Back to Journals » Clinical Ophthalmology » Volume 20
Subfoveal Choroidal Thickness in Clinically Significant Pseudophakic Cystoid Macular Edema: An Interocular Comparison with Contralateral Pseudophakic Eyes
Received 26 February 2026
Accepted for publication 23 May 2026
Published 10 June 2026 Volume 2026:20 605546
DOI https://doi.org/10.2147/OPTH.S605546
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Kadriye Demir,1 Erkan Çelik2
1Department of Ophthalmology, Sakarya University Medical Education and Research Hospital, Sakarya, Turkey; 2Department of Ophthalmology, Sakarya Dünyagöz Hospital, Sakarya, Turkey
Correspondence: Kadriye Demir, Department of Ophthalmology, Sakarya University Medical Education and Research Hospital, Sakarya, 54000, Turkey, Email [email protected] Erkan Çelik, Department of Ophthalmology, Sakarya Dünyagöz Hospital, Sakarya, 54000, Turkey, Email [email protected]
Purpose: To evaluate subfoveal choroidal thickness (SCT) in eyes with clinically significant pseudophakic cystoid macular edema (PCME) and compare it with the contralateral pseudophakic eyes that underwent uncomplicated cataract surgery within a similar postoperative period using enhanced depth imaging optical coherence tomography (EDI-OCT).
Methods: This retrospective observational study included 25 patients with clinically significant PCME following uneventful phacoemulsification and posterior chamber intraocular lens implantation. The control group consisted of contralateral pseudophakic eyes that had undergone uncomplicated cataract surgery within one month of the affected eye and did not develop PCME. SCT and central macular thickness (CMT) were measured using spectral-domain OCT with EDI mode. Best-corrected visual acuity (BCVA), age, and sex were recorded. Paired comparisons were performed between PCME eyes and pseudophakic fellow eyes to minimize the confounding effect of surgery-related choroidal changes.
Results: The mean age of the patients was 66.13 ± 5.44 years (range, 59– 77). 14 (56%) were male and 11 (44%) were female. The mean interval between cataract surgery and PCME diagnosis was 6.2 ± 1.6 weeks. The mean CMT was significantly higher in PCME eyes (458.20 ± 92.30 μm) compared with pseudophakic fellow eyes (235.66 ± 28.43 μm, p < 0.001). The mean SCT was 297.27 ± 24.52 μm in PCME eyes and 289.41 ± 22.16 μm in pseudophakic fellow eyes. Although SCT was numerically greater in PCME eyes, the difference did not reach statistical significance (p = 0.18).
Conclusion: SCT was slightly higher in eyes with PCME compared to contralateral pseudophakic eyes operated within a similar postoperative period; however, the difference was not statistically significant, which may partly be related to the limited sample size. These findings suggest that choroidal thickening observed in PCME may largely reflect postoperative inflammatory changes rather than a disease-specific choroidal mechanism.
Keywords: pseudophakic cystoid macular edema, subfoveal choroidal thickness, enhanced depth imaging optical coherence tomography
Introduction
Cystoid macular edema is one of the most common postoperative complications of cataract surgery and a major cause of suboptimal visual recovery.1–3 On optical coherence tomography (OCT), it is characterized by central macular thickening, intraretinal cystic hyporeflective spaces, and occasionally subfoveal fluid.4 The reported incidence of pseudophakic cystoid macular edema (PCME) varies widely, ranging from 1% to 30%, largely due to differences in diagnostic criteria, imaging modalities, and study populations.5 Several intraoperative and postoperative factors, including vitreous loss, vitreous traction at incision sites, retained lens fragments requiring vitrectomy, iris trauma, posterior capsule rupture, intraocular lens dislocation, early postoperative capsulotomy, and the use of iris-fixated or anterior chamber intraocular lenses, have been associated with an increased risk of PCME.6–8 Enhanced depth imaging optical coherence tomography (EDI-OCT), a recent advancement in ocular imaging, allows more detailed and reliable assessment of the choroid.9 Increasing evidence suggests that the choroid undergoes structural alterations in various retinal and inflammatory conditions.10–12 Moreover, several studies have demonstrated that uncomplicated cataract surgery itself may induce transient changes in subfoveal choroidal thickness (SCT), likely related to postoperative inflammatory and vascular responses.13–17
Only a limited number of studies have specifically investigated SCT in the acute phase of PCME, and their findings remain inconsistent. While some authors have reported choroidal thinning in eyes with PCME, others have demonstrated increased choroidal thickness, suggesting a possible inflammatory component.18,19 Importantly, many previous studies used phakic fellow eyes or non-operated controls, which may not adequately account for surgery-induced choroidal changes and therefore limit the interpretation of SCT alterations in PCME.
Given these methodological limitations and the potential confounding effect of cataract surgery on choroidal thickness, the present study aimed to evaluate SCT in eyes with clinically significant PCME and compare them with contralateral pseudophakic eyes that underwent uncomplicated cataract surgery within a similar postoperative period.
Methods
This retrospective observational study included 25 eyes of 25 patients diagnosed with clinically significant PCME after uneventful phacoemulsification and posterior chamber intraocular lens implantation. The control group consisted of the contralateral pseudophakic eyes of the same patients, which had also undergone uncomplicated cataract surgery within one month of the operated eye but did not develop PCME. This design was specifically adopted to minimize the confounding effects of postoperative choroidal alterations related to cataract surgery. All surgeries were performed using a standardized phacoemulsification technique. All patients received standard postoperative topical antibiotic and corticosteroid therapy following cataract surgery. Patients were excluded if they had a history of glaucoma, diabetic retinopathy, uveitis, retinal vascular diseases, previous ocular surgery other than cataract surgery, axial length greater than 25 mm or less than 21 mm, significant interocular axial length difference (>0.3 mm), or refractive error difference greater than 1.0 diopters. All patients underwent a comprehensive ophthalmologic examination, including best-corrected visual acuity (BCVA), slit-lamp biomicroscopy, intraocular pressure measurement, and dilated fundus examination. PCME was initially suspected based on clinical fundus findings and confirmed by characteristic OCT features, including intraretinal cystic spaces, and supported by fluorescein angiography (FFA). SCT was measured using the Cirrus spectral-domain OCT system (Carl Zeiss Meditec AG, Germany) with EDI-OCT mode. SCT was defined as the vertical distance from the outer border of the retinal pigment epithelium–Bruch’s membrane complex to the inner scleral surface at the subfoveal point, measured using the built-in caliper tool. To reduce the influence of diurnal variation, all OCT scans were obtained within a standardized morning time window (09:00–11:00 AM). All measurements were independently performed by two experienced masked ophthalmologists, and the average of the two measurements was used for analysis. Interobserver reproducibility was evaluated using the intraclass correlation coefficient (ICC), which demonstrated excellent agreement (ICC > 0.90), with interobserver variability remaining within 5 µm.
Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). The normality of data distribution was assessed using the Shapiro–Wilk test. Since the data were normally distributed, paired t-tests were used to compare PCME eyes and contralateral pseudophakic eyes. Descriptive statistics were presented as mean ± standard deviation, median (Q1–Q3), 95% confidence intervals, coefficient of variation (CV, %), and minimum–maximum values. A p-value < 0.05 was considered statistically significant.
Results
The mean age of the patients was 66.13 ± 5.44 years (range, 59–77 years). 14 (56%) were male and 11 (44%) were female. The mean interval between cataract surgery and the diagnosis of PCME was 6.2 ± 1.6 weeks (range, 4–10 weeks) (Table 1). In all patients, the contralateral eye had also undergone uncomplicated phacoemulsification within one month and remained free of PCME during the study period. CMT was significantly higher in eyes with PCME (458.20 ± 92.30 µm) compared with contralateral pseudophakic eyes (235.66 ± 28.43 µm, p < 0.001). The mean SCT was 297.27 ± 24.52 µm in PCME eyes and 289.41 ± 22.16 µm in pseudophakic fellow eyes. Although SCT values were numerically greater in PCME eyes, the difference was not statistically significant (p = 0.18) (Table 2).
 |
Table 1 Demographic Characteristics of Patients with PCME |
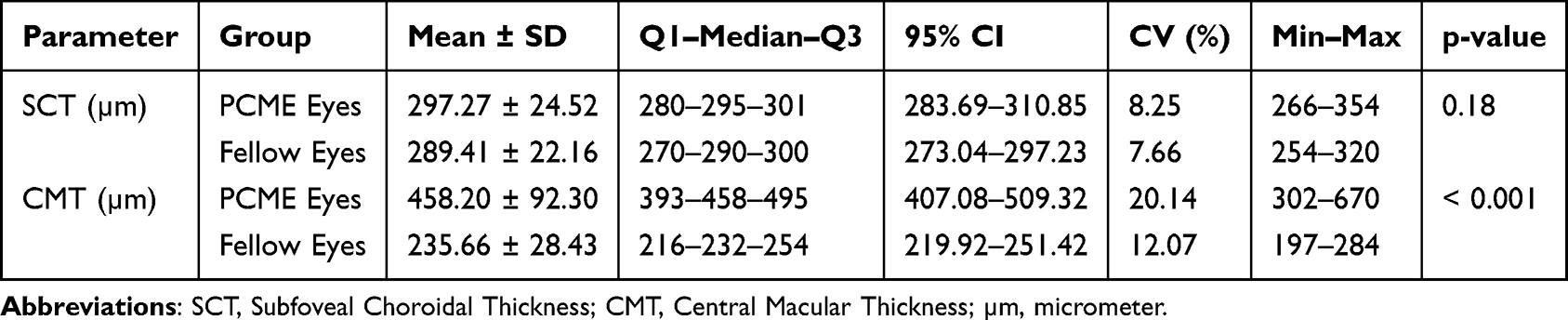 |
Table 2 Comparison of OCT Parameters Between PCME and Fellow Eyes |
Discussion
In our study, no statistically significant difference in SCT was observed between eyes with PCME and their fellow eyes. To our knowledge, only a limited number of studies in the literature have evaluated SCT in PCME. Odrobina et al investigated SCT in patients with clinically significant PCME and reported that the choroid was significantly thinner in affected eyes compared with fellow eyes.18 They suggested that reduced blood flow in the choriocapillaris might limit the delivery of oxygen and nutrients to the outer retina, resulting in hypoxia and contributing to the pathogenesis of macular edema. In contrast, Fleissig et al demonstrated that SCT was increased in the acute phase of PCME and subsequently decreased after the resolution of edema, supporting an inflammatory mechanism.19 In their study, SCT was significantly higher at baseline in PCME eyes compared to fellow eyes but decreased after resolution, although it still remained thicker than in the fellow eyes. Notably, in both of these studies, the fellow eyes were phakic and had not undergone cataract surgery, unlike our study in which the control eyes were contralateral pseudophakic eyes operated within a similar postoperative period. Postoperative inflammation following cataract surgery is recognized as an important risk factor contributing to the development of PCME. Inflammatory mediators are thought to disrupt the blood–retinal barrier, facilitating fluid leakage and subsequent edema formation.20,21 However, inflammation alone may not fully explain the occurrence of macular edema after uneventful cataract surgery, suggesting that additional structural and vascular mechanisms may also be involved. Several studies have demonstrated that cataract surgery itself can induce transient changes in SCT. Falcão et al reported significant increases in both choroidal and macular thickness in the early postoperative period, followed by a gradual return toward baseline values during follow-up.22 Similarly, Ibrahim et al observed postoperative thickening of the subfoveal choroid that regressed to near preoperative levels over time.23 These findings indicate that postoperative SCT thickening is most likely related to transient inflammatory and vascular responses triggered by surgical trauma rather than permanent structural alterations.
The transient increase in SCT after cataract surgery complicates the interpretation of studies evaluating choroidal changes in PCME. In the study by Fleissig et al, the observed increase in SCT during the acute phase of PCME may have been partially attributable to surgery-related effects rather than PCME-specific mechanisms. To attribute choroidal thickening directly to PCME, it would be necessary to demonstrate that the fellow eye, operated within a comparable timeframe but without developing PCME, does not exhibit a similar postoperative increase in SCT. In this context, the use of contralateral pseudophakic eyes as controls in our study provides a more appropriate framework for distinguishing surgery-related choroidal alterations from changes potentially associated with PCME. Moreover, previous reports have shown that choroidal thickening may persist for up to six months after cataract surgery, regardless of the presence of PCME.24,25 In contrast to these findings, Odrobina et al reported that the choroid was thinner in PCME eyes compared with fellow eyes, a finding that contradicts studies demonstrating choroidal thickening after cataract surgery independent of PCME.13–18 The authors proposed that reduced blood flow at the level of the choriocapillaris may impair the delivery of oxygen and nutrients to the outer retina, leading to hypoxia and thereby contributing to macular edema formation. They further speculated that mechanisms similar to those observed in diabetic retinopathy may also play a role in the pathogenesis of PCME. However, as suggested in that study, to assert that a thinner choroid contributes to the development of PCME, preoperative baseline measurements would be necessary. In another study including 95 patients, a significant increase in SCT was observed after cataract surgery, and it was reported that the increase was greater in eyes with PCME. However, since only three patients with PCME were included, this finding may not be statistically meaningful.14 In our study, although SCT was numerically greater in eyes with PCME, the difference did not reach statistical significance. Importantly, the fellow eyes in our cohort were also pseudophakic and had undergone uncomplicated cataract surgery within a similar postoperative period. Therefore, the absence of a significant interocular difference suggests that the observed increase in SCT may reflect a shared postoperative inflammatory response rather than a PCME-specific choroidal alteration. Nevertheless, subtle alterations in the choroidal vasculature may still be present despite the absence of statistically significant differences in SCT measurements. Accordingly, the use of contralateral pseudophakic eyes allows a more methodologically controlled comparison between eyes. These findings also suggest that SCT alone may have limited utility as a diagnostic or prognostic biomarker for PCME.
The intensive use of postoperative anti-inflammatory medications, as well as our relatively small sample size, may have limited the ability to detect subtle interocular differences, increased the possibility of a type II error, and may partially explain discrepancies with previous reports. However, if, as suggested by Odrobina et al, a thinner choroid contributes to the development of PCME through mechanisms similar to those observed in diabetic retinopathy, preoperative baseline SCT measurements would be required to confirm such a hypothesis.
Conclusion and Limitations
In this study, SCT was slightly higher in eyes with clinically significant PCME compared to contralateral pseudophakic eyes; however, the difference did not reach statistical significance. These findings suggest that although retinal thickening remains the hallmark of PCME, the contribution of choroidal structural alterations to its pathogenesis remains uncertain. Several methodological limitations should be considered when interpreting these results. The retrospective design and relatively modest sample size may have limited statistical power and precluded the availability of preoperative baseline SCT measurements. Although the use of contralateral pseudophakic eyes operated within a similar postoperative period reduced surgery-related confounding, the absence of preoperative baseline data limits the ability to determine whether subtle pre-existing interocular differences in SCT were present. Furthermore, SCT was evaluated at a single time point during active edema, and longitudinal postoperative changes were not assessed. Future prospective studies including larger cohorts, standardized measurement protocols, preoperative baseline data, and longitudinal follow-up are warranted to more clearly define the contribution of the choroid to PCME development.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author, Kadriye Demir, upon reasonable request.
Ethics Committee Approval
This study was approved by the Ethics Committee of Sakarya University (Approval No: E-43012747-050.04-475083-283). All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Yilmaz T, Cordero-Coma M, Gallagher MJ. Ketorolac therapy for the prevention of acute pseudophakic cystoid macular edema: a systematic review. Eye. 2012;26(2):2528. doi:10.1038/eye.2011.296
2. Grzybowski A, Sikorski BL, Ascaso FJ, Huerva V. Pseudophakic cystoid macular edema: update 2016. Clin Interv Aging. 2016;11:1221–6. doi:10.2147/CIA.S111761
3. Juthani VV, Clearfield E, Chuck RS. Non-steroidal anti-inflammatory drugs versus corticosteroids for controlling inflammation after uncomplicated cataract surgery. Cochrane Database Syst Rev. 2017;7(7):CD010516. doi:10.1002/14651858.CD010516.pub2
4. Ursell PG, Spalton DJ, Whitcup SM, Nussenblatt RB. Cystoid macular edema after phacoemulsification: relationship to blood-aqueous barrier damage and visual acuity. J Cataract Refract Surg. 1999;25(11):1492–1497. doi:10.1016/S0886-3350(99)00196-0
5. Yonekawa Y, Kim IK. Pseudophakic cystoid macular edema. Curr Opin Ophthalmol. 2012;23(1):26–32. doi:10.1097/ICU.0b013e32834cd5f8
6. Shelsta HN, Jampol LM. Pharmacologic therapy of pseudophakic cystoid macular edema: 2010 update. Retina. 2011;31(1):4–12. doi:10.1097/IAE.0b013e3181fd9740
7. Kim SJ, Belair ML, Bressler NM, et al. A method of reporting macular edema after cataract surgery using optical coherence tomography. Retina. 2008;28(6):870–876. doi:10.1097/IAE.0b013e318169d04e
8. Blair ML, Kim SJ, Thorne JE, et al. Incidence of cystoid macular edema after cataract surgery in patients with and without uveitis using optical coherence tomography. Am J Ophthalmol. 2009;148(1):128–135. doi:10.1016/j.ajo.2009.02.029
9. Spaide RF, Koizumi H, Pozonni MC. Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol. 2008;146(4):496–500. doi:10.1016/j.ajo.2008.05.032
10. Rewbury R, Want A, Varughese R, Chong V. Subfoveal choroidal thickness in patients with diabetic retinopathy and diabetic macular oedema. Eye. 2016;30(12):1568–1572. doi:10.1038/eye.2016.187
11. Lindner M, Bezatis A, Czauderna J, et al. Choroidal thickness in geographic atrophy secondary to age-related macular degeneration. Invest Ophthalmol Vis Sci. 2015;56(2):875–882. doi:10.1167/iovs.14-14933
12. Maruko I, Iida T, Sugano Y, Ojima A, Sekiryu T. Subfoveal choroidal thickness in fellow eyes of patients with central serous chorioretinopathy. Retina. 2011;31(8):1603–1608. doi:10.1097/IAE.0b013e31820f4b39
13. Aslan Bayhan S, Bayhan HA, Muhafiz E, Kırboğa K, Gürdal C. Evaluation of choroidal thickness changes after phacoemulsification surgery. Clin Ophthalmol. 2016;10:961–967. doi:10.2147/OPTH.S94096
14. Pierru A, Carles M, Gastaud P, Baillif S. Measurement of subfoveal choroidal thickness after cataract surgery in enhanced depth imaging optical coherence tomography. Invest Ophthalmol Vis Sci. 2014;55(8):4967–4974. doi:10.1167/iovs.14-14172
15. Ohsugi H, Ikuno Y, Ohara Z, et al. Changes in choroidal thickness after cataract surgery. J Cataract Refract Surg. 2014;40(2):184–191. doi:10.1016/j.jcrs.2013.07.036
16. Shahzad R, Siddiqui MAR, Zafar S, Kausar F, Shahzad MH. Choroidal thickness changes following cataract surgery using swept source optical coherence tomography. Can J Ophthalmol. 2018;53(1):60–64. doi:10.1016/j.jcjo.2017.06.019
17. Celik E, Cakır B, Turkoglu EB, Doğan E, Alagoz G. Effect of cataract surgery on subfoveal choroidal and ganglion cell complex thicknesses measured by enhanced depth imaging optical coherence tomography. Clin Ophthalmol. 2016;10:2171–2177. doi:10.2147/OPTH.S105992
18. Odrobina D, Laudańska-Olszewska I. Choroidal thickness in clinically significant pseudophakic cystoid macular edema. Retina. 2015;35(1):136–140. doi:10.1097/IAE.0000000000000273
19. Fleissig E, Cohen S, Iglicki M, Goldstein M, Zur D. Changes in choroidal thickness in clinically significant pseudophakic cystoid macular edema. Retina. 2018;38(8):1629–1635. doi:10.1097/IAE.0000000000001747
20. Cunha-Vaz JG, Travassos A. Breakdown of the blood-retinal barriers and cystoid macular edema. Surv Ophthalmol. 1984;28(6):485–492. doi:10.1016/0039-6257(84)90230-3
21. Wolf EJ, Braunstein A, Shih C, Braunstein RE. Incidence of visually significant pseudophakic macular edema after uneventful phacoemulsification in patients treated with nepafenac. J Cataract Refract Surg. 2007;33(9):1546–1549. doi:10.1016/j.jcrs.2007.05.018
22. Falcão MS, Gonçalves NM, Freitas-Costa P, Beato JB, Rocha-Sousa A, Carneiro Â. Choroidal and macular thickness changes induced by cataract surgery. Clin Ophthalmol. 2013;8:55–60. doi:10.2147/OPTH.S53989
23. Ibrahim AM, Elgouhary SM, Nassar MK, El Batanony AH. Changes in choroidal thickness after cataract surgery. Semin Ophthalmol. 2018;33(5):664–670. doi:10.1080/08820538.2017.1416410
24. Noda Y, Ogawa A, Toyama T, Ueta T. Long-term increase in subfoveal choroidal thickness after surgery for senile cataracts. Am J Ophthalmol. 2014;158(3):455–9.e1. doi:10.1016/j.ajo.2014.05.016
25. Yılmaz T, Karci AA, Yilmaz İ, Yılmaz A, Yıldırım Y, Sakalar YB. Long-term changes in subfoveal choroidal thickness after cataract surgery. Med Sci Monit. 2016;22:1566–1570. doi:10.12659/msm.898714
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subfoveal Choroidal Thickness After Successful Retinal Detachment Repair with Persistent Subretinal Fluid at the Macula
Mansour AM, Parodi MB, Uwaydat SH, Lima LH, Charbaji S, Casella AM, López-Guajardo L, Belotto S, Wu L, Schwartz SG, Smiddy WE, Hassoun MM, Pérez-Salvador García E, Mansour HA, Elnahry AG, Hamam RN
Clinical Ophthalmology 2025, 19:1847-1854
Published Date: 11 June 2025
The Acute Effects of Caffeine on OCT and OCTA Parameters: A Systematic Review and Meta-Analysis
Veiga DM, Ivanov YA, Júnior AYF, Rebolho MEF, Gerente BGDSM, Amaral DC, Jacometti R, Guedes J, Monteiro ML, Louzada RN
Clinical Ophthalmology 2026, 20:568498
Published Date: 11 April 2026