Back to Journals » ImmunoTargets and Therapy » Volume 14
Soluble Programmed Cell Death-1: A Potential Predictor of HBsAg Loss in Pediatric Patients with Chronic Hepatitis B Undergoing Peginterferon Therapy
Authors Yang G, Gan Y, Xia M, Fu Q, Zhang M, Luo K, Wang Z
Received 3 June 2025
Accepted for publication 25 October 2025
Published 4 November 2025 Volume 2025:14 Pages 1223—1231
DOI https://doi.org/10.2147/ITT.S541485
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Guifeng Yang,1,2,* Yifan Gan,2,3,* Muye Xia,2,3,* Qunfang Fu,1 Mingxia Zhang,1 Kangxian Luo,1 Zhanhui Wang2,3
1The Group of Prevention and Therapy for CHB, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 2Department of Infectious Diseases, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 3Key Laboratory of Infectious Diseases Research in South China (Ministry of Education), Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhanhui Wang, Department of Infectious Diseases, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China, Tel +86-20-62787314, Email [email protected]
Purpose: Soluble programmed cell death-1 (sPD-1) level can predict hepatitis B surface antigen (HBsAg) loss in adult chronic hepatitis B (CHB) patients. However, whether sPD-1 level can serve as a potential seromarker for predicting HBsAg loss in pediatric patients remained to determine.
Patients and Methods: Ninety-two pediatric HBeAg-positive CHB patients who received peginterferon (PegIFN) therapy with available serum samples were studied retrospectively. The average follow-up time was 45.0 months. Virological biomarkers and sPD-1 were serially measured.
Results: A total of 45 (48.9%) children achieved HBsAg loss at the end of treatment (EOT), and 84.4% (38/45) of them remained HBsAg-negative at the end of follow-up. At baseline, sPD-1 levels were comparable between patients who subsequently achieved HBsAg loss and those who did not (P = 0.217). However, a significantly more pronounced increase in sPD-1 levels was observed during PegIFN treatment in the HBsAg loss group (Ptrend < 0.001). Consequently, at weeks 12, 24, and EOT, sPD-1 levels were significantly higher in children with HBsAg loss compared to those without (P < 0.001 at all time-points). In ROC curve analysis, sPD-1 had strong discriminatory ability for HBsAg loss at weeks 12 and 24, with area under ROC scores of 0.842 (95% CI, 0.744– 0.946) and 0.863 (95% CI, 0.758– 0.969), respectively, slightly lower than HBsAg but higher than HBV DNA.
Conclusion: Early on-treatment serum sPD-1 level has a potential predictive value for HBsAg loss in pediatric patients with HBeAg-positive CHB, which might provide a clue to optimize the management of PegIFN therapy. However, a prospective, multi-center study is warranted for further validation.
Keywords: Chronic hepatitis B, HBsAg loss, peginterferon, soluble programmed cell death-1
Introduction
Hepatitis B virus (HBV) infection is a worldwide health problem that causes HBV-related morbidity and mortality.1 Approximately 90% newborns of HBeAg-positive mothers will develop into chronic infections after acute exposure.2 HBsAg loss is usually regarded as the resolution of chronic HBV infection. However, spontaneous loss of HBsAg is rarely acquired during the long-term follow-up, with an average annual clearance rate of 1% in children and 1.02% in adult with CHB.3,4 Furthermore, treatment-induced HBsAg loss with currently available antiviral therapy is also uncommon in adult.5 Surprisingly, peginterferon (PegIFN), as one of the first-line treatment option for CHB, can yield a relatively high rate of HBsAg loss in children with a finite course.6–8 However, it is costly and may lead to numerous adverse events. Therefore, identifying factors predicting HBsAg loss is crucial for improving clinical decision-making around early initiation of PegIFN treatment.
Up to date, there were limited available seromarkers to predict HBsAg loss in pediatric patients undergoing PegIFN treatment. Few studies reported that age and HBsAg level were independent predictors of HBsAg loss in pediatric CHB patients with interferon-alfa treatment.9,10 However, immunology-related biomarkers are lacking. Recently, a prospective study demonstrated the predictive value of soluble programmed cell death 1 (sPD-1) for HBsAg loss in adult patients with CHB undergoing PegIFN-based therapy.11 Given the fundamental immunological differences between pediatric and adult CHB patients, particularly in T-cell exhaustion and plasticity,12 biomarker behavior may differ significantly across age groups. Whether sPD-1 level can serve as a potential immunology marker for the predictive of HBsAg loss in pediatric patients needs to be determined.
PD-1 is an inhibitory receptor, and interaction with its ligand PD-L1 plays a crucial role in mediating the inhibition of T cell activation.13,14 sPD-1 is derived from the splicing of exon 3 of the complete PD-1 sequence, and shows an ability of enhancing the specific T cell response through inhibiting the PD-1/PD-L1 pathway.15 The level of sPD-1 has been reported to be correlated with the prognosis of HBV infection.16,17 In addition, sPD-1 level plays an important role in predicting HBeAg seroclearance in patients with or without treatment and spontaneous HBsAg loss in inactive patients.18–20 In the present study, we sought to evaluate the utility of sPD-1 level as a potential predictor for HBsAg loss in pediatric patients with CHB, which may enhance clinical decision-making during early PegIFN intervention.
Materials and Methods
Study Population
This is a retrospective study, and all the cases were derived from a real-world study, encompassing children aged 1 to 13 years. They were continuously enrolled at Nanfang Hospital (Guangzhou, China) between January 2014 and August 2021. All of them were HBsAg and HBeAg positive at least 6 months, with 2–10 ULN (the upper limit of normal, 40 U/L) ALT levels, and were not receiving any HBV antiviral therapy at the time of enrollment. Exclusion criteria included having co-infection with human immunodeficiency or hepatitis C or D virus, or having evidence of liver decompensation or hepatocellular carcinoma or other chronic liver disease or autoimmune disease. Generally, children received PegIFN treatment for 48 weeks, and the dose was based on the body surface area, in detail, 0.51–0.53 m2, 45 mg/w; 0.54–0.74 m2, 65 mg/w; 0.75–1.08 m2, 90 mg/w; 1.09–1.51 m2, 135 mg/w; and >1.51 m2, 180 mg/w. All the cases were regularly tested serological markers every 12 weeks during the course of PegIFN therapy, and every 12–24 weeks within 12 months after PegIFN discontinuation, and then every 6–12 months thereafter. Cases who met two of the following three items at week 12 or week 24 during the course of PegIFN treatment were defined as non-responders, according to the stopping rules established for adults:21,22 (1) HBsAg decreased < 0.5 lg IU/mL, (2) HBeAg decreased < 0.5 lg COI, (3) HBV DNA decreased < 1 lg IU/mL. These cases were switched from PegIFN to entecavir (ETV) treatment and assigned to the group of without HBsAg loss for analysis. Serum samples were obtained and stored at −30°C prior to analysis. Informed consent was obtained from the parents of each child before the initial of treatment. This study was conducted according to Declaration of Helsinki guidelines and was approved by the Chinese ethics committee of registering clinical trials (ChiECRCT-20140020).
Laboratory Measurements
Serum sPD-1 levels were assessed using a commercially available ELISA kit (MyBiosource), the quantification range of which was between 0.2 and 60 ng/mL. The levels of sPD-1 were measured at multiple time points before, during (weeks 12 and 24) the course and the end of treatment (EOT) with PegIFN, as well as during the follow-up period within 12 months after PegIFN discontinuation. However, sPD-1 levels were not measured after switching to ETV treatment.
Serum HBV DNA levels were assessed using the TaqMan polymerase chain reaction assay (COBAS TaqMan, Roche Molecular System) with a quantification range between 20 IU/mL and 1.7 × 108 IU/mL. Serum HBsAg titers and HBeAg levels were detected by chemiluminescent assays (Roche Diagnostics). For quantitative analysis, values beyond the defined limit of detection were set to the nearby limit value. The levels of ALT and aspartate aminotransferase (AST) were measured locally in accordance with standard procedures.
Statistical Analysis
HBsAg loss was defined as a negative HBsAg result at EOT of PegIFN therapy. Durable HBsAg loss was defined as HBsAg persistently undetectable at the end of follow-up (EOF). HBsAg seroreversion was defined as a positive HBsAg result at EOF following HBsAg loss. Data were expressed as the mean ± SE or frequencies (percentages) when appropriate. Associations between variables were tested using Chi-square, Mann–Whitney U or Spearman correlation when appropriate. The predictive values of the different seromarkers for HBsAg loss during the early initiation of PegIFN treatment were summarized using the receiver operating characteristic (ROC) curve analysis. Individuals who acquired HBsAg loss were excluded from this analysis. All statistical analyses were performed using the statistical software package SPSS (v23.0) (SPSS Chicago, IL). A two-sided P value less than 0.05 was considered significant.
Results
Patient Characteristics
A total of 92 HBeAg-positive pediatric CHB patients with available samples were included in this study. Among them, 45 (48.9%) patients cleared HBsAg at EOT, while 47 (51.1%) did not. Among the 47 patients without HBsAg loss, 26 (28.3%) were defined as non-responders according to the stopping rules.
The baseline characteristics of patients with and without HBsAg loss were compared in Table 1. There were no differences between groups with regard to sex, HBV genotype, ALT, AST, HBsAg titers and sPD-1 levels. However, compared to those without HBsAg loss, children with HBsAg loss had younger age (44.8 ± 4.7 months vs 61.2 ± 5.4 months; P = 0.008), higher levels of HBeAg (3.01 ± 0.05 lg COI vs 2.55 ± 0.13 lg COI; P = 0.018) and lower levels of HBV DNA (7.30 ± 0.12 lg IU/mL vs 7.66 ± 0.11 lg IU/mL; P = 0.026).
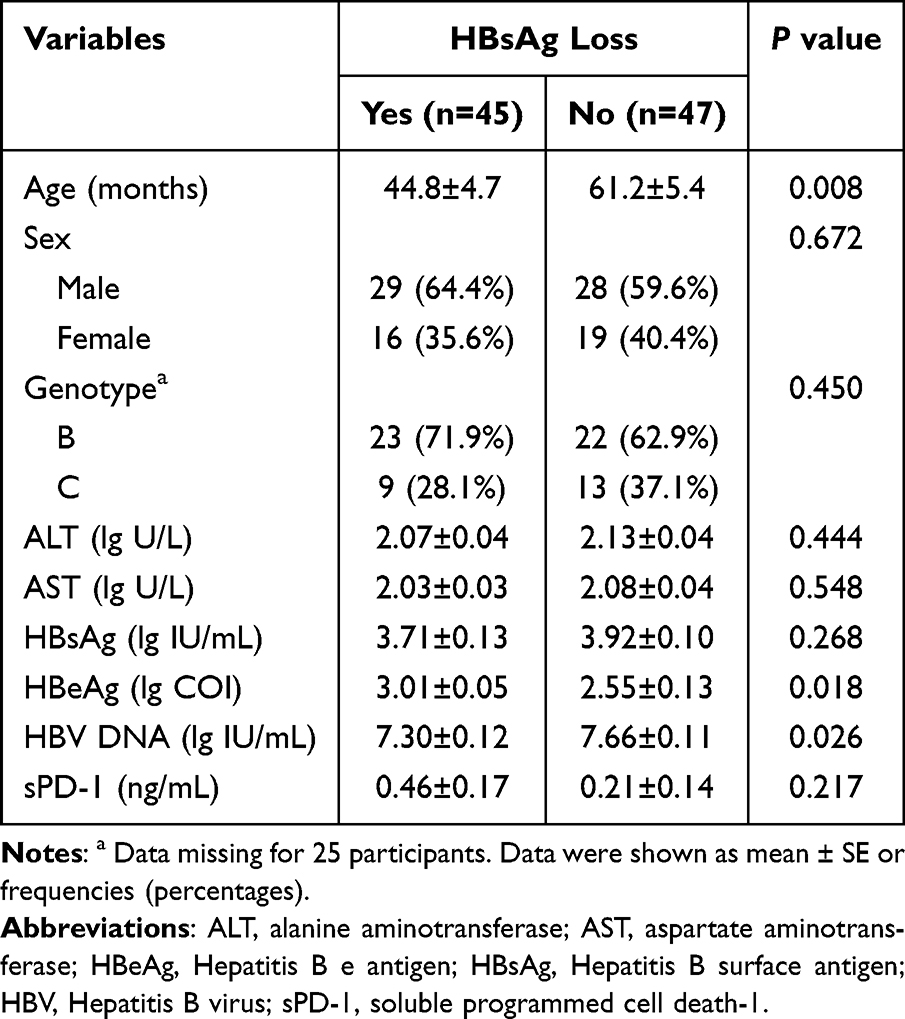 |
Table 1 Characteristics of Demographic Features for Pediatric Patients with and without HBsAg Loss |
Association Between sPD-1 Levels and HBV-Related Laboratory Parameters
Baseline sPD-1 levels did not differ in genotype and sex, and were not associated with baseline age, ALT, AST and HBeAg. However, they showed a strongly inverse correlation with HBsAg (r = −0.570, P < 0.001), and HBV DNA (r = −0.522, P < 0.001) (Figure 1, Figure S1).
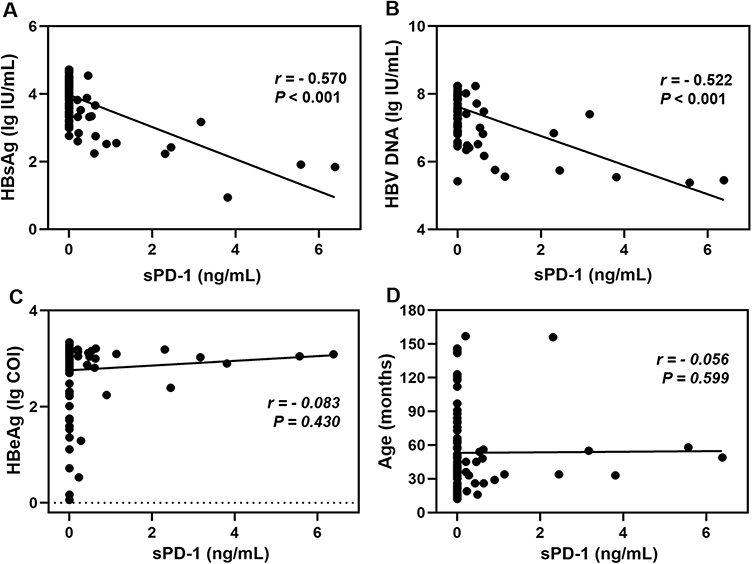 |
Figure 1 Correlations between baseline serum sPD-1 levels and (A) HBsAg (lg IU/mL), (B) HBV DNA (lg IU/mL), (C) HBeAg (lg COI) and (D) Age (months). Abbreviations: HBeAg, Hepatitis B e antigen; HBsAg, Hepatitis B surface antigen; HBV, Hepatitis B virus; sPD-1, soluble programmed cell death-1. |
Trajectories of sPD-1 Levels During the PegIFN Treatment
As shown in Figure 2, the mean sPD-1 levels gradually increased during the course of PegIFN treatment in cases with HBsAg loss: from 0.46 ng/mL at baseline to 3.52 ng/mL at week 12, to 8.12 ng/mL at week 24, and finally to 15.02 ng/mL at EOT (Ptrend < 0.001). A similar trend was observed in cases without HBsAg loss, though it was less pronounced (Ptrend < 0.001).
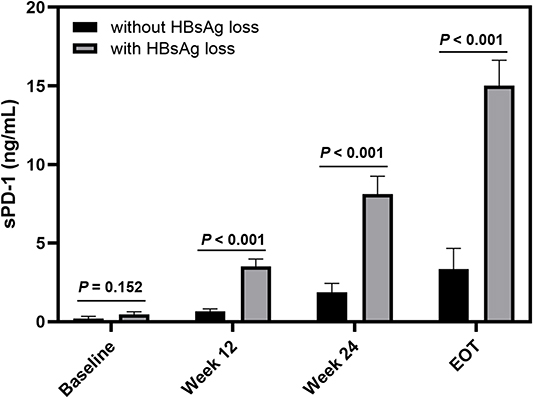 |
Figure 2 Serial serum sPD-1 levels in pediatric patients with and without HBsAg loss at baseline, week 12, week 24 and EOT. Abbreviations: EOT, end of treatment; HBsAg, Hepatitis B surface antigen; sPD-1, soluble programmed cell death-1. |
At baseline, the levels of sPD-1 were comparable in children with or without HBsAg loss (P = 0.152). However, it was significantly higher in children with HBsAg loss, compared to those without HBsAg loss at the weeks 12 and 24, as well as at EOT (P < 0.001 for all the three comparisons). Correlation analysis indicated that sPD-1 levels were strong negatively associated with HBsAg levels (r = −0.871, P < 0.001; r = −0.810, P < 0.001) and HBV DNA load (r = −0.788, P < 0.001; r = −0.726, P < 0.001) at weeks 12 and 24, respectively (Figure 3).
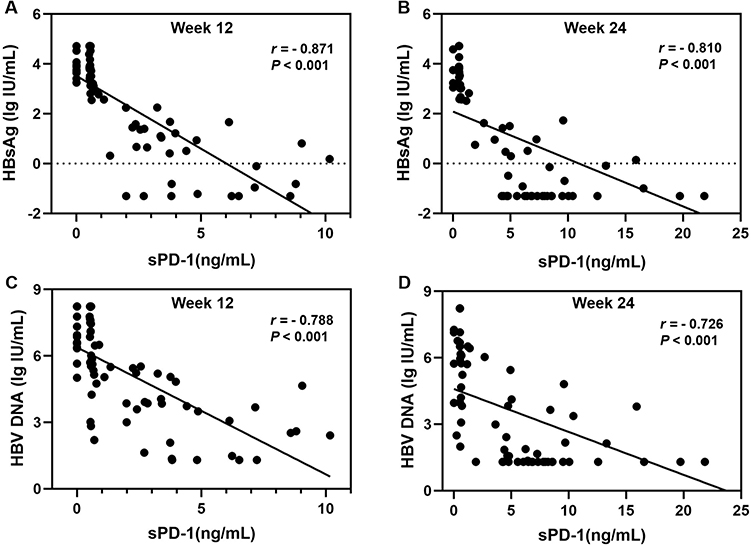 |
Figure 3 The sPD-1 levels strong inverse correlation with HBsAg and HBV DNA levels at Week 12 and 24, respectively. (A and B) HBsAg (lg IU/mL) and (C and D) HBV DNA (lg IU/mL). Abbreviations: HBsAg, Hepatitis B surface antigen; HBV, Hepatitis B virus; sPD-1, soluble programmed cell death-1. |
Serum sPD-1 Levels as Predictors of HBsAg Loss During the PegIFN Therapy
To illustrate the predictive value of single biomarker for HBsAg loss, ROC curves analysis was conducted, with sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) calculated at optimal cut-offs determined by Youden’s index (Table 2). At week 12, sPD-1, HBsAg, and HBV DNA demonstrated strong discriminatory ability, with AUROCs of 0.845 (95% CI, 0.744–0.946), 0.881 (95% CI, 0.798–0.965), and 0.782 (95% CI, 0.676–0.899), respectively. sPD-1 achieved a sensitivity of 76.7% and specificity of 88.6%, with a PPV of 85.2% and NPV of 81.6%. Similarly, at week 24, sPD-1 and HBsAg maintained excellent performance, with AUROCs of 0.863 (95% CI, 0.758–0.969) and 0.881 (95% CI, 0.781–0.981), respectively, both showing identical sensitivity (76.5%), specificity (85.7%), PPV (76.5%), and NPV (85.7%). In contrast, HBeAg levels consistently exhibited poor discriminatory ability across all time points, with all AUROC scores ≤ 0.65 and no significant predictive utility.
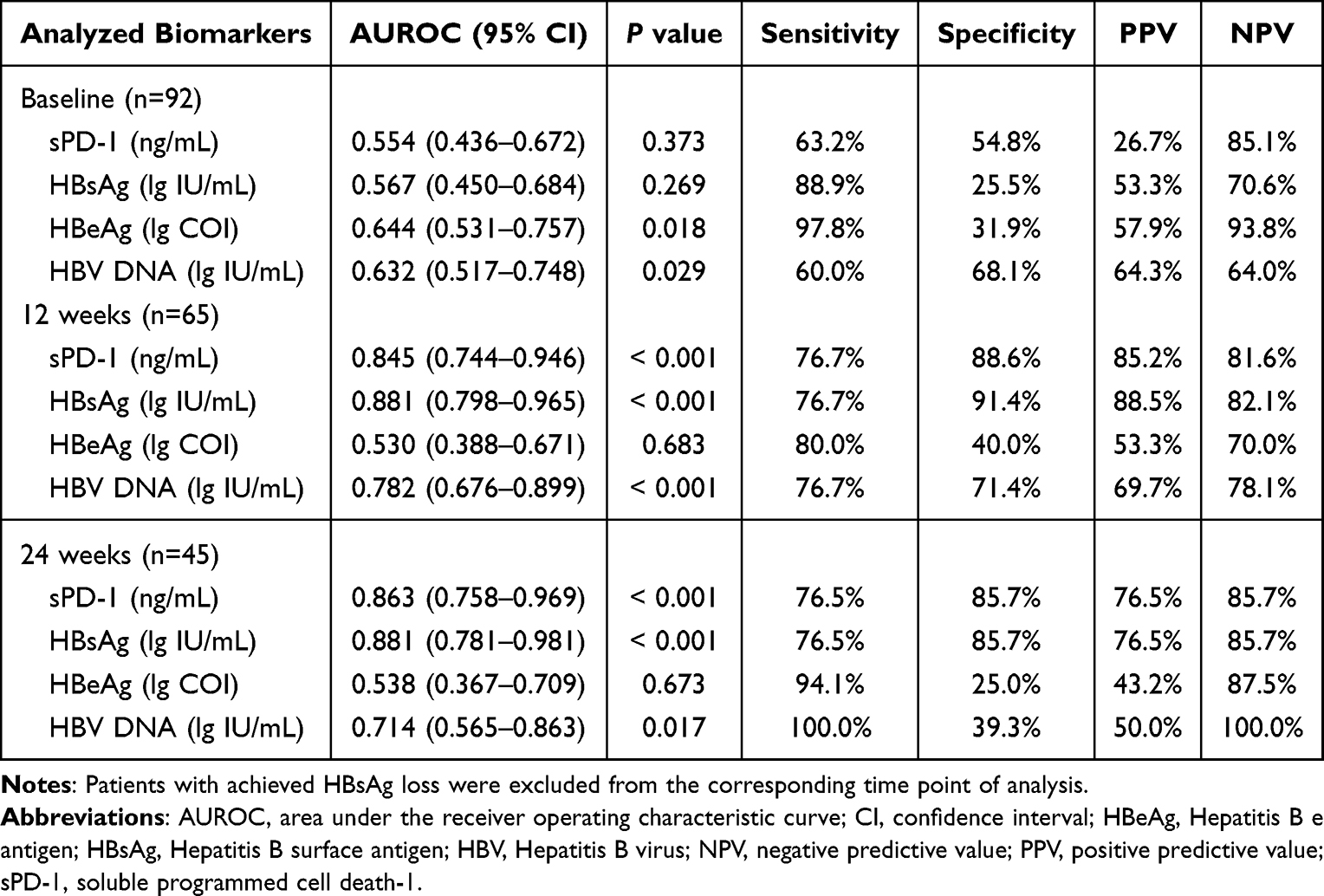 |
Table 2 HBsAg Loss Prediction Was Assessed by sPD-1, HBsAg, HBeAg, and HBV DNA at Baseline, 12 weeks and 24 weeks of PegIFN Treatment |
Follow-up sPD-1 Levels Predict Durable HBsAg Loss After PegIFN Discontinuation
A total of 85 children who had available data on HBsAg levels entered the long-term observational follow-up study with a mean duration of 45.0 months. This included 45 cases with HBsAg loss and 40 cases without HBsAg loss. We found that HBsAg loss was durable in 38 out of 45 individuals (84.4%) at EOF, while seven patients (15.6%) experienced HBsAg seroreversion. Among the 40 cases without HBsAg loss, 36 cases were switched from PegIFN to ETV treatment, and only three of them (8.3%) achieved HBsAg loss.
Except for the 36 individuals with sequential therapy, 87.8% (43/49) had accessible data on serum sPD-1 levels during the follow-up period within 12 months after the discontinuation of Peg-IFN. Individuals with durable HBsAg loss had the highest sPD-1 levels, followed by patients with HBsAg seroreversion, and then those without HBsAg loss (P = 0.009). Additionally, the sPD-1 levels at follow-up were higher than the levels at EOT in patients with durable HBsAg loss (P < 0.001) (Figure S2). However, it remained static in patients with HBsAg seroreversion and without HBsAg loss (P = 0.873, P = 0.744, respectively). Furthermore, in ROC curve analysis, sPD-1 levels at follow-up proved to be a strong predictor of durable HBsAg loss at EOF, achieving an AUROC of 0.804 (95% CI: 0.649–0.959), with a sensitivity of 90.3%, specificity of 66.7%, PPV of 87.5%, and NPV of 72.7% (Figure S3).
Discussion
Identification of factors correlated with HBsAg loss in CHB patients received PegIFN intervention has potentially important clinical significance informing clinical decision-making. Since HBsAg loss is not easily achieved in CHB patients, neither with PegIFN nor nucleos(t)ide analogs (NAs) treatment, previous studies have focus more on factors associated with HBsAg decline or HBeAg seroconversion.21–23 Limited data suggested that age and HBsAg levels can predict HBsAg loss in pediatric CHB patients with IFN treatment.9,10 In the present study, we explore the sPD-1 levels as a predictor of HBsAg loss in pediatric CHB patients with PegIFN intervention. Firstly, we found that the levels of sPD-1 were significantly higher in children with HBsAg loss than in those without HBsAg loss at all of the analyzed time points, except for baseline. Furthermore, serum sPD-1 levels showed a strong negative correlation with HBsAg and HBV DNA levels.18,24 Lastly, the levels of sPD-1 could well discriminate cases with and without HBsAg loss around early PegIFN intervention. However, no significant difference in baseline sPD-1 levels was observed between patients with and without HBsAg loss. These findings indicate that sPD-1 level serves as a dynamic, on-treatment response biomarker to guide personalized PegIFN therapy in HBeAg-positive children, rather than as a baseline biomarker. The levels of sPD-1 could provide early, immunologically relevant feedback during the first 12–24 weeks of treatment, which may optimize the risk–benefit ratio of PegIFN therapy by enabling early, data-driven decisions.
Recent data from a study in HBeAg-negative adults demonstrated that during PegIFN-based therapy, both sPD-1 and HBsAg levels declined in parallel, with a steeper decrease observed in patients achieving HBsAg loss.11 In striking contrast, our study in HBeAg-positive pediatric patients revealed an inverse pattern: while HBsAg levels decreased as expected, sPD-1 levels increased progressively throughout treatment, particularly in those who achieved HBsAg loss. This discrepancy might be due to the fundamental differences in immune context between pediatric and adult CHB. Children with CHB typically harbor a less exhausted HBV-specific T-cell compartment,25 characterized by lower baseline expression of membrane-bound PD-1. PegIFN therapy in this setting appears to activate and expand functional T-cell responses, which in turn drives increased transcription and shedding of sPD-1, a soluble decoy that may further amplify immune reconstitution by blocking PD-1/PD-L1 inhibitory signals.26 In contrast, adults in the referenced study had long-standing infection and, critically, had received NAs therapy for over a year prior to PegIFN initiation. Prolonged antigen exposure in adults leads to profound T-cell exhaustion and high baseline PD-1 expression.27,28 NAs pretreatment may partially restore T-cell function and downregulate PD-1 expression,29 including its soluble form, resulting in the observed decline in sPD-1 during subsequent PegIFN therapy. Thus, the divergent sPD-1 trajectories do not represent conflicting findings, but may rather highlight that sPD-1 dynamics are context-dependent, shaped by age, HBeAg status, prior antiviral exposure, and the baseline degree of T-cell exhaustion. In pediatric patients with preserved immune plasticity, rising sPD-1 serves as a biomarker of successful immune activation; in adults with exhausted immunity and NAs pretreatment, falling sPD-1 may reflect partial immune restoration.
A previous study showed that lower HBsAg levels and young children were correlated with a higher rate of HBsAg loss in patients receiving IFN treatment,10 and our analysis confirmed these findings. Quantification of HBsAg has been regarded as an important marker of viral control, and has been reported to associate with the covalently closed circular DNA (cccDNA) levels in HBeAg-positive individuals.4,30 What’s more, as reported that IFN might have direct effects on the stability or transcription of cccDNA in vitro.31 Therefore, it was reasonable to observe that quantitative HBsAg could predict HBsAg loss in our study. In addition, we also found HBV-DNA alone could offer a good prediction of HBsAg loss. We speculated this might be due to the fact that a relatively low levels of HBV DNA integration and clonal hepatocyte expansion in children with HBeAg-positive CHB, resulting in a good association between HBsAg and HBV DNA levels, as reported in acute hepatitis.32,33
Several important limitations warrant acknowledgment. First, this was a retrospective, single-center study, which inherently limits the generalizability of our findings. Additionally, due to early discontinuation of PegIFN in non-responders (per protocol-defined stopping rules), serial sPD-1 measurements were incomplete for a subset of patients. This may introduce selection bias and limits our ability to fully characterize sPD-1 kinetics across all response trajectories. Consequently, our observations regarding the association between on-treatment sPD-1 dynamics and HBsAg loss require validation in prospective, multi-center cohorts. Second, while our data suggest a strong correlation between rising sPD-1 levels and HBsAg loss, we did not perform mechanistic immunological assays (eg, HBV-specific T-cell profiling) to directly link sPD-1 to immune reconstitution. Future studies should integrate immune monitoring to elucidate the precise biological mechanisms by which sPD-1 contributes to viral control. Third, baseline imbalances existed between responders and non-responders in key variables, including age, HBeAg titer, and HBV DNA level, which may act as confounders. Although these factors are themselves known predictors of response, their uneven distribution underscores the need for multivariate modeling or matched-cohort designs in future investigations to isolate the independent predictive value of sPD-1.
Conclusion
Our findings suggest that sPD-1 may serve as a dynamic, on-treatment immunological biomarker for predicting HBsAg loss in pediatric patients with HBeAg-positive CHB receiving PegIFN therapy, rather than as a static baseline predictor. However, these results require validation in prospective, multi-center studies before clinical implementation.
Acknowledgment
The authors would like to thank all the included children and their parents for their cooperation with this study.
Funding
This work was supported by the Science and Technology Program of Guangzhou (201803010041).
Disclosure
No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article. On behalf of all authors, the corresponding author states that there is no conflict of interest.
References
1. Tang LSY, Covert E, Wilson E. et al. Chronic hepatitis B infection: a review. JAMA. 2018;319(17):1802–1813. doi:10.1001/jama.2018.3795
2. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67(4):1560–1599. doi:10.1002/hep.29800
3. Yang Y, Huang A, Zhao Y. Spontaneous loss of chronic HBV infection markers in treatment-naive children: a systematic review and pooled meta-analyses. Expert Rev Anti Infect Ther. 2021;19(5):649–660. doi:10.1080/14787210.2021.1845652
4. Yeo YH, Ho HJ, Yang HI, et al. Factors associated with rates of HBsAg seroclearance in adults with chronic HBV infection: a systematic review and meta-analysis. Gastroenterology. 2019;156(3):635–646e639. doi:10.1053/j.gastro.2018.10.027
5. Moini M, Fung S, Bode LGM. HBsAg loss as a treatment endpoint for chronic HBV infection: HBV cure. Viruses. 2022;15(1):14. doi:10.3390/v15010014
6. Wirth S, Zhang H, Hardikar W, et al. Efficacy and safety of peginterferon Alfa-2a (40KD) in children with chronic hepatitis B: the PEG-B-ACTIVE study. Hepatology. 2018;68(5):1681–1694. doi:10.1002/hep.30050
7. Liu Y, Li H, Yan X, et al. Long-term efficacy and safety of peginterferon in the treatment of children with HBeAg-positive chronic hepatitis B. J Viral Hepat. 2019;26(1):69–76. doi:10.1111/jvh.13154
8. Fan H, Lin L, Jia S, et al. Interferon alpha treatment leads to a high rate of hepatitis B surface antigen seroconversion in Chinese children with chronic hepatitis B. J Viral Hepat. 2019;26(Suppl 1):77–84. doi:10.1111/jvh.13165
9. Li J, Fan P, Xu Z, et al. Functional cure of chronic hepatitis B with antiviral treatment in children having high-level viremia and normal or mildly elevated serum aminotransferase. J Clin Transl Hepatol. 2023;11(5):1011–1022. doi:10.14218/JCTH.2023.00014
10. Pan J, Wang H, Yao T, et al. Clinical predictors of functional cure in children 1-6 years-old with chronic hepatitis B. J Clin Transl Hepatol. 2022;10(3):405–411. doi:10.14218/JCTH.2021.00142
11. Guo H, Wu L, Yu C, et al. Predictive value of soluble PD-1 for HBsAg loss in HbeAg-negative patients with chronic hepatitis B: results from a prospective study. Hepatol Int. 2025;19(4):809–819. doi:10.1007/s12072-025-10826-2
12. Zheng JR, Wang ZL, Feng B. Hepatitis B functional cure and immune response. Front Immunol. 2022;13:1075916. doi:10.3389/fimmu.2022.1075916
13. Tang S, Kim PS. A high-affinity human PD-1/PD-L2 complex informs avenues for small-molecule immune checkpoint drug discovery. Proc Natl Acad Sci USA. 2019;116(49):24500–24506. doi:10.1073/pnas.1916916116
14. Sharpe AH, Pauken KE. The diverse functions of the PD1 inhibitory pathway. Nat Rev Immunol. 2018;18(3):153–167. doi:10.1038/nri.2017.108
15. Wu H, Miao M, Zhang G, et al. Soluble PD-1 is associated with aberrant regulation of T cells activation in aplastic anemia. Immunol Invest. 2009;38(5):408–421. doi:10.1080/08820130902912332
16. Zhou L, Li X, Huang X, et al. Soluble programmed death-1 is a useful indicator for inflammatory and fibrosis severity in chronic hepatitis B. J Viral Hepat. 2019;26(7):795–802. doi:10.1111/jvh.13055
17. Khan M, Zhao Z, Arooj S, et al. Soluble PD-1: predictive, prognostic, and therapeutic value for cancer immunotherapy. Front Immunol. 2020;11:587460. doi:10.3389/fimmu.2020.587460
18. Hu HH, Jeng WJ, Pan MH, et al. Serum soluble programmed cell death 1 levels predict spontaneous functional cure in inactive carriers with chronic hepatitis B. Aliment Pharmacol Ther. 2022;55(5):558–567. doi:10.1111/apt.16752
19. Xia J, Huang R, Chen Y, et al. Profiles of serum soluble programmed death-1 and programmed death-ligand 1 levels in chronic hepatitis B virus-infected patients with different disease phases and after anti-viral treatment. Aliment Pharmacol Ther. 2020;51(11):1180–1187. doi:10.1111/apt.15732
20. Chu YJ, Jeng WJ, Pan MH, et al. Serum soluble programmed death-1 levels predict the spontaneous HBeAg seroclearance in chronic hepatitis B. J Gastroenterol. 2022;57(6):423–432. doi:10.1007/s00535-022-01874-8
21. Sonneveld MJ, Rijckborst V, Boucher CA, et al. Prediction of sustained response to peginterferon alfa-2b for hepatitis B e antigen-positive chronic hepatitis B using on-treatment hepatitis B surface antigen decline. Hepatology. 2010;52(4):1251–1257. doi:10.1002/hep.23844
22. Fried MW, Piratvisuth T, Lau GK, et al. HBeAg and hepatitis B virus DNA as outcome predictors during therapy with peginterferon alfa-2a for HBeAg-positive chronic hepatitis B. Hepatology. 2008;47(2):428–434. doi:10.1002/hep.22065
23. Buster EH, Hansen BE, Lau GK, et al. Factors that predict response of patients with hepatitis B e antigen-positive chronic hepatitis B to peginterferon-alfa. Gastroenterology. 2009;137(6):2002–2009. doi:10.1053/j.gastro.2009.08.061
24. Tan N, Luo H, Kang Q, et al. High levels of soluble programmed death-1 are associated with virological response in chronic hepatitis B patients after antiviral treatment. Virus Res. 2022;309:198660. doi:10.1016/j.virusres.2021.198660
25. Le Bert N, Gill US, Hong M, et al. Effects of hepatitis b surface antigen on virus-specific and global T cells in patients with chronic hepatitis b virus infection. Gastroenterology. 2020;159(2):652–664. doi:10.1053/j.gastro.2020.04.019
26. Song MY, Park SH, Nam HJ, et al. Enhancement of vaccine-induced primary and memory CD8(+) T-cell responses by soluble PD-1. J Immunother. 2011;34(3):297–306. doi:10.1097/CJI.0b013e318210ed0e
27. McLane LM, Abdel-Hakeem MS, Wherry EJ. CD8 T cell exhaustion during chronic viral infection and cancer. Annu Rev Immunol. 2019;37(1):457–495. doi:10.1146/annurev-immunol-041015-055318
28. Fisicaro P, Barili V, Rossi M, et al. Pathogenetic mechanisms of T cell dysfunction in chronic HBV infection and related therapeutic approaches. Front Immunol. 2020;11:849. doi:10.3389/fimmu.2020.00849
29. Shu Y, Li S, Du Y, et al. Anti-HBV treatment partially restores the dysfunction of innate immune cells and unconventional T cells during chronic HBV infection. Front Immunol. 2025;16:1611976. doi:10.3389/fimmu.2025.1611976
30. Thompson AJ, Nguyen T, Iser D, et al. Serum hepatitis B surface antigen and hepatitis B e antigen titers: disease phase influences correlation with viral load and intrahepatic hepatitis B virus markers. Hepatology. 2010;51(6):1933–1944. doi:10.1002/hep.23571
31. Lucifora J, Xia Y, Reisinger F, et al. Specific and nonhepatotoxic degradation of nuclear hepatitis B virus cccDNA. Science. 2014;343(6176):1221–1228. doi:10.1126/science.1243462
32. Meier MA, Calabrese D, Suslov A, et al. Ubiquitous expression of HBsAg from integrated HBV DNA in patients with low viral load. J Hepatol. 2021;75(4):840–847. doi:10.1016/j.jhep.2021.04.051
33. Jaroszewicz J, Calle Serrano B, Wursthorn K, et al. Hepatitis B surface antigen (HBsAg) levels in the natural history of hepatitis B virus (HBV)-infection: a European perspective. J Hepatol. 2010;52(4):514–522. doi:10.1016/j.jhep.2010.01.014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Predictive Nomogram for Myelosuppression Risk in Chronic Hepatitis B Patients Treated with Peginterferon
Fu J, Deng T, Zheng T, Shi P, Zhu W, Tao M, Wen Z, Wu X
Infection and Drug Resistance 2025, 18:1793-1805
Published Date: 9 April 2025