Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Spontaneous Rupture of Hepatocellular Carcinoma: Pathogenesis, Clinical Management, Prognostic Factors, and Future Directions
Authors Cheng Y ![]() , Ye F
, Ye F ![]() , Chen Y
, Chen Y
Received 2 June 2025
Accepted for publication 10 October 2025
Published 27 October 2025 Volume 2025:12 Pages 2421—2428
DOI https://doi.org/10.2147/JHC.S540510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Yuan Cheng,1,* Feng Ye,2,* Yongjun Chen2
1Department of Medical Oncology, Jinling Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, 210002, People’s Republic of China; 2Department of General Surgery, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongjun Chen, Email [email protected]
Abstract: Spontaneous rupture of hepatocellular carcinoma (srHCC) is a life-threatening complication with complex pathophysiology and heterogeneous clinical presentations. This review aims to provide an up-to-date summary of the pathogenesis, clinical features, treatment strategies, prognostic factors, and emerging research in srHCC. We discuss current understanding of risk factors and rupture mechanisms, outline diagnostic and therapeutic approaches—including surgical, interventional, and systemic options—and explore postoperative management and prognosis. We also highlight recent clinical evidence and unmet research needs. Understanding the multifaceted nature of srHCC is essential to improve outcomes and guide future research directions.
Keywords: spontaneous rupture, hepatocellular carcinoma, TACE, conversion therapy, prognosis, adjuvant therapy
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common malignancy and the third leading cause of cancer-related mortality worldwide.1 According to the GLOBOCAN 2022 estimates, there were approximately 865,000 new cases and 758,000 deaths due to HCC globally, with China accounting for nearly half of both incidence and mortality. HCC remains a major focus of cancer control in China.1,2
Spontaneous rupture of hepatocellular carcinoma (srHCC) is one of the most severe and life-threatening acute complications of HCC. It typically presents with sudden onset of severe abdominal pain, peritoneal irritation, and hemorrhagic shock. The incidence of srHCC ranges from 3% to 15%, with a particularly high prevalence among cirrhotic patients in East Asia.3–5 Due to its abrupt onset and rapid progression, srHCC frequently results in massive hemorrhage and high early mortality, with acute-phase mortality rates reported between 25% and 75%.4 In the TNM staging system, ruptured HCC is classified as stage T4, and conventional wisdom has long held that such patients have a dismal prognosis and are unsuitable for curative treatment.6,7 Despite being a relatively rare but critical complication, srHCC remains underrepresented in current guidelines. The diversity of clinical presentations and the lack of consensus on optimal management strategies underscore the need for a comprehensive review that consolidates current knowledge and identifies future directions.
However, recent real-world studies suggest that the prognosis of srHCC is not uniformly poor. A subset of patients can achieve meaningful mid- to long-term survival, including 5-year survival, following timely hemostasis, staged hepatectomy, and appropriate adjuvant therapy.8,9 These findings highlight the biological heterogeneity of srHCC and challenge the traditional notion that rupture universally indicates advanced disease. With advancements in interventional radiology, intraoperative management, and systemic therapies—such as immunotherapy and targeted agents—treatment strategies for srHCC have evolved from an emergency-oriented approach to a more comprehensive and potentially curative paradigm.4
Nevertheless, patients with srHCC are often excluded from major Phase III clinical trials, leading to a paucity of high-level evidence. Significant regional and institutional variability in treatment strategies further underscores the need for standardized care. There is an urgent demand to systematically consolidate existing evidence, refine treatment algorithms, and define future research priorities to improve clinical outcomes in this challenging patient population. This review aims to bridge these gaps by providing a contemporary overview of srHCC, including its pathogenesis, clinical presentation, diagnostic strategies, therapeutic approaches, prognostic determinants, and emerging directions in clinical research. By integrating available data and highlighting unresolved questions, we hope to guide clinical practice and inform the design of future studies focused on this high-risk yet potentially treatable population.
Pathogenesis and Risk Factors
Pathophysiological Mechanisms
srHCC is an acute and life-threatening complication, typically resulting from the interplay of tumor burden, vascular abnormalities, underlying liver disease, and prior therapeutic interventions.10,11
Structurally, tumor characteristics play a fundamental role in the rupture process. Large, rapidly growing tumors—particularly those located subcapsularly or exhibiting exophytic growth patterns—are prone to central necrosis, which leads to increased local tension and ultimately rupture.10–12 This elevated intratumoral pressure, particularly when combined with thin overlying liver parenchyma, can compromise the tumor capsule and predispose to rupture. Histopathological studies have demonstrated that ruptured HCC lesions often display features of vascular fragility, including reduced elastic fibers in vessel walls, basement membrane disruption, and endothelial denudation. These are frequently accompanied by downregulation of von Willebrand factor and upregulation of matrix metalloproteinases (MMPs), collectively suggesting a marked increase in tumor-associated vascular fragility.13 In addition, abnormal tumor angiogenesis, often characterized by disorganized and leaky neovessels, contributes to mechanical instability and increases the risk of bleeding and rupture.
Moreover, chronic liver disease can further compromise vascular integrity and stress tolerance. Conditions such as cirrhosis, portal hypertension, and hypoalbuminemia reduce vascular compliance and heighten bleeding risk.14,15 Systemic inflammation and fibrosis in cirrhotic livers may also reduce the liver’s ability to buffer mechanical stress, enhancing susceptibility to rupture under pressure. Both systemic and portal hypertension, through persistent hemodynamic stress and resultant hyaline degeneration, is considered an independent risk factor for rupture.16
Certain therapeutic interventions may also precipitate srHCC. Transarterial chemoembolization (TACE) can induce tumor necrosis and elevate intratumoral pressure, increasing the likelihood of capsular rupture.17 Anti-angiogenic agents such as sorafenib and ramucirumab, by inhibiting VEGF-mediated vascular repair, may contribute to increased microvascular fragility and trigger rupture events in susceptible patients.15,18
Risk Factors
Numerous clinical studies have identified a variety of risk factors associated with srHCC, encompassing host characteristics, tumor biology, and treatment history. Among host-related factors, male sex is associated with a higher incidence, possibly due to hormonal influences and gender-related tumor biology.19 Comorbid conditions such as hypertension, cirrhosis, ascites, and hypoalbuminemia are linked to impaired vascular stability and hepatic reserve, with hypertension being widely recognized as an independent predictor of rupture.11,16,20 Additionally, metabolic dysfunction-associated fatty liver disease (MAFLD) and obesity are emerging risk factors, as their often silent progression may lead to undetected tumor enlargement and diagnostic delay.21
Tumor characteristics are critical determinants of rupture risk. Lesions larger than 5 cm, subcapsular or exophytic in growth, and those with portal or hepatic venous invasion, are particularly susceptible.10 Elevated serum alpha-fetoprotein (AFP) levels (eg, ≥400 ng/mL) reflect aggressive tumor biology and are closely correlated with rupture occurrence.11
Therapy-related factors are also relevant. TACE-induced tumor necrosis and pressure elevation may provoke rupture, especially in tumors adjacent to the liver capsule.17 Anti-angiogenic therapies can compromise microvascular integrity and have been implicated in cases of treatment-associated srHCC.15,18
Clinical Presentation and Diagnosis
Clinical Manifestations
srHCC is a fulminant complication with rapid progression and high mortality. The most common initial symptom is sudden onset of severe pain in the right upper quadrant or generalized abdominal pain, often accompanied by nausea, vomiting, and diaphoresis—reflecting autonomic nervous system activation.4 In more severe cases, patients may rapidly develop hypotension, tachycardia, altered consciousness, or even hemorrhagic shock. Reported rates of shock range from 30% to 90%.4,22
Some patients may present only with abdominal distension or progressive anemia, particularly those with poor baseline liver function or underlying chronic liver disease. In such cases, clinical manifestations may be subtle or nonspecific, making early recognition more challenging.5,22
This wide spectrum of clinical presentations—from overt hemorrhagic shock to vague abdominal discomfort—often complicates timely diagnosis. In patients with compensated cirrhosis or subclinical tumor rupture, symptoms may be insidious, leading to diagnostic delays.
Furthermore, overlapping signs with other causes of acute abdomen (eg, perforated peptic ulcer, ruptured spleen, or spontaneous bacterial peritonitis) may obscure clinical suspicion and necessitate prompt imaging for differentiation.
Diagnostic Strategies
The diagnosis of srHCC requires an integrated assessment of clinical presentation, laboratory findings, and imaging. Elevated alpha-fetoprotein (AFP) levels may support the diagnosis of HCC, particularly when AFP ≥ 400 ng/mL, which is also a known risk factor for rupture.11,23 Laboratory tests should include complete blood count, liver function tests, and coagulation profiles to evaluate bleeding severity, hepatic reserve, and coagulation status. When indicated, diagnostic paracentesis can confirm hemoperitoneum.24
Imaging plays a central role in confirming the diagnosis. Abdominal ultrasonography is a useful initial screening tool to detect tumors and intra-abdominal fluid. Contrast-enhanced computed tomography (CT) is the preferred modality, with a reported diagnostic accuracy of 75% to 100%.14 CT can identify peritumoral subcapsular hematomas, hemoperitoneum, and contrast extravasation within the tumor—considered direct signs of rupture.24
Contrast-enhanced ultrasound (CEUS) is a non-invasive and highly sensitive tool for detecting subcapsular rupture and active bleeding, particularly in patients unable to undergo CT.25,26 Digital subtraction angiography (DSA), although not a first-line diagnostic tool, is highly valuable in emergency settings where interventional therapy is needed. DSA not only confirms the bleeding source but also allows for immediate transarterial embolization.
In terms of differential diagnosis, other causes of hemoperitoneum should be considered, including splenic rupture, ruptured ectopic pregnancy, and ruptured abdominal aortic aneurysm.
Therapeutic Advances in srHCC
Initial Management and Supportive Care
srHCC is a life-threatening emergency characterized by rapid onset and progression. The primary therapeutic objective is immediate hemostasis and stabilization of hemodynamics. Initial management includes strict bed rest, nil per os (NPO), continuous monitoring of vital signs, and comprehensive supportive measures such as fluid resuscitation, transfusion, hemostatic therapy, liver protection, correction of coagulopathy, and maintenance of internal homeostasis.
For patients with limited hemorrhage, transiently stable hemodynamics, or those ineligible for surgery due to terminal disease status, conservative treatment may serve as a temporary or palliative approach. However, conservative treatment yields limited efficacy, with hemostatic success rates of approximately 40% and in-hospital mortality exceeding 66%, mainly due to hemorrhagic shock and liver failure.3,27 Therefore, in patients not at end-stage disease, supportive therapy alone should not be the first-line strategy; early transition to more definitive and active interventions is essential to improve prognosis.
Non-Surgical Treatment: Transarterial Embolization and Sequential Approaches
Interventional radiology remains the mainstay of non-surgical management for srHCC, particularly in patients unsuitable for immediate surgery. Transarterial embolization (TAE) achieves hemostasis by occluding the tumor’s feeding artery, with reported success rates ranging from 86% to 99%.3 When combined with chemotherapeutic agents as part of transarterial chemoembolization (TACE), the approach not only controls bleeding but may also suppress tumor growth, potentially creating a window for subsequent surgical resection.5,28 However, careful evaluation of hepatic functional reserve is critical to prevent post-embolization liver failure.
The advantages of interventional therapy include minimal invasiveness, technical feasibility, repeatability, and relative hepatic safety, making it particularly suitable for patients with moderate to advanced disease and preserved liver function.29 Nevertheless, as a non-curative modality, TAE/TACE cannot eradicate residual peritoneal tumor cells, and the risk of rebleeding remains substantial. Reports indicate that some patients may experience rebleeding within one week, with a mortality rate reaching 52%.28 Thus, early reassessment of surgical eligibility after initial hemostasis is strongly recommended, with integration of interventional and surgical strategies as part of a comprehensive treatment plan.
Surgical Treatment: Emergency vs Staged Hepatectomy
Hepatectomy remains one of the few potentially curative options for patients with spontaneous rupture of srHCC, and is generally classified into emergency hepatectomy (EmPH) and staged hepatectomy (SPH).22 EmPH may be considered in patients with moderate hemorrhage, hemodynamic stability, and resectable disease based on imaging, aiming to achieve simultaneous hemostasis and tumor clearance.30 However, in the emergency setting, full assessment of tumor margins, metastatic spread, and liver function is often limited, potentially compromising R0 resection rates and increasing postoperative risks.31 Reported R0 resection rates for EmPH range from 81% to 91%, but in-hospital mortality varies widely from 7.6% to 50%.20,31 Some meta-analyses have indicated that TAE/TACE is associated with fewer complications and lower mortality compared to EmPH,22 whereas other studies reported higher 30-day mortality in the TACE group,1 suggesting inconsistent evidence.
In contrast, SPH is performed after initial hemostasis via TAE/TACE and once the patient’s condition stabilizes. This approach has shown better safety profiles and long-term outcomes.22 Preoperative optimization enables improved perioperative tolerance and higher radical resection rates.32 Studies demonstrate that patients undergoing SPH have superior overall survival (OS) and disease-free survival (DFS) compared to those receiving interventional therapy alone.33
Timing of surgery is critical. Performing resection within 8 days of tumor rupture has been associated with reduced risk of peritoneal dissemination and improved survival outcomes.31,34 To further minimize peritoneal seeding, intraoperative peritoneal lavage, omentectomy, and postoperative hyperthermic intraperitoneal chemotherapy (HIPEC) for high-risk patients may be employed,34 potentially lowering recurrence rates and enhancing long-term survival.
Evolution of Combined Strategies: Sequential Surgery and Conversion Therapy
Given the dual challenge of hemorrhage control and oncologic management in srHCC, a single treatment modality is often insufficient. A widely adopted strategy is the sequential approach—initial hemostasis using TAE/TACE followed by staged surgical resection once the patient stabilizes.35 This method leverages the low risk and efficacy of minimally invasive embolization and the curative potential of surgery, making it particularly suitable for patients with borderline hepatic function or unstable condition at presentation.36 Studies have confirmed the superiority of this approach in terms of perioperative complications, transfusion requirements, and mortality rates.37,38 Propensity score-matched analyses have also demonstrated improved survival outcomes with sequential resection compared to TACE alone.34
Conversion therapy is also emerging as a promising strategy for initially unresectable cases. Combining TACE with targeted agents (eg, sorafenib) or immunotherapy (eg, PD-1 inhibitors) may downstage tumors and facilitate subsequent R0 resection.34,35 Preliminary studies have reported significant improvements in progression-free survival (PFS) and overall survival (OS) with this approach,39,40 particularly in patients with high tumor burden, inadequate future liver remnant, or marginal liver function.
There is a paradigm shift in the management of srHCC—from “hemostasis first” to a dual focus on both bleeding control and comprehensive oncologic treatment. Treatment decisions should be individualized, considering multiple factors such as hemorrhage severity, liver function reserve, tumor burden, and overall patient condition.34 A multidisciplinary team (MDT) approach is essential for developing tailored strategies that maximize therapeutic benefit and improve long-term outcomes. Table 1 summarizes the therapeutic modalities and key clinical considerations discussed in this section.
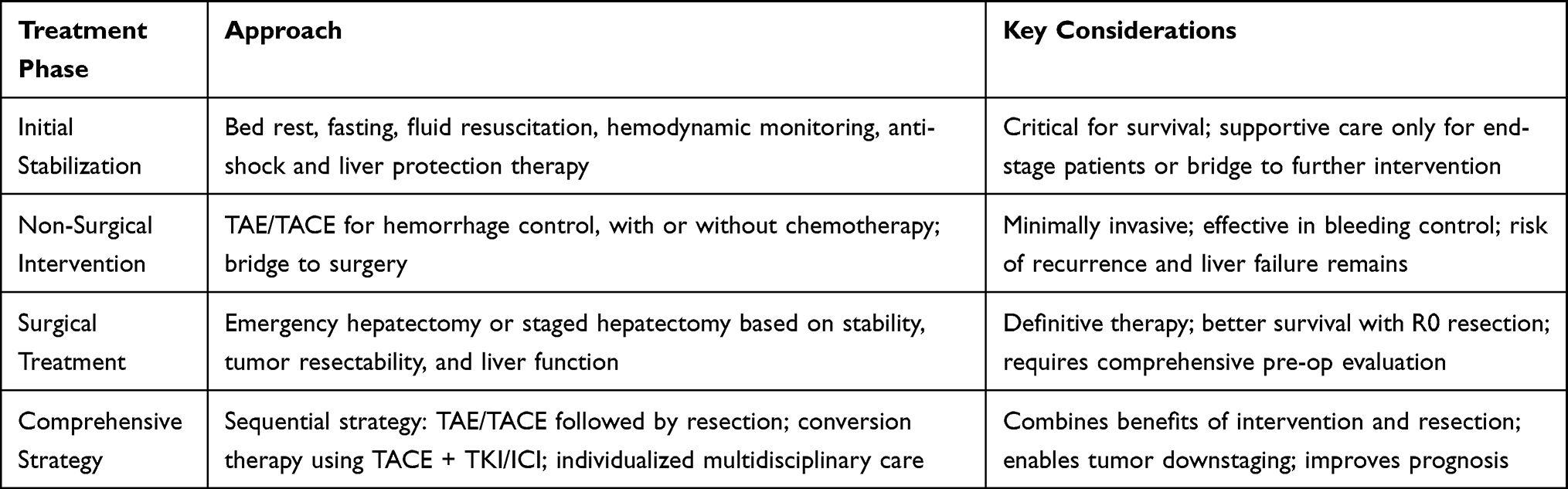 |
Table 1 Summary of Therapeutic Strategies for srHCC by Treatment Phase |
Prognostic Factors and Recurrence Patterns
Patients with srHCC generally exhibit poorer overall prognosis compared to those with non-ruptured HCC. Several studies have reported that the 1-, 3-, and 5-year overall survival (OS) rates following surgery in srHCC patients are approximately 66%, 23%, and 10%, respectively, which are significantly lower than those in non-ruptured counterparts (P < 0.001).8,41 Nevertheless, selected patients undergoing R0 resection followed by systemic therapy may achieve long-term survival comparable to non-ruptured HCC cases.10
Key prognostic factors for srHCC can be categorized into three major domains: hepatic functional status, tumor characteristics, and treatment strategies.
First, liver function plays a critical role. Established negative prognostic indicators include Child-Pugh class B/C, underlying cirrhosis, hypoalbuminemia, elevated INR, total bilirubin, and serum creatinine levels.1,33,42–44 Notably, the Child-Pugh classification remains one of the most accessible and reliable predictors of postoperative outcomes, as it integrates multiple dimensions of hepatic reserve. Advanced Child-Pugh stage (B or C) is consistently associated with impaired tolerance to surgery and higher recurrence risk. Additionally, elevated serum AFP levels (eg, ≥400 ng/mL) are associated with increased risk of recurrence and poorer survival outcomes.33,44 AFP is not only a diagnostic and surveillance marker but also serves as a surrogate for aggressive tumor biology. Persistent elevation of AFP after surgery may indicate residual disease or early recurrence and thus warrants close monitoring.
Second, tumor burden and biology are major determinants of outcome. A maximum tumor diameter >5 cm, multifocal disease, presence of microvascular invasion (MVI), and portal vein tumor thrombosis (PVTT) are all strongly linked to postoperative recurrence.33 Among these, tumor size and multifocality reflect the intrinsic aggressiveness and dissemination potential of the tumor. Integration of tumor burden into risk models may improve individualized recurrence prediction. Among these, MVI is considered one of the most powerful predictors of recurrence after resection, with a reported hazard ratio (HR) of approximately 2.09.45
Third, the modality and timing of intervention substantially influence prognosis. Achieving R0 resection has consistently been shown to significantly improve OS, with some studies reporting a reduction in mortality risk by over 50% (HR ≈ 2.24).46 Compared to emergency hepatectomy, staged hepatectomy following TAE/TACE yields better long-term survival and lower risk of peritoneal dissemination.33,38 Notably, elective resection performed within 8 days of rupture is associated with reduced peritoneal seeding and improved outcomes.31
Regarding recurrence patterns, srHCC patients exhibit a unique predisposition to peritoneal metastasis due to tumor cell spillage during rupture. Studies have demonstrated a significantly higher rate of peritoneal recurrence in srHCC patients compared to non-ruptured HCC (eg, 30% vs 5.9%; P < 0.001).11,24,46 Intraoperative peritoneal lavage and early surgical intervention may help mitigate this risk.
Adjuvant Therapy and Long-Term Outcomes
Patients with srHCC face a high risk of postoperative recurrence, particularly those with high-risk pathological features such as microvascular invasion (MVI), portal vein tumor thrombosis (PVTT), or multifocal disease.24,32,47 As a result, adjuvant therapy has been proposed as a critical strategy to improve disease-free survival (DFS) and overall survival (OS).
Transarterial chemoembolization (TACE) remains the most widely studied adjuvant approach in this setting. One study demonstrated that, among high-risk patients, postoperative adjuvant TACE significantly improved 5-year OS (29.8% vs 20.9%, P = 0.010), although no significant benefit was observed for DFS.24 Another investigation reported that the combination of TACE with tyrosine kinase inhibitors (TKIs) significantly improved 1- and 2-year DFS rates in high-risk HCC, suggesting the potential of combinatorial regimens.48
More recently, immunotherapy-based adjuvant strategies—particularly combinations involving PD-1/PD-L1 inhibitors and antiangiogenic agents (eg, atezolizumab plus bevacizumab)—have gained attention. Preliminary evidence indicates that TACE combined with PD-1/PD-L1 inhibitors and TKIs may enhance progression-free survival (PFS) and OS in advanced HCC,49,50 raising the possibility of application in the postoperative srHCC setting.
However, it is important to note that no prospective randomized studies to date have specifically investigated adjuvant therapy in srHCC. Current evidence is largely based on retrospective analyses or post hoc subgroup observations from broader HCC trials.24,48,51 Therefore, future research should prioritize well-designed, multicenter prospective trials to define the true efficacy and safety of various adjuvant strategies in this unique patient population. Efforts should also focus on optimizing combination regimens to further improve long-term outcomes in srHCC survivors.
Future Directions
srHCC remains a clinical emergency with complex treatment challenges and uncertain prognosis. Current management largely relies on clinical experience, lacking standardized guidelines and high-level evidence. Future advancements will require breakthroughs in data integration, therapeutic strategy optimization, and research infrastructure development.
First, a nationwide, multicenter real-world database should be established to systematically capture diagnostic, therapeutic, and follow-up information of srHCC patients. This would enable robust risk stratification, personalized treatment pathway development, and help overcome current limitations in sample size and treatment heterogeneity.
Second, the promotion of prospective, multicenter clinical trials is critical to improving the level of evidence for srHCC management. While current strategies are mainly based on retrospective data, future studies should focus on predefined endpoints related to surgical timing, interventional-surgical sequencing, and adjuvant therapies.
Third, optimizing adjuvant and conversion therapies is a priority. Postoperative recurrence remains high in srHCC, and preliminary data suggest potential benefits of TACE combined with targeted or immunotherapeutic agents in high-risk patients. However, dedicated prospective trials are required to validate these findings and determine the most effective regimens.
Fourth, development of a classification-based, personalized treatment algorithm is recommended. Clinical subtyping based on rupture characteristics and risk of peritoneal dissemination may guide stage-specific decision-making and facilitate more precise management.
In addition, perioperative optimization strategies may reduce the risk of peritoneal seeding. Evidence suggests that surgical intervention within eight days of rupture may help control dissemination. Intraoperative peritoneal lavage and high-frequency postoperative surveillance could aid in early detection and management of recurrence.
Finally, it is imperative to actively include srHCC patients in clinical trials. Many current HCC studies exclude this population, leading to a significant gap in evidence-based guidance. Future research frameworks should relax exclusion criteria or create dedicated trials for srHCC, thus improving treatment accessibility and scientific rigor.
Conclusion
Spontaneous rupture of hepatocellular carcinoma (srHCC) is a life-threatening complication, but recent advances in diagnosis, interventional radiology, surgery, and systemic therapies have improved outcomes in selected patients. Timely and individualized management can lead to meaningful survival, sometimes comparable to non-ruptured cases.
However, challenges remain, including high recurrence rates, lack of standard treatment protocols, and limited evidence for adjuvant therapy. Future efforts should focus on building multicenter databases, conducting prospective studies, and developing risk-adapted treatment strategies to optimize outcomes in this unique HCC subtype.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Cai W, Yin DL. Advances in the diagnosis and treatment of ruptured hepatocellular carcinoma. Int J Surg. 2023;50(12):797–802.
4. Xia F, Ndhlovu E, Zhang M, et al. Ruptured hepatocellular carcinoma: current status of research. Front Oncol. 2022;12:848903. doi:10.3389/fonc.2022.848903
5. Sahu SK, Chawla YK, Dhiman RK, et al. Rupture of hepatocellular carcinoma: a review of literature. J Clin Exp Hepatol. 2019;9(2):245–256. doi:10.1016/j.jceh.2018.04.002
6. Nuño-Guzmán CM, Marín-Contreras ME. Ruptured hepatocellular carcinoma and non-alcoholic fatty liver disease, a potentially life-threatening complication in a population at increased risk. Ann Hepatol. 2020;19(1):3–4. doi:10.1016/j.aohep.2019.11.001
7. Chun YS, Pawlik TM, Vauthey JN. Edition of the AJCC cancer staging manual: pancreas and hepatobiliary cancers. Ann Surg Oncol. 2018;25(4):845–847. doi:10.1245/s10434-017-6025-x
8. Aoki T, Kokudo N, Matsuyama Y, et al. Prognostic impact of spontaneous tumor rupture in patients with hepatocellular carcinoma: an analysis of 1160 cases from a nationwide survey. Ann Surg. 2014;259(3):532–542. doi:10.1097/SLA.0b013e31828846de
9. Kwon JH, Song GW, Hwang S, et al. Surgical outcomes of spontaneously ruptured hepatocellular carcinoma. J Gastrointest Surg. 2021;25(4):941–953. doi:10.1007/s11605-020-04555-0
10. Choudhury A, Mukund A, Roy A, Sharma D, Heo S, Choi WM. Managing complex hepatocellular carcinoma subtypes: diffuse infiltrative, large tumours, and tumour rupture-the challenges and strategies. J Clin Exp Hepatol. 2025;15(3):102505. doi:10.1016/j.jceh.2025.102505
11. Zhang Z, Tan S, Tang H, et al. Risk factors and survival analysis of spontaneously ruptured hepatocellular carcinoma: a retrospective cohort study in bilateral centers. Ann Surg Oncol. 2025;32:7283–7284. doi:10.1245/s10434-025-17999-y
12. Wang C, Huang X, Lan X, et al. Research progress of spontaneous ruptured hepatocellular carcinoma: systematic review and meta-analysis. Front Oncol. 2022;12:973857. doi:10.3389/fonc.2022.973857
13. Zhu LX, Geng XP, Fan ST. Spontaneous rupture of hepatocellular carcinoma and vascular injury. Arch Surg. 2001;136(6):682–687. doi:10.1001/archsurg.136.6.682
14. Sandomenico F, Arpaia V, De Rosa F, et al. Spontaneously ruptured hepatocellular carcinoma: computed tomography-based assessment. Diagnostics. 2023;13(6):1021. doi:10.3390/diagnostics13061021
15. Rombolà F, Caravetta A, Mollo F, et al. Sorafenib, risk of bleeding and spontaneous rupture of hepatocellular carcinoma. A clinical case. Acta Medica. 2011;54(4):177–179. doi:10.14712/18059694.2016.46
16. Chen Y, Guo D, Li X, et al. Predictors of spontaneous rupture of hepatocellular carcinoma and clinical outcomes following hepatectomy. Front Oncol. 2022;12:820867. doi:10.3389/fonc.2022.820867
17. Tartaglia N, Di Lascia A, Cianci P, et al. Hemoperitoneum caused by spontaneous rupture of hepatocellular carcinoma in noncirrhotic liver. A case report and systematic review. Open Med. 2020;15(1):739–744. doi:10.1515/med-2020-0202
18. Haider A, Siddiqa A, Mehmood M, et al. Ramucirumab-induced hepatocellular carcinoma rupture and gastrointestinal perforation. Am J Case Rep. 2021;22:e929493. doi:10.12659/AJCR.929493
19. Obeidat AE, Wong LL. Spontaneous rupture of hepatocellular carcinoma: new insights. J Clin Exp Hepatol. 2022;12(2):483–491. doi:10.1016/j.jceh.2021.05.010
20. Aziz H, Kwon Y, Park A, et al. Comprehensive review of clinical presentation, diagnosis, management, and prognosis of ruptured hepatocellular carcinoma. J Gastrointest Surg. 2024;28(8):1357–1369. doi:10.1016/j.gassur.2024.05.018
21. Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16(10):589–604. doi:10.1038/s41575-019-0186-y
22. Yan J, Li T, Deng M, et al. Ruptured hepatocellular carcinoma: what do interventional radiologists need to know. Front Oncol. 2022;12:927123. doi:10.3389/fonc.2022.927123
23. Xu K, Ryu D, Choi H, et al. Prognosis and recurrence of spontaneously ruptured hepatocellular carcinoma treated after hepatectomy: a single institution experience. Medicine. 2024;103(24):e38555. doi:10.1097/MD.0000000000038555
24. Huang A, Guo DZ, Wang YP, et al. The treatment strategy and outcome for spontaneously ruptured hepatocellular carcinoma: a single-center experience in 239 patients. J Cancer Res Clin Oncol. 2022;148(11):3203–3214. doi:10.1007/s00432-022-03916-3
25. Pang E, Chan A, Ho SG, et al. Contrast-enhanced ultrasound of the liver: optimizing technique and clinical applications. AJR Am J Roentgenol. 2018;210(2):320–332. doi:10.2214/AJR.17.17843
26. Fang C, Anupindi SA, Back SJ, et al. Contrast-enhanced ultrasound of benign and malignant liver lesions in children. Pediatr Radiol. 2021;51(12):2181–2197. doi:10.1007/s00247-021-04976-2
27. Zhong F, Cheng XS, He K, et al. Treatment outcomes of spontaneous rupture of hepatocellular carcinoma with hemorrhagic shock: a multicenter study. Springerplus. 2016;5(1):1101. doi:10.1186/s40064-016-2762-8
28. Schwarz L, Bubenheim M, Zemour J, et al. Bleeding recurrence and mortality following interventional management of spontaneous HCC rupture: results of a multicenter European study. World J Surg. 2018;42(1):225–232. doi:10.1007/s00268-017-4163-8
29. Guo J, Wang W, Zhang Y, et al. Comparison of initial tumor responses to transarterial bland embolization and drug-eluting beads-transarterial chemoembolization in the management of hepatocellular carcinoma: a propensity-score matching analysis. J Gastrointest Oncol. 2021;12(4):1838–1850. doi:10.21037/jgo-21-370
30. Zhang W, Huang Z, Che X. Emergency versus delayed hepatectomy following transarterial embolization in spontaneously ruptured hepatocellular carcinoma survivors: a systematic review and meta-analysis. World J Surg Oncol. 2022;20(1):365. doi:10.1186/s12957-022-02832-7
31. Wu JJ, Zhu P, Zhang ZG, et al. Spontaneous rupture of hepatocellular carcinoma: optimal timing of partial hepatectomy. Eur J Surg Oncol. 2019;45(10):1887–1894. doi:10.1016/j.ejso.2019.02.033
32. Lee HS, Choi GH, Choi JS, et al. Staged partial hepatectomy versus transarterial chemoembolization for the treatment of spontaneous hepatocellular carcinoma rupture: a multicenter analysis in Korea. Ann Surg Treat Res. 2019;96(6):275–282. doi:10.4174/astr.2019.96.6.275
33. Wang W, Meng T, Chen Y, et al. Propensity score matching study of 325 patients with spontaneous rupture of hepatocellular carcinoma. Hepatobiliary Surg Nutr. 2022;11(6):808–821. doi:10.21037/hbsn-21-45
34. Xia F, Zhang B, Zhu P. Discussion on the issues related to spontaneous rupture of hepatocellular carcinoma. Abdom Surg. 2025;38(1):1–6.
35. Cheng GG, Peng SS. Risk factors and therapeutic advances of spontaneous rupture and hemorrhage of hepatocellular carcinoma. Int J Surg. 2023;50(8):562–566.
36. Wang J, Tu B. Advances in the treatment of ruptured bleeding in primary liver cancer. Mod Med Health. 2019;35(14):2173–2175.
37. Liu MF, Liu LX. Current status of diagnosis and treatment of spontaneous rupture and hemorrhage of primary liver cancer. Med Recapitul. 2017;23(16):3193–3196, 3201.
38. Yu C, Gao CB, Chen CL. Analysis of risk factors and therapeutic advances in spontaneous rupture and hemorrhage of primary liver cancer. J Med Theor Pract. 2024;37(21):3623–3626, 3622.
39. Zu L, Song JJ, Zheng LY. Efficacy and safety of transarterial chemoembolization combined with sorafenib in the treatment of intermediate and advanced liver cancer complicated with ruptured hemorrhage. J Hepatobiliary Pancreat Surg. 2021;33(10):581–584, 595.
40. Qin LH, Wang LD, Jia SJ, Jia ZZ. Interpretation of the 2023 Chinese guidelines for clinical practice of TACE treatment in hepatocellular carcinoma. Electron J Surg. 2023;10(4):10–14.
41. Li J, Huang L, Liu CF, et al. Risk factors and surgical outcomes for spontaneous rupture of BCLC stages A and B hepatocellular carcinoma: a case-control study. World J Gastroenterol. 2014;20(27):9121–9127. doi:10.3748/wjg.v20.i27.9121
42. Xia F, Zhang Q, Chen X, et al. Comparison of the prognosis of BCLC stage A ruptured hepatocellular carcinoma patients after undergoing transarterial chemoembolization (TACE) or hepatectomy: a propensity score-matched landmark analysis. Surg Endosc. 2022;36(12):8992–9000. doi:10.1007/s00464-022-09351-2
43. Zheng L, Fang S, Wu F, et al. Efficacy and safety of TACE combined with sorafenib plus immune checkpoint inhibitors for the treatment of intermediate and advanced tace-refractory hepatocellular carcinoma: a retrospective study. Front Mol Biosci. 2020;7:609322. doi:10.3389/fmolb.2020.609322
44. Xia F, Zhu P, Chen XP, et al. Prognostic analysis of postoperative survival for ruptured hepatocellular carcinoma with or without cirrhosis. J Oncol. 2022;2022:7531452. doi:10.1155/2022/7531452
45. Lv TR, Liu F, Jin YW, et al. Meta-analysis of prognostic factors for overall survival among resected patients with spontaneous ruptured hepatocellular carcinoma. J Gastrointest Surg. 2023;27(12):2983–3000. doi:10.1007/s11605-023-05860-0
46. Joliat GR, de Man R, Rijckborst V, et al. Long-term outcomes of ruptured hepatocellular carcinoma: international multicentre study. Br J Surg. 2024;111(4):znae093. doi:10.1093/bjs/znae093
47. Xia F, Ndhlovu E, Liu Z, et al. Alpha-fetoprotein+alkaline phosphatase (A-A) score can predict the prognosis of patients with ruptured hepatocellular carcinoma underwent hepatectomy. Dis Markers. 2022;2022:9934189. doi:10.1155/2022/9934189
48. Lin K, Wei F, Huang Q, et al. Postoperative adjuvant transarterial chemoembolization plus tyrosine kinase inhibitor for hepatocellular carcinoma: a multicentre retrospective study. J Hepatocell Carcinoma. 2022;9:127–140. doi:10.2147/JHC.S352480
49. Zhu HD, Li HL, Huang MS, et al. Transarterial chemoembolization with PD-(L)1 inhibitors plus molecular targeted therapies for hepatocellular carcinoma (CHANCE001). Signal Transduct Target Ther. 2023;8(1):58. doi:10.1038/s41392-022-01235-0
50. Ji J, Zhou C, Yan LL, et al. Transarterial chemoembolization plus tyrosinkinase inhibitors and PD-1 inhibitors for spontaneously ruptured hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2024;47(3):299–309. doi:10.1007/s00270-023-03653-1
51. Li ZX, Zhang QF, Huang JM, et al. Safety and efficacy of postoperative adjuvant therapy with atezolizumab and bevacizumab after radical resection of hepatocellular carcinoma. Clin Res Hepatol Gastroenterol. 2023;47(7):102165. doi:10.1016/j.clinre.2023.102165
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Decaprenyl Diphosphate Synthase Subunit 1 (PDSS1): A Potential Prognostic Biomarker and Immunotherapy-Target for Hepatocellular Carcinoma
Yang Y, Li J, Tang M, Nie B, Huang W
Cancer Management and Research 2022, 14:1627-1639
Published Date: 3 May 2022
Identification of KRBA1 as a Potential Prognostic Biomarker Associated with Immune Infiltration and m6A Modification in Hepatocellular Carcinoma
Liu Y, Fu B, Yu Z, Song G, Zeng H, Gong Y, Ding Y, Huang D
Journal of Hepatocellular Carcinoma 2022, 9:497-516
Published Date: 31 May 2022
Gustave Roussy Immune Score Predicts Outcomes in Hepatocellular Carcinoma Treated with TACE and Immunotherapy
Qin L, Xu XY, Yang H, Li W, Zhang S, Shen J, Zhu X
Journal of Hepatocellular Carcinoma 2026, 13:563292
Published Date: 26 February 2026
Prognostic Impact of the Systemic Immune-Inflammation Index in Unresectable Hepatocellular Carcinoma Undergoing Second-Line Combination Therapy: A Multicenter Study
Chen X, Li X, Jiang Y, Xie Q, Zhang P, Zhou X, Wei C, Xie P, Cao L
Cancer Management and Research 2026, 18:613658
Published Date: 3 June 2026
Adjuvant Sintilimab Plus Bevacizumab After Curative Resection of Spontaneously Ruptured Hepatocellular Carcinoma: Protocol for a Prospective, Exploratory, Single-Arm Study (CLEAR-2)
Cheng Y, Ye F, Sun HC, Chen Y
Journal of Hepatocellular Carcinoma 2026, 13:614872
Published Date: 16 July 2026