Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Serum Uric Acid-to-Serum Creatinine Ratio, Thyroid Function, and Gestational Diabetes Mellitus Risk during Early Pregnancy among Chinese Women
Authors Song S ![]() , Duo Y, Zhang Y, Qiao X, Chen Y, Fu Y, Dong Y, Yuan T, Zhao W
, Duo Y, Zhang Y, Qiao X, Chen Y, Fu Y, Dong Y, Yuan T, Zhao W
Received 31 August 2024
Accepted for publication 12 March 2025
Published 7 July 2025 Volume 2025:18 Pages 2235—2246
DOI https://doi.org/10.2147/DMSO.S486695
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Shuoning Song,1 Yanbei Duo,1 Yuemei Zhang,2 Xiaoli Qiao,3 Yan Chen,3 Yong Fu,1 Yingyue Dong,1 Tao Yuan,1 Weigang Zhao1
1Department of Endocrinology, Key Laboratory of Endocrinology of Ministry of Health, Peking Union Medical College Hospital, Chinese Academy of Medical Science and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Obstetrics, Haidian District Maternal and Child Health Care Hospital, Beijing, People’s Republic of China; 3Department of Obstetrics, Beijing Chaoyang District Maternal and Child Health Care Hospital, Beijing, People’s Republic of China
Correspondence: Tao Yuan, Email [email protected]; [email protected] Weigang Zhao, Email [email protected]
Objective: This study aimed to explore the relationship between serum uric acid-to-serum creatinine (UA:SCr) ratio and thyroid function within the normal range and in gestational diabetes mellitus (GDM) during early pregnancy in Chinese women.
Methods: A total of 958 pregnant women were enrolled in this prospective double-center cohort study. Liver function, renal function, and thyroid function were tested during 6– 12 weeks of gestation and oral glucose tolerance tests were conducted for 24– 28 weeks to screen for GDM. Associations between UA:SCr ratio and thyroid function and GDM were examined by linear and logistic regression analyses.
Results: The incidence of GDM was 19.3% (185/958) in this study. UA:SCr ratio and free thyroxine (FT4) were significantly higher in pregnant women with GDM in the highest preBMI quartile than the normal glucose tolerance group (median 5.22, IQR 4.47– 5.87 vs median 4.87, IQR 4.05– 5.61, mean difference − 0.52, P=0.04; median 1.13, IQR 1.02– 1.28 vs median 1.18, IQR 1.07– 1.32, mean difference 0.14, P=0.02). Both UA:SCr ratio and FT4 were associated with risk of GDM in pregnant women in the highest preBMI quartile (RR 0.331, 95% CI 1.094– 1.772, P=0.007; RR − 1.533, 95% CI 0.055– 0.853, P=0.029). For pregnant women in the third and fourth preBMI quartiles, the UA:SCr ratio was significantly correlated with euthyroid function (FT4 and UA:SCr ratio): preBMI quartile 3 — β=0.659, 95% CI 0.231– 1.087), P=0.003; FT4 and UA:SCr ratio in preBMI quartile 4 — β=− 0.263, 95% CI − 0.516 to− 0.011, P=0.041; TSH and UA:SCr ratio in preBMI-quartile 4 — β=0.131, 95% CI 0.008– 0.253, P=0.036. Further analysis revealed that FT4 was associated with risk of GDM in pregnant women in the highest UA:SCr ratio quartile (RR 0.052, 95% CI 1.010– 1.096, P=0.012). There was also an interaction effect between FT4 and UA:SCr ratio in relation to the risk of GDM in the highest UA:SCr ratio quartile (P=0.02).
Conclusion: Both UA:SCr ratio and FT4 were associated with the risk of GDM in early pregnancy, particularly among women in the highest prepregnancy BMI quartile. FT4 level within the normal range was correlated with UA:SCr ratio in women in the third and fourth prepregnancy BMI quartiles. These results suggest the complex interplay of metabolic changes during early pregnancy and provide new insights for the early prevention and management of GDM.
Keywords: pregnancy, uric acid, thyroid function, gestational diabetes mellitus, glucose and lipid metabolism
Introduction
Gestational diabetes mellitus (GDM), one of the most common medical complications of pregnancy, is defined as a state restricted to pregnant women whose impaired glucose tolerance is first discovered during pregnancy.1,2 The International Diabetes Federation (IDF) reported that the pooled global standardized prevalence of GDM was 14% and the regional standardized prevalence of GDM varied from 7.1% to 27.6%.3 GDM not only increases the risk of pregnancy complications and adverse perinatal outcomes such as premature delivery, preeclampsia, and macrosomia but also affects the long-term health of the mother and fetus, leading to a higher risk of metabolic disorders in the future.4,5 Therefore, an increasing number of studies have focused on finding risk factors for GDM that may help predict and prevent GDM.
Serum uric acid (UA) is a water-soluble antioxidant mainly produced by the liver that has been shown to directly inhibit the damage caused by free radicals and also to protect cell membranes.6,7 Elevated UA levels are thought to be an intermediary factor in adipose tissue that regulates endocrine disorders that promote inflammation, and may be an influential factor leading to metabolic disorders.1 Previous studies have reported an association between UA and increased risk of insulin resistance and type 2 diabetes in the general population, but the relationship between UA and risk of GDM is controversial and relatively limited.8,9 Some researchers have claimed that the inconsistent conclusions may be due to differences in renal function since the UA levels might be influenced by SCr, leading to alterations in UA levels independently of metabolic changes, which could affect the interpretation of UA.10 Therefore, the UA:SCr ratio could be a better predictor representing renal function-normalized SUA. The UA:SCr ratio has been reported as an indicator related to metabolic and cardiovascular diseases,11–14 nonalcoholic fatty liver disease,15 risk of stroke recurrence,16 preeclampsia,17,18 adverse pregnancy outcomes,19 and even all-cause mortality.20 However, the relationship between the UA:SCr ratio and GDM remains unclear.
Thyroid function is closely related to metabolism, and thyroid dysfunction during pregnancy can increase the incidence of complications of pregnancy and adverse perinatal outcomes, as well as affect infant thyroid function and growth.21 Recently, several researchers found that different levels of thyroid function, even within normal range, might affect maternal metabolism and infant growth.22 Low thyroid function within the reference range may have a negative effect on cognitive function,23 and a negative association with the risk of GDM was observed for the highest free thyroxine (FT4)-concentration tertile even in normal range.24 However, other researchers have found that pregnancy outcomes are not altered by variation in thyroid function within the normal range in women free of thyroid disease.25
While previous studies have examined the relationship between the UA:SCr ratio and GDM or thyroid function separately, the interplay among these three factors in early pregnancy remains poorly understood. Some studies have pointed to a correlation between thyroid hormone and UA levels, but this correlation remains controversial,26,27 providing a new perspective on our understanding of metabolic interactions and risk of GDM in early pregnancy. Based on these studies, we hypothesized that the UA:SCr ratio and euthyroid function were associated with the risk of GDM and that the interaction between them might contribute to metabolism during early pregnancy. Therefore, this study aimed to investigate the relationship between the UA:SCr ratio, euthyroid function, and the risk of GDM during early pregnancy in a cohort of Chinese women.
Methods
This was a prospective bicenter cohort study started in 2019 in Haidian District Maternal and Child Health Care Hospital and Chaoyang District Maternal and Child Health Care Hospital, Beijing, China. All pregnant women with records in the two hospitals matching the inclusion criteria were asked to take part in the study. For all participants in the present study, all available clinical and laboratory data were recorded and verified by two researchers at the same time.
The ethics committees of all participating centers approved the study protocol. The study was conducted under the guidance of the Major New Drugs Innovation and Development Program (clinical trial NCT03246295). Written informed consent was obtained from each participant, and the study was performed in accordance with the Declaration of Helsinki as revised in 2013.
Study Participants
Inclusion criteria were: (1) gestation age at entry <12 weeks; (2) without DM before pregnancy; and (3) acceptance to participate in the study and a signed consent form. Exclusion criteria were: (1) double or multiple pregnancy; (2) fasting blood glucose ≥5.1 mmol/L at baseline; and (3) any acute or other chronic disease, such as severe liver and renal dysfunction, heart disease, or autoimmune disease.
Sample-size calculations in the primary study were focused on the prediction value of variables for GDM (two-tailed at 5% significance). We required a sample size of 667 (assuming five risk factors and a 15% indication rate of GDM), rising to 741 when allowing for a 10% loss to follow-up. The effect size between the UA:SCr ratio and euthyroid function was considered small based on a previous study. To have 80% power to detect the association between the UA:SCr ratio and euthyroid function, the total sample size calculated was 395 (power 0.8, α=0.05, two-tailed, and 5% significance). A moderate effect size was assumed for the association between the UA:SCr ratio and the risk of GDM, the sample size for GDM was calculated to be 55, and the total sample size was 366. On this basis, a total of 958 pregnant women with clinical and laboratory data at 6–12 weeks’ gestation and 75 g oral glucose tolerance test (OGTT) at 24–28 weeks’ gestation were included in the present study. A perinatal database of 802 women was collected from electronic health records.
Measurements
Participants were measured for body weight and height at the first prenatal visit (6–12 weeks’ gestation), and body weight was monitored during the whole course. Body mass index (BMI) was determined by dividing body weight in kilograms by height in meters squared based on measurements taken by trained nurses at the first prenatal visit. Measurements of systolic blood pressure and diastolic blood pressure were taken by trained nurses with an automatic blood pressure monitor. Previous adverse pregnancy outcomes (including embryo damage and spontaneous abortion) were asked by attending doctors and recorded in electronic health records. Fasting blood samples were collected at the first prenatal visit to examine liver function (including alanine aminotransferase, aspartate aminotransferase, and total bilirubin), renal function (including serum creatine, UA, and urea nitrogen), and thyroid function (FT4, thyroid stimulating hormone [TSH], and thyroid peroxidase antibodies). Free triiodothyronine (FT3) could not be analyzed, since routine thyroid function screening during pregnancy at the study hospitals does not include FT3. Euthyroid function was defined as a TSH and FT4 concentration within the normal range of the 2.5thto 97.5th percentile.28 The 75 g OGTT was conducted in all participants during 24–28 weeks’ gestation, and GDM was diagnosed according by the International Association of the Diabetes and Pregnancy Study Groups criterion in 2010: fasting plasma glucose ≥5.1 mmol/L, but <7 mmol/L; 1 h plasma glucose ≥10 mmol/L; or 2 h plasma glucose ≥8.5 mmol/L.29 Perinatal and neonatal outcomes were pregnancy-induced hypertension (including preeclampsia or eclampsia), premature delivery (<37 weeks), cesarean section, postpartum hemorrhage (blood loss from the genital tract ≥500 mL after giving birth),30 LGA (large for gestational age), and SGA (small for gestational age).
Fasting blood samples were sent to Peking Union Medical College Hospital to examine fasting blood glucose, fasting insulin, and fasting C-peptide. The 75 g OGTT was administered at each maternal and child health-care hospital after overnight fasting (blood samples were obtained at fasting and 1 h and 2 h after glucose overload). UA was detected by the coupled uricase–peroxidase method and SCr by the sarcosine oxidase method (Beckman AU680). Thyroid function was detected by electrochemiluminescent technique (Roche Cobas e601, Roche diagnostic).
Statistical Analysis
All analyses were conducted using the statistical program SPSS (version 24, SPSS, Chicago, IL) and G*Power 3.1. Continuous variables were tested for normality of distribution. Variables with approximately normal distributions were presented as mean ± SD (including age, BMI, systolic blood pressure, and diastolic blood pressure), and the other with skewed distributions were presented as median (interquartile range). Categorical variables were presented as percentage (number). Two-sample Student t test was used for continuous variables with approximately normal distributions. Mann–Whitney test was used for continuous variables with skewed distributions. χ2 test was used for categorical variables. The linear trend was calculated by linear-by-linear association tested to determine whether there was a significant graded increase in glucose & lipids level, thyroid function and the risk of GDM with increasing UA:SCr ratio quartiles. The association of UA:SCr ratio and thyroid function as well as GDM were examined by linear regression analysis and binary logistic regression analysis, respectively. To assess confounding, we did stratified analysis by separately examining each of four preBMI groups and covariates (age, family history of DM and parity) were entered into the logistic regression model. Statistical significance was inferred from two-sided P values <0.05.
Results
Among the 958 women in this cohort, GDM incidence was 19.3% (185/958) and 802 had perinatal outcomes. The baseline characteristics, perinatal outcomes, and neonatal characteristics of those with GDM and normal glucose tolerance (NGT) are presented in Table 1. Age, BMI during the first and second trimester, alanine aminotransferase, total cholesterol, triglyceride, low-density-lipoprotein cholesterol, fasting glucose in first trimester, insulin, C-peptide, blood glucose level during OGTT, UA, SCr, UA:SCr ratio, rate of pregnancy-induced hypertension, premature delivery, and cesarean delivery were all significantly higher in the GDM group than the NGT group. FT4, TSH, and the percentage of positive TPOAb were similar in two groups. Stratification analysis based on preBMI quartiles showed a UA:SCr ratio in the GDM group in the highest preBMI quartile that was significantly higher than that in the NGT group, while FT4 in the GDM group in the highest preBMI quartile was significantly lower (median 5.22, IQR 4.47–5.87 vs median 4.87, IQR 4.05–5.61, P=0.04; median 1.13, IQR 1.02–1.28 vs median 1.18, IQR 1.07–1.32, P=0.02) (Supplementary Table 1).
 |
Table 1 Baseline characteristics, neonatal characteristics, and perinatal outcomes in women with and without GDM |
To examine glucose and lipid metabolism, thyroid function, and risk of GDM according to UA:SCr ratio in the first trimester in further detail, subjects were divided into quartiles of UA:SCr ratio based on their distribution (quartile 1, ≤3.79; quartile 2, 3.79–4.41; quartile 3, 4.41–5.20; and quartile 4, ≥5.20) (Table 2). The linear trends of FT4 levels, triglyceride, high-density-lipoprotein cholesterol, low-density-lipoprotein cholesterol, fasting blood glucose in first trimester, insulin, C-peptide, homeostasis model assessment of insulin resistance, plasma glucose levels during OGTT, and incidence of GDM according to UA:SCr ratio quartiles were all statistically significant. The incidence of GDM in the third quartile of UA:SCr ratio was up to 28.7% (68/237).
 |
Table 2 Metabolism variables according to UA:SCr ratio quartiles |
Linear regression was used to examine the association of UA:SCr ratio and thyroid function within normal ranges (Table 3). FT4 and TSH were not associated with UA:SCr according to preliminary analysis. However, analysis based on preBMI quartiles showed that FT4 was positively related to UA:SCr ratio in women in the third preBMI quartile (β=0.636, 95% CI 0.210–1.061, P=0.004) and the correlation was still significant after adjustment for age (β=0.659, 95% CI 0.231–1.087, P=0.003). FT4 was significantly negatively related to UA:SCr ratio (β=-0.263, 95% CI −0.516 to −0.011, P=0.041), and TSH was significantly positively related to UA:SCr ratio (β=0.131, 95% CI 0.008–0.253, P=0.036) in women with the highest preBMI quartile.
 |
Table 3 Association of euthyroid function and UA:SCr ratio based on BMI |
The crude and multivariate-adjusted relative risk (RR) of GDM determined by UA:SCr ratio and thyroid function is shown in Table 4 and Table 5. Higher UA:SCr ratio was associated with increased risk of GDM, even after adjustment for age and family history of DM and parity (RR 0.226, 95% CI 1.097–1.432, P=0.001). However, further analysis showed the relationship between UA:SCr ratio and GDM was significant only in women in the highest preBMI quartile (RR 0.331, 95% CI 1.094–1.772, P=0.007). Similarly, higher FT4 was associated with decreased risk of GDM in those in the highest preBMI quartile (RR −0.533, 95% CI 0.055–0.853, P=0.029). However, interaction effect analysis showed there was no interaction effect between preBMI, UA:SCr ratio, FT4.
 |
Table 4 Association between UA:SCr ratio and GDM based on BMI |
 |
Table 5 Association between thyroid function and GDM based on BMI |
The association between euthyroid function and risk of GDM based on UA:SCr ratio quartiles is shown in Table 6. Preliminary analysis showed euthyroid function was not associated with risk of GDM. However, after adjusted for confounding factors, including age, preBMI, and family history of DM and parity, FT4 was associated with GDM in pregnant women in the highest UA:SCr ratio quartile (RR 0.052, 95% CI 1.010–1.096, P=0.012), and there was an interaction effect between FT4 and UA:SCr ratio in relation to the risk of GDM in the highest UA:SCr ratio quartile (P=0.02).
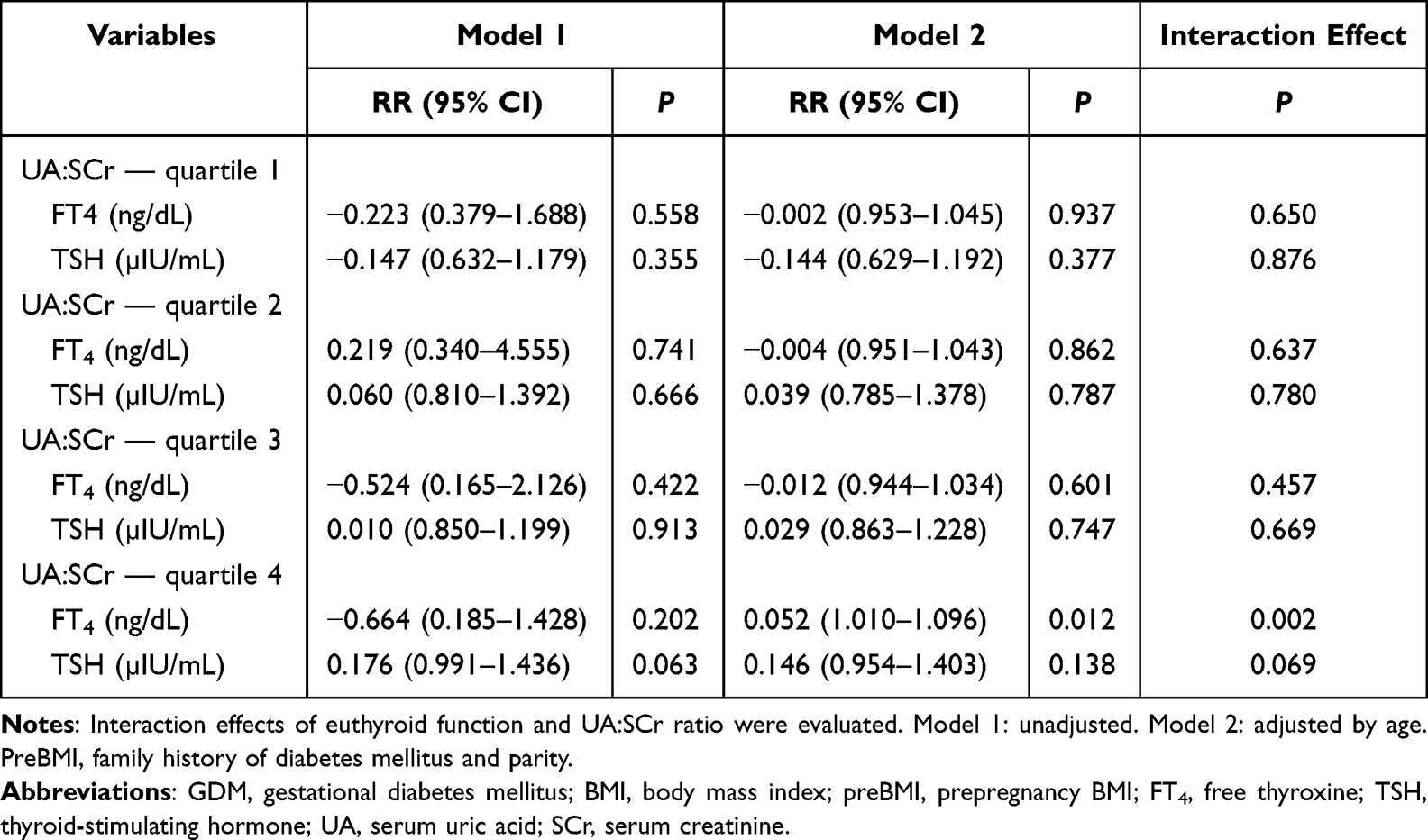 |
Table 6 Association between thyroid function and GDM based on UA:SCr ratio |
Discussion
In this prospective bicenter cohort study, we found that the UA:SCr ratio and FT4 in normal ranges were associated with the risk of GDM and that there was interaction effect between the UA:SCr ratio and FT4. The relationship between the UA:SCr ratio and euthyroid function was also observed in women in the third and fourth quartiles of preBMI. These findings imply that both UA:SCr ratio and FT4 are implicated in metabolic regulation during early pregnancy, and their interplay might influence glucose metabolism. To the best of our knowledge, this is the first study to examine the association between UA:SCr ratio and thyroid function within the normal range and the risk of GDM.
UA is the final oxidation product of purine metabolism and is closely related to metabolic disease. However, the relationship between UA levels and GDM remains controversial.31 A cohort study of 85,609 pregnant women found UA levels at 13–18 weeks’ gestation were significantly higher in the GDM group.32 However, Güngör ES et al reported SCr was significantly higher in women with GDM, whereas UA was similar in women with or without GDM.33 However, increased UA commonly occurs as a consequence of renal dysfunction, and some previous studies have ignored the effect of renal function on UA.34–36 The UA:SCr ratio, which represents renal function-normalized SUA, is associated with diverse adverse outcomes.37 Therefore, we consider the UA:SCr ratio a better indicator to evaluate UA level, as endogenous UA depends primarily on renal clearance function. Previous studies have reported that the UA:SCr ratio was an independent risk factor of cardiovascular disease and metabolic disease, and was even associated with total and cause-specific mortality in large populations.38 A prospective study enrolled 96,378 participants from the Kailuan study without stroke and myocardial infarction at baseline and found that the highest-quartile UA:SCr ratio was associated with the highest risk of cardiovascular disease and stroke.37 Chao et al found a significant positive correlation existed between UA:SCr ratio and metabolic syndrome risk in Chinese individuals aged ≥45 years and claimed it could be a new predictive marker for metabolic syndrome risk. Baseline UA:SCr ratio was independently and significantly associated with preserved β-cell function and future renal function decline among diabetic patients.39,40 The increase in oxidative stress associated with UA:SCr ratio can lead to senescence and apoptosis in human umbilical vein endothelial cells.41 Previous studies have reported that UA:SCr ratio was associated with certain adverse health outcomes in specific conditions, such as metabolic syndrome in postmenopausal women or diabetic patients, chronic kidney disease in diabetic individuals, and liver function in normal subjects.37 To our knowledge, the association between UA:SCr ratio and glucose and lipid metabolism during pregnancy has not yet been characterized. In this study, fasting glucose levels, lipid levels, and insulin resistance all showed an increasing trend with the UA:SCr ratio across the four groups. These changes might not be clinically significant in the short term since the values remained within normal limits, but they imply that UA:SCr ratios were associated with metabolic status during early pregnancy, and this ratio’s long-term influence deserves further investigation.
An increasing number of epidemiological studies have shown elevated serum UA levels in patients with polycystic ovary syndrome, endometriosis, etc.42,43 Serum UA in preeclampsia was significantly associated with both maternal (cesarean section and severe hypertension) and adverse neonatal (low birth weight) outcomes, which seems clinically useful in predicting pregnancy outcomes.44 Some studies have reported UA:SCr ratio as a new marker of preeclampsia.17 However, the evidence for the effect of UA on GDM remains controversial, and few studies have reported the relationship between UA:SCr and GDM. In this study, both UA and UA:SCr ratios were significantly higher in women with GDM and we found that the UA:SCr ratio was associated with the risk of GDM, but the relationship was only found in those in the highest preBMI quartile. Elevated level of SUA can induce inflammation and oxidative stress,45 and fructose-induced hyperuricemia is believed to mediate fructose-induced insulin resistance,46 leading to insulin resistance and decreased glucose uptake.47 At the same time, it was acknowledged that BMI was closely related to UA and GDM. We assume that BMI has a stronger effect on GDM and that the UA:SCr ratio can further increase the risk of GDM only when the effect of BMI on GDM reaches a plateau.
It is acknowledged that abnormal thyroid function can influence the metabolism during pregnancy.28,48–51However, the association between thyroid function in the normal range and risk of GDM is controversial.24,52 A longitudinal study of 2927 singleton pregnant women found that higher FT3 and FT4 and lower central thyroid resistance indices were associated with increased risk of GDM.53 Veltri et al found that pregnancy outcomes were not altered by variation in thyroid function within the normal range in women free of thyroid disease.25 In this study, we found that FT4 in the GDM group among women in the highest preBMI quartile was significantly lower than that in the NGT group. FT4 was associated with risk of GDM among women in the highest preBMI quartile and UA:SCr ratio quartile. Further analysis implied that an interaction between UA:SCr ratio and FT4 might affect glucose metabolism during early pregnancy. However, due to the lack of FT3, further analysis and the potential mechanism of euthyroid function were limited. Although the detailed mechanism remains unclear, these findings suggest the complex pathogenesis of GDM and highlight the need for the detection of additional factors to better prevent GDM. A more comprehensive understanding of these factors could lead to improved risk assessment and early intervention strategies.
Previous studies have suggested that there might be a positive correlation between serum UA levels and hyperthyroidism, but the relationship between euthyroid function and serum UA in healthy people is controversial. A study of 4460 participants reported decreased sensitivity to thyroid hormones was associated with elevated levels of serum UA in people with normal thyroid function, and different age-groups and BMI groups impacted the association between impaired thyroid hormone sensitivity and serum UA.54 A retrospective study of 48526 healthy subjects showed that under normal thyroid function, there were significant differences in TSH, FT3, and FT4 between groups with different UA levels and UA levels were linearly correlated with FT3 and FT4, but not with TSH.55 Another study reported a negative correlation between low UA content and FT3 in a Chinese Han population, suggesting that reduced UA content may serve as a risk factor to predict poor thyroid function in Chinese individuals.27 Production of the thyroid hormone increases by approximately 50% during pregnancy, and the burden of thyroid dysfunction can occur in many pregnant women and has a profound impact.56 However, the relationship between euthyroid function and serum UA during pregnancy is unclear. In this study, we found that FT4 was positively correlated with the UA:SCr ratio in the third preBMI quartile, though significantly negatively correlated with the UA:SCr ratio, and TSH was significantly positively correlated with the UA:SCr ratio in the highest preBMI quartiles. Physiologically, thyroid hormones play a significant role in stimulating metabolism in the human body. As thyroid hormone levels increase, more adenosine triphosphate is consumed, leading to higher levels of adenine ribonucleotides, which may further affect purine metabolism and make serum UA levels higher.54 A certain stimulation of the thyroid axis may occur in a state of excess energy metabolism, but the thyroid does not compensate for the increased energy consumption due to its state of excess energy metabolism. We speculate that the different relationship between thyroid function and UA:SCr ratio in pregnant women in different BMI groups might be because of the complex negative feedback mechanism of the hypothalamic–pituitary–thyroid axis and the interplay between UA mechanisms and insulin resistance, as well as thyroid function.
The innovations of this study are as follows. First, this is the first study to explore the relationship between the UA:SCr ratio in early pregnancy and thyroid function as well as GDM risk. Second, this was a prospective bicenter study with little information bias, so the results obtained are more reliable than those from a retrospective study. Third, we excluded patients with pregestational diabetes and thyroid disease to reduce interference. However, there are also limitations. First, the loss to follow-up was higher than expected, mainly due to the fact that the COVID-19 pandemic was impeding regular follow-up of participants at designated hospitals. However, the participants who were lost to follow up had not known their status of glucose metabolism before and were nonselective, so the withdrawal bias was limited and the results are relatively reliable. Second, although some confounding factors were considered and stratified analysis was performed to decrease the potential influence of these factors on the results, confounding bias cannot be eliminated. For example, diet, which is closely related to risk of GDM, was not recorded in this study. Third, previous studies reported FT3, FT4, and thyroid sensitivity might be associated with metabolism. However, there was no opportunity to investigate the association with FT3, because it was not measured in more than half the pregnant women in this study, which limited further investigation on euthyroid function and UA:SCr ratio as well as GDM. Therefore, future studies should be conducted to increase the reliability and generality of the results.
Conclusion
In summary, this study found that UA:SCr ratio and FT4 were associated with the risk of GDM in early pregnancy, particularly among women in the highest prepregnancy BMI quartile. Furthermore, FT4 levels within the normal range were correlated with UA:SCr ratio in women in the third and fourth prepregnancy BMI quartiles. These findings suggest that UA:SCr, especially in conjunction with BMI, may have potential value in assessing GDM risk. However, further research is needed to confirm these findings, explore the underlying mechanisms, and determine the clinical utility of the UA:SCr ratio and FT4 in GDM risk prediction and management.
Data Sharing
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The ethics committees of all participating centers approved the study protocol (Peking Union Medical College Hospital, Institute of Beijing Medical Science Chinese Academy of Medical Sciences, Haidian District Maternal and Child Health Care Hospital and Beijing Chaoyang District Maternal and Child Health Care Hospital) and the study was performed in accordance with the Declaration of Helsinki as revised in 2013. Written informed consent was obtained from each participant.
Consent
All participants provided written consent to the inclusion of material pertaining to themselves and acknowledged they had been fully anonymized such that they cannot be identified via the paper.
Acknowledgments
The authors thank all the participants in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis, interpretation, or all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study was supported by the 13th Five-Year National Science and Technology Major Project for New Drugs under grant 2019ZX09734001 (to Weigang Zhao).
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. Ali N, Rahman S, Islam S, et al. The relationship between serum uric acid and lipid profile in Bangladeshi adults. BMC Cardiovasc Disord. 2019;19(1):42. doi:10.1186/s12872-019-1026-2
2. Committee on Practice Bulletins-Obstetrics. ACOG practice bulletin no. 190 summary: gestational diabetes mellitus. Obstet Gynecol. 2018;131(2):406–408. doi:10.1097/AOG.0000000000002498
3. Wang H, Li N, Chivese T, et al. Diabetes atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by international association of diabetes in pregnancy study group’s criteria. Diabet Res Clin Pract. 2022;183:109050. doi:10.1016/j.diabres.2021.109050
4. Billionnet C, Mitanchez D, Weill A, et al. Gestational diabetes and adverse perinatal outcomes from 716,152 births in France in 2012. Diabetologia. 2017;60(4):636–644. doi:10.1007/s00125-017-4206-6
5. Damm P, Houshmand-Oeregaard A, Kelstrup L, Lauenborg J, Mathiesen ER, Clausen TD. Gestational diabetes mellitus and long-term consequences for mother and offspring: a view from Denmark. Diabetologia. 2016;59(7):1396–1399. doi:10.1007/s00125-016-3985-5
6. Becker BF. Towards the physiological function of uric acid. Free Radic Biol Med. 1993;14(6):615–631. doi:10.1016/0891-5849(93)90143-I
7. Spitsin SV, Scott GS, Kean RB, Mikheeva T, Hooper DC. Protection of myelin basic protein immunized mice from free-radical mediated inflammatory cell invasion of the central nervous system by the natural peroxynitrite scavenger uric acid. Neurosci Lett. 2000;292(2):137–141. doi:10.1016/S0304-3940(00)01446-4
8. Wan X, Xu C, Lin Y, et al. Uric acid regulates hepatic steatosis and insulin resistance through the NLRP3 inflammasome-dependent mechanism. J Hepatol. 2016;64(4):925–932. doi:10.1016/j.jhep.2015.11.022
9. Kobayashi G, Okada H, Hamaguchi M, et al. Association between uric acid levels and incidence of type 2 diabetes: population-based Panasonic cohort study 11. Diabet Res Clin Pract. 2023;195:110179. doi:10.1016/j.diabres.2022.110179
10. Wang R, Wu S, Wang J, Li W, Cui J, Yao Z. A nonlinear correlation between the serum uric acid to creatinine ratio and the prevalence of hypertension: a large cross-sectional population-based study. Ren Fail. 2024;46(1):2296002. doi:10.1080/0886022X.2023.2296002
11. Cao T, Tong C, Halengbieke A, et al. Serum uric acid to creatinine ratio and metabolic syndrome in middle-aged and elderly population: based on the 2015 CHARLS. Nutr, Metab Cardiovasc Dis. 2023;33(7):1339–1348. doi:10.1016/j.numecd.2023.05.004
12. Tang Z, Liu H, Ding Y, Yuan C, Shao Y. Association between serum uric acid to serum creatinine ratio with cardiovascular and all-cause mortality in adults with hypertension. Sci Rep. 2024;14(1):18008. doi:10.1038/s41598-024-69057-4
13. Zhong D, Liu D, Guo Y, et al. Association of the serum uric acid to creatinine ratio with metabolic syndrome in the middle age and older population in China. Front Endocrinol. 2022;13:1060442. doi:10.3389/fendo.2022.1060442
14. Zhao L, Qiu X. Higher ratio of serum uric acid to serum creatinine (SUA/SCr) increases the risk of metabolic unhealthy phenotype. Nutr, Metab Cardiovasc Dis. 2023;33(10):1981–1988. doi:10.1016/j.numecd.2023.07.013
15. Wang R, Xue F, Wang L, et al. Serum uric acid to creatinine ratio is associated with higher prevalence of NAFLD detected by fibroscan in the United States. J Clin Lab Anal. 2022;36(8):e24590. doi:10.1002/jcla.24590
16. Gong Y, Tian X, Zhou Y, et al. Association between serum uric acid to serum creatinine ratio and poor functional outcomes in patients with acute ischemic stroke. Eur J Neurol. 2022;29(11):3307–3316. doi:10.1111/ene.15521
17. Piani F, Agnoletti D, Baracchi A, et al. Serum uric acid to creatinine ratio and risk of preeclampsia and adverse pregnancy outcomes. J Hypertens. 2023;41(8):1333–1338. doi:10.1097/HJH.0000000000003472
18. Mohamed RA, Ali IA. Role of neutrophil / lymphocyte ratio, uric acid / albumin ratio and uric acid / creatinine ratio as predictors to severity of preeclampsia. BMC Pregnancy Childbirth. 2023;23(1):763. doi:10.1186/s12884-023-06083-6
19. Zhang E, Su S, Gao S, et al. Elevated serum uric acid to creatinine ratio is associated with adverse pregnancy outcomes: a prospective birth cohort study. Int J Med Sci. 2024;21(9):1612–1621. doi:10.7150/ijms.95313
20. Ding Z, Fan Y, Yao C, Gu L. The association between the serum uric acid to creatinine ratio and all-cause mortality in elderly hemodialysis patients. BMC Nephrol. 2022;23(1):177. doi:10.1186/s12882-022-02798-4
21. Weetman AP. Thyroid disease in pregnancy in 2011: thyroid function--effects on mother and baby unraveled. Nat Rev Endocrinol. 2011;8(2):69–70. doi:10.1038/nrendo.2011.217
22. Vrijkotte TGM, Hrudey EJ, Twickler MB. Early maternal thyroid function during gestation is associated with fetal growth, particularly in male newborns. J Clin Endocrinol Metab. 2017;102(3):1059–1066. doi:10.1210/jc.2016-3452
23. Yu Z-W, Shan Z-Y. Thyroid function variations within the reference range and cognitive function: a two-sample Mendelian randomization study. J Affect Disord. 2024;357:156–162. doi:10.1016/j.jad.2024.05.007
24. Chen G-D, Gou X-Y, Pang -T-T, et al. Associations between thyroid function and gestational diabetes mellitus in Chinese pregnant women: a retrospective cohort study. BMC Endocr Disord. 2022;22(1):44. doi:10.1186/s12902-022-00959-y
25. Veltri F, Kleynen P, Grabczan L, et al. Pregnancy outcomes are not altered by variation in thyroid function within the normal range in women free of thyroid disease. Eur J Endocrinol. 2018;178(2):189–197. doi:10.1530/EJE-17-0628
26. Xing Y, Yang L, Liu J, Ma H. The association with subclinical thyroid dysfunction and uric acid. Int J Endocrinol. 2021;2021:9720618. doi:10.1155/2021/9720618
27. Wang X-J, Qian X-W, Zhang X, et al. Association of serum uric acid with thyroid function in health check-up participants. Chin Med J. 2020;133(12):1409–1414. doi:10.1097/CM9.0000000000000840
28. Ad Hoc Writing Committee for Guideline on Diagnosis and Management of Thyroid Diseases during Pregnancy and Postpartum (2nd edition) CSoE, Chinese Medical Association, Chinese Society of Perinatology, Chinese Medical Association. Guideline on diagnosis and management of thyroid diseases during pregnancy and postpartum (2nd edition). Chin J Perinat Med. 2019;(8):505–539.
29. Metzger BE, Gabbe SG, Persson B, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(7):676–682. doi:10.2337/dc10-0719
30. Sentilhes L, Merlot B, Madar H, Sztark F, Brun S, Deneux-Tharaux C. Postpartum haemorrhage: prevention and treatment. Expert Rev Hematol. 2016;9(11):1043–1061. doi:10.1080/17474086.2016.1245135
31. Su S, Zhang E, Gao S, et al. Serum uric acid and the risk of gestational diabetes mellitus: a systematic review and meta-analysis. Gynecol Endocrinol. 2023;39(1):2231101. doi:10.1080/09513590.2023.2231101
32. Zhao Y, Zhao Y, Fan K, Jin L. Serum uric acid in early pregnancy and risk of gestational diabetes mellitus: a cohort study of 85,609 pregnant women. Diabetes Metab. 2022;48(3):101293. doi:10.1016/j.diabet.2021.101293
33. Güngör ES, Danişman N, Mollamahmutoğlu L. Relationship between serum uric acid, creatinine, albumin and gestational diabetes mellitus. Clin Chem Lab Med. 2006;44(8):974–977. doi:10.1515/CCLM.2006.173
34. Holme I, Aastveit AH, Hammar N, Jungner I, Walldius G. Uric acid and risk of myocardial infarction, stroke and congestive heart failure in 417,734 men and women in the Apolipoprotein MOrtality RISk study (AMORIS). J Intern Med. 2009;266(6):558–570. doi:10.1111/j.1365-2796.2009.02133.x
35. Ong G, Davis WA, Davis TME. Serum uric acid does not predict cardiovascular or all-cause mortality in type 2 diabetes: the Fremantle diabetes study. Diabetologia. 2010;53(7):1288–1294. doi:10.1007/s00125-010-1735-7
36. Hozawa A, Folsom AR, Ibrahim H, Nieto FJ, Rosamond WD, Shahar E. Serum uric acid and risk of ischemic stroke: the ARIC study. Atherosclerosis. 2006;187(2):401–407. doi:10.1016/j.atherosclerosis.2005.09.020
37. Wang A, Tian X, Wu S, et al. Metabolic factors mediate the association between serum uric acid to serum creatinine ratio and cardiovascular disease. J Am Heart Assoc. 2021;10(23):e023054. doi:10.1161/JAHA.121.023054
38. Mazidi M, Katsiki N, Banach M. Α higher ratio of serum uric acid to serum creatinine could predict the risk of total and cause specific mortality- insight from a US national survey. Int J Cardiol. 2021;326:189–193. doi:10.1016/j.ijcard.2020.05.098
39. Li M, Gu L, Yang J, Lou Q. Serum uric acid to creatinine ratio correlates with β-cell function in type 2 diabetes. Diabetes Metab Res Rev. 2018;34(5):e3001. doi:10.1002/dmrr.3001
40. Kawamoto R, Ninomiya D, Kikuchi A, et al. Serum uric acid to creatinine ratio is a useful predictor of renal dysfunction among diabetic persons. Diabetes Metab Syndr. 2019;13(3):1851–1856. doi:10.1016/j.dsx.2019.04.023
41. Yu M-A, Sánchez-Lozada LG, Johnson RJ, Kang D-H. Oxidative stress with an activation of the renin-angiotensin system in human vascular endothelial cells as a novel mechanism of uric acid-induced endothelial dysfunction. J Hypertens. 2010;28(6):1234–1242. doi:10.1097/HJH.0b013e328337da1d
42. Hu J, Xu W, Yang H, Mu L. Uric acid participating in female reproductive disorders: a review. Reprod Biol Endocrinol. 2021;19(1):65. doi:10.1186/s12958-021-00748-7
43. Powers RW, Bodnar LM, Ness RB, et al. Uric acid concentrations in early pregnancy among preeclamptic women with gestational hyperuricemia at delivery. Am J Obstet Gynecol. 2006;194(1):160. doi:10.1016/j.ajog.2005.06.066
44. Adu-Bonsaffoh K, Kudaya DQ, Fidelis B, Fondjo LA, Ahenkorah J. Alteration in maternal serum uric acid levels in pre-eclampsia and associated perinatal outcomes: a cross-sectional study in Ghana. Pan Afr Med J. 2024;47:49. doi:10.11604/pamj.2024.47.49.37106
45. Sautin YY, Nakagawa T, Zharikov S, Johnson RJ. Adverse effects of the classic antioxidant uric acid in adipocytes: NADPH oxidase-mediated oxidative/nitrosative stress. Am J Physiol Cell Physiol. 2007;293(2):C584–C596. doi:10.1152/ajpcell.00600.2006
46. Johnson RJ, Perez-Pozo SE, Sautin YY, et al. Hypothesis: could excessive fructose intake and uric acid cause type 2 diabetes?. Endocr Rev. 2009;30.
47. Zhi L, Yuzhang Z, Tianliang H, Hisatome I, Yamamoto T, Jidong C. High uric acid induces insulin resistance in cardiomyocytes in vitro and in vivo. PLoS One. 2016;11(2):e0147737. doi:10.1371/journal.pone.0147737
48. Wang X, Zhang E, Tian Z, et al. The association between dyslipidaemia in the first trimester and adverse pregnancy outcomes in pregnant women with subclinical hypothyroidism: a cohort study. Lipids Health Dis. 2024;23(1):13. doi:10.1186/s12944-023-01998-7
49. Sert UY, Buyuk GN, Engin Ustun Y, Ozgu Erdinc AS. Is there any relationship between thyroid function abnormalities, thyroid antibodies and development of Gestational Diabetes Mellitus (GDM) in pregnant women?. Medeni Med J. 2020;35(3):195–201. doi:10.5222/MMJ.2020.29964
50. Yanachkova V, Kamenov Z. The relationship between thyroid dysfunction during pregnancy and gestational diabetes mellitus. Endokrynol Pol. 2021;72(3):226–231. doi:10.5603/EP.a2021.0016
51. Wang J, Gong X-H, Peng T, Wu J-N. Association of thyroid function during pregnancy with the risk of pre-eclampsia and gestational diabetes mellitus. Endocr Pract. 2021;27(8):819–825. doi:10.1016/j.eprac.2021.03.014
52. Huang K, Su S, Wang X, et al. Association between maternal thyroid function in early pregnancy and gestational diabetes: a prospective cohort study. J Clin Endocrinol Metab. 2024;109(2):e780–e787. doi:10.1210/clinem/dgad518
53. Liu Z-M, Li G, Wu Y, et al. Increased central and peripheral thyroid resistance indices during the first half of gestation were associated with lowered risk of gestational diabetes-analyses based on Huizhou birth cohort in South China. Front Endocrinol. 2022;13:806256. doi:10.3389/fendo.2022.806256
54. Xie H, Li N, Zhou G, et al. The association between the thyroid feedback quantile-based index and serum uric acid in U.S. adults. Eur J Med Res. 2023;28(1):259. doi:10.1186/s40001-023-01214-3
55. Chao G, Zhu Y, Fang L. Retrospective analysis of the correlation between uric acid and thyroid Hormone in people with normal thyroid function. J Diabetes Res. 2019;2019:5904264. doi:10.1155/2019/5904264
56. Alexander EK, Pearce EN, Brent GA, et al. Guidelines of the American thyroid association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid. 2017;27(3):315–389. doi:10.1089/thy.2016.0457
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Pre-Pregnancy Hemoglobin Level on the Association Between Pre-Pregnancy Body Mass Index and Gestational Diabetes Mellitus: A Retrospective Cohort Study in a Single Center in China
Wu K, Ke HH, Gong W, Hu H, Chen L
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3767-3775
Published Date: 8 December 2022
A Comparative Cross-Sectional Study Between Gestational Diabetes Mellitus and Preeclampsia: Medication Adherence, Depression and Quality of Life
Noor R, Abbas G, Khurram H, Aslam A, Randhawa FA, Assiri A, Shah S
International Journal of Women's Health 2026, 18:565083
Published Date: 8 January 2026
Longitudinal Assessment of Routine Blood–Derived Inflammatory Indices in Women with Diet-Controlled Gestational Diabetes: A Retrospective Study
Jiang H, Xin W, Li Z, Gao S, Wang J
International Journal of Women's Health 2026, 18:611520
Published Date: 15 July 2026