Back to Journals » Patient Preference and Adherence » Volume 17
Shared Decision-Making in Hemophilic Arthropathy Rehabilitation: A Qualitative Study
Authors Liu YQ ![]() , Guo YL, Xu J, Geng WJ, Li ZZ, Jia M, Liu YD, Zhao H
, Guo YL, Xu J, Geng WJ, Li ZZ, Jia M, Liu YD, Zhao H
Received 20 October 2022
Accepted for publication 11 January 2023
Published 25 January 2023 Volume 2023:17 Pages 249—257
DOI https://doi.org/10.2147/PPA.S394095
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yan-Qiu Liu,1 Yu-Lin Guo,2 Jia Xu,3 Wen-Jing Geng,1 Zhen-Zhen Li,4 Ming Jia,1 Yu-Dan Liu,1 Hua Zhao1
1College of Nursing, Shanxi University of Chinese Medicine, Jinzhong, Shanxi, People’s Republic of China; 2Department of Rehabilitation, The Second Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 3Department of Nephrology, Shanxi Bethune Hospital, Taiyuan, Shanxi, People’s Republic of China; 4Department of Hematology, The Second Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China
Correspondence: Hua Zhao, College of Nursing, Shanxi University of Chinese Medicine, Jinzhong, Shanxi, People’s Republic of China, Tel +86 13903465019, Email [email protected]
Purpose: To probe into the needs and barriers underlying patients’ participation in shared decision-making related to rehabilitation nursing for hemophilic arthropathy.
Patients and Methods: The phenomenological research approach was adopted to conduct a series of semi-structured, in-depth interviews with 15 patients with hemophilic arthropathy undergoing rehabilitative treatments, 10 caregivers, and 7 healthcare providers from a hemophilia treatment center in Shanxi province, China. Colaizzi’s seven-step method of data analysis was applied to organize, analyze, and extract the themes from the interview materials.
Results: Three main themes emerged from the analysis: the status quo of the healthcare system (insufficient decision support systems and mismatch between healthcare providers’ and patients’ resources), circumstances of provider–patient interactions (lack of information exchange and unbalanced power structure between healthcare providers and patients), and patient-related factors influencing participation in decision-making (lack of self-efficacy, personal characteristics, family and social decision support, and attitude toward participation in decision-making).
Conclusion: Participation in rehabilitation decision-making among patients with hemophilic arthropathy is affected by multiple barriers. Healthcare professionals should improve their understanding of shared decision-making, offer patients active guidance on participating in the decision-making process, prioritize their affective needs, and formulate professional and effective solutions to support shared decision-making as early as possible.
Keywords: hemophilic arthropathy, shared decision-making, rehabilitation program, nursing, joint function, qualitative research
Introduction
Hemophilia is an X-linked recessive hereditary disease with clinical manifestations including acute spontaneous hemorrhages and persistent bleeding. More than 80% of the bleeding episodes occur at specific joints (eg, ankles, knees, and elbows).1 Chronic recurrent hemorrhages and hematoma lead to progressive joint damage, which gradually develops into hemophilic arthropathy.2 The condition is subsequently accompanied by persistent chronic pain and limited joint function, eventually resulting in disability and deformity.3,4 Routine rehabilitation training can reduce the frequency of joint hemorrhages, thus achieving the goal of preventing, relieving, and reversing the functional disorder experienced by hemophilic patients.5,6
Traditionally, rehabilitation training often adopts the paternalistic model of decision-making, predominantly focusing on unilateral consultations and lacking elements of interactive collaboration. Patients tend to participate in the program less proactively and exhibit lower levels of self-management capabilities,7 which results in considerable disparities in the rehabilitation outcomes. Therefore, how to effectively involve patients in rehabilitation is, at present, a pressing issue to be addressed by China’s healthcare industry. As the most widely recognized clinical decision-making model to date, shared decision-making refers to the process in which healthcare providers communicate details with patients on an equal footing, explicitly informing them of the benefits and risks of different options, honoring their choice and autonomy, and make personalized medical decisions congruent with their values and preferences.8
In recent years, shared decision-making has been gradually applied to the field of rehabilitation training; however, the application is still in its infancy and presents a number of implementation barriers. The phenomenological research approach is a cognitive process, which explores the essence of the actual phenomenon from the perspective of people who have experienced the phenomenon, so as to understand the significance it gives to the phenomenon.9 In order to ensure the integrity, accuracy, and credibility of phenomenological research, researchers should analyze the collected data according to seven steps: reading and re-reading the transcript, identifying significant statements, formulating meanings, clustering themes, developing an exhaustive description, producing the fundamental structure, and seeking verification of the fundamental structure.10 Based on the healthcare provider–patient–caregiver perspective, this study aimed to elucidate the needs and barriers underlying patients’ participation in shared decision-making in rehabilitation nursing for hemophilic arthropathy using the phenomenological approach. Its purpose is to provide a basis for the implementation of shared decision-making for rehabilitation patients as well as a frame of reference for formulating targeted shared decision-making solutions to help patients set realistic expectations and improve their rehabilitation effectiveness.
Materials and Methods
Research Subjects
Purposive sampling was employed to select patients with hemophilic arthropathy undergoing rehabilitative treatments, caregivers, and healthcare providers from a hemophilia treatment center in Shanxi province, China, as research subjects, between May and July 2022. Inclusion criteria for patients were (1) individuals meeting the diagnostic criteria for hemophilia and hemophilic arthropathy;11 (2) having basic comprehension and communication skills; and (3) providing informed consent and voluntarily participating in this study. The exclusion criteria were (1) conditions complicated by severe damage of other vital organs and (2) cognitive and verbal communication disorders. Inclusion criteria for caregivers were (1) individuals participating in the rehabilitation decision-making process for the patient and (2) providing informed consent and voluntarily participating in this study. The exclusion criteria were (1) paid caregivers and (2) inability to communicate. Inclusion criteria for healthcare providers were (1) familiarity with the rehabilitation decision-making process for hemophilic patients as well as with the mentality of patients and caregivers; (2) involved in the rehabilitation of hemophilic patients; (3) having at least five years of service in the related field; and (4) providing informed consent and voluntarily participating in this study. The exclusion criterion was non-permanent employee of the hospital.
The sample size was determined based on when the interview data reached “saturation”, which meant the point of no new themes emerging from data analysis. A total of 15 patients, 10 caregivers, and 7 healthcare providers were interviewed in this study. Their general information is presented in Tables 1–3.
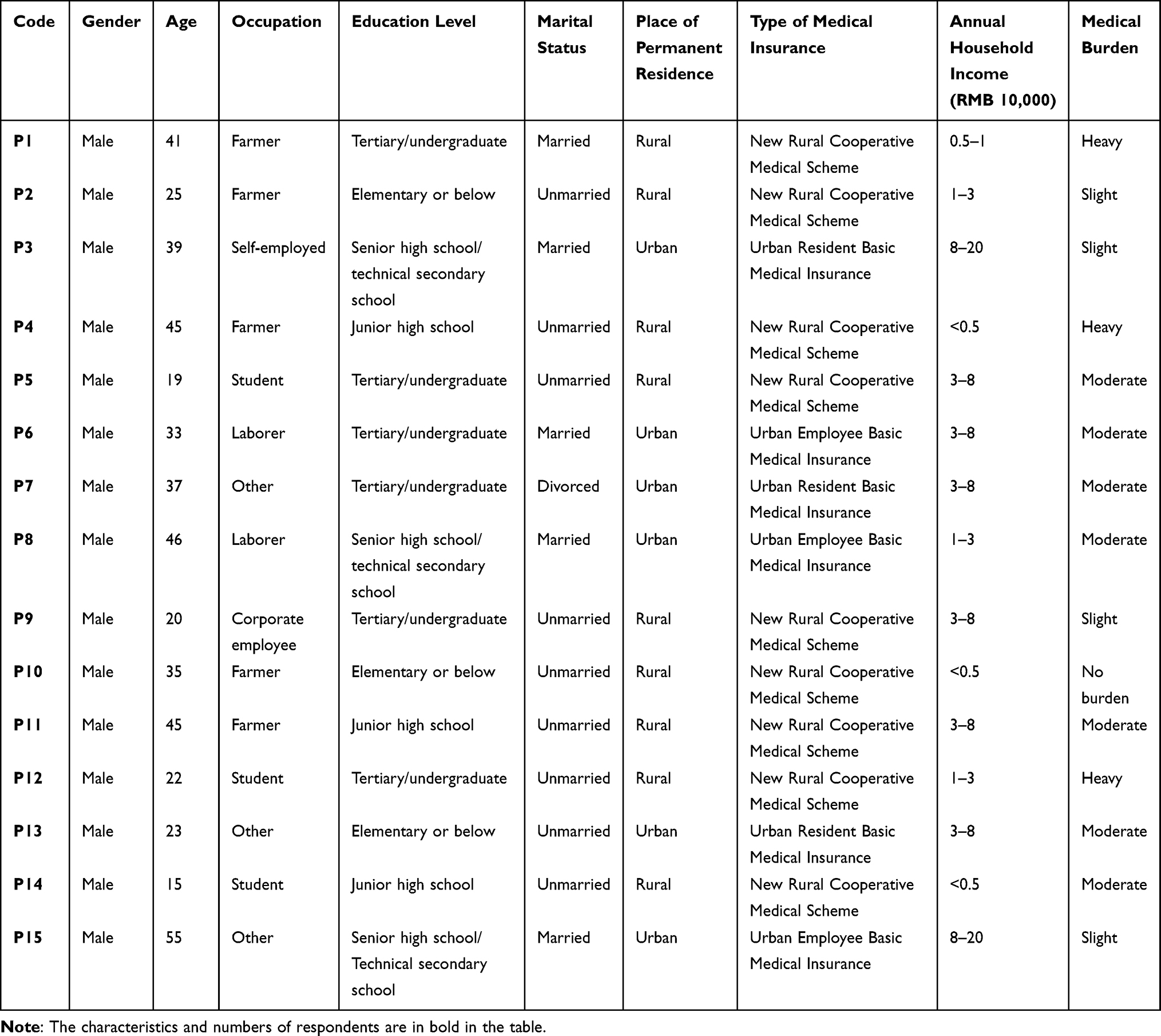 |
Table 1 General Information of Interviewed Patients (n = 15) |
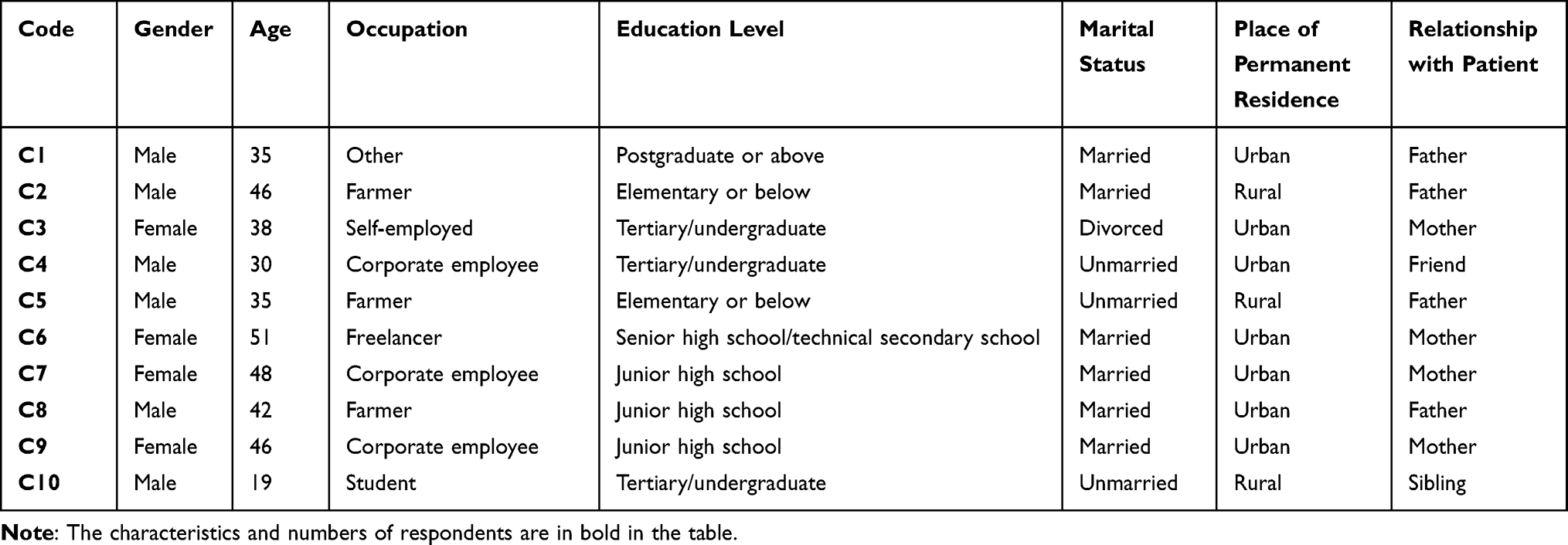 |
Table 2 General Information of Interviewed Caregivers (n = 10) |
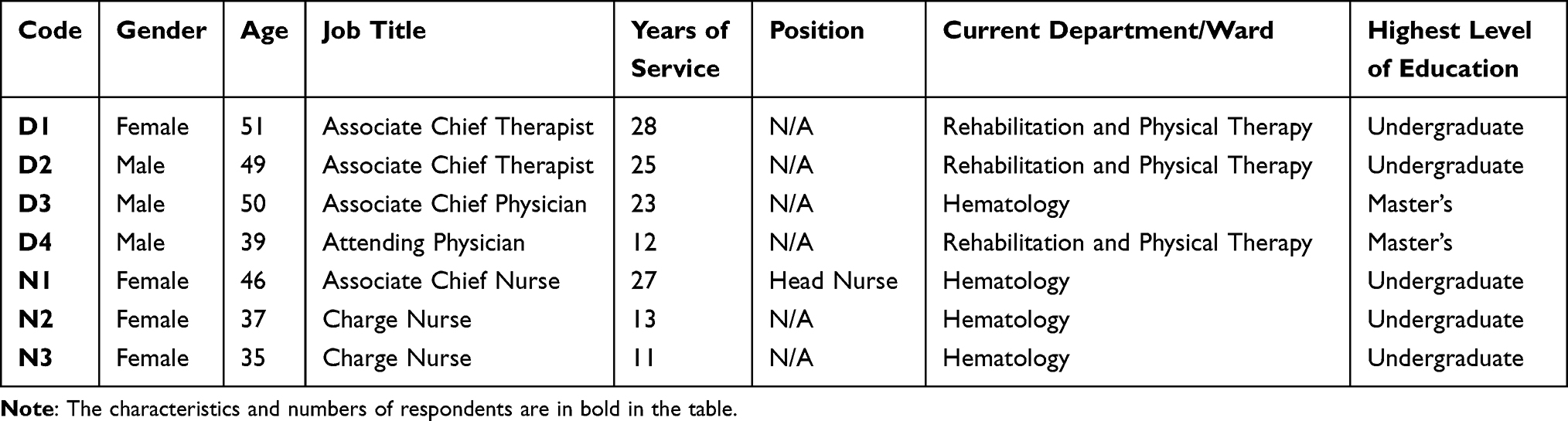 |
Table 3 General Information of Interviewed Healthcare Providers (n = 7) |
Methods
Researchers
The research team had developed a solid theoretical and practical foundation from years of clinical practice and scientific research in hemophilia as well as from experience in conducting practical research in this regard. With diverse experiences in interviews and data analysis across different types of qualitative studies, the interviewers were able to build a relationship of trust with the interviewees, thereby obtaining interview data that was comprehensive and objective in nature.
Data Collection
The phenomenological approach of qualitative research was adopted to collect data using semi-structured interviews.9 An interview outline was drafted prior to the study based on a combination of the research purpose, opinions from experts in hemophilic rehabilitation, and related literature. Pre-interviews were also conducted with two patients, a caregiver, and a nurse to revise and finalize the formal interview outline based on their feedback. The interview outline for the patients was as follows: (1) How was your current rehabilitation program determined, and were you consulted during the process? (2) How did the healthcare providers introduce different rehabilitation programs to you, and how did you feel after being introduced to them? (3) How did you consider/decide on which rehabilitation program to select? (4) Can the guidance currently provided by healthcare providers satisfy your needs, and what kind(s) of help and support do you think will facilitate your decision-making? (5) Are you willing to participate in the discussion and selection of your rehabilitation program, and what are the factors influencing your participation? The interview outline for the caregivers was as follows: (1) How was the patient’s current rehabilitation program determined? (2) What kind(s) of help do you think healthcare providers should offer during the process of rehabilitation decision-making? (3) Do you think patients should participate in the formulation of their rehabilitation program, and why? The interview outline for healthcare providers was as follows: (1) What do you think about the status quo of the rehabilitation training currently available to patients, and what are the areas that can be refined, in your opinion? (2) Would you actively inform patients of the process and scope of decision-making in relation to their rehabilitation program, and why? (3) Do you think patients should participate in the shared decision-making process for their rehabilitation training, and is the shared decision-making model achievable? (4) What do you think are the barriers/facilitators to patients’ participation in the shared decision-making for their rehabilitation training? (5) If a shared decision-making solution is to be developed for the rehabilitation training of hemophilic patients, what should be included?
The interviewees were briefed in detail on the purpose, significance, procedures, and principle of data confidentiality of this study before the formal interviews. After obtaining their informed consent for procedures, such as audio-recording the interviews, they were asked to sign an informed consent form. A quiet and secluded room was selected to carry out the interviews. During interviews, the participants were encouraged to express their honest thoughts. Each interview lasted for around 30 minutes and could be terminated immediately if the interviewee experienced any physical discomfort or if there was any other reason to do so.
Ethical Consideration
This study was reviewed and approved by the Ethics Committee of the Second Hospital of Shanxi Medical University (Approval number: (2022) YX No. (103)). Written informed consent was obtained from all interviewees before the formal interview, including the publication of anonymized responses.
Data Organization and Analysis
Interview data were transcribed into text, and were kept on file and organized using the Nvivo 11.0 qualitative data analysis software within 24 hours after the interviews. Based on Colaizzi’s seven-step method of data analysis,10 the data were encoded, extracted, and clustered before further comparing and refining the themes. The findings were validated by the interviewees to ensure their accuracy.
Results
A total of three themes and eight sub-themes were identified. They included (1) the status quo of the healthcare system (insufficient decision support systems and mismatch between healthcare providers’ and patients’ resources); (2) circumstances of provider–patient interactions (lack of information exchange and unbalanced power structure between healthcare providers and patients); and (3) patient-related factors influencing participation in decision-making (lack of self-efficacy, personal characteristics, family and social decision support, and attitude toward participation in decision-making).
Theme 1: Healthcare System Status Quo
Insufficient Decision Support Systems
Decision aids are tools that elucidate the risks, benefits, and harms associated with each treatment option and help patients make specific and deliberated choices by clarifying their personal values and preferences.12 Nevertheless, there is currently a lack of standardized decision aids in clinical practices.
P5:I would like to know more about rehabilitation; it would’ve been great if there were more reference materials for us, like some sort of handbooks of rehabilitation training or popular science videos.
As shared decision-making was initiated relatively late in China, there is still a lack of related policies, and most healthcare providers are unfamiliar with what it entails.
D1:I’ve heard of this decision-making approach, but our department has never tried the full process. We’re unsure about how it actually works and know little about how to evaluate patients’ values and preferences and how to provide information.
As online information is highly variable in its quality nowadays, patients often struggle to determine the credibility of a piece of information and have difficulties accessing correct knowledge about a disease, which aggravates their psychological burden.
C4:We’re curious to know if rehabilitation exercise is safe and afraid of bleeding again. We did an online search; some say it’s good, and some say it’s bad. The more we looked into it, the more confused we were.
Mismatch Between Resources
At present, China’s medical resources are increasingly strained. Owing to their busy schedules and heavy workloads, clinical healthcare providers do not have enough time to discuss detailed information about different options with patients. As a result, patients are unable to fully understand their options and make choices that best suit them.
P10:The doctors are too busy. The outpatient clinic is so crowded that, whenever I ask them a question, they’ll only give me a simple two-sentence explanation. I still don’t really understand it but feel too embarrassed to ask them again.
D2:We have arranged fixed rehabilitation training sessions every day, and we have quite a lot of work to do. We’d like to discuss more about the rehabilitation plans with the patients, but some of them know very little about their own conditions and dither when making a decision. What could’ve been settled in five minutes ends up dragging on for far too long.
N1:Our jobs as nurses are rather complicated and tedious. Shared decision-making is still a prototype for the time being. Putting it into practice will be complicated and require us to spend significantly more time at work. We won’t be able to finish the rest of our work.
Theme 2: Circumstances of Provider–Patient Interactions
Lack of Information Exchange
Shared decision-making requires both healthcare providers and patients to communicate on an equal footing and discuss the rehabilitation procedures and goals jointly, to help patients set reasonable expectations. However, as the medical knowledge involved is highly specialized and extensive, the knowledge of the disease cannot be communicated in detail in a short amount of time. The disparities in patients’ access to and understanding of information result in information asymmetry between them and healthcare providers.13
P13:I’m not a well-educated person. The doctor told me a lot of things, but I understood none of them.
P9:The doctor used a lot of technical terms that I didn’t understand and said it’s hard to explain everything at once. But I still want to get a better grasp of the rehabilitation training because I’m afraid that something will go wrong.
During the interviews, a lack of self-efficacy was also found to be a factor influencing information exchange in some healthcare providers. This included a lack of communication skills and specialized knowledge in decision support.
N3:I want to help my patients too, but they sometimes ask questions that I’m unable to answer. We’ve never been systematically trained either, so we don’t know how to give them guidance and put things into practice.
Unbalanced Power Structure
Influenced by conventional thinking, patients tend to inwardly recognize doctors’ authority. They place their decision-making power completely in their doctors’ hands and exhibit excessive reliance on the latter.
C2:Doctors are professionals. After seeing so many patients, they’re bound to have a lot of experience. We’re willing to do everything they say.
During the interviews, both the healthcare providers and the patients were found to have an unclear understanding of their roles. Accustomed to keeping a tighter control over the substance of communication, doctors tend to guide patients toward a predetermined decision and overlook their genuine needs during the decision-making process.
C8:The doctor introduced a number of rehabilitation approaches to us briefly and, without consulting me or the patient when developing the rehabilitation plan, informed us straight away which one was the best suited for us based on the patient’s current condition.
Theme 3: Patient-Related Factors
Lack of Self-Efficacy
With limited knowledge and understanding of the disease, patients are unable to clearly communicate their personal needs during the decision-making process and struggle to make the optimal decision as a result.
C6:We know nothing about the methods of joint rehabilitation. When the doctor asked us to share our thoughts, we didn’t know what to say.
A targeted rehabilitation program should be developed based on a patient’s specific conditions, but some patients are uncertain about their own values and preferences and do not know which option is in their best interests.
P2:The doctor asked me which option I preferred. My mind was a complete blank, and I didn’t know what was best for my circumstances. Eventually, I resorted to doing what the doctor said.
Personal Characteristics
During the interviews, age, education level, and economic status were found to have a significant influence on patients’ willingness to participate in decision-making.
P14:I wish the doctor and my parents could tell me more about the condition I’m currently in. I’m old enough now. I need to know the specifics of my condition to better protect my knees.
C9:We’re not well-educated people. We won’t understand a thing even if we listen all day, and it’s a waste of the doctor’s time. We might as well cut to the chase and make a decision.
P1:I’m from a struggling household. Some of the rehabilitation items cannot be reimbursed through the New Rural Cooperative Medical Scheme, and I only do them once in a while on my return visits. As for how the rehabilitation works, I just listen to what the doctor says and do as I’m told—it’s as simple as that.
Family and Social Decision Support
During the rehabilitation process, patients need more than support in terms of specialized information about their diseases. They also harbor a need for mental and psychological recognition and encouragement from people, such as their families and healthcare providers, which constitutes another crucial factor influencing their decision-making.
P12:I used to shy away from exercising because I was afraid of having to be injected with the clotting factor if I bleed again. The factor VIII infusions are too expensive. But my parents were supportive the whole time, so I eventually reached out to the doctor to discuss how I could exercise.
P6:The doctors’ and nurses’ attitudes matter a lot. Their encouragement gives me confidence. Sometimes, though, they may speak in a stiffer voice. Whenever that happens, my heart sinks, and I feel like I’m never going to get better.
Attitude Toward Participation in Decision-Making
Hemophilia is a condition that requires lifelong treatments. When confronted with the disease, patients often experience intense psychological stress and an overwhelming sense of disease burden, thus displaying less willingness to make decisions.
P4:This leg of mine [referring to his right leg] is disabled permanently. I can’t take care of myself and have to go through a battle just to put on a pair of shoes [laughs wryly]. Rehabilitation is useless to me at this point, not to mention decision-making.
P5:At first, I thought rehabilitation training could restore my functioning and allow me to move freely at the very least. But a few sessions in, and not much had happened. The doctor said there were a few more courses of treatment to go through, but I didn’t want to continue because it had put too much stress on my family, financially.
Despite the above, most patients felt positive about participating in the decision-making process for their rehabilitative treatments.
P7:I’m more than happy to take part in the discussions regarding of my leg. I want to get rid of the crutches and walk on my own as soon as possible.
P3:Joining the discussions will allow me to make decisions based on my own needs and result in a more reasonable rehabilitation program.
Discussion
Building a Professional and Effective Decision Support System
At present, information about the rehabilitative treatments of hemophilic arthropathy is relatively dispersed. Meanwhile, it is difficult to separate credible from untrustworthy online information. While patients who lack the ability to identify specialized information are prone to experience informational confusion, the key phases of the decision-making process require them to weigh the pros and cons of each option based on their own circumstances14 in order to make the optimal choice. However, healthcare providers at public hospitals are often preoccupied with work and have insufficient time to communicate with patients, likely resulting in an understanding gap between them during the decision-making process—a finding in line with those of recent studies.15,16 Decision aids are tools that facilitate patients’ participation and support shared decision-making; they can improve patients’ understanding about disease-related knowledge and promote their participation in the decision-making process.17,18 Thus, healthcare providers should draw on well-established decision aids as a basis to actively construct a localized model of shared decision-making for the rehabilitation of patients with hemophilic arthropathy and provide scientific and reliable information that can aid patients’ deliberated decision-making. Meanwhile, decision coaching19 can be integrated into clinical decision-making to guide patients through making personalized choices. To successfully implement shared decision-making, it is also crucial for the management of hospitals and organizations to prioritize and support it, allocate resources reasonably, adjust the workflow accordingly, and create a medical environment conducive to such implementation.
Define Participants’ Roles and Positions in Shared Decision-Making
For a long time, paternalistic decision-making has created a custom in which healthcare providers habitually place themselves in a dominant position, while patients honor and recognize their authority, excessively relying on them, thus severely undermining patients’ participation in the decision-making process. This finding is consistent with that reported by Ubel et al.20 Furthermore, patients tend to be more passive throughout the medical decision-making process due to their limited understanding of the disease and lack of confidence in their decisions. During the process of shared decision-making, however, healthcare providers and patients are collaborators and should come together to develop a rehabilitation program suited to the latter’s conditions.21 A study by Bailo et al22 described doctors and patients as experts in different fields, with the former providing specialized medical knowledge and the latter clarifying their personal preferences and values; equality between both parties is the core prerequisite for implementing shared decision-making. Therefore, it is important to enhance healthcare providers’ understanding about shared decision-making, carry out targeted learning and training, build awareness toward shared decision-making, guide and aid patients’ participation in this process, and place a patient-centric medical model into practice. Meanwhile, healthcare providers should step up their promotional and educational efforts, strengthening the promotion and education surrounding knowledge related to shared decision-making through various means. The “teach-back” method,23 for example, can be employed to heighten patients’ awareness of information related to shared decision-making, as the dynamic interactive process can improve their communication with healthcare providers, promote their active participation in the decision-making process, and increase satisfaction with the decisions.
Considering Patients’ Affective Needs and Encouraging Their Participation in Decision-Making
Hemophilia is a lifelong bleeding disorder that is costly to treat. Owing to an overwhelming self-perceived burden, patients are likely to exhibit behaviors such as passive coping. To counteract this, when communicating with patients, healthcare providers should place an emphasis on experiencing their affect. A study24 showed that affective empathy between healthcare providers and patients can eliminate cognitive differences between them and encourage patients to lower their mental guard, thus helping them relieve any negative emotions and establish healthy beliefs. Moreover, connections can be forged with related social support systems to ease patients’ financial burden. During the interviews, family support was found to be of great significance to patients’ participation in decision-making. Hence, healthcare providers should also make active efforts to facilitate family members’ participation in decision-making and guide them in providing more support for the patients. By doing so, they can leverage the positive role of family members in rehabilitation and enable patients to confront their illnesses in the correct manner, thereby boosting the decision quality.
Conclusion
The current study found that participation in rehabilitation decision-making among patients with hemophilic arthropathy is affected by various barriers. Healthcare providers should improve their understanding of shared decision-making, offer patients active guidance on participating in the decision-making process, prioritize their affective needs, and encourage family members to participate in the process. Meanwhile, a localized solution for shared decision-making support should be researched and developed as soon as possible to help hemophilic patients understand evidence-based information of guiding significance to rehabilitation and enhance their self-efficacy, to achieve the joint development of individualized, comprehensive rehabilitation programs.
Acknowledgments
We would like to thank Editage for English language editing.
Funding
This study has been conducted through a project grant from the Scientific Research Foundation for Doctoral Programs of Shanxi University of Chinese Medicine, grant no.: 2020BK16.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020;26:1–158. doi:10.1111/hae.14046
2. Pulles AE, Mastbergen SC, Schutgens RE, Lafeber FP, van Vulpen LF. Pathophysiology of hemophilic arthropathy and potential targets for therapy. Pharmacol Res. 2017;115:192–199. doi:10.1016/j.phrs.2016.11.032
3. Wyseure T, Mosnier LO, von Drygalski A. Advances and challenges in hemophilic arthropathy. Semin Hematol. 2016;53(1):10–19. doi:10.1053/j.seminhematol.2015.10.005
4. Valentino LA. Blood-induced joint disease: the pathophysiology of hemophilic arthropathy. J Thromb Haemost. 2010;8(9):1895–1902. doi:10.1111/j.1538-7836.2010.03962.x
5. Stephensen D, Bladen M, McLaughlin P. Recent advances in musculoskeletal physiotherapy for haemophilia. Ther Adv Hematol. 2018;9(8):227–237. doi:10.1177/2040620718784834
6. Scaturro D, Benedetti MG, Lomonaco G, et al. Effectiveness of rehabilitation on pain and function in people affected by hemophilia. Med. 2021;100(50):e27863. doi:10.1097/MD.0000000000027863
7. Xu Y, Wang YY, Wang Y, et al. Self-management dilemma in patients with hemophilic arthropathy: a qualitative study. Chin J Nurs. 2021;56(4):534–539.
8. Hoffmann T, Bakhit M, Michaleff Z. Shared decision making and physical therapy: what, when, how, and why? Braz J Phys Ther. 2022;26(1):100382. doi:10.1016/j.bjpt.2021.100382
9. Neubauer BE, Witkop CT, Varpio L. How phenomenology can help us learn from the experiences of others. Perspect Med Educ. 2019;8(2):90–97. doi:10.1007/s40037-019-0509-2
10. Colaizzi P. Psychological research as a phenomenologist views it [M]. In: Valle R, King M, editors. Existential Phenomenological Alternatives for Psychology. Oxford, England: Oxford University Press; 1978:5–7.
11. Thrombosis and Hemostasis Group, Chinese Society of Hematology. Chinese Medical Association and Hemophilia Treatment Center Collaborative Network of China. Chinese guidelines on the treatment of hemophilia (version 2020). Chin J Hematol. 2020;41(4):265–271.
12. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4(4):CD001431. doi:10.1002/14651858.CD001431.pub5
13. van Til JA, Drossaert CH, Punter RA, IJzerman MJ. The potential for shared decision-making and decision aids in rehabilitation medicine. J Rehabil Med. 2010;42(6):598–604. doi:10.2340/16501977-0549
14. Kim K, Yang J. Decision-making process related to treatment and management in Korean women with breast cancer: finding the right individualized healthcare trajectory. Appl Nurs Res. 2017;35:99–105. doi:10.1016/j.apnr.2017.02.022
15. Huang C, Lam L, Zhong Y, Plummer V, Cross W. Chinese mental health professionals’ perceptions of shared decision-making regarding people diagnosed with schizophrenia: a qualitative study. Int J Ment Health Nurs. 2021;30(1):189–199. doi:10.1111/inm.12771_1
16. Obeidat RF, Lally RM. Jordanian physicians’ perceived barriers and facilitators to patient participation in treatment decision-making: an exploratory study. Indian J Cancer. 2018;55(4):377–381. doi:10.4103/ijc.IJC_122_18
17. Chenel V, Mortenson WB, Guay M, Jutai JW, Auger C. Cultural adaptation and validation of patient decision aids: a scoping review. Patient Prefer Adherence. 2018;12:321–332. doi:10.2147/PPA.S151833
18. Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, Magallón-Botaya R, Romero-Martín M, Gómez-Salgado J. Interventions to facilitate shared decision-making using decision aids with patients in Primary Health Care: a systematic review. Med. 2020;99(32):e21389. doi:10.1097/MD.0000000000021389
19. O’Connor AM, Stacey D, Légaré F. Coaching to support patients in making decisions. BMJ. 2008;336(7638):228–229. doi:10.1136/bmj.39435.643275.BE
20. Ubel PA, Scherr KA, Fagerlin A. Empowerment failure: how shortcomings in physician communication unwittingly undermine patient autonomy. Am J Bioeth. 2017;17(11):31–39. doi:10.1080/15265161.2017.1378753
21. Negrier C, Seuser A, Forsyth A, et al. The benefits of exercise for patients with haemophilia and recommendations for safe and effective physical activity. Haemophilia. 2013;19(4):487–498. doi:10.1111/hae.12118
22. Bailo L, Vergani L, Pravettoni G. Patient preferences as guidance for information framing in a medical shared decision-making approach: the bridge between nudging and patient preferences. Patient Prefer Adherence. 2019;13:2225–2231. doi:10.2147/PPA.S205819
23. Seely KD, Higgs JA, Nigh A. Utilizing the “teach-back” method to improve surgical informed consent and shared decision-making: a review. Patient Saf Surg. 2022;16(1):12. doi:10.1186/s13037-022-00322-z
24. Vinson AH, Underman K. Clinical empathy as emotional labor in medical work. Soc Sci Med. 2020;251:112904. doi:10.1016/j.socscimed.2020.112904
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Experiences with Higher-Risk Myelodysplastic Syndromes and Improving Patient-Centered Treatment Decision-Making: A Qualitative Study of Patients, Caregivers, and Providers
Maravic MC, Land N, Prood N, Cagle C, May SG, Batt K, Sabate EJ, Afulezi N, Jhaveri TZ, Iraca T, Hogea C
Cancer Management and Research 2025, 17:1215-1232
Published Date: 24 June 2025
Shared Decision-Making on Fertility Preservation in Reproductive-Aged Women with Gynecological Cancer: A Qualitative Study of Patients’ and Health Care Professionals’ Perspectives
Lin Y, Ma Q, Wang X, Li X, Jin M, Wei Q, Jiang L
International Journal of Women's Health 2025, 17:5155-5168
Published Date: 5 December 2025
Experiences Related to Learned Helplessness and Support Needs Among Patients with Recurrent Implantation Failure Undergoing in vitro Fertilization and Embryo Transfer: A Qualitative Study
Guo S, Peng X, Xie C, Leng W, Zhou L, Zhang M, Cai S
Psychology Research and Behavior Management 2026, 19:620415
Published Date: 16 June 2026