Back to Journals » Clinical Interventions in Aging » Volume 20
Sex Differences in the Association Between Inflammatory Biomarkers (Hs-CRP, IL-6, IL-10, TNF-α) and Frailty in Hospitalized Adults Aged ≥65 in Taizhou, China: A Cross-Sectional Study
Authors Yang H, Xiao J ![]() , Zhang W, Liu X, Mao H, Xu D
, Zhang W, Liu X, Mao H, Xu D
Received 1 August 2025
Accepted for publication 25 November 2025
Published 1 December 2025 Volume 2025:20 Pages 2267—2281
DOI https://doi.org/10.2147/CIA.S553964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Zhi-Ying Wu
Heng Yang,1 Jiechenming Xiao,2 Weihong Zhang,2 Xiaoyu Liu,1 Huiping Mao,2 Dan Xu2
1Department of Emergency, Taizhou First People’s Hospital, Taizhou, Zhejiang, People’s Republic of China; 2Department of Nursing, Taizhou First People’s Hospital, Taizhou, Zhejiang, People’s Republic of China
Correspondence: Huiping Mao, Department of Nursing, Taizhou First People’s Hospital, No. 218, Hengjie East Road, Taizhou, Zhejiang, 318020, People’s Republic of China, Email [email protected] Dan Xu, Department of Nursing, Taizhou First People’s Hospital, No. 218, Hengjie East Road, Taizhou, Zhejiang, 318020, Email [email protected]
Purpose: Frailty is a prevalent geriatric syndrome that is strongly related to systemic inflammation; nevertheless, sex differences in its association with inflammation remain poorly understood. We aimed to investigate sex-specific associations between inflammatory biomarkers and frailty in a large cohort of hospitalized older adults.
Patients and Methods: This cross-sectional study with 4,438 older adults aged ≥ 65 years was conducted at Taizhou First People’s Hospital (Taizhou, China) between 23/08/2024 and 31/05/2025. The 28-item Frailty Index (FI-28, score ≥ 0.25 indicates frail) was used to measure frailty. High-sensitivity CRP (hs-CRP) (immunofluorescence), interleukin-6 (IL-6), interleukin-10 (IL-10), and tumor necrosis factor-alpha (TNF-α) (flow cytometry) were measured; biomarkers underwent ln-transformation. Multivariate logistic regression was used to calculate adjusted odds ratios (aORs) for frailty per 1 standard deviation (SD) rise in ln-transformed biomarkers, controlling for confounders. Sex-specific differences were evaluated using interaction tests.
Results: Women experienced frailty at a higher rate than men did (37.68% vs 22.8%, P < 0.001). After adjustment, high levels of IL-6, hs-CRP, and IL-10 in frail older adults were significantly linked to frailty risk (all P < 0.001). Nevertheless, TNF-α did not (p = 0.983). The relationship of frailty with IL-6, hs-CRP, and IL-10 was found to be significantly altered by sex, according to interaction tests (Pinteraction < 0.001). The relationship of inflammatory markers with frailty risk differed by sex. In women, raised hs-CRP, IL-6, and IL-10 (all P < 0.001) levels showed a strong link to greater frailty risk. In men, though these markers were significantly related to frailty, their strength was lower: hs-CRP, IL-6, and IL-10 (all P < 0.001). TNF-α showed no independent association in either group.
Conclusion: In older adults, elevated levels of hs-CRP, IL-6, and IL-10 are associated with higher frailty risk; the associations are significantly stronger in women than in men. These findings emphasize considering sex differences in frailty management; however, longitudinal studies are required to confirm causality.
Keywords: frailty syndrome, biomarkers, inflammatory, sex differences, aging, disability evaluation, healthy aging
Introduction
The syndrome, known as frailty, is defined by a multi-system functional deterioration that comes with aging and makes people more susceptible to small stressors that can cause disability as well as death. A large-scale survey study involving 62 countries reveals that the global prevalence of frailty in the older population varies between 7% and 24%.1 As the global population ages, the number of people aged 60 and above is projected to reach 2.1 billion by 2050.2 Therefore, frailty has become a major health concern as it poses significant challenges for healthcare providers due to its association with higher risks of hospitalization, falls, unmet care needs, and premature death.3 However, frailty is a dynamic and actually revocable development, making early identification and proactive intervention essential to prevent the progression of illness and disability and to reduce the burden on families and society.
Inflammation is closely associated with the development and progression of frailty in older adults, with accumulating cross-sectional and longitudinal evidence suggesting it may play a role in this process.4,5 Frailty can develop as a result of the long-term inflammatory biomarker release linked to aging, which promotes muscle atrophy, alters mitochondrial function, and hastens metabolic diseases.6,7 Hs-CRP and IL-6 remain the most extensively studied; a meta-analysis of 32 cross-sectional studies confirmed that adults with frailty and pre-frailty had significantly higher hs-CRP levels than their robust peers.8 A meta-analysis of 38 studies showed that older adults with frailty had 2.1-fold higher IL-1β levels, which is a critical activator of the NLRP3 inflammasome. This association was independent of comorbidities.8,9 Regarding frailty and mortality prediction, the Inflammatory Index Score (IIS) performs better than individual markers. According to a 10-year longitudinal study, IIS was associated with a 62% increased risk of frailty and had a greater discriminatory power than IL-6 or hs-CRP.10 Even after controlling for cofounders like sex as well as age, a number of cross-sectional studies have constantly found significant relationships of frailty with raised inflammatory marker levels, IL-10, IL-6, C-reactive protein (CRP), and TNF-α.11,12 However, other studies reported no clear association between frailty and CRP, TNF-α, or IL-10.6
Sex may regulate the biological processes affecting epigenetic modifications and mitochondrial dysfunction during aging.7,13 According to multiple large-scale international cohorts, including the Toledo Study of Healthy Aging (Spain), the English Longitudinal Study of Ageing (ELSA, UK), and the ESTHER Cohort (Germany), the occurrence and progression of frailty have been related to inflammatory biomarkers, such as hs-CRP and IL-6.14–16 However, many studies generally consider sex a confounder, often overlooking its potential regulatory impact on inflammatory pathways involved in frailty. Immune responses vary by sex and continue to change in both healthy and diseased conditions, with notable differences between men and women in disease manifestations.17 Female mice showed a stronger relationship of frailty with inflammation than male mice, as evidenced by the positive relationship found between frailty scores as well as serum levels of the pro-inflammatory cytokine IL-6 in mouse experiments.14 Few studies, however, have examined the sex-specific relationship between inflammation and frailty in the older adults. Consequently, more research in this field is required.18 Current frailty management often uses a “one-size-fits-all” approach that overlooks individual differences, especially sex-related mechanisms. Many studies fail to analyze data separately by sex, missing important variations. Moreover, research has focused mainly on describing mechanisms rather than addressing clinical management and intervention needs of older patients. With the development of precision medicine, especially in older patients, emphasizing sex-specific inflammatory biomarkers as diagnostic, intervention, and frailty management tools in older adults is crucial.
Therefore, the purpose of this study was to determine the association between inflammatory biomarkers and frailty in older inpatients (both men and women) who were aged ≥65 years. The primary hypothesis was supported by earlier evidence: Elevated levels of IL-6, hs-CRP, and IL-10 are associated with higher frailty risk, and this association differs across men and women (biomarker × sex was the primary interaction). TNF-α was included as a secondary biomarker because of its inconsistent associations with frailty in previous studies. Conclusions from this research might be used to generate hypotheses for sex-specific preventative and treatment strategies for older adults (to be validated in longitudinal studies).
Materials and Methods
Study Design and Setting
We used a cross-sectional research design because it eliminated the need for long-standing follow-up and helped us quickly and affordably evaluate the relationship of inflammatory biomarkers with frailty in a sizable population of older men as well as women.19 This study was conducted at Taizhou First People’s Hospital in Zhejiang Province, China. This Grade III Class A hospital serves approximately 170,000 older residents in urban and suburban areas, with an aging rate as high as 28.20% in this region. The reporting guidelines for Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) were adhered to in the study’s framework and reporting.20
Study Population
Potential participants were selected from older adults at Taizhou First People’s Hospital’s Geriatric Comprehensive Ward, Traditional Chinese Medicine Inpatient Department, and Geriatric Rehabilitation Ward between 23/08/2024 and 31/05/2025. Eligible patients who visited the assigned departments Monday through Friday (excluding public holidays) during the research were recruited via convenience sampling. With 4,674 potential applicants and 4,438 enrolled, the participation rate was 94.95%.
Inclusion Criteria
- Age: ≥65 years;
- Consciousness and communication skills: Conscious (Glasgow Coma Scale score ≥13), capable of completing basic question-and-answer conversations independently or with family members’ help (eg, responding to questions about name, age, and medical history);
- Sensory function: No severe hearing or speech impairment (capable of articulating requirements or responding to inquiries, no complete aphasia);
- Cognitive function: neither a Chinese Mini-Mental State Examination score of >24 points (normal or moderate cognitive impairment) nor a diagnosis of any mental disorders (eg, schizophrenia, major depressive disorder with cognitive impairment);
- Informed consent: The patient or their immediate family members will voluntarily participate.
Exclusion Criteria
- End-stage diseases: Based on the oncologist’s diagnostic and imaging data, the patient has been diagnosed with advanced cancer (Tumor, Nodes, and Metastasisstage IV or expected survival <6 months);
- Acute inflammation/trauma: Acute infection (eg, pneumonia or urinary tract infection, defined as body temperature >38.5 °C and white blood cell count >10 × 109/L in routine blood tests) or acute trauma (eg, fracture, post-operative recovery period <2 weeks) within the previous 30 days before enrollment;
- Drug usage that affects inflammation levels: Prolonged use (≥3 months) of glucocorticoids (eg, prednisone ≥5 mg/day), biologics (eg, anti-tumor necrosis factor medications), or immunosuppressants (eg, cyclosporine, tacrolimus), as confirmed by reviewing the patient’s prescription records;
- Data integrity: Missing rate of key indicators (eg, Frailty Index items or inflammatory biomarker test results) >5% or the inability to supplement complete data through multiple follow-ups;
Sample Size
The PASS 2021 software helped us compute the smallest vital sample size. Fan et al found that 8.9% of people 65 and older had frailty.21 Using an expected prevalence (p) of 0.089, a 95% confidence level, an allowable error (d) of 0.05, and considering a 20% attrition rate, we needed 629 participants. However, since for this analysis the participants were stratified by sex with an equivalent men-to-women ratio, the minimum sample size required to achieve statistical significance was set at 1,258 participants.
PASS 2021 software was used to calculate the a priori power, setting the attrition rate at 20%, power at 90%, and α at 0.05 (two-sided). Studies on Chinese older adults, including those by Xu et al and Fan et al, were cited for their effect sizes (aORs and sex interaction effect sizes).6,22 The actual number of recruited individuals was 4438 (actual power >99.9%); the minimal sample sizes needed for the primary association analysis were 386, 292, and 338 cases, respectively, to detect the associations between frailty and hs-CRP, IL-6, and IL-10. The minimum sample size needed per sex for each biomarker for the sex interaction analysis ranged from 308 to 512 cases, whereas the actual number of enrolled men and women was 2,320 and 2,118, respectively (actual power >99.8%). Every analysis complied with the statistical power criteria.
Research Tools
The patient’s clinical characteristics, frailty levels, and serum biomarker levels were acquired as follows.
Clinical Characteristics
Table S1 displays the definitions and codes for each covariate. Briefly, age was a continuous variable (years); sex was a categorical variable (1 = men, 0 = women); alcohol consumption was classified as never, past, or current drinker (current: >7 units/week for women, >14 units/week for men; 1 unit = 10 g pure alcohol); smoking was classified as never, past, or current smoker (current: ≥1 cigarette/day); educational level was a categorical variable (<5 years, ≥5 years); residence was a categorical variable (urban/rural); BMI was a continuous variable (kg/m2); comorbidity was defined as having two or more chronic diseases (The classification codes for chronic diseases are shown in Table S2) (0 = absent or 1 = present). Data were extracted from medical records and validated by reviewing physician diagnoses, laboratory results, and medication use. Polypharmacy was defined as five or more medications (based on the Chinese Geriatric Inappropriate Medication Directory) (0 = absent or 1 = present).
Frailty Assessment
The 28-item Frailty Index (FI-28), a validated instrument for Chinese older adults developed by Fan et al.21 The FI-28 consists of 28 items about medical conditions (based on professional diagnoses or self-reported physical measurements), symptoms, signs, and other physical indicators. Medical records were used to collect data from F1 to F14. Patients self-reported data from F15 to F24, and trained researchers objectively evaluated data from F25 to F28. The inflammatory biomarker findings of the participants were hidden from the scoring staff to minimize assessment bias. Each item was scored as either 0 (no impairment, ideal state) or 1 (maximum impairment, detrimental state). Using three categories, the FI-28 score was calculated by dividing the total deficit score by 28. A stable (non-frail) condition was denoted by FI ≤0.10 (three or fewer deficits), which denotes minimal stress vulnerability and no significant functional impairment. A pre-frail score of 0.10 < FI < 0.25 (four to six deficits) suggested mild functional decline and an increased risk of developing frailty. A frail score FI ≥0.25 (seven or more deficits) indicated severe multi-system functional impairment and a high risk of disability, hospitalization, or death. FI-28 was validated in Chinese adults and found applicable to hospitalized populations; it utilizes region-specific cutoffs and discriminates frailty-related outcomes (such as hospitalization rate), consistent with the sample’s characteristics.
Inflammatory Biomarkers
EDTA-K2 anticoagulant tubes were used to collect plasma samples, which were used to detect IL-6, IL-10, and TNF-α. Using conventional plain tubes, serum samples were collected to detect hs-CRP. To separate the plasma of IL-6, IL-10, and TNF-α, centrifugation was conducted for 20 min at 2,000 to 4,000 rpm. Consequently, centrifugation was conducted for 10 ti 15 min at 3,000 to 4,000 rpm to separate the serum of hs-CRP. All centrifugation procedures were conducted at room temperature to avoid sample degradation.
To ensure sample stability, all samples were processed and analyzed immediately. Within 4 h after blood collection, plasma processing and detection were completed for IL-6, IL-10, and TNF-α. If immediate detection was not possible, the separated plasma was stored between 2°C and 8°C and examined within 24 h. To avoid result bias caused by prolonged sample storage, serum separation for hs-CRP was completed within 2 h of blood collection and detection within 4 h.
Separated plasma samples for IL-6, IL-10, and TNF-α were stored between 2°C and 8°C for a maximum of 24 h. Additionally, serum samples for hs-CRP were stored between 2°C and 8°C for a maximum of 3 days. Samples were protected from light and kept out of frequent freeze–thaw cycles to prevent biomarker degradation during storage.
A FACSCanto II flow cytometer (BD Biosciences, San Jose, CA, USA) was used to measure IL-6, IL-10, and TNF-α. The Siemens BN ProSpec specific protein analyzer (Siemens Healthineers, Erlangen, Germany), a fully automated platform designed for precise serum protein measurement was used for the hs-CRP assay.
The enzyme-linked immunosorbent assay principle was used to detect TNF-α, IL-6, and IL-10. Before each assay, reagent-matched calibrators, which could be traced to international standards (eg, World Health Organization/National Institute for Biological Standards and Control reference materials), were used for calibration. Using the calibrators included in the kit, multi-point calibration was conducted for hs-CRP in accordance with the instrument operation manual. Samples with severe hemolysis or lipemia were excluded. The supplementary materials (Table S3) describe the limit of detection (LOD), dynamic range, assay platform, manufacturer, and intra- as well as inter-batch coefficients of variation (CV) for the detection of biomarker samples.
Data Collection and Quality Control
Eight qualified research staff, including five registered nurses and three registered nurses with at least 2 years of geriatric research experience, collected the data. Registered nurses collected sociodemographic information and medical history from electronic medical records; experienced nurses conducted interviews with patients and their families to measure frailty; and certified laboratory technicians detected biomarkers.
All staff completed a 2-h standardized training session encompassing research protocols, tool operation, ethical compliance, and data entry. Three steps were used to implement quality control:
- Daily on-site supervision: Ten percent of daily data was reviewed by a senior nurse for completeness/consistency, and any problems were resolved within 24 h.
- Data entry was conducted weekly, after two staff members double-checked and verified the information. To promptly verify any data with uncertainties or missing values, the patients, their families, or electronic medical records were consulted.
- Monthly meetings: After recording minutes and providing retraining for non-compliance, the team examined 20% of the monthly data for protocol adherence.
Only first-admission data were included for patients who were hospitalized more than once. Within 24 h after admission, anthropometric measurements (height, weight, and waist/hip circumference) were recorded using calibrated equipment in a standardized environment (flat floor, good lighting).
- Height was measured twice (average used; third measurement if difference >0.5 cm) using a wall-mounted stadiometer (Seca 213, ±0.1 cm).
- Weight was measured twice using a digital scale (Tanita BC-418, ±0.1 kg), which was tared before use. A third measurement was taken if the difference was >0.3 kg, and the average weight was considered.
- Waist/hip circumference was measured twice at standard anatomical sites (average used), using a non-elastic tape (Seca 201, ±0.1 cm).
Using approved standards, the instruments were calibrated regularly (scale weekly, stadiometer/tape monthly). BMI was calculated as the weight (kg) divided by the height2 (m2). Samples or variables with >5% missing data were excluded, and extreme values were flagged during data entry. To reduce detection bias, laboratory staff were blinded to clinical data.
Ethical Considerations
Taizhou First People’s Hospital’s Ethics Committee licensed our experiment (approval number: 2024-KY044-01). Informed consent was obtained from the patients or their family members who participated in our study. Participants were assured of the confidentiality of their responses, with all data anonymized and securely stored according to ethical guidelines. This study complies with the principles outlined in the Declaration of Helsinki.
Statistical Analysis
Missing data were evaluated at both patient and variable levels. Data were excluded at the patient level if the overall missing rate of the key variables (inflammatory biomarkers, FI score, and covariates) was >5%. Data were excluded at the variable level if the missing rate across all patients was >5% (no variables exceeded this threshold). Multiple imputations by chained equations were used to account for missing data. Natural logarithmic transformation (ln) was applied to inflammatory markers, such as IL-6, hs-CRP, TNF-α, and IL-10, because of the large outliers. The ln-transformed scale was standardized for the entire sample (not stratified by sex) to ensure consistent effect size interpretation. Sex stratification was used in descriptive analyses. The Shapiro–Wilk test was conducted for normality. For normally distributed data, we show that continuous variables as mean ± standard deviation; for non-normally distributed data, we show them as interquartile range (IQR). For categorical variables, we used frequency as well as percentage.
We compared normalized continuous variables via the t-test and non-normally distributed continuous variables via the Mann–Whitney U-test. When necessary, we carried out Fisher’s exact tests or chi-square tests to compare categorical data. We considered variables showing significant variances between women as well as men as potential confounders and adjusted them in subsequent models. Sex-specific associations between inflammatory markers and frailty were examined using stratified logistic regression. We considered frailty (binary) the dependent variable, but inflammatory markers as the primary independent variables. According to a pre-established protocol, the variables included in logistic regression models were prespecified (not data-driven). Selection was based on three criteria: theoretical relevance, literature support, and clinical relevance. Age, sex, alcohol consumption, smoking history, educational level, residence, BMI, comorbidities, and polypharmacy were the final predetermined factors. No data-driven selection methods were used.
All logistic regression models used frailty (binary: 1 = frail, 0 = non-frail) as the dependent variable (Y), with the general equation:
Logit(P(Y=1)) = β0 + β1X1 + β2X2 +……+ βKXK
- Crude model: Logit(P(Y=1)) = β0 + β1 ×Biomarker
- Model 1 (adjusted for age and sex): Logit(P(Y=1)) = β0 + β1 × Biomarker + β2 × Age + β3 ×Sex
- Model 2 (Sex interaction model): Logit(P(Y=1)) = β0 + β1 × Biomarker + β2 × Sex + β3 × (Biomarker × Sex) + ƩβK × covariates (age, alcohol, smoking, education, residence, BMI, comorbidity, polypharmacy)
We carried out the interaction test to find whether the link between the predictor (inflammatory marker) and result (frailty) varies between sexes. For this test, the term sex was combined with each inflammatory marker, and all covariates were included to ensure the unbiasedness and scientific validity. We found a statistically significant sex-based variance if the p-value was <0.05. The coefficient β3 of the interaction term reflects the sex difference in the association between frailty and biomarkers: exp(β3) is the ratio of ORs (women/men). This association varies by sex, as indicated by a significant β3 (p<0.05). The study protocol’s hypotheses served as the basis for all analyses. Because this study was hypothesis-driven rather than exploratory and involved non-independent tests, yielding few successful tests, multiple testing correction was not conducted.20,22 RStudio 4.3.2 (Posit, PBC, Boston, MA, USA) was used to conduct statistical analyses. Additionally, Microsoft Visio Drawing was used to design the STROBE flowchart and the forestplot utility in RStudio to generate the forest plots.
Results
The analyses included 4,438 older inpatients (age: 65–105 years, mean age: 76.44 ± 7.73 years), of whom 2,320 were men (52.28%) and 2,118 were women (47.72%). Frailty was present in 22.8% older women and 37.68% older men (Table 1). The flowchart of participant recruitment and enrollment is shown in Figure 1. The frailty rate was 14.88% points higher in women than in men (37.68% vs 22.8%). After controlling for age, this absolute difference remained significant (adjusted prevalence difference: 14.24%), indicating that women are affected disproportionately. Additionally, women with frailty had higher upper limit values of hs-CRP, IL-6, and IL-10 than men with frailty (hs-CRP: 422.36 vs 339.06, IL-6:6742.9 VS 5435.84, IL-10: 1503.04 VS 903.61) (Table 2, The boxplot is shown in Figure S1).
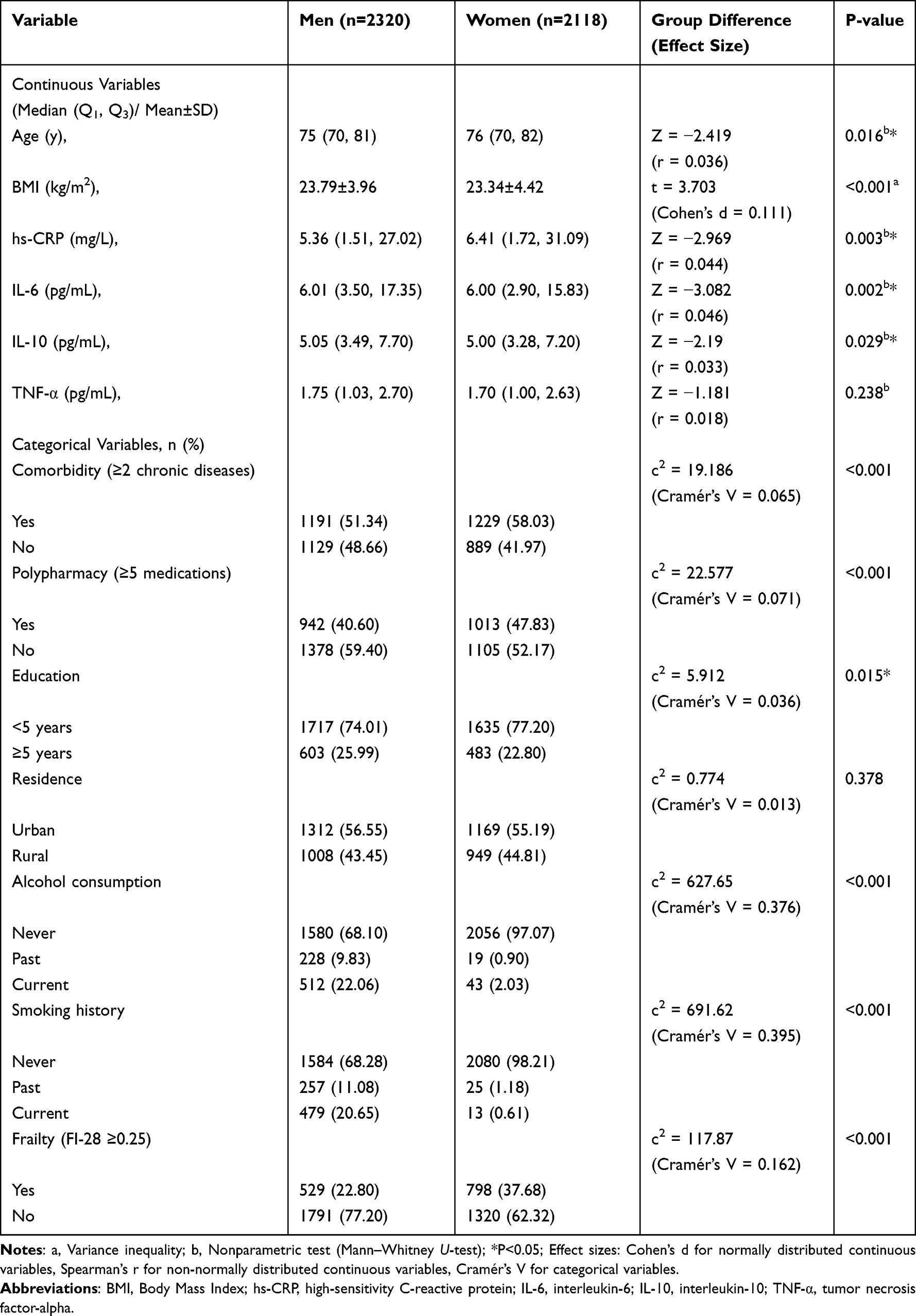 |
Table 1 All Baseline Characteristics and Intergroup Differences Between the Men and Women Groups |
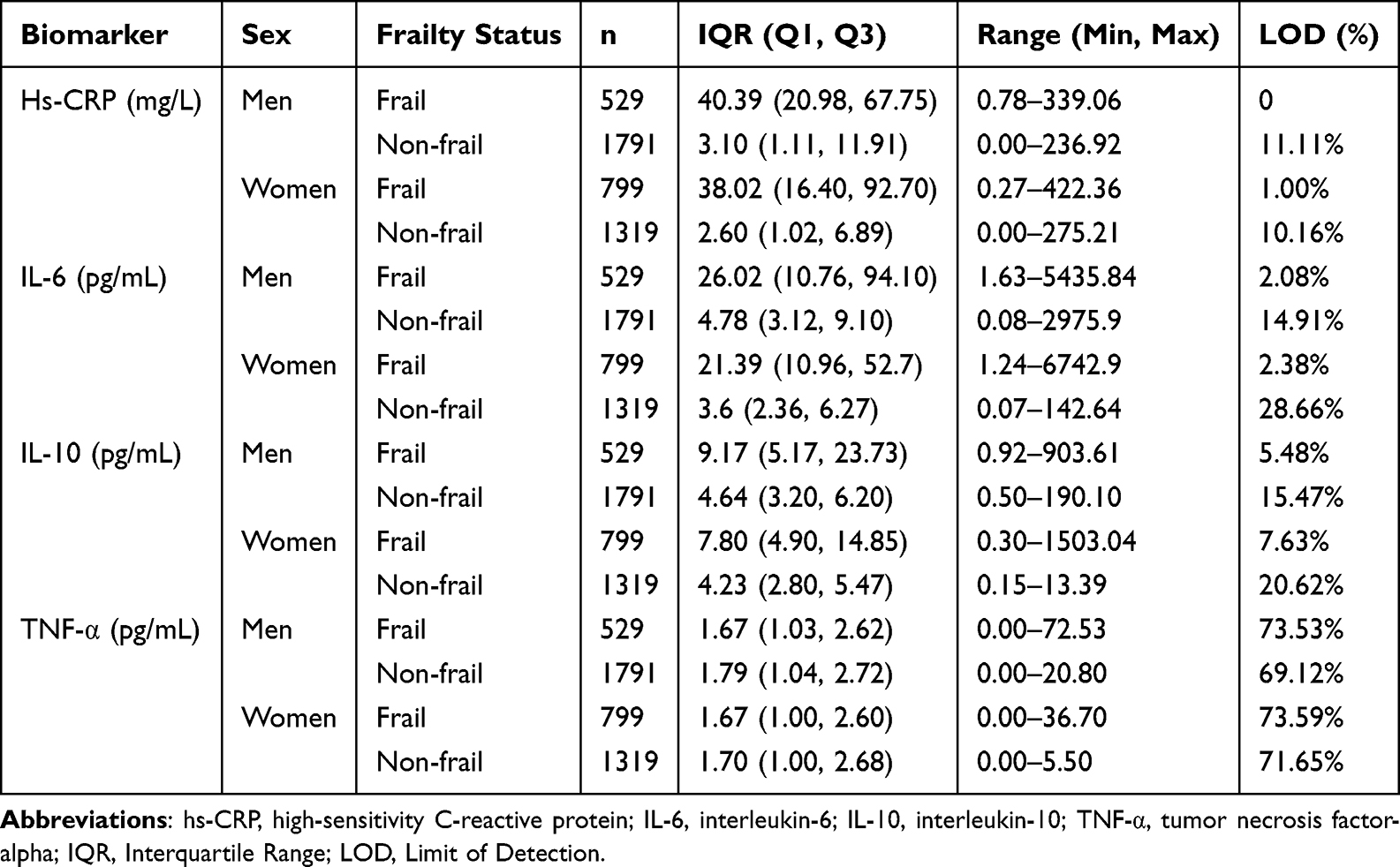 |
Table 2 Descriptive Statistics of Inflammatory Biomarkers Stratified by Sex and Frailty Status |
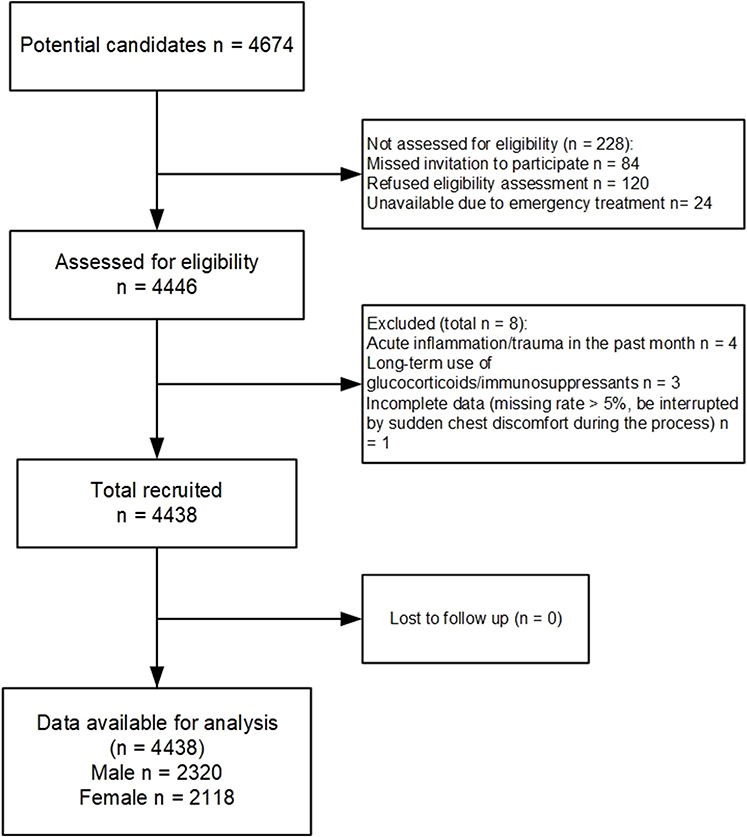 |
Figure 1 STROBE Flowchart of Participant Recruitment and Enrollment. |
We found that elevated IL-6, hs-CRP, and IL-10 (P < 0.05) levels were significantly linked to frailty, according to the non-adjusted regression model. When age as well as sex were taken into account, this link was still statistically significant (Table 3). The AUC values of the model 1 range from 0.7 to 0.903, and the VIF values range from 1.001 to 1.09. No association was noted between TNF-α (P > 0.05) and frailty risk.
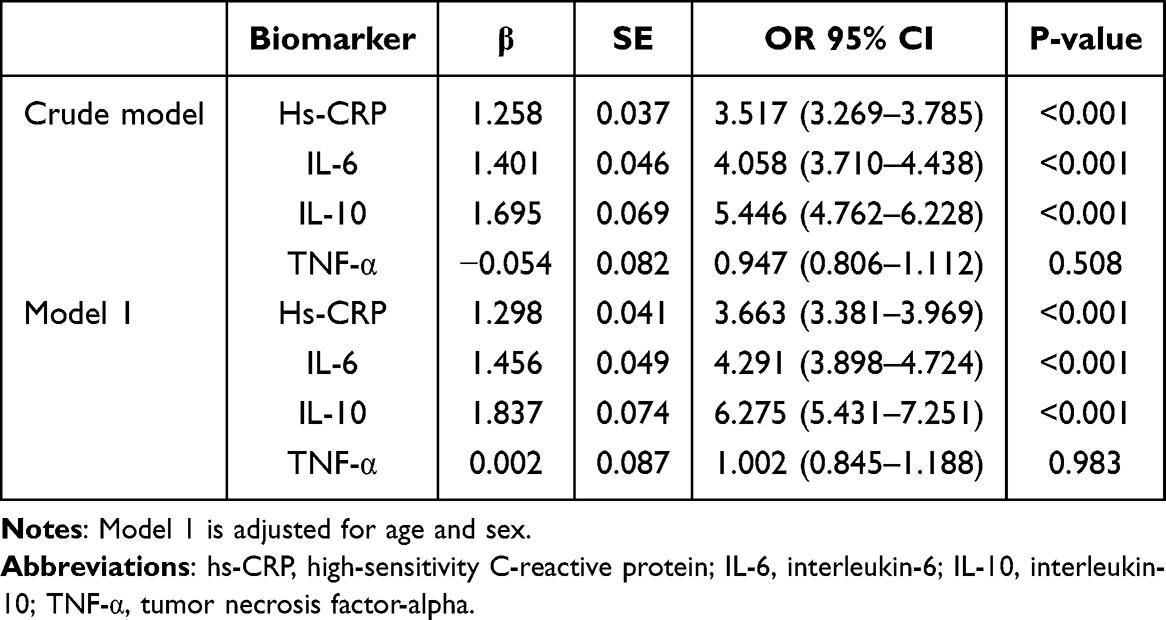 |
Table 3 Association Between Inflammatory Biomarkers and Frailty in the Entire Sample (N = 4438) |
Men and women differed significantly in IL-6 (aOR 95% CI: 2.906 (2.321–3.639), P < 0.001), hs-crp (aOR 95% CI: 1.394 (1.166–1.667), P < 0.001), and IL-10 (aOR 95% CI: 2.4 (1.771–3.307), P < 0.001) as shown by the interaction test (Table 4). The AUC values of the interaction model range from 0.739 to 0.888, and the VIF values range from 1.852 to 3.652.
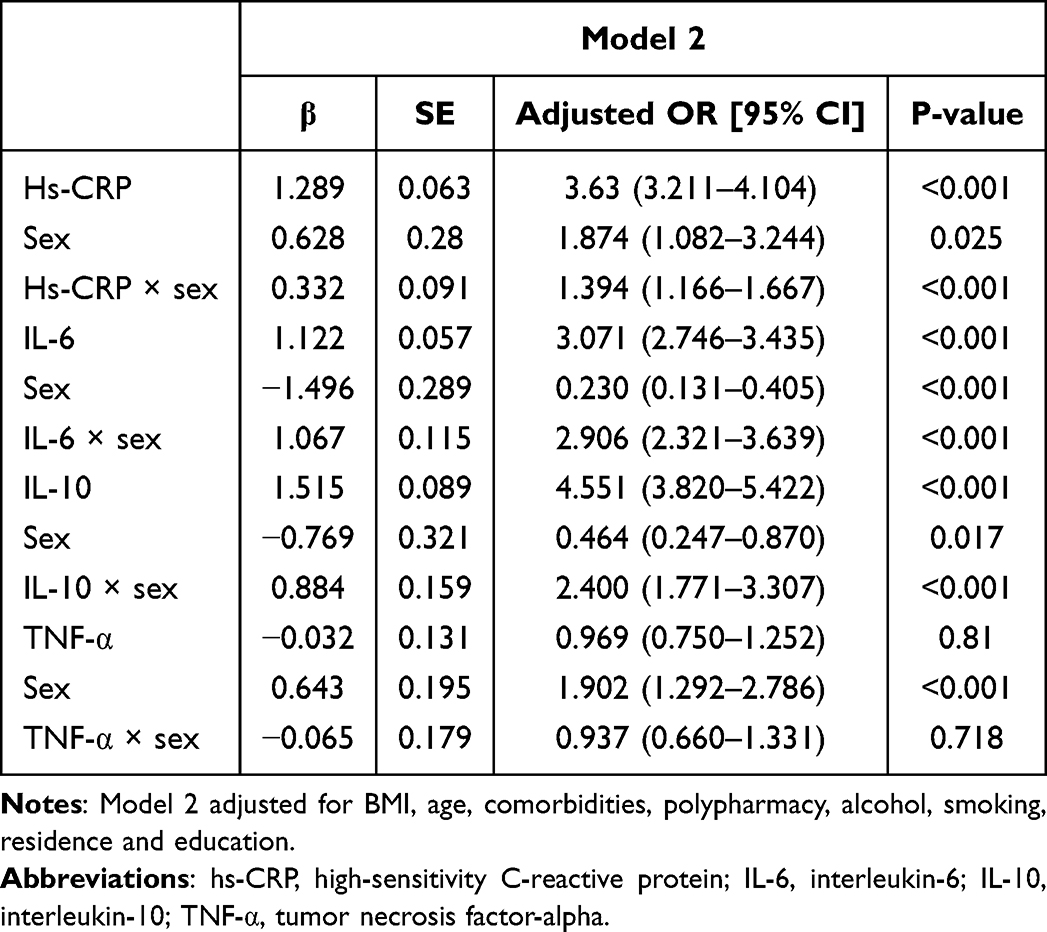 |
Table 4 Interaction Analysis Between Inflammatory Biomarkers and Frailty Status (n = 4438) |
Spearman correlation coefficients were used to assess pairwise correlations among hs-CRP, IL-6, IL-10, and TNF-α. The findings of statistical analysis were as follows: hs-CRP had correlation coefficients of 0.611 (P < 0.05), 0.401 (P < 0.05), and 0.003 (P > 0.05) with IL-6, IL-10, and TNF-α, respectively. IL-6 had correlation coefficients of 0.551 (P < 0.05) and 0.006 (P > 0.05) with IL-10 and TNF-α, respectively. IL-10 and TNF-α had a correlation coefficient of 0.339 (P < 0.05).
We discovered a significant relationship of IL-6, hs-CRP, and IL-10 with sex (P interaction < 0.001). To find the correlation degree between frailty risk and IL-6, hs-CRP, and IL-10 levels in older women as well as men, we carried out a stratified analysis. For men, the frailty risk increased 3.725 times for every standard deviation rise in hs-CRP (aOR = 3.725; 95% CI: 3.275–4.236; P < 0.001). The risk increased 4.937 times in women with the same hs-CRP rise (aOR = 4.937; 95% CI: 4.318–5.644; P < 0.001). Comparable tendencies were observed for IL-6 and IL-10, with both markers showing a significantly greater impact on frailty risk in women than in men (Table 5 and Figure 2). For the sex-stratified models, the AUC values range from 0.845 to 0.923, and the VIF values range from 1.027 to 1.108. The significantly higher aOR in women, along with the non-overlapping confidence intervals, suggests a stronger association between hs-CRP, IL-6, and IL-10 and frailty in older women compared to men.
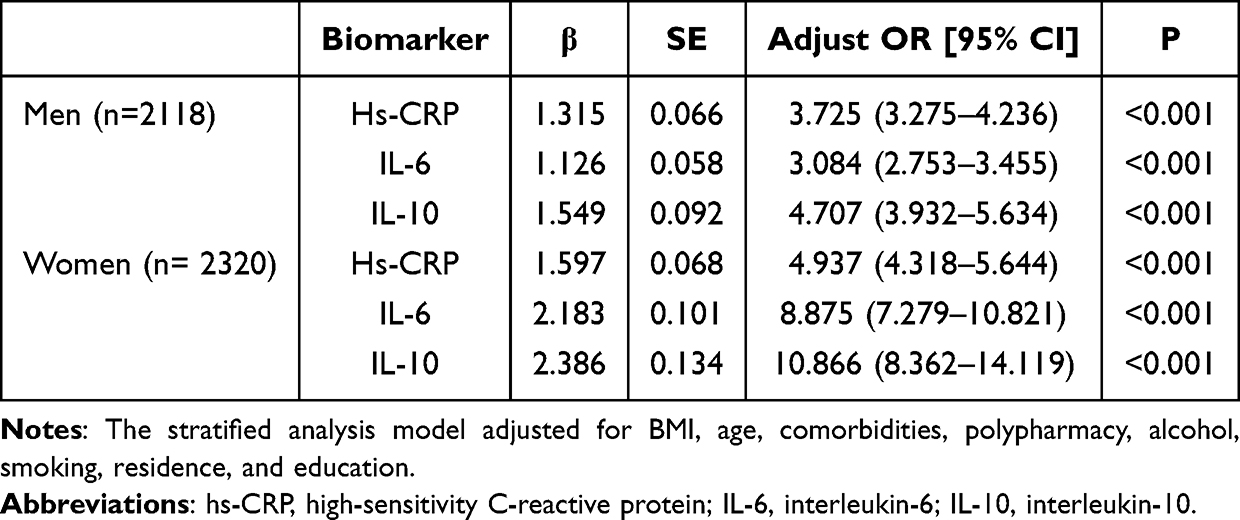 |
Table 5 Relationship of Inflammatory Markers with Frailty Risk in Men and Women Groups |
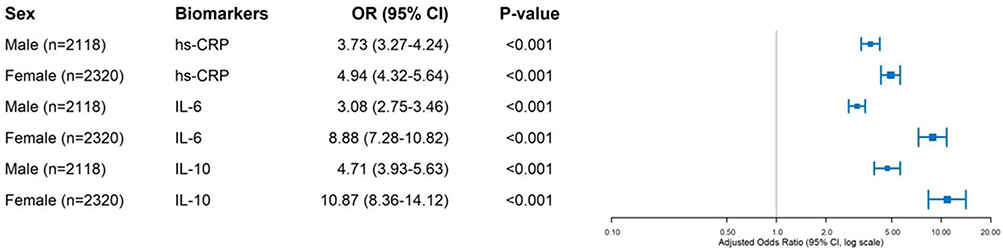 |
Figure 2 Forest plots of the association between inflammatory markers and frailty risk in men and women populations. Abbreviations: BMI, Body Mass Index; hs-CRP, high-sensitivity C-reactive protein; IL-6, interleukin-6; IL-10, interleukin-10; TNF-α, tumor necrosis factor-alpha; FI-28, The 28-item Frailty Index; aORs, adjusted odds ratios; SD, standard deviation; IIS, Inflammatory Index Score; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; LOD, limit of detection; CV, coefficients of variation. |
The odds ratios (ORs) for the associations between IL-6, IL-10, and frailty were particularly high among older women: 8.875 (95% CI: 7.279–10.821) for IL-6 and 10.866 (95% CI: 8.362–14.119) for IL-10. Therefore, this study further analyzed the sex-specificity of inflammatory biomarkers in patients with frailty by using quartile-stratified analysis to convert continuous biomarkers into categorical variables (Q1–Q4 vs Q1). Across all quartile groups (Q2–Q4) of IL-6 and IL-10, the adjusted ORs for women were 19.4%–34.7% (for IL-6) and 40.6%–61.0% (for IL-10) of those for men, with no overlap in their 95% CIs. Thus, there is a higher correlation between frailty risk and inflammatory biomarkers in women at the same inflammatory level (Table 6).
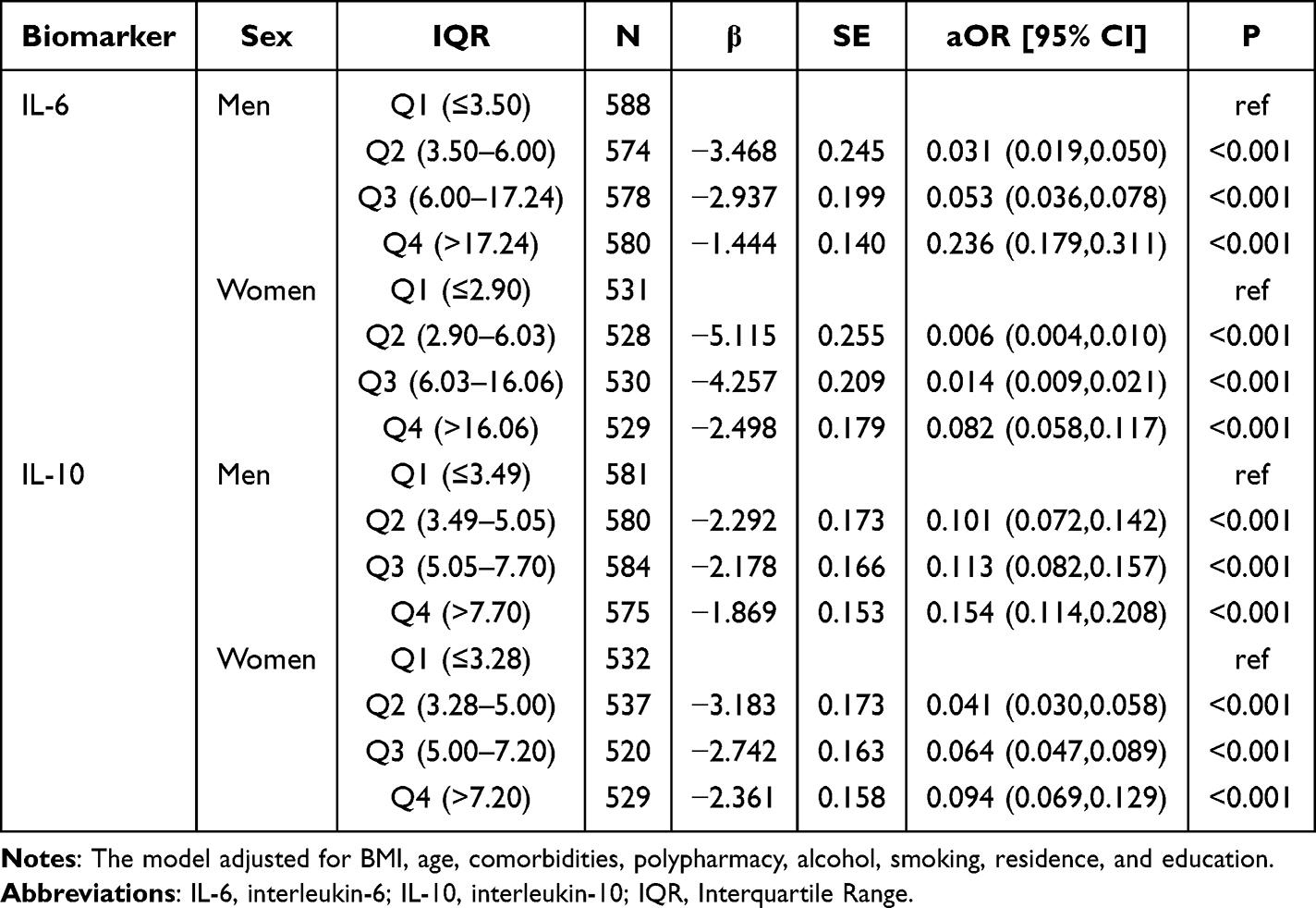 |
Table 6 Association Between Quartiles of Inflammatory Biomarkers and Frailty, Stratified by Sex |
Discussion
Frailty is a prevalent as well as intricate geriatric syndrome that increases the risk of hospitalization, disability, and death in older adults by reducing physiological reserve and making them more susceptible to stressors. Current frailty assessments mainly focus on visible signs like sarcopenia and slow gait, overlooking internal biological changes that may lead to an early diagnosis. Thus, the World Health Organization has created the Integrated Care for Older Persons (ICOPE) guidelines to promote healthy aging, highlighting the importance of early frailty detection and prevention. Biomarkers could be used to detect the underlying physiological damage that occurs before physical symptoms appear. Current research has not sufficiently examined sex-specific differences in the relationship of inflammatory biomarkers with frailty development, despite the fact that this relationship has been thoroughly explored. Therefore, our purpose was to methodically look into the sex-specific relationships of inflammatory biomarkers with frailty in older adults, to better understand how sex influences these relationships and to inform more tailored approaches to frailty management. To our knowledge, this study adds to evidence highlighting sex as a potential effect modifier in the inflammation-frailty association, complementing prior findings of sex-specific inflammatory patterns in older adults.
We found a higher frailty prevalence than what He et al reported (8% for men, 11% for women), likely due to the hospitalized status of our older participants, who generally have poorer physical function and physiological reserves than community-dwelling older adults. Differences in frailty assessment tools may also contribute to variability. When we took BMI, age, and comorbidities into account, higher IL-6, hs-CRP, and IL-10 levels were significantly linked to raised frailty risk (p < 0.001), but TNF-α was not (p > 0.05). Although their function as “predictive biomarkers” needs to be confirmed in longitudinal research, hs-CRP, IL-6, and IL-10 are related to frailty, in line with previous cross-sectional studies.11,12,23–25 Elevated IL-6 levels are associated with a higher risk of frailty, and preclinical studies suggest a potential mechanism via disrupted insulin signaling, increased inflammatory protein production, and impaired muscle homeostasis—though our cross-sectional design cannot confirm this causal pathway.26 It causes muscle breakdown by means of the mitogen-activated protein kinase pathway as well as the nuclear factor kappa-light-chain-enhancer of activated B cells.27,28 Interestingly, despite IL-10’s well-established anti-inflammatory function, it was positively linked to frailty, in contrast to its known anti-inflammatory role. We speculate that chronically elevated IL-10 may impair immune regulation and trigger muscle catabolism via the ubiquitin–proteasome system, matching what Wang et al reported, ie, that high IL-10 levels predicted reduced grip strength.29 The lack of association with TNF-α may be due to low baseline levels and limited variation. The weak correlation of TNF-α with other markers further explains its non-significant association with frailty, as it may act through distinct biological pathways not overlapping with hs-CRP, IL-6, or IL-10. Additionally, interventions targeting frailty often reduce CRP and IL-6 but have little effect on TNF-α, suggesting distinct biological roles.23 Despite its non-significant association with this study, TNF-α remains a relevant cytokine for the development of frailty and requires further investigation.
In our study, women showed greater frailty incidence than men (37.68% vs 22.8%), which is in line with previous experiments.30,31 More importantly, even after we controlled for confounding variables, women showed a stronger link of frailty with IL-6, hs-CRP, and IL-10 than did men. Combined with the quartile analysis results of IL-6 and IL-10, these findings also confirm that the associations of IL-6 and IL-10 with frailty in older women are significantly stronger than those in older men. Our Spearman correlation analysis revealed strong associations between hs-CRP, IL-6, and IL-10 (range: 0.401–0.611), which aligns with previous studies showing coordinated activation of pro-inflammatory and regulatory inflammatory pathways in frailty.9,18,23 Importantly, the VIF values for all biomarkers were <10, indicating no severe multicollinearity. This validates the stability of our multivariate logistic regression models. Kane et al also conducted a study on mice and found a sex-specific relationship of frailty with pro-inflammatory cytokines, suggesting that this link is weaker in male mice than in female mice.14 However, higher inflammation levels only provide a partial explanation for the higher incidence of frailty in women.32 Women are much more likely than men to be frail, which is likely due to variations in body composition, hormones, mitochondrial function, and epigenetic regulation.
After menopause, women experience a rapid decline in estrogen levels. Estrogen is a key protective factor that maintains DNA methylation homeostasis and histone acetylation by regulating epigenetic enzymes such as sirtuin 1. Its abrupt decline accelerates genome-wide hypomethylation, X chromosome inactivation escape, and upregulation of pro-inflammatory non-coding RNA expression during the aging process in women, leading to immune homeostasis disruption.33 Concurrently, estrogen deficiency impairs mitochondrial function through two key pathways: inhibition of the “estrogen-related receptor alpha–peroxisome proliferator-activated receptor gamma coactivator 1-alpha” pathway, which lowers mitochondrial biogenesis. PTEN-induced putative kinase 1/Parkin RBR E3 ubiquitin protein ligase (PINK1/Parkin)-mediated mitochondrial autophagy pathway disruption causes damaged mitochondria to accumulate and reactive oxygen species (ROS) to burst.34,35 The aforementioned epigenetic disorders and mitochondrial dysfunction form a cascading amplification effect. Through the cGAS-STING pathway, mitochondrial DNA (mtDNA) release triggers innate immunity, while the secretion of ROS promotes NLRP3 inflammasome assembly.34,35 Collectively, this results in the elevation of systemic inflammation levels, particularly CRP and IL-6, in women. Disparities in hormone levels as well as control also have unique, sex-specific effects on frailty. Some age-related diseases linked to frailty are made more likely by the fact that testosterone increases the effects of growth hormone while estrogen decreases hepatic sensitivity to it.36–38
Women who have higher body fat percentages alongside less muscle mass may be more prone to frailty as well as inflammation. Reduced muscle offers less anti-inflammatory support, while excess fat, especially around the abdomen, releases inflammatory markers.37,39,40 This chronic inflammation can speed up muscle loss and impair physical function, creating a cycle that promotes frailty. Behavioral sex differences may cause more frailty in women, as reporting health problems and seeking medical attention are more common among women.41 In addition, sex chromosomes may also contribute to higher inflammatory levels in women. Women may overexpress certain genes linked to inflammation, especially X chromosome ones.36,42–44 Our hypothesis is that sex differences associated with inflammation may lie at the intersection of multiple factors, including genetic inheritance, immune cells, and social behavior, with multiple factors acting together to cause sex differences in inflammatory markers in frail older patients.
Notably, endothelial dysfunction (ED) is a major mediator of inflammation and downstream adverse clinical events, particularly severe cardiac events.45,46 Specifically, elevated inflammatory markers, such as IL-6, hs-CRP, and IL-10, do not directly induce frailty-related adverse outcomes. Instead, by blocking nitric oxide signaling and causing phenotypic shifts toward proinflammatory and prothrombotic states, they disrupt endothelial homeostasis.45 Compared with individuals with normal endothelial function, older adults with frailty having both elevated inflammation and ED are 3.8 times more likely to experience adverse cardiac events.46 Considering the association between inflammation and frailty and the potential poor prognosis of frailty, future management of inflammation-related frailty should concurrently focus on endothelial function and sex-specific ED differences.
These findings highlight the relevance of considering sex differences when investigating the association between inflammation and frailty in hospitalized older adults. Future studies into the sex-specific biological processes causing frailty may be guided by the stronger associations between hs-CRP, IL-6, IL-10 and frailty in women than in men. However, because the clinical utility of inflammatory biomarkers (eg, for frailty screening or monitoring) needs to be validated in prospective cohorts, including determining whether these biomarker predict incident frailty or response to interventions, their utility cannot be concluded from this cross-sectional study. Before assessing sex-specific screening pathways or setting clinical thresholds, future research should use longitudinal designs to confirm the temporal relationship between these inflammatory markers and frailty progression.
This study has several limitations. First, convenience sampling from three distinct hospital departments introduced selection bias, possibly overrepresenting older adults with chronic diseases and overestimating the association between inflammation and frailty. Individuals with healthy cognition but physical impairment and at a high risk of frailty may have been excluded because of the need for strong communication skills. Second, because frailty and cognitive impairment overlap inflammatory pathways (eg, IL-6-mediated neuroinflammation), excluding participants with cognitive impairment may underestimate associations. Additionally, cognitive status was eliminated as a potential modifier of the inflammation-frailty association. Third, single-timepoint biomarker assessments did not capture dynamic inflammatory changes (eg, from subclinical infections or hospital stress) or tissue-specific inflammation (eg, muscle inflammation), which more directly contribute to frailty-related muscle atrophy. Fourth, potential batch effects during 10-month biomarker detection (eg, reagent lot differences, instrument calibration) may introduce systematic bias, particularly for low-concentration markers (TNF-α), and distort sex differences. Fifth, there is still incomplete medication confounding adjustment. Despite excluding individuals under glucocorticoids or immunosuppressants, we only adjusted for polypharmacy (binary) rather than specific anti-inflammatory drugs (eg, nonsteroidal anti-inflammatory drugs and statins) that lower hs-CRP/IL-6, which might cause residual confounding. Additional residual factors include sex hormones, lifestyle habits, and environmental influences, among others. Sixth, the cross-sectional design precludes the validation of sex-specific inflammatory thresholds for predicting frailty progression and causal inference (ie, differentiating inflammation as a cause versus a consequence of frailty). Finally, mechanistic interpretation of sex differences in inflammation is limited by insufficient information on genetic/epigenetic markers and sex hormones (eg, estradiol). To overcome these limitations, future studies should use multi-center sampling, increase the sample size across age groups, include individuals with cognitive impairment, use repeated biomarker measurements (with batch effect correction), account for specific medications, and conduct longitudinal follow-up.
Conclusion
In this study, cross-sectional data identified sex-specific associations between inflammatory biomarkers (IL-6, hs-CRP, and IL-10) and frailty in older adults. Elevated levels of IL-6, hs-CRP, and IL-10 were significantly associated with frailty in both sexes after controlling for potential confounders. However, these associations were stronger in older women than in older men, indicating that sex may modify the mentioned association.
These findings provide a biological rationale for sex-specific therapeutic strategies in frailty management: Even before overt physical symptoms manifest, proactive monitoring of hs-CRP, IL-6, and IL-10 in older women (eg, yearly screening in hospitalized or high-risk community-dwelling women) may help identify early frailty risk. Researchers may explore whether anti-inflammatory approaches differ in their efficacy by sex. For example, they may investigate whether women benefit more from IL-6-targeted interventions because of their stronger association with frailty.
Notably, because this cross-sectional design could not confirm causality or intervention efficacy, these therapeutic applications need to be validated in longitudinal and interventional research. Nevertheless, however, to advance individualized treatment for older adults, these results necessitate incorporating sex differences into frailty research and clinical practice, extending beyond a “one-size-fits-all” approach. To validate sex-specific inflammatory thresholds for frailty risk, evaluate the effectiveness of sex-specific interventions, and determine the temporal direction of the inflammation-frailty association, future research should prioritize longitudinal follow-up. Finally, these findings should be translated into actionable recommendations for geriatric care and precision medicine.
Data Sharing Statement
The data of this study are available on request from the corresponding author (Dan Xu). The data are not publicly available due to privacy or ethical restrictions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Taizhou University Nursing Discipline Development Special Fund Project (grant number: 202212 and grant number: 202206) and Zhejiang Provincial Medical and Health Science and Technology Plan (grant number: 2025KY1857).
Disclosure
The authors report no conflicts of interest in this work.
References
1. O’Caoimh R, Sezgin D, O’Donovan MR, et al. Prevalence of frailty in 62 countries across the world: a systematic review and meta-analysis of population-level studies. Age Ageing. 2021;50(1):96–104. doi:10.1093/ageing/afaa219
2. World Health Organization. Ageing. Available from: Https://www.who.int/health-topics/ageing#tab=tab_1.
3. Sargent L, Nalls M, Singleton A, et al. Moving towards the detection of frailty with biomarkers: a population health study. Aging Cell. 2024;23(2):e14030. doi:10.1111/acel.14030
4. RSDSA G, Ácc M, Rolland Y, Vellas B, de Souto Barreto P. Frailty biomarkers under the perspective of geroscience: a narrative review. Ageing Res Rev. 2022;81:101737. doi:10.1016/j.arr.2022.101737
5. Angulo J, El Assar M, Álvarez-Bustos A, Rodríguez-Mañas L. Physical activity and exercise: strategies to manage frailty. Redox Biol. 2020;35:101513. doi:10.1016/j.redox.2020.101513
6. Xu Y, Wang M, Chen D, Jiang X, Xiong Z. Inflammatory biomarkers in older adults with frailty: a systematic review and meta-analysis of cross-sectional studies. Aging Clin Exp Res. 2022;34(5):971–987. doi:10.1007/s40520-021-02022-7
7. Kristensen TN, Loeschcke V, Tan Q, Pertoldi C, Mengel-From J. Sex and age specific reduction in stress resistance and mitochondrial DNA copy number in Drosophila melanogaster. Sci Rep. 2019;9(1):12305. doi:10.1038/s41598-019-48752-7
8. Tylutka A, Ł W, Zembron-Lacny A. Level of IL-6, TNF, and IL-1β and age-related diseases: a systematic review and meta-analysis. Front Immunol. 2024;15:1330386. doi:10.3389/fimmu.2024.1330386
9. Soysal P, Stubbs B, Lucato P, et al. Inflammation and frailty in the elderly: a systematic review and meta-analysis. Ageing Res Rev. 2016;31:1–8. doi:10.1016/j.arr.2016.08.006
10. Moldovan F. Sterile inflammatory response and surgery-related trauma in elderly patients with subtrochanteric fractures. Biomedicines. 2024;12(2):354. doi:10.3390/biomedicines12020354
11. E TVH, De Glas NA, Portielje JEA, et al. Biomarkers of the ageing immune system and their association with frailty - A systematic review. Exp Gerontol. 2023;176:112163. doi:10.1016/j.exger.2023.112163
12. McKechnie DGJ, Patel M, Papacosta AO, et al. Associations between inflammation, coagulation, cardiac strain and injury, and subclinical vascular disease with frailty in older men: a cross-sectional study. BMC Geriatr. 2022;22(1):405. doi:10.1186/s12877-022-03106-3
13. El Assar M, Rodríguez-Sánchez I, Álvarez-Bustos A, Rodríguez-Mañas L. Biomarkers of frailty. Mol Aspects Med. 2024;97:101271. doi:10.1016/j.mam.2024.101271
14. Kane AE, Howlett SE. Sex differences in frailty: comparisons between humans and preclinical models. Mech Ageing Dev. 2021;198:111546. doi:10.1016/j.mad.2021.111546
15. He L, Yang J, Fang Y. Longitudinal analysis on inflammatory markers and frailty progression: based on the English longitudinal study of aging. Eur Geriatr Med. 2024;15(5):1323–1330. doi:10.1007/s41999-024-00998-9
16. Sampathkumar NK, Bravo JI, Chen Y, et al. Widespread sex dimorphism in aging and age-related diseases. Hum Genet. 2020;139(3):333–356. doi:10.1007/s00439-019-02082-w
17. Feng Z, Liao M, Zhang L. Sex differences in disease: sex chromosome and immunity. J Transl Med. 2024;22(1):1150. doi:10.1186/s12967-024-05990-2
18. Fritzenschaft L, Boehm F, Rothenbacher D, Denkinger M, Dallmeier D. Association of blood biomarkers with frailty-A mapping review. Ageing Res Rev. 2025;109:102761. doi:10.1016/j.arr.2025.102761
19. Wang X, Cheng Z. Cross-sectional studies: strengths, weaknesses, and recommendations. Chest. 2020;158(1S):S65–S71. doi:10.1016/j.chest.2020.03.012
20. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
21. Fan J, Yu C, Guo Y, et al. Frailty index and all-cause and cause-specific mortality in Chinese adults: a prospective cohort study. Lancet Public Health. 2020;5(12):e650–e660. doi:10.1016/S2468-2667(20)30113-4
22. Rothman KJ. No adjustments are needed for multiple comparisons. Epidemiology. 1990;1(1):43–46. doi:10.1097/00001648-199001000-00010
23. Picca A, Coelho-Junior HJ, Calvani R, Marzetti E, Vetrano DL. Biomarkers shared by frailty and sarcopenia in older adults: a systematic review and meta-analysis. Ageing Res Rev. 2022;73:101530. doi:10.1016/j.arr.2021.101530
24. Tembo MC, Holloway-Kew KL, Bortolasci CC, et al. Association between serum interleukin-6 and frailty in older men: cross-sectional data. Eur Geriatr Med. 2021;12(4):887–892. doi:10.1007/s41999-021-00490-8
25. Zeng M, Li Y, Zhu Y, Sun Y. Inflammatory markers and clinical factors as key independent risk factors for frailty: a retrospective study. BMC Geriatr. 2025;25(1):404. doi:10.1186/s12877-025-06033-1
26. Samson LD, Buisman AM, Ferreira JA, et al. Inflammatory marker trajectories associated with frailty and ageing in a 20-year longitudinal study. Clin Transl Immunology. 2022;11(2):e1374. doi:10.1002/cti2.1374
27. Marcos-Pérez D, Sánchez-Flores M, Proietti S, et al. Association of inflammatory mediators with frailty status in older adults: results from a systematic review and meta-analysis. Geroscience. 2020;42(6):1451–1473. doi:10.1007/s11357-020-00247-4
28. Zhang L, Zeng X, He F, Huang X. Inflammatory biomarkers of frailty: a review. Exp Gerontol. 2023;179:112253. doi:10.1016/j.exger.2023.112253
29. Wang C, Wang J, Wan R, Kurihara H, Wang M. The causal association between circulating cytokines with the risk of frailty and sarcopenia under the perspective of geroscience. Front Endocrinol. 2024;15:1293146. doi:10.3389/fendo.2024.1293146
30. Gordon EH, Peel NM, Samanta M, Theou O, Howlett SE, Hubbard RE. Sex differences in frailty: a systematic review and meta-analysis. Exp Gerontol. 2017;89:30–40. doi:10.1016/j.exger.2016.12.021
31. Corbi G, Cacciatore F, Komici K, et al. Inter-relationships between sex, frailty and 10-year survival in older italian adults: an observational longitudinal study. Sci Rep. 2019;9(1):18416. doi:10.1038/s41598-019-54897-2
32. Pothier K, Gana W, Bailly N, Fougère B. Associations between frailty and inflammation, physical, and psycho-social health in older adults: a systematic review. Front Psychol. 2022;13:805501. doi:10.3389/fpsyg.2022.805501
33. Herbst A, Prior SJ, Lee CC, et al. Skeletal muscle mitochondrial DNA copy number and mitochondrial DNA deletion mutation frequency as predictors of physical performance in older men and women. Geroscience. 2021;43(3):1253–1264. doi:10.1007/s11357-021-00351-z
34. Hägg S, Jylhävä J. Sex differences in biological aging with a focus on human studies. Elife. 2021;10:e63425. doi:10.7554/eLife.63425
35. Furman D, Campisi J, Verdin E, et al. Chronic inflammation in the etiology of disease across the life span. Nat Med. 2019;25(12):1822–1832. doi:10.1038/s41591-019-0675-0
36. Olivieri F, Marchegiani F, Matacchione G, et al. Sex/sex-related differences in inflammaging. Mech Ageing Dev. 2023;211:111792. doi:10.1016/j.mad.2023.111792
37. Park C, Ko FC. The science of frailty. Sex Differences Clin Geriatr Med. 2021;37(4):625–638. doi:10.1016/j.cger.2021.05.008
38. Ostan R, Monti D, Gueresi P, Bussolotto M, Franceschi C, Baggio G. sex, aging and longevity in humans: an update of an intriguing/neglected scenario paving the way to a sex-specific medicine. Clin Sci. 2016;130(19):1711–1725. PubMed: 27555614. doi:10.1042/CS20160004
39. Gheller BJ, Riddle ES, Lem MR, Thalacker-Mercer AE. Understanding age-related changes in skeletal muscle metabolism: differences between females and males. Annu Rev Nutr. 2016;36:129–156. doi:10.1146/annurev-nutr-071715-050901
40. Kent-Braun JA, Ng AV, Young K. Skeletal muscle contractile and noncontractile components in young and older women and men. J Appl Physiol. 2000;88(2):662–668. doi:10.1152/jappl.2000.88.2.662
41. Gordon EH, Hubbard RE. Differences in frailty in older men and women. Med J Aust. 2020;212(4):183–188. doi:10.5694/mja2.50466
42. Gordon EH, Hubbard RE. The Pathophysiology of Frailty: why sex is so important. J Am Med Dir Assoc. 2018;19:4–5. doi:10.1016/j.jamda.2017.10.009
43. Casimir GJ, Duchateau J. sex differences in inflammatory processes could explain poorer prognosis for males. J Clin Microbiol. 2011;49(1):478–479. doi:10.1128/JCM.02096-10
44. Zeidan RS, McElroy T, Rathor L, Martenson MS, Lin Y, Mankowski RT. Sex differences in frailty among older adults. Exp Gerontol. 2023;184:112333. doi:10.1016/j.exger.2023.112333
45. Calila H, Bălășescu E, Nedelcu RI, Ion DA. Endothelial dysfunction as a key link between cardiovascular disease and frailty: a systematic review. J Clin Med. 2024;13(9):2686. PMID: 38731215; PMCID: PMC11084631. doi:10.3390/jcm13092686
46. Prabhahar A, Batta A, Hatwal J, Kumar V, Ramachandran R, Batta A. Endothelial dysfunction in the kidney transplant population: current evidence and management strategies. World J Transplant. 2025;15(1):97458. PMID: 40104196; PMCID: PMC11612885. doi:10.5500/wjt.v15.i1.97458
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Frailty with Patient-Report Outcomes and Major Clinical Determinants in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Yang M, Liu Y, Zhao Y, Wang Z, He J, Wang Y, Anme T
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:907-919
Published Date: 12 April 2024
Yoga Practice as a Potential Sarcopenia Prevention Strategy in Indonesian Older Adults: A Cross-Sectional Study
Meiliana A, Dewi NM, Latarissa IR, Barliana MI, Alfian SD, Yulianti T, Wijaya A
Open Access Journal of Sports Medicine 2025, 16:3-13
Published Date: 10 January 2025
Targeting Cellular Senescence for Healthy Aging: Advances in Senolytics and Senomorphics

Alum EU, Izah SC, Uti DE, Ugwu OPC, Betiang PA, Basajja M, Ejemot-Nwadiaro RI
Drug Design, Development and Therapy 2025, 19:8489-8522
Published Date: 19 September 2025