Back to Journals » Journal of Pain Research » Volume 19
Spinal Cord Stimulation and DREZ Lesioning for Refractory Postherpetic Neuralgia: An Exploratory Case Series
Authors Jin W, Yang D, Li J, Tao W, Ren Z, Yu T, Sun S, Xu C, Shi C, Hu Y, Shu W
Received 27 December 2025
Accepted for publication 11 April 2026
Published 22 April 2026 Volume 2026:19 583921
DOI https://doi.org/10.2147/JPR.S583921
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Alaa Abd-Elsayed
Weipeng Jin,1,* Dou Yang,1,* Junchi Li,2 Wei Tao,3 Zhiwei Ren,1 Tao Yu,1 Shuo Sun,1 Chengwei Xu,4 Chengyu Shi,5 Yongsheng Hu,1 Wei Shu1
1Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Neurosurgery, The University of Hong Kong- Shenzhen Hospital, Shenzhen, People’s Republic of China; 3Department of Neurosurgery 2, South China Hospital, Medical School, Shenzhen University, Shenzhen, People’s Republic of China; 4Neurosurgery Department, The Affiliated Hospital of Inner Mongolia Medical University, Inner Mongolia, People’s Republic of China; 5Department of Cardiovascular Physiology, Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama University, Okayama, Japan
*These authors contributed equally to this work
Correspondence: Yongsheng Hu, Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China, Tel +86-13611342511, Email [email protected] Wei Shu, Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China, Tel +86-18500570180, Email [email protected]
Purpose: Refractory postherpetic neuralgia (PHN) remains one of the most challenging forms of neuropathic pain after herpes zoster infection, often resistant to conventional therapy. Neurosurgical interventions—particularly spinal cord stimulation (SCS) and dorsal root entry zone (DREZ) lesioning—offer potential benefit, yet optimal selection of surgical treatment remains unclear. This study explores the clinical evidence application of SCS and DREZ lesioning, focusing on clinical outcomes, safety, and costs.
Patients and Methods: This retrospective single-center series included ten patients with refractory PHN treated between 2011 and 2023. Eight underwent SCS trials; those achieving ≥ 30% pain reduction (Numeric Rating Scale, NRS) received permanent implants. Patients with insufficient response proceeded to DREZ lesioning. Pain intensity and disability were evaluated using NRS and the Pain Disability Index (PDI) after a minimum 24-month follow-up. Treatment success was defined as ≥ 30% reduction in NRS. Secondary outcomes included complications, hospital stay, and procedural costs.
Results: Among the eight patients who underwent SCS trials, three achieved ≥ 30% pain reduction and proceed to permanent implantation, with 24-month pain relief rates of 70%, 40%, and 0, respectively. Of the five patients with inadequate SCS response, one subsequently underwent DREZ lesioning; while two additional patients who declined SCS underwent primary DREZ lesioning. At 24 months, pain relief among DREZ-treated patients was 90%, 80%, and 60%, respectively. One patient developed mild segmental sensory loss at the lesioned levels without functional impairment, and no serious complications were observed.
Conclusion: In this small, single-center case series, both SCS and DREZ lesioning achieved meaningful pain reduction in carefully selected patients with refractory postherpetic neuralgia. SCS offers a minimally invasive, reversible option for patients demonstrating effective trial stimulation, whereas DREZ may provide durable analgesia for those with failed SCS or central dorsal horn pathology. These findings are exploratory and hypothesis-generating, underscoring the need for prospective multicenter studies to refine patient selection based on clinical evidence and optimize neurosurgical management.
Keywords: postherpetic neuralgia, spinal cord stimulation, neuromodulation, neurostimulation, dorsal root entry zone lesioning, neuropathic pain
Introduction
Postherpetic neuralgia (PHN) is a chronic neuropathic pain syndrome characterized by pain persisting for months or years after healing of the herpes zoster rash. It arises from varicella-zoster virus–induced injury to peripheral nerves and the dorsal root ganglion, often leading to irreversible sensitization of the dorsal horn and impaired descending inhibition.1 Compared with many other chronic neuropathic pain conditions, PHN more characteristically involves the dorsal roots, dorsal root ganglia, and peripheral nerves, with pain typically distributed along specific dermatomes. About 15–20% of herpes zoster patients develop PHN, a condition often difficult to treat.2 The resulting pain—typically characterized by burning, stabbing, or electric sensations—can severely impact quality of life.3–5 Conventional treatments, including antivirals, anticonvulsants, antidepressants, and nerve blocks, provide only partial relief for a subset of patients, and long-term management remains a formidable challenge.2,6,7
Neurosurgical interventions have gradually emerged as viable options for intractable PHN, particularly spinal cord stimulation (SCS) and dorsal root entry zone (DREZ) lesioning.8–13 SCS modulates pain transmission by activating large-diameter afferent fibers within the dorsal columns, thereby engaging segmental and supraspinal inhibitory mechanisms. Numerous studies have reported that SCS can alleviate neuropathic pain of peripheral or central origin, including PHN.14–16 However, the efficacy of SCS often depends on the integrity of the dorsal columns; extensive deafferentation or dorsal horn scarring may compromise stimulation effects. In such circumstances, DREZ lesioning—which targets hyperactive nociceptive neurons within the dorsal horn—may provide more direct and durable pain suppression. Originally developed for avulsion-related pain, DREZ procedures have since been adapted for other refractory neuropathic conditions, including PHN, with promising results in small series.14,17
Despite these therapeutic advances, the selection criteria for SCS and DREZ lesioning remain incompletely defined. In clinical practice, SCS is generally favored as the first-line neurosurgical option because it is minimally invasive and reversible. However, when patients show inadequate response to SCS or exhibit radiological and intraoperative findings suggestive of more severe neural injury, DREZ lesioning may be more appropriate. A few publications describe isolated experience with either SCS or DREZ lesioning alone, leaving clinicians uncertain not only about when to transition from neuromodulation to ablative intervention, but also about when ablative surgery may be preferred in selected patients.
The present study sought to address this gap by retrospectively analyzing a consecutive series of patients with refractory PHN treated with SCS or DREZ lesioning. We aimed to evaluate the long-term efficacy, safety, and cost profiles of these two approaches and to provide practical insights into patient selection. Through direct comparison of outcomes across treatment modalities in a single-center cohort, together with clinical experience and observed radiological and intraoperative findings, this exploratory analysis sought to support clinical interpretation and patient selection rather than establish a fixed treatment algorithm, while also providing exploratory observations that may help interpret differential treatment responses in PHN.
Materials and Methods
Study Design
This study was designed as a retrospective, single-center case series. Aiming to explore the efficacy of DREZ lesioning and SCS in the treatment of postherpetic neuralgia, as well as to investigate the optimal mechanism-based sequencing of these surgical interventions. We retrospectively cted clinical data on patients diagnosed with PHN who underwent either DREZ lesioning or SCS at our institution between 2011 and 2023 (Figure 1). All patients were followed up for at least 2 years via outpatient visits or telephone interviews. This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Xuanwu Hospital, Capital Medical University (Approval No. Clinical Research Ethics Approval [2025]021–001). Owing to its retrospective nature, the IRB waived the requirement for informed consent. All patient data were anonymized prior to analysis, and confidentiality of patient information was strictly maintained in accordance with institutional and ethical guidelines.
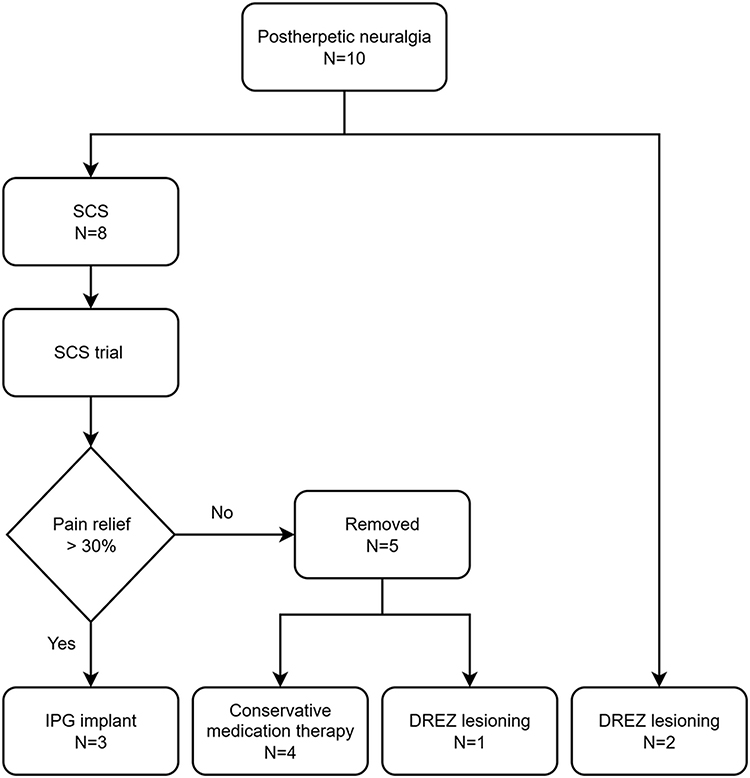 |
Figure 1 The study flow-chart: Ten patients with refractory postherpetic neuralgia (PHN) were included. Eight underwent a spinal cord stimulation (SCS) trial; three achieved satisfactory pain relief (≥30% NRS reduction) and proceeded to implantable pulse generator (IPG) implantation. Four patients without sufficient relief had their trial electrodes removed and continued conservative management, while one underwent subsequent dorsal root entry zone (DREZ) lesioning. Of the three IPG recipients, one later had the device explanted due to loss of efficacy. Two patients underwent DREZ lesioning as the initial intervention. |
Subjects
Patients were included if they had a clinically confirmed diagnosis of herpes zoster with persistent neuropathic pain lasting more than six months and no response to optimized medical management, including antivirals, anticonvulsants, antidepressants, and nerve blocks. Exclusion criteria included patients with severe immunosuppression, active systemic infection, or psychiatric or psychological disorders that could interfere with accurate pain assessment or postoperative evaluation.
Surgical Technique
Spinal Cord Stimulation (SCS)
The SCS procedure was performed in two stages: a trial stimulation phase followed by permanent implantation for patients who demonstrated a favorable response.
- Trial Screening
All patients first underwent a screening trial using either a surgical paddle lead or a percutaneous cylindrical electrode (Medtronic, Minneapolis, MN; Rishena, China, JS). The target spinal level was selected based on the patient’s dermatomal pain distribution. Under local anesthesia and fluoroscopic guidance, the electrode was placed in the dorsal epidural space. Intraoperative testing ensured that stimulation-induced paresthesia adequately covered the painful region. The electrode was anchored to the fascia and connected to an external pulse generator through a subcutaneous extension. SCS was delivered using a conventional Medtronic system with a tonic stimulation program. Commonly used parameters included a frequency of 40–60 Hz, a pulse width of 200–500 μs, and an amplitude between the sensory threshold and the uncomfortable threshold. The trial period lasted 5–14 days, during which pain intensity and function were closely monitored. A positive response was defined as ≥30% reduction in NRS score sustained for at least 48 hours, accompanied by improved daily activity. Patients meeting these criteria proceeded to permanent implantation, while no responders had their trial leads removed.
- Permanent System Implantation
Permanent implantation was performed under general anesthesia. A subcutaneous tunnel was created from the lead exit site to a pocket in the abdominal or pectoral region, where the implantable pulse generator (IPG) was placed and connected to the electrode (Figure 2). Proper system function was verified intraoperatively before closure.
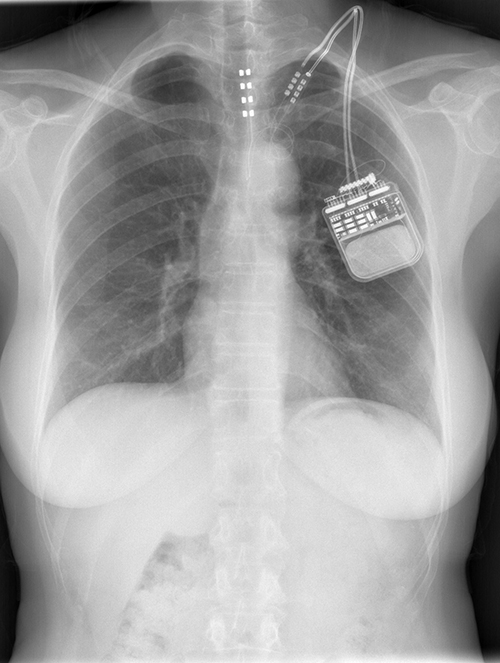 |
Figure 2 Fluoroscopic imaging of SCS system placement. Anteroposterior and lateral X-rays demonstrate proper positioning of the epidural electrode and subcutaneous implantable pulse generator (IPG) in a representative patient with PHN. |
DREZ Lesioning
DREZ lesioning was conducted under general anesthesia with the patient in the prone position. The target spinal segment corresponded to the dermatome of maximal pain. After a laminectomy, the dorsal root entry zone was exposed microscopically. Characteristic intraoperative findings included atrophy and yellowish discoloration of the affected dorsal roots, consistent with chronic zoster-related pathology. Lesions were created using microbipolar coagulation at a depth of approximately 3 mm, and an angle of about 35° from the midline along the root entry zone (Figure 3). Coagulations were applied sequentially along the identified segments until the pathological area was covered. Hemostasis was secured, and the wound was closed in standard fashion.
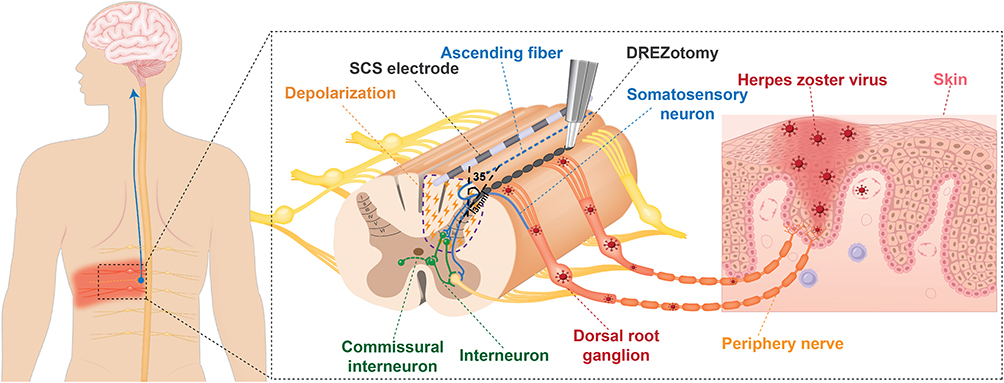 |
Figure 3 Schematic illustration of the mechanisms of SCS and DREZ lesioning in postherpetic neuralgia. SCS modulates abnormal afferent transmission through dorsal column activation, whereas DREZ lesioning interrupts hyperactive nociceptive neurons within the dorsal horn, providing complementary yet mechanism-specific analgesia. |
To ensure optimal efficacy while preserving adjacent neural structures, intraoperative neurophysiological monitoring, including somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs), was continuously employed throughout the procedure. This approach enabled precise localization of functional boundaries and controlled lesioning within the dorsal root entry zone, thereby reducing the risk of neurological deficits while effectively interrupting aberrant pain pathways.
Outcome Assessment and Follow-up
All patients were followed for at least 24 months after surgery. Postoperative evaluations were performed at 1, 3, 6, 12, and 24 months, and subsequently on an annual basis when possible. Clinical follow-up included both outpatient visits and telephone interviews conducted by the treating neurosurgeon or trained research staff not directly involved in the surgical procedures. Pain intensity was measured using the Numeric Rating Scale (NRS, 0–10), where 0 represented no pain and 10 the worst imaginable pain.18 Functional disability was evaluated using the Pain Disability Index (PDI), which quantifies the impact of pain on seven domains of daily life (range 0–70). Both NRS and PDI were documented at baseline, immediately postoperatively, and at each scheduled follow-up. Treatment success was defined as a ≥30% reduction in NRS score at the final follow-up, representing a clinically meaningful improvement according to established criteria for chronic pain intensity change described by Farrar et al and endorsed by subsequent Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials consensus statements.19,20 All adverse events were systematically recorded and categorized as surgical, hardware-related, or neurological. Economic data, including total hospitalization duration and direct treatment costs, were cted from institutional billing records for exploratory cost comparison between SCS and DREZ lesioning. All costs are reported in Chinese Yuan (CNY) and referenced to 2023 price levels.
Statistical Analysis
Given the small sample size and exploratory design, only descriptive statistical methods were applied. Continuous variables (eg, NRS, PDI, hospitalization duration, and treatment cost) were summarized as mean ± standard deviation (SD) or median with interquartile range (IQR), depending on data distribution. Categorical variables were reported as counts and percentages. Between-group differences for SCS and DREZ lesioning were described qualitatively to illustrate clinical trends rather than to test statistical significance. Post hoc power analysis was performed based on paired comparisons of baseline and final follow-up pain scores in the overall cohort. All analyses and data visualizations were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA) and G*power (Version: 3.1.9.7). No formal hypothesis testing or power calculation was conducted, and all numerical comparisons should be interpreted as exploratory.
Results
Patient Demographics and Clinical Characteristics
A total of ten patients with refractory PHN were included between October 2011 and February 2023. The medical characteristics of the participants are delineated in Table 1. The cohort comprised 6 males and 4 females, with an average age of 66.3 ± 8.9 years (range: 58–84 years). The duration of PHN symptoms exhibited considerable variability, ranging from 7 to 192 months, with a mean of 53.2 ± 54.7 months. Pain was localized on the left side in 6 patients and on the right side in 4 patients. The painful area was restricted to a single dermatome in 2 patients, while 8 patients had involvement of 2 or more dermatomes, with a mean of 2.60 ± 1.17 dermatomes. The affected dermatomes were predominantly distributed in the thoracic segments, with T7–T8 being the most commonly involved levels.
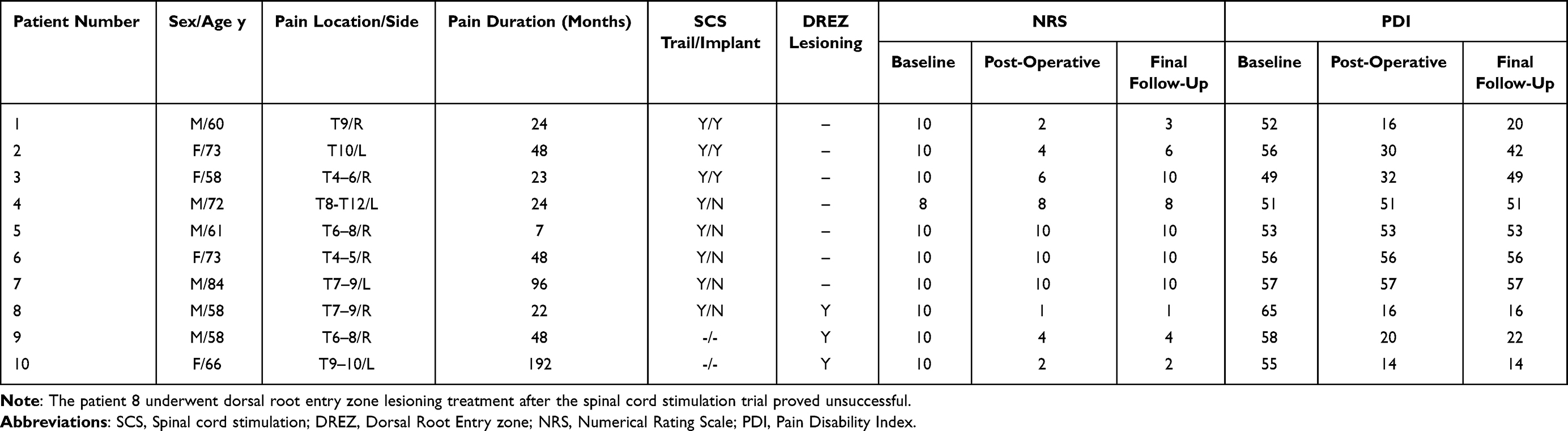 |
Table 1 Patient Characteristics and Treatment Outcomes Following SCS and DREZ Lesioning for Postherpetic Neuralgia |
Medical comorbidities were discerned in two patients diagnosed with malignancies, one patient with diabetes mellitus, and one individual receiving extended immunosuppressive therapy for rheumatoid arthritis. All subjects had previously undergone numerous conservative treatment approaches, including oral pharmacotherapy (eg, opioids, anticonvulsants, tricyclic antidepressants) and interventional techniques (eg, nerve blocks, transforaminal epidural injections, radiofrequency ablation, intrathecal pump).
At the onset of the investigation, the NRS score for 9 patients was 10, while 1 patient scored 8. Baseline pain intensity scores averaged NRS 9.8±0.6, and baseline function disability (PDI) averaged 55.2±4.5.
Spinal Cord Stimulation Outcomes
Eight patients underwent an initial SCS trial (Figure 4a). Three achieved ≥30% pain reduction and proceeded to permanent implantation. Following implantation, their pain relief rates were 80%, 60%, and 40%, respectively. At the final follow-up beyond 24 months, two of these three patients (66.7%) maintained substantial long-term pain reduction, and the third patient showed an initially favorable response but experienced diminishing benefit within two months, ultimately requesting device removal. In SCS-implanted patients, mean NRS scores improved from 10.0±0.0 preoperatively to 4.0±2.0 at 1 month and 6.3±3.5 at 24 months. Mean PDI decreased from 52.3±3.5 to 37.0±15.1 at the last follow-up.
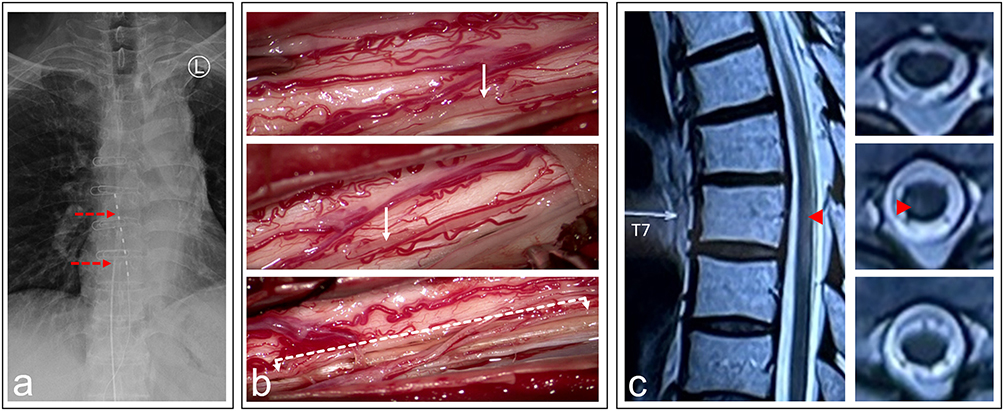 |
Figure 4 Illusion Case (Patient 8): (a) Anteroposterior radiograph showing the SCS lead (white dashed line), indicated by the upper red arrow, and the intrathecal morphine pump catheter, indicated by the lower red arrow. (b) Intraoperative microscopic view during DREZ lesioning, showing an atrophic and yellowish dorsal root (white arrow) compared with the contralateral normal root—direct in vivo evidence of herpes zoster–induced nerve injury. The dashed double-headed arrow indicates the extent and orientation of the DREZ lesion. (c) T2-weighted MRI showing a hyperintense signal within the dorsal horn (red arrowhead), corresponding to the dermatomes affected by herpes zoster pain. The white arrow, present on the original radiologic image, indicates the T7 vertebral level. |
Five patients who failed to achieve adequate relief during the trial period had their electrodes removed. Among these, one later received DREZ lesioning due to persistent intractable pain. No device-related infections or hardware malfunctions were observed, and no permanent neurological deficits occurred.
Outcome of DREZ Lesioning
A total of three patients underwent DREZ lesioning, including one SCS non-responder. At 24 months, three patients achieved long-term pain relief of 90%, 80%, and 60%, respectively. Mean NRS decreased from 10 to 3.5, and mean PDI improved from 59.3 ± 5.1 to 17.3 ± 4.1. One patient developed segmental sensory loss in the lesioned dermatomes without functional limitation. In the three patients who underwent DREZ lesioning, the atrophic dorsal roots observed intraoperatively were T7–9, T6–8, and T9–10, respectively, which corresponded well to the dermatomal distribution identified on preoperative physical examination (Figure 4b). No severe complications such as motor weakness, cerebrospinal fluid leakage, or wound infection were recorded.
Health Economy and Complications
The mean hospital stay was 18.4 days for SCS and 13.7 days for DREZ lesioning. The mean total surgical cost (including operation, device, and anesthesia) was approximately 2-fold higher for SCS (¥133,700) than for DREZ (¥56,100), primarily due to the implantable pulse generator expense. Despite higher initial costs, SCS offered the advantage of reversibility and lower surgical morbidity.
Discussion
This study presents a single-center, mechanism-informed case series evaluating SCS and DREZ lesioning in patients with refractory PHN. Among 10 patients treated between 2011 and 2023, SCS provided meaningful pain reduction in selected individuals, while DREZ lesioning yielded more consistent and durable analgesia, even in patients with failed SCS or dorsal horn pathology. Both procedures were safe, with no major neurological or systemic complications. Despite higher initial costs, SCS offered the advantages of reversibility and minimal invasiveness, whereas DREZ demonstrated superior long-term stability of pain control. These findings support the continued exploration of a stepwise, mechanism-based approach in which SCS serves as a reversible first-line intervention and DREZ lesioning as a definitive option when neuromodulation fails.
The pathophysiology of PHN involves both peripheral and central mechanisms, including persistent dorsal horn hyperexcitability and glial activation. Neuromodulation via SCS aims to modulate aberrant dorsal column transmission by activating inhibitory interneurons and descending pathways (Figure 3).21 Several studies have reported significant pain relief with SCS in neuropathic pain syndromes, including PHN, with success rates ranging from 40% to 70%.8,9 However, patients with severe deafferentation or dorsal column scarring often experience suboptimal outcomes, as effective paresthesia coverage becomes difficult to achieve.
In contrast, DREZ lesioning directly targets hyperactive nociceptive neurons within the dorsal horn, thereby interrupting abnormal spontaneous discharges that sustain chronic pain (Figure 3). Originally introduced by Nashold and Sindou for brachial plexus avulsion pain, the technique has since been applied to other central pain syndromes, including PHN, with reported long-term pain relief in 60–90% of cases. Recent series have shown that careful patient selection, precise lesion depth (approximately 2–3 mm), and limited segmental targeting can maximize efficacy while minimizing complications. Our results align with these findings, confirming that DREZ lesioning can provide durable relief in carefully selected PHN patients when SCS fails or is anatomically unsuitable.
DRG stimulation has emerged as a promising neuromodulation technique for the treatment of PHN, particularly in patients with localized, dermatomal pain. Compared with conventional SCS, DRG stimulation may allow more precise targeting of the affected segment and may reduce off-target paresthesia.14,22 In the present series, DRG stimulation was not used primarily because the relevant devices had not yet received formal FDA approval during the study period. In addition, many patients in our cohort presented with long-standing, refractory pain with relatively broader or more complex distributions, which were considered less suitable for focal neuromodulation approaches. Further studies are needed to clarify the optimal indications and timing of DRG stimulation in PHN. From a mechanistic perspective, DRG stimulation may be particularly relevant in PHN cases with predominantly segmental and peripheral drivers. In contrast, SCS and DREZ lesioning may address broader central modulation and dorsal horn–level mechanisms, respectively.
Intraoperative microscopic observation in this series provided direct in vivo evidence of herpes zoster–induced injury to the dorsal root nerves within the spinal canal (Figure 4b). To our knowledge, such findings have not been previously reported in living patients. This observation bridges a critical gap in understanding the pathophysiology of PHN, which until now has relied primarily on postmortem histopathological reports demonstrating varicella-zoster–related damage to dorsal roots and dorsal horn neurons.23–27
The degree of neural injury inflicted by the varicella-zoster virus likely exerts a major influence on PHN severity, chronicity, and treatment responsiveness. In Patient 8, preoperative magnetic resonance imaging revealed focal T2-hyperintense signals within spinal cord segments corresponding to the dermatomes of zoster pain, suggesting viral invasion of the dorsal horn (Figure 4c). This radiological finding was later confirmed intraoperatively, where distinct atrophy and yellowish discoloration of the affected dorsal roots were visualized. Such extensive dorsal horn and DREZ involvement may explain the poor response to both SCS and intrathecal morphine therapy observed in this patient.
This study underscores the importance of a mechanism-informed strategy in the surgical management of refractory postherpetic neuralgia. By integrating SCS and DREZ lesioning within a unified treatment algorithm, our findings demonstrate that these procedures function not as competing alternatives but as complementary, sequential interventions. SCS is most effective when neuropathic pain arises predominantly from peripheral or segmental mechanisms and the dorsal columns remain structurally intact, allowing adequate paresthesia coverage.28–30 In contrast, DREZ lesioning directly targets central dorsal horn hyperexcitability and should be considered when imaging or intraoperative findings reveal irreversible dorsal horn or dorsal root injury, or when SCS fails to provide durable relief. This stepwise, pathology-guided approach promotes individualized surgical planning, improves treatment efficiency, and informs resource allocation.
From an economic perspective, treatment pathways differed in their overall cost burden. Although SCS offers a less invasive and reversible initial option, failure of neuromodulation may necessitate additional surgical intervention. In such cases, the cumulative cost appeared to be higher than that of DREZ lesioning alone, while remaining lower than the total cost of successful permanent SCS treatment. Therefore, while a stepwise approach beginning with SCS may be clinically attractive, its economic implications should also be considered. In addition, the long-term burden associated with persistent pain should not be overlooked, including ongoing pharmacological therapy, outpatient visits, and reduced quality of life. However, because the follow-up duration in the present study was limited and postoperative medication use varied across patients, these longer-term economic factors were not fully captured and warrant further investigation.
Several limitations should be acknowledged. First, the sample size was small, and the retrospective, single-center design limited the generalizability of the findings. The lack of randomization, together with the inherent heterogeneity of PHN presentation, also precludes formal statistical comparison between groups. A post hoc power analysis demonstrated a large effect size (Cohen’s d = 0.89) with an estimated statistical power of 0.71. Although this suggests a clinically meaningful treatment effect, the statistical power remained below the conventional threshold of 0.80, and the small sample size and heterogeneous treatment responses across patients further limit the strength of interpretation. Therefore, these findings should be interpreted cautiously and considered hypothesis-generating. Second, neuroimaging or neurophysiological correlates of treatment response were not systematically analyzed, which might have further clarified the basis for treatment selection. Third, the economic data were exploratory and based on local cost structures, with costs reported in Chinese Yuan (CNY) at 2023 price levels. These findings may not be directly applicable to other healthcare systems or economic settings.
Future work should focus on prospective multicenter studies integrating quantitative sensory testing, spinal imaging, and neurophysiological monitoring to refine selection criteria and optimize procedural outcomes. Incorporating patient-reported quality-of-life measures and long-term follow-up beyond two years will also be critical to establishing evidence-based algorithms for neurosurgical management of refractory PHN.
Conclusion
This study suggests that both SCS and DREZ lesioning can provide meaningful pain reduction in patients with refractory postherpetic neuralgia. SCS offers a minimally invasive, reversible option for patients with preserved dorsal column function and successful trial stimulation, and DREZ lesioning may provide durable analgesia in selected patients, particularly those with failed SCS or predominant dorsal horn involvement. However, given the retrospective and descriptive design, no conclusions regarding comparative superiority can be drawn. Future prospective, multicenter studies incorporating imaging and neurophysiological correlates are warranted to validate these exploratory observations and refine patient selection for optimal long-term outcomes.
Abbreviations
SCS, Spinal cord stimulation; DREZ, Dorsal Root Entry zone; NRS, Numerical Rating Scale; PDI, Pain Disability Index.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Beijing Natural Science Foundation (Z210009).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chae JS, Im J, Choi YJ, Lee HJ, Kim WJ. Comparison of the severity of zoster-associated pain and incidence of postherpetic neuralgia in patients with and without pre-existing spinal disorders at the same spinal nerve level: a retrospective multicenter study. JPM. 2023;13(9):1286. doi:10.3390/jpm13091286
2. Lin CS. Interventional treatments for postherpetic neuralgia: a systematic review. Pain Phys. 2019;22(3):209–11. doi:10.36076/ppj/2019.22.209
3. Johnson R, Rice A. Clinical practice. Postherpetic neuralgia. N England J Med. 2014;371(16):1526–1533.
4. Matthews S, De Maria A, Passamonti M, et al. The economic burden and impact on quality of life of herpes zoster and postherpetic neuralgia in individuals aged 50 years or older in Italy. Open Forum Infect Dis. 2019;6(2):ofz007. doi:10.1093/ofid/ofz007
5. Sampathkumar P, Drage LA, Martin DP. Herpes zoster (Shingles) and postherpetic neuralgia. Mayo Clin Proc. 2009;84(3):274–280. doi:10.4065/84.3.274
6. Chang B, Wang S, Mei J. Neuromodulation for postherpetic neuralgia: preliminary experience in a single center. Clin Neurol Neurosurg. 2024;244:108438. doi:10.1016/j.clineuro.2024.108438
7. Onakpoya IJ, Thomas ET, Lee JJ, Goldacre B, Heneghan CJ. Benefits and harms of pregabalin in the management of neuropathic pain: a rapid review and meta-analysis of randomised clinical trials. BMJ Open. 2019;9(1):e023600. doi:10.1136/bmjopen-2018-023600
8. Harke H, Gretenkort P, Ulrich Ladleif H, Koester P, Rahman S. Spinal cord stimulation in postherpetic neuralgia and in acute herpes zoster pain. Anesthesia Analg. 2002;94(3):694–700. doi:10.1097/00000539-200203000-00040
9. Kim J, Kim D, Lee M, et al. Spinal cord stimulation for intractable postherpetic neuralgia. J Korean Neurosurg Soc. 2003;34(10):366–368.
10. Villanueva-Perez V, Palmisani S, Asensio-Samper J, et al. Spinal cord stimulation as treatment for post-herpes neuralgia refractory to conventional therapy. Rev Neurol. 2011;53(3):190–191.
11. Moriyama K. Effect of temporary spinal cord stimulation on postherpetic neuralgia in the thoracic nerve area. Neuromodulation. 2009;12(1):39–43. doi:10.1111/j.1525-1403.2009.00186.x
12. Shu W, Li Y, Tao W, Hu Y. Spinal cord stimulation combined with microsurgical DREZotomy for pain due to syringomyelia. Br J Neurosurg. 2016;30(5):585–587. doi:10.3109/02688697.2016.1173187
13. Deer TR, Mekhail N, Provenzano D, et al. The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: the neuromodulation appropriateness consensus committee. Neuromodulation. 2014;17(6):515–550. doi:10.1111/ner.12208
14. Texakalidis P, Tora MS, Boulis NM. Neurosurgeons’ armamentarium for the management of refractory postherpetic neuralgia: a systematic literature review. Stereotact Funct Neurosurg. 2019;97(1):55–65. doi:10.1159/000499476
15. Anisimov ED, Andrushkevich OM, Dzhafarov VM, Amelina EV, Rzaev JA, Slavin KV. Long-term effects of spinal cord stimulation on pain in postherpetic neuralgia. Stereotact Funct Neurosurg. 2024;1–7. doi:10.1159/000542138
16. Li J, Li Y, Shu W. Case report: peripheral nerve stimulation relieves post-traumatic trigeminal neuropathic pain and secondary hemifacial dystonia. Front Neurol. 2023;14:1107571. doi:10.3389/fneur.2023.1107571
17. Weipeng J, JunChi L, Wei T, et al. Long-term outcomes of dorsal root entry zone lesioning for neuropathic pain after brachial plexus avulsion: a 10-year follow-up study. Neurosurgery. 2025. doi:10.1227/neu.0000000000003757
18. Dworkin R, Wyrwich K. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. 2008;146(3):238–244.
19. Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
20. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. doi:10.1016/j.pain.2004.09.012
21. Melzack R, Wall P. Pain mechanisms: a new theory. Science. 1965;150(3699):971–979.
22. Dorner A, Dascalu I, Osborn J, Varshney V. Dorsal root ganglion stimulation for postherpetic neuralgia: a pilot scoping review of the current evidence. Cureus. 2025. doi:10.7759/cureus.93664
23. Moshayedi P, Thomas D, Rinaldo CR, et al. Subacute histopathological features in a case of varicella zoster virus myelitis and post-herpetic neuralgia. Spinal Cord Ser Cases. 2018;4(1). doi:10.1038/s41394-018-0068-5
24. Arakawa K, Nakagawa M, Abe Y, Morimatsu H. T2 high-signal-intensity zone of the spinal cord dorsal horn in patients treated with spinal cord stimulation for herpes zoster-associated pain: a retrospective case–control study. J Anesth. 2025;39(2):273–281. doi:10.1007/s00540-025-03458-1
25. Yacubian Fernandes A, Fernandes Da Silva FE, Hamamoto Filho PT, Talamoni Fonoff E. MR diffusion tensor imaging applied to the spinal cord of patients with neuropathic pain secondary to herpes zoster infection. J Clin Neurosci. 2024;130:110912. doi:10.1016/j.jocn.2024.110912
26. Devor M. Rethinking the causes of pain in herpes zoster and postherpetic neuralgia: the ectopic pacemaker hypothesis. Pain Rep. 2018;3(6):e702.
27. Reda H, Greene K, Rice FL, Rowbotham MC, Petersen KL. Natural history of herpes zoster: late follow-up of 3.9 years (n = 43) and 7.7 years (n = 10). Pain. 2013;154(10):2227–2233. doi:10.1016/j.pain.2013.04.015
28. Sun L, Peng C, Joosten E, et al. Spinal cord stimulation and treatment of peripheral or central neuropathic pain: mechanisms and clinical application. Neural Plast. 2021;2021(1):1–9. doi:10.1155/2021/5607898
29. Dombovy-Johnson ML, Hunt CL, Morrow MM, Lamer TJ, Pittelkow TP. Current evidence lacking to guide clinical practice for spinal cord stimulation in the treatment of neuropathic pain in spinal cord injury: a review of the literature and a proposal for future study. Pain Pract. 2020;20(3):325–335. doi:10.1111/papr.12855
30. Huang Q, Duan W, Sivanesan E, et al. Spinal cord stimulation for pain treatment after spinal cord injury. Neurosci Bull. 2019;35(3):527–539. doi:10.1007/s12264-018-0320-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Retrospective Efficacy and Cost-Containment Assessment of 10 kHz Spinal Cord Stimulation (SCS) in Non-Surgical Refractory Back Pain Patients
Kapural L, Calodney A
Journal of Pain Research 2022, 15:3589-3595
Published Date: 16 November 2022
Efficacy and Safety of Pulsed Radiofrequency in Herpes Zoster Related Trigeminal Neuralgia: A Systematic Review and Meta-Analysis
Wang C, Dou Z, Yan M, Wang B
Journal of Pain Research 2023, 16:341-355
Published Date: 2 February 2023
Painful Peripheral Neuropathies of the Lower Limbs and/or Lower Extremities Treated with Spinal Cord Stimulation: A Systematic Review with Narrative Synthesis
Burkey AR, Chen J, Argoff CE, Edgar DR, Petersen EA
Journal of Pain Research 2023, 16:1607-1636
Published Date: 18 May 2023
Spinal Cord Stimulation for Intractable Visceral Pain Originating from the Pelvic and Abdominal Region: A Narrative Review on a Possible New Indication for Patients with Therapy-Resistant Pain
Bieze M, van Haaps AP, Kapural L, Li S, Ferguson K, de Vries R, Schatman ME, Mijatovic V, Kallewaard JW
Journal of Pain Research 2024, 17:691-736
Published Date: 19 February 2024
Longitudinal Changes in Sensory Processing and Clinical Outcomes During Spinal Cord and Dorsal Root Ganglion Stimulation to Treat Chronic Pain: A Pilot Study
Rogers ER, Sankarasubramanian V, Kyi WHT, Mirzakhalili E, Anaya CJ, Loechli J, Harte SE, Patil PG, Chiravuri S, Lempka SF
Journal of Pain Research 2025, 18:4455-4470
Published Date: 29 August 2025