Back to Journals » Clinical Ophthalmology » Volume 20
Tetracaine Eye Drops as a Preemptive Topical Skin Anesthesia for Botulinum Toxin Type A Injections in Blepharospasm Patients: A Randomized Controlled Trial
Authors Pinitpanich N, Hirunwiwatkul P ![]() , Ongprakobkul C
, Ongprakobkul C ![]() , Tulvatana W
, Tulvatana W ![]()
Received 2 March 2026
Accepted for publication 7 May 2026
Published 15 May 2026 Volume 2026:20 603168
DOI https://doi.org/10.2147/OPTH.S603168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Navinda Pinitpanich,1,* Parima Hirunwiwatkul,1,2,* Chuthamas Ongprakobkul,1,2 Wasee Tulvatana1,2
1Ophthalmology Department, King Chulalongkorn Memorial Hospital, Bangkok, Thailand; 2Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
*These authors contributed equally to this work
Correspondence: Parima Hirunwiwatkul, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand, Email [email protected]
Purpose: To evaluate the efficacy and safety of topical tetracaine eye drops as a preemptive skin anesthetic during botulinum toxin type A injection in blepharospasm patients.
Patients and Methods: A double-blind, split-face randomized controlled trial was conducted in 17 participants diagnosed with benign essential blepharospasm between November 2023 and July 2024. Each patient received randomized treatment on opposite sides of the face: a cotton pad soaked with 5 mL of 0.5% tetracaine ophthalmic solution on one side and normal saline solution on the other, for 30 minutes. The cotton pad temperature, the injection dose, and the techniques were controlled on each side. A single neuro-ophthalmologist performed the injection. Pain scores were immediately rated after the injection, using a numeric rating scale from 0 to 10. Jankovic rating scale and complications were assessed on the day of injection, then 1 month and 3 months after injection.
Results: The numeric rating scale on the side receiving topical 0.5% tetracaine eye drops was significantly lower than the side receiving topical normal saline solution (4.56 ± 2.63 vs 6.71 ± 2.54, p = 0.013). There were no significant differences in the Jankovic rating scale, cotton pad temperature, bleeding at the injection site, and other complications between the two groups.
Conclusion: The application of 0.5% tetracaine ophthalmic solution as a preemptive topical skin anesthesia can decrease pain during botulinum toxin type A injection for blepharospasm patients without affecting the efficacy or producing any significant complications.
Keywords: botulinum toxin, blepharospasm, pain, tetracaine, anesthesia
Introduction
Botulinum toxin type A (BoNT-A) is considered the first line and most effective treatment for blepharospasm.1 More than 95% of patients with blepharospasm experience significant symptom alleviation after BoNT-A injection.2 BoNT-A has also become a popular treatment for various medical and cosmetic purposes.3,4
Typically, the effects of BoNT-A injections last for several months before the gradual return of all muscle activity. The mean duration of the symptom-free period is approximately 3 months after injection.2 Repeated injections are usually necessary to maintain the desired therapeutic effect in blepharospasm. This treatment usually causes pain from the injection with needles, which possibly leads to anxiety and discomfort before and during the procedure. Several local complications, including pain, have been noted with the use of this drug.
Currently, there is no standard guideline for decreasing pain sensation during BoNT-A injections. Several techniques are used as a preemptive anesthesia, ie, to apply before the injection to minimize pain during BoNT-A injections. These modalities include topical anesthetic creams such as topical lidocaine-prilocaine cream,5–7 topical amethocaine,8 and lidocaine-tetracaine cream,9,10 but the usage is limited due to the requirement of the application time of 30 to 60 minutes before the injection. Other methods that can also minimize pain include the application of ice,11,12 alkalinization of the local anesthetic agent with sodium bicarbonate,13–15 use of finer needles,16,17 and vibration.18,19
Most studies have focused on the efficacy of topical lidocaine or tetracaine cream as an anesthetic agent for dermatologic laser procedures and BoNT-A injection, which have proven to be safe and effective in producing local dermal anesthesia. However, applying topical lidocaine-prilocaine cream to the periocular area may cause ocular irritation and skin reactions at the application site, such as redness, swelling, and itching.
The application of tetracaine HCl ophthalmic solution in a specific area causes temporary numbness. The most significant impact occurs 10–20 seconds after administration, and its effect remains for 10–20 minutes. When eye drops are used, around 80% of the medication enters the bloodstream by crossing the highly vascularized mucous membrane in the nasopharynx. The routes of systemic absorption include the conjunctiva, lacrimal system, and aqueous humor, as well as the skin on the cheek and eyelids. The minimal transdermal absorption of topical eye drops through the epidermis also results in a minimal impact on systemic bioavailability.20,21
The primary objective of this study is to evaluate the efficacy of tetracaine eye drops as a preemptive topical skin anesthetic in reducing pain prior to BoNT-A injections. The secondary objective is to assess the safety of tetracaine eye drops as a topical skin anesthetic and its impact on the efficacy of BoNT-A.
Methods
The double-blind, split-face design, randomized control trial (protocol registered in the Thai Clinical Trials Registry, TCTR20230530007) was conducted at the Ophthalmology Department, King Chulalongkorn Memorial Hospital, Bangkok, Thailand. The study was approved by the Faculty of Medicine, Chulalongkorn University’s Institutional Review Board (Certificate of Approval No. 1184/2023) and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants before enrollment, including the subject’s consent to publish the image in Figure 1. This study was carried out from November 2023 to July 2024.
 |
Figure 1 Participants randomly received a U-shaped cotton pad soaked with 5 mL of 0.5% tetracaine hydrochloride ophthalmic solution on one side, while the opposite side was applied with 5 mL of 0.9% sodium chloride as a control. Both applications were covered with plastic wrap and applied to the skin 30 minutes prior to the botulinum toxin type A injection. Published with permission from the participant. |
Participants
We recruited patients with a confirmed diagnosis of benign essential blepharospasm who underwent BoNT-A (OnabotulinumtoxinA: Botox®, Allergan Pharmaceuticals Ireland, Westport, Ireland) treatment in the botulinum toxin clinic, Ophthalmology Department, King Chulalongkorn Memorial Hospital, Bangkok, Thailand. Inclusion criteria were patients aged 18 years or older diagnosed with benign essential blepharospasm in both eyes by experienced neuro-ophthalmologists who had received their last BoNT-A injection more than 3 months prior or had never received a BoNT-A injection. Exclusion criteria were patients with a history of an allergic reaction to BoNT-A or tetracaine HCl eye drops (Alcon Laboratories, Fort Worth, TX, USA), neuromuscular diseases, any active infection in the treatment area, anticoagulant use, bleeding disorders, previous facial cosmetic surgical procedures such as eyebrow lifts and other periorbital surgery, psychological disease, and different blepharospasm severity between both eyes.
After the informed consent process, a neuro-ophthalmologist (P.H.) evaluated clinical characteristics of participants including spasm severity, lagophthalmos, extraocular muscle action, lid position, and ptosis before the experiment.
Study Protocol
Each participant was randomly assigned to receive different interventions on each side of the face. The randomization process was conducted to designate the intervention side allocation (left or right) using blocks of four using a random sequence computer generator by one investigator (N.P). Allocation concealment using sealed opaque envelopes was then performed. The BoNT-A injection was prescribed to each participant as indicated. Before starting the procedure, an investigator cut the 2×2.5-inch cotton pad into a U-shape with a 3.5 cm diameter. A cotton pad soaked with 5 mL of 0.5% tetracaine HCl eye drops was applied to the intervention side of the face, while the control face side received a cotton pad soaked with 5 mL of normal saline solution (NSS). The cotton pads were then covered with a plastic wrap, as shown in Figure 1, for 30 minutes.22 The temperature of the soaked cotton pads was measured before the skin application to ensure similar temperatures on both sides. After the 30-minute skin application, the plastic wrap and cotton pads were removed. Then, an investigator evaluated the complications after application of the tetracaine eye drops as a topical skin anesthesia. A single researcher (C.O.) who was masked to the intervention side allocation evaluated the signs and symptoms of complications such as skin erythema, edema, irritation, blanching, contact urticaria, or allergic contact dermatitis before injection. The onabotulinumtoxinA injection was immediately performed.
All injections were done using insulin syringes with 30-gauge needles and always started with the right side. The injection dose and injection technique completed on both sides of the face were identical. All injections were performed by a single experienced neuro-ophthalmologist (P.H). Outcome measurements were performed on the day of BoNT-A injection and then 1 month (4–6 weeks) and 3 months (12–14 weeks) after injection.
Pain score was assessed immediately after injection using a numeric rating scale (NRS). The NRS was rated from 10 for the most unbearable pain to 0 for no pain and recorded by a trained research assistant who was masked to the treatment allocation. Bleeding at the injection site was evaluated after injection by a single researcher (C.O).
At 1 month after injection, participant follow-up was performed through a hospital’s telemedicine application to evaluate gradings of spasm severity and spasm frequency according to the Jankovic rating scale (JRS). BoNT-A-related complications, including lagophthalmos, extraocular muscle limitation, facial palsy, ptosis, or any other adverse reactions resulting from the injection, were also recorded.
At 3 months after injection, the patients were assessed at the botulinum toxin clinic for the severity and frequency of spasm, complications of BoNT-A injection, and the efficacy of BoNT-A injections. Subjects reported spasm recurrence using diaries given on the day of injection to record the first date of sensing the spasm (spasm recurrence) and the first date of having limited ability to perform daily life activities (spasm symptoms affecting daily life). The duration was then calculated from the date of injection and reported in weeks. Subsequently, the neuro-ophthalmologist provided treatment based on standard guidelines, which included regular BoNT-A injections.
Blinding
All those involved in the study including the subjects, injecting physician (P.H)., and outcome assessors were unaware of the intervention arms throughout the study.
Statistical Analysis
The sample size was calculated using two dependent means (pair-matched) according to a previous study regarding the effect of cold compression as a pain-relieving for BoNT-A injection.23 The mean pain score was 6.5 (Standard deviation (SD) = 1.5) in the control group. The pain score in the cold compression group was significantly lower than that of the control group (p < 0.001). The minimal clinically important difference (MCID) was determined as a 20% reduction in pain from the mean score of 6.5, resulting in a ∆ (Delta) value of 1.3.
Fourteen subjects (14 sides of injected face per group) were required to achieve a power of 90% and a 5% significance to detect the mean difference. A total of 17 participants were included, allowing for a 20% dropout rate.
We used the IBM SPSS Statistics for Macintosh, Version 29.0.2.0, Armonk, NY: IBM Corp for all analyses. Baseline characteristics were described using counts (percentage), median (interquartile range), and mean with SD. The normality of data was determined by histogram plots and Shapiro–Wilk tests. A paired t-test was used to compare the mean difference of the NRS pain score between the experimental and control sides. The Wilcoxon signed-rank test was used to compare the medians of spasm severity and frequency, complications of BoNT-A injection, and efficacy of BoNT-A injections between 2-sided sample. All reported p-values were 2-sided, with a p-value less than 0.05 considered statistically significant.
Results
Seventeen patients with benign essential blepharospasm were enrolled between November 2023 and July 2024. There were no dropouts or exclusions after randomization (Figure 2).
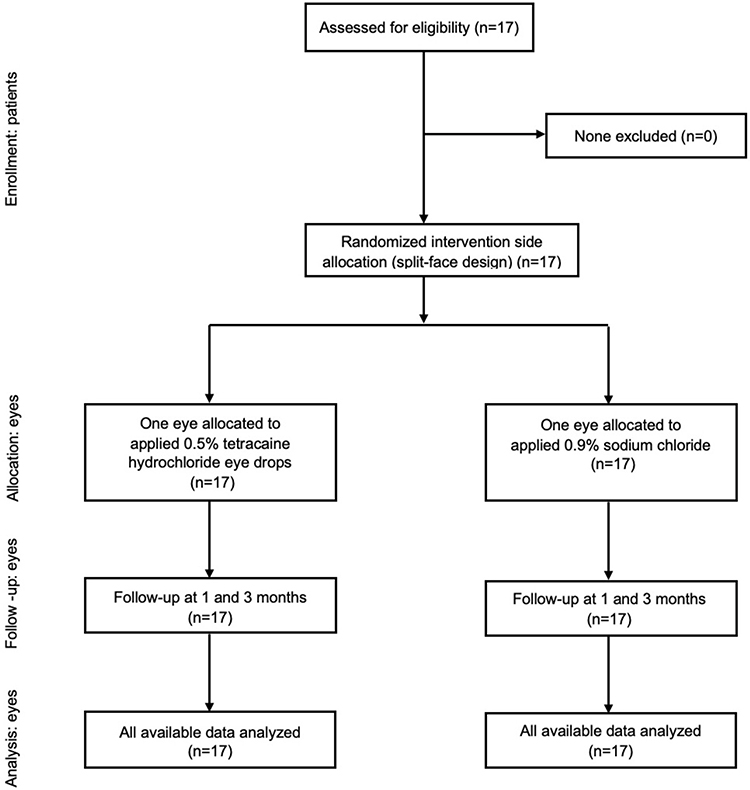 |
Figure 2 CONSORT diagram shows the study flowchart. |
Their ages ranged from 33 to 68 years (mean, 58 ± 10.82 years). Seven were male (41.17%), and 10 (58.82%) were female. Nine patients had an underlying disease of hypertension, diabetes mellitus, or dyslipidemia. The median Jankovic spasm severity and spasm frequency were 4 [IQR 3,4]. Baseline characteristics and demographic data are shown in Table 1.
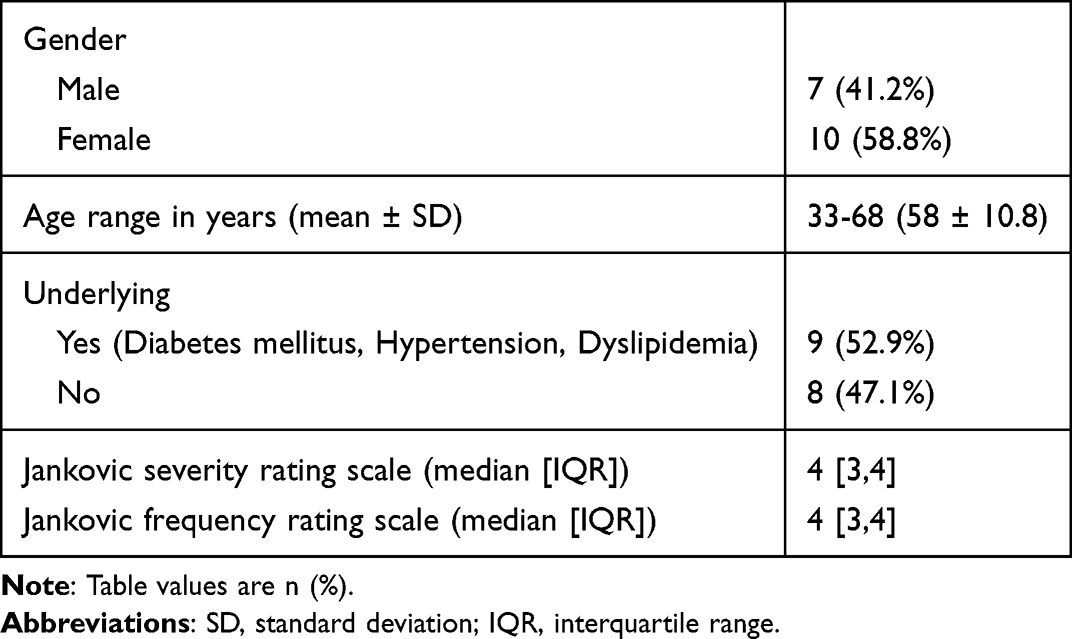 |
Table 1 Baseline Characteristics and Demographic Data (N = 17) |
The mean ± SD of the immediate post-injection NRS pain score was 4.56 ± 2.63 in the experimental group and 6.71 ± 2.54 in the control group. The mean pain score of the experimental group was significantly lower than the control group (mean difference 2.15; 95% confidence interval (95% CI) 0.522 to 3.772, p-value = 0.013). Eleven patients from 17 patients (64.7%) reported 20% reduction or more in pain scores. There was no difference in mean ± SD temperature in degrees Celsius between the cotton pads in the tetracaine HCl eye drop group and NSS group (22.32 ± 0.72 versus 22.21 ± 0.70; p-value = 0.319).
The secondary outcome showed no significant difference in bleeding at the injection site between the experimental group and the control group. Bleeding occurred in two participants of each group, indicating an equivalent incidence rate. The JRS of spasm severity and frequency was not significantly different between the two groups at any observed time points (p-value = 1.000).
Spasm recurrence was observed at a median of 7.5 [IQR 4.2, 9.0] weeks after injection on the experimental side and 8.0 [IQR 4.2, 9.0] weeks on the control side (p-value = 1.000). Spasm symptoms affecting daily life were reported at a median of 10 [IQR 10, 11.0] weeks after injection in both groups (p-value = 1.000). A summary of the results for both groups is presented in Table 2.
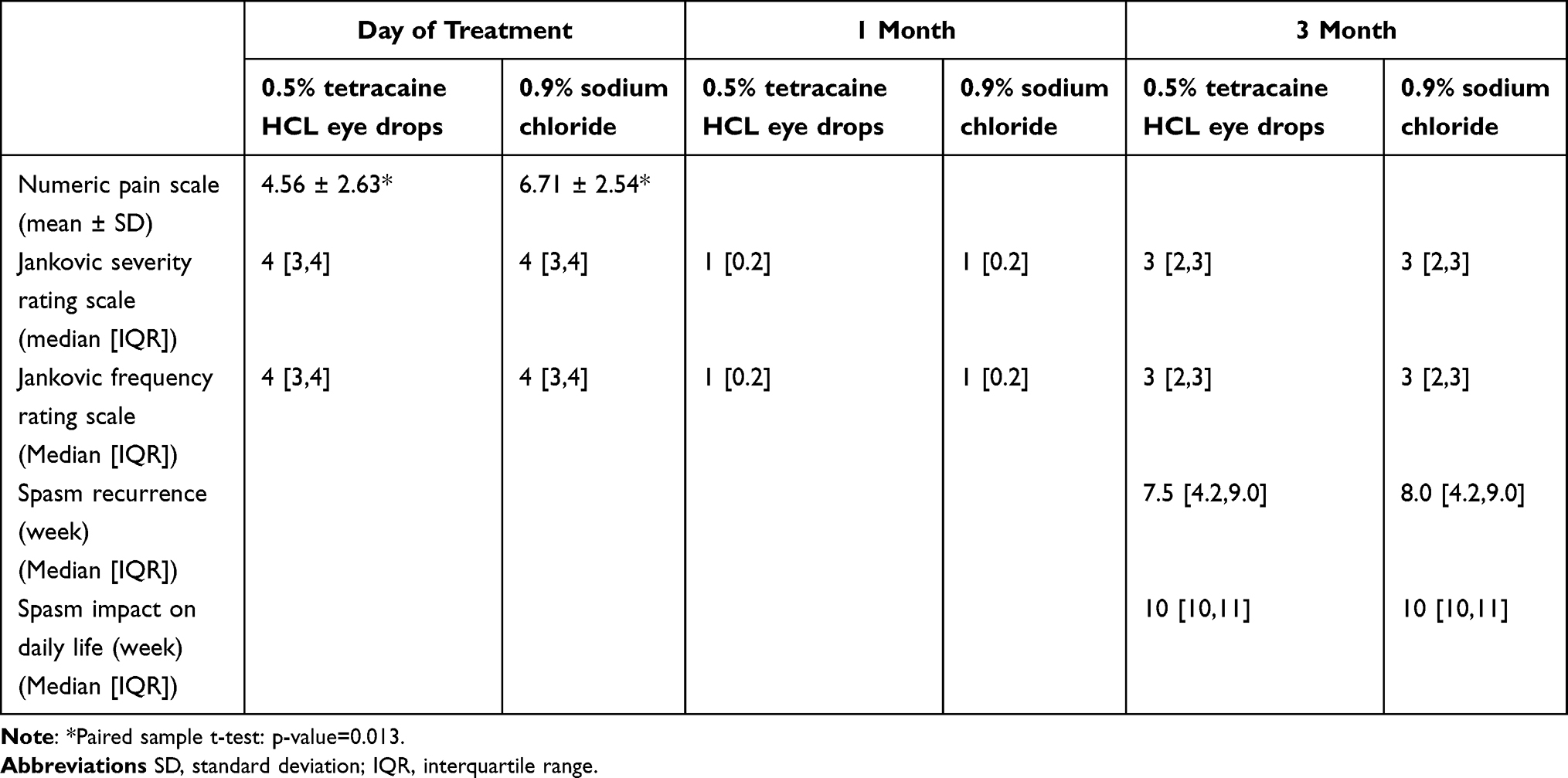 |
Table 2 Outcome Variables of Topical 0.5% Tetracaine Hydrochloride Eye Drops versus Topical 0.9% Sodium Chloride (Day of Treatment, 1 Month, and 3 Month) |
No other complications were observed in both groups on the day of treatment, 1 month, and 3 months.
Discussion
The study findings revealed that the application of 0.5% tetracaine ophthalmic solution as a topical skin anesthesia prior to BoNT-A injection could significantly reduce pain compared to NSS without affecting BoNT-A efficacy or causing any serious complications.
Although there are several methods for minimizing pain during BoNT-A injections, such as topical lidocaine-prilocaine cream, vibration, and cold compression, a major side effect limiting their utilization is ocular irritation. To address this need, we investigated the use of 0.5% tetracaine HCl ophthalmic solution as a topical skin anesthetic.
The topical lidocaine-prilocaine cream can cause significant ocular side effects due to its alkaline pH and potential for chemical irritation. A previous case report demonstrated corneal abrasions and conjunctivitis resulting from accidental exposure to topical lidocaine-prilocaine cream during procedures involving the periocular region.24 Our results found no evidence of any side effects related to the application of 0.5% tetracaine HCl ophthalmic solution as a topical skin anesthetic, including no ocular irritation or skin adverse effects, suggesting the safety of this application.
Bleeding at the injection site following BoNT-A injection was comparable in both groups. This result differed from previous studies, which investigated the impact of cold compression on bleeding at the injection site and found a statistically significant difference in post-injection bleeding between the groups that applied a cold compress before the injection and the group with no intervention. This approach is considered safe for future use.23,25
Other complications after injection, such as lagophthalmos, extraocular muscle action, drooping corners of the mouth, ptosis, or any other adverse reactions resulting from the injection, did not occur in any groups. The findings could be explained by the fact that injections between the two sides were the same unit, the same injection technique, and a single injecting physician. It may imply that the tetracaine HCI anesthetic does not increase or decrease the efficacy of BoNT-A.
Our study investigated the efficacy of BoNT-A by assessing the time to recurrence of spasm and time to spasm affecting daily life, in contrast to previous studies that primarily evaluated efficacy based on the mean duration of effect.26,27 Our findings indicated no significant differences in the efficacy of BoNT-A, contrary to a previous study, which found that topical anesthetics could decrease the efficacy of BoNT-A, possibly due to their nerve-inactivation effect interfering with the nerve stimulation required for BoNT-A to be effective.28
This study comes with potential strengths, mostly stemming from the study design. A double-blind, randomized controlled trial, comparing the pain score, bleeding, and other complications between both sides of the face, was performed at the same time in each participant to avoid other possible confounders. In our study design, we minimized potential error related to the accuracy of participant recall by informing the participants before treatment that they were assigned to compare the outcome measures between both injection sides and by evaluating immediately post-treatment. The study design also reduced other possible biases by using sealed envelopes for allocation concealment and assessing all participants with all masked investigators. Moreover, the study findings enhance clinical applicability because of the widespread availability and routine use of topical anesthetic agents as standard medications in ophthalmologic practice.
The limitations of this study, including a small sample size, resulted in increased variability, which affected the wide range of confidence intervals and standard deviation. Although statistical significance was achieved, the 95% confidence interval for the mean difference in NRS between the two arms was rather wide, potentially limiting the ability to demonstrate the clinical significance of the NRS outcome. A larger sample size in future studies would better establish the clinical significance of this endpoint by increasing the precision of the comparison.
The first facial side receiving the injection was not randomized. Due to the proximity of the right facial side to the right-hand-dominant neuro-ophthalmologist injector, we performed all injections on the right side first to standardize the technique and minimize sequence effect bias. However, this may limit the generalizability to left-hand-dominant injectors or other injection sequences.
The NRS, used as the primary outcome measure, is practical for routine assessments but has limitations due to its discrete nature and lower sensitivity compared to the visual analog scale (VAS). The VAS would be preferred in further studies because it provides greater detail and more accurate results. Additionally, it may be useful to assess patient preferences regarding the use of 0.5% tetracaine HCl eye drops as a topical anesthetic for their next BoNT-A injection.
In our study, at 1-month post-injection, BoNT-A efficacy was assessed using the JRS to evaluate spasm severity and frequency via telemedicine. However, this approach may compromise the grading accuracy, as the condition is episodic in nature and subtle muscle spasms may not be reliably detected through video-based assessment.
In conclusion, the application of 0.5% tetracaine HCl eye drops as a topical anesthesia before BoNT-A injections significantly reduced pain without affecting the efficacy of the BoNT-A or causing any complications. The findings of this study support this option to decrease pain in patients with blepharospasm who require treatment with BoNT-A injections.
Acknowledgments
We are grateful to Mrs. Nutmathika Purananunak and Ms. Ruttanabhorn Chonramak, research assistants, for their valuable assistance in collecting Numeric Rating Scale data and supporting the research data collection. The original datasets generated over the course of this research are available upon request.
Funding
This study was supported by the Ratchadapiseksompotch Research Fund, Faculty of Medicine, Chulalongkorn University (Grant number GA67/012). The funder was not involved in the study design, data collection, analysis, interpretation, or manuscript preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Osako M, Keltner JL. Botulinum A toxin (Oculinum®) in ophthalmology. Surv Ophthalmol. 1991;36(1):28–8. doi:10.1016/0039-6257(91)90207-V
2. Dutton JJ. Botulinum-A toxin in the treatment of craniocervical muscle spasms: short- and long-term, local and systemic effects. Surv Ophthalmol. 1996;41(1):51–65. doi:10.1016/S0039-6257(97)81995-9
3. Mandeville JTH, Rubin PAD. Injectable agents for facial rejuvenation: botulinum toxin and dermal filling agents. Int Ophthalmol Clin. 2004;44(1):189–212. doi:10.1097/00004397-200404410-00018
4. Sarrabayrouse MAM. Indications and limitations for the use of botulinum toxin for the treatment of facial wrinkles. Aesthetic Plast Surg. 2002;26(4):233–238. doi:10.1007/s00266-002-2030-x
5. Eppley BL. Easing Botox administration with EMLA cream. Aesthet Surg J. 2004;24(1):79–81. doi:10.1016/j.asj.2003.10.002
6. Kashkouli MB, Salimi S, Bakhtiari P, Parvaresh MM, Sanjari MS, Naseripour M. EMLA cream application without occlusive dressing before upper facial botulinum toxin injection: a randomized, double-blind, placebo-controlled trial. Ann Plast Surg. 2008;60(4):353–356. doi:10.1097/SAP.0b013e31812f6e0f
7. Söylev MF, Koçak N, Kuvaki B, Özkan SB, Kir E. Anesthesia with EMLA® cream for botulinum A toxin injection into eyelids. Ophthalmologica. 2002;216(5):355–358. doi:10.1159/000066186
8. Browne J, Raza A, Awad I, Tan B, McAdoo J, Shorten G. The effects of EMLA and a topical formulation of 4%amethocaine (Ametop) on pain associated with retrobulbar injection. Anaesthesia. 1999;54(6):596–598. doi:10.1046/j.1365-2044.1999.00842.x
9. Alster TS, Lupton JR. Evaluation of a novel topical anesthetic agent for cutaneous laser resurfacing: a randomized comparison study. Dermatol Surg. 2002;28(11):1004–1006. doi:10.1046/j.1524-4725.2002.02100.x
10. Kim WO, Song BM, Kil HK. Efficacy and safety of a lidocaine/tetracaine medicated patch or peel for dermatologic procedures: a meta-analysis. Korean J Anesthesiol. 2012;62(5):435–440. doi:10.4097/kjae.2012.62.5.435
11. Linder JS, Edmonson BC, Laquis SJ, Drewry RD Jr, Fleming JC. Skin cooling before periocular botulinum toxin A injection. Ophthalmic Plast Reconstr Surg. 2002;18(6):441–442. doi:10.1097/00002341-200211000-00010
12. Sarifakioglu N, Sarifakioglu E. Evaluating the effects of ice application on the pain felt during botulinum toxin type-A injections: a prospective, randomized, single-blind controlled trial. Ann Plast Surg. 2004;53(6):543–546. doi:10.1097/01.sap.0000139563.51598.75
13. Alghonaim Y, Hijazi LO, Alraee SA, Alqubaisy Y. Injection site pain, onset and duration of action of botulinum toxin reconstituted in normal saline with and without sodium bicarbonate: a prospective, single center, randomized, double-blind interventional study. Plastic Surgery. 2022;30(3):227–232. doi:10.1177/22925503211011971
14. Davies RJ. Buffering the pain of local anaesthetics: a systematic review. Emerge Med. 2003;15(1):81–88. doi:10.1046/j.1442-2026.2003.00413.x
15. Dressler D, Adib Saberi F, Bigalke H. Botulinum toxin therapy: reduction of injection site pain by pH normalisation. J Neural Transm. 2016;123(5):527–531. doi:10.1007/s00702-016-1522-9
16. Iwanaga M, Kamoi K. Patient perceptions of injection pain and anxiety: a comparison of NovoFine 32-gauge tip 6mm and Micro Fine Plus 31-gauge 5mm needles. Diabetes Technol Ther. 2009;11(2):81–86. doi:10.1089/dia.2008.0027
17. Yomtoob DE, Dewan MA, Lee MS, Harrison AR. Comparison of pain scores with 30-gauge and 32-gauge needles for periocular botulinum toxin type A injections. Ophthalmic Plast Reconstr Surg. 2009;25(5):376–377. doi:10.1097/IOP.0b013e3181b1e526
18. Kuwahara H, Ogawa R. Using a vibration device to ease pain during facial needling and injection. Eplasty. 2016;16:e9.
19. Mally P, Czyz CN, Chan NJ, Wulc AE. Vibration anesthesia for the reduction of pain with facial dermal filler injections. Aesthetic Plast Surg. 2014;38(2):413–418. doi:10.1007/s00266-013-0264-4
20. Farkouh A, Frigo P, Czejka M. Systemic side effects of eye drops: a pharmacokinetic perspective. Clin Ophthalmol. 2016;10:2433–2441. doi:10.2147/OPTH.S118409
21. Vaajanen A, Vapaatalo H. A single drop in the eye – effects on the whole body? Open Ophthalmol J. 2017;11(1):305–314. doi:10.2174/1874364101711010305
22. Doshi SN, Friedman PM, Marquez DK, Goldberg LH. Thirty-minute application of the S-Caine peel prior to nonablative laser treatment. Dermatol Surg. 2003;29(10):1008–1011. doi:10.1046/j.1524-4725.2003.29292.x
23. Pituksung A, Chirapapaisan N, Konlakij D, Suratako R, Kumteam K. The effect of cold compression as the pain relieving for botulinum toxin A injection for the blepharospasm patients. Nurs Sci J Thai. 2015;33(2):61–67.
24. Eaglstein FN. Chemical injury to the eye from EMLA cream during erbium laser resurfacing. Dermatologic Surg. 1999;25(7):590–591. doi:10.1046/j.1524-4725.1999.98289.x
25. Saeliw P, Preechawai P, Aui-aree N. Evaluating the effects of ice application on patient comfort before and after botulinum toxin type A injections. J Med Assoc Thai. 2010;93(10):1200–1204.
26. Ababneh OH, Cetinkaya A, Kulwin DR. Long-term efficacy and safety of botulinum toxin A injections to treat blepharospasm and hemifacial spasm. Clin Exp Ophthalmol. 2014;42(3):254–261. doi:10.1111/ceo.12165
27. Gill HS, Kraft SP. Long-term efficacy of botulinum A toxin for blepharospasm and hemifacial spasm. Can J Neurol Sci. 2010;37(5):631–636. doi:10.1017/S0317167100010817
28. Sami MS, Soparkar CNS, Patrinely JR, Hollier LM, Hollier LH. Efficacy of botulinum toxin type A after topical anesthesia. Ophthalmic Plast Reconstr Surg. 2006;22(6):448–452. doi:10.1097/01.iop.0000248989.33572.3c
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Spinal Anaesthesia as an Adjunct to General Anaesthesia for Laparoscopic Abdominoperineal Rectal Amputation
Antunes M, Baumgärtel A, Gjessing PF, Ytrebø LM
Journal of Pain Research 2023, 16:1855-1865
Published Date: 31 May 2023
The Effect of Caudal Ropivacaine and Morphine on Postoperative Analgesia in Total Laparoscopic Hysterectomy: A Prospective, Double-Blind, Randomized Controlled Trial
Qin Y, She H, Peng W, Zhou X, Wang Y, Jiang P, Wu J
Journal of Pain Research 2023, 16:3379-3390
Published Date: 4 October 2023
Dexmedetomidine and Dexamethasone as Adjuvants to the Local Anesthetic Mixture in Rhomboid Intercostal and Sub-Serratus Block for Video-Assisted Thoracoscopic Surgery: A Randomized, Double-Blind, Controlled Trial
Liu QF, Shi CN, Tong JH, Li KP, Yang JJ, Ji MH, Liu QR
Drug Design, Development and Therapy 2024, 18:4485-4496
Published Date: 7 October 2024