int J Retina Vitreous. 2024;10(1). doi:10.1186/S40942-024-00607-8
18. Regatieri CV, Novais EA, Branchini L, et al. Choroidal thickness in older patients with central serous chorioretinopathy. Int J Retina Vitreous. 2016;2(1):1–6. doi:10.1186/S40942-016-0046-7/FIGURES/4
19. Nickla DL, Wallman J. The multifunctional choroid. Prog Retin Eye Res. 2010;29(2):144–168. doi:10.1016/J.PRETEYERES.2009.12.002
20. Işik MU, Akay F, Akmaz B, Güven YZ, Şahin ÖF. Evaluation of subclinical alterations in retinal layers and microvascular structures with OCT and OCTA in healthy young short-term smokers. Photodiagnosis Photodyn Ther. 2021;36:102482. doi:10.1016/J.PDPDT.2021.102482
21. Yeung SC, Park JY, Park D, You Y, Yan P. The effect of systemic and topical ophthalmic medications on choroidal thickness: a review. Br J Clin Pharmacol. 2022;88(6):2673–2685. doi:10.1111/BCP.15237
22. Mansour AM, Koaik M, Lima LH, et al. Physiologic and psychologic risk factors in central serous chorioretinopathy. Ophthalmol Retina. 2017;1(6):497–507. doi:10.1016/J.ORET.2017.02.009
23. Toussaint BM, Shaikh AM, Sisk RM. Caffeine and CSCR: is there a link? Emerging evidence suggests a causal relationship between caffeine and central serous chorioretinopathy. 2015. Available from: https://www.retina-specialist.com/article/caffeine-and-cscr-is-there-a-link.
24. Raimundo M, Mira F, Cachulo ML, et al. Adherence to a mediterranean diet, lifestyle and age-related macular degeneration: the coimbra eye study – report 3. Acta Ophthalmol. 2018;96(8):e926–e932. doi:10.1111/AOS.13775
25. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:372. doi:10.1136/BMJ.N71
26. Jacobs M, Demas N, Hemesath A, et al. Optical coherence tomography angiography: investigating vessel density changes induced by caffeine in healthy subjects. J Ophthalmol. 2024;2024(1):5597188. doi:10.1155/2024/5597188
27. Tugan BY, Subasi S, Pirhan D, Karabas L, Yuksel N, Kucuk KD. Evaluation of macular and peripapillary vascular parameter change in healthy subjects after caffeine intake using optical coherence tomography angiography. Indian J Ophthalmol. 2022;70(3):879–889. doi:10.4103/IJO.IJO_1989_21
28. Altinkaynak H, Ceylan E, Kartal B, Keleş S, Ekinci M, Olcaysu OO. Measurement of choroidal thickness following caffeine intake in healthy subjects. Curr Eye Res. 2016;41(5):708–714. doi:10.3109/02713683.2015.1020168
29. Dogan M, Akdogan M, Sabaner MC, Gobeka HH. Morphological changes in retinochoroidal microvasculature after caffeinated versus decaffeinated coffee consumption. Photodiagnosis Photodyn Ther. 2022;40. doi:10.1016/j.pdpdt.2022.103138
30. Karti O, Zengin MO, Kerci SG, Ayhan Z, Kusbeci T. Acute effect of caffeine on macular microcirculation in healthy subjects: an optical coherence tomography angiography study. Retina. 2019;39(5):964–971. doi:10.1097/IAE.0000000000002058
31. Dervişoğulları MS, Totan Y, Yüce A, Kulak AE. Acute effects of caffeine on choroidal thickness and ocular pulse amplitude. Cutan Ocul Toxicol. 2016;35(4):281–286. doi:10.3109/15569527.2015.1104330
32. Law VK, Lam AK. Effect of caffeine on superficial retinal vasculature of the macula in high myopes using optical coherence tomography angiography – a pilot study. J Optom. 2022;15(3):210–218. doi:10.1016/j.optom.2021.06.005
33. Zhu X, Zhu J, Wang Y, et al. A moderate dosage of coffee causes acute retinal capillary perfusion decrease in healthy young individuals. BMC Ophthalmol. 2022;22(1). doi:10.1186/s12886-022-02638-x
34. Doğan M, Akdoğan M, Alizada A, et al. Impacts of Camellia sinensis fermentation end-product (black tea) on retinal microvasculature: an updated OCTA analysis. J Sci Food Agric. 2021;101(15):6265–6270. doi:10.1002/jsfa.11294
35. Doğan M, Sabaner MC, Akar AT, et al. Evaluation of the effect of energy drink consumption on retina and choroid: an optical coherence tomography and optical coherence tomography angiography study. Cutan Ocul Toxicol. 2020;39(4):295–297. doi:10.1080/15569527.2020.1755977
36. Toprak G, Alkan Y. Comparison of the short-term effect of coffee, energy drink, and water on the eyes in young healthy subjects. Cureus. 2023;15(11). doi:10.7759/cureus.48335
37. Alotaibi W, Alhazmi M, Khormi S, Almaslokh T, Alanazi M, Althomali M. Variations in choroidal thickness between emmetropic and myopic eyes after caffeine intake. Indian J Ophthalmol. 2024;72(Suppl 3):S488–S494. doi:10.4103/IJO.IJO_2502_23
38. Shoeibi N, Rajaei P, Ghobadi M, et al. Acute effects of coffee consumption on the microcirculation of macula and optic nerve head. Nutr Health. 2022. doi:10.1177/02601060221130424
39. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366. doi:10.1136/BMJ.L4898
40. Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355. doi:10.1136/BMJ.I4919
41. Abbas A, Hefnawy MT, Negida A. Meta-analysis accelerator: a comprehensive tool for statistical data conversion in systematic reviews with meta-analysis. BMC Med Res Methodol. 2024;24(1):1–11. doi:10.1186/S12874-024-02356-6/FIGURES/8
42. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1). doi:10.1186/1471-2288-14-135
43. Higgins J, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.5. Cochrane; 2024.
44. Ferré S. An update on the mechanisms of the psychostimulant effects of caffeine. J Neurochem. 2008;105(4):1067–1079. doi:10.1111/J.1471-4159.2007.05196.X
45. Fujiwara T, Imamura Y, Margolis R, Slakter JS, Spaide RF. Enhanced depth imaging optical coherence tomography of the choroid in highly myopic eyes. Am J Ophthalmol. 2009;148(3):445–450. doi:10.1016/j.ajo.2009.04.029
46. Kalsner S. A coronary vasoconstrictor substance is present in regular and “decaffeinated” forms of both percolated and instant coffee. Life Sci. 1977;20(10):1689–1696. doi:10.1016/0024-3205(77)90344-7
47. Alhasaniah AH. l-carnitine: nutrition, pathology, and health benefits. Saudi J Biol Sci. 2023;30(2):103555. doi:10.1016/J.SJBS.2022.103555
48. Yildiz O, Ulusoy KG. Effects of taurine on vascular tone. Amino Acids. 2022;54(12):1527–1540. doi:10.1007/S00726-022-03198-6
49. Poole R, Kennedy OJ, Roderick P, Fallowfield JA, Hayes PC, Parkes J. Coffee consumption and health: umbrella review of meta-analyses of multiple health outcomes. BMJ. 2017;359(j5024). doi:10.1136/BMJ.J5024
50. Fujiwara A, Morizane Y, Hosokawa M, et al. Factors affecting foveal avascular zone in healthy eyes: an examination using swept-source optical coherence tomography angiography. PLoS One. 2017;12(11):e0188572. doi:10.1371/JOURNAL.PONE.0188572
51. Michalewski J, Michalewska Z, Nawrocka Z, Bednarski M, Nawrocki J. Correlation of choroidal thickness and volume measurements with axial length and age using swept source optical coherence tomography and optical low-coherence reflectometry. Biomed Res Int. 2014;2014:1–7. doi:10.1155/2014/639160
52. Kiel JW, van Heuven WA. Ocular perfusion pressure and choroidal blood flow in the rabbit. Invest Ophthalmol Vis Sci. 1995;36(3):579–585.
53. Polak K, Luksch A, Berisha F, Fuchsjaeger-Mayrl G, Dallinger S, Schmetterer L. Altered nitric oxide system in patients with open-angle glaucoma. Arch Ophthalmol. 2007;125(4):494–498. doi:10.1001/ARCHOPHT.125.4.494
54. Reitsamer HA, Zawinka C, Branka M. Dopaminergic vasodilation in the choroidal circulation by d1/d5 receptor activation. Invest Ophthalmol Vis Sci. 2004;45(3):900–905. doi:10.1167/IOVS.03-0997
55. Li C, Fitzgerald MEC, Del Mar N, Haughey C, Reiner A. Defective choroidal blood flow baroregulation and retinal dysfunction and pathology following sympathetic denervation of choroid. Invest Ophthalmol Vis Sci. 2018;59(12):5032–5044. doi:10.1167/IOVS.18-24954
56. Delgado E, Marques-Neves C, Rocha I, Sales-Luís J, Silva-Carvalho L. Intrinsic vasomotricity and adrenergic effects in a model of isolated rabbit eye. Acta Ophthalmol. 2009;87(4):443–449. doi:10.1111/J.1755-3768.2008.01285.X
57. Lee SW, Yu SY, Seo KH, Kim ES, Kwak HW. Diurnal variation in choroidal thickness in relation to sex, axial length, and baseline choroidal thickness in healthy Korean subjects. Retina. 2014;34(2):385–393. doi:10.1097/IAE.0B013E3182993F29
58. Alanazi M, Caroline P, Alshamrani A, Alanazi T, Liu M. Regional distribution of choroidal thickness and diurnal variation in choroidal thickness and axial length in young adults. Clin Ophthalmol. 2021;15:4573–4584. doi:10.2147/OPTH.S334619
59. Nishida Y, Fujiwara T, Imamura Y, Lima LH, Kurosaka D, Spaide RF. Choroidal thickness and visual acuity in highly myopic eyes. Retina. 2012;32(7):1229–1236. doi:10.1097/IAE.0B013E318242B990
60. Mahmud M, Ahem A, Bastion MLC, et al. The relationship between choroidal and photoreceptor layer thickness with visual acuity in highly myopic eyes. Front Cell Neurosci. 2022;16. doi:10.3389/FNCEL.2022.800065
61. Sanchez-Cano A, Orduna E, Segura F, et al. Choroidal thickness and volume in healthy young white adults and the relationships between them and axial length, ammetropy and sex. Am J Ophthalmol. 2014;158(3):574–583.e1. doi:10.1016/j.ajo.2014.05.035
62. Flores-Moreno I, Lugo F, Duker JS, Ruiz-Moreno JM. The relationship between axial length and choroidal thickness in eyes with high myopia. Am J Ophthalmol. 2013;155(2):314–319.e1. doi:10.1016/J.AJO.2012.07.015
63. Gupta N, Padidam S, Tewari A. Acute macular neuroretinopathy (AMN) related to energy drink consumption. BMJ Case Rep. 2019;12(12):e232144. doi:10.1136/BCR-2019-232144
64. Ratra D, Dalan D, Prakash N, et al. Quantitative analysis of retinal microvascular changes in prediabetic and diabetic patients. Indian J Ophthalmol. 2021;69(11):3226–3234. doi:10.4103/IJO.IJO_1254_21
65. Kim SW, Oh J, Kwon SS, Yoo J, Huh K. Comparison of choroidal thickness among patients with healthy eyes, early age-related maculopathy, neovascular age-related macular degeneration, central serous chorioretinopathy, and polypoidal choroidal vasculopathy. Retina. 2011;31(9):1904–1911. doi:10.1097/IAE.0B013E31821801C5
66. Nagaoka T, Kitaya N, Sugawara R, et al. Alteration of choroidal circulation in the foveal region in patients with type 2 diabetes. Br J Ophthalmol. 2004;88(8):1060–1063. doi:10.1136/BJO.2003.035345
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Spotlight on Lattice Degeneration Imaging Techniques

Maltsev DS, Kulikov AN, Shaimova VA, Burnasheva MA, Vasiliev AS
Clinical Ophthalmology 2023, 17:2383-2395
Published Date: 16 August 2023
Caffeine in Hepatocellular Carcinoma: Cellular Assays, Animal Experiments, and Epidemiological Investigation
Shan L, Zhao N, Wang F, Zhai D, Liu J, Lv X
Journal of Inflammation Research 2024, 17:1589-1605
Published Date: 11 March 2024
Subfoveal Choroidal Thickness After Successful Retinal Detachment Repair with Persistent Subretinal Fluid at the Macula
Mansour AM, Parodi MB, Uwaydat SH, Lima LH, Charbaji S, Casella AM, López-Guajardo L, Belotto S, Wu L, Schwartz SG, Smiddy WE, Hassoun MM, Pérez-Salvador García E, Mansour HA, Elnahry AG, Hamam RN
Clinical Ophthalmology 2025, 19:1847-1854
Published Date: 11 June 2025
Serum Apolipoprotein B and B/A1 Ratio as Early Negative Biomarkers for OCT- and OCTA-Detected Retinal Changes in Diabetic Macular Edema
Soedarman S, Julia M, Gondhowiardjo TD, Kurnia KH, Prasetya ADB, Triyoga IF, Sasongko MB
Clinical Ophthalmology 2025, 19:2165-2178
Published Date: 9 July 2025
Subfoveal Choroidal Thickness in Clinically Significant Pseudophakic Cystoid Macular Edema: An Interocular Comparison with Contralateral Pseudophakic Eyes
Demir K, Çelik E
Clinical Ophthalmology 2026, 20:605546
Published Date: 10 June 2026