Back to Journals » Drug Design, Development and Therapy » Volume 20
Sugammadex for Neuromuscular Blockade Reversal and Postoperative Recovery in Laparoscopic Bariatric Surgery: A Randomized Controlled Trial
Authors Wang QQ, Duan JL, Li LT, Dong J, Zhu YJ, Zhang JW
Received 25 September 2025
Accepted for publication 20 February 2026
Published 10 March 2026 Volume 2026:20 570281
DOI https://doi.org/10.2147/DDDT.S570281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Qian-Qian Wang,1 Jun-Li Duan,1 Ling-Tong Li,1 Jing Dong,1 Yi-Jing Zhu,1 Jian-Wen Zhang2
1College of Anesthesiology, Shanxi Medical University, Taiyuan, Shanxi, 030001, People’s Republic of China; 2Department of Anesthesiology, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, Shanxi, 030032, People’s Republic of China
Correspondence: Jian-Wen Zhang, Department of Anesthesiology, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, No. 99 of Longcheng Street, Xiaodian District, Taiyuan, Shanxi, 030032, People’s Republic of China, Tel +8613994299284, Email [email protected]
Objective: The aim of this study was to evaluate the effect of sugammadex on the quality of postoperative recovery among patients undergoing laparoscopic bariatric surgery.
Methods: In this randomized controlled trial, 60 patients scheduled for laparoscopic bariatric surgery were allocated to receive either neostigmine (N group) or sugammadex (S group) for neuromuscular blockade reversal. At the conclusion of surgery, the N group received intravenous neostigmine 0.04 mg/kg with atropine 0.02 mg/kg, while the S group received intravenous sugammadex 2 mg/kg. The primary outcome was the Quality of Recovery-15 (QoR-15) score at 24 hours postoperatively. Secondary outcomes included anesthesia recovery time, time to train-of-four (TOF) ratio ≥ 0.9, extubation time, time to achieve a modified Aldrete score ≥ 9, Richmond Agitation-Sedation Scale (RASS) scores, Visual Analogue Scale (VAS) pain scores after extubation, and time to first postoperative flatus/defecation.
Results: QoR-15 scores at 24 hours postoperatively were significantly higher in the S group compared with the N group (p < 0.001), with the intergroup Cohen’s d was 1.547 (95% CI: 1.014 to 2.293). The S group demonstrated shorter anesthesia recovery time, time to achieve TOF ratio ≥ 0.9, extubation time, and time to modified Aldrete score ≥ 9 (p < 0.05). RASS scores immediately and 10 minutes after extubation were higher in the S group (p < 0.05). No significant differences were observed between groups in VAS pain scores at any postoperative time point or in total opioid consumption (p > 0.05). Time to first postoperative flatus/defecation were shorter in the S group (p < 0.05).
Conclusion: The sugammadex administration in patients undergoing laparoscopic bariatric surgery could expedite reversal of neuromuscular blockade, shorten anesthesia recovery time, and facilitate gastrointestinal function restoration. It also improved postoperative quality of recovery without elevating pain intensity or increasing opioid consumption.
Keywords: enhanced recovery after surgery, laparoscopic bariatric surgery, neostigmine, quality of recovery, sugammadex
Introduction
The global prevalence of obesity and related metabolic disorders, including hypertension, coronary heart disease, diabetes mellitus, and obstructive sleep apnea, has risen substantially in recent years, representing a major public health burden.1 Laparoscopic bariatric surgery is the most effective intervention for severe obesity and its comorbidities. However, obese patients often present with obstructive sleep apnea or obesity hypoventilation syndrome, placing them at high perioperative risk. Residual neuromuscular blockade (RNMB) following intraoperative muscle relaxant use may increase the risk of regurgitation, aspiration, hypoxemia, carbon dioxide retention, and even cardiac arrest.2,3 Prompt and complete reversal of neuromuscular blockade is therefore critical to minimize RNMB and maintain airway patency in this high-risk population.
Neostigmine, an acetylcholinesterase inhibitor, is widely used for reversal but has a ceiling effect and may cause incomplete reversal, particularly in patients with severe obesity. It also induces cholinergic adverse effects including bradycardia and bronchospasm, requiring co-administration of anticholinergic agents such as atropine.4 Sugammadex is a selective antagonist that rapidly and completely reverses rocuronium- or vecuronium-induced neuromuscular blockade without affecting muscarinic receptors or plasma cholinesterase, thus avoiding the need for anticholinergic co-administration.5,6 This profile is especially advantageous for obese patients with cardiovascular or respiratory comorbidities.
Previous studies confirm that sugammadex enables faster neuromuscular reversal than neostigmine.7–12 However, most investigations focus only on reversal speed and completeness, while its effects on postoperative sedation, pain control, gastrointestinal function, and overall recovery quality remain poorly defined in patients undergoing laparoscopic bariatric surgery. As these patients are particularly vulnerable to postoperative respiratory complications and delayed recovery, clarifying the comprehensive effects of sugammadex is clinically important.
This study therefore evaluated the effects of sugammadex on neuromuscular recovery, sedation, pain management, and overall recovery quality in patients undergoing laparoscopic bariatric surgery. We hypothesized that sugammadex would accelerate neuromuscular reversal, anesthesia emergence, and gastrointestinal recovery, improve pain control and recovery quality, and support enhanced recovery after surgery in this population.
Materials and Methods
Study Participants
Ethical approval of this study was granted by the Ethics Committee of Shanxi Bethune Hospital (YXLL-2024-195), and the study was registered with the Chinese Clinical Trial Registry (ChiCTR2400093208). Written informed consent was obtained from all participants prior to enrollment. A total of 60 patients with a clinical diagnosis of metabolic syndrome who were scheduled to undergo elective laparoscopic sleeve gastrectomy under general anesthesia at Shanxi Bethune Hospital between December 2024 and May 2025 were included.
The sample size was calculated based on a pilot study with 10 patients in each group. In the pilot study, the Quality of Recovery-15 (QoR-15) scores (mean ± standard deviation [SD]) at 24 hours postoperatively were 120.93 ± 12.23 in the N group and 129.52 ± 10.11 in the S group. Using a two-sided test with a significance level (α) of 0.05 and a power (1−β) of 0.80, and assuming a 1:1 allocation ratio, a minimum of 27 patients per group was required (calculated using SAS 9.4, SAS Institute, Cary, NC, USA). To account for an anticipated 10% dropout rate, 30 patients were enrolled in each group.
Inclusion criteria were as follows: age between 18 and 50 years; body mass index (BMI) ≥ 32.5 kg/m2; American Society of Anesthesiologists (ASA) physical status classification I–III; and New York Heart Association (NYHA) functional class I–II. Exclusion criteria consisted of a history of central nervous system or respiratory system disorders; severe hepatic or renal dysfunction; neuromuscular disorders; use of medications known to interact with rocuronium during the perioperative period; or inability to cooperate with the study or refusal to provide written informed consent.
This study was designed as a prospective, double-blind, randomized controlled trial (RCT). Randomization was conducted using a random number table generated with SPSS version 26.0 (IBM Corporation, Armonk, NY, USA). Participants were allocated in a 1:1 ratio to either the neostigmine group (N group) or the sugammadex group (S group). Both participants and outcome assessors were blinded to group allocation. At the end of surgery, the group assignment was revealed by the attending anesthesiologist via a sealed opaque envelope. Medications were prepared based on corrected body weight and administered intravenously. The N group received neostigmine 0.04 mg/kg with atropine 0.02 mg/kg, while the S group received sugammadex 2 mg/kg according to the medication package insert and previous research.13–15 Both medications were diluted to a total volume of 10 mL using normal saline. All surgical procedures were carried out by the same surgical team. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Anesthetic Management
All investigators completed unified standardized training for QoR-15/ Richmond Agitation-Sedation Scale (RASS) assessments. Preoperative fasting was maintained for 6 hours for solid food and 2 hours for clear fluids. Mechanical bowel preparation was not performed. Upon arrival in the operating room, peripheral venous access was established. Standard monitoring included electrocardiography, noninvasive blood pressure, pulse oximetry, end-tidal carbon dioxide partial pressure (PetCO2), and bispectral index (BIS). Neuromuscular monitoring was conducted using a Veryark- Train-of-four (TOF) device (Guangxi VERYARK Technology Co., Ltd., China), with bilateral electrode placement over the ulnar nerve at the wrist and a force transducer positioned between the right thumb and index finger. The temperature sensor surface was placed in contact with the intrinsic hand muscles. TOF stimulation of the adductor pollicis was applied at 50 mA, 2 Hz frequency, 200 μs pulse width, and 20-second intervals.
During the perioperative period, the principle of anesthetic medication management based on different weight standards formulated in the “Expert Consensus on Anesthesia Management for Obese Patients (2017)” in China was implemented.16 Total Body Weight (TBW) represents the actual measured weight of the patient.
Ideal Body Weight (IBW) refers to the weight corresponding to a healthy body fat ratio that varies with age. It can be approximately calculated based on height and gender. A common simple formula is: for Male, Height −100 (cm); for Female, Height −105 (cm).
Adjusted Body Weight (ABW): The calculation of adjusted body weight takes into account the increase in lean body weight and drug distribution volume in obese individuals. Calculation formula: ABW (kg) = IBW (kg)+0.4 [TBW (kg)–IBW (kg)].
Lean Body Weight (LBW) represents the weight after removing fat. The most commonly used calculation formula is as follows:


Anesthesia induction was achieved with intravenous midazolam 0.05 mg/kg (TBW), sufentanil 0.5 μg/kg (LBW), and propofol 2 mg/kg (TBW). Following loss of consciousness, baseline neuromuscular calibration was conducted. Intravenous rocuronium 0.9 mg/kg (LBW) was administered, and endotracheal intubation was performed under direct laryngoscopy once the TOF count reached zero. Volume-controlled mechanical ventilation was initiated with the following parameters: oxygen flow at 2 L/min, FiO2 of 40%, tidal volume set at 6 mL/kg (IBW), respiratory rate of 12 breaths/min, an inspiration-to-expiration ratio of 1:2, and a positive end-expiratory pressure of 5 cmH2O (1 cmH2O = 0.098 kPa). Ventilation was adjusted intraoperatively to maintain PetCO2 between 35–45 mmHg (1 mmHg = 0.133 kPa) and airway pressure < 30 cmH2O.
Anesthesia was maintained via total intravenous anesthesia. Propofol infusion was titrated to sustain BIS values between 40 and 60. Remifentanil infusion was adjusted according to blood pressure and heart rate, with the aim of maintaining hemodynamic stability within ± 20% of baseline values. Neuromuscular blockade was continuously monitored, targeting a TOF count of 0 and post-tetanic count of 0–1. Supplemental doses of rocuronium 0.2–0.3 mg/kg (LBW) were administered if TOF count was ≥ 1. Pneumoperitoneum pressure was maintained between 12 and 16 mmHg. The operating room temperature was controlled at 24 °C, and active warming methods, including fluid warming and forced-air warming, were employed to maintain core body temperature above 36 °C.
All patients received intravenous palonosetron 0.25 mg thirty minutes prior to surgical completion to prevent postoperative nausea and vomiting. Rocuronium infusion was discontinued at the time of peritoneal closure, while propofol and remifentanil infusions were stopped at skin closure. Upon reappearance of T2 during neuromuscular monitoring, participants in the N group received neostigmine 0.04 mg/kg combined with atropine 0.02 mg/kg (ABW), whereas those in the S group received sugammadex 2 mg/kg (ABW). Extubation was performed once the TOF ratio recovered to ≥ 0.9, consciousness returned, and spontaneous breathing resumed. Patients were transferred to the post-anesthesia care unit and subsequently to the general ward once a modified Aldrete score of ≥ 9 was achieved. Multimodal postoperative analgesia consisted of: (1) ultrasound-guided rectus sheath block with 30 mL of 0.33% ropivacaine; (2) intravenous patient-controlled analgesia using sufentanil 100 μg diluted to 100 mL with normal saline, programmed with a 2 mL loading dose, 1 mL/h background infusion, 2 mL bolus dose, and a 15-minute lockout interval; and (3) intravenous ibuprofen 0.8 g administered every 12 hours.
Outcome Measures
Primary Endpoint
The primary endpoint was the QoR-15 score assessed 24 hours after surgery (Supplementary Table 1).
Secondary Endpoints
Secondary endpoints included the following: (1) time to achieve a TOF ratio ≥ 0.9, measured from administration of the neuromuscular blockade antagonist to attainment of TOF ratio ≥ 0.9; (2) anesthesia recovery time, defined as the interval from neuromuscular blockade antagonist administration to eye opening in response to verbal command; extubation time, defined as the interval from antagonist administration to removal of the endotracheal tube; and time to achieve a modified Aldrete score ≥ 9; (3) RASS scores assessed immediately after extubation and at 10, 30, and 60 minutes post-extubation; (4) Visual Analogue Scale (VAS) pain scores recorded immediately after extubation and at 10, 30, and 60 minutes post-extubation, as well as total opioid consumption within the first 48 postoperative hours; (5) time to first postoperative flatus/defecation; (6) incidence of adverse events, including postoperative nausea and vomiting, agitation, hypoxemia, bradycardia, and allergic reactions.
Statistical Analysis
Statistical analyses were conducted using SPSS 26.0 software (IBM Inc., New York, NY). Continuous variables with normal distribution are expressed as mean ± standard deviation () and compared using independent-samples t-tests. Repeated measures of normally distributed data were analyzed using repeated-measures analysis of variance. Non-normally distributed continuous variables are presented as median (interquartile range) and compared using the Mann–Whitney U-test; repeated measures were assessed using generalized estimating equations (GEE). Categorical variables are reported as frequencies or percentages and compared using chi-squared tests. A value of p < 0.05 is considered statistically significant.
Results
Baseline Characteristics
A total of 75 patients scheduled for elective laparoscopic sleeve gastrectomy under general anesthesia were initially assessed for eligibility. Participation was declined by 8 patients, and 7 were excluded for not meeting the inclusion criteria (n = 2, age > 50 years; n = 3, age < 18 years; n = 1, NYHA class III; n = 1, BMI < 32.5 kg/m2). Ultimately, 60 patients were enrolled in the study. The participant selection process is illustrated in Figure 1.
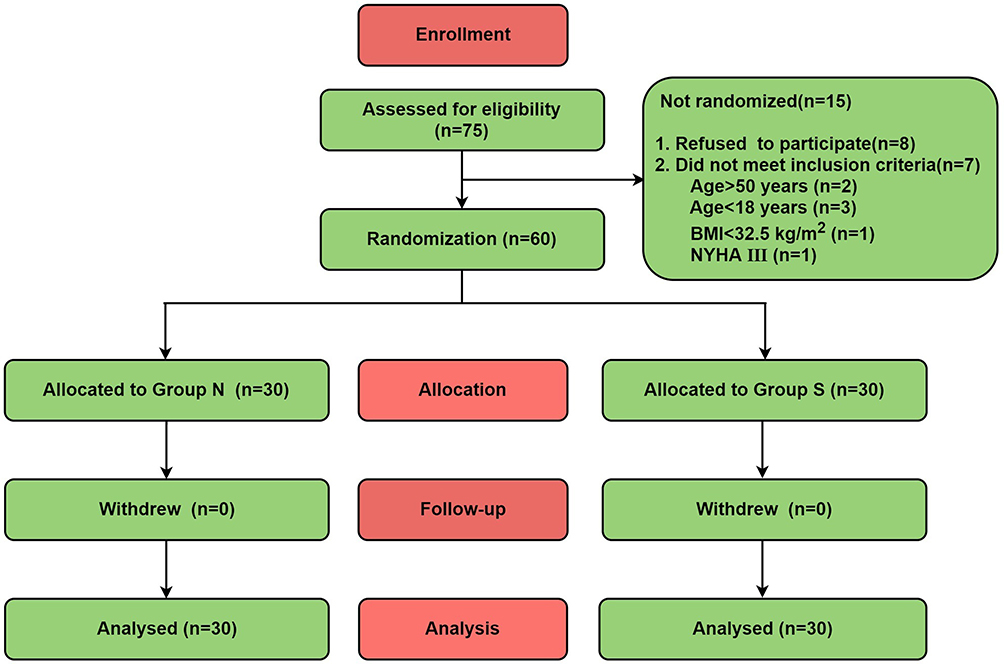 |
Figure 1 Participant flow diagram. Abbreviations: Group N, Neostigmine Group; Group S, Sugammadex Group; BMI, denotes Body Mass Index; NYHA, denotes New York Heart Association. |
No statistically significant differences were identified between groups in sex distribution, age, BMI, ASA physical status classification, surgical duration, or anesthesia duration (p > 0.05) (Table 1). Perioperative anesthetic drug consumption, intraoperative fluid intake, and estimated blood loss were comparable between the two groups (p > 0.05) (Table 1).
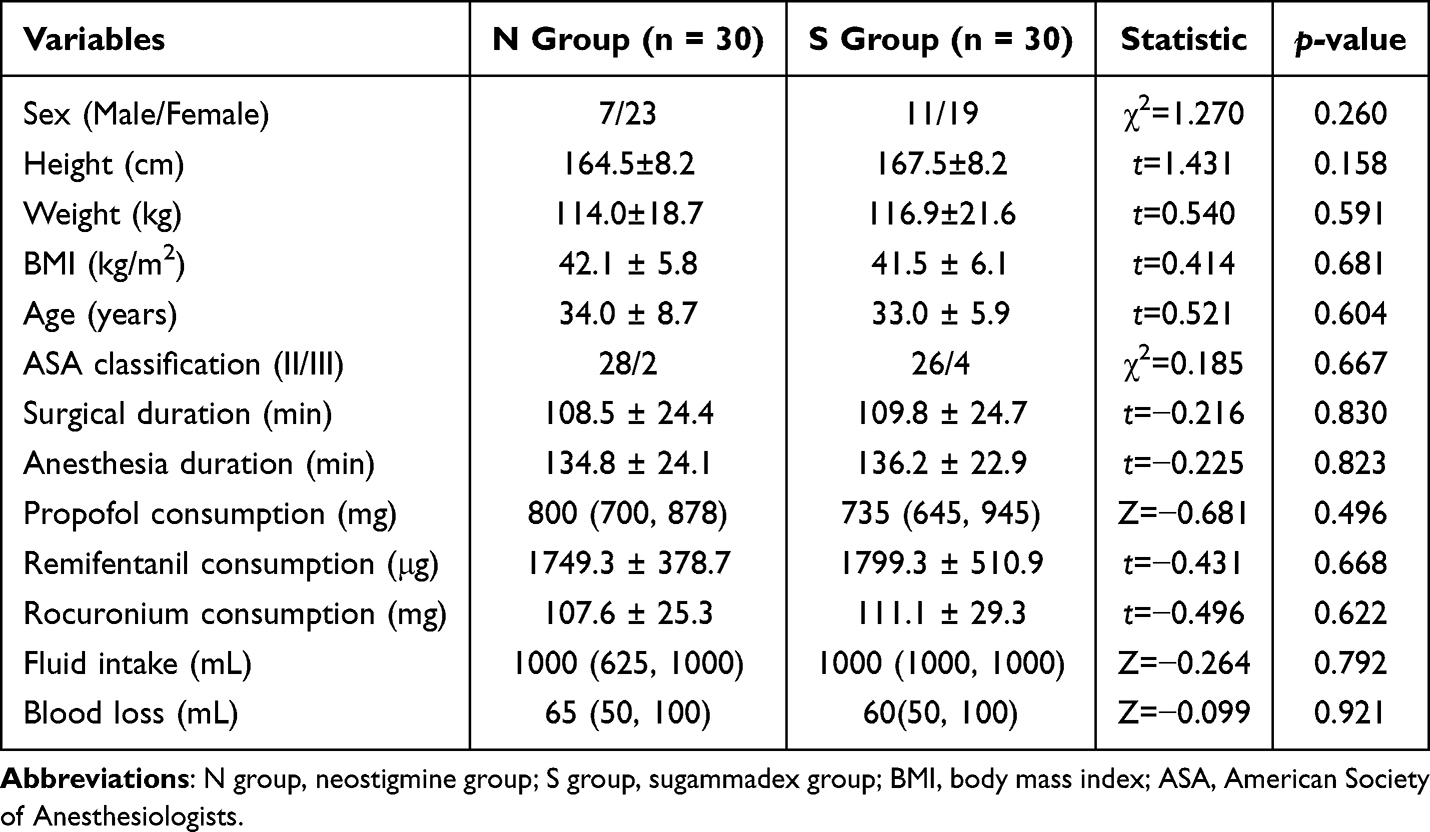 |
Table 1 Baseline Characteristics of Patients in Both Groups |
Primary Endpoint
Baseline QoR-15 scores, assessed 24 hours preoperatively, were comparable between the two groups (p > 0.05). QoR-15 scores at 24 hours postoperatively were significantly higher in the S group compared with the N group (129.00[126.00,132.00] vs 120.00 [115.75,123.75]; Z = - 4.866, p < 0.001), with the intergroup Cohen’s d was 1.547 (95% CI: 1.014 to 2.293), indicating statistically significant and clinical large effects (Table 2).
 |
Table 2 Comparison of Quality of Recovery-15 (QoR-15) Scores |
Secondary Endpoints
Anesthesia recovery time was markedly shorter in the S group compared with the N group (5.97 ± 1.50 vs 9.97 ± 2.99; t = 6.555, p < 0.001), with a mean difference of −4.00 (95% CI: −5.22 to −2.78, p < 0.001) (Table 3).
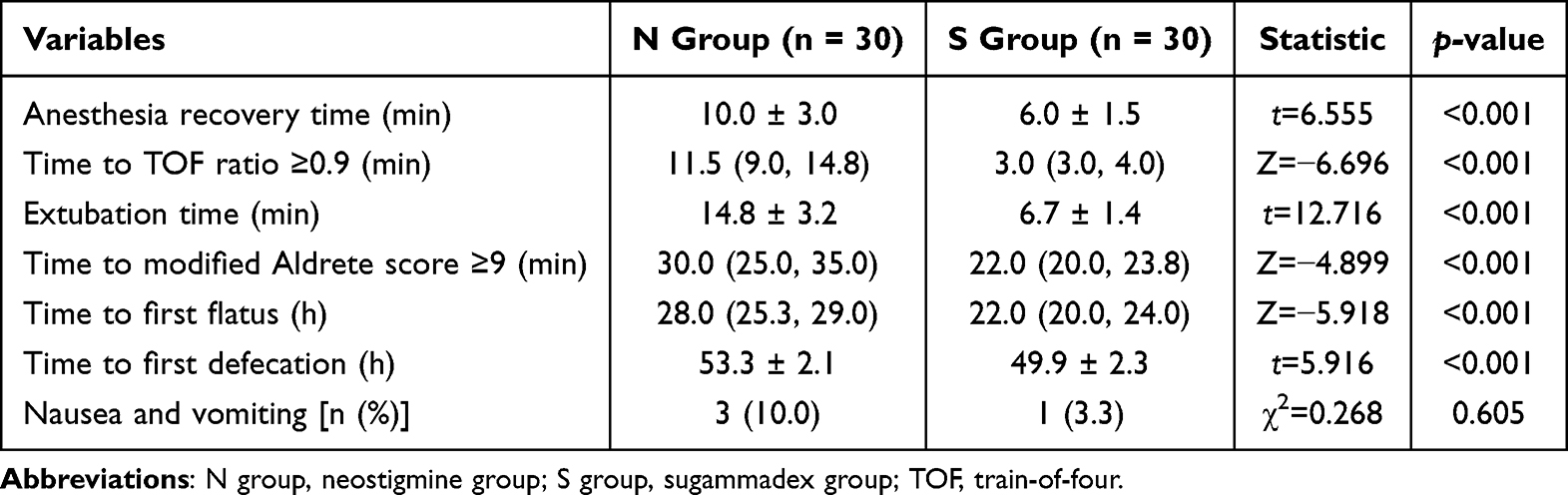 |
Table 3 Postoperative Outcomes in the Two Groups |
The anesthesia extubation time was significantly shorter in the S group than the N group (6.73 ± 1.36 vs 14.77 ± 3.18; t = 12.716, p < 0.001), with a mean difference of −8.00 (95% CI: −10.00 to −6.00, p < 0.001) (Table 3).
The time required to achieve a TOF ratio ≥ 0.9 was significantly reduced in the S group than the N group (3.00[3.00, 4.00] vs 11.50 [9.00, 14.75]; Z=−6.696, p < 0.001), with a median difference of −8.00 (95% CI: −10.00 to −7.00, p < 0.001)(Table 3).
The time to reach a modified Aldrete score ≥ 9 and first postoperative flatus/defecation were both significantly reduced in the S group compared to the N group (all p < 0.001) (Table 3).
The incidence of postoperative nausea and vomiting did not differ significantly between the groups (p > 0.05) (Table 3). No other adverse reactions were reported in either group.
Significantly higher RASS scores were observed in the S group immediately after extubation and at 10 minutes post-extubation (p < 0.05), with no significant differences found at subsequent time points (p > 0.05) (Table 4).
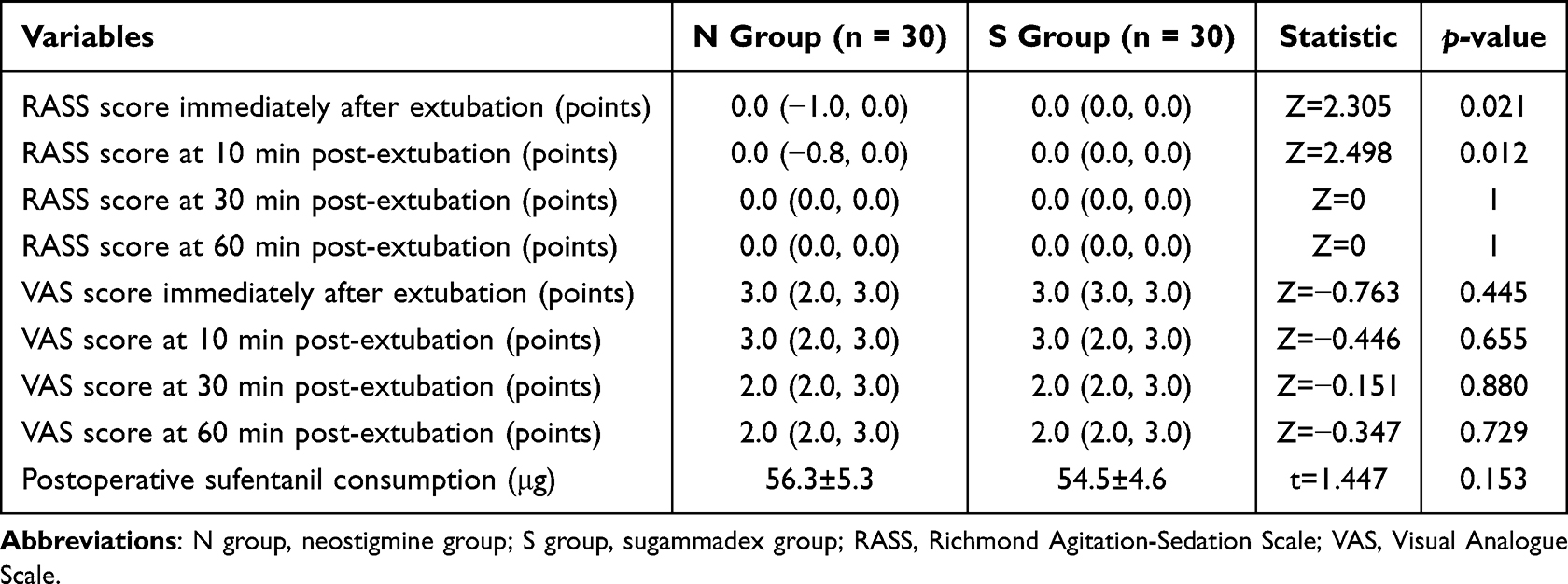 |
Table 4 Comparison of Postoperative Richmond Agitation-Sedation Scale (RASS) Scores, Visual Analogue Scale (VAS) Pain Scores, and Sufentanil Consumption |
VAS pain scores indicated no statistically significant effects of time, group, or interaction (p > 0.05) (Table 4). Total sufentanil consumption via patient-controlled analgesia within 48 hours postoperatively was similar between the two groups (p > 0.05) (Table 4).
Discussion
The present study demonstrated that, compared with neostigmine, sugammadex expedited the achievement of a TOF ratio ≥ 0.9 and a modified Aldrete score ≥ 9, shortened anesthesia recovery, extubation, and first flatus/defecation times, and significantly improved QoR-15 scores at 24 hours postoperatively without increasing pain intensity or opioid consumption in patients undergoing laparoscopic bariatric surgery.
The QoR-15 scale is a well-established instrument for evaluating early postoperative recovery quality.17–20 Myles et al suggested that a change of at least 6 points represents the minimal clinically important difference for this scale.21,22 In the present study, QoR-15 scores were significantly higher in the sugammadex group, with a Cohen’s d of 1.547 (95% CI: 1.014 to 2.293), indicating both statistically significant and clinically large effects. These findings support that sugammadex improves overall early recovery beyond conventional reversal agents.
Anesthesia recovery time, extubation time, and time to reach a modified Aldrete score ≥ 9 were also significantly shorter in the sugammadex group. These results indicate enhanced early postoperative recovery and patient comfort. Kim et al reported similar improvements in physiological recovery with sugammadex in ambulatory surgery.23 The underlying mechanism likely involves rapid elimination of muscle relaxants, reduced residual blockade, and diminished interference with respiratory and circulatory function. Notably, the most direct mechanism underlying these improvements is the complete neuromuscular recovery achieved by sugammadex, which directly meets the criteria for safe tracheal extubation and thereby accelerates anesthesia emergence.
RASS sedation scores immediately and 10 minutes after extubation were higher in the sugammadracs group, indicating earlier and smoother emergence. Guen et al reported comparable findings with increased BIS values following sugammadex administration.24 According to the differentiation theory, neuromuscular blocking agents reduce afferent input from muscle spindles and suppress cortical activity. Rapid reversal by sugammadex restores muscle spindle function and afferent signaling, which may promote arousal and emergence from anesthesia.25,26 Because direct evidence in this field remains limited, further studies are needed to clarify the precise mechanisms.
Patients with obesity frequently experience severe postoperative pain and require higher opioid doses after laparoscopic bariatric surgery. Sugammadex has been associated with reduced respiratory complications, but its effect on postoperative pain remains controversial. Castro et al reported lower pain scores and analgesic requirements with sugammadex in bariatric surgery,13 whereas Oh et al observed increased analgesic use after gastric cancer surgery.27 Emery et al proposed that restored muscle tone may lead to earlier perception of surgical pain.28
In the present study, however, no significant differences were detected in VAS pain scores or total opioid consumption between groups. This may be explained by the standardized multimodal analgesia regimen, including ultrasound-guided rectus sheath block, patient-controlled analgesia, and intravenous ibuprofen, which provided effective and balanced pain control in both groups. Moreover, co-administration of atropine with neostigmine may have mitigated its prokinetic and pro-nociceptive effects. The relatively small sample size may also have limited the detection of subtle between-group differences.
Laparoscopic bariatric surgery is often complicated by postoperative ileus due to pneumoperitoneum, intestinal manipulation, and anesthesia-related gastrointestinal suppression. Vaghiri et al showed that sugammadex accelerates bowel motility recovery compared with acetylcholinesterase inhibitors.29 Our study similarly demonstrated shorter times to first flatus and defecation in the sugammadex group.30–37 This benefit may be attributed to the lack of interaction between sugammadex and the cholinergic system. Unlike neostigmine, sugammadex does not require anticholinergic co-administration, which can impair intestinal motility.31 Sugammadex may also sequester steroid hormones that inhibit gastrointestinal motility, further promoting recovery.36,38
Postoperative nausea and vomiting (PONV) are common after bariatric surgery. In the present study, the incidence of PONV did not differ significantly between groups, consistent with a meta-analysis by Subramani et al in morbidly obese patients.39 Although sugammadex may improve respiratory function and reduce CO2-related PONV triggers, routine long-acting antiemetics likely minimized between-group differences. Ding et al reported reduced PONV with sugammadex in bariatric surgery,30 but such differences may be obscured by comprehensive antiemetic prophylaxis. The relatively small sample may also limit detection of significant differences.
Although sugammadex is more costly than neostigmine/atropine, it significantly shortened multiple intraoperative and postoperative time metrics, including anesthesia recovery, extubation, time to modified Aldrete score ≥9, and time to first flatus and defecation. These improvements may reduce PACU length of stay, improve operating room turnover, and enhance hospital efficiency, potentially offsetting higher drug costs.40, For obese patients, especially those with obstructive sleep apnea and high risk of residual neuromuscular blockade, the rapid, predictable reversal provided by sugammadex reduces the risk of respiratory compromise and supports safer recovery.
Despite higher acquisition costs, the favorable recovery profile and safety advantages suggest that sugammadex provides clinically meaningful benefits over neostigmine/atropine in patients undergoing laparoscopic bariatric surgery. Further studies with formal cost-effectiveness analyses are warranted to confirm its economic and clinical value in this high-risk population.
Limitation
This study has several limitations. First, the single-center design and relatively small sample size may have reduced statistical power, and the lack of multicenter validation limits generalizability despite the use of randomization. Second, perioperative unblinding risk was present: the characteristic rapid neuromuscular blockade reversal effect of sugammadex may have enabled assessors to identify intervention groups via objective parameters, introducing assessment bias. To mitigate this in future research, objective blinding verification strategies are recommended, including standardized blinded confidence surveys for outcome assessors at key perioperative time points and third-party independent analysis of physiological indicators to ensure blinding integrity. Third, the study only assessed short-term postoperative recovery at 24 hours, without evaluating long-term outcomes. Fourth, this was a single-center study with a relatively homogeneous ethnic population, and the follow-up period was limited to 24 hours postoperatively. Future large-scale, multicenter studies with diverse ethnic populations and longer follow-up durations (eg, assessment using the QoR‑40 quality of recovery scale at 7 days postoperatively) are warranted to validate the long-term benefits of sugammadex in this population. Future research should incorporate multicenter designs, larger sample sizes, extended follow-up periods, and comprehensive assessment tools for postoperative pain and gastrointestinal function, and implement the aforementioned blinding checks to more thoroughly assess the clinical utility of sugammadex.
Conclusion
In summary, sugammadex administration in patients undergoing laparoscopic bariatric surgery could expedite reversal of neuromuscular blockade, shorten anesthesia recovery time, and facilitate gastrointestinal function restoration. It also improved postoperative quality of recovery without elevating pain intensity or increasing opioid consumption.
Trial Registration
Full name of the registry: Chinese Clinical Trial Registry (https://www.chictr.org.cn)
Trial registration number: ChiCTR2400093208
Date of registration: 2024.11.29
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Shanxi Bethune Hospital (YXLL-2024-195). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
The trial received funding from the graduate education fund of Shanxi Medical University.
Disclosure
The authors declare that they have no competing interests.
References
1. GBD. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1223–10. doi:10.1016/S0140-6736(20)30752-2
2. Li D, Wang YY, Zhou Y, et al. Efficacy and safety of sugammadex doses calculated on the basis of corrected body weight and total body weight for the reversal of deepneuromuscular blockade in morbidly obese patients. J Int Med Res. 2021;49(1):300060520985679. doi:10.1177/0300060520985679
3. Han J, Ryu JH, Koo BW, et al. Effects of sugammadex on post-operative pulmonary complications in laparoscopic gastrectomy: a retrospective cohort study. J Clin Med. 2020;9(4):1232. doi:10.3390/jcm9041232
4. Lang B, Han L, Zeng L, et al. Efficacy and safety of sugammadex for neuromuscular blockade reversal in pediatric patients: an updated meta-analysis of randomized controlled trials with trial sequential analysis. BMC Pediatr. 2022;22(1):295–297. doi:10.1186/s12887-022-03288-0
5. Ji S-H, Huh KY, Oh J, et al. Reversal of rocuronium-induced intense neuromuscular blockade by sugammadex in Korean children: a pharmacokinetic and pharmacodynamic analysis. Clin Transl Sci. 2023;16(1):92–103. doi:10.1111/cts.13429
6. Moon TS, Reznik S, Pak T, et al. Sugammadex versus neostigmine for reversal of rocuronium-induced neuromuscular blockade: a randomized, double-blinded study of thoracic surgical patients evaluating hypoxic episodes in the early postoperative period. J Clin Anesth. 2020;64:109804. doi:10.1016/j.jclinane.2020.109804
7. Lee Y-J, Oh A-Y, Koo B-W, et al. Postoperative residual neuromuscular blockade after reversal based on a qualitative peripheral nerve stimulator response. Eur J Anaesthesiol. 2020;37(3):196–202. doi:10.1097/EJA.0000000000001157
8. Niu LX, Wang Y, Yao CL, et al. Efficacy and safety of neuromuscular blockade in overweight patients undergoing nasopharyngeal surgery. Med Sci Monit. 2020;26:e926452. doi:10.12659/MSM.926452
9. Mraovic B, Timko NJ, Choma TJ. Comparison of recovery after sugammadex or neostigmine reversal of rocuronium in geriatric patients undergoing spine surgery: a randomized controlled trial. Croat Med J. 2021;62(6):606–613. doi:10.3325/cmj.2021.62.606
10. Murphy GS, Avram MJ, Greenberg SB, et al. Neuromuscular and clinical recovery in thoracic surgical patients reversed with neostigmine or sugammadex. Anesth Analg. 2021;133(2):435–444. doi:10.1213/ANE.0000000000005294
11. Farag E, Rivas E, Bravo M, et al. Sugammadex versus neostigmine for reversal of rocuronium neuromuscular block in patients having catheter-based neurointerventional procedures: a randomized trial. Anesth Analg. 2021;132(6):1666–1676. doi:10.1213/ANE.0000000000005533
12. Yu YL, Wang HJ, Bao QQ, et al. Sugammadex versus neostigmine for neuromuscular block reversal and postoperative pulmonary complications in patients undergoing resection of lung cancer. J Cardiothorac Vasc Anesth. 2022;36(9):3626–3633. doi:10.1053/j.jvca.2022.03.033
13. Castro DS, Leão P, Borges S, et al. Sugammadex reduces postoperative pain after laparoscopic bariatric surgery: a randomized trial. Surg Laparosc Endosc Percutan Tech. 2014;24(5):420–423. doi:10.1097/SLE.0000000000000049
14. Zhang Y, Jiang Y, Lei Q, et al. Phase III clinical trial comparing the efficacy and safety of adamgammadex with sugammadex for reversal of rocuronium-induced neuromuscular block. Br J Anaesth. 2024;132(1):45–52. doi:10.1016/j.bja.2023.10.022
15. Wang Y, Yang O, Yin Y, et al. Effects of sugammadex on quality of recovery after laparoscopic bariatric surgery in severely obesepatients. Chin J Anesthesiol. 2022;42(8):911–915.
16. Wang G, Deng X, Zuo M, et al. Expert Consensus on Anesthesia Management for Obese Patients (2017)[M]. People’s Medical Publishing House; 2017 in Chinese: 655.
17. Myles PS, Boney O, Botti M, et al. Systematic review and consensus definitions for the Standardised Endpoints in Perioperative Medicine (StEP) initiative: patient comfort. Br J Anaesth. 2018;120(4):705–711. doi:10.1016/j.bja.2017.12.037
18. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
19. Myles PS, Shulman MA, Reilly J, et al. Measurement of quality of recovery after surgery using the 15-item quality of recovery scale: a systematic review and meta-analysis. Br J Anaesth. 2022;128(6):1029–1039. doi:10.1016/j.bja.2022.03.009
20. Wessels E, Perrie H, Scribante J, et al. Quality of recovery in the perioperative setting: a narrative review. J Clin Anesth. 2022;78:110685. doi:10.1016/j.jclinane.2022.110685
21. Myles PS, Myles DB, Galagher W, et al. Minimal clinically important difference for three quality of recovery scales. Anesthesiology. 2016;125(1):39–45. doi:10.1097/ALN.0000000000001158
22. Myles PS, Myles DB. An updated minimal clinically important difference for the QoR-15 scale. Anesthesiology. 2021;135(5):934–935. doi:10.1097/ALN.0000000000003977
23. Kim NY, Koh JC, Lee K-Y, et al. Influence of reversal of neuromuscular blockade with sugammadex or neostigmine on postoperative quality of recovery following a single bolus dose of rocuronium: a prospective, randomized, double-blinded, controlled study. J Clin Anesth. J Clin Anesthesia. 2019;57:97–102. doi:10.1016/j.jclinane.2019.02.014
24. Guen ML, Roussel C, Chazot T, et al. Reversal of neuromuscular blockade with sugammadex during continuous administration of anaesthetic agents: a double-blind randomised crossover study using the bispectral index. Anaesthesia. 2020;75:5):583–590.
25. Kim D, Ahn JH, Jung H, et al. Effects of neuromuscular blockade reversal on bispectral index and frontal electromyogram during steady-state desflurane anesthesia: a randomized trial. Sci Rep. Sci Rep. 2019;9(1):10486. doi:10.1038/s41598-019-47047-1
26. Giuffrida M, Ledingham NS, Machi P, et al. Rapid arousal from anaesthesia after reversal of deep rocuronium-induced neuromuscular block with sugammadex in a neuroradiological procedure. BMJ Case Rep. 2021;14(8):e242820. doi:10.1136/bcr-2021-242820
27. Oh TK, Ji E, Na H-S. The effect of neuromuscular reversal agent on postoperative pain after laparoscopic gastric cancer surgery: comparison between the neostigmine and sugammadex. Medicine. 2019;98(26):e16142. doi:10.1097/MD.0000000000016142
28. Emery CF, France CR, Harris J, et al. Effects of progressive muscle relaxation training on nociceptive flexion reflex threshold in healthy young adults: a randomized trial. Pain. 2008;138(2):375–379. doi:10.1016/j.pain.2008.01.015
29. Vaghiri S, Prassas D, Krieg S, et al. The postoperative effect of sugammadex versus acetylcholinesterase inhibitors in colorectal surgery: an updated meta-analysis. J Clin Med. 2023;12(9):3235. doi:10.3390/jcm12093235
30. Ding X, Zhu X, Zhao C, et al. Use of sugammadex is associated with reduced incidence and severity of postoperative nausea and vomiting in adult patients with obesity undergoing laparoscopic bariatric surgery: a post-hoc analysis. BMC Anesthesiol. BMC Anesthesiol. 2023;23(1):163. doi:10.1186/s12871-023-02123-y
31. Deljou A, Schroeder DR, Ballinger BA, et al. Effects of sugammadex on time of first postoperative bowel movement: a retrospective analysis. Mayo Clin Proc Innov Qual Outcomes. 2019;3(3):294–301. doi:10.1016/j.mayocpiqo.2019.06.003
32. Cho HY, Kim H, Yoon S, et al. Effect of sugammadex on the recovery of gastrointestinal motility after open pancreaticoduodenectomy: a single-center retrospective study. Minerva Anestesiol. 2021;87(10):1100–1108. doi:10.23736/S0375-9393.21.15668-8
33. Deljou A, Soleimani J, Sprung J, et al. Effects of reversal technique for neuromuscular paralysis on time to recovery of bowel function after craniotomy. Am Surg. 2023;89(5):1605–1609. doi:10.1177/00031348211058631
34. Chae YJ, Joe HB, Oh J, et al. Thirty-day postoperative outcomes following sugammadex use in colorectal surgery patients: retrospective study. J Clin Med. 2019;8(1):97. doi:10.3390/jcm8010097
35. Hunt ME, Yates JR, Vega H, et al. Effects on postoperative gastrointestinal motility after neuromuscular blockade reversal with sugammadex versus neostigmine/ Glycopyrrolate in colorectal surgery patients. Ann Pharmacother. 2020;54(12):1165–1174. doi:10.1177/1060028020929061
36. Traeger L, Hall TD, Bedrikovetski S, et al. Effect of neuromuscular reversal with neostigmine/glycopyrrolate versus sugammadex on postoperative ileus following colorectal surgery. Techniq Coloproctol. 2023;27(3):217–226. doi:10.1007/s10151-022-02695-w
37. An J, Noh H, Kim E, Lee J, Woo K, Kim H. Neuromuscular blockade reversal with sugammadex versus pyridostigmine/glycopyrrolate in laparoscopic cholecystectomy: a randomized trial of effects on postoperative gastrointestinal motility. Korean J Anesthesiol. 2020;73(2):137–144. doi:10.4097/kja.19360
38. Sen A, Erdivanli B, Tomak Y, et al. Reversal of neuromuscular blockade with sugammadex or neostigmine /atropine: effect on postoperative gastrointestinal motility. J Clin Anesth. 2016;32:208–213. doi:10.1016/j.jclinane.2016.03.010
39. Subramani Y, Querney J, He S, et al. Efficacy and Safety of sugammadex versus neostigmine in reversing neuromuscular blockade in morbidly obese adult patients: a systematic review and meta-analysis. Anesth Essays Res. 2021;15(1):111–118. doi:10.4103/aer.aer_79_21
40. Thiruvenkatarajan, Smith V, Wong DT, et al. Cost-effectiveness of sugammadex versus neostigmine for neuromuscular blockade reversal in obese patients undergoing laparoscopic surgery. J Clin Anesth. 2022;78:110689. doi:10.1016/j.jclinane.2022.110689
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Rocuronium and Cisatracurium in Ophthalmic Surgeries in Association with the Incidence of Intraoperative Bradycardia- A Retrospective Study
Wu SC, Chin JC, Hung KC, Hsu CY, Tsai YF, Illias AM
Drug Design, Development and Therapy 2025, 19:7247-7257
Published Date: 20 August 2025
Sugammadex versus Neostigmine Reversal After Thoracoscopic Thymectomy in Myasthenia Gravis: A Multicenter, Randomized Controlled Trial
Hu C, Liu S, Xi C, Du Y, Su S, Wang Y, Wu L, Chen H, Wang G
Drug Design, Development and Therapy 2025, 19:11965-11976
Published Date: 30 December 2025
Sugammadex and Postoperative Respiratory Failure in Head and Neck Surgery: A Cohort Study
Hung KC, Yu TS, Lai YC, Chen IW
Drug Design, Development and Therapy 2026, 20:580072
Published Date: 7 February 2026
Sugammadex vs Neostigmine for Reversal of Neuromuscular Blockade and Association with Postoperative Atelectasis After Video-Assisted Thoracoscopic Surgery: A Propensity Score-Matched Cohort Study
Hung KC, Weng HL, Wu JY, Hsu CW, Yang CP, Lai YC, Chen IW
Drug Design, Development and Therapy 2026, 20:593657
Published Date: 6 March 2026