Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
TACE Combined with Ralox-HAIC (Oxaliplatin Puls Raltitrexed) and System Therapy in Patients with Unresectable Hepatocellular Carcinoma
Authors Liu R ![]() , Cao G, Li L
, Cao G, Li L ![]() , Liu J, Cao H, Xing M
, Liu J, Cao H, Xing M ![]() , Feng Y, Li Z
, Feng Y, Li Z ![]() , Wang B
, Wang B ![]()
Received 27 March 2026
Accepted for publication 13 June 2026
Published 18 June 2026 Volume 2026:13 609273
DOI https://doi.org/10.2147/JHC.S609273
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Imam Waked
Ruiqing Liu,1 Guangshao Cao,1 Lupeng Li,1 Jianwen Liu,1 Huicun Cao,1 Mengyan Xing,1 Yangbo Feng,2 Zesheng Li,3 Boyu Wang4
1Department of Interventional Oncology, Henan Provincal People’s Hospital, Zhengzhou, People’s Republic of China; 2Department of Interventional Oncology, Zhengzhou University People’s Hospital, Zhengzhou, People’s Republic of China; 3Department of Ultrasound, Zhengzhou University People’s Hospital, Zhengzhou, People’s Republic of China; 4Department of Clinical Medicine, Henan Medical College of Zhengzhou University, Zhengzhou, People’s Republic of China
Correspondence: Ruiqing Liu, Email [email protected]
Objective: To retrospective analysis the efficacy and safety of Transarterial Chemoembolization (TACE) combined with Hepatic Arterial Infusion Chemotherapy (Ralox-HAIC, Oxaliplatin + Raltitrexed) and systemic therapy in patients with unresectable Hepatocellular Carcinoma (uHCC).
Methods: Clinical data of patients with uHCC who received TACE combined with Ralox-HAIC followed by sequential systemic therapy at our hospital between January 2023 and December 2024 were analyzed. The primary endpoint was Objective Response Rate (ORR). Secondary endpoints included Progression-Free Survival (PFS), Overall Survival (OS) and treatment safety.
Results: A total of thirty-six patients with complete data were included. Efficacy evaluation showed: Complete Response (CR) in 6 cases (16.67%), Partial Response (PR) in 22 cases (61.11%), Stable Disease (SD) in 5 cases (13.89%), and Progressive Disease (PD) in 2 cases (5.56%). The ORR was 77.78%, and the Disease Control Rate (DCR) was 91.67%. The median PFS was 12.0 months, and the median OS was 19.0months. The one-year and two-year survival rates were 89% and 38%, respectively. No Grade 4 treatment-related adverse events or treatment-related deaths occurred.
Conclusion: TACE combined with Ralox-HAIC and systemic therapy demonstrated a high ORR and DCR with manageable safety in uHCC, warranting further prospective studies for validation.
Keywords: carcinoma, hepatocellular, chemoembolization, therapeutic, infusion chemotherapy, hepatic artery, raltitrexed, oxaliplatin
Introduction
Hepatocellular Carcinoma (HCC) ranks sixth in incidence and third in mortality among malignant tumors worldwide.1 A significant number of patients are diagnosed at intermediate or advanced stages, thereby precluding the possibility of curative treatment. The IMbrave150 study has demonstrated that the combination of anti-angiogenic targeted therapies with immune checkpoint inhibitors can significantly improve tumor response rates.2,3 As a result, current national and international guidelines recommend systemic therapy, primarily involving a combination of targeted and immunotherapeutic agents, as the preferred treatment approach for uHCC.4,5 HCC is notably hypervascular, and in cases with a substantial tumor burden, systemic therapy alone often exhibits a delayed therapeutic effect. Recent studies suggest that integrating local therapies, such as transarterial chemoembolization (TACE) or hepatic arterial infusion chemotherapy (HAIC), with systemic treatments can significantly enhance tumor response rates.6–8
TACE induces ischemic necrosis by occluding the arteries that supply the tumor, thereby effectively controlling lesions and rapidly diminishing tumor burden.9 However, in patients with substantial tumor burdens, such as those with massive HCC, the efficacy of TACE alone is limited, and it poses risks including liver abscess and liver failure. HAIC administers high concentrations of chemotherapeutic agents directly to the tumor site. Research indicates that HAIC offers significant advantages for treating large HCC or those with portal vein tumor thrombus.10 The combination of TACE and HAIC can synergistically reduce tumor blood supply through embolization while simultaneously enhancing cytotoxic effects via continuous infusion. This approach has the potential to improve therapeutic efficacy and mitigate the risk of complications associated with excessive embolization.11
The currently prevalent HAIC regimen is the FOLFOX protocol, which demonstrated superior efficacy compared to sorafenib monotherapy.10,12 Nevertheless, the time-dependent nature of fluorouracil in this regimen necessitates prolonged infusion periods (up to 48 hours), which can lead to extended bed rest, thereby increasing the risk of thrombosis and resulting in poor patient tolerance. Additionally, complications such as arterial catheter blockage are noted. In recent years, the Ralox regimen, which combines oxaliplatin and raltitrexed, has gained traction in the treatment of advanced liver cancer, exhibiting an objective response rate and disease control rate of 52.3% and 75.6%, respectively, with a median survival time of 8.7 months.13,14 Oxaliplatin, a third-generation platinum compound, exerts its antitumor effects by inhibiting tumor cell proliferation and inducing apoptosis through the formation of DNA cross-links.15 Raltitrexed, a specific inhibitor of thymidylate synthase, is characterized by a prolonged half-life (approximately 198 hours) and requires only a brief infusion duration (approximately 1 hour), eliminating the risk of fluorouracil-associated cardiotoxicity.16,17 Compared to the FOLFOX regimen, the Ralox regimen significantly reduces infusion time, thereby minimizing associated complications.18
For patients with uHCC, TACE combined with Ralox-HAIC can achieve effective local tumor control and rapidly reduce tumor burden. Subsequent sequential systemic therapy can further consolidate therapeutic efficacy and prolong long-term survival. At present, the therapeutic strategy of TACE combined with Ralox-HAIC followed by sequential systemic therapy has not been reported in uHCC, representing an unmet clinical research gap worthy of further exploration. This study aims to analyze the efficacy and safety of TACE combined with Ralox-HAIC and systemic therapy in patients with uHCC treated between January 2023 and December 2024.
Methods-Patients
Study Design and Populations
Inclusion Criteria
All enrolled patients were aged 18 to 70 years and had a definitive diagnosis of HCC confirmed by pathological examination or typical radiological manifestations. All cases were staged as Barcelona Clinic Liver Cancer (BCLC) B or C, with primary tumor burden confined to the liver and at least one measurable intrahepatic lesion. Contrast-enhanced CT or MRI performed within two weeks prior to treatment was required for baseline tumor evaluation. Patients were required to have a Child-Pugh score≤7 points (Child-Pugh A or B) and an Eastern Cooperative Oncology Group (ECOG) performance status of 0–1. All participants received TACE combined with Ralox-HAIC, followed by sequential targeted therapy plus immunotherapy, and had complete clinical imaging and follow-up data.
Exclusion Criteria
Patients were excluded if they had concurrent other malignant tumors, severe hepatic or renal dysfunction, or incomplete clinical information and unavailable follow-up data.
This retrospective study was approved by the Medical Ethics Committee of Henan Provincial People’s Hospital (Ethical Approval No: (2025) Ethics Review No. 114). The Institutional Review Board waived the requirement for individual patient informed consent because the study was a retrospective analysis using de-identified clinical medical records, without any additional invasive procedures or intervention to patients. All patient-related data were strictly anonymized and kept confidential throughout the study. The study protocol was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
TACE and HAIC Procedures
All interventional procedures were conducted by physicians with over a decade of experience. The TACE procedure involved femoral artery puncture and catheterization, followed by angiography to delineate the tumor’s blood supply. Superselective catheterization of the target vessel was performed, and an iodized oil emulsion (comprising iodized oil and pirarubicin) was injected for embolization, with additional gelatin sponge or microspheres used as needed. The catheter was retained in the tumor-feeding artery, allowing the patient to return to the ward for continuous infusion chemotherapy. To prevent blockage, the catheter was flushed with heparin solution before infusion and was externally secured for protection.
Ralox-HAIC Regimen
85 mg/m2of Oxaliplatin was mixed with 250 mL of 5% glucose solution and administered at a rate of 70 mL/h, with 0.1 mL of 2% lidocaine added to prevent arterial spasms. Raltitrexed at 3 mg/m2was combined with 100 mL of normal saline and infused at 100 mL/h.
Systemic Therapy
Systemic Therapy involved rechecking blood tests (complete blood count, liver and kidney function) five to seven days after TACE combined with HAIC treatment. Once these indices recovered, targeted combined immunotherapy was started. Targeted therapy included agents like Lenvatinib, Apatinib, and Bevacizumab, while immune checkpoint inhibitors included Sintilimab, Tislelizumab, Camrelizumab, and Atezolizumab. Throughout the treatment, patients’ blood pressure, thyroid, pituitary, liver, and kidney functions were regularly monitored, and any adverse reactions were addressed promptly.
Assessment and Outcomes
The initial follow-up was conducted one month post-treatment, followed by subsequent assessments every 4 to 8 weeks until either the patient’s death or the study’s cutoff date of July, 2025. Each follow-up visit comprised a comprehensive evaluation, including the collection of medical history, physical examination, laboratory investigations (encompassing complete blood count, liver function tests, creatinine levels, coagulation parameters, and alpha-fetoprotein), and imaging studies (contrast-enhanced abdominal CT/MRI and chest CT). Tumor response was evaluated in accordance with the modified Response Evaluation Criteria in Solid Tumors (mRECIST) by two independent radiologists, with any discrepancies resolved by a third senior physician. The primary endpoint of the study was the Objective Response Rate (ORR), defined as the proportion of patients achieving complete response (CR) or partial response (PR). Secondary endpoints included the Disease Control Rate (DCR), defined as the proportion of patients achieving CR, PR, or stable disease (SD), as well as Progression-Free Survival (PFS) and Overall Survival (OS).
Statistical Analysis
The data analysis was conducted utilizing SPSS software. Ninety-five percent confidence intervals (CIs) were computed for the objective response rate (ORR), disease control rate (DCR), and survival rates. Progression-free survival (PFS) and overall survival (OS) were evaluated employing the Kaplan-Meier method, with median values and corresponding 95% CIs being calculated.
Results
Patient Population
Between January 2023 and December 2024, a cohort of 45 patients underwent treatment with TACE combined with Ralox-HAIC. Of these, 9 patients were excluded due to either the absence of systemic therapy or incomplete data, resulting in a final sample size of 36 patients for analysis. The median age of the cohort was 53 years, ranging from 35 to 65 years. The gender distribution comprised 33 males (91.7%) and 3 females (8.3%). Hepatitis B infection was prevalent in 88.9% of the patients. The median maximum tumor diameter was recorded at 8.7 cm, with a range of 2 to 19 cm. In terms of disease staging, 28 patients (77.8%) were classified as Barcelona Clinic Liver Cancer (BCLC) stage B, while 8 patients (22.2%) were at stage C. Half of the patients were treatment-naïve, whereas the remaining 50% received the regimen following postoperative recurrence or failure of prior local therapy. Further details are presented in Table 1. Regarding treatment specifics, the 36 patients collectively underwent 86 cycles of TACE combined with Ralox-HAIC, with a median of 2.4 treatment sessions per patient. Specifically, 4 patients (11.1%) completed 4 cycles, 8 patients (22.2%) completed 3 cycles, and 24 patients (66.7%) completed 2 cycles.
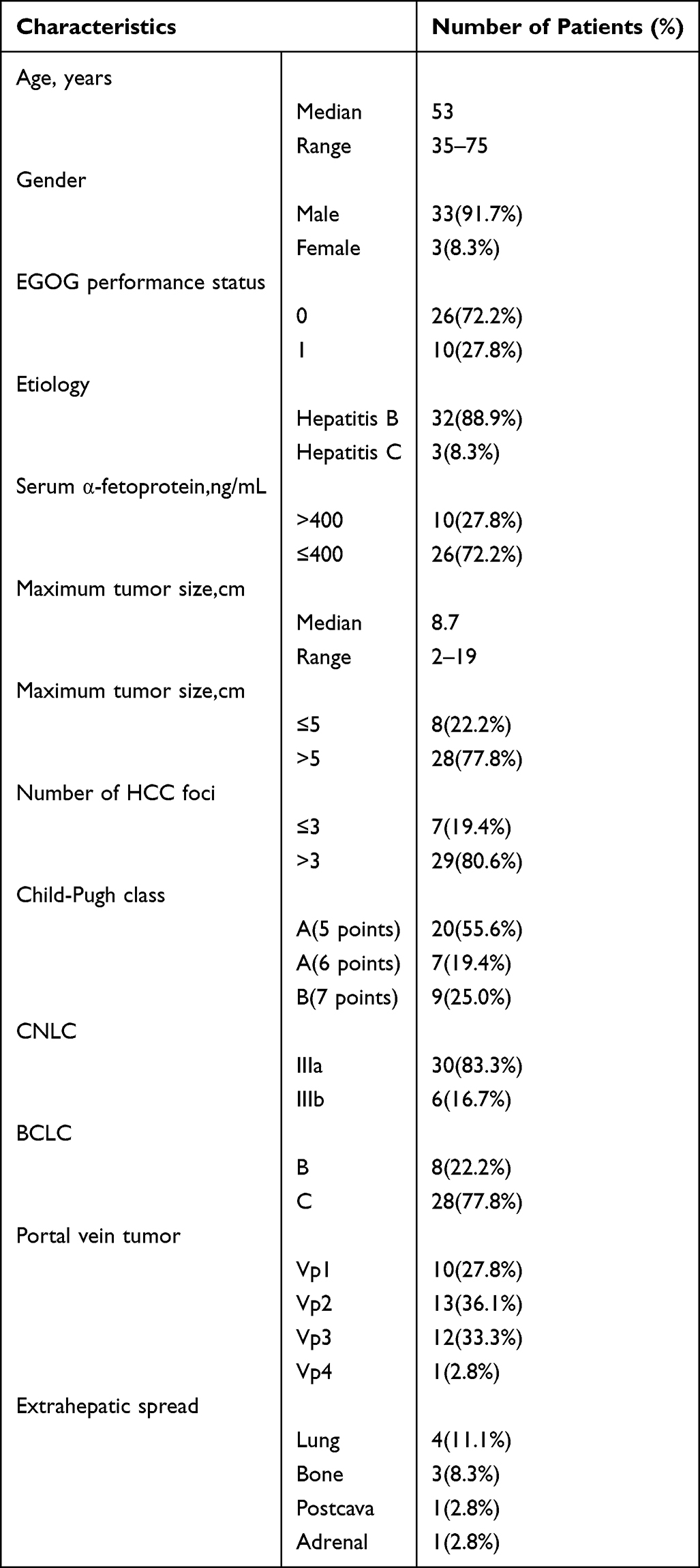 |
Table 1 Baseline Characteristics of the Patient Population (n=36) |
Among the 36 patients, 26 (72.2%) received lenvatinib, 6 (16.7%) received apatinib, and 4 (11.1%) received bevacizumab. 25 (69.4%) received sintilimab, 3 (8.3%) received tislelizumab, 5 (13.9%) received carfilzumab, and 3 (8.3%) received atezolizumab.
Efficacy Results
The median follow-up duration was 22.0 months. The efficacy assessment revealed a complete response (CR) in 6 cases (16.67%), partial response (PR) in 22 cases (61.11%), stable disease (SD) in 5 cases (13.89%), and progressive disease (PD) in 2 cases (5.56%). The overall response rate (ORR) was 77.78% (95% confidence interval [CI]: 50.0–80.0%), while the disease control rate (DCR) was 91.67% (95% CI: 65.0–90.0%) (refer to Figure 1). The median progression-free survival (PFS) was 12.0 months (95% CI: 7.37–16.63), and the median overall survival (OS) was 19.0months (95% CI: 13.97–24.03) (refer to Figure 2). The survival rates at 1 year and 2 years were 89% and 38%, respectively.
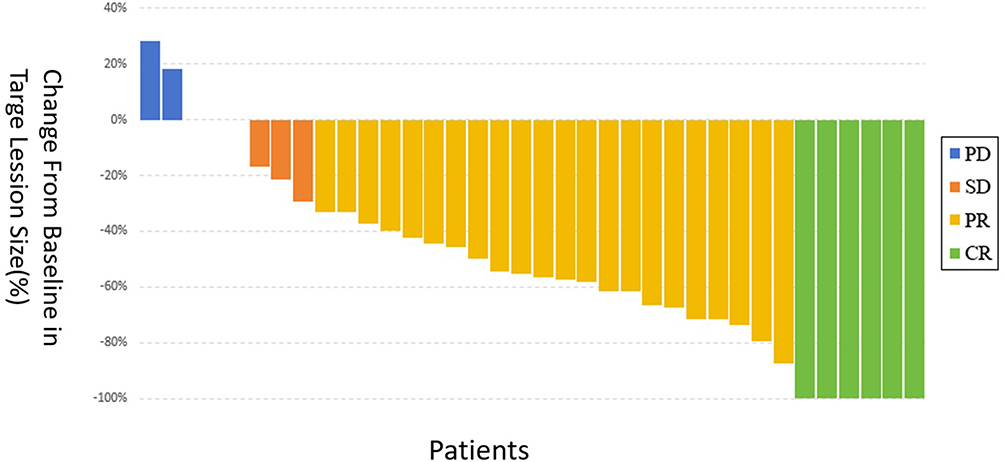 |
Figure 1 Waterfall plot for the best percentage change in target lesions size after treatment in 36 patients who underwent TACE+Ralox-HAIC plus system therapy. |
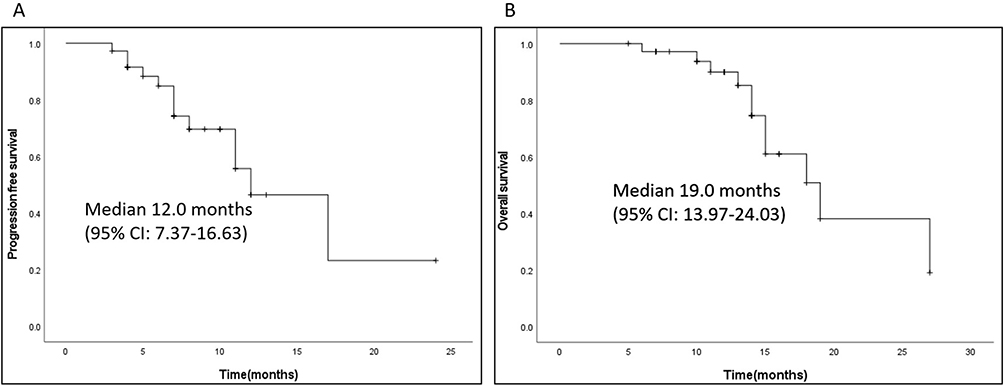 |
Figure 2 Kaplan-Meier curves for progression free survival (A) and overall survival (B) in 36 patients who underwent at least one post-treatment efficacy assessment. |
A patient with uHCC and portal vein tumor thrombus began receiving three sessions of TACE + Ralox-HAIC treatment in March 2023, followed by sequential combination of targeted and immunotherapy. The patient achieved a complete response (CR) state and was regularly followed up. As of July 2025, when the follow-up ended, the patient’s condition remained stable (refer to Figure 3).
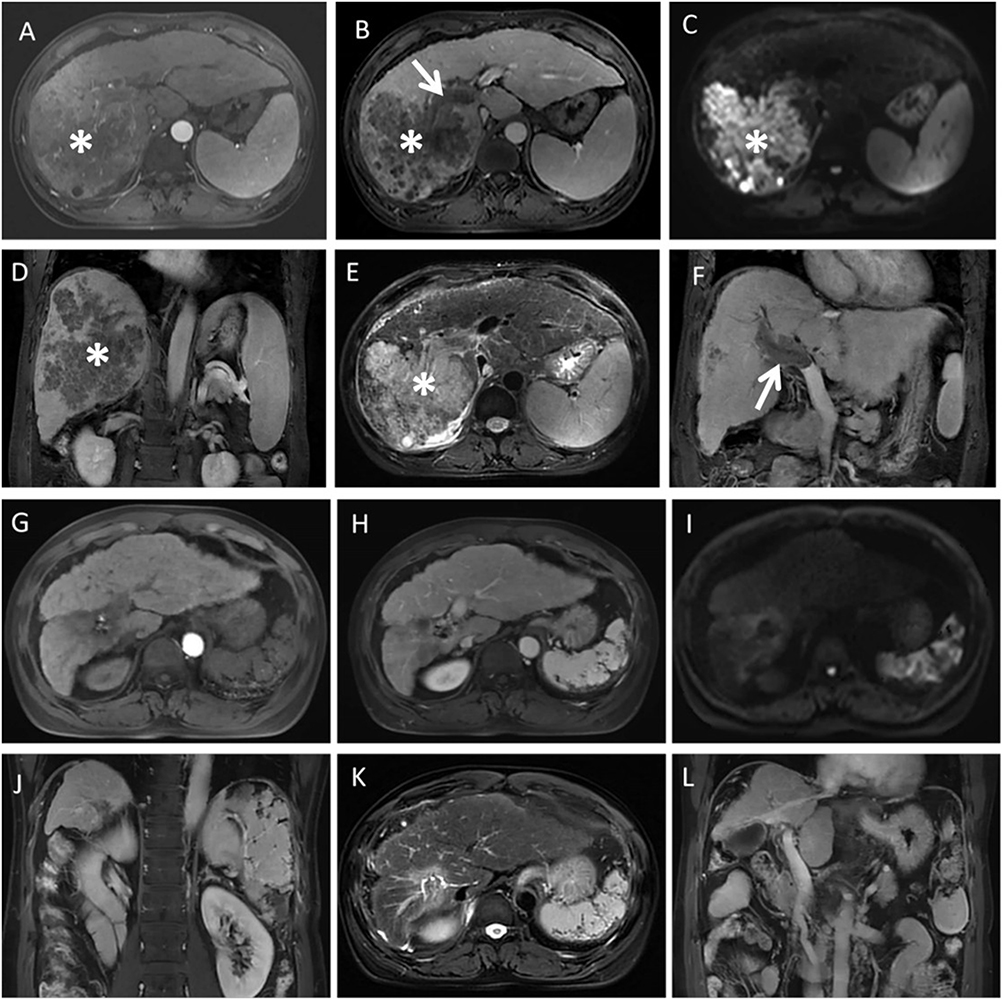 |
Figure 3 The 50-year-old male patient diagnosed with unresectable hepatocellular carcinoma (uHCC) accompanied by portal vein tumor thrombus (PVTT), classified as Barcelona Clinic Liver Cancer (BCLC) stage C, in March 2023. Due to the ineligibility for surgical resection, the patient commenced TACE combined with Ralox-HAIC for a total of three cycles. During the initial cycle, the patient was administered lenvatinib (8 mg once daily) and sintilimab (200 mg every three weeks). On March 23, 2023, magnetic resonance imaging (MRI) revealed the tumor (indicated by a white asterisk) during the arterial phase (A), in the venous phase (B), diffusion-weighted imaging (DWI) (C), coronal view (D), T2-weighted imaging (E), and another coronal view (F) demonstrated the presence of the portal vein tumor thrombus (indicated by a white arrow). Subsequent imaging on July 25, 2025, included arterial phase (G), venous phase (H), DWI (I), coronal view (J), T2-weighted imaging (K), and an additional coronal view (L). |
At the time of data cutoff, five patients remained on the initial targeted therapy and immunotherapy regimen. Twenty-six patients had their systemic treatment regimen changed. One patient achieved radiological and clinical response enabling conversion to surgical resection. One patient was unable to tolerate further active treatment due to poor performance status and received best supportive care only. One patient underwent Y90 radioembolization.
Safety
Treatment-related adverse events were primarily of Grade 1–3 severity. No Grade 4 or higher severe adverse reactions or treatment-related fatalities were observed. Common adverse events included hypertension (25.6%), hypothyroidism (30.6%), diarrhea (22.2%), proteinuria (16.7%), elevated transaminases (11.1%), and immunosuppression (manifested as leukopenia and thrombocytopenia) (Table 2). One patient experienced myelosuppression followed by a liver abscess post-procedure, which improved following drainage and anti-infection therapy. Another patient developed immune-related hypopituitarism, which was managed with hormone replacement therapy.
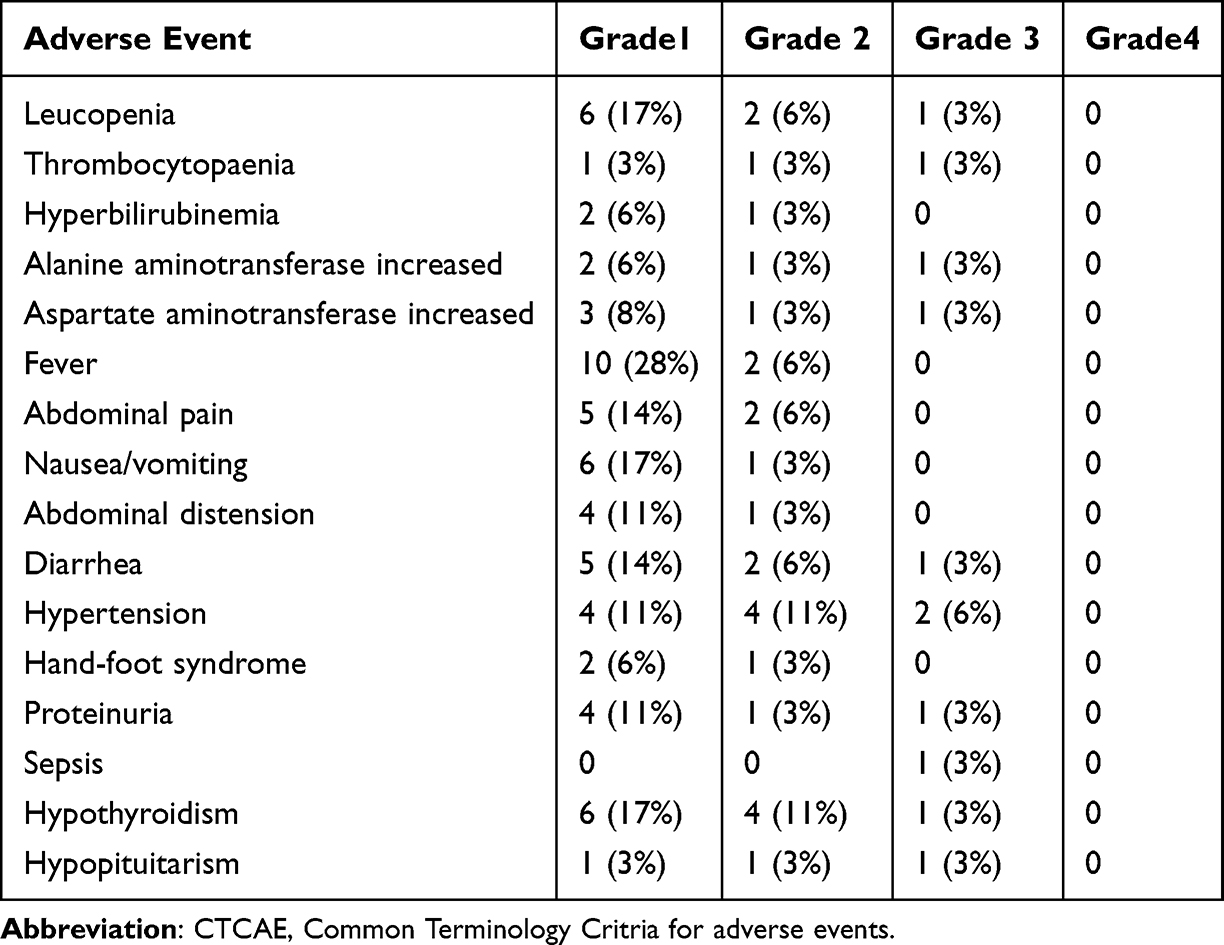 |
Table 2 Treatment-Related Adverse Events of the Patient Population (n=36) (According to CTCAE v4.03) |
Discussion
This single-center study evaluated the efficacy and safety of TACE in combination with Ralox-HAIC and systemic therapy for patients with uHCC. The findings revealed an Objective Response Rate (ORR) of 77.78%, a Disease Control Rate (DCR) of 91.67%, a median Progression-Free Survival (PFS) of 12.0 months, a median Overall Survival (OS) of 19.0 months, and 1-year and 2-year survival rates of 89% and 38%, respectively. Previous studies, such as IMbrave150, have highlighted the significance of systemic therapy in the management of advanced liver cancer.2,3 Nevertheless, for patients with a high tumor burden, the effectiveness of systemic therapy alone is often inadequate.19 In such cases, local therapy can play a crucial complementary role.20 TACE is the standard local treatment for intermediate-stage unresectable HCC; however, the ORR for TACE alone typically ranges from 30% to 50%. Its effectiveness is limited for advanced-stage HCC, which is prevalent in China, and it carries risks such as liver abscess formation. Recent research suggests that the combination of TACE with HAIC can substantially enhance patient prognosis.21 Early investigations by Korean and Japanese researchers employed cisplatin combined with fluorouracil regimens for HAIC, yielding efficacy rates of 21–27%.22,23
The primary innovation of this study lies in the strategic integration of low-dose TACE (using only 10 mg of epirubicin emulsified with iodized oil for embolization, without intraoperative chemotherapy infusion) with sequential Ralox-HAIC and systemic therapy. Unlike conventional TACE combined with HAIC, our approach first achieves tumor devascularization via TACE, followed by continuous high-concentration chemotherapy through Ralox-HAIC to residual lesions and portal vein tumor thrombi. Additionally, the Ralox-HAIC regimen (oxaliplatin plus raltitrexed) offers a shorter infusion duration compared with FOLFOX-HAIC, thereby improving patient compliance and reducing catheter-related complications. Furthermore, the triplet combination leverages synergistic mechanisms: TACE-induced neoantigen release enhances PD-1 inhibitor efficacy, targeted therapy normalizes tumor vasculature to facilitate chemotherapy accumulation, and HAIC exerts direct cytotoxic effects. This mechanistic synergy translated into an ORR of 77.78% and a median OS of 19.0 months, which compare favorably with historical data from TACE monotherapy (ORR 30–50%) or systemic therapy alone (IMbrave150: ORR ~30%). Thus, this study provides preliminary evidence for a novel, practically optimized combination strategy for unresectable HCC, particularly in patients with high tumor burden.
Chinese researchers have implemented the FOLFOX-HAIC regimen, which has demonstrated significantly greater efficacy compared to sorafenib.10,12 Nonetheless, the regimen’s requirement for prolonged continuous infusion presents challenges, including suboptimal patient compliance and elevated risks of thrombosis and catheter blockage. In response, the Ralox-HAIC regimen, which combines oxaliplatin and raltitrexed and is characterized by a shorter infusion duration, has been developed. Numerous studies have validated its safety and efficacy. Investigations conducted at Fujian Provincial Cancer Hospital and Southern Medical University have reported substantial response and disease control rates with the Ralox-HAIC regimen.14,18,24 Furthermore, recent research suggests that Ralox-HAIC, when combined with systemic therapy, can achieve an objective response rate (ORR) of 66.7%.13
The strategy implemented in this study involved initially conducting TACE embolization intraoperatively, utilizing only 10 mg of epirubicin emulsified with iodized oil for embolization, without the infusion of chemotherapeutic agents. This was subsequently followed by a sequential Ralox-HAIC continuous infusion, in conjunction with systemic therapy. This approach resulted in an objective response rate (ORR) of 77.78%, with adverse reactions being generally manageable. Notably, one patient experienced myelosuppression and another developed a liver abscess; both patients had histories of multiple prior treatments and showed improvement following active management. Furthermore, one instance of hypopituitarism was deemed to be associated with immunotherapy.
The efficacy observed in this study surpasses that reported in some previous studies. Several factors may account for this enhanced efficacy: Firstly, the TACE and Ralox-HAIC exhibits a synergistic effect, particularly in cases of hypervascular or extensive HCC. Following the embolization of primary feeding arteries by TACE, HAIC facilitates the continuous delivery of high-concentration chemotherapeutic agents to residual lesions, venous tumor thrombi, or satellite foci.25 Secondly, targeted therapies can inhibit angiogenesis following embolization and promote vascular normalization, thereby enhancing the accumulation of chemotherapeutic agents within the tumor. Thirdly, the ischemia and necrosis induced by TACE can lead to the release of neoantigens, which may potentiate the efficacy of PD-1 inhibitors.26 The integration of local and systemic therapies may collectively modulate the tumor microenvironment, augment immune cell infiltration, and thereby enhance the effectiveness of immunotherapy.27
This study has several limitations. Due to the small sample size, limited novelty (the innovation being primarily at the regimen-combination level rather than a mechanistic breakthrough), and moderate study design quality (single-center, non-randomized, without a direct comparator arm), the current findings lack sufficient persuasiveness and robustness. Therefore, these results should be interpreted as hypothesis-generating rather than conclusive.
In summary, this study demonstrates that the combination of TACE with Ralox-HAIC and systemic therapy exhibits promising anti-tumor activity (ORR 77.78%, median OS 19.0 months) with a manageable safety profile in patients with unresectable HCC. The strategy of low-dose TACE embolization followed by sequential Ralox-HAIC infusion represents a clinically innovative optimization that enhances drug delivery and leverages local–systemic synergy. Large-scale, prospective, randomized controlled trials are warranted to validate the clinical efficacy of this triplet regimen.
Funding
This work was supported by the Henan Provincial Science and Technology Research Project, China (LHGJ20240028).
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–10. doi:10.3322/caac.21834
2. Finn RS, Qin S, Ikeda M, et al. IMbrave150 Investigators. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
3. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873. doi:10.1016/j.jhep.2021.11.030
4. Reig M, Sanduzzi-Zamparelli M, Forner A, et al. BCLC strategy for prognosis prediction and treatment recommendations: the 2026 update. J Hepatol. 2025;84(3):631–654. doi:10.1016/j.jhep.2025.10.020
5. Department of Medical Administration, National Health Commission of the People’s Republic of China. Guidelines for the diagnosis and treatment of primary liver cancer (2024 edition). Chin J Gen Surg. 2024;33(4):475–530. doi:10.7659/j.issn.1005-6947.2024.04.001.
6. Zhu HD, Li HL, Huang MS, et al. Transarterial chemoembolization with PD- (L)1 inhibitors plus molecular targeted therapies for hepatocellular carcinoma (CHANCE001). Signal Transduct Target Ther. 2023;8(1):58. doi:10.1038/s41392-022-01235-0
7. Jin ZC, Zhong BY, Chen JJ, et al. Real-world efficacy and safety of TACE plus camrelizumab and apatinib in patients with HCC (CHANCE2211): a propensity score matching study. Eur Radiol. 2023;33(12):8669–8681. doi:10.1007/s00330-023-09754-2
8. Li S, Wu J, Wu J, et al. Prediction of early treatment response to the combination therapy of TACE plus lenvatinib and anti-PD-1 antibody immunotherapy for unresectable hepatocellular carcinoma: multicenter retrospective study. Front Immunol. 2023;14:1109771. doi:10.3389/fimmu.2023.1109771
9. Villanueva A. Hepatocellular carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
10. He M, Li Q, Zou R, et al. Sorafenib plus hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin vs sorafenib alone for hepatocellular carcinoma with portal vein invasion: a randomized clinical trial. JAMA Oncol. 2019;5(7):953–960. doi:10.1001/jamaoncol.2019.0250
11. Chen S, Shi F, Wu Z, et al. Hepatic Arterial Infusion Chemotherapy Plus Lenvatinib and Tislelizumab with or Without Transhepatic Arterial Embolization for Unresectable Hepatocellular Carcinoma with Portal Vein Tumor Thrombus and High Tumor Burden: a Multicenter Retrospective Study. J Hepatocell Carcinoma. 2023;10:1209–1222. doi:10.2147/JHC.S417550
12. Chen L, Martinelli E, Cheng A, et al. Pan-Asian adapted ESMO clinical practice guidelines for the management of patients with intermediate and advanced/relapsed hepatocellular carcinoma: a TOS-ESMO initiative endorsed by CSCO, ISMPO, JSMO, KSMO, MOS and SSO. Ann Oncol. 2020;31:334–351. doi:10.1016/j.annonc.2019.12.001
13. Zang M, Li Q, Hu X, et al. Camrelizumab Combined with Lenvatinib and RALOX-Hepatic Arterial Infusion Chemotherapy for Unresectable Hepatocellular Carcinoma (Cal Era): a Prospective, Single-Arm, Phase II Trial. Liver Cancer. 2025;14(6):1–12. doi:10.1159/000546575
14. Chen S, Wang X, Yuan B, et al. Apatinib plus hepatic arterial infusion of oxaliplatin and raltitrexed for hepatocellular carcinoma with extrahepatic metastasis: phase II trial. Nat Commun. 2024;15(1):8857. doi:10.1038/s41467-024-52700-z
15. Lyu J, Liu Z, Liu W, et al. Effect of Oxaliplatin or 5-FU on Proliferation of Human Hepatoma Cell HepG2 after Hypoxia and Serum Limitation. Prog Mod Biomed. 2013;13(33):6460–6462.
16. Gunasekara NS, Faulds D. Raltitrexed. A review of its pharmacological properties and clinical efficacy in the management of advanced colorectal cancer. Drugs. 1998;55(3):423e35. doi:10.2165/00003495-199855030-00012
17. Clarke SJ, Hanwell J, Boer M, et al. Phase I trial of ZD1694, a new folate-based thymidylate synthase inhibitor, in patients with solid tumors. J Clin Oncol. 1996;14(5):1495e503. doi:10.1200/JCO.1996.14.5.1495
18. Zang MY, Li Q, Hu X, et al. Hepatic arterial infusion chemotherapy with oxaliplatin plus raltitrexed versus oxaliplatin plus fluorouracil in intermediate and advanced hepatocellular carcinoma: a retrospective study. J Clin Oncol. 2023;125(Pt A):111019. doi:10.1016/j.intimp.2023.111019
19. Breder VV, Vogel A, Merle P, et al. IMbrave150: exploratory efficacy and safety results of hepatocellular carcinoma (HCC) patients (pts) with main trunk and/or contralateral portal vein invasion (Vp4) treated with atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in a global Ph III study. J Clin Oncol. 2021;39(15_suppl):4073. doi:10.1002/cam4.3618
20. Palmer DH, Malagari K, Kulik LM. Role of locoregional therapies in the wake of systemic therapy. J Hepatol. 2020;72(2):277–287. doi:10.1016/j.jhep.2019.09.023
21. Guo W, Gao J, Zhuang W, et al. Efficacy and safety of hepatic arterial infusion chemotherapy combined with transarterial embolization for unresectable hepatocellular carcinoma: a propensity score-matching cohort study. JGH Open. 2020;4(3):477–483. doi:10.1177/0300891625132783
22. Choi JH, Chung WJ, Bae SH, et al. Randomized, prospective, comparative study on the effects and safety of sorafenib vs. hepatic arterial infusion chemotherapy in patients with advanced hepatocellular carcinoma with portal vein tumor thrombosis. Cancer Chemother Pharmacol. 2018;82(3):469–478. doi:10.1007/s00280-018-3638-0
23. Ikeda M, Shimizu S, Sato T, et al. Sorafenib plus hepatic arterial infusion chemotherapy with cisplatin versus sorafenib for advanced hepatocellular carcinoma: randomized phase II trial. Ann Oncol. 2016;27(11):2090–2096. doi:10.1093/annonc/mdw323
24. Chen S, Zhang K, Liu W, et al. Hepatic arterial infusion of oxaliplatin plus raltitrexed in patients with intermediate and advanced stage hepatocellular carcinoma: a Phase II, single-arm, prospective study. Eur J Cancer. 2020;134:90–98. doi:10.1016/j.ejca.2020.03.032
25. Li QJ, He MK, Chen HW, et al. Hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin versus transarterial chemoembolization for large hepatocellular carcinoma: a randomized Phase III trial. J Clin Oncol. 2022;40(2):150–160. doi:10.1200/JCO.21.00608
26. Yuan YC, He W, Yang ZW, et al. TACE-HAIC combined with targeted therapy and immunotherapy versus TACE alone for hepatocellular carcinoma with portal vein tumour thrombus: a propensity score matching study. Int J Surg. 2023;109(5):1222–1230. doi:10.1097/JS9.0000000000000256
27. Zhong BY, Fan WZ, Guan JJ, et al. Combination locoregional and systemic therapies in hepatocellular carcinoma. Lancet Gastroenterol Hepatol. 2025;10(4):369–386. doi:10.1016/S2468-1253(24)00247-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Tyrosine Kinase Inhibitors Plus Anti-PD-1 Antibodies with Hepatic Arterial Infusion Chemotherapy or Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma
Yu B, Zhang N, Feng Y, Zhang Y, Zhang T, Wang L
Journal of Hepatocellular Carcinoma 2023, 10:1735-1748
Published Date: 6 October 2023
Comparable Clinical Outcomes Between Transarterial Chemoembolization or Hepatic Arterial Infusion Chemotherapy Combined with Tyrosine Kinase Inhibitors and PD-1 Inhibitors in Unresectable Hepatocellular Carcinoma
Long T, Yang Z, Zeng H, Wu W, Hu Z, Yang Z, Hu D, Zhou Z, Chen M, Zhang Y
Journal of Hepatocellular Carcinoma 2023, 10:1849-1859
Published Date: 20 October 2023
Safety and Efficacy of TACE-HAIC Combined with Lenvatinib and PD-1 Inhibitors in Large Intermediate-Stage Hepatocellular Carcinoma: A Multi-Center Retrospective Study
Ni J, Li C, Sun H, Liu Y, Guo G, Zhou X, Zhou Z, Fan R, Hu H, Xu L
Journal of Hepatocellular Carcinoma 2026, 13:586001
Published Date: 24 April 2026
Raltitrexed in Hepatocellular Carcinoma: Mechanistic Rationale and Clinical Evidence from Arterial-Based Therapies
Jia X, Ding Y, Chen Y, Wang W
Journal of Hepatocellular Carcinoma 2026, 13:601493
Published Date: 28 April 2026
Efficacy and Safety of TACE-HAIC Combined with Molecular Targeted Therapy and Immune Checkpoint Inhibitors for Unresectable Hepatocellular Carcinoma
Feng Z, Wang X, Xu J, Chen S, Hao M, Hu H, Qiu S, Liao Y, Yu W, Fang Z
Journal of Hepatocellular Carcinoma 2026, 13:588860
Published Date: 22 May 2026