Back to Journals » Patient Preference and Adherence » Volume 17
SPUR: A Patient-Reported Medication Adherence Model as a Predictor of Admission and Early Readmission in Patients Living with Type 2 Diabetes
Authors Wells J ![]() , Wang C
, Wang C ![]() , Dolgin K
, Dolgin K ![]() , Kayyali R
, Kayyali R ![]()
Received 21 November 2022
Accepted for publication 14 January 2023
Published 19 February 2023 Volume 2023:17 Pages 441—455
DOI https://doi.org/10.2147/PPA.S397424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Joshua Wells,1 Chao Wang,2 Kevin Dolgin,3 Reem Kayyali1
1Department of Pharmacy, Kingston University, Kingston upon Thames, KT1 2EE, UK; 2Faculty of Health, Science, Social Care and Education, Kingston University, Kingston upon Thames, KT2 7LB, UK; 3Behavioural Science Department, Observia, Paris, 75015, France
Correspondence: Reem Kayyali, Department of Pharmacy, Kingston University, Penrhyn Road, Kingston upon Thames, KT1 2EE, UK, Tel/Fax +44 208 417 2561, Email [email protected]
Purpose: Poor medication adherence (MA) is linked to an increased likelihood of hospital admission. Early interventions to address MA may reduce this risk and associated health-care costs. This study aimed to evaluate a holistic Patient Reported Outcome Measure (PROM) of MA, known as SPUR, as a predictor of general admission and early readmission in patients living with Type 2 Diabetes.
Patients and Methods: An observational study design was used to assess data collected over a 12-month period including 6-month retrospective and 6-month prospective monitoring of the number of admissions and early readmissions (admissions occurring within 30 days of discharge) across the cohort. Patients (n = 200) were recruited from a large South London NHS Trust. Covariates of interest included: age, ethnicity, gender, level of education, income, the number of medicines and medical conditions, and a Covid-19 diagnosis. A Poisson or negative binomial model was employed for count outcomes, with the exponentiated coefficient indicating incident ratios (IR) [95% CI]. For binary outcomes (Coefficient, [95% CI]), a logistic regression model was developed.
Results: Higher SPUR scores (increased adherence) were significantly associated with a lower number of admissions (IR = 0.98, [0.96, 1.00]). The number of medical conditions (IR = 1.07, [1.01, 1.13]), age ≥ 80 years (IR = 5.18, [1.01, 26.55]), a positive Covid-19 diagnosis during follow-up (IR = 1.83, [1.11, 3.02]) and GCSE education (IR = 2.11, [1.15,3.87]) were factors associated with a greater risk of admission. When modelled as a binary variable, only the SPUR score (− 0.051, [− 0.094, − 0.007]) was significantly predictive of an early readmission, with patients reporting higher SPUR scores being less likely to experience an early readmission.
Conclusion: Higher levels of MA, as determined by SPUR, were significantly associated with a lower risk of general admissions and early readmissions among patients living with Type 2 Diabetes.
Keywords: predictive model, logistic regression, patient reported outcome measure, type 2 diabetes
Introduction
In 1997, a systematic review of interventions to support patients with prescribed medicines was conducted by Haynes et al.1 The review concluded that the potential benefits of such interventions, which were often complex and difficult to deliver, were limited by the current level of medication adherence achieved by patients. The World Health Organisation (WHO) later quoted Haynes et al in 20012 with a call to action for a systems approach to improving the management of chronic conditions, stating that increasing the effectiveness of adherence interventions may have a far greater impact on the health of the population than any improvement in specific medical treatments.
Despite this call to action, over two decades later conservative estimates suggest that the cost of non-adherence to health-care systems sits somewhere between €1.25Bn to $290Bn per year across parts of Europe and the US.2,3
The staggering costs associated with non-adherence are somewhat less surprising when we begin to quantify the extent of the issue. Although adherence rates are highly dependent on factors such as the clinical condition, type and/or complexity of drug therapy, many studies cite within the range of approximately only 30–75% of patients taking their medications as prescribed.4–11 Poor adherence is associated with worsening clinical outcomes in the hospital setting, which include an increased risk of admission,12 mortality,13 and length of stay.14 These cases are often preventable12 and present significant economic implications, particularly in the event of early readmissions (admissions occurring within 30 days of discharge) whereby financial penalties have been brought against hospitals in the UK since 2011 for these events.15 Conversely, interventions specifically designed to support patients with their medicines have shown encouraging improvements in mortality, readmission risk and primary medication adherence in areas such as cardiovascular disease,16 mental health,17 general medicine,18 and post-surgical care.19 The positive effects associated with these interventions have also extended into the post-discharge phase, particularly when led by pharmacists, with improvements to not only readmission rates, but also general attendance to emergency departments and reduced health-care costs in secondary care settings.18,20,21
The desire for effective medication adherence interventions is clear, with significant evidence available to support their role in improving patient care and reducing health-care utilisation. Such interventions have seen particular development and advancements through the lens of digital, mobile, and technological health innovation in more recent years such as automated medication reminders, electronic cap monitors, and applications designed for patient education.22–24 However, as emphasised by Pal et al,24 such advancements are not a technological panacea given the complex relationship between adherence and socio-clinical factors such as the impact of interpersonal relationships, communication with health-care professionals, and patient motivation/self-efficacy as a few examples of factors that impact adherence outcomes. Furthermore, as discussed by Granger and Bosworth,22 although many factors have been associated with poor adherence, their use in predictive application is limited by the absence of an available strong predictive model.
Previous work by Rosen et al25 sought to develop a predictive model of 30-day readmission using retrospective medication adherence data derived from the 4-item Morisky Green Levine Scale (MGL Scale)26 completed by 385 inpatients from a tertiary care centre in Los Angeles. Although widely used as a quasi-gold-standard patient-reported outcome measure (PROM) of medication adherence, the MGL Scale has previously demonstrated low internal consistency estimates of reliability (<0.7) and poor predictive validity in some populations.26 Furthermore, despite its simple 4-item design and ease of implementation, the MGL Scale fails to address the specific drivers of poor medication adherence behaviour that are both numerous and complex.27 To this extent, development of a predictive model that integrates data derived from a PROM with such a specific scope of adherence reporting may fail to fully address the holistic nature of medication adherence behaviour. Notably, both the validity and reporting of PROMs of medication adherence, particularly in Type 2 diabetes, have seen scrutiny in recent years despite the wide variety of PROMs currently available.28,29 These findings were in part due to poor uptake of standardised validation guidance, such as the COSMIN30 criteria, that supports the development and validation of PROMs. Through the design and delivery of an international multi-arm series of studies in line with the COSMIN criteria, the SPUR tool has been developed as a holistic PROM to assess medication adherence behaviour in patients with long-term conditions. The proposed SPUR model framework31 and initial model development32 process have been reported previously. Furthermore, psychometric properties for populations based in the US33 and France34 have been reported, in addition to a UK-based cohort of patients living with type 2 diabetes (VMATT2)35 that produced a more concise SPUR tool – SPUR-27. This study sought to develop a predictive model of early readmission and general admission risk using the SPUR-27 tool as a holistic PROM of medication adherence.
Materials and Methods
Study Design
Data for this study were derived from a cohort of previously recruited participants (n = 200) from Kingston NHS Foundation Trust in the cross-sectional phase of the preceding VMATT2 study, which sought to demonstrate the psychometric properties of SPUR-27 in patients living with type 2 diabetes. Subsequently, observational cohort data for recruited participants were collected over a 12-month period that comprised hospital admission data both 6 months before and after participation in the VMATT2 study. Hence, this study followed an observational design in line with the STROBE36 cohort guidelines and is reported as such. The study (VMATT2) protocol and documentation were submitted via IRAS (ID:270768) for review with approval received from the NHS Health Research Authority (HRA) research ethics committee (Ref:19/NW/0685) in December 2019. The recruitment of the first and final participants for the VMATT2 study took place in January 2020 and October 2021, respectively, hence the period of observational data collected ranged between July 2019 and March 2022. Participants were provided with a patient information sheet and written informed consent was obtained prior involvement in the study. Observational data were derived from the Trust’s Electronic Health Record (EHR) and handled in accordance with the Trust’s data protection and patient confidentiality policies. The present study was conducted in compliance with the ethical principles for research documented in the Declaration of Helsinki.
Sample Characteristics
Participants eligible for the VMATT2 study were ≥18 years of age, prescribed ≥1 antiglycaemic agent and able to speak English. Participants had a minimum 6-month history of prescribed medications. Excluding factors included participants with significant co-morbidities that may affect adherence, eg, active cancer, severe psychiatric illness, or registration with another study at the time of recruitment that involved an investigational medicinal product. More specifically, the research team considered the unique impact and experience of cancer diagnoses and treatment on drivers of medication adherence behaviour, such as interpersonal relationships and health-care utilisation, that led to the exclusion of this patient group at this stage of development for SPUR-27.37 Severe psychiatric illness was defined as those experiencing significant and debilitating psychological impairment or cognitive deficits that limited occupational or functional activity. Therefore, this would also prevent individuals from completing the consent form/survey independently or with adequate capacity and hence was an exclusion criteria for this study. All participants included in the observational analysis had completed the SPUR-27 tool in addition to providing socio-clinical data included in the questionnaire.
Variables of Interest
The outcome variables of interest included the number of admissions 6 months before and after completing the SPUR-27 tool, as well as number of early readmissions (admissions occurring within 30 days of discharge) within the observational period. The count outcomes were further dichotomized to indicate whether the patient was admitted or re-admitted early, which is useful clinically when considering those patients who may benefit most from any targeted intervention. Clinical data, which included admission data during the observational period, were derived from the EHR. The main variable of interest assessed as part of the model was medication adherence (derived from the SPUR-27 tool). The Medication Adherence Rating Scale (MARS),38 Beliefs about Medicines Questionnaire (General/Specific) (BMQ-G/BMQ-S)39 and Diabetes Treatment Satisfaction Questionnaire (DTSQ)40 were validated PROMs previously implemented in the VMATT2 study as comparators for the new SPUR-27 tool. The results for the MARS, BMQ-G/S and DTSQ were used as comparators in this model to examine other PROMs of medication adherence behaviour and treatment satisfaction with respect to predicting admission risk. Two objective measures of adherence, the Medication Possession Ratio (MPR) and HbA1c, were also included. Covariates of interest included: age, ethnicity, gender, level of education, income, Body Mass Index (BMI), the Index of Multiple Deprivation (IMD), the number of prescribed medicines for type 2 diabetes and the number of medical conditions. This study was conducted during the Covid-19 pandemic, therefore any positive diagnosis of Covid-19 during the 12-month observational period was also recorded and included in this model.
Statistical Analysis
All descriptively reported data were analysed using SPSS version 26.0 for Windows.
For modelling count outcomes, a Poisson or negative binomial model was employed. Akaike’s information criterion (AIC) was used to select the appropriate type of model. Potential non-linear effects were modelled as fractional polynomial or restricted cubic spline terms. A link test was used to further check the final model specifications. For the binary version of the outcomes, the same set of covariates were used in logistic regression models. Given the relatively small sample size used in this study,41 Firth’s penalized maximum likelihood estimator was employed for its “remarkably stable performance”.42
Pseudo R2 was used for measuring model goodness-of-fit (McFadden’s for count outcome and Tjur’s for binary outcome models). In addition, for binary outcome models, the area under the receiver operating characteristic curve (AUC) and calibration plots were produced to assess models’ discrimination ability and calibration.
Results
Sociodemographic data were available for the entire cohort previously recruited during the VMATT2 cross-sectional study (n = 200). All participants provided their consent to participate in the follow-up observational study (100% response rate). Participant age, education, and income were collected as ordinal data and are reported as such. The modal age was 70–79 years (n = 74, 37.0%), education was reported predominantly at GCSE level or equivalent (n = 85, 42.5%) and almost three-quarters of participants indicated that they were retired (n = 146, 73.0%). Participants identifying as female represented 36.0% (n=72/200) of the cohort. Most participants were White (n = 152, 76.0%). BMI data were available for all participants (mean ± SD, 28.4 ± 5.5) and indicated that a large proportion of participants were above their recommended weight. Almost two-thirds (n=124/200, 62.0%) of participants did not meet a HbA1c target of ≤7.0% (53mmol/mol). The mean ± SD number of antiglycaemic agents and comorbidities were 1.9 ± 0.9 and 6.6 ± 2.7, respectively. The modal IMD rank by decile was 9 indicating (mean ± SD, 7.3 ± 2.2) that the cohort was broadly affluent based on the level of deprivation attributed to their postcode during the observational period (Table 1).
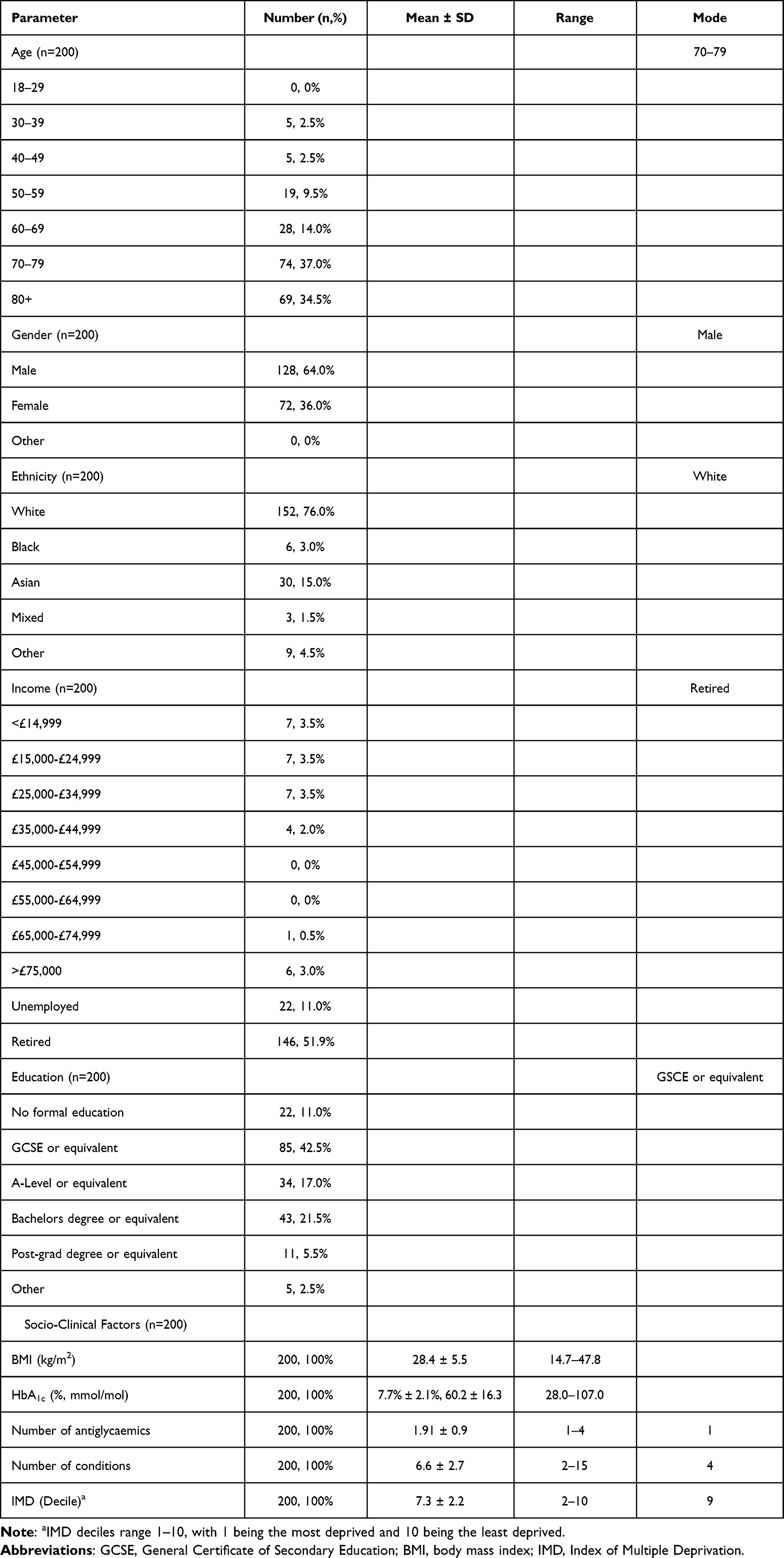 |
Table 1 Study Sample Characteristics |
Retrospective admission data were available for all participants (n = 200, 100%); however, the complete prospective data set (6-month period following completion of SPUR-27) were limited to a sample of 190 participants as a result of mortality prior to discharge or missing data from the EHR (n = 10) (Table 2). In total, 425 admissions were recorded during the observational period. Of those admissions, 254 (59.7%, n=254/425) were recorded as early readmissions. These early readmissions were reported in 98 participants, providing an early readmission rate of 48% (n=98/200) for this sample. Over half (51.5%, n=103/200) of the participants had ≥1 recorded admission in the 6 months prior to completion of the SPUR-27 questionnaire. The figure was similar for admissions in the 6-month follow-up period (56.8%, n=108/190). In total, 71% (n=142/200) of the cohort experienced a minimum of one admission within the observational period with ≥1 early readmission being recorded in 69% of cases (n=98/142).
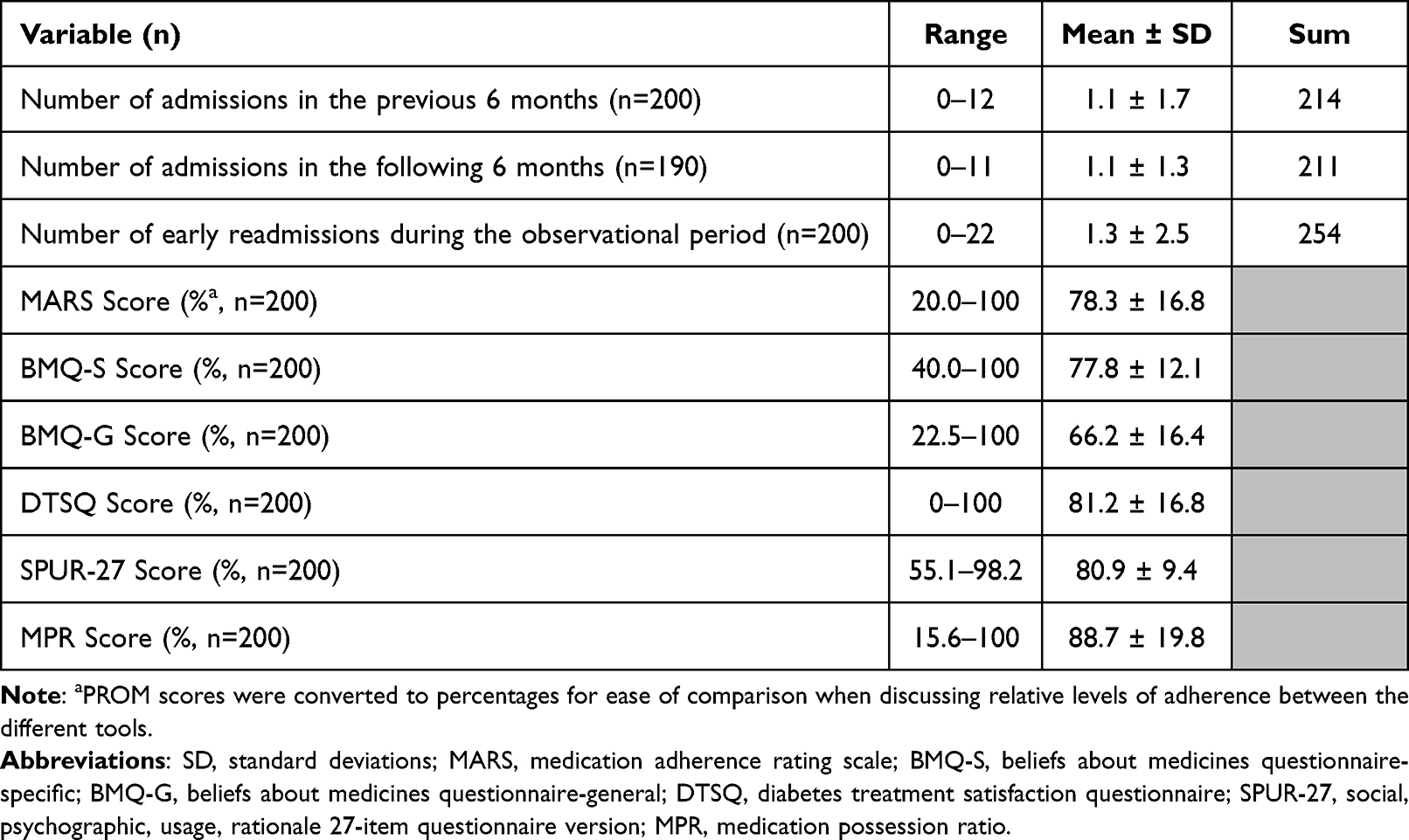 |
Table 2 Admissions & Adherence |
Data for average PROM scores were converted to percentages to assess against the crude cut-off score of 80% that is commonly assigned to the calculation of MPRs to determine whether patients are adherent to their medicines (Table 2).43 The starkest difference in adherence reporting was observed between scores for MPR and BMQ-G, with 80% (n=160/200) and 22% (n=44/200) of participants recording scores ≥80%, respectively. In relation to SPUR-27 as a multifactorial PROM of adherence, 57% (n=116/200) of the participants observed scores ≥80% which was reflective of adherence scores reported broadly in the literature for those living with a long-term condition, including type 2 diabetes.
The main variable of interest was the SPUR-27 Score. Other factors were adjusted in regression models to reduce confounding and as such, are exploratory in nature. The modelling results (coefficients and their 95% confidence intervals) are presented in the following two tables (Tables 3 and 4) for the two different types of outcomes (admission within 6-month post-study completion and early readmission within the observational period). For each type of outcome, two models were estimated: outcome as a count or binary variable. For count models, the exponentiated coefficient indicates incident ratios (IR). For example, as shown in Table 3, a one unit increase in SPUR-27 (Coefficient = −0.024, 95% CI, [−0.045, −0.003] is associated with a decrease in the number of admissions by a factor of 0.98 (IR = 0.98, 95% CI, [0.96, 1.00]). In other words, a higher SPUR-27 score (increased adherence) was associated with a lower number of admissions in the follow-up period. In addition to SPUR-27, the following factors were significantly associated (positive coefficient) with the number of admissions in the 6-month follow-up period as a count variable (IR, 95% CI): age ≥80 years (IR = 5.18, 95% CI, [1.01, 26.55]), GCSE level education or equivalent (IR = 2.11, 95% CI, [1.15,3.87]), number of medical conditions (IR = 1.07, 95% CI, [1.01, 1.13]), a positive Covid-19 diagnosis in the 6-month follow-up period (IR = 1.83, 95% CI, [1.11, 3.02]), BMQ-S score (IR = 1.02, 95% CI, [1.00, 1.04])), and HbA1c (IR = 1.02, 95% CI, [1.01, 1.03]) (Table 3). However, two factors were MPR score (IR = 0.99, 95% CI, [0.98, 1.00]), and a positive Covid-19 diagnosis within the 6-month period before study completion (IR = 0.65, 95% CI, [0.43, 1.00]) demonstrated significant negative coefficients. When modelled as a binary outcome (Coefficient, 95% CI), a higher HbA1c (0.027, 95% CI, [0.003, 0.050]), a lower SPUR-27 score (−0.048, 95% CI, [−0.094, −0.003]), a lower MPR score (−0.026, 95% CI, [−0.049, −0.004]), and a higher number of medical conditions (0.193, 95% CI, [0.061, 0.324]), remained significantly associated with an admission in the follow-up observational period. The IMD decile (higher scores reflecting lower deprivation) was an additional factor that was positively and significantly (0.181, 95% CI, [0.023, 0.339]) associated with an admission.
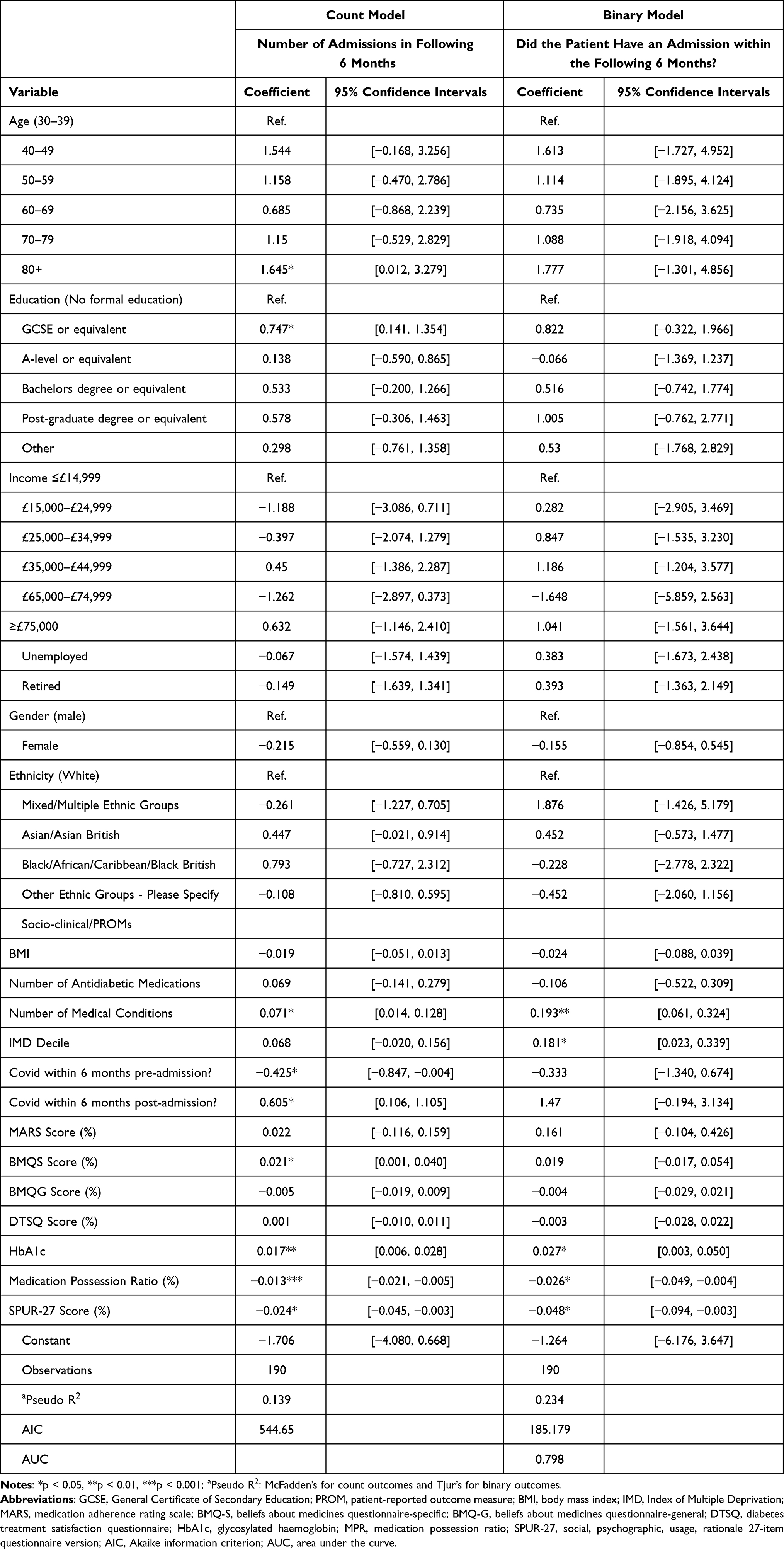 |
Table 3 Regression Model Results for Admissions in the 6-Month Follow-Up Period |
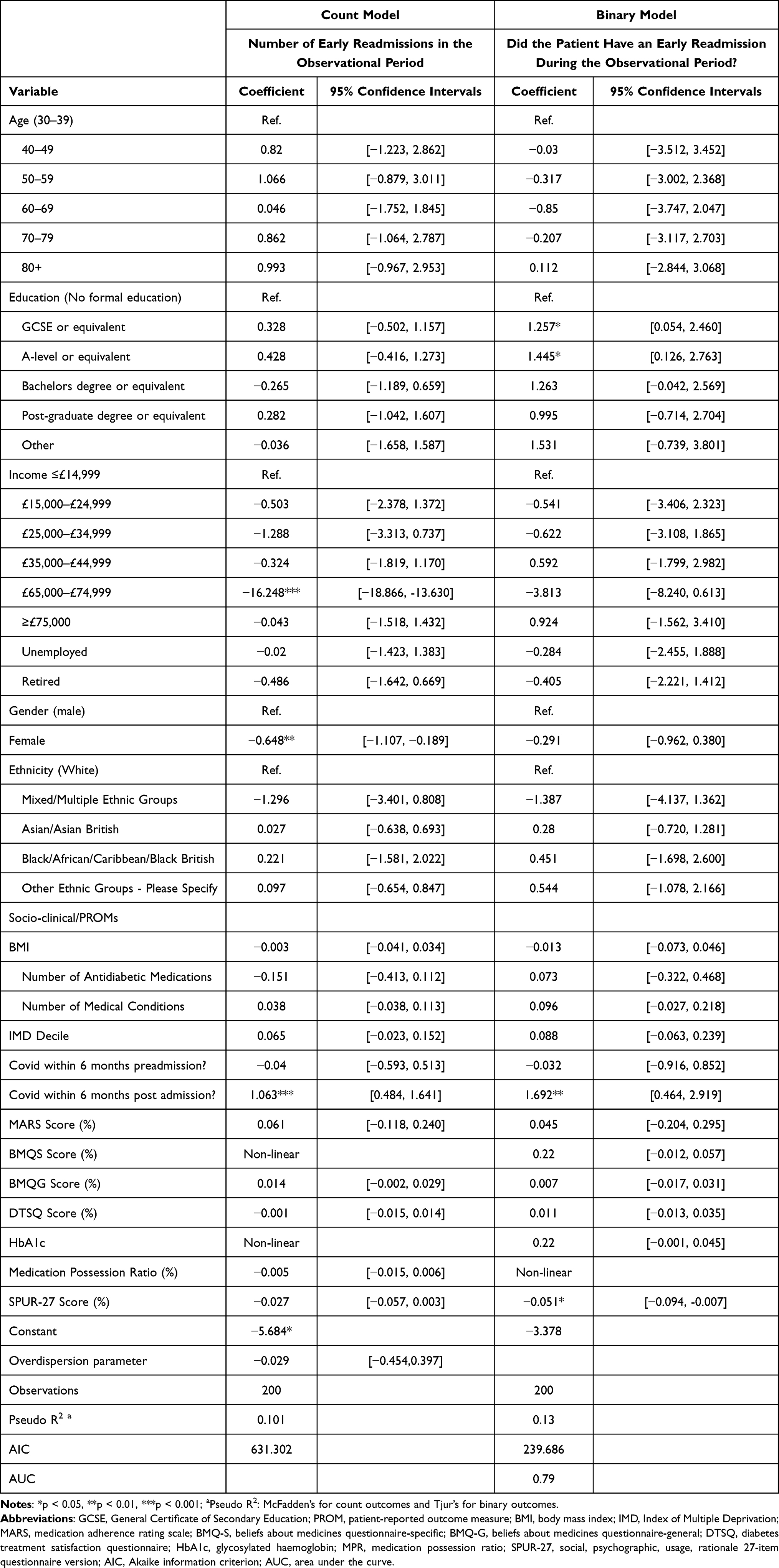 |
Table 4 Regression Model Results for Early Readmissions in the Observational Period |
With respect to early readmissions as a count outcome, only one factor, Covid-19 diagnosis in the 6-month follow-up period, was positively and significantly (IR = 2.90, 95% CI, [1.62, 5.16]) associated with the outcome (Table 4). Inverse associations were observed for patients identifying as female (IR = 0.52, 95% CI, [0.33, 0.83]), and those with an annual income of £65,000-£74,999. The coefficient of income £65,000-£74,999 is very large (−16.248) for the count outcome, suggesting an unrealistically large effect. As explained earlier, the main variable of interest in this study is SPUR-27 score and the purpose of adjusting other factors is to avoid confounding, so their effects should be treated as exploratory in nature. It is worth noting that the number of patients in each income category is very low: for example, there is only one patient with income of £65,000-£74,999 (Table 1), – this lower sample size (n = 1) makes the estimated effect highly unreliable (this participant happened to have zero early readmissions) so an artificially high effect. A larger sample size is required to better understand the impact of income. Both BMQ-S and HbA1c are found to have a statistically significant and non-linear relationship with the number of early readmissions. A Covid-19 diagnosis in the 6-month follow-up period continued to be a significant (1.692, 95% CI, [0.464, 2.919]) factor associated with early readmission in the binary model, in addition to patients reporting either a GCSE (1.257, 95% CI, [0.054, 2.460]) or A-level (or equivalent) education (1.445, 95% CI, [0.126, 2.763]). The SPUR-27 score was the only factor inversely associated with the binary outcome (−0.051, 95% CI, [−0.094, −0.007]), indicating that patients with a higher SPUR-27 score that were more adherent to their medicines were less likely to experience an early readmission in the observational period.
The calibration plots for the binary outcome models are presented in Figures 1 and 2. Both plots demonstrate that the model is reasonably well calibrated. However, further data external to the population for this study are required to validate the models.
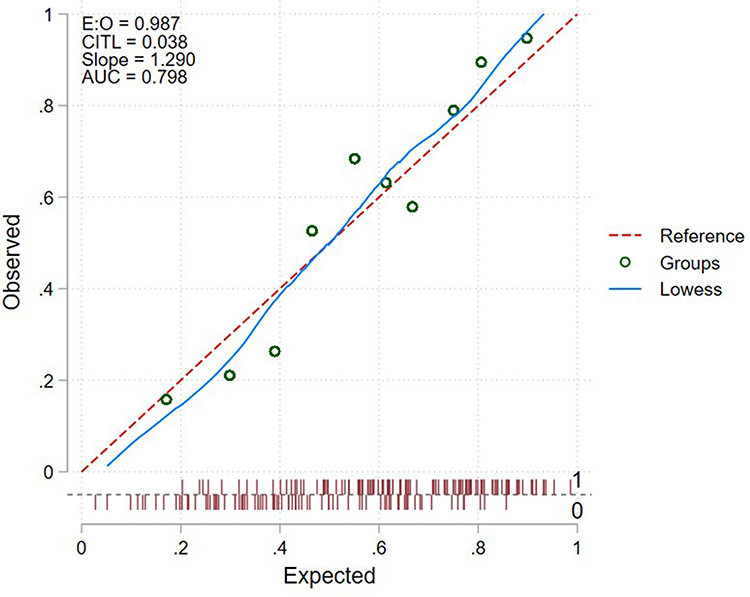 |
Figure 1 SPUR-27 Binary Outcome Model Calibration Plot: Did the patient have an admission within 6 months post-discharge?. Abbreviations: E:O, expected: observed ratio; CITL, calibration in the large index; AUC, area under the curve; LOWESS, locally weight scatterplot smoothing. Notes: E:O (Best = 1); CITL (Best = 0); All circles refer to the probability groups (Best = closer to the reference line). |
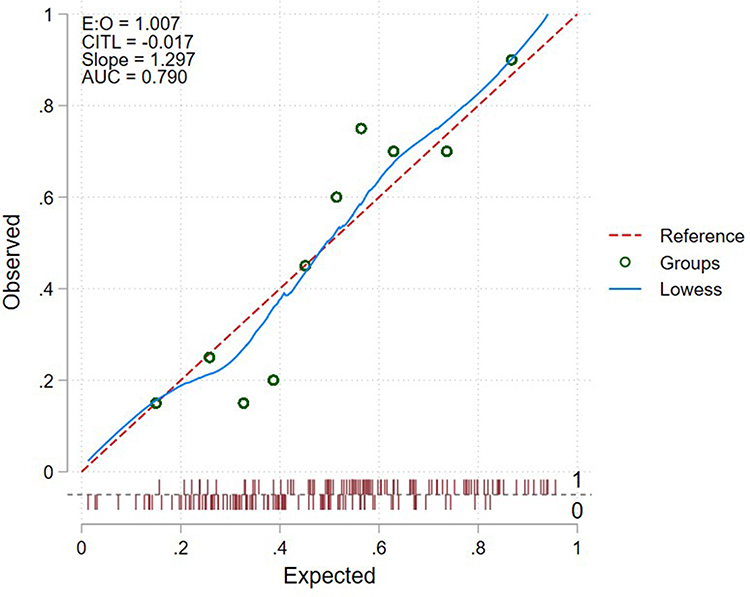 |
Figure 2 SPUR-27 Binary Outcome Model Calibration Plot: Did the patient have an early readmission within 6 months post-discharge?. Abbreviations: E:O, expected:observed ratio; CITL, calibration in the large index; AUC, area under the curve; LOWESS, locally weight scatterplot smoothing. Notes: E:O (Best = 1); CITL (Best = 0); All circles refer to the probability groups (Best = closer to the reference line). |
Discussion
This study sought to develop a predictive model of both general admission and early readmission in patients living with type 2 diabetes using SPUR-27, a novel holistic PROM of medication adherence, in addition to other socio-clinical factors associated with admission risk. The results provide early evidence of the predictive model, with SPUR-27 identified as a significant predictor of both general admission and early readmission.
In total, 425 admissions were recorded during the observational period. Over half of all recorded admissions were classified as early readmissions across a sample of 98 participants, providing an early readmission rate of 48% for this sample. This finding appears to be disproportionately high when compared to early readmission rates in similar sample populations of acute surgical or medical patients, including those with cardiometabolic disease with figures ranging from 7.6% to 19%.44–48 Covid-19 was considered as a potential factor that may explain this discrepancy given that 22% (n=44/200) of the sample reported a positive diagnosis within the observational period. However, similar samples of patients diagnosed with Covid-19 have reported readmission rates closer to ~7.5%.49,50 Participants for this study were broadly older (>70 years), observed poor adherence to HbA1c targets and their medicines, and reported a relatively high mean number of comorbidities (6.6 ± 2.7), hence one might justify some increase in readmission rates on these confounding factors. Conversely, this cohort of patients was found to be affluent in respect to their socio-economic status, therefore one could also argue that a lower readmission rate would be expected in this sample, particularly given the evidence that older patients (>65 years) from deprived areas are more prone to readmission.47 The very high proportion of early readmissions identified in this study certainly warrants further investigation given that the case for causality can neither be attributed to poor medication adherence alone, as identified by SPUR-27, nor any other obvious predictive factor.
Although this study was unable to provide a more definitive answer to explain the high proportion of early readmissions, it did successfully describe several factors associated with this outcome as part of the predictive model. Notably, the only factor positively associated with an early readmission in both the binary and count models was a Covid-19 diagnosis in the 6-month follow-up period. Several factors including type 2 diabetes, obesity, male gender, and being over the age of 65 have been linked to an increased risk of Covid-19 morbidity and mortality.51–54 Aside from type 2 diabetes as an inclusion criterion for this study, the sample was predominantly male (64%), >65 years of age, and overweight when classified using BMI. It is therefore not unexpected that this cohort would be more vulnerable to Covid-19 associated morbidity and mortality that might warrant additional admissions or readmissions within the observational period. Participants who reported their gender as female were significantly less likely than male participants to have an early readmission. This result is reaffirmed by the wider literature which demonstrates that male participants living with type 2 diabetes are more likely to be hospitalised and experience early readmissions.55,56 Although poorly explored in type 2 diabetes specifically, a few studies have highlighted that participants with lower levels of education have an increased risk of early readmission.57,58 When compared to participants without a formal education, patients with a Bachelor’s degree or higher did not observe a significantly increased risk of early readmission, however those who either reported a GCSE or A-level equivalent education were significantly more likely to experience this outcome. Finally, SPUR-27 was the only PROM to significantly predict the likelihood of an early readmission in the model. Similarly to Rosen et al,25 patients with higher levels of medication adherence were less likely to experience an early hospital readmission. Neither objective measure of adherence, MPR and HbA1c, demonstrated any significant association with the outcome variable. Holistic measures, such as SPUR-27, may therefore have an increasingly important role to play in identifying and tackling early readmission risk when compared to other standard PROMs and objective clinical measures.
As with the model of early readmission, a higher SPUR-27 score was also predictive of a lower general admission risk in this population. However, both MPR and HbA1c were also significant predictors of general admission in this model, in addition to one PROM, BMQ-S. Surprisingly, the BMQ-S score, which indicates that a patient recognises the necessity of their medicines as well as having low concerns about their potential long-term effects, was associated with an admission. To our knowledge, the BMQ-S has not been used as part of any similar predictive model for admission risk, hence no direct comparison could be drawn from the wider literature. It was hypothesised that the inverse relationship, if any, would be significant, especially given that high necessity and low concern with medicines have been associated with both improved adherence and lower health-care utilisation.59 Future studies with a larger sample are required to determine the validity of this result. Increasing age (>80 years), comorbidities, and a GCSE level of education were predictive of an admission in this model, however an unexpected factor of interest was a Covid-19 diagnosis in the 6-month prior to study participation, which was associated with a lower risk of admission. The authors previously outlined the role of Covid-19 diagnoses in admission and early readmission risk, particularly for this cohort of patients living with type 2 diabetes.52,53 One possible explanation may come from Nyland et al60 and their recent study investigating the initiation of type 2 diabetes treatments, including GLP-1R agonists, pioglitazone, and DPP-4 inhibitors in patients prior to a Covid-19 diagnosis. Most notably, those patients that received a GLP-1R agonist 6 months prior to their Covid-19 diagnosis observed a 33% reduction in hospitalisation. This study did not specifically investigate the initiation of novel therapies for participants either before or during the observational period and is therefore unable to comment on whether medicines such as GLP-1R agonists were prescribed retrospectively in this cohort. However, during the pandemic a “vulnerable” status was applied to people living with type 2 diabetes with respect to Covid-19. Patients may have been more cognizant of their risk and therefore increasingly likely to access healthcare and improve their medication adherence as a result, particularly both during or following a Covid-19 diagnosis, that may have inadvertently reduced the likelihood of a future hospital admission.
Models may be subject to unreliable risk estimates even when they report good discrimination.61 Furthermore, as emphasized by Van Calster and Vickers,62 a model with a lower AUC but better calibration may be more useful, particularly in the context of clinical decision-making. Both models observed an AUC close to ~0.8 as well as reasonable calibration. Further data are required for external validation; however, this early evidence of discrimination and calibration is encouraging for the development of a clinically relevant predictive model in patients living with type 2 diabetes that encompasses a holistic PROM of MA.
Although Firth’s penalized maximum likelihood estimator was employed in this study, the sample size was relatively small. Future external validation with a larger sample will help to address this potential limitation. Moreover, based on IMD, there was an overrepresentation of affluent patients within the sample, with 78.5% (n=157/200) reporting an IMD decile ≥6. In the binary general admission model, patients with a higher IMD decile (less deprivation) were more likely to experience an admission. This result contradicts the early readmission model that observed lower readmission risk in more affluent patients, as well as the wider literature.47 Therefore, although the sample was reflective of the local population, further evaluation with patients from a broader range of socioeconomic backgrounds and levels of deprivation should be conducted.
Conclusion
In summary, this study successfully developed a predictive model for both general admission and early readmissions in patients living with type 2 diabetes. The model also provided early evidence for SPUR-27, a holistic PROM of medication adherence, as a reliable predictor of both outcomes in the study population when compared to other PROMs and objective measures of medication adherence. This finding may have relevance for future work that can look to address the development of tailored intervention pathways based on admission risk among patients with poor medication adherence identified using SPUR-27 both in and out of hospital settings, such as community pharmacies, GP surgeries, nursing homes and domiciliary settings. Several other notable predictors of admission risk that have been previously associated with type 2 diabetes were also identified in the model including age, gender, multimorbidity and perhaps the most novel factor, Covid-19 diagnoses pre- and post-admission. These results add to the existing evidence base as well as highlighting the potential relationship between pre-Covid treatment initiation and reduced admission risk that warrants future exploration. Despite a small sample size, this study employed a number of statistical methods to improve both the performance and clinical relevance of the model, such as the Firth’s penalized estimator. Future work is required to conduct external validation of the model and to understand its applicability to broader and more diverse samples of patients living with type 2 diabetes.
Acknowledgments
The authors thank the Kingston Hospital NHS Foundation Trust research department, as well as the diabetes team for their support with this study during the Covid-19 pandemic. We would also like to give huge thank you to all the participants who supported this study, particularly when faced with the challenges of the Covid-19 pandemic.
Disclosure
KD reports being the General Manager of Observia. JW receives funding for his PhD via Observia, however he did not receive financial remuneration for this work. The authors report no other conflicts of interest in this work.
References
1. Haynes RB, McKibbon KA, Kanani R. Systematic review of randomised trials of interventions to assist patients to follow prescriptions for medications. Lancet. 1996;348(9024):383–386. doi:10.1016/S0140-6736(96)01073-2
2. Eduardo Sabaté (WHO/NMH/CCH). Adherence to Long-Term Therapies: Policy for Action. World Health Organization (WHO); 2001.
3. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. 2018;8:1. doi:10.1136/BMJOPEN-2017-016982
4. Timmerman L, Stronks DL, Groeneweg JG, Huygen FJ. Prevalence and determinants of medication non-adherence in chronic pain patients: a systematic review. Acta Anaesthesiol Scand. 2016;60(4):416–431. doi:10.1111/AAS.12697
5. Cheen MHH, Tan YZ, Oh LF, Wee HL, Thumboo J. Prevalence of and factors associated with primary medication non-adherence in chronic disease: a systematic review and meta-analysis. Int J Clin Pract. 2019;73(6):e13350. doi:10.1111/IJCP.13350
6. Chapman SCE, Horne R. Medication nonadherence and psychiatry. Curr Opin Psychiatry. 2013;26(5):446. doi:10.1097/YCO.0B013E3283642DA4
7. Crawshaw J, Auyeung V, Norton S, Weinman J. Identifying psychosocial predictors of medication non-adherence following acute coronary syndrome: a systematic review and meta-analysis. J Psychosom Res. 2016;90:10–32. doi:10.1016/J.JPSYCHORES.2016.09.003
8. Foley L, Larkin J, Lombard-Vance R, et al. Prevalence and predictors of medication non-adherence among people living with multimorbidity: a systematic review and meta-analysis. BMJ Open. 2021;11:44987. doi:10.1136/bmjopen-2020-044987
9. Fischer MA, Stedman MR, Lii J, et al. Primary medication non-adherence: analysis of 195,930 electronic prescriptions. J Gen Intern Med. 2010;25(4):284–290. doi:10.1007/S11606-010-1253-9/TABLES/5
10. Yeam CT, Chia S, Tan HCC, Kwan YH, Fong W, Seng JJB. A systematic review of factors affecting medication adherence among patients with osteoporosis. Osteoporos Int. 2018;29(12):2623–2637. doi:10.1007/S00198-018-4759-3
11. Seng JJB, Tan JY, Yeam CT, Htay H, Foo WYM. Factors affecting medication adherence among pre-dialysis chronic kidney disease patients: a systematic review and meta-analysis of literature. Int Urol Nephrol. 2020;52(5):903–916. doi:10.1007/S11255-020-02452-8
12. Mongkhon P, Ashcroft DM, Scholfield CN, Kongkaew C. Hospital admissions associated with medication non-adherence: a systematic review of prospective observational studies. BMJ Qual Saf. 2018;27(11):902–914. doi:10.1136/BMJQS-2017-007453
13. Vestbo J, Anderson JA, Calverley PMA, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/THX.2009.113662
14. Payero MÁ, Martínez López De CN, Samartín MU, Vila AM, Vázquez LC, Corrales GP. Medication non-adherence as a cause of hospital admissions. Farm Hosp. 2014;38(4):328–333. doi:10.7399/FH.2014.38.4.7660
15. Department of Health. Payment by Results Guidance for 2011–12 [Internet]; 2011. Available from: http://webarchive.nationalarchives.gov.uk/20130507170152/https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/151911/dh_126157.pdf.pdf.
16. Ruppar TM, Cooper PS, Mehr DR, Delgado JM, Dunbar-Jacob JM. Medication adherence interventions improve heart failure mortality and readmission rates: systematic review and meta-analysis of controlled trials. J Am Heart Assoc. 2016;5:6. doi:10.1161/JAHA.115.002606
17. Readdean KC, Heuer AJ, Scott Parrott J. Effect of pharmacist intervention on improving antidepressant medication adherence and depression symptomology: a systematic review and meta-analysis. Res Social Adm Pharm. 2018;14(4):321–331. doi:10.1016/J.SAPHARM.2017.05.008
18. Leguelinel-Blache G, Dubois F, Bouvet S, et al. Improving patient’s primary medication adherence: the value of pharmaceutical counseling. Medicine. 2015;94:41. doi:10.1097/MD.0000000000001805
19. Verloo H, Chiolero A, Kiszio B, Kampel T, Santschi V. Nurse interventions to improve medication adherence among discharged older adults: a systematic review. Age Ageing. 2017;46(5):747–754. doi:10.1093/AGEING/AFX076
20. Delgado-Silveira E, Vélez-Díaz-Pallarés M, Muñoz-García M, Correa-Pérez A, Álvarez-Díaz AM, Cruz-Jentoft AJ. Effects of hospital pharmacist interventions on health outcomes in older polymedicated inpatients: a scoping review. Eur Geriatr Med. 2021;12(3):509–544. doi:10.1007/S41999-021-00487-3
21. Bach QN, Peasah SK, Barber E. Review of the role of the pharmacist in reducing hospital readmissions. J Pharm Pract. 2019;32(6):617–624. doi:10.1177/0897190018765500
22. Granger BB, Bosworth HB. Medication adherence: emerging use of technology. Curr Opin Cardiol. 2011;26(4):279. doi:10.1097/HCO.0B013E328347C150
23. Gandapur Y, Kianoush S, Kelli HM, et al. The role of mHealth for improving medication adherence in patients with cardiovascular disease: a systematic review. Eur Heart J Qual Care Clin Outcomes. 2016;2(4):237–244. doi:10.1093/EHJQCCO/QCW018
24. Pal P, Sambhakar S, Dave V, et al. A review on emerging smart technological innovations in healthcare sector for increasing patient’s medication adherence. Global Health J. 2021;5(4):183–189. doi:10.1016/J.GLOHJ.2021.11.006
25. Rosen OZ, Fridman R, Rosen BT, Shane R, Pevnick JM. Medication adherence as a predictor of 30-day hospital readmissions. Patient Prefer Adherence. 2017;11:801–810. doi:10.2147/PPA.S125672
26. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. doi:10.1097/00005650-198601000-00007
27. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4). doi:10.4065/mcp.2010.0575
28. Gonzalez JS, Schneider HE. Methodological issues in the assessment of diabetes treatment adherence. Curr Diab Rep. 2011;11(6):472–479. doi:10.1007/S11892-011-0229-4
29. Wells J, Crilly P, Kayyali R, Systematic A. Analysis of reviews exploring the scope, validity, and reporting of patient-reported outcomes measures of medication adherence in type 2 diabetes. Patient Prefer Adherence. 2022;16:1941–1954. doi:10.2147/PPA.S375745
30. Mokkink Cecilia AC, Prinsen Donald L, Patrick Jordi LB, Mokkink CL. COSMIN Study Design checklist for Patient-reported outcome measurement instruments. Available from: www.cosmin.nl.
31. Dolgin K. The SPUR model: a framework for considering patient behavior. Patient Prefer Adherence. 2020;14. doi:10.2147/PPA.S237778
32. Tugaut B, Shah S, Dolgin K, et al. Development of the SPUR tool: a profiling instrument for patient treatment behavior. J Patient Rep Outcomes. 2022;6(1):1–10. doi:10.1186/S41687-022-00470-X
33. de Bock E, Dolgin K, Arnould B, Hubert G, Lee A, Piette JD. The SPUR adherence profiling tool: preliminary results of algorithm development. Curr Med Res Opin. 2021;38(2):171–179. doi:10.1080/03007995.2021.2010437
34. Bock E, Dolgin K, Kombargi L, et al. Finalization and validation of questionnaire and algorithm of SPUR, a new adherence profiling tool. Patient Prefer Adherence. 2022;16:1213–1231. doi:10.2147/PPA.S354705
35. Wells JS, Husseini A, Okoh S, et al. SPUR: psychometric properties of a patient-reported outcome measure of medication adherence in type 2 diabetes. BMJ Open. 2022;12(9):e058467. doi:10.1136/BMJOPEN-2021-058467
36. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and Elaboration. PLoS Med. 2007;4(10):e297. doi:10.1371/JOURNAL.PMED.0040297
37. Little M, Jordens CFC, Paul K, Montgomery K, Philipson B. Liminality: a major category of the experience of cancer illness. J Bioeth Inq. 2022;19(1):37–48. doi:10.1007/S11673-022-10175-X/METRICS
38. Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating Scale (Mars) for the psychoses. Schizophr Res. 2000;42:3. doi:10.1016/S0920-9964(99)00130-9
39. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47:6. doi:10.1016/S0022-3999(99)00057-4
40. Bradley C, Lewis KS. Measures of psychological well‐being and treatment satisfaction developed from the responses of people with tablet‐treated diabetes. Diabetic Med. 1990;7:5. doi:10.1111/j.1464-5491.1990.tb01421.x
41. Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and cox regression. Am J Epidemiol. 2007;165(6):710–718. doi:10.1093/AJE/KWK052
42. van Calster B, van Smeden M, de Cock B, Steyerberg EW. Regression shrinkage methods for clinical prediction models do not guarantee improved performance: simulation study. Stat Methods Med Res. 2020;29(11):3166–3178. doi:10.1177/0962280220921415
43. Ahmadipour H, Farajzadegan Z, Kachoei A, Pirdehghan A. Secondary prevention by enhancing adherence in diabetic patients. Int J Prev Med. 2010;1:1. doi:10.4103/ijpvm.IJPVM_302_16
44. Wang H, Zhao T, Wei X, Lu H, Lin X. The prevalence of 30-day readmission after acute myocardial infarction: a systematic review and meta-analysis. Clin Cardiol. 2019;42(10):889–898. doi:10.1002/CLC.23238
45. Kwok CS, Wong CW, Shufflebotham H, et al. Early readmissions after acute myocardial infarction. Am J Cardiol. 2017;120(5):723–728. doi:10.1016/J.AMJCARD.2017.05.049
46. Conway R, Byrne D, O’Riordan D, Silke B. Outcomes in acute medicine - Evidence from extended observations on readmissions, hospital length of stay and mortality outcomes. Eur J Intern Med. 2019;66:69–74. doi:10.1016/J.EJIM.2019.06.001
47. Shebehe J, Hansson A. High hospital readmission rates for patients aged ≥65 years associated with low socioeconomic status in a Swedish region: a cross-sectional study in primary care. Scand J Prim Health Care. 2018;36(3):300–307. doi:10.1080/02813432.2018.1499584
48. Rubin DJ, Recco D, Turchin A, Zhao H, Golden SH. External validation of the diabetes early re-admission risk indicator (Derri TM). Endocr Pract. 2018;24(6):527–541. doi:10.4158/EP-2018-0035
49. Huang CW, Desai PP, Wei KK, Liu ILA, Lee JS, Nguyen HQ. Characteristics of patients discharged and readmitted after COVID-19 hospitalisation within a large integrated health system in the United States. Infect Dis. 2021;53(10):800–804. doi:10.1080/23744235.2021.1924398
50. Nematshahi M, Soroosh D, Neamatshahi M, Attarian F, Rahimi F. Factors predicting readmission in patients with COVID-19. BMC Res Notes. 2021;14(1):1–6. doi:10.1186/S13104-021-05782-7
51. Huang R, Zhuid L, Xue L, et al. Clinical findings of patients with coronavirus disease 2019 in Jiangsu province, China: a retrospective, multi-center study. PLoS Negl Trop Dis. 2020;14(5):e0008280. doi:10.1371/JOURNAL.PNTD.0008280
52. Yeo I, Baek S, Kim J, et al. Assessment of thirty-day readmission rate, timing, causes and predictors after hospitalization with COVID-19. J Intern Med. 2021;290(1):157–165. doi:10.1111/JOIM.13241
53. Zheng Z, Peng F, Xu B, et al. Risk factors of critical & mortal COVID-19 cases: a systematic literature review and meta-analysis. J Infect. 2020;81(2):e16–e25. doi:10.1016/J.JINF.2020.04.021
54. Kwok S, Adam S, Hoong HJ, et al. Obesity: a critical risk factor in the COVID-19 pandemic. Clin Obes. 2020;10(6):e12403. doi:10.1111/COB.12403
55. Collins J, Abbass IM, Harvey R, et al. Predictors of all-cause 30 day readmission among Medicare patients with type 2 diabetes. Curr Med Res Opin. 2017;33(8):1517–1523. doi:10.1080/03007995.2017.1330258
56. Comino EJ, Harris MF, Islam MDF, et al. Impact of diabetes on hospital admission and length of stay among a general population aged 45 year or more: a record linkage study. BMC Health Serv Res. 2015;15(1):1–13. doi:10.1186/S12913-014-0666-2
57. Rubin DJ. Hospital readmission of patients with diabetes. Curr Diab Rep. 2015;15(4):1–9. doi:10.1007/S11892-015-0584-7
58. Rubin D, Handorf E, McDonnell M. predicting early readmission risk among hospitalized patients with diabetes. Diabetes & Obesity Management; 2013. Available from: https://endo.confex.com/endo/2013endo/webprogram/Paper7796.html.
59. Salgado T, Marques A, Geraldes L, Benrimoj S, Horne R, Fernandez-Llimos F. Cross-cultural adaptation of the beliefs about medicines questionnaire into Portuguese. Sao Paulo Med J. 2013;131(2):88–94. doi:10.1590/S1516-31802013000100018
60. Nyland JE, Raja-Khan NT, Bettermann K, et al. Diabetes, drug treatment, and mortality in COVID-19: a multinational retrospective cohort study. Diabetes. 2021;70(12):2903–2916. doi:10.2337/DB21-0385
61. van Calster B, McLernon DJ, van Smeden M, et al. Calibration: the Achilles heel of predictive analytics. BMC Med. 2019;17(1):1–7. doi:10.1186/S12916-019-1466-7
62. van Calster B, Vickers AJ. Calibration of risk prediction models: impact on decision-analytic performance. Med Decision Mak. 2015;35(2):162–169. doi:10.1177/0272989X14547233/ASSET/IMAGES/LARGE/10.1177_0272989X14547233
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors and Predictive Model for Dermatomyositis Associated with Rapidly Progressive Interstitial Lung Disease
Wang K, Tian Y, Liu S, Zhang Z, Shen L, Meng D, Li J
Pharmacogenomics and Personalized Medicine 2022, 15:775-783
Published Date: 1 September 2022
Construction of a Nomogram-Based Prediction Model for the Risk of Diabetic Kidney Disease in T2DM
Wang X, Liu X, Zhao J, Chen M, Wang L
Diabetes, Metabolic Syndrome and Obesity 2024, 17:215-225
Published Date: 12 January 2024
Cost-Savings Associated with Multi-Disciplinary Team Approach for Reducing Macrovascular and Microvascular Complications in Patients with Type 2 Diabetes: A Predictive Model
Alshowair A, Altamimi S, Alruhaimi FA, Alshahrani S, Alsuwailem F, Alkhaldi M, Abdalla H, Alkhuraiji FH, Alaqeel MS, Almureef SS, Alhawasy S, Abdel-Azeem A
ClinicoEconomics and Outcomes Research 2024, 16:211-223
Published Date: 4 April 2024
Development and Validation of a Machine Learning-Based Predictive Model for Peripheral Neuropathy Risk in Elderly Patients with Type 2 Diabetes
Peng J, Xue D, Li J, Wei L, Wang Y
Risk Management and Healthcare Policy 2026, 19:573535
Published Date: 8 January 2026