Back to Journals » International Journal of Women's Health » Volume 17
Shared Decision-Making on Fertility Preservation in Reproductive-Aged Women with Gynecological Cancer: A Qualitative Study of Patients’ and Health Care Professionals’ Perspectives
Authors Lin Y ![]() , Ma Q, Wang X, Li X, Jin M, Wei Q, Jiang L
, Ma Q, Wang X, Li X, Jin M, Wei Q, Jiang L
Received 28 August 2025
Accepted for publication 26 November 2025
Published 5 December 2025 Volume 2025:17 Pages 5155—5168
DOI https://doi.org/10.2147/IJWH.S563769
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Yiwen Lin,1,* Qian Ma,2,* Xiaoyu Wang,1 Xianwen Li,3 Min Jin,2 Qing Wei,2 Ling Jiang1
1Department of Nursing, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou, 215000, People’s Republic of China; 2Department of Gynecology, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou, 215000, People’s Republic of China; 3School of Nursing, Nanjing Medical University, Nanjing, 211166, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ling Jiang, Nanjing Medical University Affiliated Suzhou Hospital, Daoqian Campus, No. 26 Daoqian Street, Gusu District, Suzhou, Jiangsu, 215002, People’s Republic of China, Tel +86-13706212877, Email [email protected]
Purpose: Guided by the Ottawa Decision Support Framework (ODSF), this study aimed to explore the experiences, perceived barriers, and support needs of both reproductive-aged women with gynecological cancer and health care professionals (HCPs) during the process of fertility preservation (FP) shared decision-making (SDM), in order to identify alignments and discrepancies between the two groups.
Patients and methods: A descriptive phenomenological qualitative study was conducted using semi-structured interviews with reproductive-aged women diagnosed with gynecological cancers and HCPs from gynecology, oncology, and reproductive medicine specialties. Patients were recruited via hospital records during outpatient visits or hospitalization, and professionals via departmental announcements and invitations. The ODSF informed the development of the interview guide. Data were analyzed using Colaizzi’s descriptive phenomenological method.
Results: A total of 11 reproductive-aged women with gynecological cancer and 12 multidisciplinary HCPs participated in the study. Among the HCPs, 7 were physicians and 5 were nurses. Analysis yielded 35 meaning unites, which were clustered into two main themes: gaps and fragmentation in meeting decisional needs and facilitators of high-quality fertility preservation decision support.
Conclusion: This study suggests that FP SDM among reproductive-aged women with gynecological cancer in China may be influenced by multiple challenges, including limited and untimely information, fragmented referral mechanisms, psychological distress, financial concerns, and sociocultural factors. Multidisciplinary team involvement, nursing support, and culturally adapted decision aids may help enhance patient participation, support preference-sensitive decision-making, and reduce decisional conflict. These findings indicate that integrating structured counseling processes, optimizing multidisciplinary pathways, and developing personalized, culturally sensitive decision aids may contribute to more patient-centered fertility care.
Keywords: fertility preservation, shared decision-making, gynecological cancer, qualitative research, Ottawa decision support framework
Introduction
Gynecological cancers, encompassing malignancies of the cervix, endometrium, ovaries, vulva, and vagina, are among the most common cancers affecting women worldwide. According to the World Health Organization (WHO), women of reproductive age are defined as those aged 15 to 49 years.1 Based on data from GLOBOCAN 2022, approximately 1.47 million women were newly diagnosed with gynecological cancers globally, of which an estimated 20.4% occurred among women of reproductive age.2 Among these, cervical cancer accounted for approximately 61% of all gynecological malignancies, followed by ovarian cancer, which accounted for 22%.2 Evidence indicated advances in early detection and oncologic therapies play a crucial role in improving survival outcomes among affected women.3,4 However, life-saving interventions such as chemotherapy, radiotherapy, and radical surgeries are often gonadotoxic, leading to temporary or permanent infertility.5 For reproductive-aged women, cancer therefore presents not only a threat to survival but also the potential loss of biological motherhood, both short- and long-term adverse psychological outcomes, including depression, anxiety, and impaired quality of life.6
Fertility preservation (FP), a set of medical interventions aimed at safeguarding reproductive potential before cancer treatment, has emerged as a critical aspect of holistic oncologic care. Technologies such as oocyte and embryo cryopreservation are now considered standard practice by major professional organizations, including the American Society of Clinical Oncology (ASCO)5 and the European Society of Human Reproduction and Embryology (ESHRE),7 with similar guidance issued in China.8,9 However, FP in gynecological cancer is generally indicated for reproductive-aged patients with early-stage disease who express a desire for future childbearing, whereas patients with advanced disease or requiring immediate treatment are typically not suitable candidates.10 Despite the availability of mature FP techniques and strong clinical guidelines recommending that patients desiring FP be referred to reproductive specialists within 24 hours of diagnosis for comprehensive counseling—including evaluation of cancer treatment plans, assessment of infertility risks, and discussion of appropriate FP options through multidisciplinary collaboration involving oncology, reproductive medicine, nursing, psychology, genetics, law, and ethics—the actual provision and uptake of such counseling remain suboptimal, with many patients not receiving timely or adequate information about FP.5,7,11 In the United States, fewer than 30% of cancer patients reported receiving FP counseling.12 Similarly, in Canada, only about 5–24% of patients received such counseling prior to cancer treatment.13 Moreover, studies conducted in the United States and the United Kingdom found that 30–60% of reproductive-aged cancer survivors reported not receiving adequate information about FP.14 These findings suggest that many patients have unmet decisional needs, including insufficient information and guidance for making informed FP choices.12–14
The gap between guideline recommendations and actual clinical uptake suggests that FP decision-making is influenced by multiple institutional, financial, and patient-level factors.15 In the Chinese context, FP procedures such as ovarian stimulation, oocyte or embryo cryopreservation, and long-term storage are generally not covered by national medical insurance, requiring patients to self-pay.16 Direct medical costs for a single cycle of assisted reproductive treatment range from approximately 25,857 to 27,166 China yuan (CNY) for conventional in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI).17 Since July 1, 2023, Beijing has incorporated 16 therapeutic assisted reproductive technology (ART) procedures in the municipal medical insurance reimbursement system, potentially alleviating some of these financial barriers.18 From the provider perspective, clinicians often report insufficient training or discomfort initiating FP discussions, particularly when prognosis is uncertain.19,20 Oncologists may also underestimate patients’ fertility concerns or assume that sociocultural or marital factors preclude the need for FP.21 These decisional challenges underscore the complexity of the FP decision-making process, which is often time-sensitive, emotionally charged, and medically complex.6,13 Shared decision-making (SDM), a collaborative process in which patients and HCPs jointly consider medical evidence alongside patient preferences, is essential in this context.22 However, implementing effective SDM in FP discussions remains difficult due to provider- and system-level barriers, as well as patient-related factors.23
Research exploring SDM in FP among reproductive-aged women with gynecological cancer is still emerging. Some studies have highlighted the value of trust, timing, and tailored information in fostering effective communication between patients and clinicians,24 and emphasized the need for integrated care pathways and interdisciplinary collaboration to support timely and informed choices.25 However, most prior studies have examined either patients or HCPs in isolation,21,26 with limited exploration of how multidisciplinary teams (MDT) facilitate FP SDM in real-world clinical contexts.13,27 In practice, challenges such as incomplete MDT mechanisms, unclear nurse roles, delays in referral and information transfer, and professional differences across disciplines can hinder patients’ access to timely and systematic decision support.28,29
In contrast, the present study explored both patients’ and HCPs’ perspectives to identify alignments and discrepancies in their experiences and perceived barriers during FP discussions. A multidisciplinary lens, incorporating views from gynecology, oncology, and reproductive medicine (ie, the Reproductive Center specializing in fertility preservation and assisted reproductive technology), was adopted to provide a comprehensive understanding of the structural and interpersonal dynamics that influence FP decisions. This dual-perspective design provides a nuanced understanding of communication dynamics within MDT and highlights key contextual factors—such as sociocultural values and system-level constraints—that shape FP SDM in China. These insights can inform the development of culturally tailored, evidence-based decision support interventions.
Theoretical Framework
The Ottawa Decision Support Framework (ODSF), developed by O’Connor et al in 1988, is an evidence-based, practical, and value-neutral framework designed to support individuals facing health or social decisions.30 The framework comprises three core components: (1) assessment of decisional needs, including evaluation of decision stage, knowledge gaps, and decisional conflict; (2) provision of tailored decision supportaimed at clarifying values, addressing barriers, and improving knowledge; and (3) evaluation of decision process and quality, focusing on value-concordance, decision delay, and regret.31 Given the multidimensional nature of FP decision-making, the ODSF provides a robust theoretical lens for analyzing decisional needs and developing strategies that promote high-quality, patient-centered choices.31 This framework highlights the importance of understanding system-, provider-, and patient-level barriers, which are particularly relevant in the context of FP among women with gynecological cancer.32 The conceptual structure of this study, guided by the ODSF, is illustrated in Figure 1, which outlines the interrelationships among decisional needs, decision support, and decision quality evaluation in FP SDM.
 |
Figure 1 Theoretical framework based on the Ottawa Decision Support Framework. |
Methods
Study Design
This study employed a descriptive phenomenological qualitative design based on Husserlian philosophy to explore the perspectives and experiences of reproductive-aged women with gynecological cancer and HCPs regarding SDM in FP. This approach was chosen to capture participants’ and HCPs’ lived experiences and the meanings they ascribe to FP SDM in real clinical contexts.33 The core epistemological principle of Husserlian phenomenology—phenomenological reduction—was followed, whereby researchers bracketed their preconceptions and assumptions to faithfully represent participants’ subjective experiences.34 The study was designed and reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Supplement 2) to enhance methodological rigor and transparency.35
Settings
This study was conducted at the Department of Gynecological Oncology and Reproductive Medicine at Suzhou Municipal Hospital in China, which houses the National Key Laboratory of Reproductive Medicine. The center specializes in gynecological malignancies and advanced reproductive medicine, providing integrated cancer treatment and FP services supported by state-of-the-art IVF laboratories and multidisciplinary tumour boards.
Since 2023, the Reproductive and Genetics Center has established a Fertility Monitoring, Assessment, and Preservation Multidisciplinary Joint Clinic. Unlike routine tumour boards that function as internal case discussions, this clinic is a patient-facing, appointment-based service where gynecologists, oncologists, reproductive specialists, and nurses offer coordinated consultations in a single visit. This clinic formed an important part of the clinical context for the present study.
Participants
Participants included reproductive-aged women with gynecological cancer and HCPs involved in FP care. Purposive sampling with maximum variation was used to ensure diversity in participants’ demographic and clinical characteristics, as well as HCPs’ professional backgrounds and practice experience. Potential patient participants were identified through hospital records and approached during outpatient visits or hospitalization, while HCPs were recruited through departmental announcements and personal invitations and contacted directly by the research team.
For patients, inclusion criteria were: (1) women aged 18–45 years; (2) pathologically diagnosed with a gynecological malignancy (including cervical, ovarian, endometrial, vulvar, or vaginal cancer) or borderline ovarian tumor; (3) recommended to receive potentially gonadotoxic treatments such as surgery, radiotherapy, or chemotherapy; (4) able to read and understand Chinese; and (5) voluntarily consented to participate. Exclusion criteria were: (1) prior history of FP interventions; (2) advanced-stage disease without opportunity for FP; (3) currently pregnant; (4) severe psychiatric illness or cognitive impairment affecting ability to provide informed consent; and (5) poor physical condition preventing participation in interviews. Patients were not required to have received FP counselling prior to the interview, as the study aimed to explore their subjective experiences, information needs, and SDM difficulties at the early stage, when they first learn that upcoming cancer treatment may affect fertility. Patients who were considering or planning to undergo FP following this diagnosis were eligible and included.
For HCPs, inclusion criteria were: (1) physicians or nurses registered in gynecology, gynecologic oncology, reproductive medicine, or related specialties; (2) ≥3 years of clinical experience; (3) involvement in cancer care or fertility services for reproductive-aged women; and (4) willingness and ability to participate with informed consent. Exclusion criteria were (1) currently not engaged in frontline clinical practice (eg, on training, research-only positions, or administrative leave); and (2) less than three years of post-qualification clinical experience.
Materials
Sociodemographic Data
Sociodemographic data for patients were obtained from hospital records and included age, marital status, education level, employment status, cancer diagnosis, treatment received, and number of children; no additional self-reported questionnaire was used.
For HCPs, data were collected from departmental records and included gender, age, marital status, education level, occupation, years of work experience, career level, and department affiliation.
Interview Guide
A semi-structured interview guide (Supplement 1) was developed based on the ODSF and previous literature. It was tailored for both patients and HCPs to explore experiences, perceptions, SDM processes, challenges, and support needs related to fertility preservation. For patients, the guide covered awareness of fertility risks, understanding of FP options, factors influencing decisions, sources of support, challenges encountered, coping strategies, decisions made, reflections, and perceived needs for decision support. For HCPs, the guide explored experiences in discussing FP with patients, perceived barriers and facilitators in SDM, interprofessional collaboration, and views on strategies to improve FP decision support. The guide was piloted with two patients and one HCP to refine clarity and flow of questions.
Data Collection
Face-to-face interviews were conducted in Chinese between June and July 2025 by two trained female researchers: a postgraduate nursing student and a head nurse who holds a postgraduate degree and has ten years of clinical experience, both trained in qualitative research. Interviews were conducted in a quiet, private consultation room to ensure comfort and confidentiality. Interviews were conducted at times and locations convenient for participants, usually in private offices or hospital meeting rooms.
All participants provided written informed consent, which included permission for the use of anonymized quotations in publications. Before each interview, researchers assessed participants’ emotional readiness and informed them that the discussion might involve sensitive topics related to fertility loss or missed fertility-preservation opportunities. Participants were reminded that they could pause or withdraw from the interview at any time without any impact on their clinical care. With participants’ permission, each interview lasted 20–45 minutes and was audio-recorded with permission. Field notes were kept to document non-verbal cues (eg, tone, gestures, facial expressions) and contextual observations. During the interviews, researchers closely monitored participants’ verbal and non-verbal expressions and provided empathetic, supportive communication when signs of discomfort were observed. Interviews were paused if participants showed emotional distress, and their willingness to continue was reassessed. After each interview, a brief debriefing session was conducted, allowing participants to express remaining concerns. Recruitment continued until data saturation was reached, defined as the point where no new themes emerged. All invited participants agreed to participate, and no one withdrew from the study.
Data Analysis
All interviews were conducted and transcribed verbatim in Chinese within 24 hours of data collection. Transcripts were checked against recordings for accuracy. Selected quotes were translated into English and back-translated to ensure fidelity of meaning.
Analysis followed Colaizzi’s descriptive phenomenological method, supported by NVivo 20.0 software: (1) Familiarization - Each transcript was read repeatedly to gain a holistic understanding. (2) Extraction of significant statements - Meaningful phrases directly related to FP decision-making and SDM were identified. (3) Formulation of meanings - Underlying meanings were derived from these statements. (4) Clustering of themes - Formulated meanings were grouped into clusters, categories, and overarching themes. (5) Exhaustive description - A comprehensive description of participants’ lived experiences was generated. (6) Fundamental structure - Essential structures of the phenomenon were distilled. (7) Validation - Themes and interpretations were discussed within the research team, and a subset of participants was invited to provide member checking to enhance credibility. To ensure rigor, two researchers (LYW and MQ) independently coded all interview transcripts, and discrepancies were resolved through discussion. The final coding framework was reviewed by the corresponding author (JL) to ensure consistency and accuracy. Reflexive memos were kept to account for researcher positionality and preconceptions.
Ethical Considerations
This study was approved by the Ethics Committee of Suzhou Municipal Hospital (Approval No. K-2025-186-K01). Written informed consent was obtained from all participants prior to data collection. Confidentiality was maintained by anonymizing transcripts, and only the research team had access to the data. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Result
A total of 11 female patients with gynecological cancer were interviewed, aged between 24 and 44 years. Twelve healthcare professionals participated in this study, comprising 7 physicians and 5 nurses. Participants were assigned identification numbers for use in quotations: patient (P) and healthcare professional (H). The characteristics of the participants are summarized in Tables 1 and 2.
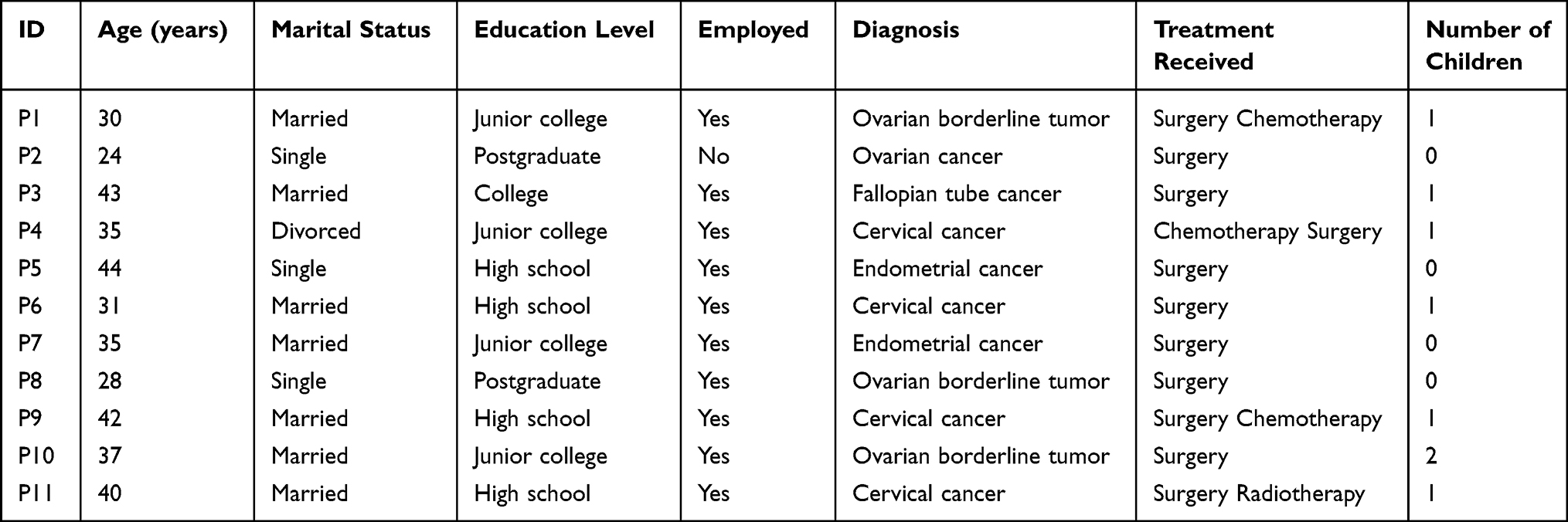 |
Table 1 Demographic and Clinical Information of the Patients (n=11) |
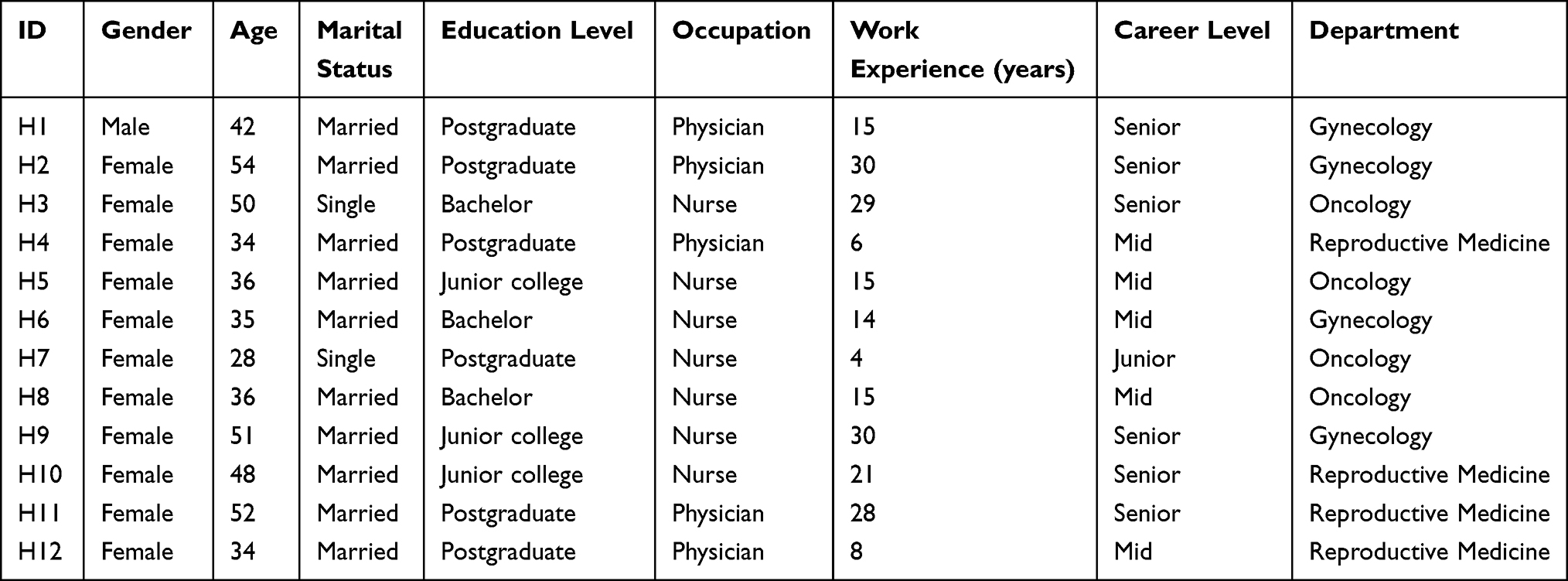 |
Table 2 Demographic Characteristics of Health Care Professionals (n=12) |
Using Colaizzi’s seven-step method, 35 meaning unites were extracted and transformed into formulated meanings, which were subsequently clustered into two themes and seven subthemes.
Gaps and Fragmentation in Meeting Decisional Needs
Patients faced notable gaps and fragmentation in the fulfillment of their decisional needs related to FP. These encompassed missed opportunities for SDM due to persistent information gaps, disrupted or absent shared decision-making processes, passive patient roles influenced by external factors, contextual limitations, and value conflicts and social pressures in FP decision-making.
Missed Opportunities for SDM Due to Information Gaps
Many patients reported that they were not aware of FP options prior to treatment. Only a minority indicated that they became aware of the possibility of using assisted reproductive technologies for FP after treatment had already begun. Patients in these situations described having missed the opportunity to consider or pursue preservation and regret or concern about their future reproductive potential. They noted that they had little or no opportunity to participate in SDM regarding FP.
P1: I didn’t know about fertility preservation until after my first chemotherapy, and I don’t know if it will affect me from having children in the future.
P9: The doctor just mentioned that it might affect my fertility, but I already have a child so I don’t care.
Information gaps were also evident among healthcare professionals, particularly nurses. Most nurses stated that they lacked training regarding FP procedures, assessment, and referral processes, and noted the absence of standardized tools or pathways in clinical practice.
H8 (nurse): There is no standard criteria for assessing whether a patient needs fertility preservation, we mainly look at her age and condition, right? Right, and see if she has ever had children.
H5 (nurse): It’s just that many people don’t know much about this concept, even young patients don’t know much about it. Forget about patients, in fact, many of our medical staff don’t know enough about fertility preservation.
HCPs described that these information gaps translated into differences in how physicians and nurses participated in FP-related discussions. Physicians typically introduced potential fertility impacts when explaining treatment plans, whereas nurses were generally less involved and often provided information only when patients actively sought it.
H2 (physician): When explaining the treatment plan to patients, I briefly mention that it might affect their fertility. For those who have reproductive intentions, I may recommend seeing a reproductive specialist
H10 (nurse): If patients ask, we try to answer, but we usually don’t know the details, so we tell them to ask the doctor again.
Passive Patient Role and Reliance on External Influencers
Many patients assumed a passive role in SDM, deferring choices to physicians. Cultural and social norms emphasizing deference to medical authority further reduced patients’ willingness to question recommendations, limiting the opportunities for SDM.
P7: The doctor said that my disease was serious, and suggested that I should have my uterus removed. My husband and I had no children, but we thought we should listen to the doctor and save my life.
For some, decision momentum was shaped by family members, informal patient networks, or recommendations from friends with similar experiences rather than professional guidance.
P1: I just did a little research on Xiaohongshu. Then I had a patient here who went there and said it was good, so I just went to do it[fertility preservation].
P5: Several of my colleagues at the company are in the same situation as me. Given my age, I feel that fertility preservation isn’t necessary anymore.
Contextual Factors Shaping and Restricting Choices
About half of the patients reported fear of undergoing additional procedures related to FP, such as oocyte retrieval, perceiving them as physically risky or burdensome on top of their cancer treatment.
P2: I just don’t want to go under the knife again. As for egg freezing, it requires those ovulation-stimulation injections. Honestly, even looking at those needles scares me a little.
H2: Yeah, because most of them are still confused about having an operation, and they’re worried.
For those with limited financial resources, FP was often perceived as a “luxury option” that had to be abandoned due to affordability concerns.
P6: There is some financial pressure, but I just had a baby and I’m not going to have any more.
Most patients often had to start cancer treatment without delay, particularly when surgery, radiotherapy, or chemotherapy schedules were time-sensitive. This limited the time available for considering FP and restricted their practical options.
P2: When I was hospitalized, my sister urged me to make this decision before chemotherapy. She insisted we should act fast, saying it would be better if I started treatment immediately after discharge. That afternoon, he[doctor] came to me at noon and gave me his advice. After doing some research myself, I made the decision that very evening.
Most HCPs reported that heavy workloads limited the time available to discuss FP with patients. They also indicated that the hospital lacked well-established referral systems, and that the absence of institutional leadership and policy support further constrained their ability to address patients’ decisional needs regarding FP.
H3: Everyone is extremely busy every day, just trying to keep up with routine tasks. If you want to take on this kind of work, it would only be possible when there’s some relief in human resources and other areas—then people might actually have the bandwidth to focus on it. Yeah, that’s right.
Value Conflicts and Social Pressures in FP SDM
Variation in value considerations was reported across patient subgroups. Younger and nulliparous patients frequently expressed concerns about future fertility and reported actively seeking FP options. Patients who already had children did not uniformly dismiss fertility concerns; for a few, changes in relationship status or future life plans led them to reconsider reproductive intentions. In contrast, other patients with children indicated that FP was unnecessary and prioritized cancer treatment or family responsibilities.
P4: I was thinking about preserving my fertility. I already have one child, but since I’m single now, what if I want to have another one in the future?
P3: My husband and I didn’t think about fertility preservation. I already have a daughter, so I felt it wasn’t necessary. I was just focused on treating the disease.
In traditional contexts, unmarried women pursuing FP were sometimes perceived as “improper”, exposing them to social stigma. Even married women occasionally avoided local hospitals due to fear that family or friends might learn of their decision. Such concerns about social judgment led a minority of patients to bypass local services or forgo FP entirely.
P1: I’m working here, and my husband is back in our hometown. I want to do this procedure here, but I don’t want anyone to know. If I went to a hospital in my hometown, people would find out.
However, the majority of HCPs recognized that such dilemmas were deeply personal and could not be resolved by medical advice alone. A few patients met medical criteria for FP but chose not to pursue it due to personal or ethical beliefs.
H5: There is a young patient in her early twenties. We strongly recommend fertility preservation for her, but she feels that since she is single and might still be able to conceive naturally in the future, she does not want to take the risk. Unfortunately, there is nothing we can do to change her decision.
Facilitators of High-Quality Fertility Preservation Decision Support
A subset of patients reported experiencing high-quality FP decision support. Key facilitators of such support included coordinated MDT involvement, structured decision tools aligned with patients’ needs, and a supportive health system and policy environment.
Multidisciplinary Team Clinic Engagement
From the patients’ perspective, coordinated input from gynecologists, reproductive specialists, and nurses supported their FP SDM. MDT clinics facilitated integrated consultations and clarified available options, but high fees, repeated travel, and the absence of a formal referral system limited access.
P11: I think this clinic is really good and necessary. Although it costs 200 RMB, I feel it’s worth it. The only inconvenience is the time, as I have to take time off work to come.
From the physicians’ perspective, awareness of the MDT clinic was limited. Many doctors were not familiar with its existence, and only a small number of patients actually registered for the service. There is a gap between potential benefits and actual utilization.
H4: Not many patients come from the gynecology department, and I feel that many healthcare professionals don’t take it [FP] very seriously. After all, here people still generally think that for this type of cancer, saving life comes first.
Participants’ Expectations for Decision Aids
Patients expressed that having structured decision aids would help them better understand their options, feel more confident in making decisions, and reduce the time and effort spent searching for reliable information.
H9: I think such a tool would be really useful. That way, I wouldn’t have to search for information everywhere and worry about encountering incorrect or misleading sources.
Clinicians expressed that, if available, decision aids could standardize information, guide counseling, reduce patients’ uncertainty, and improve communication efficiency. They also emphasized the need to present both risks and benefits to ensure informed SDM and minimize potential disputes.
H1: If such a decision aid were available, it would benefit both us and the patients. But the risks also need to be communicated—you can’t only talk about the benefits, because if a risk occurs later and the patient didn’t accept it, it could cause problems. Without adequate disclosure and proper documentation, it might still be problematic and could lead to disputes.
Supportive Policy and Health System Environment
HCPs emphasized the need for supportive policies and a well-organized health system to facilitate FP. Participants highlighted that strong leadership, better coordination between departments, and institutional changes—such as clearer referral processes and routinely discussing FP in cancer care—were key to improving access and ensuring consistent support for patients.
H5: In our gynecology department, there is really nothing in place. The lack of attention is closely related to the doctors—they haven’t embraced this concept, and it’s hard for us to take the lead. Many team leaders came up through older training systems, and their perspectives are already fixed. Even if you know the literature, they may not have the capacity to adopt it.
Discussion
This study explored the perspectives of both patients and HCPs on FP shared decision-making in reproductive-aged women with gynecological cancer, guided by the ODSF. Our findings highlight substantial gaps between the growing recognition of SDM and its implementation in clinical practice. Despite increasing awareness of patient-centered care, FP decisions are often fragmented, delayed, and shaped by systemic, cultural, and psychosocial constraints.36
Lack of Timely and Individualized Information Support
A prominent barrier identified was the lack of timely and individualized information support. Many patients reported not receiving any fertility preservation–related information prior to initiating cancer treatment, which may restricted their ability to make informed choices that balance survival with fertility goals.37 This reflects a fundamental tension between the efficiency-oriented nature of cancer treatment and the patient-centered philosophy of care. As a result, FP discussions frequently shifted from collaborative deliberation to procedural notification, leaving patients in a passive role reliant on physicians, family members, or peers for guidance.38 However, in China, additional socio-cultural factors intensify this challenge. In a context where physician authority and family-centered SDM are deeply rooted, patients’ voices were often marginalized. Cultural values such as family harmony and filial piety emphasize the family’s deep involvement in medical SDM, often placing collective decisions above individual autonomy.39 Ritual governance further explains the cultural roots of power imbalances in healthcare relationships, where patients commonly defer to physician authority, and nurses’ roles in SDM are often limited.40 Medical paternalism, coupled with familial prioritization, constrained women’s autonomy, with patients opting for silence or compliance to maintain harmony within the family and the physician–patient relationship. Such dynamics contrast with many Western contexts, where individual autonomy is typically prioritized, open communication is encouraged, and patient empowerment is emphasized, with patient voices actively solicited in SDM processes.41
Influence of Fertility Intentions and Psychological Distress
Fertility intention may be a key determinant shaping FP SDM. Women with strong fertility desires actively sought information and reported profound regret when opportunities were missed.42 The desire for more children at the time of cancer diagnosis was associated with the experience of higher regret in a sample of women at reproductive age with gynecologic cancer.43 In contrast, those with weaker fertility preferences tended to prioritize cancer treatment over FP, even when clinically eligible. For instance, in a qualitative study among reproductive-aged women with cancer in Greece, a patient with an existing family described that despite formerly desiring more children, the urgency to commence chemotherapy immediately superseded her fertility considerations.44 Importantly, many patients encountered FP counseling while still in shock post-diagnosis, with psychological distress—such as anxiety, fear, and uncertainty—suppressing fertility discussions and delaying the expression of reproductive goals.45
Financial Barriers and Health System Disparities
Economic considerations may represented a critical barrier. Consistent with prior studies, financial concerns strongly influenced FP SDM.46 However, our study further revealed that perceived financial toxicity—patients’ anticipatory fear of unaffordable costs—often outweighed actual financial burden. Misconceptions arose from fragmented information and the widespread assumption of out-of-pocket payment, despite partial insurance coverage for certain procedures. Without transparent financial counseling, patients defaulted to self-limiting decisions, prematurely abandoning FP options, consistent with prior findings that financial toxicity leads to treatment non-adherence and compromised care access.47 In China, the inclusion of assisted ART services in medical insurance has entered a preliminary exploratory stage. Although substantial progress has been made under central policy guidance, some provincial pilot programs have incorporated selected ART into local reimbursement schemes, yet significant regional disparities remain in coverage, reimbursement rates, and payment ceilings.48 Moreover, most local policies neither specify necessary medical indications nor set age limits for ART, raising concerns about potential misuse of these technologies for non-medical purposes.49 To further improve reproductive health services, efforts should focus on expanding public–private partnerships, enhancing equitable access across regions, and addressing cultural stigma surrounding infertility.50
Facilitators of SDM: MDT Involvement and Nursing Roles
Beyond the identified barriers, several facilitators were recognized that could enhance patients’ engagement in SDM for FP. MDT involvement was perceived as potentially crucial for supporting patients in making informed, preference-sensitive decisions, consistent with international guidelines.7,51 However, implementation remains insufficient. This is partly due to the divergent philosophies between oncology, focused on survival, and reproductive medicine, focused on fertility and quality of life.52 In addition, more recent research indicates that only a small proportion of reproductive-age women with newly diagnosed gynecologic cancers are referred to fertility specialists, highlighting that the lack of structured referral mechanisms remains a major barrier to FP.53 Moreover, the absence of performance incentives and the limited awareness of healthcare providers regarding FP further hinder its integration into routine oncology practice, compounding the challenges in delivering comprehensive care to reproductive-age cancer patients.54 In many countries, dedicated fertility navigators help coordinate consultations, provide tailored information, and support patients throughout the SDM process.55 In China, however, such a role has not yet been established, leaving patients without consistent guidance. Within this context, nurses play a pivotal mediating role by providing information, emotional support, and guidance, helping patients cope with decisional anxiety, clarify their values, and actively participate in decision-making.56 Particularly during the initial diagnosis stage, nurses are responsible for preliminary screening, referral, and information delivery, serving a critical function that empowers patients, reduces decisional conflict, and minimizes subsequent regret.19
Need for Culturally Adapted Decision Aids
Patients also expressed the need for culturally adapted decision aids, which have been shown to improve knowledge, reduce decisional conflict, and promote active participation.57 Currently, information is often delivered primarily through verbal explanations, leading to misunderstanding, cognitive overload, or over-reliance on clinicians’ recommendations.58 Guidelines7,51 recommend providing decision aids early—at cancer diagnosis or treatment planning—to help patients understand options, weigh pros and cons, and enhance decision-making capacity. In China, Yuan59 developed decision aids for reproductive-aged women with cancer, demonstrating clinical applicability, though limitations remain, such as lack of cancer-type differentiation. Future development should focus on personalized, disease-specific, culturally adapted tools that accommodate patients’ educational backgrounds, cultural practices, and information preferences, ensuring both scientific rigor and usability.
Limitations and Strengths
This study was conducted at a single tertiary hospital in eastern China with relatively well-developed resources, including a Fertility Monitoring, Assessment, and Preservation Joint Clinic and multidisciplinary collaboration. Therefore, the experiences of patients and HCPs may primarily reflect this institutional context and may not fully represent other clinical settings with different resource levels. Although psychologists were not included, some nurses hold qualifications as psychological counselors, providing partial insight into psychosocial aspects of FP SDM. Despite efforts to ensure rigor, the influence of the researchers cannot be entirely eliminated, as prior assumptions and professional background may have affected data collection and analysis.
Despite these limitations, the study has notable strengths. It focuses on reproductive-aged women with gynecological cancers and incorporates perspectives from a multidisciplinary group of healthcare providers, reflecting real-world FP collaboration. The study systematically identified decisional needs and highlighted the need for culturally adapted decision aids. Although some barriers resemble those reported internationally, our findings may provide context-specific insights into FP decision-making in China, suggesting persistent systemic gaps, absence of fertility navigators, limited culturally adapted resources, and the pivotal role of nurses in supporting patients, especially in physician-led settings. These locally grounded insights may inform improvements in FP care. Future research should consider integrating psychological professionals, operationalizing MDT models, and conducting cross-cultural studies to understand contextual influences on SDM.
Conclusion
This study highlights the complex interplay of clinical, cultural, and systemic factors influencing fertility preservation (FP) decision-making among reproductive-aged women with gynecological cancer in China. Guided by the ODSF, our findings reveal significant gaps between the ideal of SDM and current clinical practice. Barriers such as limited and untimely information, fragmented referral mechanisms, psychological distress, financial concerns, and entrenched sociocultural norms restricted patients’ autonomy and often relegated them to passive roles. Conversely, facilitators including multidisciplinary collaboration, nursing involvement, and the use of culturally adapted decision aids demonstrate potential to enhance informed, preference-sensitive decisions and reduce decisional conflict. These insights underscore the urgent need for structured FP counseling, equitable financial policies, and the integration of SDM frameworks into oncology practice. Future work should focus on developing personalized, context-specific decision aids, strengthening multidisciplinary pathways, and conducting cross-cultural research to better understand and address disparities in FP SDM. Ultimately, empowering women to participate actively in choices that balance survival with fertility goals is essential to advancing both reproductive health equity and patient-centered cancer care.
Acknowledgments
We sincerely thank all participants for sharing their experiences and perspectives.
Funding
This research was supported by the Suzhou Municipal Health Commission, Key Project of Science and Technology Program (Grant No. ZDXM2024011).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Women of reproductive age (15-49 years) population (thousands). Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/women-of-reproductive-age-%2815-49-years%29-population-%28thousands%29?utm_source=chatgpt.com.
2. Cancer today. Available from: https://gco.iarc.who.int/today/.
3. Tran C, Diaz-Ayllon H, Abulez D, et al. Gynecologic cancer screening and prevention: state of the science and practice. Curr Treat Options Oncol. 2025;26:167–178. doi:10.1007/s11864-025-01301-z
4. Zhao M, Teng X-M, Yan Q, et al. Risk assessment and fertility counseling for hereditary gynecological cancer syndromes. Cancer Med. 2025;14:e71206. doi:10.1002/cam4.71206
5. Su HI, Lacchetti C, Letourneau J, et al. Fertility preservation in people with cancer: ASCO guideline update. J Clin Oncol. 2025;43:1488–1515. doi:10.1200/JCO-24-02782
6. Stroeken Y, Hendriks F, Beltman J, et al. Quality of life and psychological distress related to fertility and pregnancy in AYAs treated for gynecological cancer: a systematic review. Cancers. 2024;16:3456. doi:10.3390/cancers16203456
7. Anderson RA, Amant F, Braat D, ESHRE Guideline Group on Female Fertility Preservation, et al. ESHRE guideline: female fertility preservation. Hum Reprod Open. 2020;2020:hoaa052. doi:10.1093/hropen/hoaa052
8. Chinese Society of Reproductive Medicine. Chinese expert consensus on fertility preservation. J Reproduct Med. 2021;30:1129–1134.
9. Fertility Preservation Committee of Chinese Maternal and Child Association. Chinese expert consensus on clinical practice of female fertility preservation. Chin J Reprod Contracep. 2021;41:383–391.
10. Liang X, Fang C, Li J, et al. Expert consensus on fertility preservation for female cancer patients in China. Chin J Clin Oncol. 2020;47:217–221.
11. Muñoz M, Santaballa A, Seguí MA, et al. SEOM clinical guideline of fertility preservation and reproduction in cancer patients (2016). Clin Transl Oncol. 2016;18:1229–1236. doi:10.1007/s12094-016-1587-9
12. Goodman LR, Balthazar U, Kim J, et al. Trends of socioeconomic disparities in referral patterns for fertility preservation consultation. Hum Reprod. 2012;27:2076–2081. doi:10.1093/humrep/des133
13. Yee S. Factors associated with the receipt of fertility preservation services along the decision-making pathway in young Canadian female cancer patients. J Assist Reprod Genet. 2016;33:265–280. doi:10.1007/s10815-015-0608-x
14. Shnorhavorian M, Harlan LC, Smith AW, et al. Fertility preservation knowledge, counseling, and actions among adolescent and young adult patients with cancer: a population-based study. Cancer. 2015;121:3499–3506. doi:10.1002/cncr.29328
15. Polavarapu M, Arsene C, Singh S, et al. Fertility preservation among patients with breast cancer: a qualitative study of patient and healthcare provider perspectives. Cureus. 2025. doi:10.7759/cureus.89704
16. Wang Y, Ma X, Diao F, et al. International experiences and enlightenments of assisted reproductive technology covered in medical insurance reimbursement. Soft Science of Health. 2025;39:89–94.
17. Qiao J, Wang Y, Zhang Q, et al. A prospective cohort analysis of the economic burden among 174 patients undergoing In Vitro Fertilization–Embryo Transfer (IVF-ET). Mater Child Health Care China. 2022;37:1845–1848.
18. Beijing Municipal Medical Insurance Bureau619_3721533.html. Beijing Municipal Human Resources and Social Security Bureau. Notice on incorporating 16 therapeutic assisted reproductive technology procedures into medical insurance and work injury insurance reimbursement. 2023. Available from: https://ybj.beijing.gov.cn/zwgk/2024zcwj/202406/t20240619_3721533.html.
19. Güngör Satılmış İ, Coşkuner Potur D, Mecdi Kaydırak M, Akın Eroğlu S. Fertility preservation in patients with cancer: nurses’ views, experiences, and perceptions of benefits and barriers. Oncol Nurs Forum. 2023;51:71–79. doi:10.1188/24.ONF.71-79
20. Kasaven LS, Mitra A, Chawla M, et al. A cross-sectional survey of healthcare professionals’ knowledge, attitude and current behaviours towards female fertility preservation services within the UK. Cancers. 2024;16:2649. doi:10.3390/cancers16152649
21. Wang L, Li J, Lu T, et al. Perspectives and clinical practices on fertility preservation for young hematologic patients: a qualitative study of healthcare providers across multiple hospitals in China. J Assist Reprod Genet. 2025;42:1415–1423. doi:10.1007/s10815-024-03380-7
22. Carmona C, Crutwell J, Burnham M, et al. Shared decision-making: summary of NICE guidance. BMJ. 2021:n1430. doi: 10.1136/bmj.n1430
23. Daly C, Micic S, Facey M, et al. A review of factors affecting patient fertility preservation discussions & decision-making from the perspectives of patients and providers. Eur J Cancer Care. 2019;28:e12945.
24. Jones G, Hughes J, Mahmoodi N, et al. What factors hinder the decision-making process for women with cancer and contemplating fertility preservation treatment? Hum Reprod Update. 2017;23:433–457. doi:10.1093/humupd/dmx009
25. Crespi C, Adams L, Gray TF, et al. An integrative review of the role of nurses in fertility preservation for adolescents and young adults with cancer. Oncol Nurs Forum. 2021;48:491–505. doi:10.1188/21.ONF.491-505
26. Sun M, Liu C, Zhang P, et al. Perspectives and needs for fertility preservation decision-making in childbearing-age patients with breast cancer: a qualitative study. Asia-pac J Oncol Nurs. 2024;11:100548. doi:10.1016/j.apjon.2024.100548
27. Gwede CK, Vadaparampil ST, Hoffe S, et al. The role of radiation oncologists and discussion of fertility preservation in young cancer patients. Pract Radiat Oncol. 2012;2:242–247. doi:10.1016/j.prro.2011.12.001
28. Wang M, Zhu L, Xiong H, et al. Lack of knowledge, the main stumbling block of fertility preservation promotion in China. J Cancer Educ. 2022;37:739–747. doi:10.1007/s13187-020-01875-2
29. Yang E, Dornisch A, Nerb L, et al. A multicomponent telehealth intervention to improve oncofertility care delivery among young cancer patients: a pilot study. J Adolesc Young Adult Oncol. 2023;12:241–249. doi:10.1089/jayao.2021.0224
30. O’Connor AM, Tugwell P, Wells GA, et al. A decision aid for women considering hormone therapy after menopause: decision support framework and evaluation. Patient Educ Couns. 1998;33:267–279. doi:10.1016/S0738-3991(98)00026-3
31. Stacey D, Légaré F, Boland L, et al. 20th anniversary Ottawa decision support framework: part 3 overview of systematic reviews and updated framework. Med Decis Making. 2020;40:379–398. doi:10.1177/0272989X20911870
32. Moghadam ES, Manzari ZS, Ghalenow HR, et al. Ottawa decision support framework to improve iranian nurses’ decision coaching skills. Indian J Crit Care Med. 2022;26:199–203. doi:10.5005/jp-journals-10071-24106
33. Sundler AJ, Lindberg E, Nilsson C, et al. Qualitative thematic analysis based on descriptive phenomenology. Nurs Open. 2019;6:733–739. doi:10.1002/nop2.275
34. Kim H-K, Jun M, Rhee S, et al. Husserlian phenomenology in Korean nursing research: analysis, problems, and suggestions. J Educ Eval Health Prof. 2020;17:13. doi:10.3352/jeehp.2020.17.13
35. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19:349–357. doi:10.1093/intqhc/mzm042
36. Njiru J, Philippe PA, Mogeni R, et al. Knowledge, attitudes, and barriers to oncofertility services among cancer patients requiring chemoradiotherapy: a systematic review. 2025.
37. Chung EH, Mebane S, Harris BS, et al. Oncofertility research pitfall? Recall bias in young adult cancer survivors. F&S Rep. 2023;4:98–103. doi:10.1016/j.xfre.2022.12.007
38. Shickh S, Leventakos K, Lewis MA, et al. Shared decision making in the care of patients with cancer. Am Soc Clin Oncol Educ Book;2023. e389516. doi: 10.1200/EDBK_389516
39. Zhang H, Yang L. Family model of cancer condition notification. Med Philos. 2020;41:17–19,33.
40. Meng M, Li X, Zhao J, et al. When western concept meets eastern culture: exploring the impact of confucianism on shared decision-making in China. Asia-Pac J Oncol Nurs. 2024;11:100586. doi:10.1016/j.apjon.2024.100586
41. Chen W, Zhang H, Xu M, et al. Differences in shared decision-making: the east-west divide. BMJ Evid-Based Med. 2024;29:289–291. doi:10.1136/bmjebm-2023-112451
42. Benedict C, Thom B, Kelvin JF. Young adult female cancer survivors’ decision regret about fertility preservation. J Adolesc Young Adult Oncol. 2015;4:213–218. doi:10.1089/jayao.2015.0002
43. Chan JL, Letourneau J, Salem W, et al. Regret around fertility choices is decreased with pre-treatment counseling in gynecologic cancer patients. J Cancer Surviv. 2017;11:58–63. doi:10.1007/s11764-016-0563-2
44. Taniskidou A-M, Voultsos P, Tarlatzis V, et al. Perceptions and experiences of fertility preservation in female patients with cancer in Greece. BMC Women’s Health. 2024;24:108. doi:10.1186/s12905-024-02955-x
45. Di Mattei VE, Taranto P, Perego G, et al. Identification of psychological profiles of cancer patients undergoing fertility preservation counseling. J Clin Med. 2023;12:4011. doi:10.3390/jcm12124011
46. Dorfman CS, Stalls JM, Shelby RA, et al. Impact of financial costs on patients’ fertility preservation decisions: an examination of qualitative data from female young adults with cancer and oncology providers. J Adolesc Young Adult Oncol. 2024;13:502–513. doi:10.1089/jayao.2023.0108
47. Abrams HR, Durbin S, Huang CX, et al. Financial toxicity in cancer care: origins, impact, and solutions. Transl Behav Med. 2021;11:2043–2054. doi:10.1093/tbm/ibab091
48. Nong Z, Huang L, Chen W, et al. Analysis on the effect of including assisted reproductive technology in medical insurance reimbursement policy. Chin Hosp Manag. 2025;45:66–69.
49. Jia L, Hu L, Xiao D. The Practice and Reflections on the Inclusion of Assisted Reproductive Technologies in Medical Insurance. China Health Insurance. 2025;23–29.
50. Zhang L, Qiao D. Perceptions of health system professionals on integrating fertility care into reproductive health policy in China. Health Care. 2025;13:555. doi:10.3390/healthcare13050555
51. Yasmin E, Balachandren N, Davies MC, et al. Fertility preservation for medical reasons in girls and women: British fertility society policy and practice guideline. Hum Fertil. 2018;21:3–26. doi:10.1080/14647273.2017.1422297
52. Woodruff TK. Oncofertility: a grand collaboration between reproductive medicine and oncology. Reprod. 2015;150:S1–10. doi:10.1530/REP-15-0163
53. Frisch EH, Yao M, Kim H, et al. Window of opportunity: rate of referral to infertility providers among reproductive-age women with newly diagnosed gynecologic cancers. J Clin Med. 2024;13:4709. doi:10.3390/jcm13164709
54. Salama M, Ataman-Millhouse L, Sobral F, et al. Barriers and opportunities of oncofertility practice in nine developing countries and the emerging oncofertility professional engagement network. J Global Oncol. 2018;4:
55. Dorfman CS, Stalls JM, Mills C, et al. Addressing barriers to fertility preservation for cancer patients: the role of oncofertility patient navigation. J Oncol Navig Surviv. 2021;12:332–348.
56. Lien C-T, Huang S-M, Hua Chen Y, et al. Evidenced-based practice of decision-making process in oncofertility care among registered nurses: a qualitative study. Nurs Open. 2021;8:799–807. doi:10.1002/nop2.684
57. Stacey D, Lewis KB, Smith M, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2024;1:CD001431. doi:10.1002/14651858.CD001431.pub6
58. Zhang W, Zhang J, Guo C, et al. The experience of fertility preservation decision-making in child-bearing period women with cancer: A qualitative Meta-synthesis. Chin J Nurs. 2023;58:1504–1511.
59. Yuan T, Liu L, He Y. Development and application of decision aids for fertility preservation in female of reproductive age with cancer. Chin Nurs Manag. 2025;25:208–213.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Shared Decision-Making in Hemophilic Arthropathy Rehabilitation: A Qualitative Study
Liu YQ, Guo YL, Xu J, Geng WJ, Li ZZ, Jia M, Liu YD, Zhao H
Patient Preference and Adherence 2023, 17:249-257
Published Date: 25 January 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
A Qualitative Study of Fertility Preservation Experience in Women with Breast Cancer
Wang Z, Yang X, Hong X, He Y, Xu A, Jiang X, Wei Q
International Journal of Women's Health 2025, 17:1143-1155
Published Date: 23 April 2025
Experiences with Higher-Risk Myelodysplastic Syndromes and Improving Patient-Centered Treatment Decision-Making: A Qualitative Study of Patients, Caregivers, and Providers
Maravic MC, Land N, Prood N, Cagle C, May SG, Batt K, Sabate EJ, Afulezi N, Jhaveri TZ, Iraca T, Hogea C
Cancer Management and Research 2025, 17:1215-1232
Published Date: 24 June 2025