Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Cost-Savings Associated with Multi-Disciplinary Team Approach for Reducing Macrovascular and Microvascular Complications in Patients with Type 2 Diabetes: A Predictive Model
Authors Alshowair A ![]() , Altamimi S, Alruhaimi FA, Alshahrani S
, Altamimi S, Alruhaimi FA, Alshahrani S ![]() , Alsuwailem F, Alkhaldi M, Abdalla H, Alkhuraiji FH, Alaqeel MS, Almureef SS, Alhawasy S, Abdel-Azeem A
, Alsuwailem F, Alkhaldi M, Abdalla H, Alkhuraiji FH, Alaqeel MS, Almureef SS, Alhawasy S, Abdel-Azeem A ![]()
Received 25 November 2023
Accepted for publication 26 March 2024
Published 4 April 2024 Volume 2024:16 Pages 211—223
DOI https://doi.org/10.2147/CEOR.S451739
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Abdulmajeed Alshowair,1 Saleh Altamimi,1 Faisal A Alruhaimi,1 Saad Alshahrani,2 Fatima Alsuwailem,3 Mona Alkhaldi,4 Haiam Abdalla,5 Fahad Hamad Alkhuraiji,6 Montaser Saad Alaqeel,6 Salman Sulaiman Almureef,7 Salman Alhawasy,8 Amro Abdel-Azeem3,9
1Community Health Excellence, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 2Academic and Training Affairs, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 3Population Health Management and Research, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 4Health Administration Office, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 5Model of Care, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 6Financial Affairs, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 7Cost Department, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 8Reporting Department, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 9Department of Community, Environmental and Occupational Medicine, Faculty of Medicine Zagazig University, Zagazig, Egypt
Correspondence: Amro Abdel-Azeem, Population Health Management and Research, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia, Tel +966547135224, Email [email protected]
Purpose: This study aims to predict the expected cost savings associated with implementing a multidisciplinary team (MDT) approach to reduce macrovascular and microvascular complications among patients with type 2 diabetes mellitus (T2DM).
Methods: This economic evaluation study was conducted in Riyadh First Health Cluster, Saudi Arabia as a predictive model conceptualized by the authors based on models used in previous studies, particularly the CORE Diabetes Model. Our model was designed based on 1) the level of glycemic control among 24,755 T2DM patients served by MDTs; 2) the expected incidence of diabetes-related complications without intervention; 3) the predicted risk reduction of developing diabetes-related complications with MDTs. Costs of complications and cost savings were then calculated and expressed as mean incremental annual cost savings adjusted for a 1% reduction in HbA1c, and a 10 mmHg reduction in systolic blood pressure (SBP).
Results: Along with the expected reduction in all diabetes-related complications, the average incremental cost savings per diabetic patient is predicted to be ($38,878) with approximately ($11,108) in the year of complication onset and ($27,770) over the subsequent post-index 10-years. On adjustment of cost savings, the average incremental cost savings are predicted to be ($22,869) for each 1% reduction in HbA1c per diabetic patient and ($27,770) for every 10 mmHg reduction in SBP per diabetic patient.
Conclusion: MDT as a model of care is effective in glycemic control among T2DM patients with a predicted significant reduction of all diabetes-related complications and in turn, a predicted significant cost savings.
Keywords: cost-savings, multi-disciplinary team, complications, type 2 diabetes, predictive model
Introduction
Diabetes has grown over the past few decades as one of the most life-threatening chronic diseases, resulting in costly complications, and increasing the burden on both individuals and the healthcare system.1 The prevalence of diabetes worldwide has been estimated in 2021 to be over 10.5% (536.6 million people), with the expectation to reach 12.2% (783.2 million) by 2045.2
The Kingdom of Saudi Arabia (KSA) has approximately seven million diabetic cases. KSA was rated by the World Health Organization (WHO) as the second-highest country in the Middle East and the seventh worldwide regarding the prevalence of diabetes.3 Around ninety percent of all cases of diabetes are Type 2 diabetes mellitus (T2DM).4,5 The increasing prevalence of diabetes in KSA is primarily resulting from population aging, advancing urbanization, and significant shifts in lifestyle in the direction of lack of exercise, increased obesity, rising smoking, high blood pressure, and unhealthy nutrition.6–8
Poor glycemic control may lead to serious macrovascular and microvascular complications including cardiovascular disease (CVD), stroke, diabetic nephropathy, diabetic retinopathy, and diabetic neuropathy (DN).9–13 The majority of those with diabetes have a minimum of one co-morbidity, and about forty percent of them have at least three co-morbidities.14 Proper control of hyperglycemia is projected to prevent or postpone the development and worsening of macrovascular and microvascular consequences of diabetes.15,16
The global health expenditures related to diabetes had been estimated at 966 billion USD in 2021 and are anticipated to increase to 1054 billion USD in 2045.2 Among the Gulf Cooperation Council (GCC) nations, The KSA recorded the highest diabetes-related expenses consuming nearly 21% of its total health expenses on the care of diabetic patients compared to 16% and 19% in other GCC.17 Inpatient care for macrovascular and microvascular complications of diabetes accounted for proximity 43% of the overall healthcare expenses of diabetes, according to the American Diabetes Association’s (ADA) estimate of the direct healthcare expenses of diabetes in 2017.11,18
Multi-Disciplinary Team (MDT) approach has been implemented in many countries that are faced with an increasing burden of cost caring for an increasing population with chronic diseases.19 Several studies concluded that using multidisciplinary teams, as a model of care delivery, was associated with improved glycemic control and a major reduction in the cumulative incidence of complications related to diabetes with a significant reduction in healthcare costs.7,20–23
Many previous studies, utilizing a variety of models, revealed that interventions to prevent or delay the complications of T2DM are translated into cost savings in healthcare expenditures.4,5,8,10–12,15 The CORE Diabetes Model (CDM) is a validated and updated model that includes risk equations based on long-term follow-up. CDM represents one of the best options for modeling complication incidence and evaluating health economic outcomes among diabetics.15,24
Globally, there is an insistent desire of nations, policymakers, and health economists to reduce the economic burden of diabetes and its related complications’ costs.8 Therefore, this study was conducted to predict the expected cost savings associated with implementing a multidisciplinary team approach for reducing the macrovascular and microvascular complications among T2DM patients.
Methods
Study Design and Setting
This economic evaluation study is conceptualized as a predictive model for expected cost savings from the expected reduction in macrovascular and microvascular complications related to T2DM after the application of the MDT approach for improving care and follow-up of chronic diseases, especially diabetics. Riyadh First Health Cluster (RFHC), in KSA, started in 2020 to provide the case manager-led MDT approach among its primary healthcare centers. From 2020 up to 2023, a total number of 24,755 patients with uncontrolled T2DM (HbA1c >8%) received care and were followed up every three months by MDTs throughout RFHC. Our study included the final analysis reports for regular measurements of some health metrics that reflect the level of glycemic control among these 24,755 diabetic patients (HbA1c and systolic blood pressure). Another hypothetical comparator group was considered in our analysis and was assumed to receive ordinary care for patients with T2DM.
Assessment of MDT Approach Outcomes
The effectiveness of the MDT approach was assumed to be a reduction of 1.7% in HbA1c and a reduction of 14 mmHg in Systolic Blood Pressure (SBP) based on three analyzed annual reports of medical affairs in RFHC from 2020 to 2023. Glycemic control was estimated firstly at baseline as HbA1c concentration and SBP measurement and then every 3 months over time with an updated mean of annual HbA1c and SBP measurements. At baseline, all served T2DM patients with uncontrolled diabetes had poor glycemic control (HbA1c >8%).
Conceptualization of Predictive Model of Risk Reduction
Our predictive model was innovated and conceptualized by the authors as a combination of a variety of cost-minimization and cost-saving estimation models used in previous studies to assess interventions to prevent or delay the complications of T2DM, particularly the CORE Diabetes Model (CDM).4,5,8,10–12,15,24 This predictive model is based on two main items 1) the expected cumulative incidence of diabetes-related complications among the hypothetical comparative group without the MDT approach; 2) the predicted risk reduction of developing diabetes-related complications among our 24,755 T2DM patients served by the MDT approach. Figure 1 illustrates the full structure of our model and the steps followed.
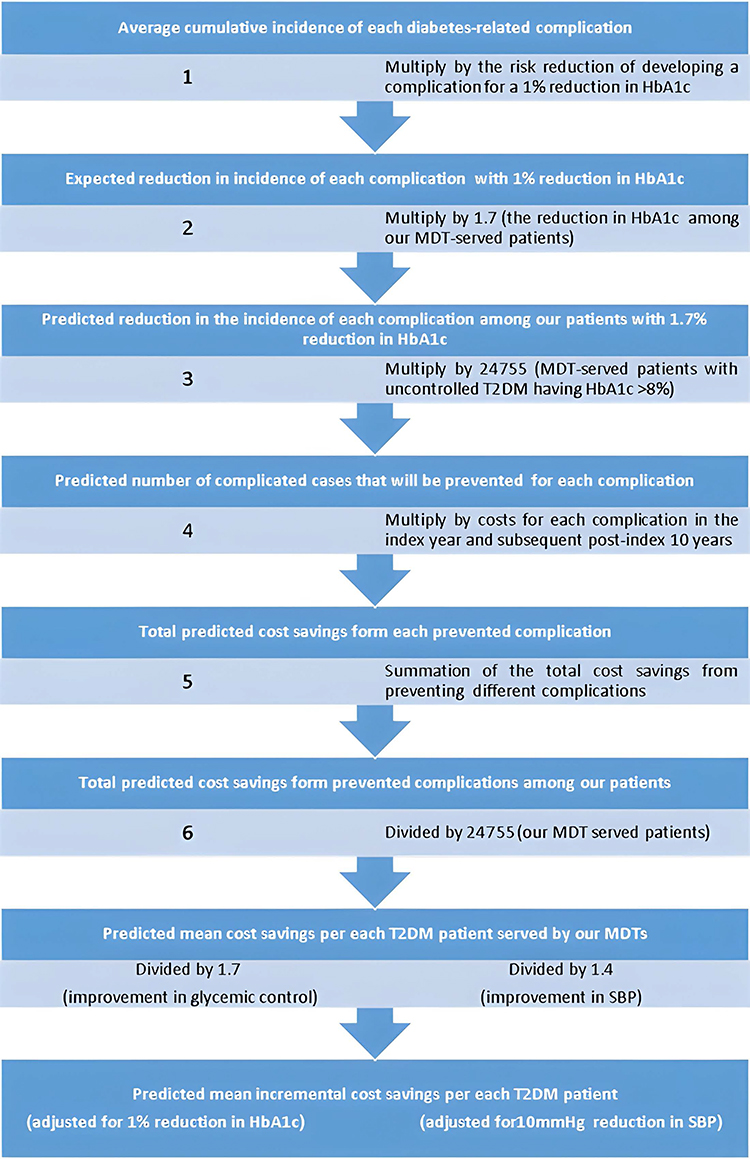 |
Figure 1 Our predictive model structure. Abbreviations: MDT, multidisciplinary team; SBP, systolic blood pressure. |
First, we estimated the average cumulative incidence of macrovascular and microvascular complications related to diabetes from the previously published relevant literature on diabetic patients receiving ordinary medical care.6,14,15,25–29
In addition, we reviewed the previously published relevant literature to estimate the average risk reduction of developing such macrovascular and microvascular complications because of proper glycemic control using the reference case of a 1% reduction in HbA1c.12,15,30–34
Second, we estimated the predicted risk reduction in such complications among our patients served by the MDT approach. This was calculated by multiplying (the average risk reduction of developing such complications per a 1% reduction in HbA1c) by 1.7 (the average reduction in HbA1c among our patients under the MDT approach).
Finally, we predicted the total number of complicated cases that will be prevented with the MDT approach by multiplying (the predicted risk reduction in the occurrence of such complications among our patients after the MDT approach) by 24,755 (the total number of patients served by the MDT approach).
Calculation of Cost Savings
We calculated the magnitude of cost differences that may arise from differences in complication incidence between both the MDT and hypothetical groups. Costs were estimated for each pair during the index year of complication, as well as the subsequent post-index 10 years. The costs included the cost of different secondary-care activities and other atypical activities (eg dialysis, amputation, physiotherapy, and prosthetics). The final costs presented in this model were exchanged for US dollars inflated to 2023 values.
First, the Financial Support Group in RFHC (FSG-RFHC) calculated the total annual costs per case, in Saudi Riyal (SR), for each diabetes-related complication pertaining to medications, procedures, consultations, and services during the year of onset of the complication event. These calculations are based on the data from 1) the five-year projects by the Strategy Planning Office at the KSA Ministry of Health, 2) the operating expenses analysis report, 3) the Center of Spending Efficiency, and 4) the price list of Saudi Medical Cities. The costs for each complication were estimated depending on the following assumptions (The average cost of one-day hospital admission Including surgery = 6465 SR; day hospital admission does not include surgery = 5479 SR; one-session Hemodialysis dialysis: = 1282 SR “3 times a week”; one-session physiotherapy = 500 SR; stent = 5000 SR per piece; 15,000–70,000 SR average for Orthotics and Prosthetics (Saudi Medical Cities Rate)). However, the costs of some complications in the subsequent post-index 10 years were estimated from the previously published relevant literature assuming a uniform distribution (ie, equal costs of complications in each post-index year).4,5,15 No discounting was calculated as we assume this constant cost pattern, aiming to determine the lowest predicted cost minimization estimates and be more precise.21
Second, the cost savings, from the reduced risk of developing each complication, were calculated by multiplying (The total costs from each complication) by (the predicted number of reduced complicated cases with the MDT approach). Then, all-complication healthcare costs resulted from the sum of total costs from each complication. All costs are adjusted to 2023 US dollars using a currency converter depending on the Saudi Central Bank price exchange rates for foreign currencies (1 USD = 3.75 SR).
Finally, we conducted a microsimulation analysis of mean incremental annual costs among both the MDT and hypothetical groups. The mean incremental cost savings were calculated by adjusting the total cost savings from the reduction in complication rates to the number of T2DM patients, a 1% reduction in HbA1c, and a 10 mmHg reduction in SBP (Figure 2).
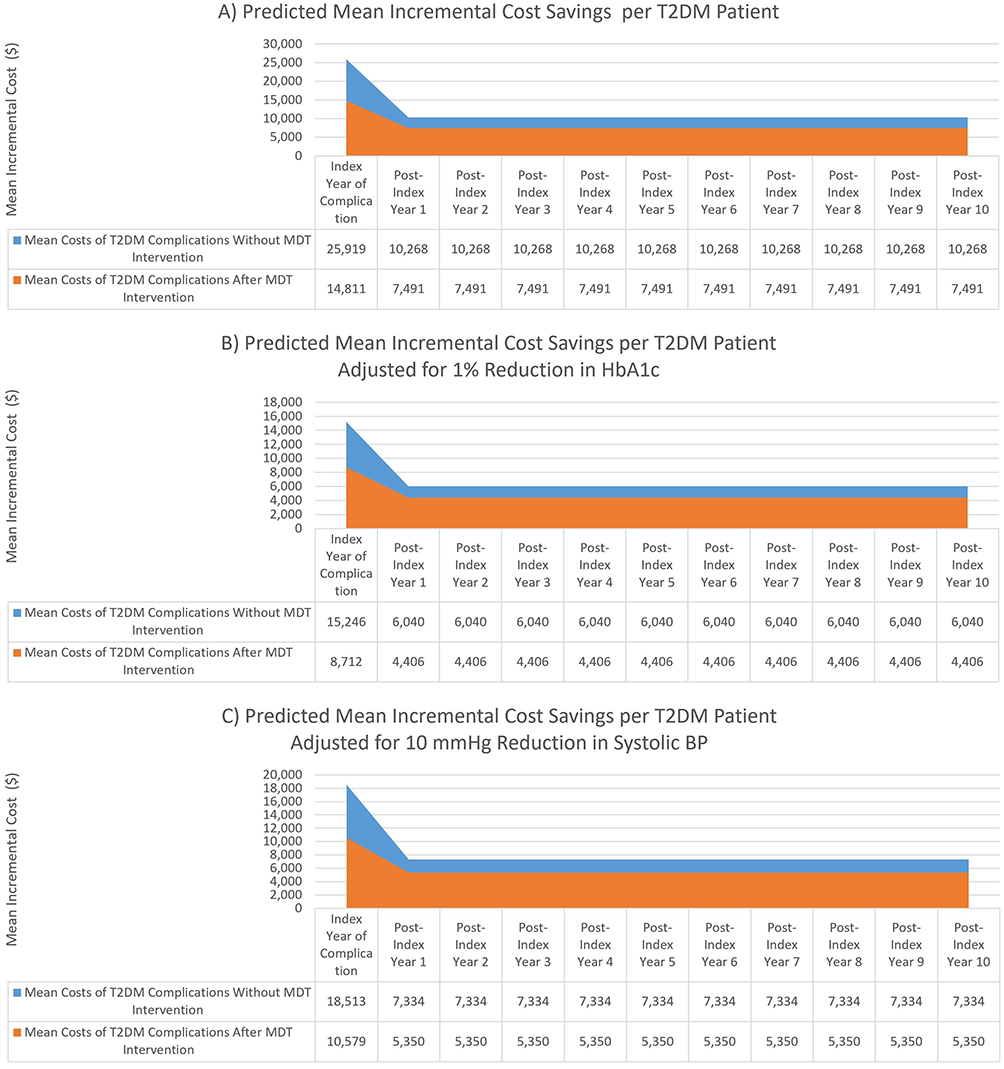 |
Figure 2 Microsimulation analysis of predicted annual mean incremental cost savings of the multi-disciplinary team approach over 10 years: (A) per T2DM patient; (B) per T2DM patient adjusted for 1% Reduction in HbA1c; (C) per T2DM patient adjusted for 10 mmHg reduction in SBP. Abbreviations: SBP, systolic blood pressure; T2DM, type 2 diabetes mellitus. |
Statistical Analysis
Data from RFHC annual reports were extracted and analyzed using SPSS version 21 software. Data were summarized and their descriptive were displayed statistics as the mean and standard deviation for (HbA1c and SBP), and as the proportions and percentages for (complication incidence and predicted risk reduction). Costs, total cost savings, and incremental cost savings were calculated and expressed in both Saudi Riyals and USD. A hierarchical algorithm was used to identify the reduction in the number of individuals with T2DM-related complications then the predicted cost savings were calculated (Figure 1). The algorithm depends on the improvements in A1C level and SB pressure (reported in Table 1); the cumulative incidence of diabetes-related complications and the predicted risk reduction with MDT intervention (reported in Table 2); and the costs associated with each macrovascular or microvascular diabetes-related complication as per case (reported in Table 3). If a T2DM subject has intervention, the model does not allow the progression of full risk ratios of developing microvascular or macrovascular complications but does allow the progression of the reduced risk ratios for such complications (reported in Table 4). All complications annual cost comparisons were conducted along a hypothesized 11 years of follow-up (the year of complication, post-index year 1 to 10) between T2DM patients intervened by MDT and their hypothetical matched controls of T2DM patients without intervention (Figure 2).
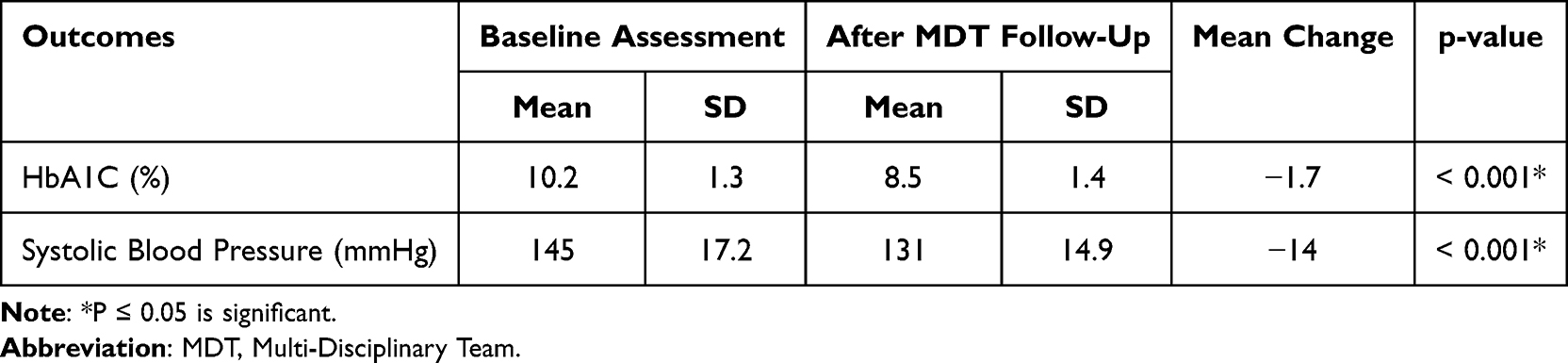 |
Table 1 Impact of Multidisciplinary Team Approach on Glycemic Control and Blood Pressure Control Among Managed T2DM Patients (N=24755) |
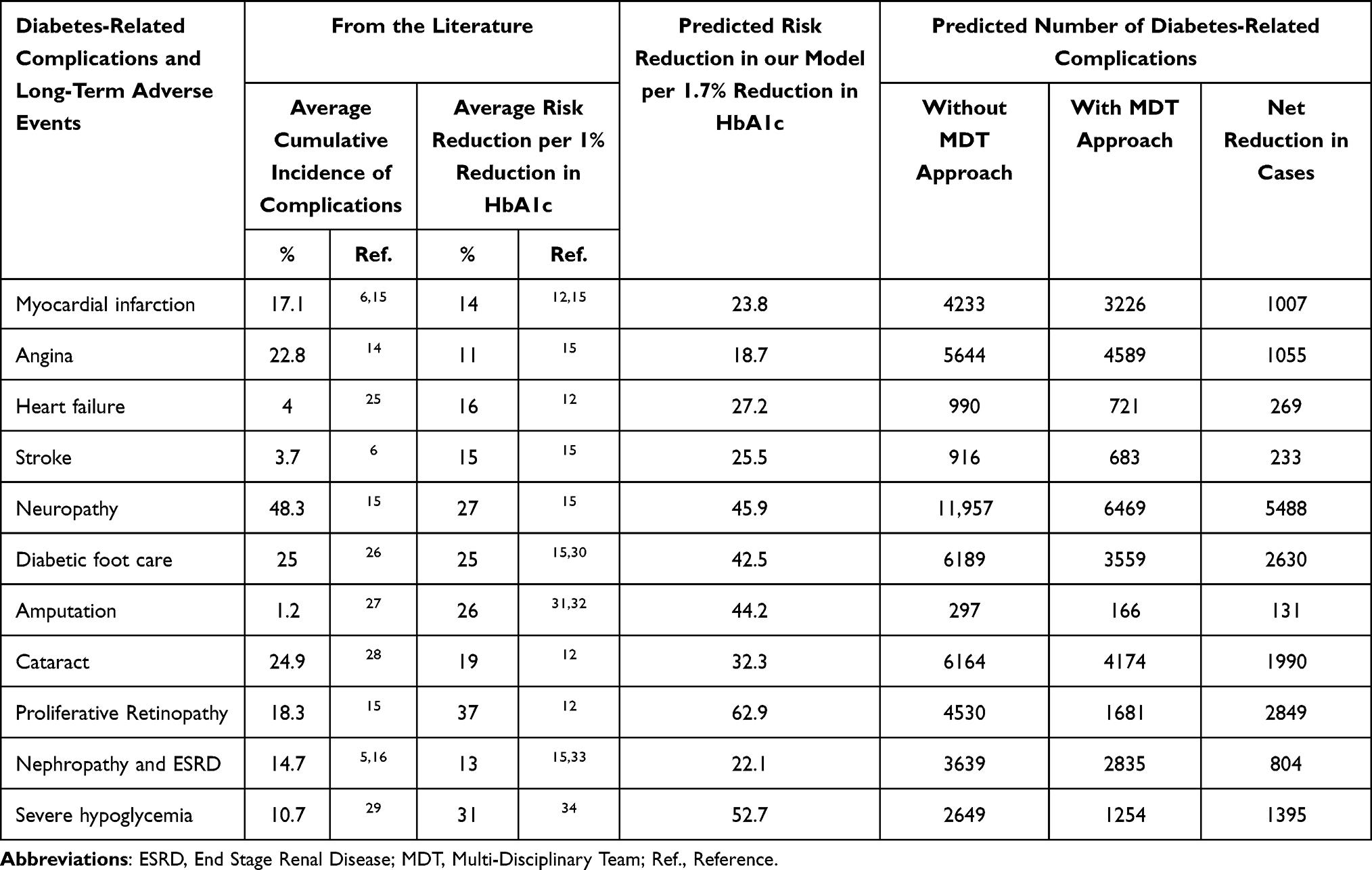 |
Table 2 Predictive Model for the Incidence and Risk Reduction of Complications per 1.7% Reduction in HbA1c Among T2DM Patients Managed by Multidisciplinary Team Approach |
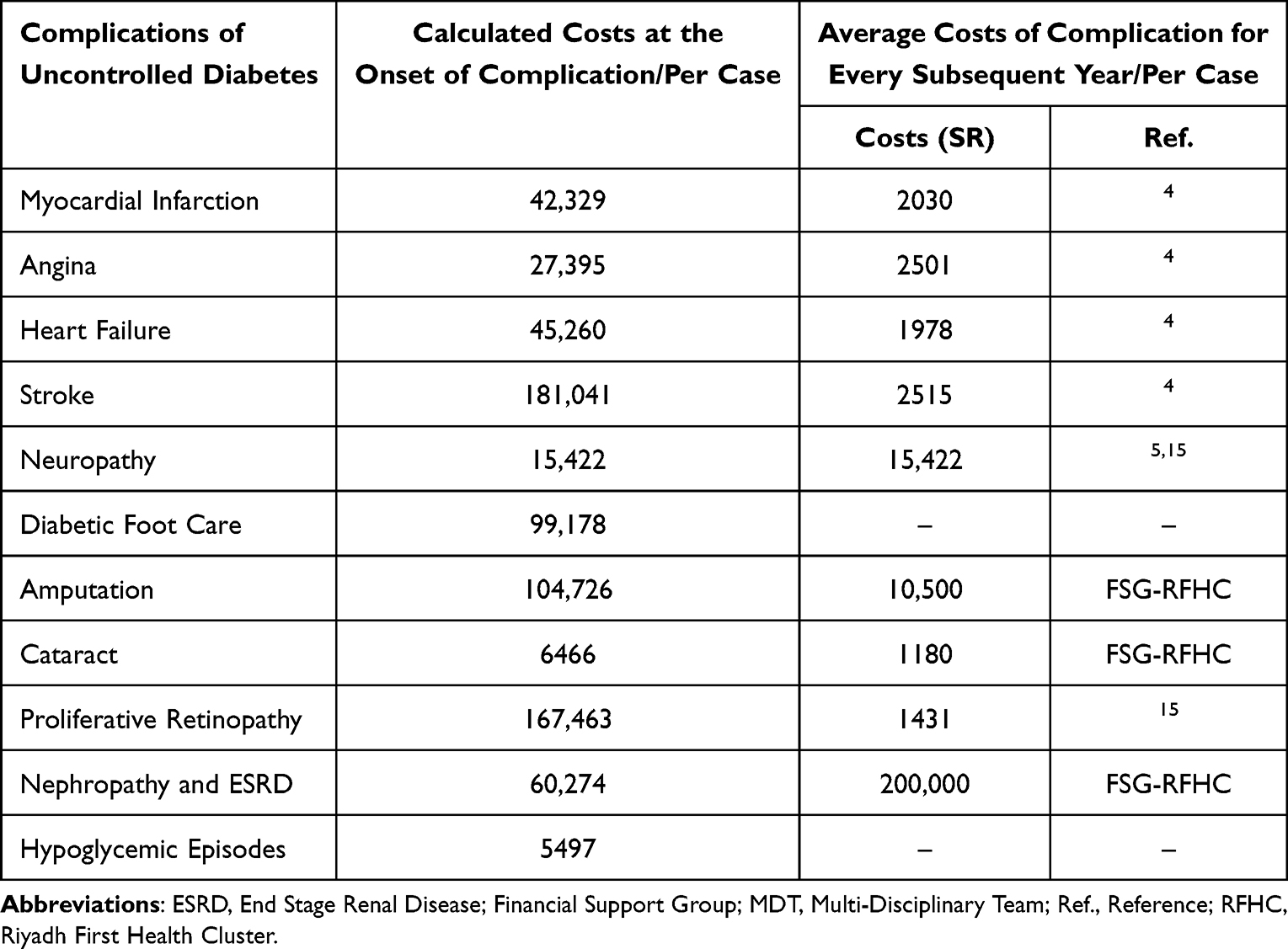 |
Table 3 Costs Associated with Macrovascular and Microvascular Complications of Diabetes per Case |
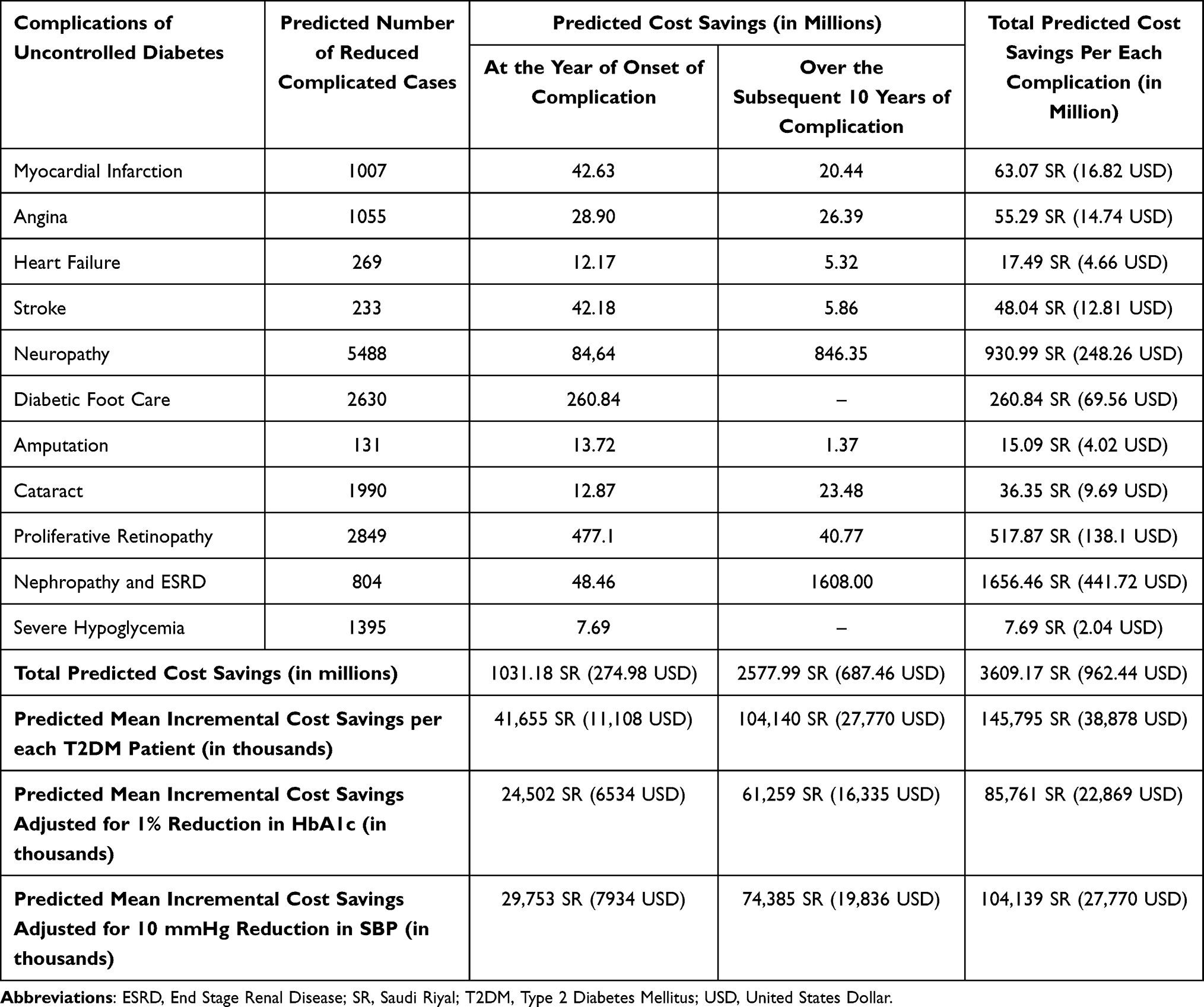 |
Table 4 Predicted Cost Savings Associated with the Implementation of Multidisciplinary Team Approach Among 24,755 T2DM Patients |
Results
The recorded improvements in the glycemic control and systolic blood pressure control of 24,755 patients with uncontrolled T2DM, who were managed by MDT approach, are included in the final analysis of our study. Table 1 summarizes the differences between the baseline and final levels of both HbA1c and systolic blood pressure after MDT intervention. There is a significant reduction in the mean levels of HbA1c from 10.2% to 8.5% (−1.7%, p < 0.001) and systolic BP from 145 mmHg to 131 mmHg (−14 mmHg, p < 0.001).
Among our cohort of 24,755 patients with T2DM, who were Managed by Multi-Disciplinary Team Approach, we predict a risk reduction in all diabetes-related complications. The risk of CVDs and stroke related to diabetes is predicted to be reduced by (18.7% for angina, 23.8% for Myocardial Infarction (MI), 27.2% for Heart Failure (HF), and 25.5% for stroke) respectively. In addition, the risk of diabetic neuropathy and its subsequent adverse events are predicted to be reduced by (45.9% for diabetic peripheral neuropathy (DPN), 42.5% for diabetic foot (DF), and 44.2% for amputation) respectively. As regards other microvascular complications, we predicted a risk reduction of 62.9% for proliferative retinopathy, 32.3% for cataracts, and 22.1% for nephropathy. In our predictive model, we will expect the MDT intervention to prevent almost 1007 MI events, 1055 cases of angina, 269 cases of HF, 233 stroke events, 5488 neuropathy cases, 2630 cases of DF, 131 amputations, 1990 cases of cataracts, 2849 retinopathy cases, 804 cases of ESRD and 1395 severe hypoglycemia events (Table 2).
Table 3 displays the calculated costs for each diabetes-related complication during the year of the complication event and predicted costs for each year following the complication. The highest costs for a complication during the index year are observed in stroke, retinopathy, amputation, DF, and nephropathy (181, 167, 104, 99, and 60 thousand SR), respectively. However, for each subsequent post-index year, the costs are higher among cases of ESRD, neuropathy, and amputation.
As shown in Table 4, the results of our predictive model expect a total cost savings of $962.44 million from the reduction in both macrovascular and microvascular complications related to diabetes during the year of complication onset ($274.98 million) and along the subsequent post-index10-years ($687.46 million). The vast majority of cost savings are related to the prevention of microvascular complications (Nephropathy, neuropathy, and retinopathy). Along with the expected reduction in all diabetes-related complications, the average incremental cost savings per diabetic patient is predicted to be ($38,878) with approximately ($11,108) in the year of complication onset and ($27,770) over the subsequent post-index 10-years. On adjustment of cost savings, the average incremental cost savings are predicted to be ($22,869) for each 1% reduction in HbA1c per diabetic patient and ($27,770) for every 10 mmHg reduction in SBP per diabetic patient.
Figure 2 illustrates the results of the microsimulation analysis of the incremental costs of diabetes-related complications. The mean incremental costs, in the year of complication and in each post-index year, are expected to be reduced to ($14,811 and $7491) per diabetic patient enrolled in MDT intervention versus ($25,919 and $10,268) among patients receiving usual care. When these complication costs are adjusted for a 1% Reduction in HbA1c, the mean incremental costs associated with the diabetes complications are expected to be reduced to ($8712 and $4406) with the MDT intervention instead of ($15,246 and $6040) without the MDT approach. On the other hand, for each reduction of 10 mmHg in SBP, we expect to reduce the mean incremental costs of diabetes complications from ($18,513 and $7334) to ($10,579 and $5350) after receiving MDT care.
Discussion
Multi-Disciplinary Team approach is implemented in many countries for better control of patients with T2DM and to improve their health outcomes.35 Our study revealed that T2DM patients, who were followed by MDTs, expressed a significant reduction in their mean levels of HbA1c and systolic blood pressure by approximately - 1.7% and 1.4 mmHg, respectively. This implies the significant impact of MDT approach in improving glycemic control among such patients, which in turn will significantly reduce the incidence of diabetes-related complications. In agreement with our study, several studies concluded that MDT approach significantly reduces the mean HbA1C with nearly the same average of our detected levels with a significant reduction in cardiovascular risks among T2DM patients.7,20–22 However, Tourkmani et al observed a better impact of MDT approach on glycemic control with more reduction in mean HbA1c levels (−3.7%) than that detected in our study.23 On the other hand, Christopher et al36 and Ismail et al37 noticed no significant impact of MDT approach in either reducing the mean HbA1c, improving glycemic control, or other secondary health outcomes among T2DM patients. This controversy in HbA1c reduction among different studies may be attributed to the differences in relative glycemic control at the baseline and the follow-up duration.
In the present study, our simulation model predicted a significant risk reduction in all diabetes-related complications because of proper glycemic control associated with MDT approach compared to the hypothetical non-interventional group. This predictive analysis expected that the 1.7% reduction in HbA1c, among 24,755 T2DM patients, will be associated with a risk reduction of 18.7% for angina, 23.8% for MI, 27.2% for HF, 25.5% for stroke, 45.9% for neuropathy, 42.5% for diabetic foot, and 44.2% for amputation, respectively. However, microvascular complications are predicted to be reduced by 62.9% for retinopathy, 32.3% for cataracts, and 22.1% for nephropathy. This is supported by the findings of several studies, which concluded that reduced HbA1c was associated with a marked risk reduction of microvascular complications, while less risk reduction was reported for MI, angina, HF, and stroke. Jendle et al revealed that with a 0.8% reduction in HbA1c, there were an average of 14% risk reduction in different cardiovascular disease complications and an average of 26% risk reduction in microvascular complications.15 In addition, Stratton et al suggested a 37% risk reduction for microvascular complications and a 21% risk reduction of endpoint events related to diabetes, and a 16% risk reduction in MI, for each 1% reduction in HbA1c.12 However, in a 5-year study of Wan et al, they reported that using MDT approach for care of 53,436 T2DM patients in primary care setting reduced the risk of diabetes-related cardiovascular disease complications by 56.6%, and microvascular complications by 11.9%.38
The microsimulation analysis in our predictive model expects marked cost savings ($962.44 million) because of the reduction in the costs associated with all diabetes-related macrovascular and microvascular complications over 10 years among 24,755 T2DM patients. Approximately, $274.98 million of these cost savings are expected to be during the year of complication onset and about $687.46 million in the subsequent post-index 10-years. That represents an average incremental cost savings of $38,878 per each T2DM Patient served by the MDT approach over a period of 10 years. When these cost savings are adjusted for the purpose of standardization, this model predicts an average incremental cost savings of $22,869 for each 1% reduction in HbA1c and $27,770 for each 10 mmHg reduction in SBP per each T2DM Patient.
Many relevant studies, among T2DM patients, showed similar temporal cost patterns and revealed that interventions to prevent or delay the complications of diabetes are translated into cost savings in healthcare expenditures.5,8,11,15,39–41
American Diabetes Association (ADA) stated that the expenditures on diabetes are 2.3 folds that of non-diabetics. They estimated the total cost to be $327 billion per year with an average of $16,750 per year for every diabetic patient.18 Jendle et al15 revealed that a 0.8% Reduction in HbA1c would be associated with reducing the costs of diabetes complications from $72,152 in the reference cohort to $63,429 in the intervention group with a net reduction of $8722. Visaria et al11 estimated the mean annual healthcare cost of all diabetes complications among uncontrolled T2DM patients to be approximately two and a half times more than controlled ($21,745 vs $8524) during the year of complication and about one and half times In post-index years ($13,761 vs $8669). Further, Afroz et al stated that proper glycemic control in T2DM patients is associated with significant cost savings through the prevention and control of complications. They detected higher healthcare costs (1.8-fold) among patients with diabetes-related complications compared to those with good glycemic control.41 On the contrary, Singh et al in India found that the majority of diabetes care costs (78%) were driven by outpatient care and medications costs. However, there is no significant difference in the costs of in-patient hospitalizations due to cardiovascular or microvascular complications.10 Siegel et al, in their systematic review, concluded that MDT interventions for T2DM patients and proper glycemic control are highly cost-effective ($11,339/QALY) in comparison with usual care.40 Moreover, Egede et al42 suggested Incremental cost-effectiveness ratios (ICERs) of $1000-$4000 per 1% reduction in HbA1c among multi-component diabetes interventions.
Our study revealed that the reduced risk of developing microvascular complications is predicted to account for the majority of these cost savings through the prevention of nephropathy and associated ESRD ($441.72 million); neuropathy and its subsequent adverse events ie DF and amputation ($321.84 million); and retinopathy ($138.1 million). However, the cost savings, from cardio-vascular and stroke risk reduction, are predicted to be ($16.82 million from MI, $14.74 million from angina, $4.66 million from HF, and $12.81 million from stroke).
In agreement with our study, Zhou et al43 found that more than a third of complications’ costs were attributable to severe diabetic nephropathy, primarily due to the expense of hemodialysis. Despite it could be anticipated that those suffering from severe nephropathy would account for the highest percentage of inpatient admissions (86.7%), also patients with severe neuropathy and severe retinopathy had high percentages of inpatient stays (79.9% and 69.4%), respectively.5 Once more, these findings support our results. Approximately half of T2DM patients develop diabetic nephropathy, and 20% out of them are severe cases.44 Chapman et al5 estimated the mean costs of £8700 per T2DM patient with severe DN and £3900 for moderate DPN, which is 13-fold that for patients without neuropathy. However, Sadosky et al45 reported total annual medical costs of $12,492 for mild DPN, $27,93 for moderate DPN, and $30,755 for severe DPN. Nearly 25% of diabetic patients will develop a diabetic foot ulcer during their lifetime, and 5% of them may have foot amputation.27 The management of diabetic foot represents an economic burden. Lu et al calculated the total costs of foot care by $5981 per patient in 2020.26 Al-Thaniet al estimated the direct procedure and therapeutic costs of foot amputation to be $59 847 and $29 961 per patient respectively with a total cost of $89 808 per amputation.32
Around 68–80% of T2DM patients experienced a minimum of one CVD incident and CRF during their lifetime, and 19–31% of them experienced multiple CVD complications.4 In accordance with a cross-sectional study done in Gulf, CKD (44.3%) and CVD (17.3%) were the most frequently linked to T2DM.46
According to findings from a retrospective claims database analysis, patients with T2DM experienced higher medical costs for cardiovascular care during initial hospitalization than patients without diabetes.4 Additionally, numerous studies have shown that CVD incidents have a considerable impact on overall and diabetes-related healthcare expenses.15,47,48
Our results verify the additional economic burden these complications possess on healthcare resources. They emphasize the necessity of glycemic control and the reduction of diabetes-related complications, as the lower the incidence of complications the more cost savings. Notably, this is the first study in the Middle East of this sort as a predictive model to expect the future cost savings associated with proper glycemic control by the MDT approach and reduction in macrovascular and microvascular complications related to diabetes.
Implication for Practices
There is not enough national data in KSA to make definitive claims given the few studies on the economic evaluation of diabetes-related complications and cost savings of diabetes interventional programs. Therefore, the findings of our study may be used at the national level as a reference and benchmark to predict future cost savings from different intervention programs for diabetes, depending on one of our two adjusted mean incremental cost savings per diabetic patient for either each 1% reduction of HbA1c or each 10 mmHg reduction in SBP. This can be calculated using one of the following two equations: First equation (Total number of T2DM patients managed by the program X average reduction in HbA1c X our mean incremental cost savings per diabetic patient for each 1% reduction of HbA1c); Second equation (Total number of T2DM patients managed by the program X average reduction in SBP X our mean incremental cost savings per diabetic patient for each 10 mmHg reduction in SBP). These reference values will help policymakers in prioritization of various diabetes-related interventions and planning more comprehensive cost-effective healthcare for T2DM patients.
Limitations of the Study
One limitation of this study is that the cost assumptions for diabetes-related complications may be conservative for many reasons. First, due to rare data on the costs of diabetes complications in KSA, and second, some of the cost data used in our analysis depended on the literature. Moreover, our analysis did not include indirect costs related to diabetes such as decreased productivity and increased absenteeism. Another limitation is that we assume the constant costs of diabetes complications over the post-index 10 years without discounting, which is not actually true as the costs of care will increase over the years.21 However, we assume this constant cost pattern, aiming to predict more precise slightly lower cost estimates. In addition, the calculated cost saving only implies the reduction in overall cost without considering the broader evaluation of effect parameters. Actually, cost saving is not the same as cost-effectiveness that still a limitation in calculating the cost evaluation. In this study, we only calculate the average incremental cost saving per case, which is acceptable. However, we did not perform the incremental cost, incremental effect or incremental cost-effectiveness ratio (ICER). Finally, the cost estimates in this study depend on the national level in KSA, so the generalization of these estimates on other countries should be done with caution, as costs of healthcare are variable from one country to another.
Conclusion
MDT model of care is found to be very effective in glycemic control among T2DM patients with a predicted significant reduction of all diabetes-related complications and in turn, a predicted significant cost savings. This study adds to the scarce evidence on economic evaluation of T2DM in KSA; however, authors emphasize future research should focus on estimating the long-term costs of T2DM-related complications from a broader perspective and the ICER of various diabetes-related interventions that already exist. Decision makers are highly recommended to build on our findings and benefit from our calculated adjusted incremental cost savings in their future planning.
Abbreviations
CDM, CORE Diabetes Model; CVD, Cardiovascular Disease; DF, Diabetic Foot; DN, Diabetic Neuropathy; ESRD, End-Stage Renal Disease; FSG, Financial Support Group; GCC, Gulf Cooperation Council; ICER, Incremental Cost-Effectiveness Ratio; KSA, Kingdom of Saudi Arabia; MDT, Multi-Disciplinary Team; Ref., Reference; RFHC, Riyadh First Health Cluster; SBP, Systolic Blood Pressure; SR, Saudi Riyal; T2DM, Type 2 Diabetes Mellitus; USD, United States Dollar; WHO, World Health Organization.
Ethical Statement
Our study is based on the analyzed annual reports of RFHC, previously published data, cost calculations, and the outputs of a predictive simulation model. Since the authors in this work did not interact with, interview, or intervene with human or animal subjects, approval from Institutional Review was not required. We confirm that all research procedures comply with the declaration of Helsinki.
Author Contributions
All authors made a significant contribution to this study whether in the conception and design of the idea for the article, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work. This research did not receive any specific funding and only the publication charges were paid by our institution (RFHC).
References
1. Magliano DJ, Chen L, Islam RM, et al. Trends in the incidence of diagnosed diabetes: a multicountry analysis of aggregate data from 22 million diagnoses in high-income and middle-income settings. Lancet Diabetes Endocrinol. 2021;9(4):203–211. doi:10.1016/S2213-8587(20)30402-2
2. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
3. Alwin Robert A, Abdulaziz Al Dawish M, Braham R, Ali Musallam M, Abdullah Al Hayek A, Hazza Al Kahtany N. Type 2 diabetes mellitus in Saudi Arabia: major challenges and possible solutions. Current Diabetes Rev. 2017;13(1):59–64. doi:10.2174/1573399812666160126142605
4. Al-Jedai AH, Almudaiheem HY, Alissa DA, et al. Cost of cardiovascular diseases and renal complications in people with type 2 diabetes mellitus in the Kingdom of Saudi Arabia: a retrospective analysis of claims database. PLoS One. 2022;17(10):e0273836. doi:10.1371/journal.pone.0273836
5. Chapman D, Foxcroft R, Dale-Harris L, et al. Insights for care: the healthcare utilisation and cost impact of managing type 2 diabetes-associated microvascular complications. Diabetes Ther. 2019;10(2):575–585. doi:10.1007/s13300-018-0548-4
6. Alramadan MJ, Magliano DJ, Alhamrani HA, et al. Lifestyle factors and macro-and micro-vascular complications among people with type 2 diabetes in Saudi Arabia. Diabetes Metabol Syndr. 2019;13(1):484–491. doi:10.1016/j.dsx.2018.11.007
7. Alotaibi YK, Al-Nowaiser N, Al Harbi TJ, Tourkmani AM, Moharram M. Improving type 2 diabetes mellitus management in Ministry of Defense Hospitals in the Kingdom of Saudi Arabia 2018–2021. BMJ Open Qual. 2023;12(2):e002037. doi:10.1136/bmjoq-2022-002037
8. Alhowaish AK. Economic costs of diabetes in Saudi Arabia. J Fam Community Med. 2013;20(1):1. doi:10.4103/2230-8229.108174
9. Iglay K, Hannachi H, Joseph Howie P, et al. Prevalence and co-prevalence of comorbidities among patients with type 2 diabetes mellitus. Curr Med Res Opin. 2016;32(7):1243–1252. doi:10.1185/03007995.2016.1168291
10. Singh K, Kondal D, Menon VU, et al. Cost-effectiveness of a multicomponent quality improvement care model for diabetes in South Asia: the CARRS randomized clinical trial. Diabetic Med. 2023;40(9):e15074. doi:10.1111/dme.15074
11. Visaria J, Iyer NN, Raval AD, et al. Healthcare costs of diabetes and microvascular and macrovascular disease in individuals with incident type 2 diabetes mellitus: a ten-year longitudinal study. Clinicoecon Outcomes Res. 2020;12:423–434. doi:10.2147/CEOR.S247498
12. Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–412. doi:10.1136/bmj.321.7258.405
13. Zhao H, Shu L, Huang W, Wang W, Song G. Difference analysis of related factors in macrovascular and microvascular complications in Chinese patients with Type 2 diabetes mellitus: a case-control study protocol. Diabetes Metabol Syndr Obes. 2019;12:2193–2200. doi:10.2147/DMSO.S213848
14. Akın S, Bölük C. Prevalence of comorbidities in patients with type–2 diabetes mellitus. Prim Care Diabetes. 2020;14(5):431–434. doi:10.1016/j.pcd.2019.12.006
15. Jendle J, Ericsson Å, Hunt B, Valentine WJ, Pollock RF. Achieving good glycemic control early after onset of diabetes: a cost-effectiveness analysis in patients with type 1 diabetes in Sweden. Diabetes Ther. 2018;9(1):87–99. doi:10.1007/s13300-017-0344-6
16. Sun B, Luo Z, Zhou J. Comprehensive elaboration of glycemic variability in diabetic macrovascular and microvascular complications. Cardiovas Diabetol. 2021;20(1):1–13. doi:10.1186/s12933-020-01200-7
17. Ellahham S. Diabetes and its associated cardiovascular complications in the Arabian Gulf: challenges and Opportunities. J Clin Exp Cardiolog. 2020;11(1):1–5.
18. American Diabetes Association. Economic costs of diabetes in the U.S. in 2017. Diabetes Care. 2018;41(5):917–928. doi:10.2337/dci18-0007
19. Hudon C, Chouinard MC, Diadiou F, Lambert M, Bouliane D. Case management in primary care for frequent users of health care services with chronic diseases: a qualitative study of patient and family experience. Ann Fam Med. 2015;13(6):523–528. doi:10.1370/afm.1867
20. Alramadan MJ, Magliano DJ, Almigbal TH, et al. Glycaemic control for people with type 2 diabetes in Saudi Arabia-an urgent need for a review of management plan. BMC Endocr Disord. 2018;18(1):62. doi:10.1186/s12902-018-0292-9
21. van Wier MF, Lakerveld J, Bot SD, Chinapaw MJ, Nijpels G, van Tulder MW. Economic evaluation of a lifestyle intervention in primary care to prevent type 2 diabetes mellitus and cardiovascular diseases: a randomized controlled trial. BMC Fam Pract. 2013;14(1):1–10. doi:10.1186/1471-2296-14-45
22. Alshowair A, Altamimi S, Alshahrani S, et al. Effectiveness of case manager led multi-disciplinary team approach on glycemic control amongst T2DM patients in primary care in Riyadh: a retrospective follow-up study. J Prim Care Community Health. 2023;14:1–8. doi:10.1177/21501319231204592
23. Tourkmani AM, Abdelhay O, Alkhashan HI, et al. Impact of an integrated care program on glycemic control and cardiovascular risk factors in patients with type 2 diabetes in Saudi Arabia: an interventional parallel-group controlled study. BMC Fam Pract. 2018;19(1):1. doi:10.1186/s12875-017-0677-2
24. Palmer AJ, Roze S, Valentine WJ, et al. The CORE Diabetes Model: projecting long-term clinical outcomes, costs and cost effectiveness of interventions in diabetes mellitus (types 1 and 2) to support clinical and reimbursement decision-making. Curr Med Res Opin. 2004;20(sup1):S5–S26. doi:10.1185/030079904X1980
25. Tashtish N, Al-Kindi SG, Oliveira GH, Robinson MR. Length of stay and hospital charges for heart failure admissions in the United States: analysis of the national inpatient sample. J Card Fail. 2017;23(8):S59. doi:10.1016/j.cardfail.2017.07.166
26. Lu Q, Wang J, Wei X, et al. Cost of diabetic foot ulcer management in China: a 7-year single-center retrospective review. Diabetes Metabol Syndr Obes. 2020;13:4249. doi:10.2147/DMSO.S275814
27. Budiman-Mak E, Epstein N, Brennan M, et al. Systolic blood pressure variability and lower extremity amputation in a non-elderly population with diabetes. Diabetes Res Clin Pract. 2016;114:75–82. doi:10.1016/j.diabres.2016.01.010
28. Kiziltoprak H, Tekin K, Inanc M, Goker YS. Cataract in diabetes mellitus. World J Diabetes. 2019;10(3):140. doi:10.4239/wjd.v10.i3.140
29. Samya V, Shriraam V, Jasmine A, et al. Prevalence of hypoglycemia among patients with type 2 diabetes mellitus in a rural health center in South India. J Prim Care Community Health. 2019;10:2150132719880638. doi:10.1177/2150132719880638
30. Alsaigh SH, Alzaghran RH, Alahmari DA, Hameed LN, Alfurayh KM, Alaql KB. Knowledge, awareness, and practice related to diabetic foot ulcer among healthcare workers and diabetic patients and their relatives in Saudi Arabia: a cross-sectional study. Cureus. 2022;14(12). doi:10.7759/cureus.32221
31. Walicka M, Raczyńska M, Marcinkowska K, et al. Amputations of lower limb in subjects with diabetes mellitus: reasons and 30-day mortality. J Diabetes Res. 2021;2021:1–8. doi:10.1155/2021/8866126
32. Al-Thani H, Sathian B, El-Menyar A. Assessment of healthcare costs of amputation and prosthesis for upper and lower extremities in a Qatari healthcare institution: a retrospective cohort study. BMJ open. 2019;9(1):e024963. doi:10.1136/bmjopen-2018-024963
33. Adler AI, Stratton IM, Neil HA, et al. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study. BMJ. 2000;321(7258):412–419. doi:10.1136/bmj.321.7258.412
34. Morales J, Schneider D. Hypoglycemia. Am j Med. 2014;127(10):S17–S24. doi:10.1016/j.amjmed.2014.07.004
35. Ni Y, Liu S, Li J, et al. The effects of nurse-led multidisciplinary team management on glycosylated hemoglobin, quality of life, hospitalization, and help-seeking behavior of people with diabetes mellitus. J Diabetes Res. 2019;9. doi:10.1155/2019/9325146
36. Celano CM, Gianangelo TA, Millstein RA, et al. A positive psychology-motivational interviewing intervention for patients with type 2 diabetes: proof-of-concept trial. Int J Psychiatry Med. 2019;54(2):97–114. doi:10.1177/0091217418791448
37. Ismail K, Winkley K, de Zoysa N, et al. Nurse-led psychological intervention for type 2 diabetes: a cluster randomised controlled trial (Diabetes-6 study) in primary care. Br J Gen Pract. 2018;68(673):531–540. doi:10.3399/bjgp18X696185
38. Wan EYF, Fung CSC, Jiao FF, et al. Five-year effectiveness of the multidisciplinary risk assessment and management programme diabetes mellitus (RAMP-DM) on diabetes-related complications and health service uses-a population-based and propensity-matched cohort study. Diabetes Care. 2018;41(1):49–59. doi:10.2337/dc17-0426
39. Singh K, Narayan KMV, Eggleston K. Economic impact of diabetes in South Asia: the magnitude of the problem. Curr Diab Rep. 2019;19(6):34. doi:10.1007/s11892-019-1146-1
40. Siegel KR, Ali MK, Zhou X, et al. Cost-effectiveness of interventions to manage diabetes: has the evidence changed since 2008? Diabetes Care. 2020;43(7):1557–1592. doi:10.2337/dci20-0017
41. Afroz A, Chowdhury HA, Shahjahan M, Hafez MA, Hassan MN, Ali L. Association of good glycemic control and cost of diabetes care: experience from a tertiary care hospital in Bangladesh. Diabetes Res Clin Pract. 2016;120:142–148. doi:10.1016/j.diabres.2016.07.030
42. Egede LE, Walker RJ, Dismuke-Greer CE, et al. Cost-effectiveness of financial incentives to improve glycemic control in adults with diabetes: a pilot randomized controlled trial. PLoS One. 2021;16(3):e0248762. doi:10.1371/journal.pone.0248762
43. Zhou Z, Chaudhari P, Yang H, et al. Healthcare resource use, costs, and disease progression associated with diabetic nephropathy in adults with type 2 diabetes: a retrospective observational study. Diabetes Ther. 2017;8(3):555–571. doi:10.1007/s13300-017-0256-5
44. Owolabi LF, Alghamdi M, Adamu B, et al. Magnitude of diabetic peripheral neuropathy in Saudi Arabia: a systematic review and meta-analysis. BMC Endocr Disord. 2022;22(1):1–12. doi:10.1186/s12902-022-01167-4
45. Sadosky A, Mardekian J, Parsons B, Hopps M, Bienen EJ, Markman J. Healthcare utilization and costs in diabetes relative to the clinical spectrum of painful diabetic peripheral neuropathy. J Diabetes Complications. 2015;29(2):212–217. doi:10.1016/j.jdiacomp.2014.10.013
46. Al-Ozairi E, Jallo MK, Hafidh K, et al. Prevalence of cardiovascular and renal co-morbidities in patients with type 2 diabetes in the gulf, a cross-sectional observational study. Diabetes Ther. 2021;12(4):1193–1207. doi:10.1007/s13300-021-01038-6
47. Annavarapu S, Ghosh S, Li Y, Moretz C, Shetty S, Prewitt T. Healthcare resource utilization among patients with T2D and cardiovascular-, heart failure-, or renal-related hospitalizations. Am J Manag Care. 2020;26(6):e166–e171.
48. Artime E, Romera I, Diaz-Cerezo S, Delgado E. Epidemiology and Economic Burden of Cardiovascular Disease in Patients with Type 2 Diabetes Mellitus in Spain: a Systematic Review. Diabetes Ther. 2021;12(6):1631–1659. doi:10.1007/s13300-021-01060-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
SPUR: A Patient-Reported Medication Adherence Model as a Predictor of Admission and Early Readmission in Patients Living with Type 2 Diabetes
Wells J, Wang C, Dolgin K, Kayyali R
Patient Preference and Adherence 2023, 17:441-455
Published Date: 19 February 2023
Construction of a Nomogram-Based Prediction Model for the Risk of Diabetic Kidney Disease in T2DM
Wang X, Liu X, Zhao J, Chen M, Wang L
Diabetes, Metabolic Syndrome and Obesity 2024, 17:215-225
Published Date: 12 January 2024
Development and Validation of a Machine Learning-Based Predictive Model for Peripheral Neuropathy Risk in Elderly Patients with Type 2 Diabetes
Peng J, Xue D, Li J, Wei L, Wang Y
Risk Management and Healthcare Policy 2026, 19:573535
Published Date: 8 January 2026