Back to Journals » Nature and Science of Sleep » Volume 17

Sleep Restriction and Weekend Sleep Compensation Relate to Eating Behavior in School-Aged Children
Authors Chamorro R ![]() , Garrido-González M
, Garrido-González M ![]() , Gutierrez M, Santos JL, Weisstaub G
, Gutierrez M, Santos JL, Weisstaub G ![]()
Received 17 January 2025
Accepted for publication 6 June 2025
Published 22 July 2025 Volume 2025:17 Pages 1671—1681
DOI https://doi.org/10.2147/NSS.S509636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Rodrigo Chamorro,1 Marcelo Garrido-González,2 Mariolly Gutierrez,3 José L Santos,4,5 Gerardo Weisstaub6
1Department of Nutrition, Faculty of Medicine, University of Chile, Santiago, Chile; 2Faculty of Education, Diego Portales University, Santiago, Chile; 3Department of Pediatrics, Finis Terrae University, Santiago, Chile; 4Department of Nutrition, Diabetes, and Metabolism, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile; 5Institute for Sustainability and Food Chain Innovation (IS-FOOD), Department of Health Sciences, Public University of Navarre, Pamplona, Spain; 6Institute of Nutrition and Food Technology, University of Chile, Santiago, Chile
Correspondence: Gerardo Weisstaub, Institute of Nutrition and Food Technology, University of Chile, Santiago, Chile, Tel +562 29781412, Email [email protected]
Purpose: Several studies showed that shortened sleep duration and subsequent sleep debt are related to obesity risk in children. We evaluated the association between habitual sleep restriction and eating behavior in school-aged children with and without obesity.
Patients and Methods: In 131 school-aged children (mean [±SD] age 10.2 ± 2.0 years), we assessed eating behavior through the Child Eating Behavior Questionnaire (CEBQ). Actigraphic recordings measured sleep patterns for 4 consecutive days, including a weekend day. CEBQ scores were calculated in sleep-restricted children (having a nighttime sleep duration < 8 hours) during week and weekend days and compared for those with (n = 67) and without obesity (n = 64). CEBQ scores were also compared between children with and without sleep compensation (a weekend catch-up in sleep duration ≥ 1 hour compared to weekdays’ sleep duration).
Results: The mean sleep duration was 8.0 ± 1.3 h, and about 70% of children slept less than the daily sleep recommendation. Children having sleep restriction had higher scores in the four CEBQ pro-ingestion dimensions (all P< 0.021) as well as lower “satiety responsiveness” but higher “emotional undereating” scores (both P< 0.049). No differences in CEBQ were found in the normal-weight group when comparing children with or without sleep restriction. In the group with obesity, however, those sleep-restricted showed lower ratings in “slowness of eating” (P< 0.015), “satiety responsiveness”, and “food fussiness” (both P< 0.035) compared to non-restricted, particularly during weekend days. Finally, children showing no sleep compensation on weekend days had higher pro-ingestion (all P< 0.020) and lower anti-ingestion scores (all P< 0.041).
Conclusion: Sleep duration was lower than the recommended sleep in this sample of school-aged children. Sleep restriction was associated with enhanced pro-ingestion eating behavior scores and reduced anti-ingestion scores. Sleep compensation appears to have a positive effect on eating behavior scores.
Keywords: sleep duration, sleep compensation, eating behavior, obesity, children
Introduction
Sleep has a close connection with body weight and obesity.1 Several studies have shown an association between sleep duration and obesity in childhood.2,3 Sleep is an essential regulator of energy balance, appetite, and weight maintenance,4,5 and shorter sleep duration is associated with an increased obesity risk among children and adolescents.6 The prevalence of obesity in early childhood decreases inversely with sleep duration, independently of other risk factors.7,8 As in other age groups, national surveys in the United States of America and several epidemiological studies emphasize sleep restriction in most children and adolescents.1,4,9 It has been shown that sleep duration is less than the recommended 9 hours in children and adolescents, with a marked decrease depending on age.10 Poor sleep in pediatric population has been associated with behavioral, cognitive, and metabolic consequences, highlighting the relevance of healthy sleep patterns for children’s health.11,12 In addition, several characteristics related to sleep patterns have been proposed to be involved in the sleep-obesity association, particularly in children. Among those, sleep quality, sleep disturbances, and sleep timing are associated with adiposity and body composition features in young adolescents.13 Besides, sleep characteristics have also been shown to be related to eating behavior at this age.14
Eating behavior is structured cognitively in humans and is associated with endogenous regulation modulated by environmental factors.15 Moreover, the influence of different eating patterns based on nutritional status has been demonstrated in children.16 Children with obesity tend to have characteristic responses to food such as eating without hunger, insensitivity to caloric preload, greater speed of eating, increased cephalic response to food, higher intake of foods with greater palatability and, in general, constant worry by food.16,17
Sleep patterns have been associated with obesity, energy intake, and eating behavior in children and adults.18,19 Some reports in children have shown that lower sleep quality (assessed by questionnaire) was associated with increased emotional overeating and food responsiveness in low-income toddlers.18 In children and adolescents (6–17 years), short sleep was associated with increased energy intake and unhealthy eating behavior at breakfast and snack meals.20 Also, short sleep duration in children with obesity (8–14 years) was related to loss-of-control eating after experiencing negative affect.21 However, fewer reports have assessed the role of sleep characteristics such as sleep debt and catch-up sleep on weekend days on children’s eating behavior. As obesity significantly influences eating behavior and also sleep may have a role in this relationship, we compared the eating behavior characteristics in children with and without obesity according to habitual sleep restriction. Our aim was to evaluate the association between habitual sleep restriction and eating behavior in school-aged children with and without obesity.
Materials and Methods
Participants
A comparative cross-sectional study was carried out. We studied children between 8 and 14 years of age, both male and female, with normal weight and obesity. Children with normal weight were recruited from a public school located in the commune of Macul (South-East area of Santiago, Chile), and children with obesity were recruited from those attending an outpatient clinic for obesity at the Clinical Care Center of the Institute of Nutrition and Food Technology (INTA, Macul, Santiago). Sample size of n=120 was based on the meta-analysis published by Sanjay et al, which reported a difference in sleep duration between healthy children and children with obesity between 30–60 min with a power of 80% (beta = 0.8) and confidence of 95% (alpha =0.05).22
We studied a group of 131 preadolescents (Tanner stages I or II), 8 to 12 years old, of both sexes, consulting at the clinical center in our Institute. We excluded participants with unanswered or uncompleted questionnaires, incomplete actigraphic recordings, obesity secondary to any pathology, eutrophic or obese children with any chronic or acute disease, and children taking prescription drugs or supplements (ie, melatonin) interfering with the sleep-wake pattern or prescription drugs affecting eating behavior.
The study protocol (#41-2005) was approved by the local Ethics Committee of INTA, University of Chile, according to the Declaration of Helsinki. Written informed consent was obtained from the parent and informed assent obtained from all children.
Anthropometrics
Weight was measured with an electronic column scale (Seca 780, Seca ©, Hamburg, DE) with an accuracy of 0.1 kg and a capacity of up to 150 kg. Height was measured using a wall-mounting measuring rod (Seca 216, Seca ©, Hamburg, DE), following the international Frankfurt method. Body mass index (BMI) was then calculated. According to the World Health Organization (WHO), nutritional status (normal weight and obesity) was evaluated using BMI according to the growth reference data for 5–19 years as proposed by the WHO standards, defining obesity as having a BMI ≥ 2 standard deviation for age and sex.23
Eating Behavior Scores
Eating behavior can be evaluated by using several instruments. The Child Eating Behavior Questionnaire (CEBQ) is one of the most used to assess eating behavior in children17 and has been validated in Chilean children (a license to use the adapted CEBQ version was granted to J.L.S).24 The CEBQ, developed in English children and adapted to the Chilean population,24 evaluates eating inclinations associated with the risk of obesity. The items are divided into 4 pro-ingestion dimensions: food responsiveness, enjoyment of food, desire to drink, and emotional overeating. Also, 4 anti-ingestion dimensions are estimated: satiety responsiveness, slowness in eating, emotional undereating, and food fussiness. In this questionnaire, a higher score indicates greater emphasis on the considered dimension of eating behavior. For this study, we used the CEBQ responded by the parents (mother and/or father) or the person in charge of each child to assess eating behavior.
Sleep-Wake Pattern
We objectively evaluated sleep and wake patterns through actigraphy. Sleep was assessed using Actigraphic recordings (Actiwatch ® 64, Respironics), placed 24 hours a day on the non-dominant hand for 4 consecutive days (including at least one weekend day). Parents and children were instructed to use the actigraph continuously and only remove it when the child bathed (noting the date and time of removal and placement in an actigraph diary). Motor activity (counts/minute) was recorded every 0.25 minutes. Sleep onset was considered when actigraphic activity showed zero values for a minimum of five minutes, nocturnal awakenings when this activity was greater than zero for more than five minutes followed by a period of sleep, and daytime awakening when motor activity was greater than zero for 5 minutes followed by wakefulness.
Actigraphic data were analyzed with Actiware-Sleep 3.4 software at the Sleep Laboratory, INTA, University of Chile. We used the Actiware-Sleep algorithm in the Sleep Analysis tool, allowing us to analyze sleep and wakefulness during nighttime automatically. After automatic processing, one researcher reviewed actograms and checked for potential sleep onset and offset misestimation. If necessary, a second automatic processing was carried out, and outcomes of interest were obtained. The following sleep-wake parameters were analyzed:
Bedtime and get-up time: the time at which the children went to bed at night and left the bed the following day, respectively (in hh:mm); sleep start: time of sleep initiation, calculated as the first 10-minute period in which no more than one epoch was scored as movement; sleep offset time, calculated as the last 10-minute period in which no more than one epoch was scored as movement (in hh:mm); time in bed: time difference between bedtime and get up time (in hours); sleep time; time difference between sleep end and sleep start time (in hours); actual sleep time: an index of the amount of the assumed sleep time that is actually sleep, calculated by dividing the actual sleep time by the assumed sleep time and multiplying by 100 (in %); wake time: time difference between sleep start and sleep end that is scored as wake (in hours); actual wake time: index of the amount of the assumed sleep time that is actually wake, calculated by dividing the awake time by the assumed sleep time and multiplying by 100 (in %); and sleep latency: the period required for sleep onset after bedtime (bedtime - sleep start, in hours).
Sleep Restriction and Sleep Compensation
We defined sleep restriction as a sleep duration of 8 hours or less, with 8 hours representing a 1-hour difference regarding the lower limit of adequate daily sleep duration (9–11 hours) for children between 6–13 years, as proposed by the National Sleep Foundation (NSF).10 According to the NSF, the recommended sleep duration was established as at least 9 hours/night, which is the lower limit of adequate daily sleep duration. As sleep patterns differ between weekdays and weekend days, with children having the chance to increase sleep duration (or compensate for sleep debt) during weekend days, we compared the effect of sleep compensation on eating behavior scores, we evaluated sleep timing and duration over week and weekend days. Further, sleep compensation was defined as a weekend catch-up in sleep duration ≥ 1 hour compared to weekdays.
To assess the role of sleep timing and its relationship with sleep regularity, we also studied social jet lag (SJL). SJL highlights the difference in sleep timing between work and free days, reflecting the difference between social and biological time.25 It has been described that SJL is highly common in Westernized societies, particularly in children and adolescents.26 We first calculated the midpoint between sleep onset and waking on weekdays (school nights) and weekends (free days, including holidays). SJL was then calculated as the difference (in hours) in the midpoint of sleep on weekdays and weekends.
Statistical Analyses
A descriptive analysis of the characteristics of the children in the sample was carried out according to the normality distribution of variables. Data are expressed as mean and standard deviation unless otherwise indicated. To evaluate differences between groups of sleep restricted and non-sleep restricted children as well as between those with and without sleep compensation over weekend days, a Student’s t-test for independent groups was used. Categorical variables’ distribution differences between groups were evaluated using the chi-squared or Fisher’s exact test as needed. In all analyses, we used a significance level of 5%. STATA® v.13.1 (Stata Corporation, College Station, TX) software was used, and GraphPad Prism 8.2 (GraphPad Prism Software, Inc. San Diego, CA) for figure processing.
Results
A total of 131 boys and girls were studied, 67 with normal-weight (51.1%) and 64 with obesity (48.9%), with a mean age of 10.2 ±2.0 years (range 7.3–14.1 years, Table 1). Most of the evaluations (71.8%) occurred in the fall and winter seasons. For the whole sample, bedtime and get-up time occurred late with an average of 22:48 ± 1:18 and 08:42 ± 01:30 h, respectively. The mean nighttime sleep onset occurred at 23:24 ± 01:18 h, while the average sleep offset time was 08:12 ± 01:30 h. About 70% of children had a sleep duration lower that the sleep recommendation range for age (at least 9 h per night). Table 1 also shows the mean scores for each of the 8 CEBQ dimensions analyzed. We also analyzed the relationship between BMI z-score and the eating behaviors scores, showing that the enjoyment of food (Pearson’s r: 0.52, p=0.0001), emotional overeating (Pearson’s r: 0.39, p=0.0001), food responsiveness (Pearson’s r: 0.53, p=0.0001), desire to drink (Pearson’s r: 0.37, p=0.0001), satiety responsiveness (Pearson’s r: - 0.20, p=0.016), and slowness in eating (Pearson’s r: - 0.34, p=0.0001), but not emotional undereating (Pearson’s r: 0.06, p=0.44) or food fussiness (Pearson’s r: - 0.11, p=0.14) were significantly correlated with BMI z-score in our sample.
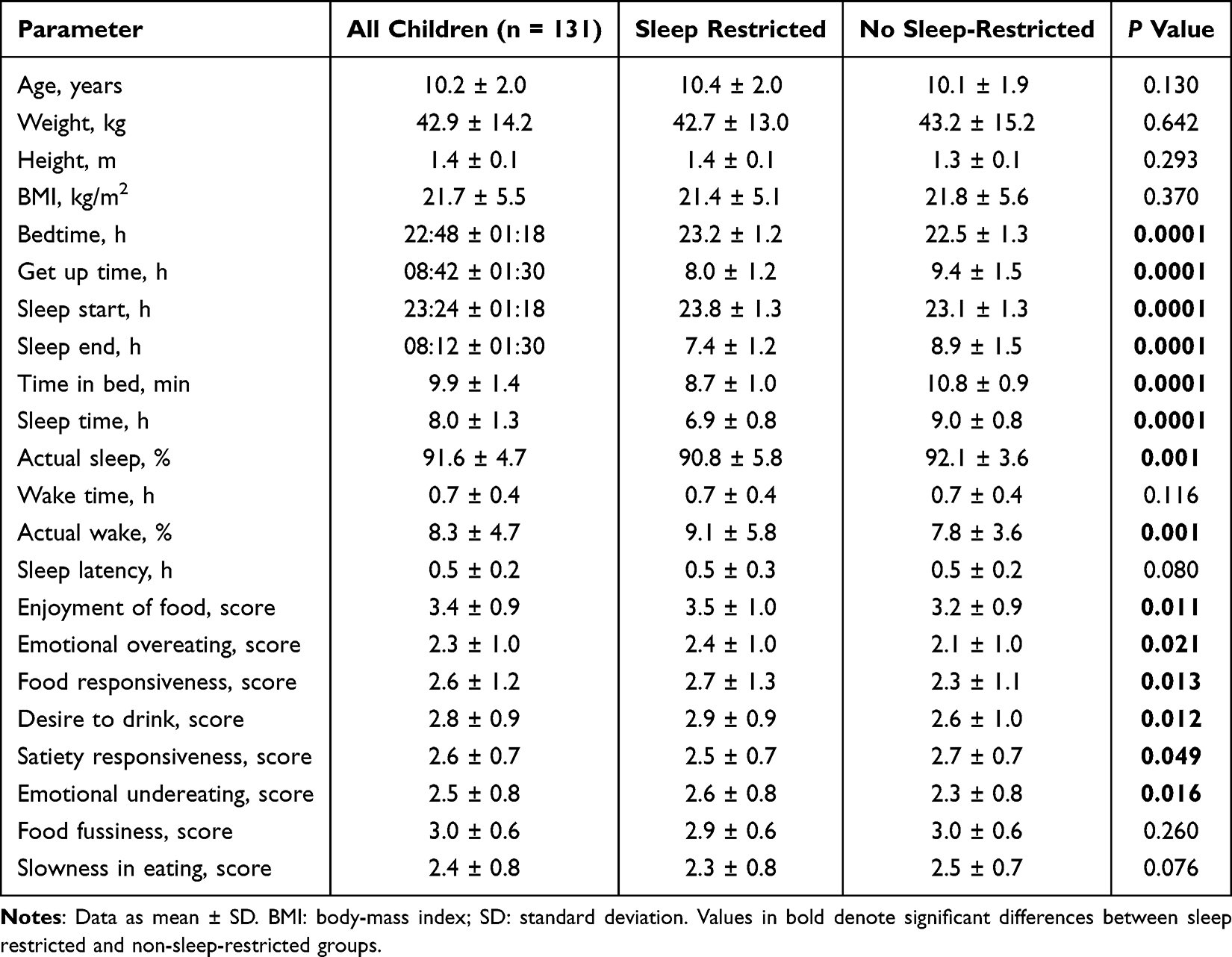 |
Table 1 Anthropometrics, Sleep, and Eating Behavior Parameters According to Habitual Sleep Restriction |
Table 1 also shows anthropometric parameters, sleep characteristics, and the eating behavior dimensions between children with and without habitual sleep restriction (defined as a nighttime sleep duration of less than 8 hours). No anthropometric differences were found between children with and without sleep restriction. As expected, sleep onset and offset times were earlier and later in the group without sleep restriction (all P < 0.0001). The non-sleep-restricted group showed lower actual wake time, indicating less sleep fragmentation during the night (P < 0.001). Regarding CEBQ dimensions, we found significantly higher scores for all pro-ingestion dimensions in the sleep-restricted group (all P < 0.021). On the other hand, two anti-ingestion dimensions’ scores were higher (satiety responsiveness) and lower (emotional undereating) in the non-sleep-restricted group (both P < 0.049, Table 1).
As shown in Table 2, no differences were found regarding CEBQ dimensions in children with normal-weight, neither during weekdays nor weekend days. The same analysis in children with obesity showed no significant differences in pro-ingestion dimensions between subgroups of children with or without sleep restriction during week or weekend days. However, during weekdays, the slowness of eating component of the anti-ingestion dimension was higher in the children with obesity but without sleep restriction (P = 0.015). Differences during weekdays were consistent, with higher satiety responsiveness and lower food fussiness in children with obesity but no sleep restriction (both P < 0.035, Table 2).
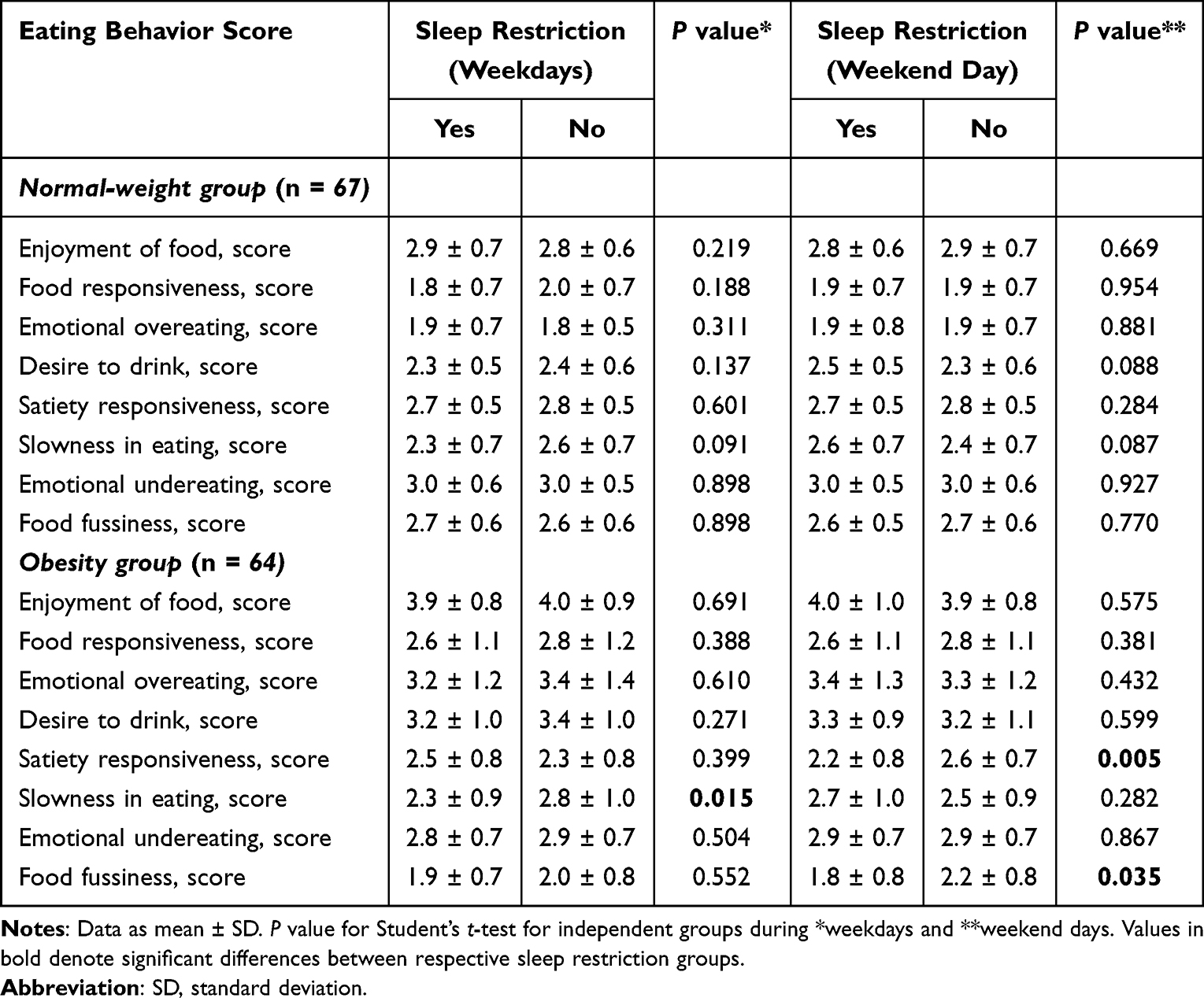 |
Table 2 Eating Behavior, Assessed by CEBQ, According to Sleep Restriction and Nutritional Status |
As shown in Figure 1, sleep compensation significantly modified CEBQ dimension scores. Enjoyment of food (P = 0.006), emotional overeating (P = 0.009), food responsiveness (P = 0.0005), and desire to drink (P = 0.020) presented a higher score in the children without sleep compensation. On the contrary, satiety responsiveness (P = 0.0007) and slowness in eating (P = 0.041) scores were lower, and emotional undereating was higher in this group (P < 0.010, Figure 1), with no differences regarding the food fussiness component. Finally, SJL measurements did not differ between children having or not sleep restriction or between those with and without sleep compensation (data not shown).
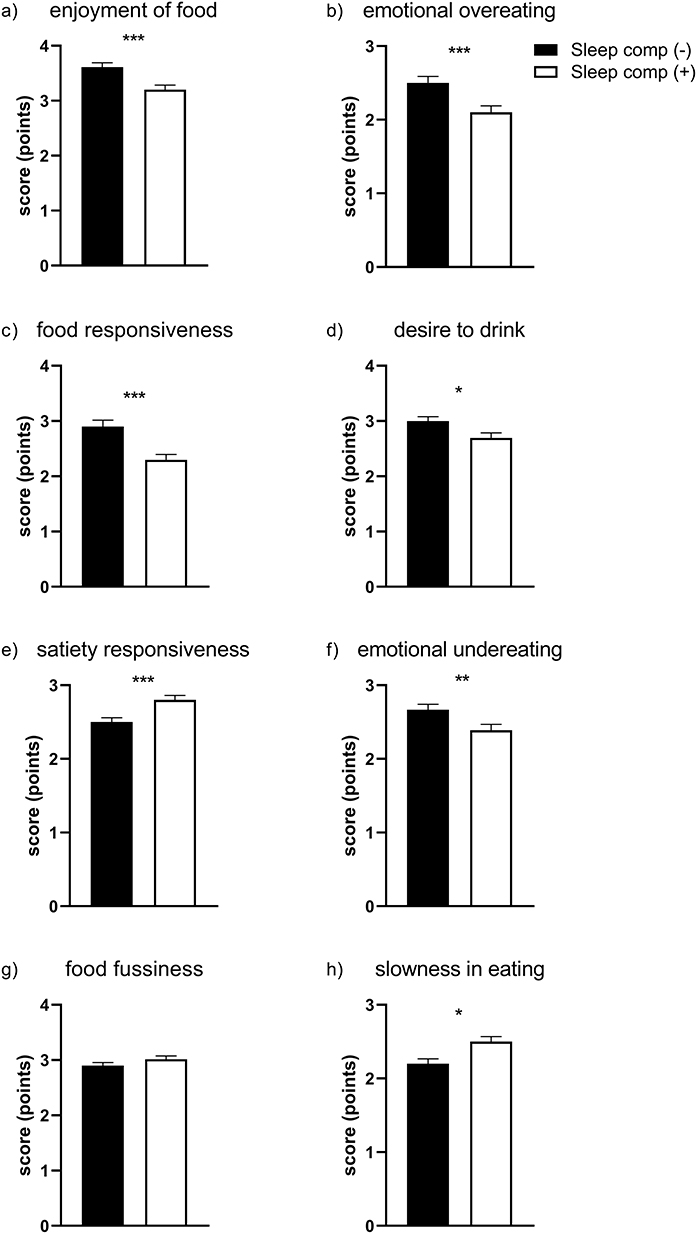 |
Figure 1 Eating behavior, assessed by CEBQ, according to sleep compensation on weekend days. CEBQ scores: (a) enjoyment of food; (b) emotional overeating; (c) food responsiveness; (d) desire to drink; (e) satiety responsiveness; (f) emotional undereating; (g) food fussiness; (h) slowness in eating. Sleep comp (-): children not having sleep compensation, defined as a weekend catch-up in sleep duration ≥ 1 hour compared to weekdays’ sleep duration; Sleep comp (+): children having sleep compensation over weekend days. Data as mean ± SEM. *p<0.05; **p<0.010; ***p<0.009. |
Discussion
In the present study, we aimed to compare eating behavior scores according to sleep patterns of school-aged children with and without obesity. Our main results show that children with habitual sleep restriction were characterized by having higher pro-ingestion and lower satiety response scores compared with their non-sleep-restricted peers. Also, we found that children without obesity showed no differences in eating behavior (assessed by CEBQ scores), irrespective of whether they were sleep-restricted or not. In children with obesity and sleep restriction, however, we found lower satiety responsiveness and higher food fussiness, particularly during weekend days. Finally, we found that children with a sleep pattern showing no sleep compensation over weekend days had higher pro-ingestion and lower anti-ingestion scores than those with sleep compensation.
Regarding sleep patterns, we found that bedtime and sleep onset occurred late in this sample of children and adolescents, with mean sleep onset time quite late in the evening (23.4 ± 1.3 h for the whole sample). Accordingly, mean sleep duration was around 8.0 hours for the entire sample, significantly shorter than the recommended sleep duration of 9 to 11 hours of sleep a day for school-age children (according to the NSF).10 These data align with previous findings reporting that children and adolescents are increasingly exposed to a regular sleep debt.4,27,28 Even when children tend to reduce the amount of sleep from school age to adolescence influenced by biological and external factors,29 having less than the recommended sleep amount is associated with metabolic, behavioral, cognitive, and academic performance consequences.10 Several factors could affect habitual children’s sleep patterns over the week. Among others, it has been reported that age, minority ethnicity, neighborhood distress, parent education, parent income, pubertal status, and BMI are all associated with a higher variability in sleep duration.30
Several studies have found a negative association between nighttime sleep duration and body mass index in children.8,31–34 Several observational studies and meta-analyses of epidemiological studies have shown that sleep duration is inversely related to BMI and adiposity in children and adolescents.3,28,35–37 More recently, some studies have evaluated the connection between pediatric sleep duration and eating behavior. Miller et al, studying a sample of 134 low-income toddlers, found lower sleep quality (assessed by questionnaire) associated with eating behavior scores (evaluated by the CEBQ-toddler), particularly with increased emotional overeating and food responsiveness.18 In a large sample of children and adolescents (6–17 years), it was reported that short sleep was associated with increased energy intake and unhealthy eating behavior at breakfast and snack meals.20 It has also been shown that short sleep in children with obesity (8–14 years) is related to loss-of-control eating after experiencing a negative mood state, suggesting that sleep characteristics are a factor in eating regulation in this age group.21,38
Interestingly, an experimental study conducted in children (8–11 years)39 showed that reducing sleep duration by 1.5 hours (achieved by delaying sleep onset) led to higher energy intake from sugar-sweetened beverages and higher energy intake after 20:00h but not earlier during the day, highlighting the adverse role of sleep restriction for meal timing in its relationship with obesity.40 A recent study in 8–12-year-old children41 reported that sleep restriction (1 hour less) over one week led to more energy-dense foods consumption. Children under the sleep restriction condition also showed increased emotional overeating and undereating without differences in satiety responsiveness, findings that are in part in line with our data showing higher emotional overeating scores in sleep-restricted children. Altogether, these results suggest that poorer sleep may increase children’s obesity by affecting eating behavior regulation, exposing them to increased emotional eating, and choosing particularly unhealthy foods.
We also found that children having no sleep compensation over weekend days had higher pro-ingestion and lower anti-ingestion scores. Our results are aligned with previous findings in 4–10-year-old children, reporting that children with obesity had a more irregular sleep pattern during the week, with shorter and more variable sleep during the weekend than on weekdays,28 and irregular sleep is associated with poor diet quality in school-aged children.42
Wing et al evaluated the effect of sleep compensation during weekend days and holidays in a large sample of school-age children (mean age ~ 9 years). They showed that sleep-restricted children who did not compensate for sleep debt over weekends/holidays had an OR 2.59 for having obesity compared with those showing sleep compensation,43 findings in line with others.44 These last results are also consistent with one report showing that weekend catch-up sleep was shorter in adolescents with obesity compared to those without obesity. In this last study, obesity was significantly associated with short sleep duration and shorter duration of weekend catch-up sleep.34 Our results that children with obesity and sleep-restriction shows differences in eating behavior components compared to normal-weight peers, and that those children with sleep compensation have improved eating behavior profile are consistent with previous evidence.45 Both a catch-up sleep and sleep regularity could be protective factors for eating regulation in school-age children.46
It is important to note that evidence is not uniform as others have shown that weekend sleep duration and weekend catch-up sleep were positively associated with eating in the absence of hunger in children and adolescents47 or found no association between weekend catch-up sleep and obesity risk.48
Several mechanisms are postulated that could explain the relationship between alterations in the sleep-wake pattern and obesity. It has been described that hormones involved in appetite regulation, such as leptin and ghrelin, are adversely modified in subjects who have short sleep,4,49,50 and the increase in the time spent awake at night would facilitate an increased energy intake. Tiredness and fatigue as consequences of sleep restriction would make it challenging to promote physical activity. A chronic lack of sleep could lead to eating energy-dense foods and a higher hedonic drive to eat.51 It has been suggested that sleep restriction could lead to increased food consumption in response to adverse emotions (emotional overeating).41 Even when we found that sleep restriction increased all scores for the pro-ingestion domain of the CEBQ, we found higher emotional overeating and emotional undereating scores in children with sleep restriction. These two components of eating behavior are closely related, and children who overeat after an emotional setting are also likely to undereat.52 It has been proposed that sleep restriction might expose children to emotional undereating when exposed to low-energy, healthier food. Still, they may display emotional overeating when exposed to more hedonic food stimuli.41 In the context of sleep restriction, children with obesity might be exposed to a higher risk for overeating and reduced anti-ingestion dimensions of the eating behavior. As we also showed here, sleep restriction might affect differently to children without obesity (for instance, increasing anti-ingestion dimensions), highlighting the relevance of sleep patterns in the modulation (and consolidation) of eating behavior through childhood and adolescence.
Among the strengths of our study are the objective evaluation of the duration and characteristics of nocturnal sleep and the use of a validated instrument to evaluate eating behavior in Chilean children. As limitations, we can mention a small sample size and the fact that we have performed only 4 days of actigraphy on each child. The low sample size could hamper the potential to find significant associations between eating behavior and main sleep characteristics, therefore, further studies assessing this relationship should be conducted in larger samples. The use of only 4 days of actigraphy was due to practical limitations for children’s use of actigraphs in the studied sample. Even when included at least one weekend day, it could prevent us looking at a more comprehensive children’s sleep pattern, as it has been shown that more than 5 days of actigraphic recordings per week are desirable in this age group.53,54 Another weakness is that we do not objectivize food intake or eating behavior, which would be desirable in a more experimental work context. Our study lacked objective measurements of eating behavior, which could bias the information collected. However, we used a questionnaire that has been widely validated in several countries, including Chile.24,55 It has been described that eating behavior, measured through CEBQ, is a relatively stable trait over time in children, showing a good reproducibility and high internal consistency.
In conclusion, sleep debt was high in this sample of school-aged children. Sleep restriction was related to enhanced pro-ingestion scores and reduced anti-ingestion components of eating behavior. Sleep compensation appears to have a positive effect on eating behavior features. Our results allow us to describe the association of sleep characteristics related to eating behavior in school-aged children. Further research is needed to assess their relevance regarding childhood obesity.
Abbreviations
CEBQ, Child Eating Behavior Questionnaire; WHO, World Health Organization; BMI, Body-mass index; NSF, National Sleep foundation; SJL, Social jet lag.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, GW, upon reasonable request.
Acknowledgments
We are grateful to all children and their parents who participated in our research. RC thanks the Chilean National Research and Development Agency (Fondecyt Iniciación Project #11230075). JLS thanks support from Chilean grant FONDECYT # 1090388.
Author Contributions
RC: Conceptualization; Investigation; Writing - Original draft and Writing, Reviewing & editing; MG: Data curation; Formal analysis; Visualization, and Writing - Reviewing & editing; MGu: Methodology, Investigation, Data curation; Formal analysis, and Writing - Reviewing & editing; JLS: Methodology; Writing - Reviewing & editing; GW: Conceptualization, Methodology, Resources, and Writing - Reviewing & editing. All authors agreed to the final version to be published in the journal to which the article has been submitted. All authors agreed to be accountable for all aspects of this work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Broussard JL, Van Cauter E. Disturbances of sleep and circadian rhythms: novel risk factors for obesity. Curr Opin Endocrinol Diabetes Obes. 2016;23(5):353–359. doi:10.1097/MED.0000000000000276
2. Chaput JP, Lambert M, Gray-Donald K, et al. Short sleep duration is independently associated with overweight and obesity in Quebec children. Can J Public Health. 2011;102(5):369–374. doi:10.1007/BF03404179
3. Cappuccio FP, Taggart FM, Kandala NB, et al. Meta-analysis of short sleep duration and obesity in children and adults. Sleep. 2008;31(5):619–626. doi:10.1093/sleep/31.5.619
4. Van Cauter E, Spiegel K, Tasali E, Leproult R. Metabolic consequences of sleep and sleep loss. Sleep Med. 2008;9:S23–S28. doi:10.1016/S1389-9457(08)70013-3
5. Kaar JL, Schmiege SJ, Vadiveloo M, Simon SL, Tovar A. Sleep duration mediates the relationship between health behavior patterns and obesity. Sleep Health. 2018;4(5):442–447. doi:10.1016/j.sleh.2018.07.004
6. Wu Y, Gong Q, Zou Z, Li H, Zhang X. Short sleep duration and obesity among children: a systematic review and meta-analysis of prospective studies. Obes Res Clin Pract. 2017;11(2):140–150. doi:10.1016/j.orcp.2016.05.005
7. Nielsen LS, Danielsen KV, Sørensen TIA. Short Sleep Duration as a Possible Cause of Obesity: Critical Analysis of the Epidemiological Evidence; 2011. doi:10.1111/j.1467-789X.2010.00724.x
8. Touchette É, Petit D, Tremblay RE, et al. Associations between sleep duration patterns and overweight/obesity at age 6. Sleep. 2008;31(11):1507–1514. doi:10.1093/sleep/31.11.1507
9. Nixon GM, Thompson JMD, Han DY, et al. Short sleep duration in middle childhood: risk factors and consequences. Sleep. 2008;31(1):71–78. doi:10.1093/sleep/31.1.71
10. Hirshkowitz M, Whiton K, Albert SM, et al. National sleep foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1(4):233–243. doi:10.1016/j.sleh.2015.10.004
11. Medic G, Wille, Hemels, Wille M, Micheline M, Hemels ME. Short- and long-term health consequences of sleep disruption. Nat Sci Sleep. 2017;9:151–161. doi:10.2147/NSS.S134864
12. Gohil A, Hannon TS. Poor sleep and obesity: concurrent epidemics in adolescent youth. Front Endocrinol. 2018;9:364. doi:10.3389/fendo.2018.00364
13. Jarrin DC, McGrath JJ, Drake CL. Beyond sleep duration: distinct sleep dimensions are associated with obesity in children and adolescents. Int J Obes. 2013;37(4):552–558. doi:10.1038/ijo.2013.4
14. Burt J, Dube L, Thibault L, Gruber R. Sleep and eating in childhood: a potential behavioral mechanism underlying the relationship between poor sleep and obesity. Sleep Med. 2014;15(1):71–75. doi:10.1016/j.sleep.2013.07.015
15. Clark HR, Goyder E, Bissell P, Blank L, Peters J. How do parents’ child-feeding behaviours influence child weight? Implications for childhood obesity policy. J Public Health. 2007;29(2):132–141. doi:10.1093/pubmed/fdm012
16. Saxton JC, Sinde S, Viana V. Children’s eating behaviour questionnaire: associations with BMI in Portuguese children. Br J Nutr. 2008;100(2):445–450. doi:10.1017/S0007114508894391
17. Carnell S, Wardle J. Measuring behavioural susceptibility to obesity: validation of the child eating behaviour questionnaire. Appetite. 2007;48(1):104–113. doi:10.1016/j.appet.2006.07.075
18. Miller AL, Miller SE, LeBourgeois MK, Sturza J, Rosenblum KL, Lumeng JC. Sleep duration and quality are associated with eating behavior in low-income toddlers. Appetite. 2019;135:100–107. doi:10.1016/j.appet.2019.01.006
19. Chaput JP, Després JP, Bouchard C, Tremblay A. The association between short sleep duration and weight gain is dependent on disinhibited eating behavior in adults. Sleep. 2011;34:1291–1297. doi:10.5665/sleep.1264
20. Liu A, Fan J, Ding C, et al. The association of sleep duration with breakfast patterns and snack behaviors among Chinese children aged 6 to 17 years: Chinese National Nutrition and Health Surveillance 2010–2012. Nutrients. 2022;14(11). doi:10.3390/nu14112247
21. Manasse SM, Haedt-Matt AA, Smith KE, et al. The moderating role of sleep duration on momentary relations between negative affect and loss-of-control eating in children and adolescents. Eur Eating Disorders Rev. 2022;30(6):815–822. doi:10.1002/erv.2908
22. Patel SR, Hu FB. Short sleep duration and weight gain: a systematic review. Obesity. 2008;16(3):643–653. doi:10.1038/oby.2007.118
23. de Onis M. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Org. 2007;85(09):660–667. doi:10.2471/BLT.07.043497
24. Santos JL, Ho-Urriola JA, González A, et al. Association between eating behavior scores and obesity in Chilean children. Nutr J. 2011;10(1):108. doi:10.1186/1475-2891-10-108
25. Wittmann M, Dinich J, Merrow M, Roenneberg T. Social jetlag: misalignment of biological and social time. Chronobiol Int. 2006;23(1–2):497–509. doi:10.1080/07420520500545979
26. Skjåkødegård HF, Danielsen YS, Frisk B, et al. Beyond sleep duration: sleep timing as a risk factor for childhood obesity. Pediatric Obes. 2021;16(1):e12698. doi:10.1111/ijpo.12698
27. Miller AL, Lumeng JC, Lebourgeois MK. Sleep patterns and obesity in childhood. Curr Opin Endocrinol Diabetes Obes. 2015;22(1):41–47. doi:10.1097/MED.0000000000000125
28. Spruyt K, Molfese DL, Gozal D. Sleep duration, sleep regularity, body weight, and metabolic homeostasis in school-aged children. Pediatrics. 2011;127(2):e345–e352. doi:10.1542/peds.2010-0497
29. Jenni OG, Carskadon MA. Sleep behavior and sleep regulation from infancy through adolescence: normative aspects. Sleep Med Clin. 2007;2(3):321–329. doi:10.1016/j.jsmc.2007.05.001
30. Moore M, Kirchner HL, Drotar D, Johnson N, Rosen C, Redline S. Correlates of adolescent sleep time and variability in sleep time: the role of individual and health related characteristics. Sleep Med. 2011;12(3):239–245. doi:10.1016/j.sleep.2010.07.020
31. Morrissey B, Taveras E, Allender S, Strugnell C. Sleep and obesity among children: a systematic review of multiple sleep dimensions. Pediatric Obes. 2020;15(4):e12619. doi:10.1111/ijpo.12619
32. Seo SH, Shim YS. Association of sleep duration with obesity and cardiometabolic risk factors in children and adolescents: a population-based study. Sci Rep. 2019;9(1):9463. doi:10.1038/s41598-019-45951-0
33. Deng X, He M, He D, Zhu Y, Zhang Z, Niu W. Sleep duration and obesity in children and adolescents: evidence from an updated and dose–response meta-analysis. Sleep Med. 2021;78:169–181. doi:10.1016/j.sleep.2020.12.027
34. Sunwoo JS, Yang KI, Kim JH, Koo DL, Kim D, Hong SB. Sleep duration rather than sleep timing is associated with obesity in adolescents. Sleep Med. 2020;68:184–189. doi:10.1016/j.sleep.2019.12.014
35. Chaput JP, Gray CE, Poitras VJ, et al. Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41(6 (Suppl. 3)):S266–S282. doi:10.1139/apnm-2015-0627
36. Miller MA, Kruisbrink M, Wallace J, Ji C, Cappuccio FP. Sleep duration and incidence of obesity in infants, children, and adolescents: a systematic review and meta-analysis of prospective studies. Sleep. 2018;41(4):1–19. doi:10.1093/sleep/zsy018
37. Chen H, Wang LJ, Xin F, Liang G, Chen Y. Associations between sleep duration, sleep quality, and weight status in Chinese children and adolescents. BMC Public Health. 2022;22(1):1136. doi:10.1186/s12889-022-13534-w
38. Parker MN, LeMay-Russell S, Schvey NA, et al. Associations of sleep with food cravings and loss-of-control eating in youth: an ecological momentary assessment study. Pediatric Obes. 2022;17(2):e12851. doi:10.1111/ijpo.12851
39. Hart CN, Spaeth AM, Egleston BL, et al. Effect of changes in children’s bedtime and sleep period on targeted eating behaviors and timing of caloric intake. Eating Behav. 2022;45:101629. doi:10.1016/j.eatbeh.2022.101629
40. Chamorro R, Jouffe C, Oster H, Uhlenhaut NH, Meyhöfer SM. When should I eat: a circadian view on food intake and metabolic regulation. Acta Physiol. 2023;237(3):e13936. doi:10.1111/apha.13936
41. Morrison S, Jackson R, Haszard JJ, et al. The effect of modest changes in sleep on dietary intake and eating behavior in children: secondary outcomes of a randomized crossover trial. Ame J Clin Nutr. 2023;117(2):317–325. doi:10.1016/j.ajcnut.2022.10.007
42. Kjeldsen JS, Hjorth MF, Andersen R, et al. Short sleep duration and large variability in sleep duration are independently associated with dietary risk factors for obesity in Danish school children. Int J Obes. 2014;38(1):32–39. doi:10.1038/ijo.2013.147
43. Wing YK, Li SX, Li AM, Zhang J, Kong APS. The effect of weekend and holiday sleep compensation on childhood overweight and obesity. Pediatrics. 2009;124(5):e994–e1000. doi:10.1542/peds.2008-3602
44. Jansen EC, Dunietz GL, Chervin RD, et al. Adiposity in adolescents: the interplay of sleep duration and sleep variability. J Pediatr. 2018;203:309–316. doi:10.1016/j.jpeds.2018.07.087
45. He F, Bixler EO, Berg A, et al. Habitual sleep variability, not sleep duration, is associated with caloric intake in adolescents. Sleep Med. 2015;16(7):856–861. doi:10.1016/j.sleep.2015.03.004
46. Choi Y, Kim S, Lee M, et al. Effect of catch-up sleep on obesity in Korean adolescents: a nationwide cross-sectional study. Front Pediatrics. 2023;11:1213558.
47. LeMay-Russell S, Tanofsky-Kraff M, Schvey NA, et al. Associations of weekday and weekend sleep with children’s reported eating in the absence of hunger. Nutrients. 2019;11(7). doi:10.3390/nu11071658
48. Huang WY, Wong SHS. Prospective associations between weekend catch-up sleep, physical activity, and childhood obesity. Childhood Obesity. 2019;15(1):40–47. doi:10.1089/chi.2018.0158
49. Meyhöfer S, Chamorro R, Hallschmid M, et al. Late, but not early, night sleep loss compromises neuroendocrine appetite regulation and the desire for food. Nutrients. 2023;15(9):2035. doi:10.3390/nu15092035
50. Zhu B, Shi C, Park CG, Zhao X, Reutrakul S. Effects of sleep restriction on metabolism-related parameters in healthy adults: a comprehensive review and meta-analysis of randomized controlled trials. Sleep Med Rev. 2019;45:18–30. doi:10.1016/j.smrv.2019.02.002
51. St-Onge MP. Sleep–obesity relation: underlying mechanisms and consequences for treatment. Obesity Rev. 2017;18:34–39. doi:10.1111/obr.12499
52. Blissett J, Farrow C, Haycraft E. Relationships between observations and parental reports of 3–5 year old children’s emotional eating using the children’s eating behaviour questionnaire. Appetite. 2019;141:104323. doi:10.1016/j.appet.2019.104323
53. Acebo C, Sadeh A, Seifer R, et al. Estimating sleep patterns with activity monitoring in children and adolescents: how many nights are necessary for reliable measures? Sleep. 1999;22(1):95–103. doi:10.1093/sleep/22.1.95
54. Gruber R, Somerville G, Wells S, Keskinel D, Santisteban JA. An actigraphic study of the sleep patterns of younger and older school-age children. Sleep Med. 2018;47:117–125. doi:10.1016/j.sleep.2018.03.023
55. Peuckert MZ, Ayala CO, Mattiello R, et al. Validation evidence for the children’s eating behaviour questionnaire (CEBQ) in Brazil: a cross-sectional study. Nutrients. 2025;17(5). doi:10.3390/nu17050851
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy of GLP-1 Analogues on Appetite Parameters, Gastric Emptying, Food Preference and Taste Among Adults with Obesity: Systematic Review of Randomized Controlled Trials
Aldawsari M, Almadani FA, Almuhammadi N, Algabsani S, Alamro Y, Aldhwayan M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:575-595
Published Date: 2 March 2023
The Association Between Short Sleep Duration and Metabolic Syndrome: A Case-Control Study
Elshoeibi AM, Akomolafe A, Al-Khulaifi A, Metwally O, Al-Khayarin R, Al Abiad AR, Al-Naemi L, Chivese T, Farooqui H
Diabetes, Metabolic Syndrome and Obesity 2023, 16:4157-4167
Published Date: 20 December 2023
Gender and Age Differences in the Relationship Between Smartphone Addiction and Sleep Duration in Korean Children: A Panel Quantile Regression Study
Jeong K, Cho S, Song D, Li R, Han S, Cho HJ, Kim J
Psychology Research and Behavior Management 2024, 17:4183-4192
Published Date: 8 December 2024
Title: A Qualitative Systematic Review of Parental Perceptions, Motivators, and Barriers to Management of Childhood Obesity
Musa S, Al-Dahshan A, Kehyayan V
Diabetes, Metabolic Syndrome and Obesity 2024, 17:4749-4765
Published Date: 11 December 2024
Serum Vitamin D Profiles of Children with Asthma in Southwest Saudi: A Comparative Cross-Sectional Study
Asseri AA
International Journal of General Medicine 2024, 17:6323-6333
Published Date: 17 December 2024