Back to Journals » Journal of Pain Research » Volume 16
The Effect of Caudal Ropivacaine and Morphine on Postoperative Analgesia in Total Laparoscopic Hysterectomy: A Prospective, Double-Blind, Randomized Controlled Trial
Authors Qin Y, She H, Peng W, Zhou X ![]() , Wang Y, Jiang P
, Wang Y, Jiang P ![]() , Wu J
, Wu J ![]()
Received 20 June 2023
Accepted for publication 26 September 2023
Published 4 October 2023 Volume 2023:16 Pages 3379—3390
DOI https://doi.org/10.2147/JPR.S426820
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ellen Soffin
Yifan Qin, Huiyu She, Wenrui Peng, Xiaofeng Zhou, Yiting Wang, Peng Jiang, Jin Wu
Department of Anesthesiology, Affiliated Hospital of Jiangsu University, Zhenjiang, People’s Republic of China
Correspondence: Jin Wu, Department of Anesthesiology, Affiliated Hospital of Jiangsu University, 438 Jie Fang Road, Zhenjiang, Jiangsu, 212001, People’s Republic of China, Email [email protected]
Purpose: Multiple regional nerve blocks proved no additional benefit in total laparoscopic hysterectomy in multimodal analgesia, as postoperative pain may mainly originate from the vaginal cuff. Theoretically, caudal block can relieve pain from the vaginal cuff by a sacral spinal nerve block. We aimed to verify whether a caudal block with ropivacaine and morphine can achieve an analgesic effect without additional adverse effects after a total laparoscopic hysterectomy.
Patients and Methods: Forty-eight patients undergoing total laparoscopic hysterectomy were randomly allocated to receive preoperative caudal block with 20 mL of mixture including 0.25% ropivacaine and 2 mg morphine (caudal block group) or sham block (sham group). The primary outcome was the postoperative 24 h cumulative sufentanil consumption.
Results: Median (IQR) sufentanil consumption in the first 24 postoperative hours of the caudal block group and the sham group was 0.00 (0.00 to 0.05) μg/kg vs 0.13 (0.04 to 0.21) μg/kg, respectively, p < 0.001. The majority of patients felt that visceral pain was more intense than incisional pain at 1, 6, 12, and 24 h post-surgery in the sham group (95.8% at 1 h, 95.8% at 6 h, 95.8% at 12 h, and 75% at 24 h post-surgery). Compared to the sham group, the caudal block reduced visceral pain scores at rest and during movement at 1 h (p < 0.001), 6 h (p < 0.001), 12 h (p < 0.001), and 24 h (p < 0.001) post-surgery. Intraoperative remifentanil consumption was significantly lower in the caudal block group than in the sham group (p = 0.004). There were no significant differences in other secondary outcomes between the two groups.
Conclusion: A caudal block with ropivacaine and morphine could provide a satisfactory analgesic effect for 24 h postoperatively without additional adverse effects after total laparoscopic hysterectomy.
Keywords: anesthesia, caudal, visceral pain, hysterectomy, pain, postoperative, postoperative nausea and vomiting, gynecologic surgical procedures
Introduction
Hysterectomy is one of the most frequently performed surgeries in females, second only to caesarean sections.1 Minimally invasive routes have been increasingly used worldwide in recent years.2–6 Compared with vaginal hysterectomy, total laparoscopic hysterectomy (TLH) has less postoperative pain and surgical advantages in cases of a large uterus, severe endometriosis or a history of pelvic inflammatory disease.7,8 However, most patients experience moderate to severe pain after surgery, especially in the early postoperative period.9–11
Recently, regional blocks have been widely used for TLH. However, a systematic review showed no clinically significant benefit in adding a transversus abdominis plane block, intraperitoneal instillation, or port-site infiltration to the multimodal analgesic regimen.12 Postoperative abdominal pain usually consists of incisional and visceral pain. Visceral pain after TLH is more intense than incisional pain.11 The visceral pain is primarily transmitted via the thoracic sympathetic trunk and sacral parasympathetic afferent nerves. Transmuscular quadratus lumborum block (TQLB), the drugs used to spread into the thoracic paravertebral space, can potentially relieve incisional and visceral pain and theoretically provide satisfactory pain relief after TLH. However, the latest clinical trial did not demonstrate an analgesic effect of TQLB after TLH.13 The authors proposed that the chief source of postoperative pain might be the vaginal cuff, as this pain is transmitted via the pelvic splanchnic nerves to S2 to S4 and the TQLB could not cover it.13,14
Although epidural block provides excellent analgesic effects in patients undergoing TLH, it is rarely performed because its complications (eg. intraoperative hypotension and impeding early mobilization) do not favor enhanced recovery after surgery.12 Caudal block is effective for the pain relief of vaginal cuff by sacral spinal nerve block and beneficial for postoperative recovery owing to the lack of motor and sympathetic blocks.15 As we known, caudal block is a commonly performed procedure for perioperative analgesia in the pediatric population but less commonly in adults, with 25 to 32% failure rates.16 As a result of the development of ultrasound techniques, the success rate of ultrasound-guided caudal blocks in adults has reached 96.9 to 100%.16 Moreover, compared with traditional epidural block, complications like dural puncture headache, transient neurologic symptoms, local anesthetic systemic toxicity, and epidural hematomas associated with a caudal block are uncommon.15
Ropivacaine is a long-acting amide local anesthetic with less motor blockade. However, a single-shot caudal block with ropivacaine might not provide a sufficient duration of analgesia.17 Adding adjunct is a commonly used method to prolong the duration of analgesia. Among the various adjuncts, opioids are the best established adjuncts for their high safety and good compatibility with local anesthetics.18
Our hypothesis and the primary purpose of this study were to evaluate that a caudal block with ropivacaine and morphine would reduce postoperative pain without additional adverse effects after TLH. To test this hypothesis, we designed a double-blind, randomized, controlled trial to compare postoperative pain in 48 patients undergoing TLH following general anesthesia with a caudal block or sham block. Block-related and opioid-related adverse effects were also evaluated.
Materials and Methods
Participants
The Scientific Research Ethics Committee of the Affiliated Hospital of Jiangsu University, China, approved this single-center, prospective, randomized controlled study (KY2022H1014-4). This study was registered in the Chinese Clinical Trial Registry and the trial registration number was ChiCTR2200065319. Informed consent was obtained from all patients in the study. Women aged 35 to 65 years, ASA physical status Ι-ΙΙ, BMI 18 to 26 kg/m2, scheduled for TLH from 1 November 2022 to 28 February 2023 were included. Exclusion criteria included contraindications for caudal block, complicated by neuromuscular disease or sensory disturbance, receiving treatment for chronic pain, or allergy to local anesthetics.
Randomization and Blinding
Participants were randomly assigned to receive a caudal block (caudal block group) or sham block (sham group) in a 1:1 ratio using computer-generated block randomization with a block size of 6. Assignment codes were kept in signed, opaque, and sealed envelopes and blinded to all patients and investigators, except for the doctor performing the block. The same skilled anesthesiologist performed the caudal block or the sham block and another anesthesiologist administered standard general anesthesia for all patients. A single investigator followed up with all patients for seven days.
Preoperative Education
The investigator responsible for follow-up educated the patients about how to report pain intensity using a Numeric Rating Scale (NRS) and the characteristics of incisional and visceral pain. For example, no pain, mild pain, moderate pain, and severe pain were defined as NRS scores of 0, 1–3, 4–6, and 7–10, respectively. Incisional pain was defined as relatively fixed abdominal pain from trocar site. Visceral pain was defined as the intra-abdominal pain whose location could not be unambiguously determined.19 Patients were also educated on how to use the patient-controlled intravenous analgesia (PCIA) pump, common adverse drug reactions, and coping with adverse drug reactions.
Presurgical Procedure
All patients were first delivered to the pre-anesthesia room and monitored for routine electrocardiography, pulse oxygen saturation, and noninvasive blood pressure measurements. Before the block, all participants received 0.02 mg/kg of midazolam and parecoxib sodium (40 mg).
In the caudal block group, a single-shot caudal block was then performed by an experienced anesthesiologist using an S8 ultrasound system (LOGIQ, GE, Boston, MA, USA) with the patients in the prone position. The long axis of the 10-MHz linear probe was perpendicular to the sacrum, and the probe was moved from the caudal-to-cranial direction to locate the cornu of the sacrum. The puncture points were marked at the midpoint between the two sacral cornua. The probe was then rotated 90° to show the sagittal ultrasound image of the sacral canal. After routine disinfection and towel spreading, the puncture point was infiltrated with local anesthetic (1% lidocaine). Subsequently, the 22-gauge needle was advanced from the caudal to the cranial direction via an in-plane technique until the needle tip was positioned in the sacral canal. Then, a single dose of 20 mL 0.25% ropivacaine with 2 mg morphine was injected into the sacral canal after confirming a negative aspiration. Floating of the sacrococcygeal ligament indicated a successful puncture.
In the sham group, the same anesthesiologist performed the sham block with the patients in the prone position. The sham block was defined as a sequence of operations including ultrasound-guided localization, disinfection, towel spreading, and local subcutaneous infiltration anesthesia at the midpoint between the two sacral cornua.
Intraoperative Management
After transferring the patients to the operating room, standard monitoring, including noninvasive blood pressure, heart rate, electrocardiogram, pulse oxygen saturation, and bispectral index, was performed. For the caudal block group, all patients were induced into general anesthesia with dexamethasone 10 mg, sufentanil 0.3 μg/kg, propofol 2.0 mg/kg, and rocuronium 0.9 mg/kg. Tracheal intubation was completed using a visual laryngoscope, and mechanical ventilation was initiated. General anesthesia was maintained with propofol at 6–8 mg/kg/h and remifentanil 0.02–0.2 μg/kg/min. The infusion speed of propofol and remifentanil was adjusted to maintain the bispectral index between 40 and 60, a mean arterial pressure (MAP) between −20% and +10%, and a heart rate between ± 20% of baseline. If the patient’s blood pressure was outside the target range and there was no response to an adjusted dose of remifentanil for 5 min, an intravenous injection of urapidil, ephedrine, or phenylephrine was chosen according to the change in the MAP value. Lactated Ringer’s solution or compound electrolyte solution was infused at a rate of 6–8 mL/kg/h during surgical procedures. Hydroxyethyl starch compensated blood loss and, if necessary, suspended red blood cell transfusion to maintain hemoglobin levels above 8 g/dl. Ondansetron (4 mg) was intravenously administered before surgery.
TLH
After tracheal intubation, the patients were placed in the dorsal lithotomy position. A uterine manipulator was placed in the vagina to assist with mobilization and surgical exposure. A 4-trocar technique was performed in TLH with one 10 mm trocar inserted below the umbilicus and three 5 mm trocars separately placed through the lower abdominal wall. The CO2 pneumoperitoneum was established with a gas pressure of 12 to 14 mmHg and a flow rate of 2–3 L/min. The remaining surgical procedures were performed in the following order: First, the round ligament, proximal portions of the fallopian tube, and utero-ovarian ligament were cut sequentially using a LigaSure electrotome. Second, the vesicouterine peritoneal fold was opened using an ultrasound knife, and the bladder was pushed downward to expose the cervicovaginal junction after a combination of sharp and blunt dissection. Third, the broad ligament, uterine vessels, cardinal ligament, and uterosacral ligament were coagulated and cut sequentially using a LigaSure. Finally, a colpotomy was performed circumferentially using an ultrasound knife around the cervix. After delivering the uterus through the vagina, the vaginal cuff was closed using laparoscopic suturing and continuous 1-Vicryl sutures.
Postoperative Management
The PCIA pump was initiated at the end of the surgery. The patient was then transferred to the post-anesthesia care unit (PACU) for awakening and extubation. The wireless PCIA pumps were set up with sufentanil 1 μg/kg, ondansetron 8 mg, and dexamethasone 10 mg with a bolus of 3 mL, lockout time of 15 min, and no background infusion doses. In the PACU, If the patient’s NRS pain score was ≥4 and there was no pain relief for 5 min after a bolus, 5 μg of sufentanil was given. In the ward, 40 mg of parecoxib sodium was intravenously administered as a rescue analgesic if the pain score remained ≥4 after two effective bolus injections.
Outcomes
The primary outcome was the postoperative 24 h cumulative sufentanil consumption. The secondary outcomes were sufentanil consumption during the four different postoperative periods, namely, 0–6 h, 6–12 h, 12–18 h, and 18–24 h, incisional and visceral pain scores at 1, 6, 12, and 24 h after surgery, intraoperative remifentanil consumption, intraoperative hemodynamics (heart rate and MAP), the number of patients needing rescue analgesics, use of vasoactive agents, lower limb muscle strength at 1 and 6 h after surgery, postoperative nausea and vomiting (PONV), pruritus, respiratory depression, the timing of first flatus, and length of hospital stay.
Assessment of Outcomes
The doses of postoperative sufentanil were collected using the computer monitoring station of the wireless PCIA pump. The pain scores at rest and during movement (turning over) were evaluated using the NRS. Intraoperative remifentanil consumption, hemodynamics at different time points (T0, after entering the pre-anesthesia room; T1, before induction; T2, before tracheal intubation; T3, after tracheal intubation; T4, the start of pneumoperitoneum; T5, 5 min after pneumoperitoneum; T6, 15 min after pneumoperitoneum; T7, 30 min after pneumoperitoneum; T8, at the end of surgery), and the use of vasoactive agents were recorded by an anesthesiologist administering general anesthesia. Lower limb muscle strength was evaluated using the Bromage scale. Postoperative nausea was classified as none (0), mild (1–3), moderate (4–7), or severe (8–10). Vomiting was assessed by time (0, 1–2, 3–5, >5 times). The respiratory depression was defined as: hypoventilation (respiratory rate < 8 breaths/min for ≥3 minutes); pain-sedation mismatch (NRS >5 with Richmond Agitation Sedation Scale ≤ 3); apnea (respiratory pauses ≥ 10s); hypoxemia (capillary oxygen saturation <90% for >10 s without oxygen).20,21 All indicators associated with evaluating respiratory depression were monitored for 12 h post-surgery by ward nurses, who reported the results the next day to the investigator responsible for collecting the follow-up information.
Sample Size Estimation
We performed a pilot study to estimate the sample size. The Mean (SD) cumulative consumption of sufentanil in the postoperative 24 h was 0.12 (0.067) μg/kg for patients undergoing TLH without caudal block. We hypothesized that a caudal block could reduce postoperative 24 h cumulative sufentanil consumption by 50%. Type I error (α) was set at 0.05 and type II error (β) at 0.2. We observed differences between the two groups when the sample size was 42 (21 per group) using PASS software (v.15.0.5, NCSS, LLC; Kaysville, Utah, USA). We calculated a sample size of 24 participants per group, accounting for a dropout rate of 10%.
Statistical Analysis
All statistical analyses were performed using SPSS (version 26.0; IBM Corp., Armonk, NY, USA). For the demographics and baseline characteristics, all continuous data were tested for normality using the Shapiro–Wilk test. Normally distributed continuous data were assessed using the Student’s t-test. Otherwise, the Mann–Whitney U-test was used. Categorical data were evaluated for significance using the Pearson χ2 test or Fisher’s exact test.
For the primary outcome, postoperative 24 h cumulative sufentanil consumption was analyzed with the Mann–Whitney U-test. For the secondary outcomes, the Mann–Whitney U-test was used to compare sufentanil consumption during the different postoperative periods between the two groups. Within-group comparisons of sufentanil consumption in the four different postoperative time periods were performed using the Friedman test. Inter-group differences in pain scores, use of vasoactive agents, lower limb muscle strength after surgery, and length of hospital stay were also assessed using the Mann–Whitney U-test. Intraoperative remifentanil consumption and the timing of first flatus were assessed using the Student’s t-test. The incidence of patients needing rescue analgesics, PONV, pruritus, and respiratory depression were assessed using the χ2 test or Fisher’s exact test. Heart rate and mean arterial blood pressure were analyzed using the repeated-measures analysis of covariance, and values at T0 were included as covariates. The intervention–time interaction was test first. Then, the intervention main effect would be tested if not significant. Otherwise, Inter-group differences at different time points would be tested using the Student’s t-test. The p-values from multiple comparisons were corrected using the Bonferroni correction. For all tests, p-value < 0.05 was considered statistically significant.
Results
Forty-eight patients were enrolled, all completing the study (Figure 1). The baseline patient characteristics were similar between the two groups (Table 1). The postoperative 24 h cumulative sufentanil consumption was lower in the caudal block group than in the sham group (p < 0.001; Figure 2). During the four different time periods after surgery, namely 0–6 h, 6–12 h, 12–18 h, and 18–24 h, sufentanil consumption was lower in the caudal block group than in the sham group (p <0.001, <0.001, =0.098 or =0.039, respectively; Figure 3). Sufentanil consumption during 0–6 h post-surgery was more than 6–12 h, 12–18 h and 18–24 h after surgery in the sham group (p = 0.009, <0.001, and <0.001, respectively; Figure 3), but no significant difference was found for any pairwise comparisons between the four time periods in the caudal block group (Figure 3).
 |
Table 1 Baseline Characteristics of the Patients in the Two Groups |
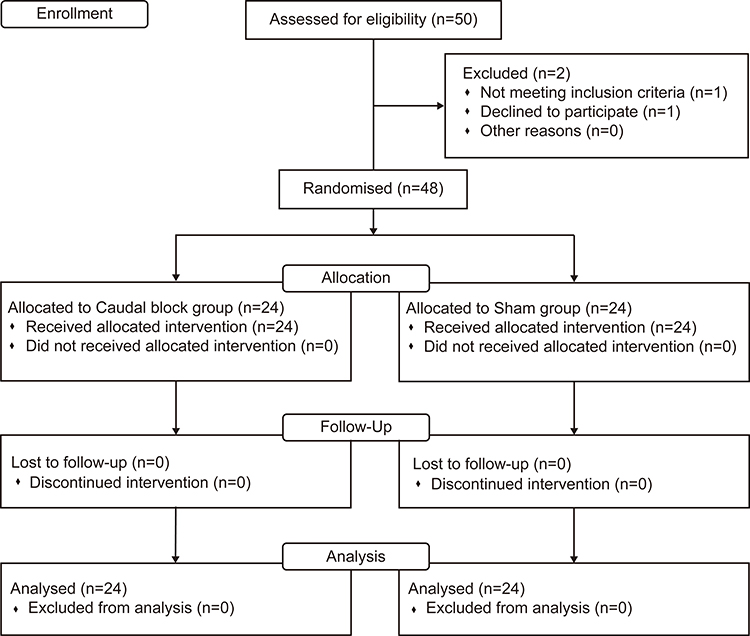 |
Figure 1 CONSORT diagram of patient recruitment. |
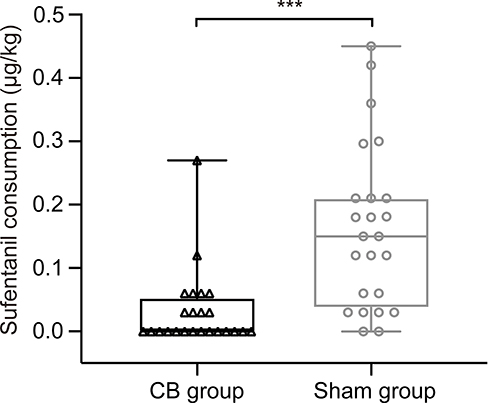 |
Figure 2 Twenty-four-hour cumulative sufentanil consumption after surgery in the caudal block and sham groups. *** Significantly different between the two groups, p < 0.001. CB, caudal block. |
 |
Figure 3 Postoperative sufentanil consumption during the indicated time periods in the caudal block group and sham group. *Significantly different between the two groups, *p < 0.05, *** p < 0.001. α Statistically significant (P < 0.05, Bonferroni corrected) differences compared to 0–6 hours. |
The patients who felt visceral pain was more intense (visceral pain score was greater than incisional score) at rest, accounting for 95.8% at 1 h, 95.8% at 6 h, 95.8% at 12 h, and 75% at 24 h post-surgery in the sham group, and only 50%, 16.7%, 12.5%, and 4.2% in the caudal block group at these four-time points, respectively. The visceral pain scores of all remaining patients were equal to their incisional pain scores, and the incisional pain scores for all patients and time points were no more than three. Compared with the sham group, the caudal block significantly reduced visceral pain scores at rest and during movement at all four-time points post-surgery (Figure 4). In contrast, incisional pain showed significant differences between the two groups only at 1, 6, and 12 h post-surgery during movement (Figure 4).
 |
Figure 4 Postoperative numerical rating scale pain scores at rest and during movement for incisional and visceral pain for 24 h postoperatively. NRS pain scores at rest for incisional pain (a) and visceral pain (b). NRS pain scores during movement for incisional pain (c) and visceral pain (d). * Significantly different between the two groups, *p < 0.05, *** p < 0.001. |
Intraoperative remifentanil consumption was significantly lower in the caudal block group than in the sham group (Table 2). There was no difference between the two groups regarding heart rate (p = 0.111; Figure 5) and mean arterial blood pressure (p=0.956; Figure 5). No statistically significant differences were observed regarding the number of patients needing rescue analgesics, use of vasoactive agents, lower limb muscle strength at 1 and 6 h after surgery, PONV, pruritus, respiratory depression, the timing of first flatus, and length of hospital stay between the two groups (Table 2).
 |
Table 2 Secondary Outcome Parameters for Patients in This Study |
 |
Figure 5 Mean (SD) heart rate (a) and mean arterial blood pressure (b) in the caudal block group and sham group over time in operation. HR, heart rate; MAP, mean arterial blood pressure; T0, after entering the pre-anesthesia room; T1, before the induction; T2, before the tracheal intubation; T3, after the tracheal intubation; T4, the start of pneumoperitoneum; T5, 5 min after pneumoperitoneum; T6, 15 min after pneumoperitoneum; T7, 30 min after pneumoperitoneum; T8, at the end of the surgery. |
Discussion
The significant finding of this trial was that caudal ropivacaine-morphine provided adequate postoperative analgesia after TLH. Caudal ropivacaine–morphine effectively reduced the demand for sufentanil within 24 h after surgery, and this effect was especially marked within 6 h after surgery. The results also showed that visceral pain was more intense than incisional pain at 1, 6, 12, and 24 hours in most individuals undergoing TLH without regional block techniques, as previously reported.11 Compared with the sham block, the caudal block significantly reduced the NRS scores of visceral pain at these four-time points, whether at rest or during movement. Moreover, the highest incisional NRS pain score during movement did not exceed three, which indicated that patients who underwent TLH only had mild incisional pain.
These conclusions are consistent with our hypotheses. We demonstrated that pain after TLH was mainly due to surgical trauma caused by a vaginal cuff suture. Postoperative pain from the top of the vagina is transmitted via the pelvic splanchnic nerves to S2 to 4 and is perceived as visceral pain in patients undergoing TLH. This may explain the ineffectiveness of the TQLB and superior hypogastric plexus block in postoperative pain relief in patients following this procedure.13,22 Mechanically, TQLB relieved visceral pain through local anesthetic spread into the thoracic paravertebral space. The superior hypogastric plexus is an integral part of transmitting pain from the uterus and accompanying structures but is not involved in pain transmission in the cervical and upper vaginal regions.14 It might be argued that pain after TLH also originates from the abdominal wall and peritoneum, as well as the uterus and cervix. The multimodal analgesic regimen used in our study containing parecoxib, dexamethasone, and sufentanil could well control the pain from the abdominal wall and peritoneum and pain from the uterus and cervix after TLH was no longer existent because they have already been removed. Moreover, caudal block aids in decreasing pain associated with the circumferential excision at the upper vagina and subsequent suturing after uterus removal, resulting in relatively lower remifentanil consumption during surgery.
Murphy et al found that the minimum volume of medication required to cover the sacral nerve in the caudal block completely was 20 mL.23 We selected 20 mL but not a larger volume, as the injection volume because we mainly aimed to block the sacral nerve roots. Moreover, a higher dose of the local anesthetic is associated with a higher likelihood of systemic toxicity. Thus, the caudal block failed to cover the trocar site and alleviate postoperative incisional pain at rest. Although the intergroup differences were found for the NRS scores of incisional pain during movement at 1 h, 6 h, and 12 h after TLH, caudal block only reduced pain scores by 0.38 (95% CI: 0.05 to 0.70), 0.29 (95% CI: −0.01 to 0.60), and 0.21 (95% CI: 0.03 to 0.38) at 1 h, 6 h, and 12 h after surgery, respectively. These reductions were less than the minimal clinically significant differences in pain scores.24
Compared with a peripheral nerve block, a caudal block has a relatively shorter duration of 4 to 6 h.17 Considering that moderate-to-severe pain still existed 6 h after TLH11 and that the caudal block was performed before general anesthesia in our study, we used morphine as an adjunct to prolong the duration of the block.25,26 Caudal blocks usually use 0.1 to 0.375% ropivacaine or 0.125 to 0.25% bupivacaine.27 To lessen toxicity and motor block, we chose ropivacaine to perform caudal block rather than bupivacaine.28,29 The clinical bolus dose of epidural morphine is 2 to 3 mg as a bolus.30 We chose low-dose morphine to reduce dose-dependent complications such as pruritus and respiratory depression.31 Although no retrieved articles reported the specific duration of caudal ropivacaine–morphine, the analgesic effect of epidural morphine was shown to last for up to 24 h in most patients;32 this could explain why caudal ropivacaine–morphine maintained an analgesic effect until 24 h after TLH.
Consistent with a previous study, none of the patients in the present study showed a reduction in lower limb muscle strength at 1 h and 6 h after surgery.33 The reasons could be attributed to the following three aspects. First, the EC50 of ropivacaine for motor blockade in epidural analgesia was 0.497%, much higher than 0.25%.34 Secondly, the duration of the caudal block without morphine was 4 to 6 h.17 The motor block is known to disappear before the sensory block. Moreover, the addition of opioids did not prolong the motor block time.35 The third reason is that caudal blocks hardly decrease adductor strength, which is the primary muscle strength measuring the extent of the motor block when using the Bromage Score.36
The caudal block did not affect the hemodynamic outcomes in our study; this was expected because the preganglionic sympathetic neurons extended from the T1 to the L2 level, which the caudal block failed to reach. No significant differences were observed in the incidence of nausea and vomiting, and no patients experienced pruritus or respiratory depression, probably because we chose low-dose morphine.
However, our study has some limitations. First, we did not test the level of hypoesthesia because our study was performed in a double-blind fashion. Second, since all patients undergoing TLH were routinely required not to ambulate until 24 h after surgery in the gynecological ward, we did not record the time to first mobilization. Instead, we measured the lower limb muscle strength. Third, our study did not record urinary retention, a possible complication of a caudal block. The insertion of a urinary catheter was a routine practice before the start of TLH, and the indwelling urinary catheter was maintained for 24 h according to the requirements of the gynecologists.
Conclusion
In conclusion, a caudal block with ropivacaine and morphine could provide a satisfactory analgesic effect for 24 h postoperatively without additional adverse effects after TLH, and postoperative pain after TLH primarily originates from the vaginal cuff.
Data Sharing Statement
The manuscript presents all the data that substantiate our conclusion. The individual deidentified participant data will be available from the corresponding author ([email protected]) for reasonable request.
Ethics Approval and Informed Consent
Informed consent was obtained from all the study patients and this study complies with the Declaration of Helsinki. The Scientific Research Ethics Committee of the Affiliated Hospital of Jiangsu University, China, approved this single-center, prospective, randomized controlled study (KY2022H1014-4).
Acknowledgments
We acknowledge the contributions of Dr Hanpeng Lai, Department of Occupational and Environmental Health, School of Public Health, Yangzhou University, Yangzhou, China, for the statistical analyses.
Funding
This study was supported by the Postgraduate Research & Practice Innovation Program of Jiangsu Province (No. SJCX23_2100), the Medical Education Collaborative Innovation Fund of Jiangsu University (No. JDY2022006), and the Scientific Research Project of “Jinshan Talents” in Zhenjiang City (No. YLJ202109).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Farquhar CM, Steiner CA. Hysterectomy rates in the United States 1990–1997. Obstet Gynecol. 2002;99(2):229–234. doi:10.1016/s0029-7844(01)01723-9
2. Laberge PY, Singh SS. Surgical approach to hysterectomy: introducing the concept of technicity. J Obstet Gynaecol Can. 2009;31(11):1050–1053. doi:10.1016/S1701-2163(16)34350-X
3. Donnez O, Jadoul P, Squifflet J, et al. A series of 3190 laparoscopic hysterectomies for benign disease from 1990 to 2006: evaluation of complications compared with vaginal and abdominal procedures. BJOG. 2009;116(4):492–500. doi:10.1111/j.1471-0528.2008.01966.x
4. Luchristt D, Brown O, Kenton K, et al. Trends in operative time and outcomes in minimally invasive hysterectomy from 2008 to 2018. Am J Obstet Gynecol. 2021;224(2):202.e1–202.e12. doi:10.1016/j.ajog.2020.08.014
5. Huang CC, Lo TS, Huang YT, et al. Surgical trends and time frame comparison of surgical types of hysterectomy: a nationwide, population-based 15-year study. J Minim Invasive Gynecol. 2020;27(1):65–73.e1. doi:10.1016/j.jmig.2019.02.020
6. Stoller N, Wertli MM, Zaugg TM, et al. Regional variation of hysterectomy for benign uterine diseases in Switzerland. PLoS One. 2020;15(5):e0233082. doi:10.1371/journal.pone.0233082
7. Lee SH, Oh SR, Cho YJ, et al. Comparison of vaginal hysterectomy and laparoscopic hysterectomy: a systematic review and meta-analysis. BMC Women Health. 2019;19(1):1–12. doi:10.1186/s12905-019-0784-4
8. Ghezzi F, Uccella S, Cromi A, et al. Postoperative pain after laparoscopic and vaginal hysterectomy for benign gynecologic disease: a randomized trial. Am J Obstet Gynecol. 2010;203(2):118.e1–8. doi:10.1016/j.ajog.2010.04.026
9. Gerbershagen HJ, Aduckathil S, van Wijck AJ, et al. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiol. 2013;118(4):934–944. doi:10.1097/ALN.0b013e31828866b3
10. Zhang L, Hao LJ, Hou XL, et al. Preoperative anxiety and postoperative pain in patients with laparoscopic hysterectomy. Front Psych. 2021;12:727250. doi:10.3389/fpsyg.2021.727250
11. Choi JB, Kang K, Song MK, et al. Pain characteristics after total laparoscopic hysterectomy. Int J Med Sci. 2016;13(8):562–568. doi:10.7150/ijms.15875
12. Lirk P, Thiry J, Bonnet MP, et al. PROSPECT Working Group. Pain management after laparoscopic hysterectomy: systematic review of literature and PROSPECT recommendations. Reg Anesth Pain Med. 2019;44(4):425–436. doi:10.1136/rapm-2018-100024
13. Hansen C, Dam M, Nielsen MV, et al. Transmuscular quadratus lumborum block for total laparoscopic hysterectomy: a double-blind, randomized, placebo-controlled trial. Reg Anesth Pain Med. 2021;46(1):25–30. doi:10.1136/rapm-2020-101931
14. Netter FH. Section 6 pelvis and perineum. In: Machado CAG, Hansen JT, Benninger B, Brueckner-Collins J, Hoagland TM, Tubbs RS, editors. Atlas of Human Anatomy.
15. Apan A, Cuvas O. Caudal block in adults: new horizons with ultrasound. Minerva Anestesiol. 2013;79(12):1332–1333.
16. Kao SC, Lin CS. Caudal epidural block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017:9217145. doi:10.1155/2017/9217145
17. Ecoffey C, Lacroix F, Giaufré E, et al. Association des Anesthésistes Réanimateurs Pédiatriques d’Expression Française (ADARPEF). Epidemiology and morbidity of regional anesthesia in children: a follow-up one-year prospective survey of the French-Language Society of Paediatric Anaesthesiologists (ADARPEF). Paediatr Anaesth. 2010;20(12):1061–1069. doi:10.1111/j.1460-9592.2010.03448.x
18. Nestor CC, Ng C, Sepulveda P, et al. Pharmacological and clinical implications of local anaesthetic mixtures: a narrative review. Anaesth. 2022;77(3):339–350. doi:10.1111/anae.15641
19. Boezaart AP, Smith CR, Chembrovich S, et al. Visceral versus somatic pain: an educational review of anatomy and clinical implications. Reg Anesth Pain Med. 2021;46(7):629–636. doi:10.1136/rapm-2020-102084
20. Gali B, Whalen FX, Schroeder DR, et al. Identification of patients at risk for postoperative respiratory complications using a preoperative obstructive sleep apnea screening tool and postanesthesia care assessment. Anesthesiol. 2009;110(4):869–877. doi:10.1097/ALN.0b013e31819b5d70
21. Tas B, Kalk NJ, Lozano-García M, et al. Undetected respiratory depression in people with opioid use disorder. Drug Alcohol Depend. 2022;234:109401. doi:10.1016/j.drugalcdep.2022.109401
22. Clark NV, Moore K, Maghsoudlou P, et al. Superior hypogastric plexus block to reduce pain after laparoscopic hysterectomy: a randomized controlled trial. Obstet Gynecol. 2021;137(4):648–656. doi:10.1097/AOG.0000000000004329
23. Murphy DT, Kavanagh EC, Poynton A, et al. MR epidurography: distribution of injectate at caudal epidural injection. Skelet Radiol. 2015;44(4):565–571. doi:10.1007/s00256-014-1963-x
24. Myles PS, Myles DB, Galagher W, et al. Measuring acute postoperative pain using the visual analog scale: the minimal clinically important difference and patient acceptable symptom state. Br J Anaesth. 2017;118(3):424–429. doi:10.1093/bja/aew466
25. Sato M, Iida T, Kikuchi C, et al. Comparison of caudal ropivacaine-morphine and paravertebral catheter for major upper abdominal surgery in infants. Paediatr Anaesth. 2017;27(5):524–530. doi:10.1111/pan.13104
26. Sato M, Bosenberg A. Ultrasound-guided quadratus lumborum block compared to caudal ropivacaine/morphine in children undergoing surgery for vesicoureteric reflex. Paediatr Anaesth. 2019;29(7):738–743. doi:10.1111/pan.13650
27. Suresh S, Ecoffey C, Bosenberg A, et al. The European society of regional anaesthesia and pain therapy/American society of regional anesthesia and pain medicine recommendations on local anesthetics and adjuvants dosage in pediatric regional anesthesia. Reg Anesth Pain Med. 2018;43(2):211–216. doi:10.1097/AAP.0000000000000702
28. Fischer C, Blanié P, Jaouën E, et al. Ropivacaine, 0.1%, plus sufentanil, 0.5 microg/mL, versus bupivacaine, 0.1%, plus sufentanil, 0.5 microg/mL, using patient-controlled epidural analgesia for labor: a double-blind comparison. Anesthesiol. 2000;92(6):1588–1593. doi:10.1097/00000542-200006000-00015
29. Hodgson PS, Liu SS. A comparison of ropivacaine with fentanyl to bupivacaine with fentanyl for postoperative patient-controlled epidural analgesia. Anesth Analg. 2001;92(4):1024–1028. doi:10.1097/00000539-200104000-00041
30. Roofthooft E, Joshi GP, Rawal N, et al. PROSPECT working group* of the European Society of Regional Anaesthesia and pain therapy and supported by the Obstetric Anaesthetists’ Association. PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations. Anesth. 2021;76:665–680. doi:10.1111/anae.15339
31. Jørgensen H, Wetterslev J, Møiniche S, et al. Epidural local anaesthetics versus opioid-based analgesic regimens on postoperative gastrointestinal paralysis, PONV, and pain after abdominal surgery. Cochrane Database Syst Rev. 2000;4:CD001893. doi:10.1002/14651858.CD001893
32. Lanz E, Kehrberger E, Theiss D. Epidural morphine: a clinical double-blind study of dosage. Anesth Analg. 1985;64:786–791. doi:10.1213/00000539-198508000-00007
33. Tsuchiya M, Kyoh Y, Mizutani K, et al. Ultrasound-guided single shot caudal block anesthesia reduces postoperative urinary catheter-induced discomfort. Minerva Anestesiol. 2013;79(12):1381–1388.
34. Lacassie HJ, Columb MO, Lacassie HP, et al. The relative motor blocking potencies of epidural bupivacaine and ropivacaine in labor. Anesth Analg. 2002;95(1):204–208. doi:10.1097/00000539-200207000-00036
35. Hamber EA, Viscomi CM. Intrathecal lipophilic opioids as adjuncts to surgical spinal anesthesia. Reg Anesth Pain Med. 1999;24(3):255–263. doi:10.1097/00115550-199924030-00015
36. Graham AC, McClure JH. Quantitative assessment of motor block in labouring women receiving epidural analgesia. Anesth. 2001;56(5):470–476. doi:10.1046/j.1365-2044.2001.01524-6.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Spinal Anaesthesia as an Adjunct to General Anaesthesia for Laparoscopic Abdominoperineal Rectal Amputation
Antunes M, Baumgärtel A, Gjessing PF, Ytrebø LM
Journal of Pain Research 2023, 16:1855-1865
Published Date: 31 May 2023
Dexmedetomidine and Dexamethasone as Adjuvants to the Local Anesthetic Mixture in Rhomboid Intercostal and Sub-Serratus Block for Video-Assisted Thoracoscopic Surgery: A Randomized, Double-Blind, Controlled Trial
Liu QF, Shi CN, Tong JH, Li KP, Yang JJ, Ji MH, Liu QR
Drug Design, Development and Therapy 2024, 18:4485-4496
Published Date: 7 October 2024
Tetracaine Eye Drops as a Preemptive Topical Skin Anesthesia for Botulinum Toxin Type A Injections in Blepharospasm Patients: A Randomized Controlled Trial
Pinitpanich N, Hirunwiwatkul P, Ongprakobkul C, Tulvatana W
Clinical Ophthalmology 2026, 20:603168
Published Date: 15 May 2026