")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Tyrosine Kinase Inhibitors Plus Anti-PD-1 Antibodies with Hepatic Arterial Infusion Chemotherapy or Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma
Authors Yu B, Zhang N, Feng Y, Zhang Y , Zhang T, Wang L
Received 24 August 2023
Accepted for publication 29 September 2023
Published 6 October 2023 Volume 2023:10 Pages 1735—1748
DOI https://doi.org/10.2147/JHC.S431917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Bingran Yu, Ning Zhang, Yun Feng, Yongfa Zhang, Ti Zhang, Lu Wang
Department of Hepatic Surgery, Shanghai Cancer Center, Shanghai Medical College, Fudan University, Shanghai, People’s Republic of China
Correspondence: Lu Wang, Department of Hepatic Surgery, Shanghai Cancer Center, Shanghai Medical College, Fudan University, No. 270 Dongan Road, Shanghai, 200032, People’s Republic of China, Email [email protected]
Background: The combination of tyrosine kinase inhibitors (TKIs) and anti-PD-1 antibodies with hepatic arterial infusion chemotherapy (HAIC) or transarterial chemoembolization (TACE) has shown encouraging anti-tumor effects in the treatment of hepatocellular carcinoma (HCC). We explored the efficacy and safety of TKIs and anti-PD-1 antibodies combined with HAIC or TACE in HCC.
Methods: Data from 302 HCC patients receiving HAIC combined with TKIs and anti-PD-1 antibodies (HAIC-TP group) and 446 HCC patients receiving TACE combined with TKIs and anti-PD-1 antibodies (TACE-TP group) were retrospectively collected. Clinicopathological characteristics, tumor response, progression-free survival (PFS), overall survival (OS), and adverse events (AEs) were compared between two groups. Propensity score matching (PSM) analysis was performed to minimize bias.
Results: The HAIC-TP group exhibited better objective response rate (RECIST: 33.1% versus 7.8%, P < 0.001; mRECIST: 51.4% versus 17.5%, P < 0.001), longer PFS (12.4 months versus 8.2 months, P < 0.001), and longer OS (not reached versus 13.8 months, P < 0.001) than TACE-TP group. Surgery was performed after combination therapy in 34 patients of the HAIC-TP group and in 7 patients of the TACE-TP group (P < 0.001). Similar results were also observed in the PSM analysis. Multivariate analysis indicated type of treatment, alpha-fetoprotein, ALBI grade, portal vein tumor thrombus, and extrahepatic status were risk factors for poor prognosis. Nausea, vomiting, diarrhea, and abdominal pain occurred more frequently in the HAIC-TP group, whereas liver dysfunction occurred more frequently in the TACE-TP group. All AEs were acceptable and manageable as a result of treatment interruption or dose modification.
Conclusion: The combination of HAIC with TKIs and anti-PD-1 antibodies is an effective and safe therapeutic regimen over TACE-based combination therapy for patients with HCC. A prospective study with a large sample size is required to validate the efficacy and safety of the combination therapy.
Keywords: hepatocellular carcinoma, hepatic arterial infusion chemotherapy, transarterial chemoembolization, combination therapy
Introduction
Hepatocellular carcinoma (HCC), which accounts for approximately 90% of all cases, is the most common pathological type of primary liver cancer.1 Liver resection is the first choice of treatment for patients with early stage HCC and is associated with a 5-year survival rate of more than 60%.1,2 Transarterial and systemic therapies are recommended for patients at intermediate or advanced stages.2 Common transarterial therapies include transarterial chemoembolization (TACE) and hepatic arterial infusion chemotherapy (HAIC). TACE is a therapy consisting of intra-arterial chemotherapy and selected embolization, whereas HAIC is an interventional therapy without using embolic materials via the hepatic arteries.3 TACE and HAIC both exert promising anti-tumor effects on unresectable HCC, with a disease control rate (DCR) of 82.0% for HAIC and a 1-year survival rate of 83.5% for TACE.4,5
As various factors should be considered in the selection of therapeutic strategies for HCC, including tumor stage, liver function, and patient general condition, a multidisciplinary treatment method is needed to improve patients’ outcomes. Combination treatments based on locoregional and systemic therapies have been proposed for the treatment of HCC.6 TACE combined with tyrosine kinase inhibitors (TKIs) and anti-PD-1 antibodies has been utilized in the treatment of HCC and is associated with favorable tumor response and manageable toxicity.7–10 Combination therapy with TKIs, anti-PD-1 antibodies, and HAIC has been reported to have acceptable toxic effects and encouraging anti-tumor activity in patients with advanced HCC.11–13 However, it remains unclear which interventional therapy yields better tumor response and survival outcomes when combined with TKIs and anti-PD-1 antibodies.
Hence, we conducted a retrospective analysis of patients with unresectable HCC and compared clinicopathological characteristics and prognosis of patients receiving HAIC combined with TKIs and anti-PD-1 antibodies with those treated with TACE when combined with TKIs and anti-PD-1 antibodies in our institution.
Materials and Methods
Patient Cohorts
This retrospective study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Fudan University Shanghai Cancer Center (FUSCC). The medical records of patients with unresectable HCC who were treated with HAIC combined with TKIs and anti-PD-1 agents (HAIC-TP group) or TACE combined with TKIs and anti-PD-1 agents (TACE-TP group) at the Department of Hepatic Surgery of FUSCC between December 2020 and July 2022 were reviewed for eligibility. Patients were included based on the following specific criteria: age ≥ 18 years; Eastern Cooperative Oncology Group performance status (ECOG PS) of 0–1; Child-Pugh class A/B liver function; at least one measurable intrahepatic lesion according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1;14 and adequate organ function [absolute neutrophil count ≥ 1.2 × 109/L, platelet count ≥ 60 × 109/L, total bilirubin (T-BIL) < 30 μmol/L, albumin (ALB) ≥ 30 g/L, aspartate transaminase (AST) and alanine transaminase (ALT) ≤ 5 × upper limit of the normal, creatinine clearance rate of ≤ 1.5 × upper limit of the normal, and left ventricular ejection ≥ 45%]. Patients were excluded if they had received other treatments for HCC during combination therapy. Patients were also excluded if they were diagnosed with other malignant tumors or if their medical information and follow-up data were incomplete.
Treatment Protocol
The Seldinger technique was used to puncture the femoral artery and a catheter was inserted into the feeding hepatic artery under digital subtraction angiography guidance. Chemotherapeutic agents (20 mg of hydroxycamptothecin and 60 mg of pirarubicin) were injected, and embolization was performed with iodized oil (3–15 mL) or gelfoam or microspheres when necessary during the TACE procedure, while the chemotherapeutic regimen of HAIC (oxaliplatin 85/m2 from hours 0 to 2 on day 1; leucovorin 400 mg/m2 from hours 2 to 3 on day 1; 5-fluorouracil 400 mg/m2 bolus at hour 3; and 2400 mg/m2 over 46 hours on days 1 and 2) was infused via the catheter in the ward. HAIC was repeated every 3 weeks, while TACE was repeated depending on the accumulation of iodized oil, which was evaluated using plain computed tomography (CT), and the enhancement of viable HCC tissue, which was evaluated by contrast-enhanced magnetic resonance imaging (MRI). TKIs [lenvatinib: a dose of 12 mg/day (for body weight ≥ 60 kg) or 8 mg/day (for body weight < 60 kg); apatinib, a dose of 250 mg/day; donafenib, a dose of 200 mg twice daily] were administered more than 1 week prior to the initial interventional therapy, and discontinued from one day before each session of the interventional therapy to the time of withdrawal of the catheter. Anti PD-1 antibodies (tislelizumab, 200 mg/3 weeks; sintilimab, 200 mg/3 weeks; toripalimab, 240 mg/3 weeks) were administered intravenously every three weeks. Dose reduction and treatment interruption depended on disease progression, unacceptable toxicity, patients’ withdrawal of consent or changes in treatment plan, and technical difficulties in repeating interventional therapy. Enhanced CT or MRI was performed to evaluate therapeutic efficacy every 6 weeks after treatment initiation.
Data Collection and Study Objectives
Clinical and radiological data were retrospectively collected from medical records. The following data were collected and analyzed: age, sex, ECOG PS score, negative or positive results for hepatitis B surface antigen (HBV) and hepatitis C antibody (HCV), ⍺-fetoprotein (AFP), albumin-bilirubin (ALBI) grade, ALB, T-BIL, ALT, AST, Child-Pugh grade, tumor number, maximum tumor diameter, presence or absence of portal vein tumor thrombus (PVTT), extrahepatic metastases, and Barcelona Clinic Liver Cancer (BCLC) stage.
The primary endpoints were the objective response rate (ORR), defined as the proportion of patients with a complete response (CR) or a partial response (PR) that was maintained for at least four weeks, and DCR, defined as the proportion of patients with ORR plus stable disease (SD). The ORR and DCR were evaluated according to RECIST version 1.1 and modified RECIST (mRECIST).14,15 The second endpoints were progression-free survival (PFS), defined as the time from commencement of treatment to progression or death from any cause, and overall survival (OS), defined as the time from commencement of treatment to death from any cause. Adverse events (AEs) were assessed according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.03.
Propensity-Score Matching Analysis
Propensity-score matching (PSM) analysis was performed to minimize the uneven distribution of covariates between two groups. The matching algorithm included age, sex, ECOG PS score, negative or positive status for HBV and HCV, AFP level, ALBI grade, ALB, T-BIL, ALT, AST, Child-Pugh class, tumor number, maximum tumor diameter, presence or absence of PVTT and extrahepatic metastasis, and BCLC stage. The MatchIt package in R (version 4.1.2) was used for the PSM analysis. The caliper width was 0.05 and a one-to-one match between the two groups was obtained by nearest-neighbor matching.
Statistics Analysis
The clinicopathological characteristics and AEs of the two groups were compared using the chi-squared test or Fisher’s exact test. The results related to tumor response were analyzed using ordinal logistic regression. PFS and OS were calculated using the Kaplan–Meier method and compared using Log rank tests. Factors with P-value < 0.05, in the univariate analysis, were candidates for entry into a multivariable Cox proportional-hazards model. All P values were two-sided, with P values < 0.05 considered significant. SPSS (version 26.0), R (version 4.1.2), and GraphPad Prism (version 9.4.1) were used to perform analyses.
Results
Patient Characteristics
Between December 2020 and July 2022, 748 HCC patients were enrolled in this study, with 302 and 446 patients in the HAIC-TP and TACE-TP groups, respectively (Figure 1). The median sessions of HAIC were 3 (range: 1–10), while the median sessions of TACE were also 3 (range: 1–11). Clinicopathological characteristics of the patients are presented in Table 1. The patients in the HAIC-TP group were younger than those in the TACE-TP group (median: 54.5 vs 57.0 years, P < 0.001). In the HAIC-TP group, more patients were classified as having an ECOG PS of 0 (33.8% vs 21.3%, P < 0.001) or HBV infection status (82.1% vs 74.2%, P = 0.014). There were significant differences in AFP (P = 0.002), T-BIL (P = 0.003), and AST (P < 0.001) between the two groups. Furthermore, significant differences were observed in some tumor characteristics, including the tumor number (P < 0.001), maximum tumor diameter (P < 0.001), PVTT (P < 0.001), and BCLC stage (P < 0.001).
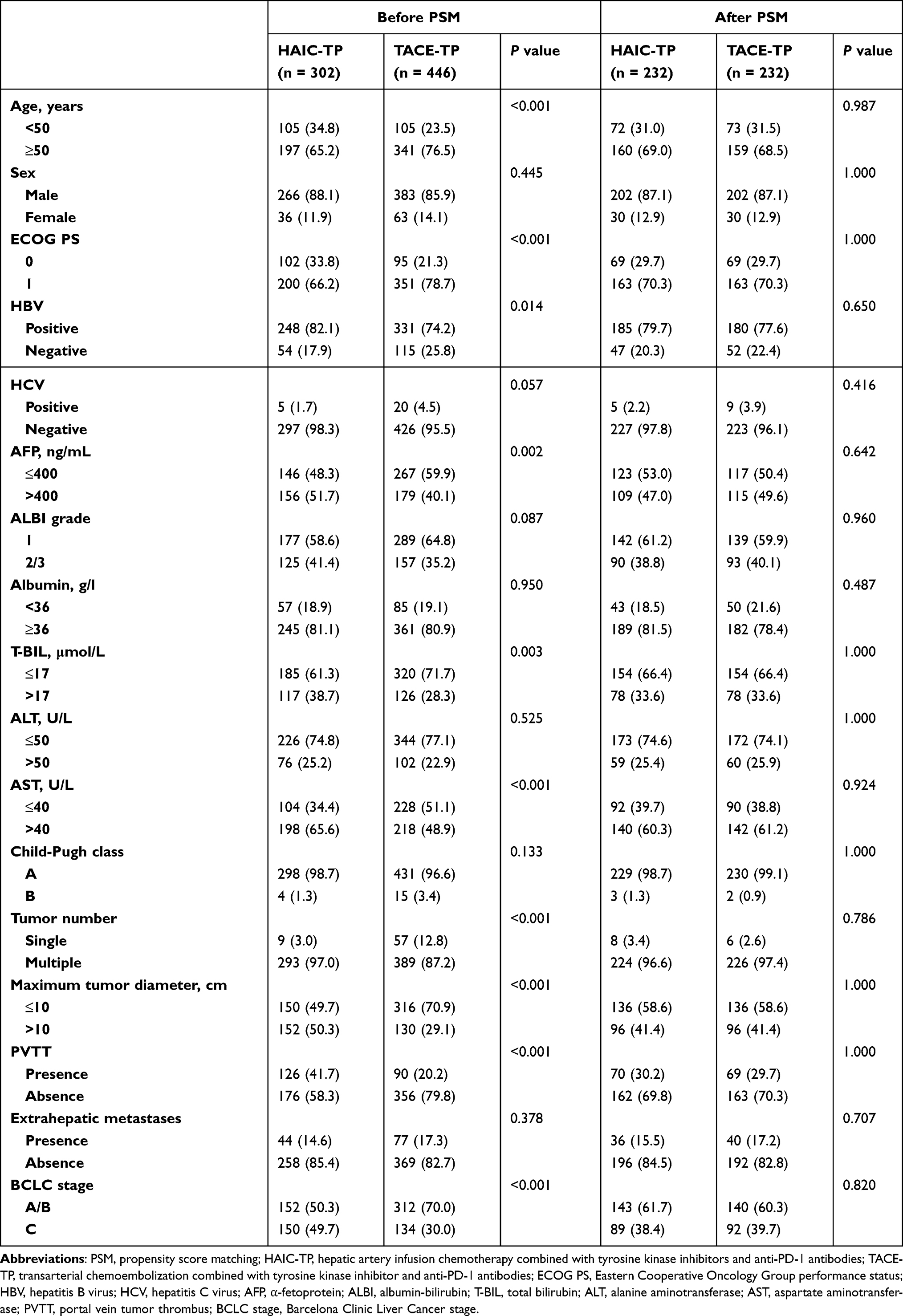 |
Table 1 Clinicopathological Characteristics Before and After PSM |
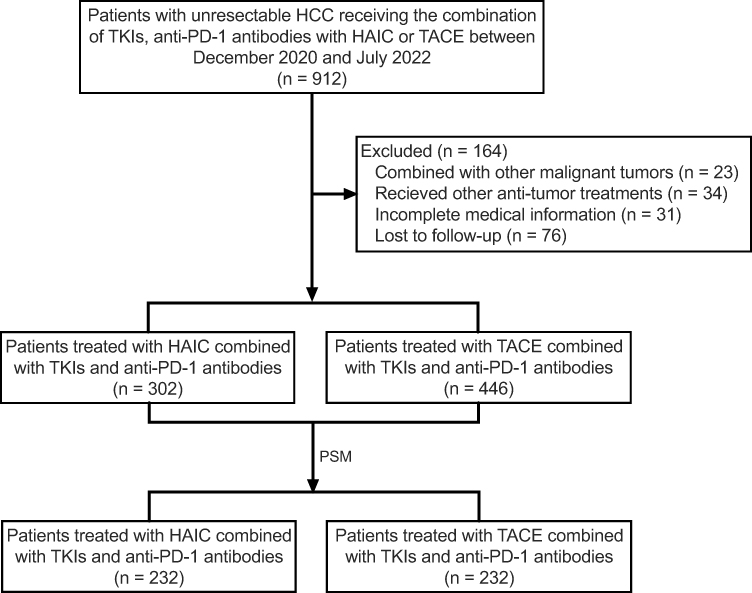 |
Figure 1 Flow diagram of the study. Abbreviations: HCC, hepatocellular carcinoma; TKIs, tyrosine kinase inhibitor; HAIC, hepatic arterial infusion chemotherapy; TACE, transarterial chemoembolization; PSM, propensity score matching. |
PSM analysis was performed to minimize bias. After PSM, 232 patients were selected from each group, and no significant difference was observed between the characteristics of the two groups.
Therapeutic Efficacy
The tumor responses are presented in Table 2. Before PSM, DCR and ORR were significantly higher in the HAIC-TP group than in the TACE-TP group based on the RECIST criteria (DCR: 77.8% vs 47.1%, P < 0.001; ORR: 33.1% vs 7.8%, P < 0.001). According to the mRECIST criteria, the HAIC-TP group also exhibited higher DCR and ORR than the TACE-TP group (DCR: 77.8% vs 47.1%, P < 0.001; ORR: 51.4% vs 17.5%, P < 0.001). After PSM, a higher DCR and ORR based on both the RECIST and mRECIST criteria were observed in the HAIC-TP group (79.7% vs 40.1%, P < 0.001; 34.5% vs 8.6%, P < 0.001; mRECIST: 79.7% vs 40.1%, P < 0.001; 52.5% vs 15.9%, P < 0.001). In addition, more patients in the HAIC-TP group underwent curative surgery because of tumor shrinkage or downstaging either before or after PSM than in the TACE-TP group (before PSM: 34 patients (11.3%) vs 7 patients (1.6%), P < 0.001; after PSM: 27 patients (11.6%) vs 4 patients (1.7%), P < 0.001). The CT or MRI scans of ten representative patients treated with a combination of HAIC with TKIs and anti-PD-1 antibodies are shown in Supplementary Figure 1.
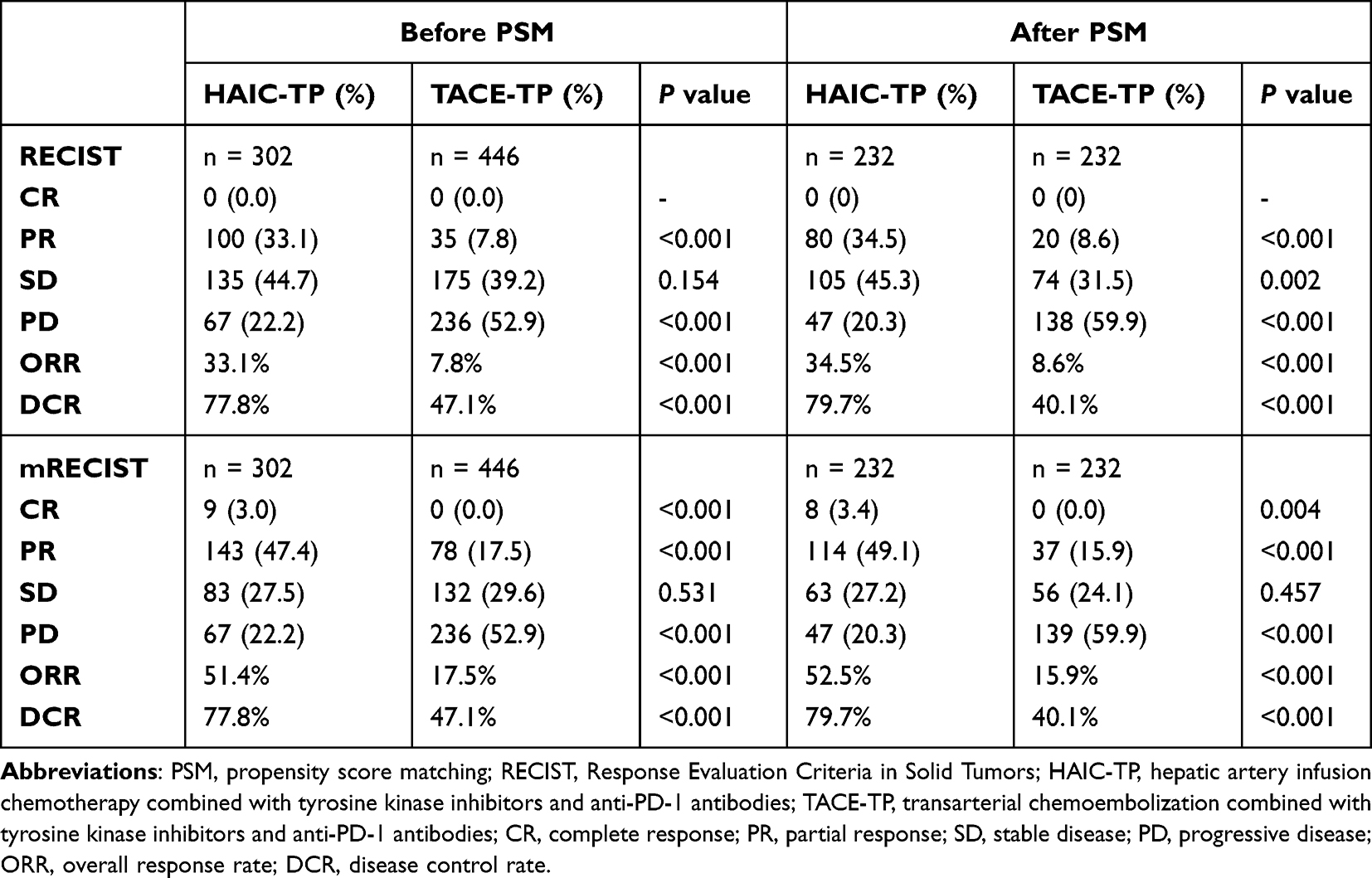 |
Table 2 Summary of Response Before and After PSM |
Survival Outcomes
The follow-up was completed in October 2022 and the median follow-up time was 14.4 months (4.4–23.7 months). The median PFS and OS of all patients was 9.9 months and 16.3 months, respectively. At the time of analysis, 128 patients (42.4%) exhibited disease progression and 52 (17.2%) had died in the HAIC-TP group; in the TACE-TP group, 236 patients (52.9%) exhibited disease progression and 153 (34.3%) had died. Before PSM, the median PFS and OS in the HAIC-TP group was 12.4 months and not reached, respectively, compared to 8.2 months and 13.8 months, respectively, in the TACE-TP group (P < 0.001; Figures 2A and B). After PSM, the median PFS and OS of the HAIC-TP group was 14.5 months and not reached, respectively, which was also significantly longer than that in the TACE-TP group (PFS: 6.8 months, OS: 12.4 months, P < 0.001; Figures 2C and D). Furthermore, subgroup analysis showed that, except for patients with single tumor or extrahepatic metastases, patients in the HAIC-TP group had a better prognosis than those in the TACE-TP group, either before PSM or after PSM (Figures 3 and 4).
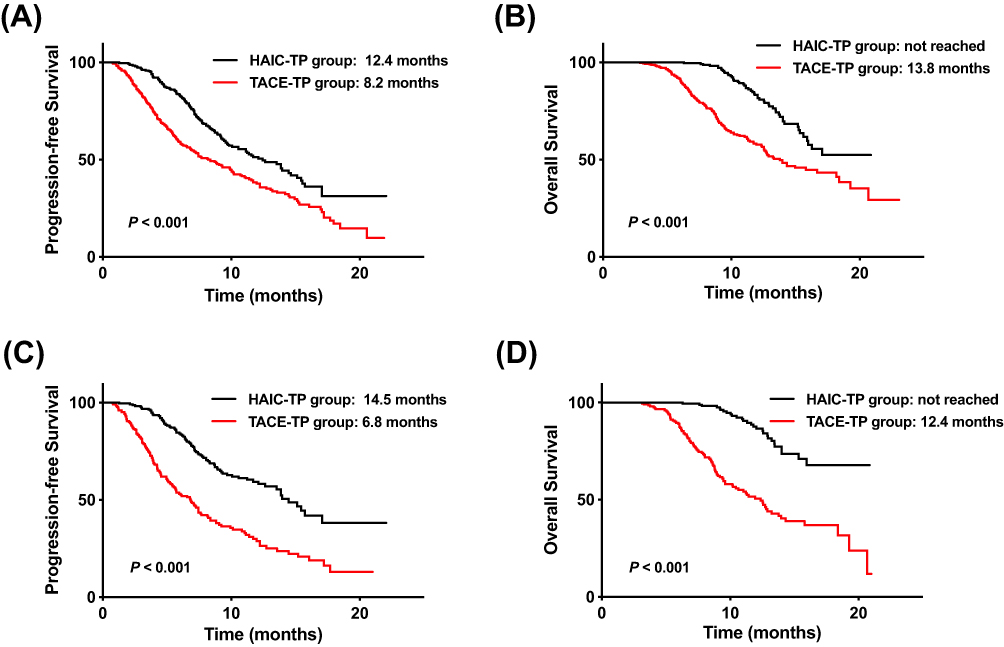 |
Figure 2 Kaplan-Meier curves for survival outcomes before and after PSM. Abbreviations: PSM, propensity score matching; PFS, progression-free survival; HAIC-TP, hepatic artery infusion chemotherapy combined with tyrosine kinase inhibitors and anti-PD-1 antibodies; TACE-TP, transarterial chemoembolization combined with tyrosine kinase inhibitor and anti-PD-1 antibodies; OS, overall survival. Notes: (A) Kaplan-Meier curves of PFS between HAIC-TP group and TACE-TP group before PSM. (B) Kaplan-Meier curves of OS between HAIC-TP group and TACE-TP group before PSM. (C) Kaplan-Meier curves of PFS between HAIC-TP group and TACE-TP group after PSM. (D) Kaplan-Meier curves of OS between HAIC-TP group and TACE-TP group after PSM. |
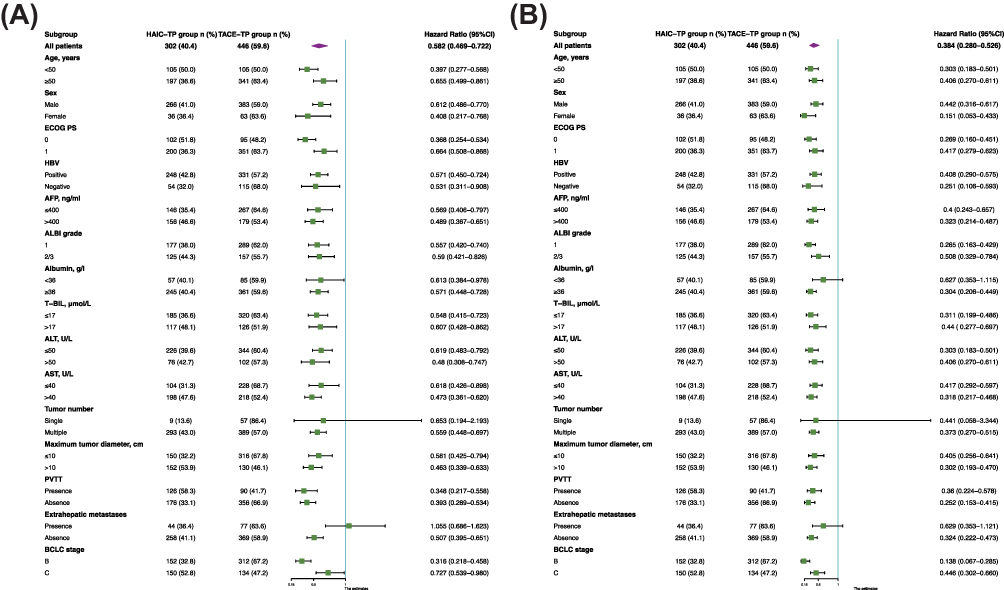 |
Figure 3 Subgroup analyses of survival outcomes before PSM. Abbreviations: PSM, propensity score matching; PFS, progression-free survival; HAIC-TP, hepatic arterial infusion chemotherapy combined with tyrosine kinase inhibitors and anti-PD-1 antibodies; TACE-TP, transarterial chemoembolization combined with tyrosine kinase inhibitors and anti-PD-1 antibodies; OS, overall survival; ECOG PS, Eastern Cooperative Oncology Group performance status; HBV, hepatitis B virus; AFP, alpha-fetoprotein; ALBI, albumin-bilirubin; T-BIL, total bilirubin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; PVTT, portal vein tumor thrombus; BCLC stage, Barcelona Clinic Liver Cancer stage. Notes: (A) Forest plots for subgroup analyses of PFS between HAIC-TP group and TACE-TP group. (B) Forest plots for subgroup analyses of OS between HAIC-TP group and TACE-TP group. |
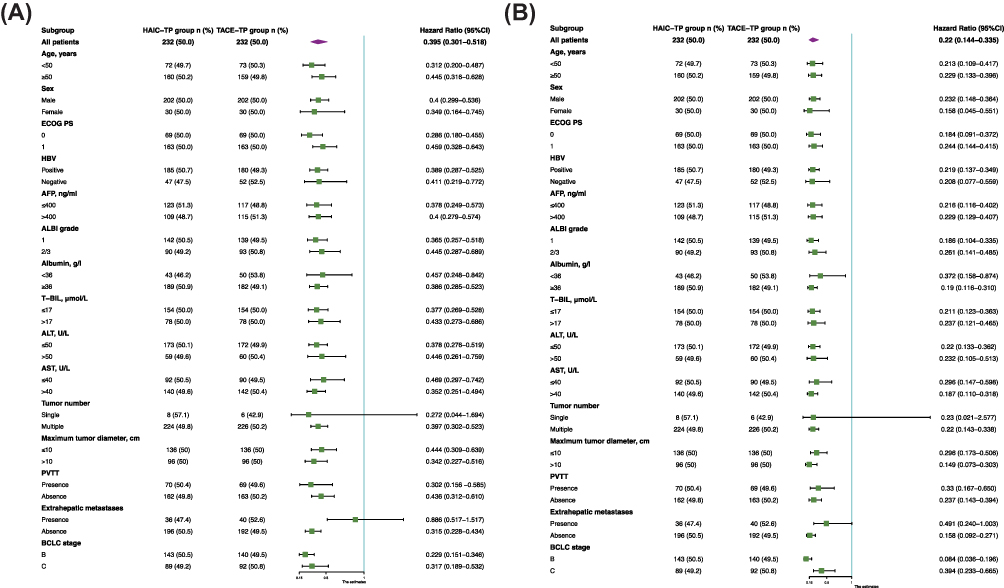 |
Figure 4 Subgroup analyses of survival outcomes after PSM. Abbreviations: PSM, propensity score matching; PFS, progression-free survival; HAIC-TP, hepatic arterial infusion chemotherapy combined with tyrosine kinase inhibitors and anti-PD-1 antibodies; TACE-TP, transarterial chemoembolization combined with tyrosine kinase inhibitors and anti-PD-1 antibodies; OS, overall survival; ECOG PS, Eastern Cooperative Oncology Group performance status; HBV, hepatitis B virus; AFP, alpha-fetoprotein; ALBI, albumin-bilirubin; T-BIL, total bilirubin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; PVTT, portal vein tumor thrombus; BCLC stage, Barcelona Clinic Liver Cancer stage. Notes: (A) Forest plots for subgroup analyses of PFS between HAIC-TP group and TACE-TP group. (B) Forest plots for subgroup analyses of OS between HAIC-TP group and TACE-TP group. |
Univariate and Multivariate Analysis of Survival
The results of the univariate and multivariate analyses of PFS and OS are presented in Table 3 and 4, respectively. Multivariate analysis demonstrated that the independent risk factors for PFS were type of treatment (HAIC-TP vs TACE-TP, HR: 2.173, 95% CI: 1.720–2.744; P < 0.001), AFP (≤ 400 ng/mL vs > 400 ng/mL, HR: 1.480, 95% CI: 1.181–1.856; P < 0.001), PVTT (presence vs absence, HR: 0.740, 95% CI: 0.581–0.942; P = 0.015), and extrahepatic metastases (HR: 0.653, 95% CI: 0.507–0.842; P = 0.001). Multivariate analysis for OS showed that type of treatment (HAIC-TP vs TACE-TP, HR: 3.333, 95% CI: 2.391–4.645; P < 0.001), AFP (≤ 400 ng/mL vs > 400 ng/mL, HR: 1.457, 95% CI: 1.088–1.951; P = 0.012), ALBI grade (1 vs 2/3, HR: 1.387, 95% CI: 1.045–1.839; P = 0.023), PVTT (presence vs absence, HR: 0.593, 95% CI: 0.431–0.816; P = 0.001), and extrahepatic metastases (presence vs absence, HR: 0.693, 95% CI: 0.502–0.958; P = 0.027) were prognostic factors.
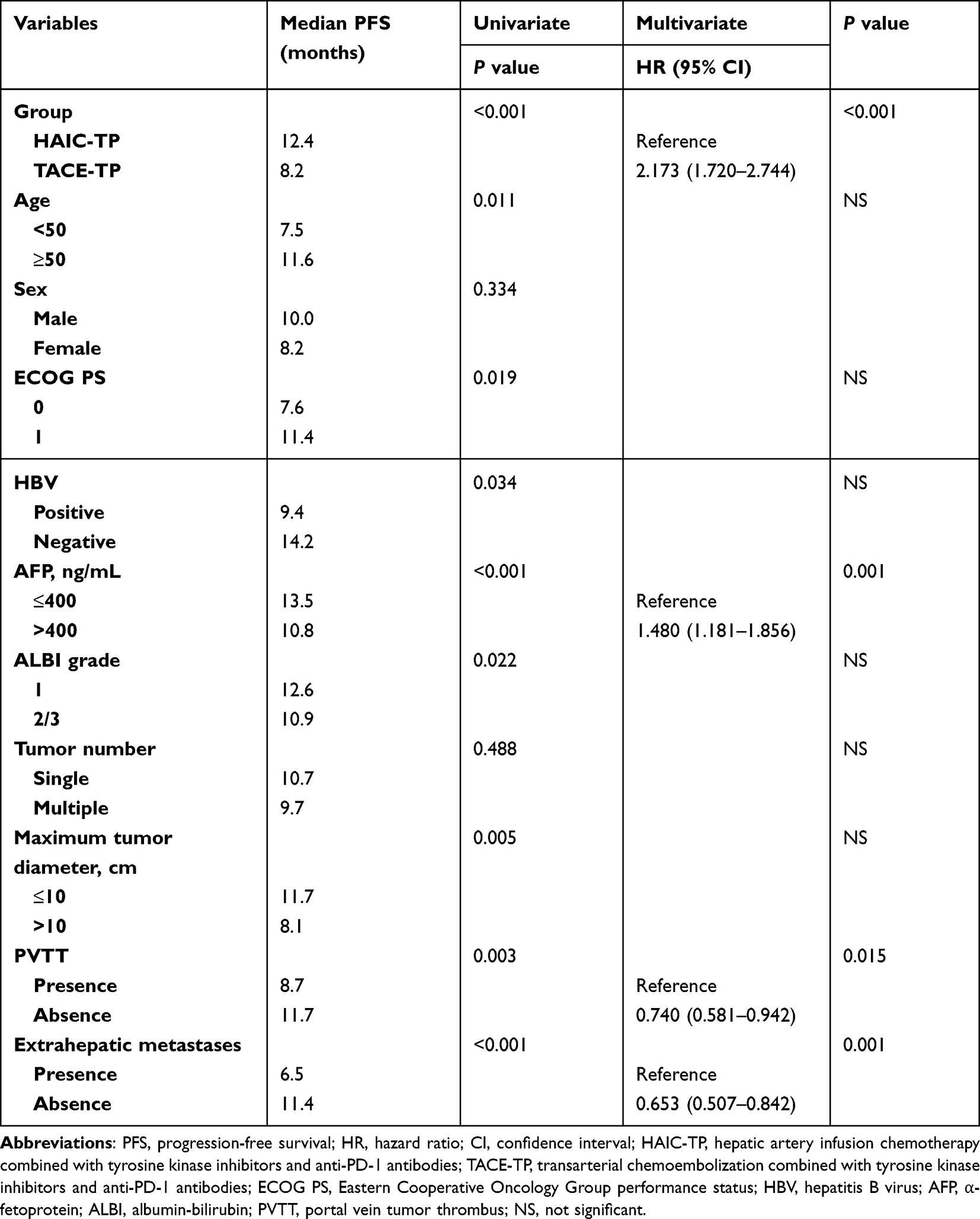 |
Table 3 Univariate and Multivariate Analysis of Progression-Free Survival in All Patients |
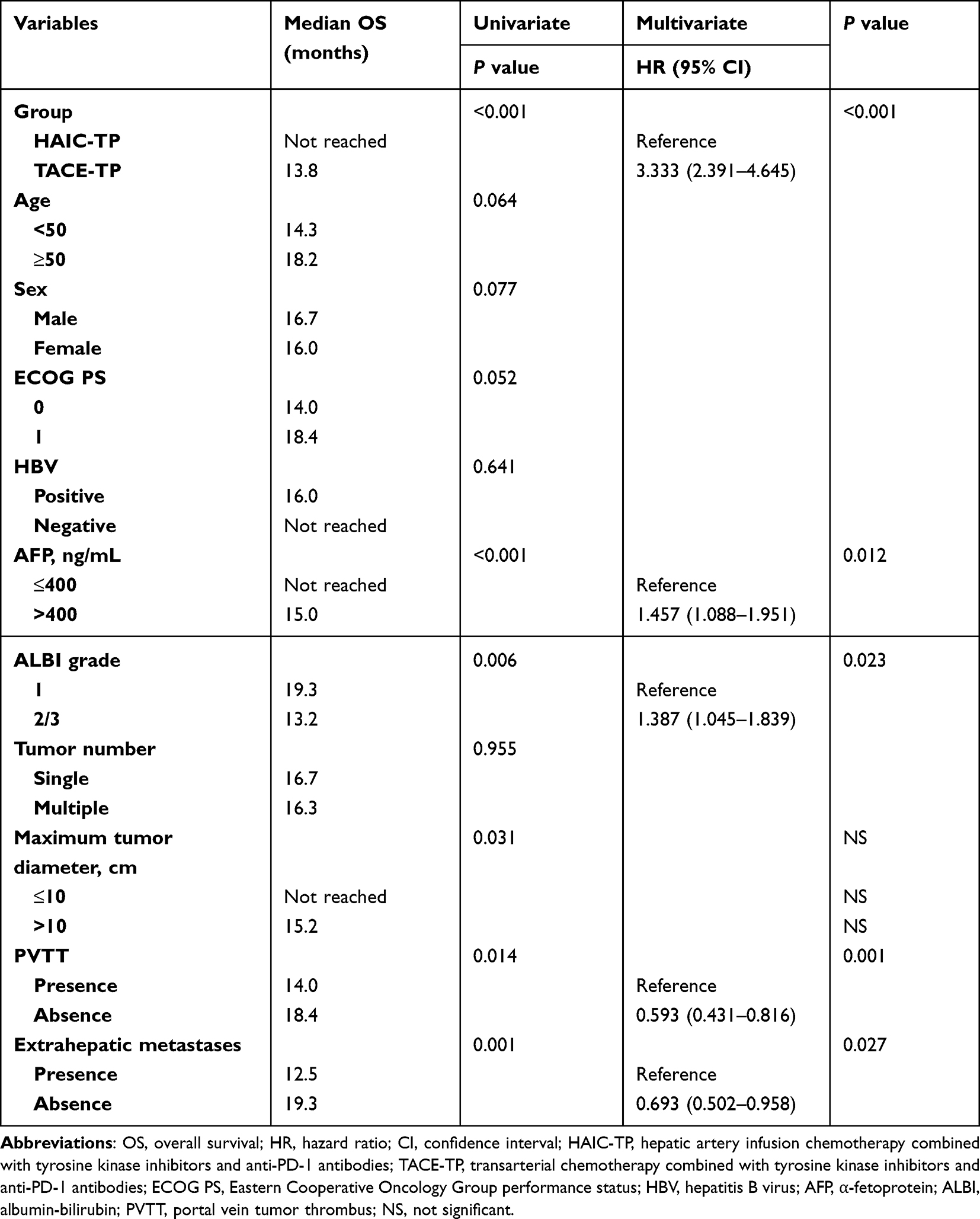 |
Table 4 Univariate and Multivariate Analysis of Overall Survival in All Patients |
Safety
No treatment-related deaths were observed in either group, and treatment-related AEs are listed in Table 5. Any grade of nausea (46.4% vs 34.3%, P = 0.001), vomiting (28.1% vs 21.5%, P = 0.047), diarrhea (25.2% vs 13.2%, P < 0.001), or abdominal pain (33.1% vs 23.8%, P = 0.006) occurred more frequently in the HAIC-TP group than in the TACE-TP group. Furthermore, more patients in the HAIC-TP group exhibited grade 3/4 diarrhea (4.3% vs 1.1%, P = 0.011) and grade 3/4 abdominal pain (5.6% vs 2.5%, P = 0.041) than those in the TACE-TP group. Any grade and grade 3/4 liver dysfunction, including elevated ALT, AST, hyperbilirubinemia, and hypoalbuminemia, were less frequent in the HAIC-TP group than in the TACE-TP group. Fever was less frequent in the HAIC-TP group than in the TACE-TP group (15.2% vs 34.8%, P < 0.001).
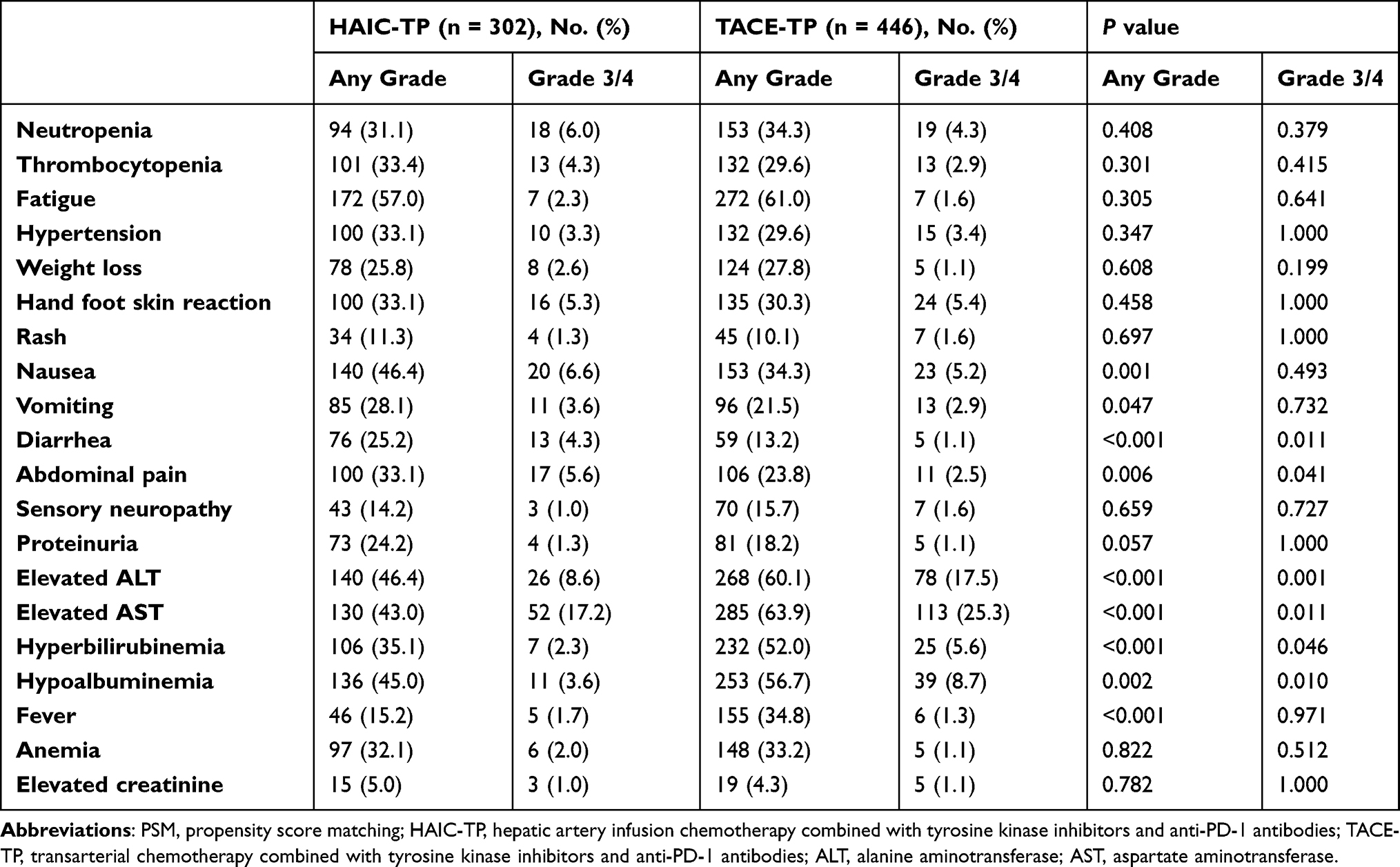 |
Table 5 Treatment-Related Adverse Events in All Patients |
Discussion
This retrospective study was the first to compare the clinicopathological characteristics and prognosis of patients treated with TKIs, anti-PD-1 antibodies, HAIC or TACE. We obtained primary evidence of the superiority of HAIC combined with TKIs and anti-PD-1 antibodies over TACE combined with TKIs and anti-PD-1 antibodies in the treatment of HCC. A clinical trial compared HAIC with TACE in the treatment of massive unresectable HCC and demonstrated that HAIC yielded a significantly better treatment response, better survival outcomes, and fewer AEs than TACE.4 In the current study, patients receiving HAIC combined with TKIs and anti-PD-1 antibodies also had a better tumor response and prognosis than those receiving a combination of TACE with TKIs and anti-PD-1 antibodies. A possible reason for this is that the continuous infusion of chemotherapeutic agents in HAIC can provide stable, local, and high concentrations of agents in tumors, and thus HAIC can promote the anti-tumor effects of TKIs and anti-PD-1 inhibitors better than TACE.4,16,17 Another possible reason is that tumor hypoxia induced by TACE can lead to the upregulation of hypoxia inducible factor-1 ⍺ (HIF-1⍺), which activates the proangiogenic response, including upregulation of the expression of vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF), and thus increase tumor angiogenesis and influence local tumor recurrence.18–21 Moreover, liver resection was performed more frequently in the HAIC-TP group than in the TACE-TP group. This result not only demonstrated HAIC-based combination therapy exhibited better efficacy than TACE-based combination therapy but is the reason that longer PFS and OS were observed in patients of the HAIC-TP group compared to the TACE-TP group.
In our study, the median PFS and OS of all patients was 9.9 months and 16.3 months, respectively, which is comparable to the survival outcomes of previous studies, with a median PFS of 4.0–16.3 months and a median OS of 8.6–24.8 months, respectively.7,8,10,22,23 In the HAIC-TP group, the median PFS was 12.4 months, which was numerically better than the 10.4 months reported in a clinical trial on Lenvatinib, Toripalimab, and HAIC.11 This difference in survival may be because patients in the current study were at earlier disease stages than those in previous clinical trial. For example, in a previous clinical trial 86.1% of patients had PVTT and 27.8% had extrahepatic metastases, compared to 41.7% and 14.6% of patients, respectively, in our study.11
To reduce the bias caused by confounding variables, PSM analysis was performed, and the same results were observed, thus substantiating the credibility of these findings.24 In addition, we performed subgroup analyses based on different clinicopathological characteristics. HAIC has a better prognosis than TACE when combined with TKIs and anti-PD-1 antibodies in most subgroups. However, for patients with single tumor, similar prognoses were observed in the HAIC-TP and TACE-TP groups. These results might be explained by the limited number of cases in the subgroup analyses. Furthermore, no significant difference in prognosis was observed in patients with extrahepatic metastases who were treated with TKIs, anti-PD-1 antibodies plus HAIC or TACE. This result indicated that when patients presented extrahepatic metastases, it was systemic treatment, instead of locoregional treatment, that played a vital role in treatment efficacy and survival outcomes.
In multivariate analysis, treatment method was a prognostic factor for survival outcomes, which further indicated that the HAIC-TP group exhibited better therapeutic efficacy than the TACE-TP group. Serum AFP levels have been shown to have both diagnostic and prognostic value in HCC.25,26 A better prognosis was observed among Asian patients with AFP > 200 ng/mL in the Check-Mate 45927 and KEYNOTE-240 trials.28 In our study, AFP level was also a prognostic factor for survival in patients with HCC, and AFP ≤ 400 ng/mL was associated with better survival outcomes. The same conclusion was reported by the study of He et al,12 which compared the efficacy of lenvatinib, toripalimab, and HAIC with lenvatinib alone for advanced HCC. The ALBI grade, based on albumin and bilirubin, is an index of liver dysfunction and a significant predictor of OS in patients with HCC after surgery, TACE and sorafenib.29,30 Our study revealed that ALBI grade was associated with OS in patients treated with a combination of interventional therapy, TKIs, and anti-PD-1 antibodies. In addition, we identified the prognostic significance of PVTT and extrahepatic metastases. Therefore, both tumor burden and tumor stage play important roles in survival outcomes in patients with HCC receiving HAIC- or TACE-based combination therapies. Further studies are required to confirm these findings.
TACE has been reported to be associated with more serious AEs than HAIC in HCC.4,31 In a previous systematic review, elevated ALT or AST levels were the most common AEs associated with combination therapy in the form of interventional therapy and TKIs plus anti-PD-1 antibodies.22 This result, as well as hyperbilirubinemia and hypoalbuminemia, was also observed in our study. Patients in the TACE-TP group had worse liver function than those in the HAIC-TP group after combination therapy. This indicates that liver function should be a selection criterion for patients who plan to receive combination therapy, especially for those who are treated with TACE-based combination therapy. Because of the continuous infusion of chemotherapeutic agents, patients in the HAIC-TP group had significantly higher frequencies of nausea, vomiting, diarrhea, and abdominal pain. Thus, it may be appropriate to administer antiemetic agents before the infusion of chemotherapeutic agents and also to use painkillers and reduce the oxaliplatin dose when patients experience abdominal pain. Moreover, owing to embolization with iodized oil in the TACE procedure, more patients in the TACE-TP group experienced fever. Notably, the above-mentioned treatment-related AEs were acceptable and manageable by means of treatment interruption or dose modification.
This study had several limitations. First, the retrospective design of the study makes it prone to various biases. Despite the insignificant differences in the baseline characteristics after PSM, other unrecognized confounders may still exist. Second, the patients were treated with various TKIs and anti-PD-1 antibodies, and it was difficult to compare their therapeutic efficacy and AEs in patients receiving combination therapy based on the same TKIs and anti-PD-1 antibodies. Finally, the follow-up time was relatively short and an insufficient number of OS events were observed. Considering these limitations, more multicenter and large-scale clinical trials are needed to explore the role of a combination of TKIs and anti-PD-1 antibodies with HAIC or TACE in HCC treatment.
Conclusion
In summary, our retrospective study showed that, for patients with HCC, the combination of HAIC with TKIs and anti-PD-1 antibodies was an effective and safe therapeutic regimen, with better treatment responses, better survival outcomes, and acceptable AEs compared to TACE-based combination therapy. In addition to treatment type, AFP level, ALBI grade, PVTT, and extrahepatic metastases were the most significant predictors associated with the prognosis of patients with HCC. Further studies are needed to verify the conclusions.
Data Sharing Statement
Data from the current study are available from the corresponding author upon reasonable request.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Fudan University Shanghai Cancer Center.
Informed Consent
Written informed consent was obtained from all patients before they were included in the study.
Funding
This work was jointly supported by the National Natural Science Foundation of China (81874182), National Science and Technology Major Project (2018ZX10723204-007-004), Shanghai Municipal Health Bureau (201940043), and the Shanghai Hospital Development Center (SHDC12019X19).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6. doi:10.1038/s41572-020-00240-3
2. Villanueva A. Hepatocellular Carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
3. Nakano M, Niizeki T, Nagamatsu H, et al. Clinical effects and safety of intra-arterial infusion therapy of cisplatin suspension in lipiodol combined with 5-fluorouracil versus sorafenib, for advanced hepatocellular carcinoma with macroscopic vascular invasion without extra-hepatic spread: a prospective cohort study. Mol Clin Oncol. 2017;7(6):1013–1020. doi:10.3892/mco.2017.1442
4. Li QJ, He MK, Chen HW, et al. Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin Versus Transarterial Chemoembolization for Large Hepatocellular Carcinoma: a Randomized Phase III Trial. J Clin Oncol. 2021:JCO2100608. doi:10.1200/JCO.21.00608
5. Chang Y, Jeong SW, Young Jang J, Jae Kim Y. Recent Updates of Transarterial Chemoembolilzation in Hepatocellular Carcinoma. Int J Mol Sci. 2020;21(21). doi:10.3390/ijms21218165
6. Zhang T, Merle P, Wang H, Zhao H, Kudo M. Combination therapy for advanced hepatocellular carcinoma: do we see the light at the end of the tunnel? Hepatobiliary Surg Nutr. 2021;10(2):180–192. doi:10.21037/hbsn-2021-7
7. Wu JY, Yin ZY, Bai YN, et al. Lenvatinib Combined with Anti-PD-1 Antibodies Plus Transcatheter Arterial Chemoembolization for Unresectable Hepatocellular Carcinoma: a Multicenter Retrospective Study. J Hepatocell Carcinoma. 2021;8:1233–1240. doi:10.2147/JHC.S332420
8. Yang F, Xu GL, Huang JT, et al. Transarterial Chemoembolization Combined With Immune Checkpoint Inhibitors and Tyrosine Kinase Inhibitors for Unresectable Hepatocellular Carcinoma: efficacy and Systemic Immune Response. Front Immunol. 2022;13:847601. doi:10.3389/fimmu.2022.847601
9. Ju S, Zhou C, Yang C, et al. Apatinib Plus Camrelizumab With/Without Chemoembolization for Hepatocellular Carcinoma: a Real-World Experience of a Single Center. Front Oncol. 2021;11:835889. doi:10.3389/fonc.2021.835889
10. Cao F, Yang Y, Si T, et al. The Efficacy of TACE Combined With Lenvatinib Plus Sintilimab in Unresectable Hepatocellular Carcinoma: a Multicenter Retrospective Study. Front Oncol. 2021;11:783480. doi:10.3389/fonc.2021.783480
11. Lai Z, He M, Bu X, et al. Lenvatinib, toripalimab plus hepatic arterial infusion chemotherapy in patients with high-risk advanced hepatocellular carcinoma: a biomolecular exploratory, Phase II trial. Eur J Cancer. 2022;174:68–77. doi:10.1016/j.ejca.2022.07.005
12. He MK, Liang RB, Zhao Y, et al. Lenvatinib, toripalimab, plus hepatic arterial infusion chemotherapy versus lenvatinib alone for advanced hepatocellular carcinoma. Ther Adv Med Oncol. 2021;13:17588359211002720. doi:10.1177/17588359211002720
13. Mei J, Tang YH, Wei W, et al. Hepatic Arterial Infusion Chemotherapy Combined With PD-1 Inhibitors Plus Lenvatinib Versus PD-1 Inhibitors Plus Lenvatinib for Advanced Hepatocellular Carcinoma. Front Oncol. 2021;11:618206. doi:10.3389/fonc.2021.618206
14. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
15. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
16. Lyu N, Kong Y, Mu L, et al. Hepatic arterial infusion of oxaliplatin plus fluorouracil/leucovorin vs. sorafenib for advanced hepatocellular carcinoma. J Hepatol. 2018;69(1):60–69. doi:10.1016/j.jhep.2018.02.008
17. Si T, Huang Z, Khorsandi SE, Ma Y, Heaton N. Hepatic arterial infusion chemotherapy versus transarterial chemoembolization for unresectable hepatocellular carcinoma: a systematic review with meta-analysis. Front Bioeng Biotechnol. 2022;10:1010824. doi:10.3389/fbioe.2022.1010824
18. Liu K, Min XL, Peng J, Yang K, Yang L, Zhang XM. The Changes of HIF-1alpha and VEGF Expression After TACE in Patients With Hepatocellular Carcinoma. J Clin Med Res. 2016;8(4):297–302. doi:10.14740/jocmr2496w
19. Wang B, Xu H, Gao ZQ, Ning HF, Sun YQ, Cao GW. Increased expression of vascular endothelial growth factor in hepatocellular carcinoma after transcatheter arterial chemoembolization. Acta Radiol. 2008;49(5):523–529. doi:10.1080/02841850801958890
20. Li X, Feng G-S, Zheng C-S, Zhuo C-K, Liu X. Expression of plasma vascular endothelial growth factor in patients with hepatocellular carcinoma and effect of transcatheter arterial chemoembolization therapy on plasma vascular endothelial growth factor level. World J Gastroenterol. 2004;10(19):2878–2882. doi:10.3748/wjg.v10.i19.2878
21. Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492–1501. doi:10.1136/gutjnl-2019-318934
22. Ke Q, Xin F, Fang H, Zeng Y, Wang L, Liu J. The Significance of Transarterial Chemo(Embolization) Combined With Tyrosine Kinase Inhibitors and Immune Checkpoint Inhibitors for Unresectable Hepatocellular Carcinoma in the Era of Systemic Therapy: a Systematic Review. Front Immunol. 2022;13:913464. doi:10.3389/fimmu.2022.913464
23. Chen S, Xu B, Wu Z, et al. Pembrolizumab plus lenvatinib with or without hepatic arterial infusion chemotherapy in selected populations of patients with treatment-naive unresectable hepatocellular carcinoma exhibiting PD-L1 staining: a multicenter retrospective study. BMC Cancer. 2021;21(1):1126. doi:10.1186/s12885-021-08858-6
24. Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10(2):150–161. doi:10.1002/pst.433
25. Munson PV, Adamik J, Butterfield LH. Immunomodulatory impact of alpha-fetoprotein. Trends Immunol. 2022;43(6):438–448. doi:10.1016/j.it.2022.04.001
26. He M, Li Q, Zou R, et al. Sorafenib Plus Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin vs Sorafenib Alone for Hepatocellular Carcinoma With Portal Vein Invasion: a Randomized Clinical Trial. JAMA Oncol. 2019;5(7):953–960. doi:10.1001/jamaoncol.2019.0250
27. Yau T, Park JW, Finn RS, et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, Phase 3 trial. Lancet Oncol. 2022;23(1):77–90. doi:10.1016/S1470-2045(21)00604-5
28. Finn RS, Ryoo BY, Merle P, et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: a Randomized, Double-Blind, Phase III Trial. J Clin Oncol. 2020;38(3):193–202. doi:10.1200/JCO.19.01307
29. Pinato DJ, Sharma R, Allara E, et al. The ALBI grade provides objective hepatic reserve estimation across each BCLC stage of hepatocellular carcinoma. J Hepatol. 2017;66(2):338–346. doi:10.1016/j.jhep.2016.09.008
30. Hansmann J, Evers MJ, Bui JT, et al. Albumin-Bilirubin and Platelet-Albumin-Bilirubin Grades Accurately Predict Overall Survival in High-Risk Patients Undergoing Conventional Transarterial Chemoembolization for Hepatocellular Carcinoma. J Vasc Interv Radiol. 2017;28(9):1224–1231 e2. doi:10.1016/j.jvir.2017.05.020
31. He MK, Le Y, Li QJ, et al. Hepatic artery infusion chemotherapy using mFOLFOX versus transarterial chemoembolization for massive unresectable hepatocellular carcinoma: a prospective non-randomized study. Chin J Cancer. 2017;36(1):83. doi:10.1186/s40880-017-0251-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.