Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Qualitative Study on the Humanistic Care Needs of Patients with Stroke and Their Families
Authors Li M, Xie H, Luo Q, Huang G, Xu G, Cheng Y, Li J
Received 2 September 2022
Accepted for publication 23 December 2022
Published 16 March 2023 Volume 2023:16 Pages 717—730
DOI https://doi.org/10.2147/JMDH.S388539
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Min Li,1 Hongzhen Xie,2 Qing Luo,3 Guangbin Huang,1 Guoxian Xu,1 Ye Cheng,1 Jun Li4
1Department of Traumatology, Chongqing University Central Hospital, Chongqing Emergency Medical Center, Chongqing, People’s Republic of China; 2Department of Health Medicine, General Hospital of Southern Theatre Command, Guangzhou, People’s Republic of China; 3Department of Neurosurgery, General Hospital of Southern Theatre Command, Guangzhou, People’s Republic of China; 4Chongqing Metropolitan College of Science and Technology, Chongqing, People’s Republic of China
Correspondence: Jun Li, Chongqing Metropolitan College of Science and Technology, No. 368, Guangcai Avenue, Yongchuan District, Chongqing, 402160, People’s Republic of China, Tel +86 18084067947, Email [email protected]
Background: International stroke care guidelines recommend the routine assessment and management of psychological and emotional problems in patients and their families after a stroke. This study aimed to explore the humanistic nursing needs of patients with stroke and their families and provide a basis for the construction of humanistic nursing practice guidelines for advanced stroke.
Methods: From September to October 2019, using the descriptive phenomenological research method, a semi-structured interview outline was formed based on a literature review and subject group discussions. A targeted sampling method was used to investigate 21 patients with stroke and 21 family members, respectively, and their care needs were investigated in depth. Colaizzi’s thematic cluster analysis was used to analyse the data, and a total of 6 themes and 14 sub-themes were summarised.
Results: The 6 themes and 14 sub-themes were as follows: ① psychological care, ② security concerns (professional personal integrity, timely response), ③ emotional care (service consciousness, positive incentives, empathy, effective communication, provision of a communication platform, personalised care), ④ respect for rights, ⑤ rehabilitation care (rehabilitation programme, professional guidance, rehabilitation configuration, continuation of services) and ⑥ family care (physical and psychological support, care guidance).
Conclusion: Among the humanistic care needs of patients with stroke and their families, the most basic physiological care accounts for the largest proportion of emotional and rehabilitation care, followed by safety care, respect for rights and family care. Based on the actual humanistic care needs of patients with stroke and their families, the practical effect of humanistic care in stroke wards can be improved. This study provides a reference for the construction of humanistic nursing practice guidelines for late stroke.
Keywords: stroke, humanistic care, qualitative research
Introduction
Stroke is an acute traumatic life event that threatens human life and health. About 75% of survivors of stroke have varying degrees of functional and psychological impairment, which places a heavy burden on families and society.1 Humanistic care that emphasises understanding, respect and attention to the actual needs of patients with stroke and their families can improve mental health and even affect recovery outcomes. According to relevant research reports, medical personnel in China receive relatively little effective humanistic care education, and their humanistic practical care abilities are relatively low.2–4 In 2018, scholars conducted a survey of 211 hospitals in China on the issue of humanistic care practice, and the results showed that the quality of humanistic care practice was not optimistic; it could even be said that there was no real humanistic care.5–7
For hospitals, effective practice is the key to delivering humanistic care for patients; however, since China’s humanistic care evaluation indicators have not been standardised, and there is a lack of proven guidelines for specialist care, the development of care standards is imperative. Since the 1990s, many scholars in China have devoted themselves to research related to humanistic care. In the early 20th century, the National Health Care Commission proposed policies related to quality care services, which provided opportunities and guidelines for humanistic care research and practice. Now, in the 21st century, humanistic care practice is dominated by the will of managers, and there is limited humanistic care from the perspective of specialist nursing.8 The development of humanistic care standards for specialities requires not only manager-led and medical staff participation but also full consideration of the care needs of patients and their families. At present, research on the humanistic care needs of patients with stroke and their families is not comprehensive enough, and there is a lack of a practical perspective to explore the humanistic care needs of this group.9 Therefore, the current study explored the practical humanistic care needs of patients with stroke and their families through semi-structured interviews to provide a reference for the construction of humanistic care practice guidelines for the later stages of stroke.
Methods
Design and Participants
The descriptive phenomenological research method was used to collect data through one-to-one structured interviews. Twenty-one patients with stroke and 21 family members were surveyed separately using a phenomenological research method that included semi-structured qualitative interviews. From September to October 2019, 21 patients and 21 family members in a tertiary care hospital in Guangzhou, who each met the inclusion and exclusion criteria, were selected for inclusion in this study and were interviewed qualitatively. The recruited patients were enrolled during treatment in the hospital’s stroke unit. The interview time was stable and clearly answered, the patient’s interview was conducted alone on the ward, and the patients and their family members were interviewed separately. Names were replaced by serial numbers (A1–A21 and B1–B21), and sample inclusion was stopped when no new themes or concepts emerged.
The patient inclusion criteria were: ① patients who met the revised diagnostic criteria of the Neurological Disorders Branch,10 ② had a confirmed diagnosis of stroke by cranial computed tomography or magnetic resonance imaging, ③ were aged ≥18 years, ④ were in a stable condition and ⑤ who participated voluntarily in this study. The patient exclusion criteria were: ① patients who were uncooperative, eg in a coma or with impaired consciousness, dementia or aphasia, ② with a previous history of dementia or psychosis and ③ with a history of alcohol or drug abuse.
The family inclusion criteria were: ① the primary family caregiver (the person in the family with primary responsibility for caregiving or who spends the most time caring),11 ② with normal verbal communication, ③ aged ≥18 years and ④ who participated voluntarily in this study. The family exclusion criteria were: ① paid carers (nannies, carers, etc.) and ② those with a history of alcohol or drug abuse or mental illness.
Detailed information on the participants was collected at the beginning of the discussion. These data included age, gender, education level, address, religion, main occupation, relationship of the family members to the patient with stroke, duration (years) of care and severity and duration of the patient’s illness. The interview took place in a quiet room to ensure that was no external interference during the interview. Before the formal interview, the purpose and method of the study were explained to the interviewees. Assurances were given that codes would be used instead of the patients’ identification data and that letters and numbers would be used to represent individuals to ensure their privacy. A consent form was signed, and the entire process was recorded simultaneously. During the interview, the researcher listened carefully, did not interrupt, remained neutral, observed changes in the interviewees’ tones, expressions, emotions and actions and recorded them in time. Each interview lasted about 120 minutes.
Establishing a Research Group
A total of 15 research group members were included, comprising five junior-, middle- and senior-level members, one director, one deputy director and one research officer from a tertiary hospital nursing department, six stroke specialist practitioners (stroke specialists, specialist nurses, rehabilitation technicians, clinical specialists, managers, etc.) and six postgraduate nursing students. The team members were involved throughout the study, discussing and identifying key issues in the research process. The data analysis in this study was completed by Li Jun, and the transcriptionists were Li Min, Xu Guoxian and Huang Guangbin, who used the inscription and statistical functions of OFFICE. The English translations were performed by team members with backgrounds in Chinese and Western studies.
Ethical Considerations
This study was approved by the ethics committee of the General Hospital of the Southern Theatre Command of the Chinese People’s Liberation Army. A full explanation of the research purpose and method, rights and obligations, use of recording equipment and other related matters was given to the interviewees. All participants provided a written and signed letter of consent before the interview, and they agreed to publish the relevant data anonymously.
Data Collection
The first draft of the qualitative interview was formed from the results of a literature review and clinical practice, and the outline of the formal interview was compiled after group discussion, expert consultation and pre-interviews. The outline is shown in Table 1 and Table 2. Interviewers were involved in each interview, and the entire interview was recorded for 30–90 minutes; the purpose, methods, rights and obligations of the study were fully explained to the interviewees, and an informed statement was signed.
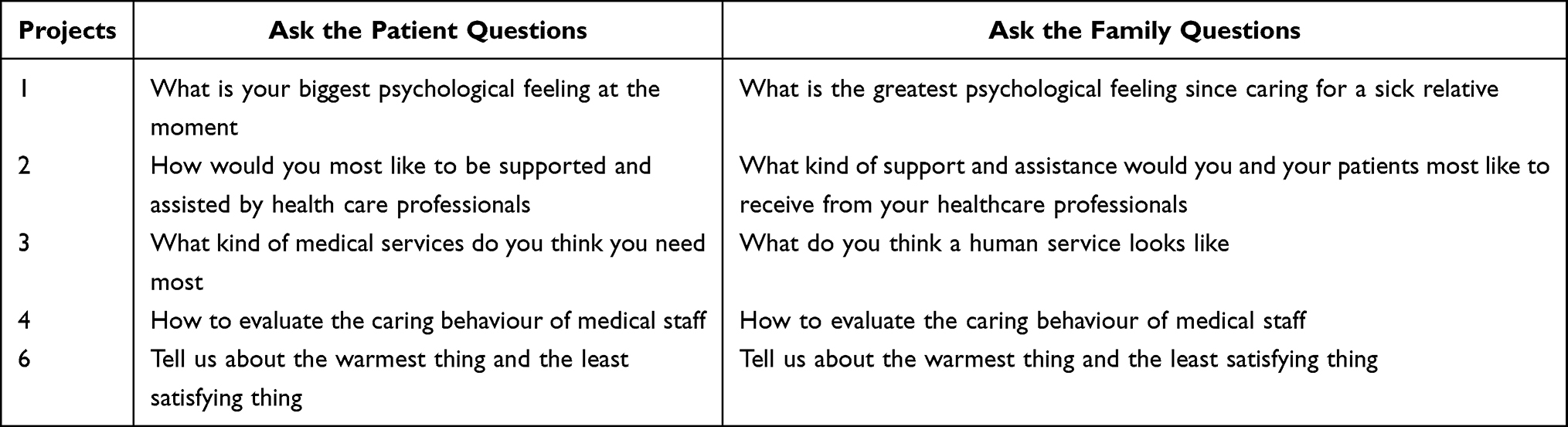 |
Table 1 Outline of the Interviews |
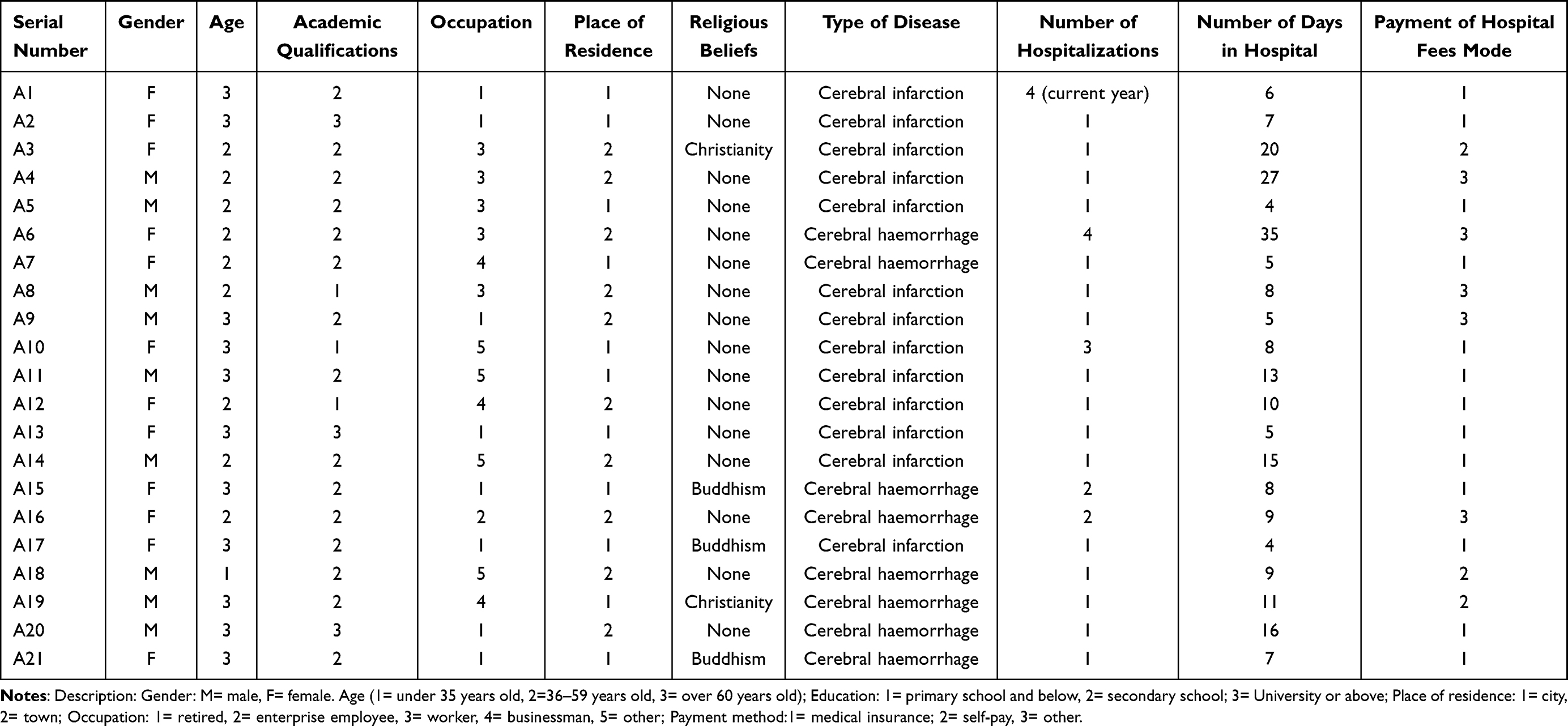 |
Table 2 Characteristic of Stroke Patients |
Data Analysis
Within 24 hours after the interview, the recorded data were translated into words, and the non-verbal data, such as the interviewees’ attitudes and actions observed during the interview, were categorised.12,13 Colaizzi’s thematic cluster analysis was used to analyse the data.
(1) The recorded data was converted into a verbatim text manuscript, which was studied repeatedly to derive an overall concept. (2) The meaningful content in the statements was extracted as initial coding keywords. (3) The keywords and repeated text fragments were analysed to form categories and subcategories. (4) Ideas were collected. (5) Detailed excerpts and descriptions of the collected views were produced. (6) The assembled ideas were systematically grouped into conceptualised themes. (7) The collated documents were returned to the interviewees to check the consistency of the statements.
Quality Control
Before the interview, a good relationship was established with the patient and their family, and a representative sample of the study population was selected. During the interview, the interviewer’s attitude remained neutral throughout, with no eliciting or suggestive statements; the analysis process was achieved in suspension, with an open-minded perspective and without prior knowledge or experience. The interviewees were encouraged to express themselves fully, clarifying inaccurate information when appropriate, and their expressions and non-verbal behaviours were recorded. After the interview, the recording was studied repeatedly and transcribed and analysed in detail. After transcription, the original recording was compared with the transcribed version, and the transcription was sent to the participant for confirmation. When there was disagreement on the refined theme, the research group held a discussion, compared the differences between the two and determined the final theme.
Results
General Participant Information
There were 42 participants from 22 cities in 8 provinces (municipalities directly under the central government) in China. There were 21 patients with stroke, with 21 corresponding family members (patients: A1 to A21; family members: B1 to B21). The male-to-female ratio was 1:1. Seven had religious beliefs, accounting for 16.7% of the participants. The age of the patients was (56.67 ± 12.10) years, the length of hospitalisation was (1.48 ± 0.83) years, and the number of hospital days was (21.00 ± 7.94) days. Seventy-six percent of the patients had a secondary school education. The family members were (43.19 ± 16.29) years old, the length of care was (297.76 ± 1239.64) days, and 72% had a secondary school education.
Table 2 and Table 3 list the basic characteristics of the participants in terms of occupation, family relationship with the patient, years of care and severity and duration of the patient’s illness. Table 4 contains the interview results.
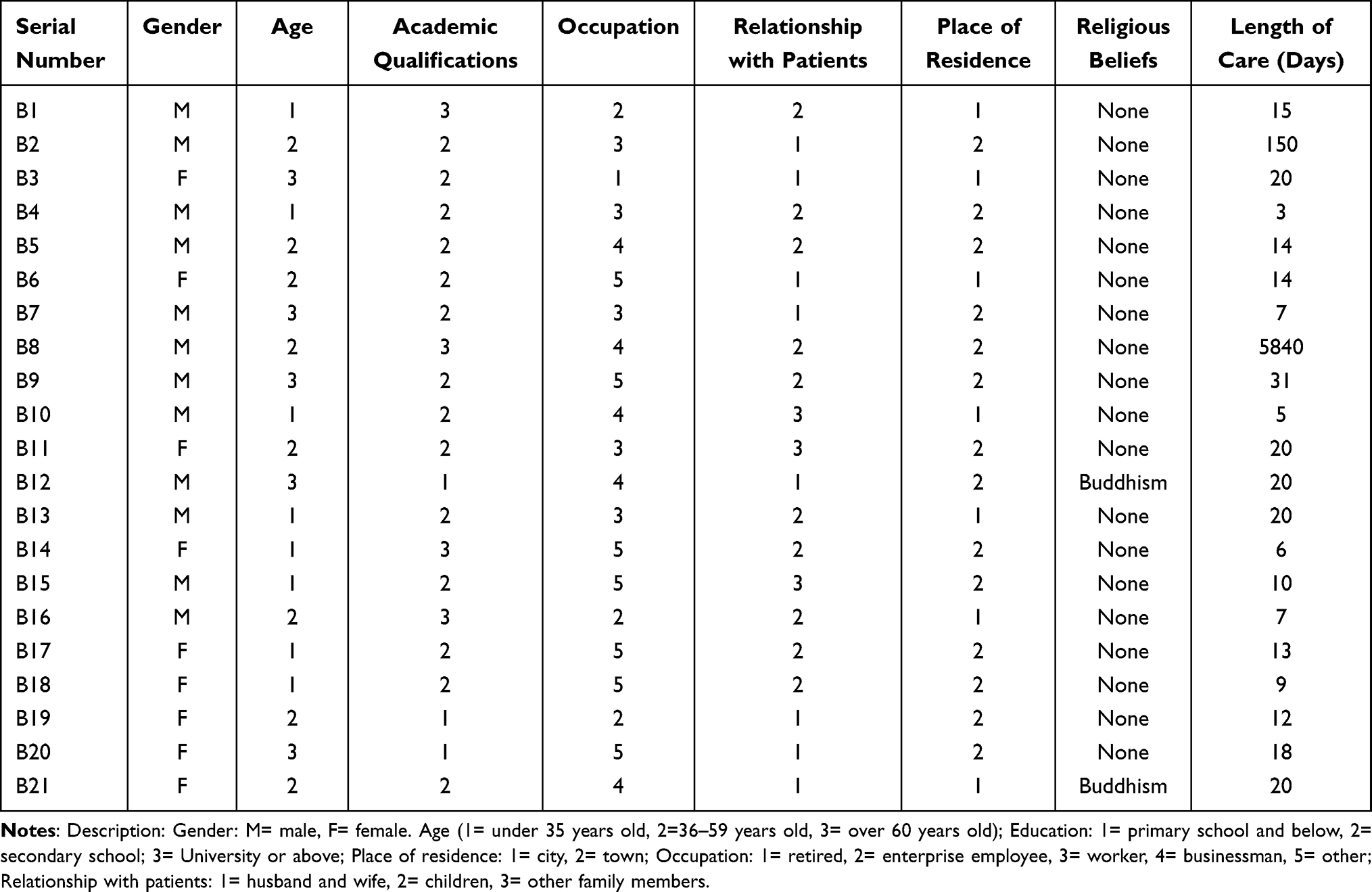 |
Table 3 Characteristic of Relatives |
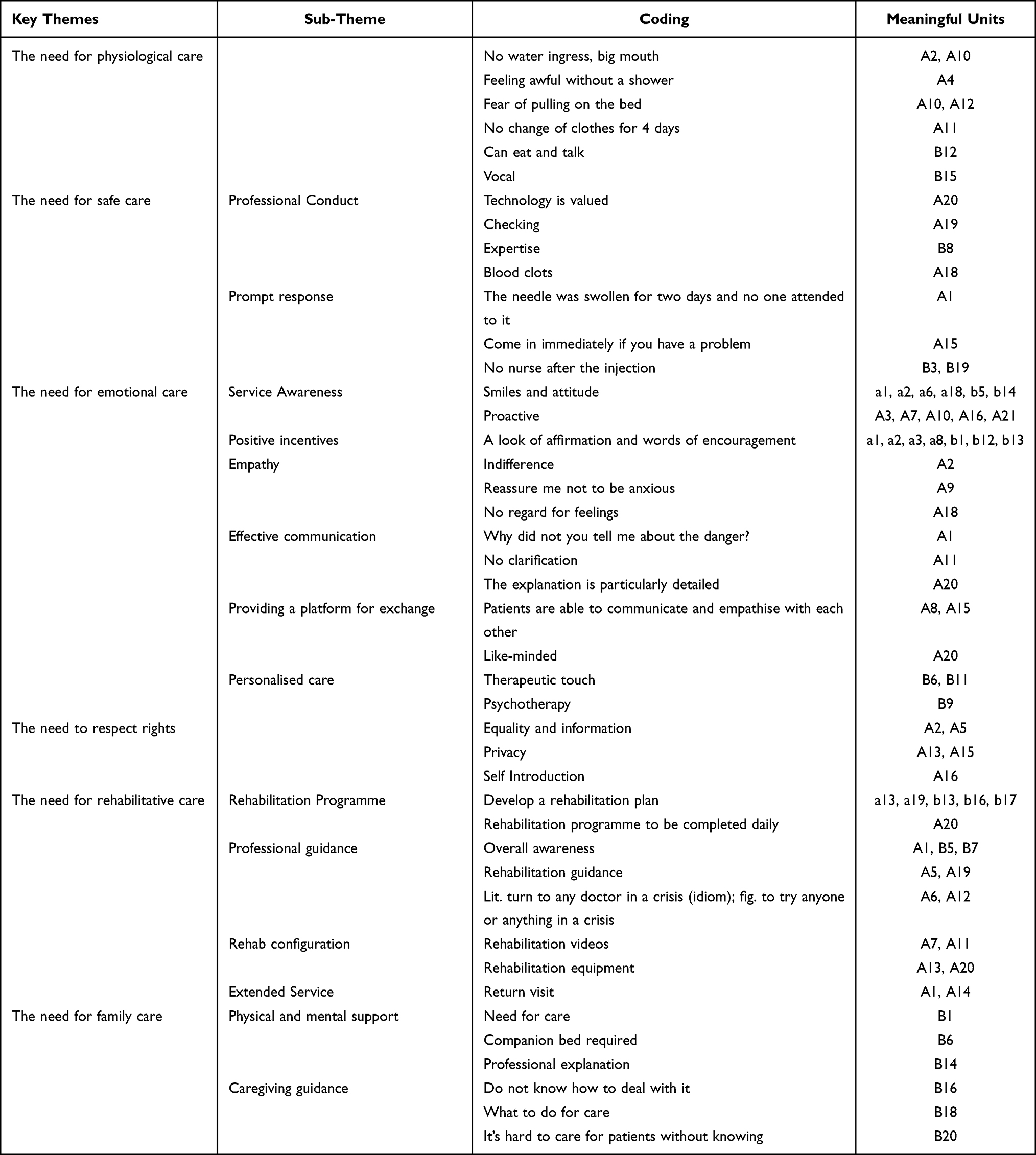 |
Table 4 Subjects, Codes, Meaningful Units |
Theme 1: The Need for Physiological Care
All the interviewees in this study agreed that physiological care was the primary humanistic need and that other humanistic needs should only be considered if an extension to life is guaranteed. The most troubling physiological problems for patients with stroke are the range of problems caused by swallowing disorders and those of elimination and discomfort caused by passive bed rest.
Respondent A2 said:
I’m a very careful person. I’ve been in hospital with a gastric tube, and I can’t take care of myself. I haven’t had a drop of water in my mouth for many days, [and] my tongue is like a wooden poke. I don’t even dare to talk because I have such a big mouth. I’d be grateful if a ‘nurse’ could help with this.
Respondent A4 said:
It’s hard not to have a bath for so many days; I feel particularly dirty… Even if I can’t wash it, it’s good to wipe it with hot water, but I can only think about it.
According to respondent A10:
I’m alone in the hospital. No one helps me on the toilet; I don’t eat or drink, or I poo on the bed…
Respondent B12 stated:
Being able to eat and talk solves a lot of problems, [like] inserting a stomach tube, [which] he always wants to pull out.
Theme 2: The Need for Safe Care
The need for safety is an instinctive response. During the interviews, 12 patients expressed helplessness and fear caused by a lack of disease-related knowledge, unknown disease progression and recovery outcome. The patients and their family members agreed that the feeling of safety comes from the professionalism of the medical staff, including responsibility, professional knowledge, operational skills and standard management.
Professional Manipulation
Respondent A18 said:
There was some blood back in the indwelling needle in my hand; one nurse drew it off each time before the drip, but the other nurse just flushed the clot straight back into the blood vessel. How did the two do it differently? Can a blood clot be harmful when pushed back into a blood vessel?
Respondent A19 stated:
Some nurses will ask you what your name is every time you come over to give a shot and issue medication, and only after they are sure will they issue the medication and give the shot; some nurses will just do it without asking your name, or they will just look at the bed number.
Respondent A20 said:
I am also a professional technician. I value this piece of technology. Before I was hospitalised in a hospital and had to give an injection, the nurse searched and searched but couldn’t find the blood vessel; it took four consecutive injections to get it. The basic skills should be well practised to reduce a lot of pain for patients; this is also the greatest care for us.
Answer Promptly
Respondent A1 said:
My indwelling needle has been swollen for 2 days, and no nurse has come to take care of it. I called her and forgot.
Respondent A15 stated
If you have a problem, you can come immediately or come more often to help me find the problem in time and deal with it earlier.
Respondent B3 reported:
No nurse for a long time after the injection.
Theme 3: The Need for Emotional Care
This theme was mentioned by a total of 29 people, accounting for approximately 70% of the total number of respondents; it was the most popular of all the themes. The sub-themes included awareness of service, positive motivation, empathy, effective communication, providing a platform for patients to interact with each other and the need for personalised care. During the interviews, eight patients were afraid to express their true feelings and needs to the medical staff for fear of being disliked, while they wished for active greetings, understanding of needs, listening to feelings, thinking differently and patience and attentiveness.
Awareness of Service
Respondent A1 said:
For us patients, we really don’t ask for much; even a smile or a look is very satisfying, the service of putting yourself in the patient’s shoes is really more useful than the treatment plan…
Respondent A10 stated:
When I was in the local hospital and wanted to get a reimbursement slip from the inpatient office, the nurse said: “you can’t use your legs; I’ll bring it over for you.” I immediately cried.
Respondent A21 said
Many people are too afraid to talk or ask. Ask them what they need and help answer their questions so that they can reach people’s hearts.
Positive Motivation
Respondent A8 reported:
The most important thing I want the medical staff to tell me is to get well soon. I feel confident after listening to them. I feel sorry for them if I don’t get well soon.
Respondent B12 said:
The hospital is the last straw; if the medical staff can’t give him encouragement, he may not have much desire to live. If the medical staff can’t give him encouragement, he may not have much faith.
Respondent B13 stated:
I hope the medical staff can give us some good cases so that we all have something to look forward to.
Empathy
Respondent A2 stated:
I told the nurse that I had a headache, and she said sure la; all day long I was lying…feeling so cold-blooded.
Respondent A9 said:
The first few days I was admitted, I always had a lot of questions to ask, and they all understood my feelings and comforted me…
Effective Communication
Respondent A1 stated:
Good communication relaxes our mind[s]. The doctor told me that my illness was more dangerous than everyone else’s in the ward but he didn’t tell me how dangerous it was. I see the other two are paralysed in bed and scared to death.
Respondent A20 said:
I saw that the doctor in the next bed was very good; he came to see him several times a day and gave him the checklist himself. He gave a particularly detailed explanation and made analogies for medical terms he didn’t understand, so he understood it as soon as he heard it.
Providing a Platform for Communication
Respondent A8 stated:
If the hospital can provide us with a platform for patients to communicate with each other, organise some patient meetings and invite discharged patients to join together to talk about their post-stroke recovery journey so that we can tread less on the pitfalls.
According to respondent A15:
The psychological hurdle is very difficult after a stroke; maybe the medical staff can understand, but how can he care so much when he’s used to seeing it? Only we, the patients, can understand each other and have a sense of compassion for each other.
Personalised Care
Respondent B6 stated:
My dad is in a coma. I wish the nurse would talk in his ear, [give] simple physical contact, give him more stimulation; maybe he could hear it, and that would help him revive.
According to respondent B11:
Maybe it’s hard to accept mentally because he had a stroke. He doesn’t talk to us; I wish there could be a nurse to hold his hand so he can feel warmth.
Respondent B9 stated:
My son used to be alive and well. Now, he is only paralysed in bed. He can’t accept his state; he is on a hunger strike and refuses treatment. I really need a psychologist to ease his mind.
Theme 4: The Need to Respect Rights
Patients with stroke are vulnerable to low self-esteem due to their neurological deficits. Many of the interviewees described how they were “not like human beings, not like ghosts” after their illness and how few medical staff really cared about their personal rights, especially their privacy.
According to respondent A13:
In the morning, the bed next door was not there, and the medical staff who checked the room were saying that this bed was positive for M toxin and something else that didn’t sound good. I thought, are they always like that? It was quite uncomfortable mentally, even though it wasn’t me who was saying it.
Respondent A15 said:
We have requests for hospital stays that will be frowned upon, being called difficult to serve. The only thing I wish I could do is to pull the curtain for me when I am being cleaned; there are men in the ward, and the door is open. Every time I have my skin checked, I lift the blanket and pull down my trousers, I’m not prepared.
Theme 5: The Need for Rehabilitation Care
Nearly 75% of stroke survivors have varying degrees of functional impairment,1 making rehabilitation care the most pressing care topic for the majority of patients and their families. A total of 22 respondents, or 52% of the total number interviewed, talked about this. The most important aspects of rehabilitation they were concerned about included rehabilitation programmes, professional guidance, rehabilitation configurations and continuity of services.
A Well-Developed Rehabilitation Plan
Respondent A20 said:
You can tell us the rehabilitation plan to be completed each day or give me a form so I know what I have to do that day or what I will be doing tomorrow.
Respondent B16 stated:
Give the patient and family a rehabilitation plan. Which step needs to be done when? Which treatment should be on when? That way, the family has a mental picture and can organise themselves in advance.
Professional Guidance
Respondent A1 said:
Being in hospital gives us an understanding of our condition or allows us to learn more about the disease. It’s particularly scary when you don’t know anything about it; once you understand it, maybe, you won’t be so scared.
Respondent A5 stated:
Help guide us when we walk past, and [when you] see that we are not exercising correctly, teach us how we should be exercising.
Respondent B7 said:
We should be told about any rehab that needs to be done earlier; we have only heard that it needs to be done earlier. We don’t know exactly how early.
Rehabilitation Configuration
Respondent A7 said:
A lot of times when we are lying in bed, we don’t have the motivation to do rehabilitation exercises, and sometimes, we forget how to do them. We can’t get out of bed, so it would be good if we could put some rehabilitation exercise videos on the ward where we can watch and learn along at any time.
Respondent A13 stated:
I can’t get out of bed. My hands and feet feel like they are frozen. I feel like there is no blood left. Is there any machine that can warm up my hands and feet?
According to respondent A20:
I feel like there’s no other configuration here apart from that machine that pushes around, and it’s hard to say how effective it is. We don’t even have a choice. Is there nothing else?
Continuing Services
Respondent A1 stated:
It would be nice to be able to ask occasionally after discharge about the progress of recovery, problems and follow-up appointments. We don’t even know which doctor’s number to call for our follow-up appointments, so it would be better if we could be seen by the bedside doctor during our stay in hospital; as we have already established a relationship upfront, we are familiar with each other and trust each other much more.
Theme 6: The Needs of Family Carers
In the interviews, most of the interviewees’ families were in the lower-middle class. Their families responded that they were under far more pressure than they thought and that, in addition to the financial burden of care, they were afraid of being left with no money but even more afraid of losing their loved ones. Many families expected medical staff to care for their patients while occasionally taking care of their families and giving support when appropriate.
Physical and Psychological Support
Respondent B1 said:
Can you do psychological comfort for the family? Help me quickly…I feel I can no longer cope and need care badly.
Respondent B6 stated:
They can’t even manage their patients. How can they have the time to care for us? I wish we could just give the family a companion bed. We’re really tired…
Care Instructions
Respondent B18 commented:
We would like to know what to do for care during hospitalisation. How does rehabilitation work? What are the precursors to a relapse? What to do about exercise…The medical staff can tell us from big data.
According to respondent B20:
We would like the medical staff to tell us how this disease was caused. What should we pay attention to in the future? Are there any dietary contraindications? It is difficult to take care of patients when we don’t know anything but only how to serve them.
Discussion
Quality Care is a Fundamental Prerequisite for Meeting the Needs of Patients
In 2010, China released the “Quality Care Service Demonstration Project Activity Programme”, and immediately, quality care became an important indicator of nursing quality evaluation.14 The content of quality care runs through the whole process of patient care, involving service attitude, communication, safety management and so on. The essence is patient centred, in line with the original intention of humanistic care.15 To better serve patients, it is natural to start with their needs. The needs of patients with stroke vary according to the period of recovery, but no matter the period, quality care is essential.16 The frequency of text coding in this study for the themes of service awareness, service response, safety of care, physical and psychological support, respect for rights, communication and guidance was high. The results of this study suggest that patients with stroke and their families are also most concerned about the quality of care, which is similar to the findings of most academics.17–19
Many needs are not met due to neurological deficits, such as eating, cleaning and independent walking. Respondent A2 said in an interview:
I’ve been in hospital with a gastric tube…and my tongue is like a wooden poke, I can’t even stand it…
which is consistent with the feelings of patients reported in a survey on human needs in intensive care units.20 The situation described by respondent A2 reflects our thoughts on the quality of primary care. At the same time, factors, such as attitude, delays and language of service, can lead to a loss of trust in healthcare institutions; studies have reported that this can lead to up to 80% of medical disputes and is an important driver of reduced patient satisfaction and tension between doctors and patients.21,22 Therefore, nursing staff can turn passive information into active service by enhancing their service awareness, strengthening their communication skills and calmly asking patients about their needs so that basic care can be completed and quality care can be truly implemented. Li Huiling’s team23 illustrated this theme well by building a basic care service chain, with remarkable results.
Second, during the nursing process, we observe changes in patients’ conditions, strictly implement core medical system and nursing protocols and strengthen anticipatory care based on perfecting the assessment, prevention, reporting and treatment plans for stroke-related complications and adverse events; thus, potential threats to patients’ lives can be detected and addressed promptly to enhance the safety of patients and their relatives and improve the patient care experience.
In line with the findings of other research,24–26 emotional care and respect for individual rights are elements of concern for patients and their families, which they expect to receive consistently. Widar27 states that considerate care can make for a helpful care experience for patients with stroke and prevent frustration. In patients with stroke, sudden functional impairment and role changes often make it hard for them to accept reality, leading to low self-esteem, anxiety, depression and other negative emotions. In these interviews, the vast majority of patients had thoughts of life as death and light-heartedness, which could be significantly reduced by effective psycho-emotional care.28 In addition, some of the interviewees reported that it was difficult to feel respected by medical staff and felt that they were treated only as patients and not as equals. Therefore, patients require care that is truly comprehensive, and emotional care and basic respect are both important elements of quality care.
Rehabilitation Care is an Urgent Component of Meeting Patients’ Needs
Quality of life is one of the most common indicators of the effectiveness of rehabilitation for patients with stroke.29 Assisting such patients to gain the ability to return to society and maximise their quality of life is the ultimate goal of humanistic care in stroke wards and is appreciated by patients and families. During the interviews, 22 respondents mentioned rehabilitation-related needs, most of whom lacked knowledge about the disease, thus delaying optimal treatment. According to Zhang Xiuying et al,30 less than 35% of patients and their families know about stroke disease and warning symptoms, and less than 40% know how to identify them and the time window for thrombolysis; however, in Malaysia and the USA,31,32 over 90% of people know the symptoms of stroke, and over 70% know they must seek treatment within the thrombolysis time window. Therefore, it is imperative to provide professional medical information and technical guidance and increase the breadth and depth of stroke knowledge to improve public health literacy. Patients and their families should also be invited to work with a multidisciplinary team to develop and implement a personalised rehabilitation plan to help them understand the stages of stroke recovery and build their confidence. This participatory approach to rehabilitation was reported in33 to have a significant impact on patients’ recovery of function and mobility and improve their quality of life. In addition, ongoing health education, pre-discharge homecare and home modification guidance, and post-discharge extended care and follow-up visits are needed to better consolidate the effects of rehabilitation treatment.
Family Care is an Integral Part of Humanistic Stroke Care Practice
Family members are the primary caregivers of patients who have had a stroke, and the quality of care can have a direct impact on the outcome of the patient’s recovery; however, this topic is often overlooked in the current healthcare system. Relevant data34,35 show that in 2019, the incidence of stroke in China was 201/100,000, with an increasing prevalence. The number of people aged 40 and over who are living with stroke is approximately 17.04 million, and the standardised prevalence of stroke in the population aged 40 and over has increased from 1.89% in 2012 to 2.58%. In contrast, at the end of 2018, the total number of registered nurses in China was only 4,098,600, and there was a gap between the bed-to-nurse ratio and the relevant standard.
In recent years, many scholars in China have gradually focused on the families of patients with stroke, but there are fewer references to family care.36–38 Studies by Wiles39 have shown that families mostly feel stressed in the early stages of caring for a patient with stroke due to a lack of appropriate caregiving knowledge. Similar findings have been reported in other studies, including the Scoping Review,40 which found that stroke carers felt that care knowledge and physical and psychological support were the most urgently needed aid. Therefore, assessing family carers’ stress reactions, the stress of caring for patients with stroke and providing information on stress management, caregiving skills training and access to professional companions can help families feel the warmth of their carers and reduce their physical and emotional stress.41
Conclusion
Based on the actual humanistic care needs of patients with stroke and their families, the practical effect of humanistic care in stroke wards can be improved. This study provides a reference for the construction of humanistic nursing practice guidelines for late stroke.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of General Hospital of Southern Theatre Command (YLL[2020]70). All participants provided a written and signed letter of consent to be interviewed.
Consent for Publication
All participants agreed to publish the relevant data anonymously.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Perna R, Harik L. The role of rehabilitation psychology in stroke care described through case examples. Neuro Rehabilit. 2020;46(2):195–204. doi:10.3233/NRE-192970
2. Xiong W, Guo M. Status investigation and analysis of doctors humanistic quality. China Med Herald. 2016;13(5):51–54.
3. Zhang JH, Ren HM, Wang JY, et al. Survey analysis of the current situation of nursing humanistic practice competence. J Nurs Sci. 2017;32(6):11–13. doi:10.3870/j.issn.1001-4152.2017.06.011
4. Li M, Zhu WJ, Luo Q, et al. Psychological experience of humanistic care among medical staff in stroke wards: a qualitative research study conducted in China. Front Psychiatry. 2022;13:791993. doi:10.3389/fpsyt.2022.791993
5. Liu YL, Yang XJ, Hu DY, et al. Research progress of nursing humanistic care standards. Chin J Nurs. 2014;49(12):1500–1505.
6. Han P, Chen XY, Zhang TS, et al. A review of issues related to humanistic care and doctor-patient relationship at home and abroad. Chin Med Ethics. 2013;26(6):768–771.
7. Shang XC, Jin XH, Lin Z, et al. Multi-center survey on humane nursing practice of the domestic hospitals. China Hospital Manage. 2018;38(05):61–63.
8. Min L. Construction of Humanistic Nursing Practice Guidelines in Stroke. Guangdong Pharmaceutical University; 2021. doi:10.27690/d.cnki.ggdyk.2021.000008
9. Guan CY, Zhang FJ, Lv CF, et al. A bibliometric analysis of the current status of nursing humanistic care evaluation research in hospitals in China. J Nurs Sci. 2019;34(03):80–83.
10. Liu M. Handbook of Clinical Evidence-Based Treatment. Neurological Disorders. People’s Health Press; 2008.
11. Fortinsky RH. Family caregiver assessment in primary care: how to strengthen the healthcare triad? J Am Geriatr Soc. 2021;69(2):286–288. doi:10.1111/jgs.16994
12. Ai YT, Hu H, Yang CM, et al. Hindrances of peripherally inserted central catheter care of leukemia patients: a qualitative study. Support Care Cancer. 2021;29(8):4339–4347. doi:10.1007/s00520-020-05941-9
13. Sousa D. Validation in qualitative research: general aspects and specificities of the descriptive phenomenological method. Qual Res Psychol. 2014;11(2):211–227. doi:10.1080/14780887.2013.853855
14. Ju ZX. Quality model nursing service-A new project of harmonious doctor-patient relationship. Chin Health Serv Manage. 2011;S1:48–49.
15. Huang XZ. Reflections on the inheritance of traditional Chinese humanistic care in quality nursing service work. J Nurs Sci. 2015;30(3):47–49. doi:10.3870/hlxzz.2015.03.047
16. Li J. A Study on Functional, Emotional and quality of Life Trajectories and Care Needs of Acute Ischemic Stroke Patients at Different Times. School of Nursing, Second Military Medical University; 2017.
17. Saad M, de Medeiros R, Mosini AC. Are we ready for a true biopsychosocial-spiritual model? The many meanings of “Spiritual”. Medicines. 2017;4(4):79. doi:10.3390/medicines4040079
18. Mahfoodh MAB, Alamoudi MA, Aljedaani MS, et al. The psychosocial needs of families during critical illness. Crit Care Nurs Q. 2021;44(2):268–276. doi:10.1097/CNQ.0000000000000360
19. Wang Y, Liu WL, Liu M. Survey and research on inpatients’ needs for nursing humanistic care. China Med Pharm. 2017;7(17):131–134. doi:10.3969/j.issn.2095-0616.2017.17.039
20. Li X, Lu SL, Guo Z, et al. Clinical application of humanistic care services in the care of conscious patients in ICU. Chongqing Med. 2021;50(S02):397–399.
21. Rejnö ÅC, Berg LK. Communication, the key in creating dignified encounters in unexpected sudden death - with stroke as example. Indian J Palliat Care. 2019;25(1):9–17. doi:10.4103/IJPC.IJPC_117_18
22. Yang LB, Zhou Y, Cui SJ, et al. Survey and analysis of the current situation of humanistic quality of physicians - taking Nanning, Guangxi as an example. Med Philosop. 2014;15(08):75–76, 83. doi:10.3969/j.issn.1002-0772.2014.15.022
23. Li HZ, Yang HH, Sui WJ, et al. Establishing a basic nursing service chain with “patients in mind”. China Nurs Manage. 2010;10(04):24–25. doi:10.3969/j.issn.1672-1756.2010.04.008
24. Li J, Gao LX. Application of humanistic care concept in neurocritical care. Chin J Pract Neurol Disord. 2019;06:692–696. doi:10.12083/SYSJ.2019.06.272
25. Huang JY, Yang XM. Exploring the need for spirituality in holistic care of stroke patients. China Nurs Manage. 2010;10(10):27–30.
26. Shang ZH, Zhu ML, Lin R, et al. A qualitative study on the care needs of acute ischemic stroke patients in different periods. Nurs J Chin People’s Liberat Army. 2018;35(18):19–23. doi:10.3969/j.issn.1008-9993.2018.18.004
27. Widar M, Ek AC, Ahlström G. Caring and uncaring experiences as narrated by persons with long-term pain after a stroke. Scand J Caring Sci. 2007;21(1):41–47. doi:10.1111/j.1471-6712.2007.00449.x
28. Wang X, Li J, Wang C, et al. The effects of mindfulness-based intervention on quality of life and poststroke depression in patients with spontaneous. Int J Geriatr Psychiatry. 2020;35(5):572–580. doi:10.1002/gps.5273
29. Xie GL. Study on the Factors Influencing the Quality of Survival of Stroke Patients and the Evidence of Chinese. Fujian University of Traditional Chinese Medicine; 2018.
30. Zhang XY, Jiang H, Zhou YQ, et al. Status and influencing factors of early recognition and emergency care for stroke. Shanghai Nurs. 2018;18(06):25–28. doi:10.3969/j.issn.1009-8399.2018.06.006
31. Ching S, Chia YC, Chew BN, et al. Knowledge on the action to be taken and recognition of symptoms of stroke in a community: findings from the May Measurement Month 2017 blood pressure screening Programme in Malaysia. BMC Public Health. 2019;19(1):1602. doi:10.1186/s12889-019-7922-7
32. Patel A, Fang J, Gillespie C, et al. Awareness of stroke signs and symptoms and calling 9-1-1 among US adults: National Health Interview Survey, 2009 and 2014. Prev Chronic Dis. 2019;16:E78. doi:10.5888/pcd16.180564
33. Day CB, Bierhals CCBK, Santos NOD, et al. Nursing home care educational intervention for family caregivers of older adults post stroke (SHARE): study protocol for a randomised trial. Trials. 2018;19(1):96. doi:10.1186/s13063-018-2454-5
34. Wang LD, Peng B, Zhang HQ, et al. Summary of the China Stroke Prevention and Control Report 2020. Chin J Cerebrovasc Dis. 2022;19(2):136–144.
35. National Health and Health Commission. Statistical bulletin on the development of health care in China in 2018 [EB/OL]; 2019. Available from: http://www.nhc.gov.cn/guihuaxxs/s10748/201905/9b8d52727cf346049de8acce25ffcbd0.shtml.
36. Chen XY. Study on the Psychological Stress Response of Family Caregivers During Emergency Stroke and Its Influencing Factors. Guangdong Pharmaceutical University; 2018.
37. Li YP, Liu CL, Tu SY, et al. Advances in research on the status of caregiver needs of stroke patients. Chin Nurs Res. 2019;33(4):616–619. doi:10.12102/j.issn.1009-6493.2019.04.016
38. Yang HP, Li J, Chen XL, et al. Psychological status of primary caregivers of hospitalized stroke patients and its correlation with coping styles and social support. J Wenzhou Med Univ. 2016;46(5):372–376. doi:10.3969/j.issn.2095-9400.2016.05.013
39. Wiles R, Pain H, Buckland S, et al. Providing appropriate information to patients and carers following a stroke. J Adv Nurs. 1998;28(4):794–801. doi:10.1046/j.1365-2648.1998.00709.x
40. Krishnan S, Pappadis MR, Weller SC, et al. Needs of stroke survivors as perceived by their caregivers: a scoping review. Am J Phys Med Rehabil. 2017;96(7):487–505. doi:10.1097/PHM.0000000000000717
41. Zhang TY, Liu XH, Fu B, et al. Current status and countermeasures of research on specialized care needs of home stroke caregivers. Chin J Gerontol. 2020;40(15):3354–3357. doi:10.3969/j.issn.1005-9202.2020.15.067
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Situational Factors Associated with Dietary Behavior in Stroke Patients During Rehabilitation: A Qualitative Study Based on the COM-B Model
Zhong W, Pan X, Li J, Zhang Y, Chen L, Sun X, Wang Z, Xu L
Patient Preference and Adherence 2026, 20:593792
Published Date: 9 March 2026