Back to Journals » Drug Design, Development and Therapy » Volume 20
Sugammadex and Postoperative Respiratory Failure in Head and Neck Surgery: A Cohort Study
Authors Hung KC ![]() , Yu TS, Lai YC, Chen IW
, Yu TS, Lai YC, Chen IW ![]()
Received 8 November 2025
Accepted for publication 31 January 2026
Published 7 February 2026 Volume 2026:20 580072
DOI https://doi.org/10.2147/DDDT.S580072
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Kuo-Chuan Hung,1 Ting-Sian Yu,2 Yi-Chen Lai,1 I-Wen Chen3
1Department of Anesthesiology, Chi Mei Medical Center, Tainan City, Taiwan; 2Department of Anesthesiology, E-Da Hospital, I-Shou University, Kaohsiung City, Taiwan; 3Department of Anesthesiology, Chi Mei Medical Center, Liouying, Tainan City, Taiwan
Correspondence: I-Wen Chen, Department of Anesthesiology, Chi Mei Medical Center, Liouying, Tainan City, Taiwan, Tel +886-6-281-2811, Fax +886-6-283-3806, Email [email protected]
Purpose: This study investigated whether sugammadex use reduces postoperative acute respiratory failure compared with neostigmine use in patients undergoing head and neck free flap reconstruction, a population at high risk for pulmonary complications.
Patients and methods: We conducted a retrospective cohort study using the TriNetX Research Network database to identify adult patients with head and neck cancer who underwent flap reconstruction surgery between January 2016 and December 2024. The patients received either sugammadex or neostigmine for rocuronium reversal. The primary outcome was acute respiratory failure within 30 days of the surgery. The secondary outcomes included composite pulmonary complications, intensive care unit (ICU) admission, major adverse cardiovascular events (MACEs), and flap failure.
Results: After propensity score matching, the analysis included 2576 patients, with 1288 patients in each group. Sugammadex use was associated with significantly lower acute respiratory failure at 30 days compared with neostigmine (hazard ratio [HR] 0.67, 95% confidence interval [CI] 0.50– 0.88, p=0.004), with persistent benefit at 90 days (HR 0.76, 95% CI 0.59– 0.99, p=0.042). Multivariate analysis confirmed that sugammadex was an independent protective factor (HR 0.61, p< 0.001). Independent risk factors included ischemic heart disease, anemia, nicotine dependence, and advanced age. No differences were observed in the other outcomes.
Conclusion: Sugammadex is the preferred neuromuscular blockade reversal strategy in head and neck flap reconstruction, offering improved respiratory safety without compromising surgical outcomes. Future prospective studies are warranted to confirm these findings and clarify their implications for perioperative management.
Keywords: sugammadex, neuromuscular blockade reversal, head and neck surgery, respiratory failure, free flap reconstruction, neostigmine
Introduction
Head and neck free flap reconstruction carries substantial respiratory morbidity, with postoperative pulmonary complications occurring in 18.8–32.7% of patients.1–3 These procedures are particularly high-risk due to prolonged surgical duration, extensive airway manipulation, tumor involvement of the aerodigestive tract, and the potential for postoperative edema compromising upper airway patency.4–6 Multiple studies have identified risk factors for postoperative pulmonary complications including advanced age, malnutrition, tumor stage, ASA >2, smoking, higher body mass index (BMI), prolonged surgery, and comorbidity burden,1,3,7–9 yet modifiable intraoperative factors remain underexplored. Residual neuromuscular blockade represents a modifiable risk factor for respiratory complications, impairing protective airway reflexes, pharyngeal muscle coordination, and effective cough, thereby increasing aspiration risk and respiratory failure.10–13 Traditional neostigmine reversal has important limitations, including incomplete reversal at deep blockade levels, parasympathetic side effects requiring anticholinergic co-administration, and variable efficacy dependent on spontaneous recovery. Sugammadex, a modified γ-cyclodextrin that directly encapsulates rocuronium molecules, provides rapid and predictable reversal regardless of the blockade depth.14–16
Emerging evidence suggests that sugammadex may reduce postoperative pulmonary complications beyond simply reversing neuromuscular blockade. The multicenter STRONGER study17 involving 45,712 patients demonstrated a 47% reduction in pneumonia and a 55% reduction in respiratory failure compared with neostigmine. A recent systematic review and meta-analysis including 28 studies confirmed that sugammadex is superior to neostigmine in reducing postoperative pulmonary complications, particularly pneumonia, reintubation, and the need for noninvasive ventilation.18 A recent study of COVID-19 patients undergoing thoracic surgery showed significantly lower respiratory failure rates with sugammadex (1.42% vs 3.25%).19 However, conflicting data exist, with a large single-center analysis finding no difference in pulmonary complications, highlighting the need for investigation in specific high-risk populations.20
Critically, no studies have examined the effects of sugammadex on respiratory outcomes, specifically in head and neck flap reconstruction—a uniquely vulnerable cohort whose risk profile warrants dedicated investigation. We therefore conducted this large-scale retrospective study to determine whether sugammadex use reduces the risk of pulmonary complications following head and neck flap reconstruction and to identify independent predictors of this complication.
Methods
Study Design and Data Source
We conducted a retrospective cohort study drawing on electronic health records from the TriNetX Research Network, a global federated platform that synthesizes de-identified patient data from healthcare organizations across multiple countries.21 This platform provided access to comprehensive clinical information, including patient diagnoses documented according to the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), procedural records captured through Current Procedural Terminology (CPT) codes, laboratory measurements, and medication administration data. The TriNetX platform has been extensively applied in both surgical and non-surgical research.22–24 Our study protocol was reviewed and approved by the Institutional Review Board of the Chi Mei Medical Center (Protocol No. 11403-E03). Given that only de-identified retrospective data were analyzed, with no patient contact or intervention, the board waived the requirement for informed consent.
Study Population
We examined adult patients (≥18 years) with head and neck cancer who underwent flap reconstruction surgery between January 1, 2016, and December 31, 2024. Eligible cases were limited to those in which rocuronium was used as the primary neuromuscular blocking agent, and surgical procedures were identified using validated CPT codes for flap reconstruction. The date of surgery was defined as the index date and served as a reference for all outcome assessments. Patients were classified according to the intraoperative reversal agent: the sugammadex group consisted of patients who received sugammadex and the control group consisted of patients who received neostigmine. This design enabled the evaluation of whether the choice of reversal agent affected postoperative respiratory outcomes.
Exclusion Criteria
To minimize confounding and ensure comparability between groups, we excluded patients with recent respiratory or infectious illnesses within one month before surgery. These conditions included pneumonia (J12–J18), pulmonary edema (J81), sepsis (A41), respiratory failure (J96), atelectasis (J98.11), and COVID-19 (U07.1). Patients with an existing tracheostomy (Z93.0) or those who had previously received critical care services were also excluded because such factors could independently influence postoperative pulmonary outcomes. In addition, individuals with neuromuscular junction or muscle diseases (G70–G73) were excluded because these disorders may alter responses to neuromuscular blocking and reversal agents. To maintain a uniform elective surgical cohort, emergency operations were excluded.
Propensity Score Matching and Data Collection
We extracted comprehensive baseline data for all eligible patients from the TriNetX database, covering the two-year period preceding each patient’s index surgery. This window captured chronic conditions, laboratory trends, and healthcare utilization relevant to treatment selection and outcomes. To minimize the confounding inherent in observational research, we applied propensity score matching to approximate randomization. Propensity scores were generated using multivariate logistic regression that included clinically relevant variables such as age, sex, race, body mass index, comorbidities, and laboratory values. Each score represents the likelihood of receiving sugammadex versus neostigmine based on baseline characteristics. Patients were matched one-to-one using a greedy nearest-neighbor algorithm without replacement, ensuring each individual contributed to a single pair. Matching quality was assessed by standardized mean differences (<0.1 indicating balance) and visual inspection of propensity score density plots, confirming comparable baseline distributions between groups.
Outcome Assessment
We defined acute respiratory failure within 30 days postoperatively as the primary outcome, given the prolonged operative time, airway manipulation, and anatomic disruption inherent to head and neck flap reconstruction. The secondary outcomes included composite pulmonary complications (pneumonia, aspiration pneumonia, or pulmonary edema), intensive care unit (ICU) admission, major adverse cardiovascular events (MACE: cardiac arrest, myocardial infarction, or cerebral infarction), and flap failure requiring reoperation. Acute respiratory failure was identified using specific ICD-10-CM diagnosis codes (J96.0), which are detailed in supplementary material 1 together with all codes used for cohort definition, exposure, and outcomes. To capture both early and delayed events, outcomes were assessed at 30-day and 90-day intervals, distinguishing perioperative complications from those arising during recovery.
Statistical Analysis
Baseline characteristics were summarized using descriptive statistics: means with standard deviations for continuous variables and counts with percentages for categorical variables. To evaluate outcome timing and probability, we applied Kaplan–Meier survival analysis, which accommodates time-to-event data and variable follow-up durations. Survival curves were compared using Log rank tests to assess statistical differences between the groups. Associations between sugammadex exposure and outcomes were quantified using Cox proportional hazards regression, yielding hazard ratios (HRs) with 95% confidence intervals. For the primary outcome of acute respiratory failure, multivariable Cox models were constructed to adjust for clinically relevant covariates and identify independent predictors. Model assumptions were verified using Schoenfeld residuals to confirm proportionality. Statistical significance was set at a two-sided α value of 0.05. All analyses were performed using TriNetX integrated statistical tools to ensure methodological consistency and reproducibility.
Results
Patient Selection and Baseline Characteristics
From the TriNetX database, we identified 14,988 eligible patients with head and neck cancer who underwent flap reconstruction surgery. After applying the exclusion criteria, the initial cohort comprised 4017 patients (75.3%) who received sugammadex and 1316 (24.7%) who received neostigmine for neuromuscular blockade reversal (Figure 1). After applying 1:1 propensity score matching, the final analysis included 2576 patients, with 1288 patients in each group.
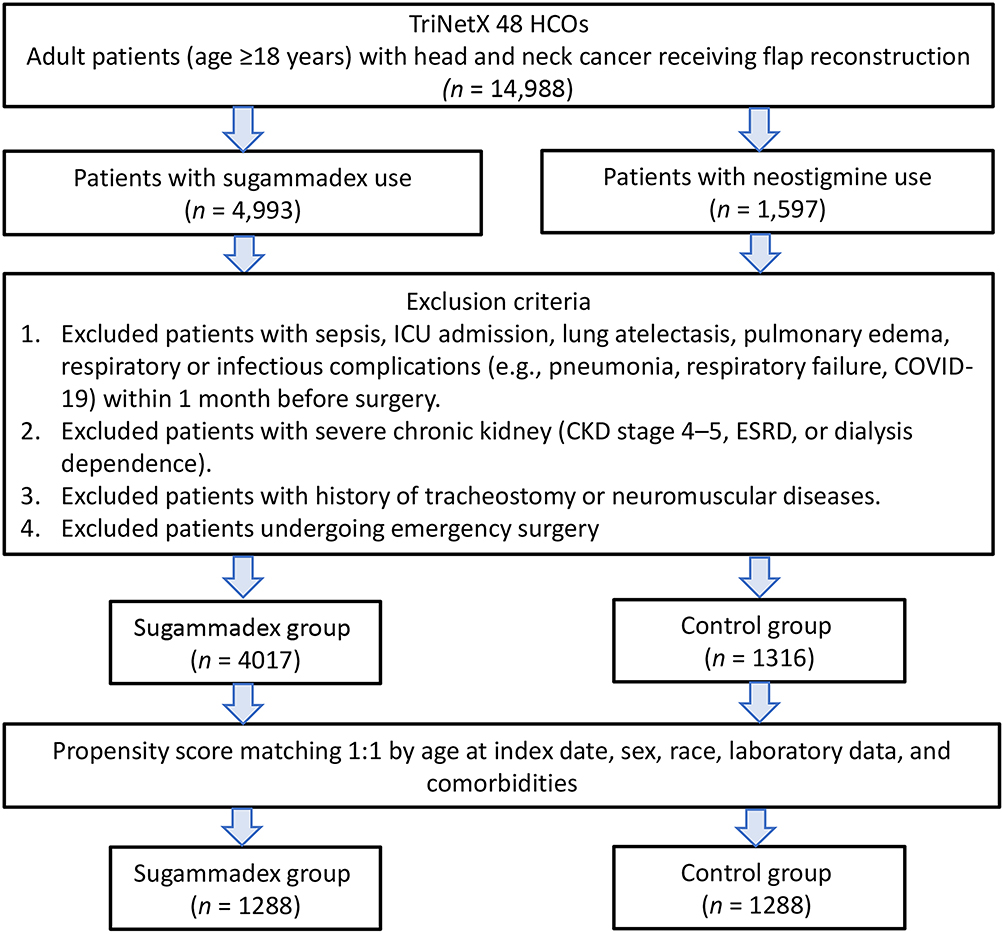 |
Figure 1 Patient selection flowchart from the TriNetX database. Abbreviations: HCOs, Healthcare Organizations; CKD, chronic kidney disease; ESRD, End-Stage Renal Disease. |
Prior to matching, the sugammadex group demonstrated several baseline differences compared to the control group, including higher mean age (63.8±11.7 vs 62.4±11.6 years, SMD=0.119), lower proportion of White patients (77.5% vs 83.1%, SMD=0.141), higher rates of malnutrition (13.6% vs 10.3%, SMD=0.104), and higher proportion with eGFR >60 mL/min/1.73m2 (70.8% vs 62.5%, SMD=0.178). Following propensity score matching, all baseline characteristics were well-balanced between groups, with standardized mean differences less than 0.1 for all variables (Table 1). After matching, both cohorts were well balanced in terms of demographics (mean age 62.5 years, with roughly one-third female), comorbidity burden, and laboratory findings. The propensity score distributions showed substantial improvement in overlap after matching, confirming a successful covariate balance (Figure 2).
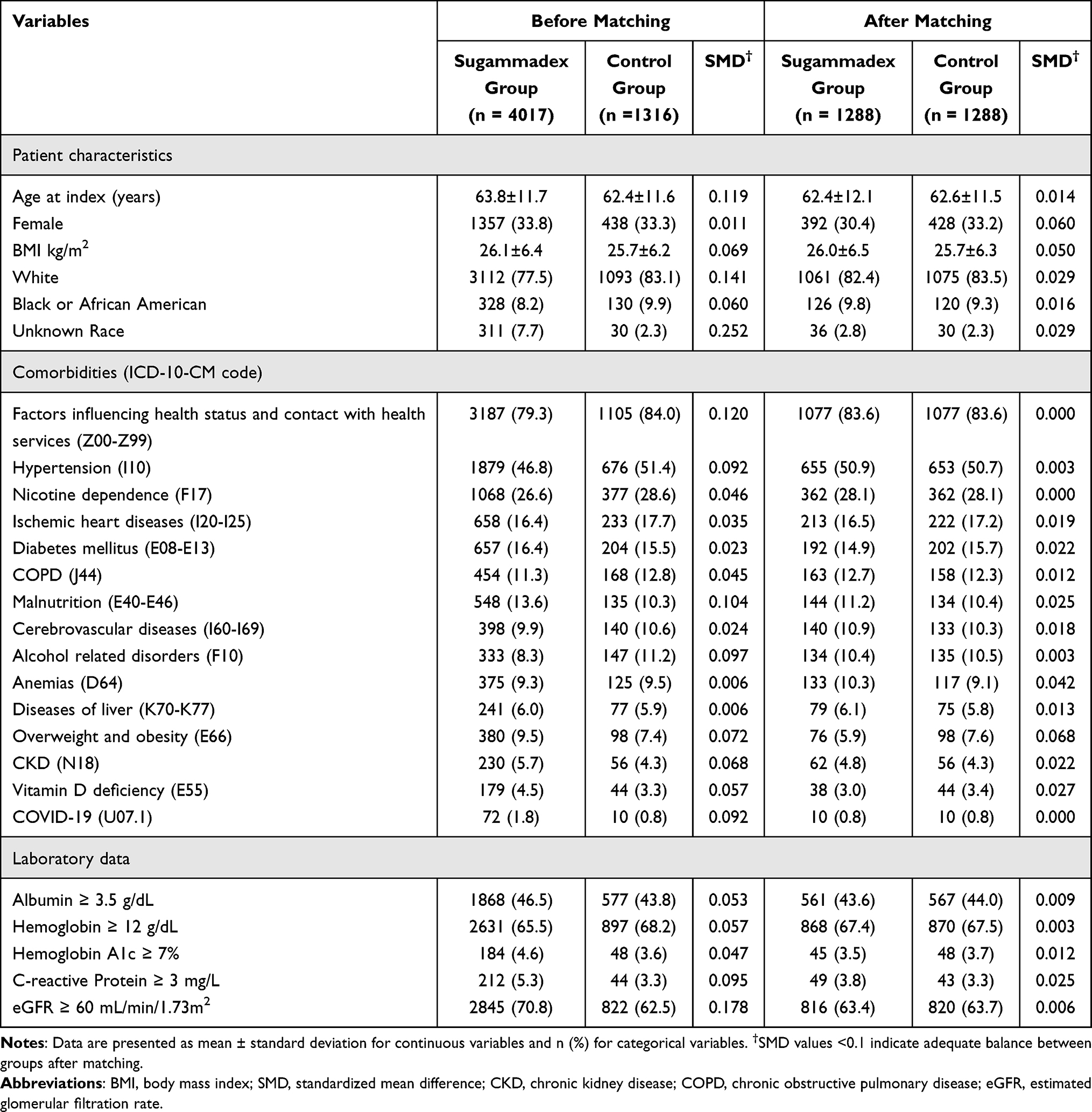 |
Table 1 Baseline Characteristics of Patients Before and After Propensity Score Matching |
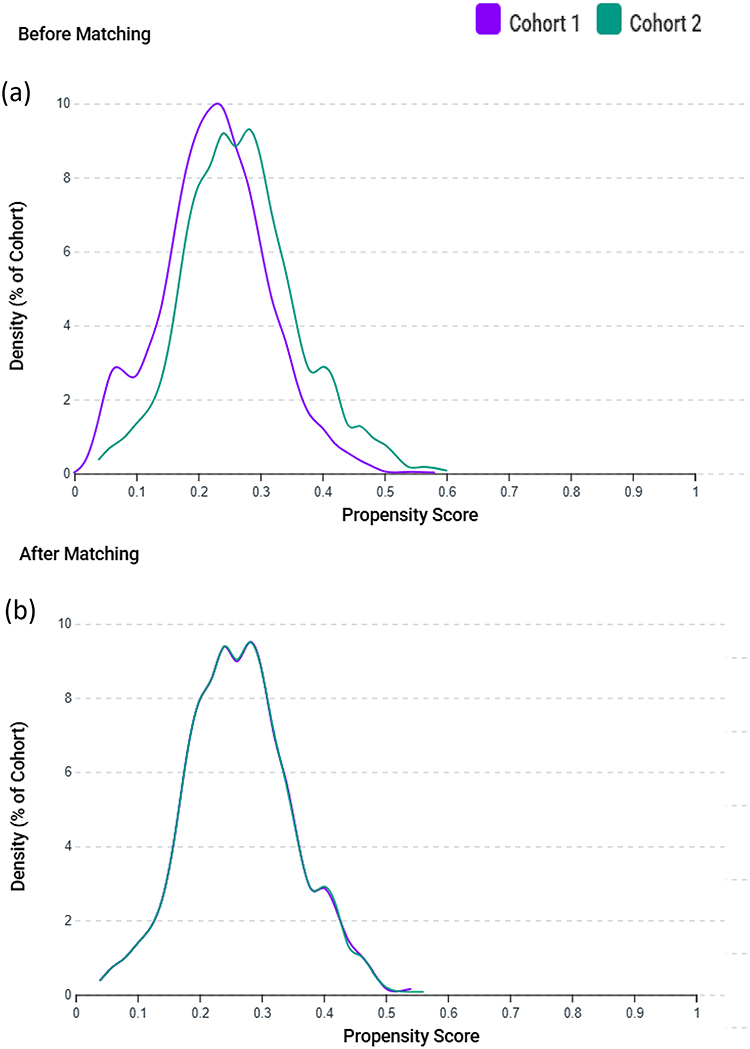 |
Figure 2 Propensity score distributions before and after matching. (a) Distribution of propensity scores between the sugammadex group (Cohort 1, purple) and the control group (Cohort 2, green) prior to matching, demonstrating an imbalance between cohorts. (b) Distribution of propensity scores after 1:1 propensity score matching by age at the index date, sex, race, laboratory data, and comorbidities, showing improved overlap and covariate balance between the two groups. |
Association Between Sugammadex Use and Postoperative Outcomes
At the 30-day follow-up, patients receiving sugammadex demonstrated a significantly lower incidence of acute respiratory failure compared to the control group (HR 0.67, 95% CI 0.50–0.88, p=0.004) (Table 2). This protective association persisted at the 90-day follow-up (HR 0.76, 95% CI 0.59–0.99, p=0.042) (Table 3). The absolute risk reduction of 2.9% at 30 days corresponds to the number needed to treat approximately 35 patients to prevent one case of acute respiratory failure. No significant differences were observed between the groups for composite pulmonary complications (pneumonia, aspiration pneumonia, or pulmonary edema) at either 30 days (8.9% vs 8.7%, p=0.972) or 90 days (11.5% vs 10.6%, p=0.484). Similarly, the risks of ICU admission, MACEs, and flap failure were comparable between the sugammadex and control groups at both time points.
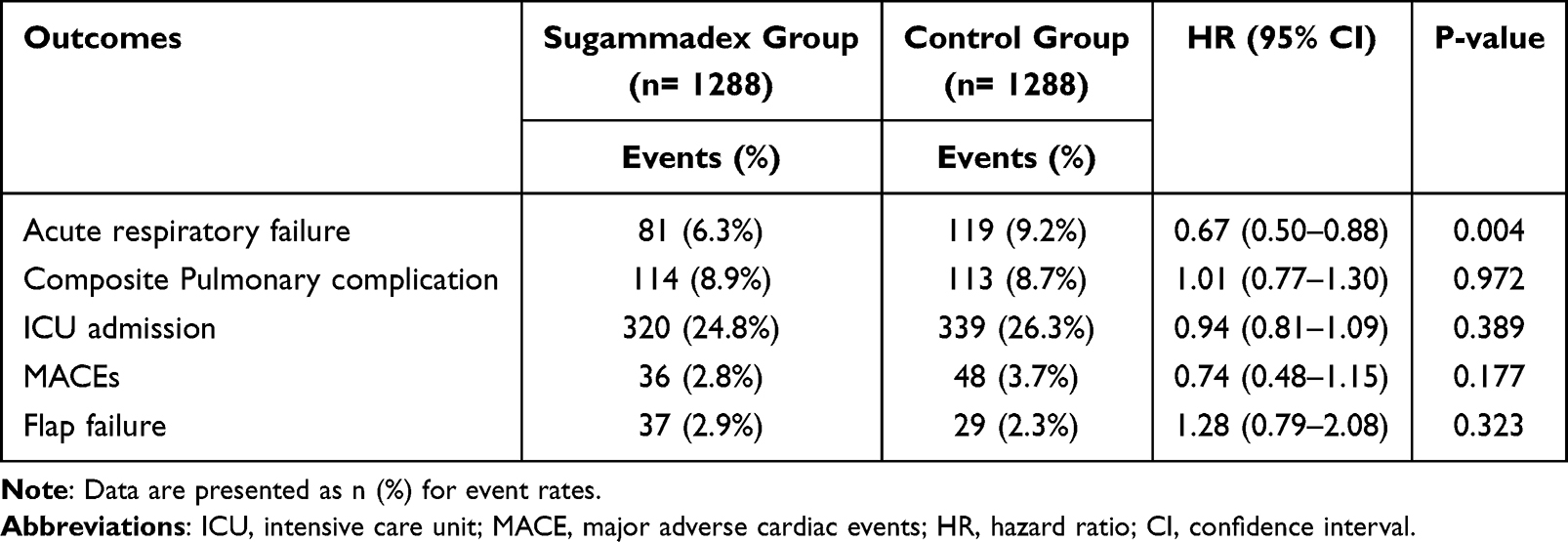 |
Table 2 Association Between Sugammadex and Postoperative Outcomes at 30-Day Follow-Up After Propensity Score Matching |
 |
Table 3 Association Between Sugammadex and Postoperative Outcomes at 90-Day Follow-Up |
Multivariate Analysis to Identify Risk Factors for Postoperative Acute Respiratory Failure
Multivariate Cox regression analysis confirmed sugammadex use as an independent protective factor against postoperative acute respiratory failure (HR 0.61, 95% CI 0.49–0.76, p<0.001) after adjusting for potential confounders (Table 4). Several patient characteristics have emerged as significant independent risk factors for respiratory failure. Ischemic heart disease conferred the highest risk (HR 1.55, p=0.001), followed by anemia (HR 1.42, p=0.026) and nicotine dependence (HR 1.37, p=0.01). Each year of increasing age was associated with a 2% increased risk (HR 1.02, p<0.001). Notably, chronic obstructive pulmonary disease, diabetes mellitus, obesity, chronic kidney disease, and malnutrition did not achieve statistical significance as independent predictors in the adjusted model, suggesting that their effects may be mediated through other pathways or may be adequately controlled by the matching process.
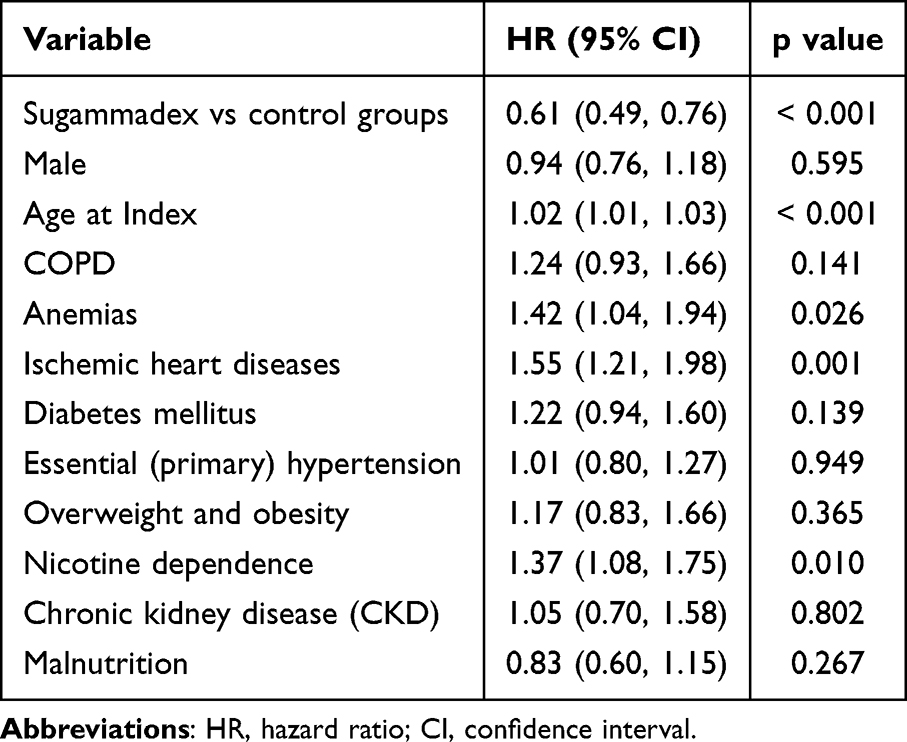 |
Table 4 Multivariate Analysis to Identify Risk Factors for Postoperative Acute Respiratory Failure |
Discussion
Our results demonstrated that sugammadex use was associated with a significantly lower incidence of acute respiratory failure than neostigmine use at both 30-day and 90-day follow-ups. The protective effect remained significant after multivariable adjustment, with sugammadex conferring a 39% reduction in the risk. Independent risk factors for acute respiratory failure include ischemic heart disease, anemia, nicotine dependence, and advancing age. No significant differences were observed between the groups for composite pulmonary complications, ICU admission, MACEs, or flap failure. These findings suggest that the choice of neuromuscular blockade reversal agent represents a clinically meaningful modifiable risk factor in this high-risk surgical population.
Head and neck free flap reconstruction is among the most complex and prolonged oncologic procedures, with surgical durations often exceeding eight to 12 hours under deep neuromuscular blockade. Extensive airway manipulation, resection of aerodigestive structures, and microsurgical anastomosis collectively increase the risk of postoperative pulmonary complications. The postoperative period is further complicated by airway edema, impaired swallowing, and the challenge of maintaining adequate flap perfusion without inducing pulmonary congestion. Reported pulmonary complication rates in this population range from 18.8% to 32.7%,1–3 far exceeding those in general surgical patients (2.7–12.6%).25–27 The pathophysiology is multifactorial: prolonged intubation and airway manipulation contribute to laryngeal edema and impaired clearance, resection disrupts swallowing and increases aspiration risk, and operative positioning promotes atelectasis and ventilation–perfusion mismatch. Residual neuromuscular blockade further amplifies respiratory vulnerability by weakening the pharyngeal and laryngeal muscles, compromising airway protection and cough efficiency. Given these risks, complete reversal of neuromuscular blockade is critical for reducing postoperative respiratory complications in this high-risk population.
Our finding of reduced acute respiratory failure with sugammadex aligns with several large-scale investigations and adds nuance to the evolving evidence. The multicenter STRONGER study by Kheterpal et al17 involving 45,712 patients across diverse surgical populations reported a 55% reduction in respiratory failure with sugammadex compared with neostigmine. Our observed 39% reduction in the head and neck cohort, though numerically lower, represents a clinically meaningful protective effect in this exceptionally high-risk population, where baseline respiratory failure rates exceed those of general surgical patients. Similarly, a recent study on COVID-19 patients undergoing thoracic surgery demonstrated decreased respiratory failure with sugammadex.19 The observation that sugammadex confers similar respiratory benefits in thoracic, COVID-19, and head and neck surgeries lends strong biological credibility to its protective role through complete neuromuscular reversal. Head and neck flap reconstruction may be an ideal procedure to reveal the benefits of sugammadex, given the combination of prolonged surgery, deep blockade, extensive airway manipulation, baseline pulmonary vulnerability, and the need for preserved airway reflexes. The persistence of benefits at 90 days suggests that early prevention of respiratory failure may avert downstream complications and promote recovery.
This study is the first to specifically evaluate the association between sugammadex use and respiratory outcomes in head and neck free flap reconstruction. Prior research on reversal agents has focused on general or thoracic surgical populations, without addressing the distinct physiological challenges of head and neck procedures. Clinically, these findings are meaningful. With an absolute risk reduction of approximately 3% and a number needed to treat of 35, adopting sugammadex as standard care could prevent one case of acute respiratory failure for every 35 patients treated. Because respiratory failure often requires intensive care, reintubation, and prolonged hospitalization, the potential clinical and economic benefits are considerable and may facilitate earlier adjuvant therapy, which is critical in oncologic recovery. The identification of ischemic heart disease, anemia, and nicotine dependence as independent predictors highlights modifiable targets for perioperative optimization. Addressing these factors through anemia correction, cardiac assessment, and smoking cessation, combined with optimal reversal agent selection may further reduce respiratory morbidity. The absence of an adjusted association with chronic obstructive pulmonary disease suggests that procedural rather than baseline pulmonary factors predominantly drive postoperative respiratory outcomes.
Although a similar analytical framework has been applied in our prior TriNetX studies,19,24 the present analysis addresses a distinct and previously unexamined clinical context—head and neck free flap reconstruction—where the balance between respiratory safety and microvascular outcomes is uniquely critical, and thus provides incremental evidence beyond prior surgical populations. The observed respiratory benefit likely reflects fundamental pharmacological differences between reversal agents. Neostigmine indirectly antagonizes neuromuscular blockade by inhibiting acetylcholinesterase, requiring sufficient spontaneous recovery to be effective and producing a ceiling effect at deep blockade levels.15,16 Additionally, its muscarinic side effects necessitate anticholinergic co-administration, potentially causing tachycardia or bronchospasm.16 In contrast, sugammadex directly encapsulates rocuronium molecules through a high-affinity chemical complex, enabling rapid and complete reversal regardless of blockade depth without cholinergic complications.15,16 This mechanistic distinction ensures more reliable restoration of neuromuscular function, providing a critical safety margin when even minor residual weakness could precipitate respiratory compromise.11,14
Flap failure rates were comparable between the sugammadex and neostigmine groups, occurring in approximately 3% of the patients in each cohort. This finding indicates that the choice of reversal agent does not compromise microvascular outcomes while potentially enhancing respiratory safety. Consistent with prior research, flap compromise in head and neck reconstruction is primarily driven by vascular events, such as thrombosis or hematoma, rather than anesthetic factors. Hsiung et al28 identified thrombosis as the strongest predictor of flap loss (Odds ratio: 86.42), along with additional contributors including hematoma formation, smoking, and specific flap types such as the posteromedial thigh flap. These mechanisms are independent of reversal of neuromuscular blockade. Moreover, concerns that sugammadex may influence coagulation have not been substantiated. A meta-analysis by Tsai et al,29 which included 1328 participants from randomized controlled trials, showed that sugammadex may transiently prolong prothrombin time without affecting activated partial thromboplastin time, suggesting no clinically meaningful impact on coagulation or bleeding risk. Taken together, these findings support the favorable benefit–risk profile of sugammadex in head and neck free flap reconstruction, reducing respiratory morbidity without jeopardizing flap survival or increasing thrombohemorrhagic complications.
Several limitations warrant consideration. First, despite propensity score matching, the retrospective observational design cannot eliminate unmeasured confounding factors. Institutional or temporal trends in practice patterns, surgeon experience, or perioperative protocols may have influenced the outcomes. Second, acute respiratory failure was identified using diagnosis codes in the TriNetX database rather than physiologic criteria (eg, PaO2/FiO2 ratios or ventilatory parameters), which may introduce outcome misclassification despite the use of standardized ICD-10-CM definitions. Third, we could not assess the depth of neuromuscular blockade at reversal, timing of reversal relative to surgical completion, or actual train-of-four ratios achieved, all of which may influence outcomes. Fourth, the study period from 2016 to 2024 encompasses evolving surgical techniques, enhanced recovery protocols, and the COVID-19 pandemic, each potentially affecting baseline complication rates and practice patterns. Fifth, we excluded patients with preexisting tracheostomy or prior critical care, limiting the generalizability to the highest-risk subgroups. Furthermore, lack of granular intraoperative data, including fluid administration volumes, vasopressor use, and transfusion requirements, represents additional unmeasured confounders. Finally, the predominantly United States patient population may limit external validity to healthcare systems with different practice patterns or patient demographics.
Conclusion
Among patients undergoing head and neck free flap reconstruction, sugammadex use was associated with significantly reduced acute respiratory failure compared with neostigmine, with effects persisting through the 90-day follow-up. Independent risk factors included ischemic heart disease, anemia, nicotine dependence, and advanced age. Given the limitations inherent to retrospective database analyses, these findings should be interpreted as hypothesis-generating. Future prospective randomized studies incorporating detailed intraoperative data—including neuromuscular blockade depth, timing of reversal, and perioperative management—are warranted to confirm these observations and clarify their clinical implications in head and neck free flap reconstruction.
Data Sharing Statement
The data utilized in this study were obtained from the TriNetX Research Network under a collaborative agreement and are not publicly available. De-identified data may be made available upon reasonable request to the corresponding author, pending approval from TriNetX and compliance with the required data-sharing agreement or network membership.
Ethics Approval Statement
The study protocol was approved by the Institutional Review Board of Chi Mei Medical Center (IRB No. 11403-E03). The requirement for informed consent was waived in accordance with institutional and national regulations governing observational research.
Patient Consent Statement
Informed consent was not required for this retrospective study, as it involved secondary analysis of pre-existing data without any interventions or direct participant interaction.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abdul-Rahman NH, Harris MK, Bottegal M, Sridharan S, Spector M, Snyderman CH. Incidence, morbidity, and mortality of pulmonary complications in free flap reconstruction: limitations of predictive models. Otolaryngol Head Neck Surg. 2025;173:603–11. doi:10.1002/ohn.1304
2. Damian D, Esquenazi J, Duvvuri U, Johnson JT, Sakai T. Incidence, outcome, and risk factors for postoperative pulmonary complications in head and neck cancer surgery patients with free flap reconstructions. J Clin Anesth. 2016;28:12–18. doi:10.1016/j.jclinane.2015.08.007
3. Loeffelbein DJ, Julinek A, Wolff KD, Kochs E, Haller B, Haseneder R. Perioperative risk factors for postoperative pulmonary complications after major oral and maxillofacial surgery with microvascular reconstruction: a retrospective analysis of 648 cases. J Craniomaxillofac Surg. 2016;44:952–957. doi:10.1016/j.jcms.2016.05.007
4. Kuo PJ, Lin PC, Hsieh CH. Airway management following head and neck microvascular reconstruction: when is a tracheostomy necessary? Risk Manag Healthc Policy. 2025;18:2551–2563. doi:10.2147/RMHP.S538063
5. McCauley P, Moore M, Duggan E. Anaesthesia for reconstructive free flap surgery for head and neck cancer. Br J Hosp Med. 2022;83:1–9. doi:10.12968/hmed.2021.0668
6. Pohlenz P, Klatt J, Schön G, Blessmann M, Li L, Schmelzle R. Microvascular free flaps in head and neck surgery: complications and outcome of 1000 flaps. Int J Oral Maxillofac Surg. 2012;41:739–743. doi:10.1016/j.ijom.2012.02.012
7. Herzog I, Panchal D, Sikder S, et al. Malnutrition in head and neck free flap reconstruction as a predictor of adverse outcomes. Ann Plast Surg. 2024;92:S251–s4.
8. Lai CJ, Shih PY, Cheng YJ, et al. Incidence and risk factors of postoperative pulmonary complications after oral cancer surgery with free flap reconstruction: a single center study. J Formos Med Assoc. 2024;123:347–356. doi:10.1016/j.jfma.2023.09.003
9. Bhowmick RS, Sarkar A, Ghosh S, Gope S, Chakraborty R. Postoperative pulmonary complication as an emerging complication in major head and neck cancer surgery: a retrospective study. Natl J Maxillofac Surg. 2023;14:471–476. doi:10.4103/njms.njms_399_21
10. Patrocínio MD, Shay D, Rudolph MI, et al. REsidual neuromuscular block prediction score versus train-of-four ratio and respiratory outcomes: a retrospective cohort study. Anesth Analg. 2021;133:610–619. doi:10.1213/ANE.0000000000005363
11. Blum FE, Locke AR, Nathan N, et al. Residual neuromuscular block remains a safety concern for perioperative healthcare professionals: a comprehensive review. J Clin Med. 2024;14:13. doi:10.3390/jcm14010013
12. Ledowski T, Szabó-Maák Z, Loh PS, et al. Reversal of residual neuromuscular block with neostigmine or sugammadex and postoperative pulmonary complications: a prospective, randomised, double-blind trial in high-risk older patients. Br J Anaesth. 2021;127:316–323. doi:10.1016/j.bja.2021.04.026
13. Alenezi FK, Alnababtah K, Alqahtani MM, Olayan L, Alharbi M. The association between residual neuromuscular blockade (RNMB) and critical respiratory events: a prospective cohort study. Perioper Med. 2021;10:14. doi:10.1186/s13741-021-00183-7
14. Huang C, Wang X, Gao S, et al. Sugammadex versus neostigmine for recovery of respiratory muscle strength measured by ultrasonography in the postextubation period: a randomized controlled trial. Anesth Analg. 2023;136:559–568. doi:10.1213/ANE.0000000000006219
15. Jones RK, Caldwell JE, Brull SJ, Soto RG. Reversal of profound rocuronium-induced blockade with sugammadex: a randomized comparison with neostigmine. Anesthesiology. 2008;109:816–824. doi:10.1097/ALN.0b013e31818a3fee
16. Carron M, Zarantonello F, Tellaroli P, Ori C. Efficacy and safety of sugammadex compared to neostigmine for reversal of neuromuscular blockade: a meta-analysis of randomized controlled trials. J Clin Anesth. 2016;35:1–12. doi:10.1016/j.jclinane.2016.06.018
17. Kheterpal S, Vaughn MT, Dubovoy TZ, et al. Sugammadex versus neostigmine for reversal of neuromuscular blockade and postoperative pulmonary complications (STRONGER): a multicenter matched cohort analysis. Anesthesiology. 2020;132:1371–1381. doi:10.1097/ALN.0000000000003256
18. Liu HM, Yu H, Zuo YD, Liang P. Postoperative pulmonary complications after sugammadex reversal of neuromuscular blockade: a systematic review and meta-analysis with trial sequential analysis. BMC Anesthesiol. 2023;23:130. doi:10.1186/s12871-023-02094-0
19. Chiu TC, Kao CL, Hung KC, et al. Comparison of sugammadex versus neostigmine for postoperative outcomes in coronavirus disease 2019 patients undergoing thoracic surgery: a cohort study. J Cardiothorac Vasc Anesth. 2025;39:1257–1265. doi:10.1053/j.jvca.2025.02.015
20. Li G, Freundlich RE, Gupta RK, et al. Postoperative pulmonary complications’ association with sugammadex versus neostigmine: a retrospective registry analysis. Anesthesiology. 2021;134:862–873. doi:10.1097/ALN.0000000000003735
21. Ludwig RJ, Anson M, Zirpel H, et al. A comprehensive review of methodologies and application to use the real-world data and analytics platform TriNetX. Front Pharmacol. 2025;16:1516126. doi:10.3389/fphar.2025.1516126
22. Chen IW, Chang LC, Ho CN, et al. Association between COVID-19 and the development of chronic kidney disease in patients without initial acute kidney injury. Sci Rep. 2025;15:10924. doi:10.1038/s41598-025-96032-4
23. Ho CN, Chung WC, Kao CL, et al. Impact of preoperative QTc interval prolongation on short-term postoperative outcomes: a retrospective study. J Clin Anesth. 2024;98:111574. doi:10.1016/j.jclinane.2024.111574
24. Hung KC, Chang LC, Lai YC, et al. Effect of sugammadex on the prevention of postoperative lung atelectasis in patients undergoing metabolic and bariatric surgery: a retrospective study. Obes Surg. 2025;35:3093–3101. doi:10.1007/s11695-025-08005-1
25. Gupta S, Fernandes RJ, Rao JS, Dhanpal R. Perioperative risk factors for pulmonary complications after non-cardiac surgery. J Anaesthesiol Clin Pharmacol. 2020;36:88–93. doi:10.4103/joacp.JOACP_54_19
26. McAlister FA, Bertsch K, Man J, Bradley J, Jacka M. Incidence of and risk factors for pulmonary complications after nonthoracic surgery. Am J Respir Crit Care Med. 2005;171:514–517. doi:10.1164/rccm.200408-1069OC
27. Piccioni F, Spagnesi L, Pelosi P, et al. Postoperative pulmonary complications and mortality after major abdominal surgery. An observational multicenter prospective study. Minerva Anestesiol. 2023;89:964–976. doi:10.23736/S0375-9393.23.17382-2
28. Hsiung PH, Huang HY, Chen WY, Kuo YR, Lin YC. Cumulative risk factors for flap failure, thrombosis, and hematoma in free flap reconstruction for head and neck cancer: a retrospective nested case-control study. Int J Surg. 2024;110:7616–7623. doi:10.1097/JS9.0000000000002069
29. Tsai YH, Kao MC, Kao HN. Effects of sugammadex on coagulation: a systematic review and meta-analysis. BMC Anesthesiol. 2025;25:196. doi:10.1186/s12871-025-03041-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Airway Management Following Head and Neck Microvascular Reconstruction: When is a Tracheostomy Necessary?
Kuo PJ, Lin P, Hsieh CH
Risk Management and Healthcare Policy 2025, 18:2551-2563
Published Date: 5 August 2025
Comparison of Rocuronium and Cisatracurium in Ophthalmic Surgeries in Association with the Incidence of Intraoperative Bradycardia- A Retrospective Study
Wu SC, Chin JC, Hung KC, Hsu CY, Tsai YF, Illias AM
Drug Design, Development and Therapy 2025, 19:7247-7257
Published Date: 20 August 2025
Sugammadex versus Neostigmine Reversal After Thoracoscopic Thymectomy in Myasthenia Gravis: A Multicenter, Randomized Controlled Trial
Hu C, Liu S, Xi C, Du Y, Su S, Wang Y, Wu L, Chen H, Wang G
Drug Design, Development and Therapy 2025, 19:11965-11976
Published Date: 30 December 2025
Sugammadex vs Neostigmine for Reversal of Neuromuscular Blockade and Association with Postoperative Atelectasis After Video-Assisted Thoracoscopic Surgery: A Propensity Score-Matched Cohort Study
Hung KC, Weng HL, Wu JY, Hsu CW, Yang CP, Lai YC, Chen IW
Drug Design, Development and Therapy 2026, 20:593657
Published Date: 6 March 2026
Sugammadex for Neuromuscular Blockade Reversal and Postoperative Recovery in Laparoscopic Bariatric Surgery: A Randomized Controlled Trial
Wang QQ, Duan JL, Li LT, Dong J, Zhu YJ, Zhang JW
Drug Design, Development and Therapy 2026, 20:570281
Published Date: 10 March 2026