Back to Journals » Patient Preference and Adherence » Volume 20
Situational Factors Associated with Dietary Behavior in Stroke Patients During Rehabilitation: A Qualitative Study Based on the COM-B Model
Authors Zhong W, Pan X, Li J, Zhang Y, Chen L, Sun X, Wang Z, Xu L
Received 5 January 2026
Accepted for publication 5 March 2026
Published 9 March 2026 Volume 2026:20 593792
DOI https://doi.org/10.2147/PPA.S593792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Weiying Zhong,1 Xi Pan,2 Jiaxuan Li,1 Yi Zhang,1 Lei Chen,1 Xueqi Sun,1 Zhi Wang,2 Lan Xu1
1Department of Nursing, the First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China; 2Department of Neurology, the First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China
Correspondence: Lan Xu; Xi Pan, Email [email protected]; [email protected]
Objective: This study investigated situational factors associated with dietary behavior in stroke patients during rehabilitation using the Capability, Opportunity, Motivation - Behavior (COM-B) model, which explains behavior via three components: capability, opportunity, and motivation.
Methods: This study employed a qualitative and descriptive design. Using purposive sampling, 17 stroke patients during rehabilitation were recruited from a tertiary hospital in Jiangsu Province, China, between July and September 2024. Semi-structured interviews were conducted, and data were analyzed using directed content analysis.
Results: The following themes and (sub)themes were identified. Capability: (1) a lack of knowledge relating to dietary management; (2) difficulty managing negative emotions; (3) reduced self-regulatory ability; (4) distress caused by symptoms of functional impairment. Opportunity: (1) support from the physical environment; (2) using and adjusting assistive feeding devices; (3) influence of the social environment; (4) accessibility and quality of external help services. Motivation: (1) clarification of eating intentions; (2) lack of focus during eating; (3) differences in food assessment.
Conclusion: The situational factors associated with dietary behavior in stroke patients during rehabilitation are influenced by a complex interplay of factors within the personal, social, and environmental domains. The application of the COM-B model in this research is a significant contribution. It not only helps to clearly categorize and understand the various situational factors but also provides a structured framework for developing targeted interventions. Interventions that promote healthy dietary behaviors for stroke patients during rehabilitation should incorporate strategies to enhance capability, optimize opportunity, and strengthen motivation.
Keywords: rehabilitation, stroke, COM-B model, dietary behavior, situational factors, qualitative research
Introduction
Stroke is defined as the acute onset of neurological dysfunction arising from ischemia or hemorrhage and persisting for more than 24 hours or until the patient’s death.1 Stroke is characterized by high incidence, disability, mortality and recurrence rates, along with substantial economic burden. The recurrence of stroke is the leading cause of long-term disability and elevated mortality among patients.2
Following the acute phase, stroke patients enter a period of rehabilitation period, which is considered a critical window for functional recovery. During this stage, rapid neurophysiological improvement occurs, and up to 90% of patients may achieve their maximum level of restoration.3 Nevertheless, during rehabilitation, stroke patients remain at increased risk of recurrence, partly due to the short stabilization time of atherosclerotic plaques, the presence of unstable plaques, and insufficient control of stroke-related risk factors within a short period of intervention. The secondary prevention guidelines for stroke4 indicate that identifying and modifying unhealthy dietary behaviors can help prevent recurrence. In a previous study, Shani et al5 reported that unfavorable dietary behaviors in patients with stroke were associated with a 44.3% increased risk of recurrence. In another study, Spence et al6 reported that the maintenance of healthy dietary behaviors was associated with almost a 50% reduction in the risk of stroke recurrence. Adherence to healthy dietary behaviors is therefore considered to modulate stroke-related pathophysiological processes, with the potential to improve clinical outcomes and reduce the likelihood of recurrence.
Dietary behavior is a complex health-related behavior that occurs on a daily basis7 and is influenced by multiple factors in addition to their interactions.8 This behavior encompasses not only dietary patterns but also situational factors, which are defined as temporal and spatial situation-specific variables, such as meal location and companions.9 From a situational perspective, dietary behavior is shaped by the interaction between individual capabilities and surrounding environmental contexts, making situational analysis essential for capturing behavior in real-life settings. Collecting data relating to the situational factors underlying dietary behavior, including social, physical, and temporal contexts, as well as emotions and intentions, in real-time natural settings is considered to yield a more accurate representation of an individual’s actual dietary behavior. Consequently, researchers are recommended to investigate the complex psychological, physiological, and behavioral processes that occur during dietary behavior by assessing situational factors on multiple occasions each day in real-world settings. Most previous research related to the situational factors associated with dietary behavior has focused on overweight individuals, the elderly, and pregnant women.10–12 The findings of these previous studies show that the dining location, dining companions, and dining environment can all exert significant influence on dietary behavior.10 Past qualitative studies on dietary behavior in stroke patients have primarily focused on exploring how stroke - related impairments may hinder dietary behavior.13 Following the onset of stroke, activity restrictions and negative emotions arising from this disease may also affect the dietary behavior of affected patients.14 Stroke-related neurological damage leads to motor dysfunction, cognitive impairment, dysphagia, and emotional disturbances, which may directly interfere with patients’ ability to prepare, consume, and regulate food intake.15–17 Motor impairments reduce physical capacity for independent eating, while cognitive deficits affect attention, executive function, and adherence to dietary recommendations. Swallowing difficulties further constrain food texture selection and meal composition, and emotional changes may alter appetite and food preferences. Together, these stroke-related outcomes reshape dietary behaviors during the rehabilitation period. Therefore, dietary behavior during stroke rehabilitation can be conceptualized as the outcome of interactions between disease-related impairments and situational factors.
Identifying pertinent situational factors during the occurrence of dietary behaviors in stroke patients during rehabilitation is of paramount importance for the formulation of evidence-based intervention strategies. However, research in this area remains scarce. Given this gap in the current literature, qualitative research is particularly well-suited, as this form of research allows for an in-depth investigation of patients’ living experiences, captures the complexity of psychosocial and contextual influences, and identifies nuanced factors that may not be readily measurable through quantitative approaches.
The utilization of a theoretical framework can strengthen qualitative research by providing a systematic approach to the investigation and interpretation of behavior. This strategy is widely regarded as a rigorous and effective strategy for understanding behaviors. Among such theoretical frameworks, the Capability, Opportunity, Motivation–Behavior (COM-B) model is highly recommended.18 Compared with models that focus on single-level determinants, the COM-B framework explicitly integrates psychological, social, and environmental dimensions and links behavioral determinants to intervention design, making it particularly suitable for examining situational influences on dietary behavior during rehabilitation.19 In addition, the COM-B model provides groundwork for the development of evidence-based behavioral interventions and has been applied to a wide range of clinical issues.20,21 However, the COM-B model has not yet been utilized in the analysis of dietary behaviors for stroke patients during rehabilitation. Although previous qualitative studies have explored barriers to healthy eating among stroke patients, most have primarily focused on functional impairments and individual-level determinants, without systematically examining situational factors within real-life rehabilitation contexts. To the best of our knowledge, limited qualitative research has applied the COM-B framework to comprehensively analyze how capability, opportunity, and motivation dynamically interact to shape dietary behaviors among stroke patients during rehabilitation. Furthermore, few studies have integrated theoretical guidance with in-depth contextual analysis to identify actionable intervention targets. Therefore, this study addresses this gap by applying the COM-B model to systematically explore situational determinants of dietary behavior and to generate theory-informed implications for clinical practice. Therefore, in the present study, we conducted semi-structured interviews with stroke patients during rehabilitation to explore situational factors influencing dietary behaviors within COM-B framework. The findings aim to inform targeted interventions and support clinical nursing practice and early prevention strategies.
Methods
This study employed a qualitative research methodology. By conducting in-depth and semi-structured interviews, we investigated the situational factors associated with dietary behavior in stroke patients during the period of rehabilitation.
Recruitment and Sampling
This study was conducted in Suzhou, a city situated in eastern China. The participants were stroke patients during the rehabilitation period who received medical treatment at the First Affiliated Hospital of Soochow University. Purposeful sampling was employed based on participant information provided by the head nurses, including patients with diverse educational backgrounds and from various residential locations; our aim was to achieve maximum heterogeneity within our research cohort. The inclusion criteria were as follows: (1) confirmed diagnosis of stroke, with clinical manifestations consistent with the Chinese diagnostic criteria for stroke;22 (2) stroke patients during the rehabilitation phase, diagnosed 2 weeks to 6 months after the onset of stroke;23 (3) age ≥ 18 years; (4) ability to articulate personal experiences. The exclusion criteria were as follows: (1) a history of psychiatric or psychological disorders; and (2) patient was unwilling to communicate their inner thoughts with the researchers. The sample size was determined based on the achievement of theme saturation, saturation was considered to have been reached when, following the final set of interviews, no new themes, sub - themes, or substantial variations in the pre - existing themes emerged. This suggested that further data collection would probably not generate additional meaningful insights, and thus the sample size was deemed adequate; ultimately, we included 17 eligible stroke patients during rehabilitation.
Data Collection
Between July 2024 and September 2024, we conducted in-depth, semi-structured interviews to investigate the personal perspectives of each participant. All participants were fully informed about the study objectives, the principle of voluntary participation, and confidentiality protocols during the pre-interview briefing session. After obtaining informed consent, interviews were audio-recorded, and contemporaneous field notes were taken to supplement the verbal data. All in-depth interviews were conducted in Mandarin by ZWY, a female researcher with a Master’ s degree in Nursing who currently serves as a senior registered nurse and has prior experience in quantitative research methodologies. Her prior role as the primary nurse for these patients enabled her to build strong rapport and trust, which contributed to the depth and authenticity of the interview data. LJX provided support for audio recording and data documentation procedures, a female researcher with a Master’ s degree in Nursing, who possessed prior experience in quantitative research methodologies. The interview guideline was developed based on the COM-B model and aimed to investigate situational factors associated with dietary behavior from the perspectives of stroke patients during rehabilitation, group discussions, and a preliminary pilot study with two patients. The final interview guideline in the Supplementary Material included the following questions: (a) How do you perceive the impact of stroke on your dietary behaviors? (b) Have you experienced any discomfort and/or challenges while engaging in dietary behaviors? (c) What coping strategies did you employ when encountering discomfort or challenges during dietary behaviors, and what were the outcomes of these strategies? (d) Which factors do you associate with your dietary behaviors? Specifically, what family-social or physical environmental factors have influenced your dietary patterns? (e) Did you receive companionship or support from family/friends while having meals? How was this support provided? (f) Could you describe your internal thoughts when engaging in abnormal dietary behaviors? For instance, under what circumstances did your dietary choices deviate from your habits? What motivated these choices? How did external influences affect your decision-making process, and what were your internal reflections at the time?
Interviews were conducted in a quiet, comfortable physician’s office. The researcher initiated each session with open-ended questions, progressively narrowing the focus based on the respondents’ answers, with each interview lasting approximately 40 minutes. All sessions were audio-recorded, after which participants had the opportunity to review their transcripts and clarify ambiguous responses during subsequent interactions. No repeat interviews were conducted. Verbatim transcriptions were performed by the interviewer within 24 hours post-interview, followed by anonymization procedures.
Data Analysis
Data collection and data analysis were carried out simultaneously. All records were imported into NVivo 12 for data management and analysis. The researchers repeatedly listened to the audio recordings, read the transcripts, and reviewed the field notes to gain a comprehensive understanding of the data. Open coding was independently performed by the researchers (ZWY, LJX) on sections relevant to the research objectives, and the text analysis. The research group discussed any discrepancies to reach a consensus. When disagreements arose, the two coders revisited the original transcripts and field notes to re-examine the context of the coded segments. If consensus could not be achieved through discussion, a third senior researcher was consulted to facilitate resolution and ensure analytical rigor. Direct content analysis was adopted for data analysis.24 First, the transcripts that reflected the situational factors related to the dietary behaviors of stroke patients during rehabilitation were used as the minimum analysis units. Second, initial data were reviewed and read repeatedly. Third, the COM-B model was used as a framework to categorize the unit of analysis. Fourth, significant ideas and concepts within the data were coded and marked, and similar codes were classified into corresponding categories to form themes and (sub)themes. Finally, the results were interpreted and analyzed, and the links between data and the results were formed.
Ethical Considerations
This study was approved by the Ethics Committee of First Affiliated Hospital of Soochow University (No. 2024012). All participants provided written informed consent before enrollment.
Rigour and Reflexivity
Before and after each interview, ZWY engaged in careful self-reflection regarding her performance and contributions throughout the interview process. Given that ZWY had previously served as the primary nurse for some participants, the potential influence of this prior nurse–patient relationship on participants’ responses was carefully considered. While pre-existing familiarity may have facilitated trust and openness, it also posed a risk of social desirability bias and responses shaped by perceived expectations.
To address this, prior to data collection, ZWY engaged in reflexive preparation, including bracketing preconceptions derived from her clinical experience with stroke patients. Through self-reflection and research team discussions, she identified and consciously set aside personal assumptions regarding patients’ dietary behaviors to minimize potential bias in both data generation and interpretation. Throughout the study, ongoing reflexive awareness was maintained to ensure that participants’ perspectives were represented as authentically as possible.
Participants were explicitly informed before each interview that ZWY was acting solely in a research capacity and that their responses would not affect their clinical care. The principles of voluntary participation, confidentiality, and the right to withdraw at any time were emphasized. Neutral and open-ended questioning techniques were employed to encourage authentic expression. Throughout data collection and analysis, ZWY maintained continuous awareness of potential role duality and its influence on the research process.
To enhance confirmability, all participant quotations were translated from Chinese into English by one of the authors and subsequently reviewed by a native English speaker to ensure linguistic accuracy and conceptual clarity. Furthermore, transferability was strengthened by providing a comprehensive description of participants’ demographic and contextual characteristics. These practices enhanced methodological rigor and transparency in the qualitative process.
Results
A total of 17 stroke patients during rehabilitation completed the interviews. General demographic information relating to the participants is detailed in Table 1. As shown in Table 2 and Figure 1, the results of the study were analyzed using the COM-B model in terms of capability, opportunity, and motivation, and the situational factors associated with dietary behavior in stroke patients during rehabilitation were identified. The following sections describe specific findings and examples of participant responses.
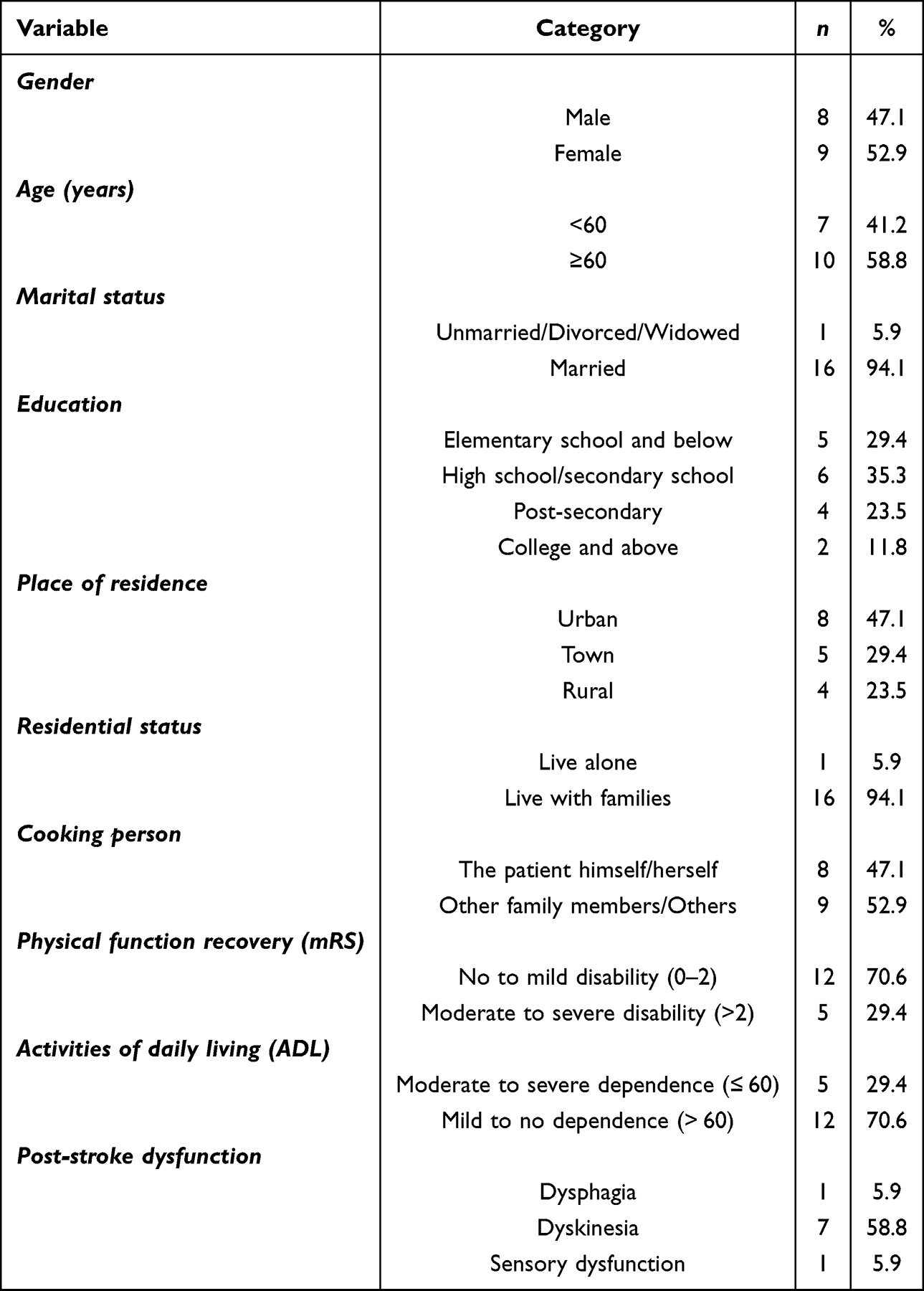 |
Table 1 Demographic Characteristics of the Participants (n=17) |
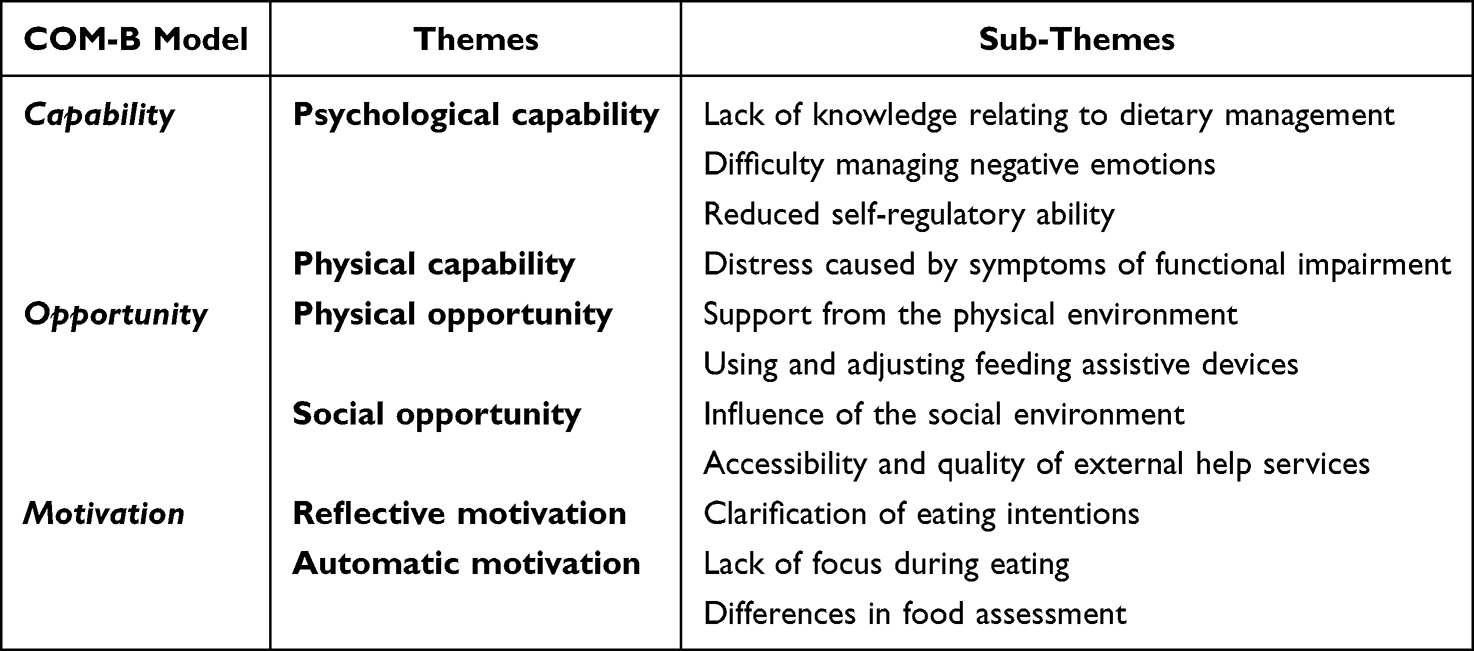 |
Table 2 Themes and Sub-Themes |
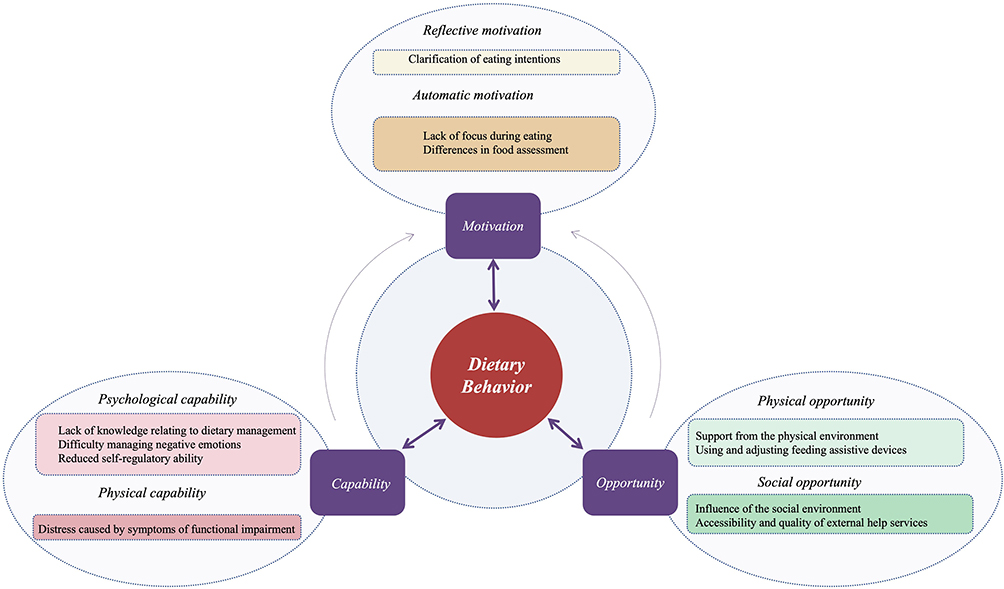 |
Figure 1 Thematic mapping of situational factors associated with dietary behavior in stroke patients during rehabilitation to the Capability, Opportunity, Motivation–Behavior Model. |
Capability
Capability in the COM-B model can be interpreted as the capability of stroke patients during rehabilitation to complete dietary behavior. In this context, capability was categorized into psychological capability and physical capability. A total of four (sub)themes emerged under this theme.
Psychological Capability
Lack of Knowledge Relating to Dietary Management
Due to a lack of knowledge and the presence of misconceptions relating to dietary management, stroke patients during rehabilitation frequently made errors in food preparation and cooking techniques. Additionally, some patients opted to reduce the variety or portion sizes of their meals after the occurrence of a disease.
These knowledge deficits sometimes coexisted with misunderstandings about appropriate dietary practices.
(After getting sick) We don’t know what we can eat. Also, we’ve been told to have a diet low in oil and salt, but we don’t know how to cook accordingly. So, we dare not eat anything. (P8, female, 50 years of age)
After a stroke, patients are commonly advised to avoid meat and consume mainly vegetables. (P5, male, 61 years of age)
With the widespread dissemination of the Internet, a multitude of non-professional information has surfaced on various online information platforms. Considering the inability of patients to discern such information, these factors ultimately misled them into adopting unhealthy dietary habits.
Given patients’ limited ability to discern reliable from unreliable information, such exposure may further reinforce these misconceptions and lead to unhealthy dietary habits.
When I am scrolling through my phone, I frequently encounter videos shared by public accounts that discuss dietary recommendations for illnesses, particularly stroke. I am uncertain whether the information provided by these individuals is accurate or reliable. (P13, female, 66 years of age)
Difficulty Managing Negative Emotions
Negative affective experiences unrelated to the sequelae of stroke were found to deplete the regulatory capacity of stroke patients during rehabilitation, thereby adversely affecting the process of dietary behavior.
Thinking about this illness makes me feel depressed, so I do not eat much. (P17, female, 60 years of age)
Stress experienced during disease coping and guilt towards family members exerted a notable influence on the dietary behaviors of our patients.
I am almost 70 years old, yet still need to be fed like a child. I am regressing instead of aging gracefully; it is really embarrassing. (P16, female, 69 years of age)
With this physical disability, I refuse to dine out with them; it is just too much trouble. (P10, female, 48 years of age)
Reduced Self-Regulatory Ability
The patients exhibited a deficiency in self-control capacity at the individual level, being unable to exercise self-control over healthy dietary behaviors effectively. Furthermore, the patients were incapable of implementing long-term and effective management of their own dietary habits.
I know I should eat them, but I just do not feel like having green leafy vegetables. (P9, male, 62 years of age)
I could stick to a healthy diet right after being discharged from the hospital, but I could not keep it up after a few days. (P11, male, 64 years of age)
Physical Capability
Distress Caused by Symptoms of Functional Impairment
Persistent physiological dysregulation and inadequate adaptive mechanisms were identified as primary contributors to restricted dietary behaviors in patients undergoing post-stroke rehabilitation.
After the stroke, (right) hand mobility has been significantly impaired, making eating extremely inconvenient. (P1, female, 64 years of age)
Apart from dyskinesia, dysphagia, and ageusia/dysgeusia also contributed to altered dietary behaviors in stroke survivors. These sensory impairments impaired perception of food temperature, texture, and taste, consequently reducing the quality of the eating experience.
I have a poor appetite right now. My mouth feels bland, and food tastes flavorless. (P2, male, 49 years of age)
I cannot eat quickly anymore. Now I really have to chew slowly and swallow carefully, or I will choke. (P10, female, 48 years of age)
Opportunity
According to the COM-B model, opportunities can be understood as all the external factors that can influence the dietary behaviors of stroke patients during rehabilitation. This encompasses the physical environment, such as time, available resources, geographical location, initiating triggers, and necessary materials, along with the social environment, including individual characteristics, perceptions, interpersonal interaction patterns, and cultural practices. A total of four (sub) themes emerged under this theme.
Physical Opportunity
Support from the Physical Environment
Stroke patients during rehabilitation frequently demonstrated diverse dietary behaviors across different physical environments, adjusting these behaviors based on their personal conditions and the limitations imposed by the surrounding environment. In various contexts and circumstances, patients may alter their dietary patterns, food choices, and meal schedules.
On Sundays, we also go out to eat to have a change of taste. (P5, male, 61 years of age)
I used to eat late when I was at the factory. At home, we have meals early. Sometimes I must eat even when my stomach is not hungry. (P11, male, 64 years of age)
The dining patterns of patients were influenced by multiple aspects of the physical environment, encompassing spatial accessibility, food procurement channels, as well as socio-cultural factors. These aforementioned factors are all likely to lead patients to make different dining choices in diverse physical environments.
Now I cannot go to places that far away. I can only go to relatively nearby supermarkets to buy groceries, but supermarkets do not have as wide a variety of vegetables as farmers’ markets. (P13, female, 66 years of age)
Using and Adjusting Feeding Assistive Devices
After being discharged from the hospital, and as the disease progressed, stroke patients during rehabilitation developed a need for self-care and showed reluctance to continue being cared for. Consequently, they began using specific assistive devices during meals to facilitate eating. These devices ensured that patients consumed food more safely and conveniently, reduced their dependence on others for assistance, and helped them to maintain self-esteem and independence.
My daughter bought me children’s chopsticks with finger rings. Otherwise, I could not hold them properly with my fingers. (P6, male, 65 years of age)
For convenience, after being discharged from the hospital, I always use a spoon to eat by myself. Otherwise, I would need to be fed. (P15, female, 37 years of age)
Social Opportunity
Influence of the Social Environment
During rehabilitation, stroke patients often underwent corresponding changes in their dietary habits and food choices in different social environments. The social environment exerted a profound influence on the dietary behaviors of individuals.
At noon, there are just the two of us at home (her and her husband). We’ll keep it simple and cook more dishes when our son comes home in the evening. (P8, female, 50 years of age)
We don’t think of eating (fruits). We don’t like them. Only our daughter does (like them). We’ll eat some only if she wants to. (P4, female, 67 years of age)
The dietary choices of patients were influenced by a multitude of factors, including cultural traditions, social norms, and interpersonal relationships, thus resulting in a diverse range of dietary behaviors. These choices not only reflected the personal preferences of the patients but also demonstrated their adaptation to and respect for the social environment they inhabited.
My husband is a Buddhist, so we all go vegetarian along with him. (P3, female, 50 years of age)
When family members or friends get together outside at a restaurant, of course, we’ll eat more because we’re happy. (P12, male, 51 years of age)
Accessibility and Quality of External Help Services
After discharge from the hospital, patients did not transition promptly back to their usual roles, leading to a consistently high demand for social support and the requirement of assistance from others to finish meals.
They helped me put the dishes into a bowl, which made it much easier for me to eat. (P16, female, 69 years of age)
During rehabilitation, stroke patients were unable to fulfill the tasks corresponding to their previous family roles, and other family members performed the original family responsibilities (such as grocery shopping and cooking).
In the past, I was the one who did all the grocery shopping and cooking at home, but now I can’t do it anymore. He (her husband) does it all by himself now. (P3, female, 50 years old)
I can’t go grocery shopping alone conveniently now. Every Sunday, our son takes us to buy groceries for the whole week. Of course, it’s not very convenient. (P14, male, 63 years of age)
Motivation
According to the COM-B model, motivation can be understood as the active process that prompts and guides patients to carry out dietary behaviors. This process can be categorized into reflective motivation and automatic motivation. In this study, these beliefs manifested as different influencing factors in most participants. A total of three (sub)themes emerged under this theme.
Reflective Motivation
Clarification of Eating Intentions
During rehabilitation, stroke patients exhibited a variety of eating intentions that exerted a direct impact on their dietary behaviors. Owing to disparities in eating intentions, patients exhibited marked differences in their dietary behaviors regarding food selection, meal frequency, and food consumption volume.
Why do I eat? I eat because I am hungry. (P5, male, 61 years of age)
I have to eat when I am hungry. (P11, male, 64 years of age)
Sometimes I do not eat just because I am hungry. I have a weak stomach, and it will make me uncomfortable if I get too hungry. (P3, female, 50 years of age)
When patients experienced boredom or sought psychological solace, eating functioned as a modality of emotional regulation rather than simply a means of energy replenishment.
Sometimes when I am extremely bored, my mouth just cannot stay still, and having a bit of snacks will make it better. (P10, female, 48 years of age)
Automatic Motivation
Lack of Focus During Eating
During meals, stroke patients undergoing rehabilitation often exhibited relatively low levels of attentiveness. Their minds were readily distracted by mobile phone notifications, childcare responsibilities, or other daily trivialities. Consequently, they were unable to maintain full concentration throughout the eating process, which in turn affected food appreciation and digestion. This scenario was particularly prevalent in the context of modern fast-paced living.
However, it is also possible that, in some cases, such distraction reflected an adaptive coping strategy, whereby patients diverted their attention to reduce discomfort or anxiety related to eating challenges during rehabilitation.
Nowadays, everyone has a mobile phone. People tend to check their phones while eating, so they eat much more slowly. (P7, male, 55 years old)
I also have to take care of my child. I cannot eat peacefully while having meals. I need someone to hold the baby for a while so that I can have a proper bite. (P13, female, 66 years of age)
Differences in Food Assessment
During dietary behavior, individual differences in the perception of food taste, overall satisfaction, and the evaluation of its deliciousness may, to a certain extent, have influenced the dietary habits and food choices of patients, potentially leading to variations in their eating behaviors. Since dietary habits are directly related to the quality of dietary intake, different evaluations and preferences for food may have affected the dietary behaviors of our patients.
The dishes he cooks are too salty. The doctor said I have high blood pressure and should avoid salt. I do not like (the food). (P8, female, 50 years of age)
I like eating meat with the skin on. It is hard for me to get used to not being allowed to eat fatty pork suddenly. There are no delicious dishes. (P2, male, 49 years of age)
If there are dishes, I like today, I will eat a bit more. If not, I will eat a bit less. (P3, female, 50 years of age)
Discussion
In this study, we investigated the cognition and attitude of stroke patients during rehabilitation towards dietary management by performing structured interviews. Our analysis revealed that these patients had a relatively strong willingness and good enthusiasm for dietary management. However, most patients lacked specific knowledge related to dietary management. In addition, our patients encountered numerous obstacles in terms of the acquisition of knowledge, including the inability to distinguish relevant information, difficulties in screening practical information due to its massive and diverse nature, and the lack of official information channels.
During rehabilitation, most stroke patients recognized the importance of dietary management for disease recovery, were willing to take the initiative to learn knowledge related to dietary management, and desired to acquire professional information to manage their diets better and promote disease rehabilitation. This finding is consistent with the findings of Mujamammi et al.25 However, with the popularization of the Internet, various information platforms have emerged; however, none of the existing official channels currently support relevant information platforms. Consequently, our patients often struggled to find authoritative and reliable dietary management information; this finding is consistent with the research conclusions of Benameur et al.26 During the acquisition of relevant information, and due to information asymmetry and the inherent lack of ability of patients to discriminate information, the factors above may lead patients to acquire inaccurate or even erroneous dietary management information. Consequently, patients might adopt inappropriate dietary management measures, which could adversely affect disease recovery. Therefore, medical staff need to strengthen dietary management education for stroke patients during the rehabilitation stage, help patients to improve their ability to identify information, guide patients to access correct information channels, and supervise the implementation of relevant information in the daily dietary practices of patients.
Our results indicate that the dietary behaviors of stroke patients during rehabilitation were influenced by a variety of situational factors; this finding was consistent with the findings of multiple international studies.10,27,28 In the present study, we investigated the situational factors associated with the dietary behaviors of stroke patients during the rehabilitation stage, encompassing three dimensions: capability, motivation, and opportunity. Specific situational factors included physical dysfunction, interference from daily chores, satisfaction with food, the actual intention related to eating, and the individuals who accompanied them during meals. These situational factors interacted collectively and exerted distinct impacts on the dietary behaviors of stroke patients during rehabilitation.
Importantly, these COM-B components operated through dynamic and reciprocal mechanisms rather than in isolation.18 For example, physical dysfunction (Capability) reduced patients’ ability to independently prepare or consume meals, thereby increasing reliance on caregivers and assistive devices (Opportunity). This dependence often altered patients’ perceived autonomy and self-efficacy, which subsequently shaped their emotional responses and motivation toward dietary adherence (Motivation). In some cases, diminished autonomy led to frustration or reduced intrinsic motivation, further weakening active engagement in dietary management. Similarly, limited access to reliable dietary information (Opportunity) constrained patients’ psychological capability by reducing their understanding of appropriate dietary practices. Insufficient knowledge undermined confidence in making dietary decisions, thereby lowering reflective motivation and intentional behavioral regulation. These interlinked processes demonstrate how changes in one COM-B component can trigger cascading effects across the system, jointly shaping dietary behaviors during stroke rehabilitation.
At the capability level, issues included a lack of knowledge relating to dietary management, distress due to symptoms of functional impairment, difficulty in controlling negative emotions, and impaired self-regulatory capacity. Limb dysfunction is one of the primary challenges faced by stroke patients during rehabilitation. When engaging in dietary activities, the functional impairments caused by stroke may prevent patients from using utensils freely or even from bringing food to their mouths. Consequently, they were unable to eat independently and often required assistance from caregivers to complete their meals. The occurrence of such situations not only restricted a patient’s autonomy but also triggered a range of psychological and emotional issues, such as feelings of frustration and helplessness. These findings are consistent with the research conducted by Bailey et al14 among stroke patients during rehabilitation. During rehabilitation, stroke patients often aspire to eat independently to reduce their reliance on caregivers and alleviate negative emotions associated with the disease.29 During the process of assisting patients with eating, healthcare professionals and caregivers should remain patient, understand the difficulties and challenges faced by patients, and provide them with sufficient support and encouragement. Offering appropriate eating aids and urging patients to complete rehabilitation training to regain independent eating ability at an early stage, are crucial for helping patients to overcome functional impairments and promote independent eating.
At the opportunity level, factors included guidance by the physical environment, social environment shaping, the accessibility and quality of external assistance services, and the acquisition and adaptation of feeding assistive devices. In addition, we found that dining location exerted a notable influence on dietary behaviors in stroke patients during rehabilitation, a finding consistent with the research by Shams-White et al10 conducted among elderly populations. Organizing regular outings for communal dining or hosting family gatherings can diversify dining settings, and such carefully designed experiences may promote healthier eating behaviors in patients. The presence of companions during meals also exerted a profound impact on dietary behaviors in stroke patients during rehabilitation, an observation that aligned with the study by Roordink et al30 in overweight populations. Beyond providing emotional support to help patients cope with eating challenges, companions can offer essential assistance and guidance to ensure safe and comfortable food intake.31 Healthcare professionals and caregivers should promptly evaluate difficulties encountered by patients during meals and provide adequate social support. Since stroke patients undergoing rehabilitation may experience frustration and helplessness due to disease-related functional impairments and negative emotions, offering emotional support is crucial for maintaining a positive mindset and facilitating the rehabilitation process.
At the motivation level, factors included deficient attentional focus while eating, discrepancies in food evaluation, and the differentiation of eating intentions. Of these, interruptions from daily life distractions stood out as a significant situational factor influencing the dietary behaviors of patients. During meals, distractions such as mobile phone notifications, childcare responsibilities, or other daily trivialities, may divert the attention of patients, thereby compromising their focus on eating. This observation aligns with the research conducted by Allan et al32 among 64 adults. Therefore, creating a quiet and comfortable eating environment with minimal external distractions is crucial for enhancing eating efficiency and dietary quality.33 Furthermore, the satisfaction of patients with food and their ability to discern genuine eating intentions also had a notable impact on their dietary behaviors; this finding was consistent with the results published by Wahl et al.34 If patients are dissatisfied with the taste of food, they may lack the motivation to eat. Offering a diverse range of food options that meet nutritional requirements while respecting the taste preferences of patients can boost their interest in eating, thereby improving their nutritional status and promoting healthy dietary behaviors.
From a theoretical perspective, our findings validate the applicability of the COM-B model in understanding dietary behaviors among stroke patients during rehabilitation. Beyond validation, this study extends the model by illustrating how post-stroke functional impairments and rehabilitation-specific situational constraints shape the dynamic interactions among Capability, Opportunity, and Motivation. In particular, the identification of cognitive fatigue, reliance on caregivers, and digital information overload further refines the situational understanding of COM-B constructs within stroke rehabilitation settings.
Under the influence of varying situational factors, dietary behaviors among stroke patients during rehabilitation exhibited notable differences. Healthcare professionals must adopt a holistic approach by considering these situational determinants when actively participating in the development and implementation of dietary management strategies for this patient population. To translate these findings into practice, concrete intervention prototypes should be developed. For example, to address the lack of dietary knowledge identified under Capability, visual low-salt and balanced-diet recipe guides tailored to patients with post-stroke cognitive fatigue could be designed. To mitigate distraction during meals under Motivation, structured mindful eating sessions or distraction-reduction protocols within rehabilitation wards could be piloted. Such targeted interventions, grounded in the COM-B framework, may enhance the feasibility and effectiveness of dietary management programs for stroke patients. This will involve establishing effective communication and fostering collaborative partnerships with the caregivers of stroke patients during rehabilitation, leveraging caregiver resources to strengthen the social support networks of patients, gaining deeper insights into the specific needs of patients, and providing personalized support and guidance.
Nevertheless, several limitations should be considered when interpreting these findings. As participants were recruited from a single rehabilitation center, certain situational themes, such as access to external assistance services and the structure of social support, may reflect local service availability and cultural characteristics. Therefore, caution is warranted when generalizing these findings to other rehabilitation settings or healthcare systems. Future multi-center studies are needed to enhance transferability and allow for deeper contextual comparisons.
Limitations
This study has several limitations that need to be considered. First, patient recruitment was conducted exclusively at a single hospital. Given that many participants were middle-aged to elderly individuals sharing similar lifestyle patterns, habits, and cultural backgrounds, the substantive content of their narratives exhibited marked homogeneity. Second, the limited sample size may have introduced potential bias into our findings. Therefore, future research should employ larger sample sizes to improve the generalizability of our findings. In addition, we recommend integrating quantitative methodologies into subsequent studies to investigate further situational factors influencing dietary behaviors in stroke patients during rehabilitation.
Conclusion
Grounded in the COM-B model theory, the findings of this study provide novel insights into the situational factors influencing dietary behaviors in stroke patients during rehabilitation. Our findings demonstrate that patients encountered diet-related situational challenges across the three COM-B domains of capability, opportunity, and motivation. Importantly, these factors did not operate in isolation; rather, they exhibited dynamic interrelationships.
Future interventions must therefore adopt a holistic approach by explicitly designing strategies that simultaneously address deficits across these domains, for example by combining practical feeding support and assistive resources under opportunity, dietary education under capability, and motivational counseling to reduce distress and strengthen intentional engagement under motivation.
Such multi-level strategies require collaboration among nurses, physicians, patients, and caregivers, as the influencing factors identified in this study span clinical guidance, daily practical support, and personal behavioral regulation.
Abbreviations
COM-B, Capability, Opportunity, Motivation Behavior.
Data Sharing Statement
The datasets of the current study are available from the corresponding author (XL, E-mail: [email protected]) on reasonable request.
Ethics
The study was conducted in accordance with the principles of the Declaration of Helsinki, and the study was approved by the Ethics Committee of First Affiliated Hospital of Soochow University (No. 2024012).
Informed Consent and Patient Details
All participants provided written informed consent before enrollment. The consent form explicitly included permission for the use and publication of anonymized data, including direct quotations. No identifiable personal information is disclosed in this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the Medical Research Project of Jiangsu Province Health Commission (No. Key Project-K2024074), Suzhou Basic Research Pilot Project — Nursing Program (No. SSD2025074), Suzhou Basic Research Pilot Project — Nursing Program (No. SSD2025077).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hankey GJ. Stroke. Lancet. 2017;389(10069):641–14. doi:10.1016/S0140-6736(16)30962-X
2. Gao Y, Xie YM, Cai YF, et al. Risk factors associated with recurrence within 90 days of ischemic stroke onset in Chinese medicine hospital: a national cross-sectional study in China. World J Tradit Chin Med. 2020;6(4):441. doi:10.4103/wjtcm.wjtcm_32_20
3. Di Pino G, Pellegrino G, Assenza G, et al. Modulation of brain plasticity in stroke: a novel model for neurorehabilitation. Nat Rev Neurol. 2014;10(10):597–608. doi:10.1038/nrneurol.2014.162
4. Wein T, Lindsay MP, Côté R, et al. Canadian stroke best practice recommendations: secondary prevention of stroke, sixth edition practice guidelines, update 2017. Int J Stroke. 2018;13(4):420–443. doi:10.1177/1747493017743062
5. Shani SD, Varma RP, Sarma PS, Sylaja PN, Kutty VR. Life style and behavioural factors are associated with stroke recurrence among survivors of first episode of stroke: a case control study. J Stroke Cerebrovasc Dis. 2021;30(4):105606. doi:10.1016/j.jstrokecerebrovasdis.2021.105606
6. Spence JD. Recent advances in preventing stroke recurrence. F1000Res. 2017;6:1017. doi:10.12688/f1000research.11597.1
7. Dunton GF. Sustaining health-protective behaviors such as physical activity and healthy eating. JAMA. 2018;320(7):639–640. doi:10.1001/jama.2018.6621
8. Ruf A, Koch ED, Ebner-Priemer U, Knopf M, Reif A, Matura S. Studying microtemporal, within-person processes of diet, physical activity, and related factors using the APPetite-mobile-app: feasibility, usability, and validation study. J Med Internet Res. 2021;23(7):e25850. doi:10.2196/25850
9. Zhong W, Pan X, Li J, et al. Examining the association between diet-related situational factor and dietary behavior: an observational study of diet-related situational factors in stroke patients during rehabilitation. Front Nutr. 2025;12:1696883. doi:10.3389/fnut.2025.1696883
10. Shams-White MM, Korycinski RW, Dodd KW, et al. Examining the association between meal context and diet quality: an observational study of meal context in older adults. Int J Behav Nutr Phys Act. 2021;18(1):67. doi:10.1186/s12966-021-01122-x
11. Chwyl C, Crochiere RJ, Forman EM. The role of everyday activities on likelihood of dietary lapse: an ecological momentary assessment study. J Behav Med. 2023;46(3):532–539. doi:10.1007/s10865-022-00365-8
12. Lindsay K, Buss C, Entringer S, Wadhwa P. Greater maternal perceived stress levels are associated with a higher dietary inflammatory index among hispanic pregnant women. Curr Dev Nutr. 2020;4:
13. Bailey RR, Ipsen M. Facilitators and barriers to performing dietary behaviors among chronic community-dwelling stroke survivors: a qualitative secondary analysis. Disabil Health J. 2022;15(3):101270. doi:10.1016/j.dhjo.2022.101270
14. Bailey R, Ipsen M. Dietary behaviors following stroke: a qualitative study of stroke survivor perspectives. Stroke. 2022;53(Suppl_1):ATP230–ATP230. doi:10.1161/str.53.suppl_1.TP230
15. Zhang L, Zhou L, Ye Q, Zhang L, Kong Y, Xia S. Impact of transcranial direct current stimulation combined with motor-cognitive intervention on post-stroke cognitive impairment. Neurol Sci. 2023. doi:10.1007/s10072-023-07156-2
16. Tang R, Guan B, Xie J, et al. Prediction model of malnutrition in hospitalized patients with acute stroke. Top Stroke Rehabil. 2024:1–15. doi:10.1080/10749357.2024.2377521
17. Ademoyegun AB, Ibitoye AG, Rasaq WA, et al. Eating difficulties among Nigerian community-dwelling stroke survivors: prevalence, correlates, and association with quality of life. BMC Public Health. 2025;25(1):519. doi:10.1186/s12889-025-21749-w
18. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
19. Chen D, Zhang H, Shao J, et al. Determinants of adherence to diet and exercise behaviours among individuals with metabolic syndrome based on the capability, opportunity, motivation, and behaviour model: a cross-sectional study. Eur J Cardiovasc Nurs. 2023;22(2):193–200. doi:10.1093/eurjcn/zvac034
20. Kavuran E, Özalp C, Ay E. The impact of a walking program on self-management, anxiety, stress, depression, quality of life, and seizure frequency in patients with epilepsy: a mixed methods approach using the COM-B behaviour change model. Epilepsy Behav. 2025;162:110149. doi:10.1016/j.yebeh.2024.110149
21. Wang WX, Qiu J, Kong LN, et al. Effects of an exercise intervention based on the COM-B model among community-dwelling prefrail older adults with diabetes: study protocol for a randomised controlled trial. BMJ Open. 2025;15(6):e098945. doi:10.1136/bmjopen-2025-098945
22. Chinese Society of Neurology of Chinese Medical Association, Cerebrovascular Division, Chinese Society of Neurology of Chinese Medical Association. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018. Chin J Neurol. 2018;51(9):666–682. doi:10.3760/cma.j.issn.1006-7876.2018.09.004
23. Kirkevold M. The unfolding illness trajectory of stroke. Disabil Rehabil. 2002;24(17):887–898. doi:10.1080/09638280210142239
24. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
25. Mujamammi AH, Alluhaymid YM, Alshibani MG, et al. Awareness of cardiovascular disease associated risk factors among Saudis in Riyadh City. J Family Med Prim Care. 2020;9(6):3100. doi:10.4103/jfmpc.jfmpc_458_20
26. Benameur K, Gandrakota N, Ali MK. Nutritional counseling of stroke patients by neurology residents, a call to action. Front Neurol. 2022;13:940931. doi:10.3389/fneur.2022.940931
27. Ghosh Roy P, Jones KK, Martyn-Nemeth P, Zenk SN. Contextual correlates of energy-dense snack food and sweetened beverage intake across the day in African American women: an application of ecological momentary assessment. Appetite. 2019;132:73–81. doi:10.1016/j.appet.2018.09.018
28. Goldschmidt AB, Smith KE, Crosby RD, et al. Ecological momentary assessment of maladaptive eating in children and adolescents with overweight or obesity. Int J Eat Disord. 2018;51(6):549–557. doi:10.1002/eat.22864
29. Miyauchi T, Sasaki S, Tanemura R. Behavioral problems and self-feeding independence among patients with acute stroke: a single-center study. Am J Occup Ther. 2024;78(5):7805205080. doi:10.5014/ajot.2024.050644
30. Roordink EM, Steenhuis IHM, Kroeze W, Hoekstra T, Jacobs N, van Stralen MM. Social environmental predictors of lapse in dietary behavior: an ecological momentary assessment study amongst dutch adults trying to lose weight. Ann Behav Med. 2023;kaac077. doi:10.1093/abm/kaac077
31. Singh P, Jayakaran P, Mani R, Hale L. The experiences of Indian people living in New Zealand with stroke. Disabil Rehabil. 2022;44(14):3641–3649. doi:10.1080/09638288.2021.1878294
32. Allan J, McMinn D, Powell D. Tracking snacking in real time: time to look at individualised patterns of behaviour. Nutr Health. 2019;25(3):179–184. doi:10.1177/0260106019866099
33. Robinson E, Aveyard P, Daley A, et al. Eating attentively: a systematic review and meta-analysis of the effect of food intake memory and awareness on eating. Am J Clin Nutr. 2013;97(4):728–742. doi:10.3945/ajcn.112.045245
34. Wahl DR, Villinger K, König LM, Ziesemer K, Schupp HT, Renner B. Healthy food choices are happy food choices: evidence from a real life sample using smartphone based assessments. Sci Rep. 2017;7:17069. doi:10.1038/s41598-017-17262-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Qualitative Study on the Humanistic Care Needs of Patients with Stroke and Their Families
Li M, Xie H, Luo Q, Huang G, Xu G, Cheng Y, Li J
Journal of Multidisciplinary Healthcare 2023, 16:717-730
Published Date: 16 March 2023
Preferences for Rehabilitation in Persons with a History of Stroke: A Discrete Choice Experiment
Noto S, Murata T, Saito S, Watanabe T, Kobayashi M
Patient Preference and Adherence 2023, 17:1611-1620
Published Date: 12 July 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Factors Influencing Adherence to Dietary Interventions Among Patients with Gestational Diabetes Mellitus in China: A Qualitative Study Based on the COM-B Model
Jia CL, Wang LJ, Li LH, Lu YJ, Yang Y
Journal of Multidisciplinary Healthcare 2025, 18:4653-4663
Published Date: 5 August 2025
Rate of Post-Stroke Depression and Associated Factors in Saudi Single Tertiary Medical Center
Aljuhani T, Alsubaie S, Al-Mutairi AM, Altheyab AS, Alsahali AM, Alhamdan AS, Alqahtani FM, Olayan LH, Senitan M
Journal of Multidisciplinary Healthcare 2025, 18:5421-5430
Published Date: 2 September 2025