Back to Journals » Drug Design, Development and Therapy » Volume 19
Sugammadex versus Neostigmine Reversal After Thoracoscopic Thymectomy in Myasthenia Gravis: A Multicenter, Randomized Controlled Trial
Authors Hu C, Liu S, Xi C, Du Y, Su S, Wang Y, Wu L, Chen H, Wang G ![]()
Received 13 October 2025
Accepted for publication 23 December 2025
Published 30 December 2025 Volume 2025:19 Pages 11965—11976
DOI https://doi.org/10.2147/DDDT.S573927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Chunhua Hu,1 Shijiang Liu,2 Chunhua Xi,1 Yingjie Du,1 Shaofei Su,3 Yue Wang,1 Lili Wu,1 Hongya Chen,1 Guyan Wang1
1Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Anesthesiology and Perioperative Medicine, The First Affiliated Hospital with Nanjing Medical University, Nanjing, People’s Republic of China; 3Central Laboratory, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Guyan Wang, Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, 1 Dongjiaominxiang Road, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86 010 58268010, Email [email protected]
Purpose: Rapid and complete reversal of residual neuromuscular blockade (rNMB) is essential for safe postoperative recovery in patients with myasthenia gravis (MG) undergoing video-assisted thoracoscopic (VATS) thymectomy. Although sugammadex provides a novel approach for reversing rocuronium-induced neuromuscular blockade, its efficacy in this high-risk population under routine-practice conditions—where reversal timing relies on clinical judgment—remains incompletely characterized. This multicenter randomized controlled trial (RCT) compared the efficacy of sugammadex versus neostigmine for reversing rNMB in patients with mild MG undergoing VATS thymectomy, specifically under this pragmatic, experience-guided scenario.
Patients and Methods: In this prospective, superiority-design RCT, MG patients scheduled for VATS thymectomy were randomized 1:1 to receive either sugammadex (2 mg/kg) or neostigmine (0.05 mg/kg with atropine 0.02 mg/kg) for reversal of rocuronium-induced neuromuscular blockade. All patients received a standard induction dose of rocuronium (0.6 mg/kg). The attending anesthesiologist, blinded to both the reversal agent and all quantitative neuromuscular monitoring data, managed blockade using a minimal-dose strategy (boluses only for clinical signs of inadequate block). This blinded anesthesiologist determined reversal timing based on clinical judgment, with administration contingent upon independent verification of a TOF count ≥ 2. The primary outcome was recovery time (interval from reversal agent administration to normalized TOF ratio of ≥ 0.9), analyzed with the Mann–Whitney U-test. Secondary outcomes included extubation time, operating room stay duration, and incidence of rNMB at extubation and post-anesthesia care unit (PACU) arrival.
Results: Among 62 randomized patients (31 per group), all patients received reversal at a train-of-four (TOF) count of ≥ 2 (median count at reversal: 3 in both groups). Sugammadex achieved significantly faster recovery (median 2.62 [IQR 1.83– 3.28] minutes; range 0.92– 5.80 minutes) versus neostigmine (14.63 [12.22– 16.30] minutes; range 10.97– 28.81 minutes), with an estimated median difference of 12.01 minutes (95% CI: 9.50– 14.52; P < 0.001). The sugammadex group also demonstrated: shorter extubation time (P < 0.001), reduced operating room (OR) stay (P < 0.001), and lower incidence of rNMB at extubation and PACU arrival (both P < 0.01). The incidence of postoperative complications was similar between groups.
Conclusion: In patients with MG undergoing VATS thymectomy, this pragmatic trial simulating routine practice demonstrates that sugammadex provides faster and more reliable reversal of moderate neuromuscular blockade (median TOF count 3) than neostigmine, leading to clinically meaningful reductions in recovery time (by 12.01 minutes), extubation time, and rNMB incidence.
Keywords: sugammadex, neostigmine, residual neuromuscular blockade, myasthenia gravis
Introduction
Myasthenia gravis (MG) is an autoimmune disorder mediated by antibodies targeting the neuromuscular junction, resulting in characteristic muscle weakness and fatigability.1 The global prevalence of MG is approximately 29 cases per million population.2 Beyond motor dysfunction, MG is associated with an elevated risk of gastrointestinal malignancies and increased mortality, underscoring the importance of early diagnosis and targeted therapeutic interventions.3 Thymectomy, particularly video-assisted thoracoscopic surgery (VATS), has emerged as the gold standard treatment due to its minimally invasive benefits, including faster recovery and fewer complications.4–6
However, as a thoracic procedure, VATS presents specific anesthetic challenges where precise neuromuscular management is essential: it is critical for ensuring adequate oxygenation during one-lung ventilation, maintaining a clear surgical field for meticulous dissection, and achieving rapid postoperative extubation.6 These requirements heighten both the dependence on neuromuscular blocking agents (NMBAs) and the risks associated with postoperative residual neuromuscular blockade (rNMB).7 Studies report rNMB incidence ranging from 0% to 90.5%, with MG patients at inherently higher risk due to preexisting neuromuscular dysfunction.8,9 This can precipitate myasthenic crises (occurring in 12.4% of MG patients), a life-threatening complication.10 Thus, effective NMBA reversal is paramount in this context.
Although quantitative neuromuscular monitoring (eg, achieving a train-of-four ratio ≥0.9) is considered as the gold standard for assessing recovery and is strongly advocated by guidelines to guide reversal,11,12 its adoption in routine practice remains suboptimal.13,14 For instance, a survey in China revealed that only 10.2% of anesthesiologists reported ever using a neuromuscular monitor.14 Consequently, in high-risk populations like MG, selecting a reversal agent that provides rapid and predictable recovery—even in settings where clinical judgment, rather than quantitative monitoring, guides the decision to reverse—assumes critical practical importance.
Traditionally, neostigmine—an acetylcholinesterase inhibitor—has been employed. However, its efficacy in MG patients is suboptimal due to the potential for delayed recovery and the risk of cholinergic crises, a risk heightened by patients’ frequent preoperative use of acetylcholinesterase inhibitors.15 In contrast, sugammadex—a selective NMBA binder—offers faster and more predictable reversal in the general population.16 Critically, however, due to their perceived high-risk status, patients with MG have been largely excluded from the pivotal randomized controlled trials (RCTs) that established the comparative efficacy of sugammadex versus neostigmine, resulting in a significant deficit of high-quality evidence for this group.17 Existing studies in MG are predominantly retrospective or single-center.18
Therefore, to address this pivotal question with higher-level evidence, we conducted one of the few prospective, multicenter RCTs to date, comparing these reversal agents in MG patients undergoing VATS thymectomy. The study was designed to simulate pragmatic practice: the decision to reverse was made solely on clinical grounds by the managing anesthesiologist (who was blinded to both the reversal agent and quantitative monitoring data), while objective outcomes were assessed using blinded quantitative monitoring. It directly compares the efficacy and safety of sugammadex versus neostigmine for reversing rocuronium-induced neuromuscular blockade in MG patients undergoing VATS thymectomy. We hypothesize that under these practice-concordant conditions, sugammadex will provide significantly faster and more complete reversal, potentially representing a safer and more effective clinical strategy for this high-risk surgical population.
Materials and Methods
Study Design and Ethics
This prospective randomized trial was designed and executed in compliance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines and the ethical principles of the Declaration of Helsinki. Ethical approvals were obtained from the institutional review boards of Beijing Tongren Hospital, Capital Medical University (Approval No.: TRRCKY2021-009-GZ (2023)-003; dated December 19, 2023) and the First Affiliated Hospital of Nanjing Medical University (Approval No.: 2023-SR-974; dated January 17, 2024). Prior to the initiation of subject recruitment, the trial was registered with ClinicalTrials.gov under the identifier NCT06436768. Written informed consent was obtained from all participants prior to randomization.
Participants
The recruitment of patients was carried out during the period from June 1, 2024, to March 5, 2025, at both Beijing Tongren Hospital, Capital Medical University and the First Affiliated Hospital of Nanjing Medical University. Eligible participants were MG patients aged 18–65 years scheduled for elective thoracoscopic thymectomy, with ASA I–III classification and BMI 18–28 kg/m2. Exclusion criteria included difficult airway, neuromuscular disorders, medications affecting neuromuscular function, contraindications to study drugs, organ insufficiency, pregnancy/lactation, inability to provide informed consent, or planned delayed extubation (ie, not in the operating room).
Randomization and Blinding
An independent statistician performed centralized 1:1 randomization using a computer-generated sequence. To maintain blinding, the allocation was concealed from all site personnel. Study medications were prepared by a non-participating nurse, with both sugammadex and the neostigmine-atropine mixture diluted to an identical 10 mL volume in indistinguishable syringes.
The attending anesthesiologist responsible for the patient’s intraoperative management and eventual extubation remained blinded to both group assignment and all quantitative monitoring data. A separate, blinded administering anesthesiologist, not involved in clinical care, delivered the study drug and immediately departed.
Sealed opaque emergency envelopes were available in the operating room. All patients, surgeons, clinical care team members (excluding the independent statistician and the drug-preparation nurse), outcome assessors, and data analysts remained blinded to the treatment allocation.
Procedure and Intervention
A standardized anesthetic protocol was followed for all participants. Patients fasted for 8 hours preoperatively and received their usual pyridostigmine dose on the morning of surgery. Upon operating room arrival, standard monitoring (electrocardiography, pulse oximetry, non-invasive blood pressure) was applied, followed by invasive arterial pressure and bispectral index (BIS) monitoring.
Quantitative neuromuscular monitoring was initiated at the adductor pollicis using an acceleromyography (AMG) monitor (JS-100, Beijing Silugao Medical Technology). After skin preparation, electrodes were positioned 2–3 cm apart over the ulnar nerve. Following anesthesia induction, the device was calibrated (CAL 2 mode), and the pre-rocuronium baseline train-of-four (TOF) ratio was documented. Stimulation parameters were set at a pulse width of 0.2 ms, frequency of 2 Hz, and a supramaximal current of 60 mA. Thenar temperature was maintained above 32°C.
Anesthesia was induced with dexamethasone 8 mg, propofol 2–2.5 mg/kg, and sufentanil 2–4 μg/kg. After establishing the baseline TOF value but before laryngoscopy, a supplemental remifentanil bolus (80–120 μg) could be administered as needed. After confirming adequate mask ventilation, rocuronium 0.6 mg/kg was administered for double-lumen tube intubation, with position confirmed by fiberoptic bronchoscopy. Mechanical ventilation was initiated utilizing a lung-protective strategy with tidal volumes of 5–6 mL/kg (ideal body weight) and end-tidal CO2 (EtCO2) maintained at 35–40 mmHg.
Anesthesia was maintained with total intravenous anesthesia (TIVA) using propofol 6–8 mg/kg/h and remifentanil 0.1–0.3 μg/kg/min, titrated to a BIS value of 45–60. Core temperature was maintained above 36°C. An ultrasound-guided intercostal nerve block with 0.375% ropivacaine was performed before closure.
Intraoperative Neuromuscular Blockade Management
Intraoperative neuromuscular blockade was managed by the attending anesthesiologist (who, as per the randomization section, was blinded to both group assignment and all quantitative monitoring data). A minimal-dose strategy was employed for rocuronium. Following the initial intubating dose, supplemental boluses (5–10 mg) were permitted only upon clear clinical signs of inadequate surgical muscle relaxation, such as spontaneous movement, respiratory efforts, or an unexplained rise in airway pressure impeding surgical progress. Rocuronium administration was typically discontinued approximately 30 minutes before the anticipated end of surgery to allow for spontaneous recovery.
Timing of Reversal: Clinical Decision and Safety Verification
The decision to administer the neuromuscular blockade reversal agent was made solely at the discretion of the blinded attending anesthesiologist, based on clinical judgment. This decision was informed by three primary factors: surgical closure, the anticipated recovery from neuromuscular blockade, and the expected time to emergence from anesthesia. Critically, this clinical decision was made independently of any quantitative neuromuscular monitor feedback.
To ensure patient safety, the protocol incorporated a mandatory safety verification step. When the attending anesthesiologist decided to reverse, an independent observer (a research assistant not involved in clinical care) checked the AMG monitor. The pre-prepared study drug (sugammadex or neostigmine-atropine) was administered by the separate blinded administering anesthesiologist only after the independent observer confirmed a real-time TOF count ≥ 2. If the TOF count was < 2, the observer informed the clinician, and administration was delayed until this safety criterion was met.
Reversal, Extubation, and Postoperative Care
Upon meeting the safety criterion, the assigned reversal agent was administered. Extubation was performed by a separate blinded clinician after confirming: return of consciousness (following commands), sustained head lift >5 seconds, adequate ventilation (respiratory rate 10–20/min, tidal volume >4 mL/kg ideal body weight, EtCO2 ≤45 mmHg, SpO2 >95% on room air), and effective cough. A standardized lung recruitment maneuver (sustained airway pressure of 30 cmH2O for 30 seconds, repeated three times) was performed pre-extubation. Patients were transferred to the post-anesthesia care unit (PACU) once hemodynamically and respiratorily stable and were discharged after achieving an Aldrete score ≥9.
Contingency Plans
Predefined contingency plans were established. For reversal failure (TOF ratio <0.9 at 30 minutes post-reversal), universal rescue administration of sugammadex (2 mg/kg) was mandated for all participants. Suspected anaphylaxis triggered immediate standard management with epinephrine, corticosteroids, and advanced life support as needed. All protocol deviations required documentation and reporting.
Measurements and Data Collection
Trained research assistants at each center collected intraoperative and postoperative data. The primary outcome was the recovery time, defined as the time from administration of the NMBA antagonist to recovery of a normalized train-of-four ratio (TOFR) ≥ 0.9 (normalized TOFR = post-antagonist TOFR/baseline TOFR).12 Secondary outcomes included extubation time, operating room stay duration, and rNMB incidence (defined as normalized TOFR < 0.9) at extubation and PACU arrival. Severe rNMB was defined as a normalized TOFR < 0.7.
Hemodynamic parameters (MAP and HR) were recorded before and after antagonist administration. PACU monitoring included vital signs (BP, HR, SpO2, temperature) recorded every 5 minutes, adherence to oxygen weaning protocols, and documentation of adverse events (weakness, hypoxemia, airway obstruction, PONV, etc). Postoperative complications (reintubation within 48 hours, pulmonary complications according to the European Perioperative Clinical Outcomes Guidelines16) and 30-day readmissions were recorded.
Additional baseline characteristics were systematically recorded, including: (1) demographic parameters (gender, age, BMI, ASA classification, smoking status, and comorbidities); (2) preoperative clinical variables (MG duration, quantitative MG score, pyridostigmine dosage, history of MG crisis, and pulmonary function test results); and (3) intraoperative parameters (anesthesia and surgical duration, total doses of anesthetic agents and rocuronium, estimated blood loss, and fluid administration).
Sample Size
Sample size determination was based on the primary outcome of recovery time using PASS software (version 15.0; NCSS, LLC) for a two-sample t-test assuming unequal variances (Satterthwaite’s method). Using a minimal clinically important difference of at least 5 minutes,19 with standard deviations of 1.5 minutes (sugammadex group)19,20 and 9 minutes (neostigmine group),21 a power of 80% (β = 0.20), and a two-sided α of 0.05, we calculated a required sample size of 58 patients (29 per group). The final sample size was increased to 64 patients (32 per group) to accommodate a potential dropout rate of approximately 10%.
Statistical Analysis
The intention-to-treat (ITT) analysis was performed using IBM SPSS Statistics 26.0 (IBM Corp, Armonk, NY, USA). Continuous variables were analyzed using independent t-tests (mean ± SD) or Mann–Whitney U-tests (median [IQR]), based on distributional assumptions. Categorical data were presented as frequencies (%) and analyzed using chi-square or Fisher’s exact tests.
Primary (recovery time) and secondary outcomes (extubation time, operating room stay) were analyzed using Mann–Whitney U-tests, with treatment effects estimated via Hodges-Lehmann estimators and 95% CI. The incidence of rNMB was compared using chi-square/Fisher’s exact tests, and the treatment effects were presented as rate differences (95% CIs, Miettinen-Nurminen method). Hemodynamic parameters were analyzed using repeated-measures ANOVA (within- group) and unpaired t-tests (between-group). All statistical tests were two-tailed, with a significance level of P < 0.05. However, for the four secondary outcomes, the significance threshold was adjusted to 0.0125 (0.05/4) using the Bonferroni correction to account for multiple comparisons.
Results
Between June 1, 2024, and March 5, 2025, 136 patients were screened, and 64 underwent randomization. Two patients (one per group) were excluded post-randomization (due to surgery cancellation and patient refusal), resulting in a final dropout rate of 3.1% (2/64), which was within the prespecified allowance of 10%. The remaining 62 patients (31 per group) comprised the final analysis set. The CONSORT flow diagram is presented in Figure 1. Baseline characteristics presented in Table 1 demonstrate well-balanced groups.
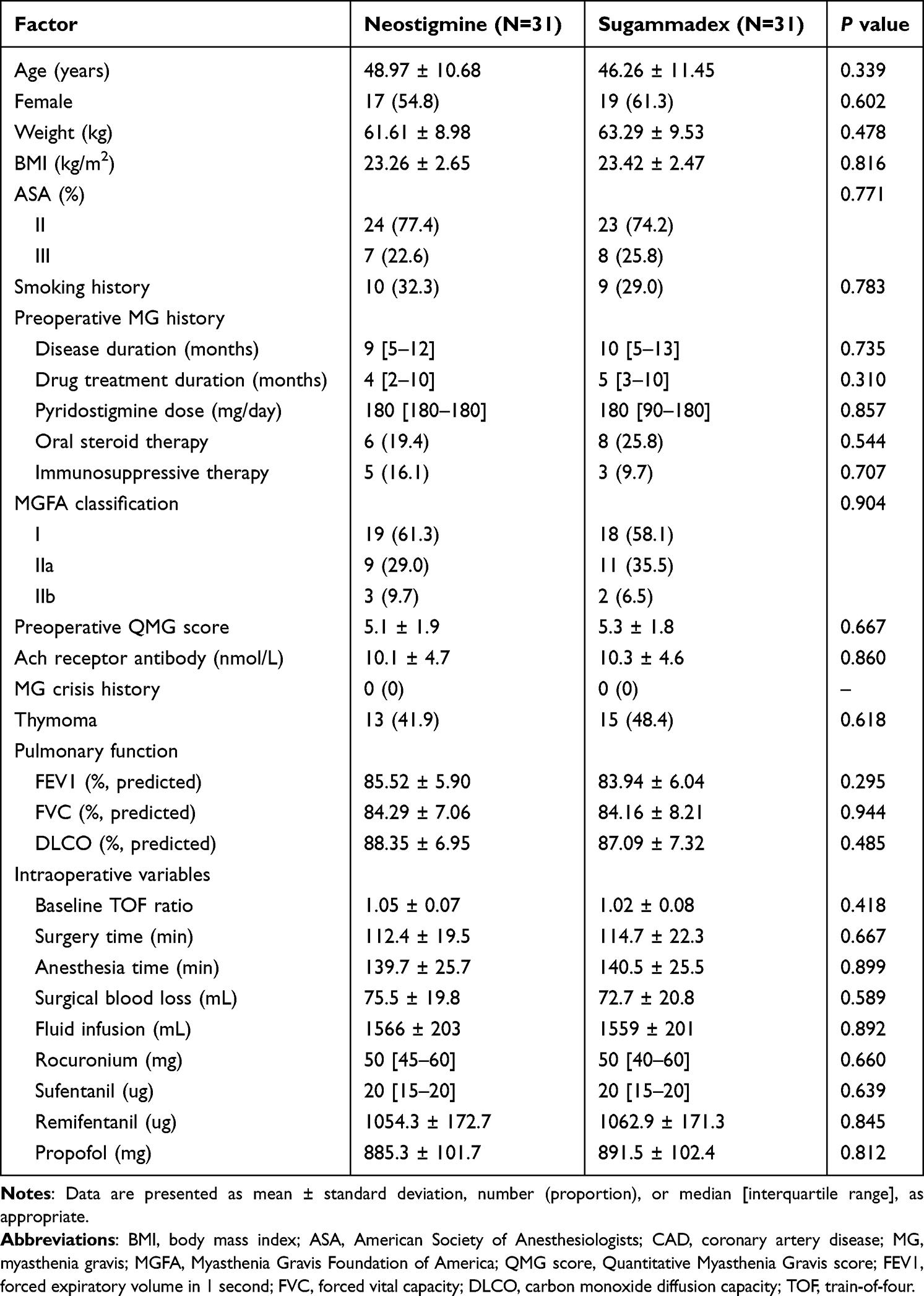 |
Table 1 Baseline Characteristics of the Studied Groups |
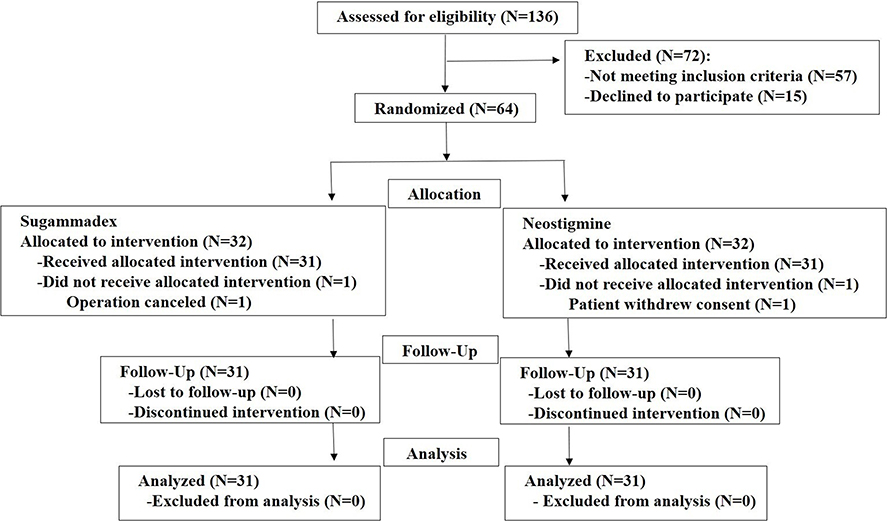 |
Figure 1 Flowchart of patient enrollment. |
Primary Outcome Results
At the time of reversal, all patients had a train-of-four (TOF) count of at least 2, with a median of 3 in both groups. No statistically significant difference was observed between the groups (P > 0.05). The primary analysis demonstrated that sugammadex provided a significantly faster neuromuscular recovery compared to neostigmine, with a clinically and statistically meaningful difference. The median recovery time was 2.62 minutes (IQR, 1.83–3.28 minutes; range, 0.92–5.80 minutes) in the sugammadex group versus 14.63 minutes (IQR, 12.22–16.30 minutes; range, 10.97–28.81 minutes) in the neostigmine group. The between-group difference was 12.01 minutes (95% CI, 9.50–14.52; P < 0.001). This treatment effect was further substantiated by cumulative incidence analysis (Figure 2), which demonstrated clear separation of the recovery time distributions between groups.
 |
Figure 2 Cumulative percentage of patients reaching normalized TOF ratio ≥ 0.9 over time in both groups. The cumulative percentage curve demonstrates that sugammadex facilitated significantly faster recovery to normalized TOF ratio ≥0.9 compared with neostigmine (P < 0.001 by the Log-rank test), with a greater proportion of patients achieving normalized neuromuscular transmission within the observed timeframe. The number at risk refers to the number of patients who had not yet achieved a TOF ratio ≥ 0.9 at each time point. TOF denotes train-of-four. |
Secondary Outcomes and Additional Findings
Secondary outcomes favored sugammadex, with reduced extubation time, operating room stay, and rNMB incidence at extubation and PACU arrival (all P < 0.0125, Bonferroni-corrected). The perioperative neuromuscular function-related variables are presented in Table 2. Sugammadex also showed shorter PACU stay and lower mild hypoxemia incidence (defined as SpO2 between 91% and 95%, P < 0.05). No between-group differences were observed in other adverse events, pulmonary complications, hospital stay, or 30-day readmissions (Table 3).
 |
Table 2 Perioperative Neuro-Muscular Function-Related Variables |
 |
Table 3 Postoperative Adverse Events and 30-Day Postoperative Follow-Up Results |
The sugammadex group maintained stable mean arterial pressure (MAP) and heart rate (HR) throughout the observation period, with no significant differences compared to baseline values (all P > 0.05). In contrast, the neostigmine group exhibited significant increases in MAP and HR at 1–10 minutes after administration (P < 0.05), which were followed by significant decreases at 20 and 30 minutes (P < 0.05). Intergroup comparisons showed that the sugammadex group had significantly lower MAP and HR at 3–10 minutes after administration (P < 0.05). No significant differences were observed between the two groups at baseline, 1 minute, 20 minutes, or 30 minutes (P > 0.05) (Figure 3).
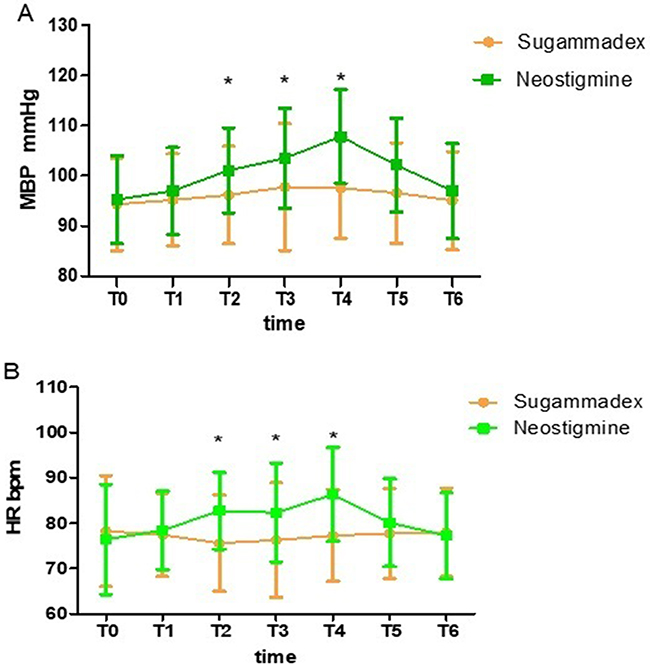 |
Figure 3 Hemodynamic changes before and after administration of neuromuscular reversal agents. (A) MAP changes; (B) HR changes. *P < 0.05 indicates statistical significance for between-group comparisons. Abbreviations: MAP, Mean Arterial Pressure; HR, Heart Rate; bpm, beats per minute; T0, immediately before administration; T1, 1 minute after administration; T2, 3 minutes after administration; T3, 5 minutes after administration; T4, 10 minutes after administration; T5, 20 minutes after administration; T6, 30 minutes after administration. |
Discussion
This multicenter RCT demonstrated that in myasthenia gravis patients eligible for early postoperative extubation, sugammadex provided superior efficacy over neostigmine for reversal of rocuronium-induced neuromuscular blockade (NMB) when administered at a median TOF count of approximately 3. The observed differential effects between the two agents in this specific population align with efficacy patterns reported in previous studies involving general surgical patients where reversal was initiated at a TOF count ≥2.
This study replicates the common clinical scenario where reversal decisions are based on qualitative judgment. Under these conditions, patients often remained under moderate neuromuscular blockade (median TOF count 3) at the end of surgery. Even then, sugammadex demonstrated a clear efficacy advantage, providing quantitative evidence that without objective monitoring, clinicians tend to reverse at deeper blockade levels—where neostigmine is less effective. This gap between objective data and subjective assessment reinforces the need for broader adoption of quantitative neuromuscular monitoring to guide reversal timing, optimize treatment, and improve patient safety, particularly in high-risk groups such as those with myasthenia gravis. Demonstrating this practice gap represents a meaningful step toward advancing clinical best practices.
Notably, patients with MG have been systematically excluded from most prior randomized trials and systematic reviews on NMB reversal,17,22,23 resulting in a pronounced evidence gap for this clinically vulnerable population.18 In general surgical populations (from which individuals with neuromuscular disorders are largely excluded), a systematic review reported a mean recovery time of 1.96 minutes for sugammadex and 12.87 minutes for neostigmine.17 In this randomized trial involving MG patients, the corresponding median recovery times were 2.62 and 14.63 minutes, respectively. Although a direct numerical comparison is limited by the different measures of central tendency, the consistent prolongation observed in our study aligns with the expected pathophysiology of MG and directly addresses the unmet need for population-specific evidence. Therefore, our findings provide the critical, practice-oriented data necessary to extend the established principles of quantitative monitoring and individualized reversal—as advocated in recent guidelines11,12—to this distinct high-risk surgical population.
In this context, the earlier prospective comparative trial by Misiolek et al provided valuable preliminary evidence.24 Their optimized protocol, which involved preoperative discontinuation of pyridostigmine combined with thoracic epidural anesthesia and administered reversal at a TOFr of 0.45, confirmed a shorter time to extubation with sugammadex.24 In contrast, our study serves as a critical complement by simulating a more prevalent clinical pathway, wherein patients continued their routine anti‑MG medications preoperatively and received general anesthesia without a routine epidural. Furthermore, the timing of reversal was designed to replicate experience-based clinical judgment. This study evaluated the performance of reversal agents under the widespread, non-standardized conditions typical of routine clinical practice, thereby enhancing the generalizability of our findings. We employed a standardized observation endpoint—administration of the reversal agent upon achieving a spontaneous TOF count of ≥2—to establish an objective baseline for comparison. Notably, no reversal failures occurred under these simulated conditions, which further attests to the high reliability of sugammadex in a routine-practice context.
A key finding of our study is that sugammadex provided rapid and profound reversal even from a moderate depth of NMB—the level most frequently encountered in routine practice—highlighting its efficacy under real-world conditions. This pharmacodynamic advantage translated into tangible clinical benefits, including a significantly shorter time to extubation and reduced operating room occupancy. Mechanistically, the direct encapsulation of rocuronium by sugammadex facilitates synchronous recovery of respiratory muscles, which provides a clear physiological basis for earlier extubation and shortens the high-risk period of postoperative mechanical ventilation.25
From a safety perspective, sugammadex markedly reduced the incidence of rNMB (TOFr < 0.9) both at extubation and upon PACU admission. This observation is consistent with reliable evidence from general surgical populations. For instance, Cammu et al reported that 15% (21/139) of the patients receiving neostigmine reversal and 2% (1/44) of those treated with Sugammadex exhibited rNMB.26 Our findings validate and extend this crucial benefit to MG patients—a population exceptionally vulnerable to respiratory compromise. Given that even mild rNMB is an established independent risk factor for postoperative pulmonary complications,27 the significantly lower incidence of hypoxemia in the sugammadex group represents a direct and clinically meaningful lung-protective outcome.
Sugammadex also demonstrated superior hemodynamic stability compared with the neostigmine-atropine combination, a finding consistent with its direct, non‑cholinergic mechanism of action and with observations reported in some non‑MG populations.28 However, it should be noted that existing comparative evidence—such as studies showing sugammadex’s advantage over neostigmine‑glycopyrrolate29 or the comparable efficacy of different anticholinergics in preventing bradycardia17—is drawn largely from non‑MG patients and may not fully represent the high‑stress context of thoracic surgery in a vulnerable cohort. In this context, the key contribution of this study lies in establishing the advantage of sugammadex specifically in the high-stress setting of thoracic surgery for patients with myasthenia gravis. The intense stimulation from double-lumen tube extubation, combined with the tachycardia-inducing effect of atropine, likely amplifies hemodynamic fluctuations associated with neostigmine. Here, the value of sugammadex extends beyond preventing bradycardia to effectively suppressing stress-induced surges in BP and HR—precisely the major challenge during extubation in thoracic surgery. Therefore, our findings underscore the necessity of optimizing the choice of neuromuscular reversal agents in high-stress surgical environments and vulnerable populations. Future studies should directly compare whether, in such contexts, refining the neostigmine-based regimen (eg, by opting for glycopyrrolate) or directly using sugammadex provides superior hemodynamic control.
While the incidence of other adverse events was similar between groups, patients receiving sugammadex experienced significantly less frequent hypoxemia in the PACU. Although the overall rate of postoperative pulmonary complications (PPCs) did not differ statistically (9.7% vs 3.2%, p > 0.05), the numerical trend consistently favored sugammadex. This directional alignment with a systematic review in which sugammadex significantly reduced severe PPCs suggests that the lack of statistical significance here may reflect the limited sample size in our MG cohort, reinforcing the need for larger trials to clarify its protective potential in this vulnerable population.
Limitations
This study has several limitations that should be acknowledged when interpreting the results. First, although the sample size provided adequate power for the primary endpoint, it remained insufficient to detect statistically significant differences in less frequent secondary outcomes; findings pertaining to these endpoints should therefore be viewed as exploratory. Moreover, this limited sample size constrains the interpretation of other clinically relevant secondary outcomes, including PACU events and hemodynamic findings, and these observations should be considered preliminary. Second, while standardized protocols for anesthesia and neuromuscular monitoring were implemented across all centers—supported by site initiation training and periodic quality audits—inherent inter‑center variations in clinical practice could not be fully eliminated. Third, the trial was designed to include only clinically stable MG patients (MGFA classification grade I–II) eligible for early extubation. Thus, the results may not be generalizable to patients with more advanced disease (grade III–V) or those requiring planned postoperative ventilation, highlighting the need for future studies in higher‑risk subgroups. Fourth, the protocol deliberately reflected a common real‑world scenario in which reversal was guided by qualitative clinical judgment rather than quantitative neuromuscular monitoring criteria. While this enhances the external validity of the findings for routine clinical practice, it also introduced variability in the depth of blockade at the time of reversal—specifically, in some cases, the reversal agent was administered at a depth of neuromuscular blockade exceeding the guideline-recommended threshold for shallow paralysis, potentially resulting in premature or suboptimal reversal. Finally, the study did not incorporate long‑term follow‑up or a formal cost‑effectiveness evaluation.
Clinical Implications and Future Research
While the present study offers robust evidence supporting the use of sugammadex in clinically stable MG patients undergoing VATS thymectomy, several important questions warrant further investigation. First, given the exclusion of patients with more severe disease (MGFA grade III–V), prospective studies or multicenter registries specifically focused on this higher-risk subgroup are urgently needed to establish safe reversal protocols for this population. Second, since sugammadex represents a higher-cost intervention compared to neostigmine, formal health-economic evaluations are warranted to assess its cost-effectiveness in the specific context of MG surgery. Such analyses should consider not only direct drug acquisition costs but also potential savings from reduced complications and shorter recovery times. Addressing these questions will be critical for optimizing resource allocation and informing the development of broader clinical guidelines.
Conclusion
This pragmatic, prospective multicenter RCT—which simulated routine clinical practice by using qualitative judgment to determine reversal timing—demonstrates that in clinically stable MG patients (MGFA class I‑II) undergoing VATS thymectomy with planned early extubation, sugammadex provides faster and more reliable reversal of moderate rocuronium‑induced neuromuscular blockade (median TOF count 3) than neostigmine. Sugammadex use resulted in clinically meaningful reductions in median recovery time (by 12.01 minutes), time to tracheal extubation, and incidence of residual neuromuscular blockade. These robust findings support the integration of sugammadex into standardized anesthesia protocols for this surgical population to enhance postoperative operational efficiency. Further research should evaluate its safety and efficacy in patients with more severe MG and assess its cost‑effectiveness in this surgical setting.
Data Sharing Statement
The original datasets generated for this study will be made available by the corresponding author without undue reservation. Interested researchers can request access via email following article publication.
Acknowledgments
The authors gratefully acknowledge the instrumental contributions of the operating room staff to the successful completion of this study.
Funding
This work was funded by the Wu Jieping Medical Foundation (Grant No. 320.6750.2020-21-10) and the Beijing Hospital Authority’s Ascent Plan (Grant No. DFL20220203), and the funders played no role in the study design, execution, or publication decisions, for which the authors are solely responsible.
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Marcus R. What is myasthenia gravis? JAMA. 2024;331(5):452. doi:10.1001/jama.2023.16872
2. Punga AR, Maddison P, Heckmann JM, Guptill JT, Evoli A. Epidemiology, diagnostics, and biomarkers of autoimmune neuromuscular junction disorders. Lancet Neurol. 2022;21(2):176–188. doi:10.1016/S1474-4422(21)00297-0
3. Hemminki K, Liu X, Ji J, Sundquist J, Sundquist K. Effect of autoimmune diseases on mortality and survival in subsequent digestive tract cancers. Ann Oncol. 2012;23(8):2179–2184. doi:10.1093/annonc/mdr590
4. Wolfe GI, Kaminski HJ, Cutter GR. Randomized trial of thymectomy in myasthenia gravis. N Engl J Med. 2016;375(20):2006–2007. doi:10.1056/NEJMoa1602489
5. Berrih-Aknin S, Le Panse R. Thymectomy in myasthenia gravis: when, why, and how? Lancet Neurol. 2019;18(3):225–226. doi:10.1016/S1474-4422(18)30467-8
6. O’Sullivan KE, Kreaden US, Hebert AE, Eaton D, Redmond KC. A systematic review of robotic versus open and video assisted thoracoscopic surgery (VATS) approaches for thymectomy. Ann Cardiothorac Surg. 2019;8(2):174–193. doi:10.21037/acs.2019.02.04
7. Kirmeier E, Eriksson LI, Lewald H, et al. Post-anaesthesia pulmonary complications after use of muscle relaxants (POPULAR): a multicentre, prospective observational study. Lancet Respir Med. 2019;7(2):129–140. doi:10.1016/S2213-2600(18)30294-7
8. Raval AD, Anupindi VR, Ferrufino CP, Arper DL, Bash LD, Brull SJ. Epidemiology and outcomes of residual neuromuscular blockade: a systematic review of observational studies. J Clin Anesth. 2020;66:109962. doi:10.1016/j.jclinane.2020.109962
9. de Boer HD, Fuchs-Buder T. Residual neuromuscular blockade and myasthenia gravis. Acta Anaesthesiol Scand. 2012;56(7):932–933; authorreply933. doi:10.1111/j.1399-6576.2012.02713.x
10. Leuzzi G, Meacci E, Cusumano G, et al. Thymectomy in myasthenia gravis: proposal for a predictive score of postoperative myasthenic crisis. Eur J Cardiothorac Surg. 2014;45(4):e76–88; discussione88. doi:10.1093/ejcts/ezt641
11. Fuchs-Buder T, Romero CS, Lewald H, et al. Peri-operative management of neuromuscular blockade: a guideline from the European Society of Anaesthesiology and Intensive Care. Eur J Anaesthesiol. 2023;40(2):82–94. doi:10.1097/EJA.0000000000001769
12. Thilen SR, Weigel WA, Todd MM, et al. 2023 American Society of Anesthesiologists Practice guidelines for monitoring and antagonism of neuromuscular blockade: A report by the American Society of Anesthesiologists Task Force on Neuromuscular Blockade. Anesthesiology. 2023;138(1):13–41. doi:10.1097/ALN.0000000000004379
13. Olesnicky BL, Lindberg A, Marroquin-Harris FB, Ren K. A survey of current management of neuromuscular block and reversal in Australia and New Zealand. Anaesth Intensive Care. 2021;49(4):309–315. doi:10.1177/0310057X21995498
14. Wu H, Lin Z, Zhou R, et al. Neuromuscular blocking agents and monitoring in China: a cross-sectional survey of current management. Front Med. 2022;9:770105. doi:10.3389/fmed.2022.770105
15. Hetherington KA, Losek JD. Myasthenia gravis: myasthenia vs. cholinergic crisis. Pediatr Emerg Care. 2005;21(8):546–548; quiz549–551. doi:10.1097/01.pec.0000173353.76142.81
16. Yin D, Tang B, Hu X, Hu H. A comparative study of sugammadex and neostigmine: a bibliometric analysis of the past 15 years. Drug Des Devel Ther. 2025;19:6357–6377. doi:10.2147/DDDT.S519235
17. Hristovska AM, Duch P, Allingstrup M, Afshari A. Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults. Cochrane Database Syst Rev. 2017;8(8):CD012763. doi:10.1002/14651858.CD012763
18. Kaye AD, Villafarra EA, Everett ES, et al. Safety and efficacy of sugammadex in management of patients with myasthenia gravis undergoing general anesthesia: a systematic review. Heliyon. 2025;11(2):e41757. doi:10.1016/j.heliyon.2025.e41757
19. Flockton EA, Mastronardi P, Hunter JM, et al. Reversal of rocuronium-induced neuromuscular block with sugammadex is faster than reversal of cisatracurium-induced block with neostigmine. Br J Anaesth. 2008;100(5):622–630. doi:10.1093/bja/aen037
20. Suy K, Morias K, Cammu G, et al. Effective reversal of moderate rocuronium- or vecuronium-induced neuromuscular block with sugammadex, a selective relaxant binding agent. Anesthesiology. 2007;106(2):283–288. doi:10.1097/00000542-200702000-00016
21. Reid JE, Breslin DS, Mirakhur RK, Hayes AH. Neostigmine antagonism of rocuronium block during anesthesia with sevoflurane, isoflurane or propofol. Can J Anaesth. 2001;48(4):351–355. doi:10.1007/BF03014962
22. Farag E, Rivas E, Bravo M, et al. Sugammadex versus neostigmine for reversal of rocuronium neuromuscular block in patients having catheter-based neurointerventional procedures: a randomized trial. Anesth Analg. 2021;132(6):1666–1676. doi:10.1213/ANE.0000000000005533
23. Moon TS, Reznik S, Pak T, et al. Sugammadex versus neostigmine for reversal of rocuronium-induced neuromuscular blockade: a randomized, double-blinded study of thoracic surgical patients evaluating hypoxic episodes in the early postoperative period. J Clin Anesth. 2020;64:109804. doi:10.1016/j.jclinane.2020.109804
24. Hanna Misiołek DC, Karpe J, Tomala A, Palaczyński P, Chełchowski J. The use of sugammadex for the reversal of neuromuscular blockade after thymectomy with videothoracoscopy in myasthenia gravis patients - a preliminary report. Kardiochirurgia i Torakochirurgia Polska. 2013;10:239–243.
25. Huang C, Wang X, Gao S, et al. Sugammadex versus neostigmine for recovery of respiratory muscle strength measured by ultrasonography in the postextubation period: a randomized controlled trial. Anesth Analg. 2023;136(3):559–568. doi:10.1213/ANE.0000000000006219
26. Cammu GV, Smet V, De Jongh K, Vandeput D. A prospective, observational study comparing postoperative residual curarisation and early adverse respiratory events in patients reversed with neostigmine or sugammadex or after apparent spontaneous recovery. Anaesth Intensive Care. 2012;40(6):999–1006. doi:10.1177/0310057X1204000611
27. Nemes R, Pongracz A, Asztalos L, et al. Guideline on the safe use of neuromuscular blocking agents. Orv Hetil. 2025;166(15):569–577. doi:10.1556/650.2025.33285
28. Tsai YH, Chen CY, Wong HF, Chou AH. Comparison of neostigmine and sugammadex for hemodynamic parameters in neurointerventional anesthesia. Front Neurol. 2023;14:1045847. doi:10.3389/fneur.2023.1045847
29. Chang HC, Liu SY, Lee MJ, Lee SO, Wong CS. Sugammadex reversal of muscle relaxant blockade provided less Post-Anesthesia Care Unit adverse effects than neostigmine/glycopyrrolate. J Formos Med Assoc. 2022;121(12):2639–2643. doi:10.1016/j.jfma.2022.04.017
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Rocuronium and Cisatracurium in Ophthalmic Surgeries in Association with the Incidence of Intraoperative Bradycardia- A Retrospective Study
Wu SC, Chin JC, Hung KC, Hsu CY, Tsai YF, Illias AM
Drug Design, Development and Therapy 2025, 19:7247-7257
Published Date: 20 August 2025
Sugammadex and Postoperative Respiratory Failure in Head and Neck Surgery: A Cohort Study
Hung KC, Yu TS, Lai YC, Chen IW
Drug Design, Development and Therapy 2026, 20:580072
Published Date: 7 February 2026
Sugammadex vs Neostigmine for Reversal of Neuromuscular Blockade and Association with Postoperative Atelectasis After Video-Assisted Thoracoscopic Surgery: A Propensity Score-Matched Cohort Study
Hung KC, Weng HL, Wu JY, Hsu CW, Yang CP, Lai YC, Chen IW
Drug Design, Development and Therapy 2026, 20:593657
Published Date: 6 March 2026
Sugammadex for Neuromuscular Blockade Reversal and Postoperative Recovery in Laparoscopic Bariatric Surgery: A Randomized Controlled Trial
Wang QQ, Duan JL, Li LT, Dong J, Zhu YJ, Zhang JW
Drug Design, Development and Therapy 2026, 20:570281
Published Date: 10 March 2026