Back to Journals » International Journal of Women's Health » Volume 18
A Comparative Cross-Sectional Study Between Gestational Diabetes Mellitus and Preeclampsia: Medication Adherence, Depression and Quality of Life
Authors Noor R, Abbas G ![]() , Khurram H
, Khurram H ![]() , Aslam A
, Aslam A ![]() , Randhawa FA, Assiri A
, Randhawa FA, Assiri A ![]() , Shah S
, Shah S ![]()
Received 3 September 2025
Accepted for publication 27 December 2025
Published 8 January 2026 Volume 2026:18 565083
DOI https://doi.org/10.2147/IJWH.S565083
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Rafia Noor,1 Ghulam Abbas,2 Haris Khurram,3 Ayesha Aslam,4 Fawad Ahmad Randhawa,5 Abdullah Assiri,6 Shahid Shah1
1Faculty of Pharmaceutical Sciences, Department of Pharmacy Practice, Government College University Faisalabad, Faisalabad, Pakistan; 2Faculty of Pharmaceutical Sciences, Department of Pharmaceutics, Government College University Faisalabad, Faisalabad, Pakistan; 3Department of Science and Humanities, National University of Computer and Emerging Science, Chiniot-Faisalabad Campus, Chiniot, Pakistan; 4Department of Neurology, King Edward Medical University, Lahore, Pakistan; 5Department of Endocrinology, Allama Iqbal Medical College Lahore, Lahore, Pakistan; 6Department of Clinical Pharmacy, College of Pharmacy, King Khalid University, Abha, Saudi Arabia
Correspondence: Shahid Shah, Email [email protected]
Background: Gestational diabetes mellitus (GDM) and preeclampsia (PE) are two of the most prevalent high-risk pregnancy problems, with significant consequences for maternal health, emotional well-being, and quality of life (QoL).
Aim: This study aimed to compare the medication adherence, depression, and QoL among women with GDM and PE.
Patients and Methods: This was a cross-sectional study conducted in 1306 women with GDM and PE. A total of 7 hospitals were included across Punjab, Pakistan, conducted between November 2024 to June 2025. Data were collected using the Medication Adherence Report Scale (MARS-5), Patient Health Questionnaire-9 (PHQ-9) and WHOQOL-BREF. Statistical analyses, including frequency, Mann–Whitney U-tests and Kruskal–Wallis test to compare the median across different factors. Exploratory data analysis (EDA) was used to assess the relation between medication adherence, depression, and QoL for different conditions. Linear regression models were employed to assess the medication adherence, depression, and QoL, among women with GDM and PE.
Results: The preeclamptic women showed higher medication adherence than those with GDM (Median=14, Q1-Q3=12-16, p=0.012). Depression scores were significant in physical health domain of QoL in preeclamptic patient (p=0.001). QoL scores (p< 0.05) were higher in physical, psychological, social, and environmental domains, particularly among women with GDM than those with PE. Overall education level, parity, and social support were significant (p< 0.05) predictor of adherence and QoL across both conditions.
Conclusion: Preeclamptic women were more likely to take their medication as prescribed than GDM women. However, our study highlights the depression as a predictor of physical health in preeclamptic patients with WHOQOL scores while women with GDM reported a better overall QoL than PE.
Keywords: depression, gestational diabetes mellitus, medication adherence, preeclampsia, quality of life
Introduction
Gestational diabetes mellitus (GDM) and preeclampsia (PE) are significant common complications in pregnancy with similar risk factors, such as obesity, advanced age, and recurrent pregnancy.1 In the 21st century, the global burden of high-risk pregnancies such as GDM and PE has shown a concerning rise, largely driven by increased maternal age, sedentary lifestyles, obesity, pre-existing chronic diseases, and socio-environmental stressors.2,3 GDM is defined as glucose intolerance that is identified for the first-time during pregnancy, while PE is clinically characterized by the development of hypertension after 20 weeks of gestation, along with the presence of proteinuria or signs of end-organ dysfunction.4,5 These conditions (GDM and PE) are linked to a heightened risk of negative outcomes,6,7 including preterm birth, low birth weight, fetal growth restriction, cesarean delivery, and neonatal death.8,9 There has been a worrying uptick in the incidence of GDM and PE in lower-middle-income countries, where challenges with health literacy and access to prenatal care are widespread.10,11
With this background, attention must be given to medication adherence, a critical component of effective healthcare especially in the treatment of these conditions. Non-compliance with antihypertensive or hypoglycemic regimens might aggravate the progression of illness and compromise maternal and newborn safety.12,13 Consequently, a high level of adherence to medication results in reduced health risks and improved therapeutic outcomes.14
In addition to adherence-related challenges, maternal depression following the prenatal phase is associated with several detrimental effects for children, including impaired cognitive and physical growth, behavioral issues, and an elevated risk of subsequent common mental illnesses in offspring.15,16 Depression during the gestational period and postpartum phase is prevalent, which leads to significant decline in quality of life (QoL), social functioning, and both parental and maternal capabilities.17,18 To address the burden of depression, healthcare systems must prioritize routine mental health screenings as part of prenatal and postpartum care.19,20 GDM can negatively affect maternal, child development, maternal and fetal health, particularly QoL, while PE can cause headache, right upper quadrant pain, vision abnormalities, and fatigue, which can negatively impact emotional and mental well-being.21,22 These medical conditions not only impair clinical results but also influence QoL and lead to psychological discomfort during pregnancy, underscoring the need to better understand the factors contributing to these challenges.23,24 Despite evidence on the clinical burden of GDM and PE, there is limited comparative research investigating how these conditions affect medication adherence, depression and QoL in pregnant women. This study aimed to compare medication adherence, depression and QoL among women diagnosed with GDM and those with PE.
Materials and Methods
Study Design and Setting
This was a cross-sectional study conducted between November 2024 to June 2025 in tertiary care hospitals. The data was recruited from a total of 7 hospitals, comprising 2 governments (Allied Hospital, Faisalabad, THQ Hospital, Burewala) and 5 private maternal health facilities (National Hospital, Faisal Hospital, Naila Medical Center, Faisalabad; Al Nafees Medical College and Hospital, Islamabad and City Hospital, Multan) across Punjab, Pakistan. Informed consent was obtained in writing from all participants prior to data collection. The confidentiality was strictly maintained throughout the study period. Ethical approval (ref. no. GCUF/ERC/492-A) was obtained from the Ethics Review Board of Government College University, Faisalabad.
Participants and Sampling
This study included all pregnant women who visited the hospital during the specified period. Out of 1306 women enrolled, 71 were eliminated for providing incomplete data, and 24 were ineligible due to study inclusion and exclusion criteria. Moreover, the statistical power associated with this sample size exceeded 90%. The final 1211 patients were comprised of 644 with GDM and 567 with PE, attending maternity clinics in the selected healthcare facilities in Punjab, Pakistan. The participants were divided into two groups on the basis of demographics: GDM or PE, based on standard clinical criteria. Only pregnant women with gestational age ≥20 weeks, aged ≥18 years and those with a confirmed diagnosis of GDM and PE were included in the study. Women with multiple pregnancy (eg, twins), comorbid life-threatening conditions, diagnosed with type 1 or type 2 diabetes mellitus and chronic hypertension before pregnancy, were excluded from the study.
Clinical Rating Scales
Data collection was carried out using three standardized and pre-validated tools: the Medication Adherence Report Scale (MARS-5), the Patient Health Questionnaire-9 (PHQ-9), and the World Health Organization Quality of Life-BREF (WHOQOL-BREF) for this population. The MARS-5 was utilized to assess medication compliance,25 and the PHQ-9 was used to investigate the depression in GDM and preeclamptic patients with a cut-off score ≥10.26 WHOQOL-BREF was used to assess QoL in all four domains: physical, psychological, environmental, and social relationships with a cut-off score <60.27
Statistical Analysis
Statistical analyses including frequencies and percentages were used for characteristics of the respondents. Mann–Whitney U-tests and Kruskal–Wallis test were used to compare the median difference in score of medication adherence, depression, and QoL for different factors. Exploratory data analysis (EDA) including the rank correlation plot, density and scatter plot with fitted LOESS model was used to assess the relation between medication adherence, depression, and QoL in different conditions. Linear regression models were employed to assess the medication adherence, depression and QoL among women whereas age and education were considered as controlled variable in all the regression models. p-value <0.05 were considered statistically significant. All the results were evaluated using R language.
Results
Participants Demographics
The demographics of the pregnant women diagnosed with GDM and PE are described in Table 1. According to the condition, 644 were diagnosed with GDM and 567 with PE. The majority of the participants were between 24 and 35 years of age, with the 31–34 years group representing the largest proportion (48.5%), followed closely by the 24–29 years group (29.8%). Regarding mean body mass index (BMI), participants with GDM was 30.1 ± 3.4 kg/m2, while those with PE had a mean BMI of 28.6 ± 4.9 kg/m2. In terms of educational attainment, a notable proportion of the participants, 479 (39.6%), had completed secondary education. When it comes to gestational age, more than half of the participants, 673 (55.6%), were in their third trimester when the data were collected, and a proportion of 530 (43.8%) were in their second trimester. Regarding parity, most of the participants had 2 children, accounting for 45.8% of the total sample. Based on clinical assessment, 877 (72.4%) of participants were advised to have a caesarean section, mostly due to maternal or fetal signs of GDM and PE.
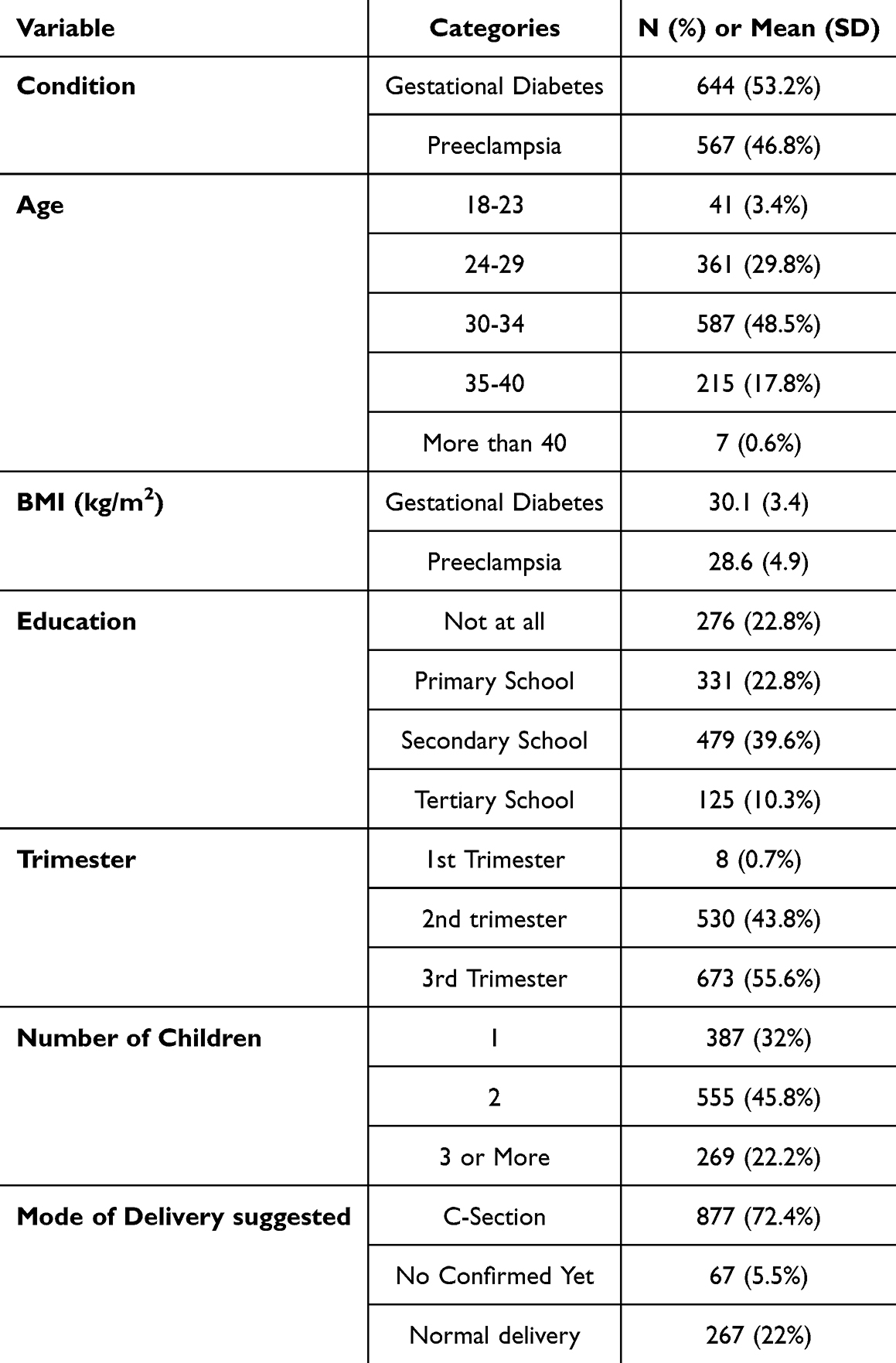 |
Table 1 Sociodemographic Characteristics of the Study |
Medication Adherence, Depression, and QoL in Pregnant Women with GDM and PE
Figure 1 shows the correlation between medication adherence, depression, and QoL among pregnant women with GDM and PE. An unexpected correlation was observed in the pattern of medication adherence, which showed a negative correlation with overall WHOQOL (r =−0.413***) while the strongest negative correlation was observed in GDM (r =−0.425***). This suggested that women who followed their treatment plans more closely felt that their daily well-being was being burdened more. A weak positive correlation existed between depression and physical health (r =0.102***), a domain of WHOQOL, statistically significant, but a weak positive correlation was observed in PE (r =0.117**). This proposed that a heightened awareness of physical symptoms among women experiencing depressive symptoms, leading them to report lower functioning in other domains while rating physical health more critically. The relationship between different factors (depression, medication adherence, general health, physical health, psychological health, social relations, and environment) with WHOQOL (Figure 2).
 |
Figure 1 Exploratory Data Analysis (EDA) of medication adherence, depression, and QoL for the condition of GDM and preeclampsia (upper diagonal: condition-wise rank correlation with significance, diagonal: condition-wise density estimation, lower diagonal: condition-wise scatter plots). Note: * means (p≤0.05), ** means (p≤0.01), *** means (p≤0.001). |
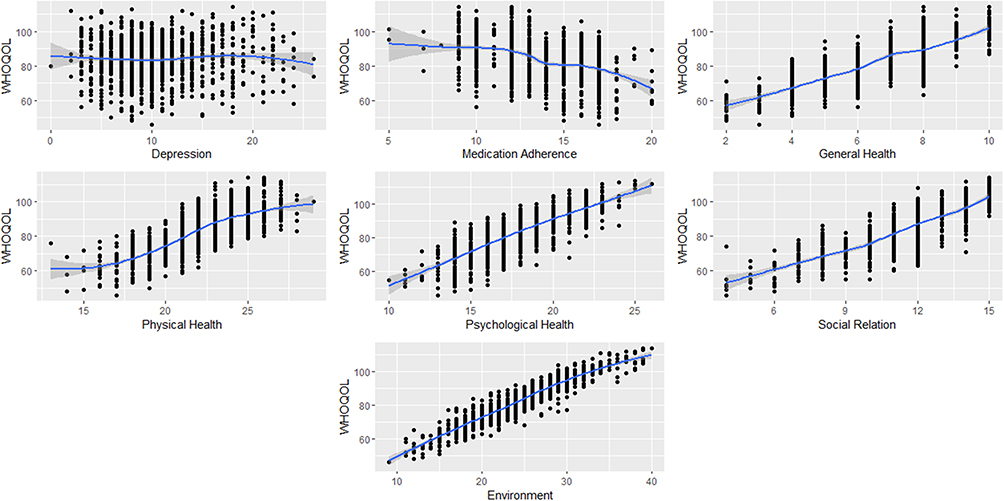 |
Figure 2 Relationship between different health factors with WHOQOL. The blue line is fitted LOESS model and gray shaded area is the 95% Confidence interval. |
Figure 3 shows the association between domains of WHOQOL (environmental, physical, psychological, and social connections) and different variables, including age, education, trimester, condition, medication adherence, and depression. This study used age 18–23, education level “not at all educated”, first trimester pregnancy, one child, and GDM as reference data. These categories were the forest plot baseline.
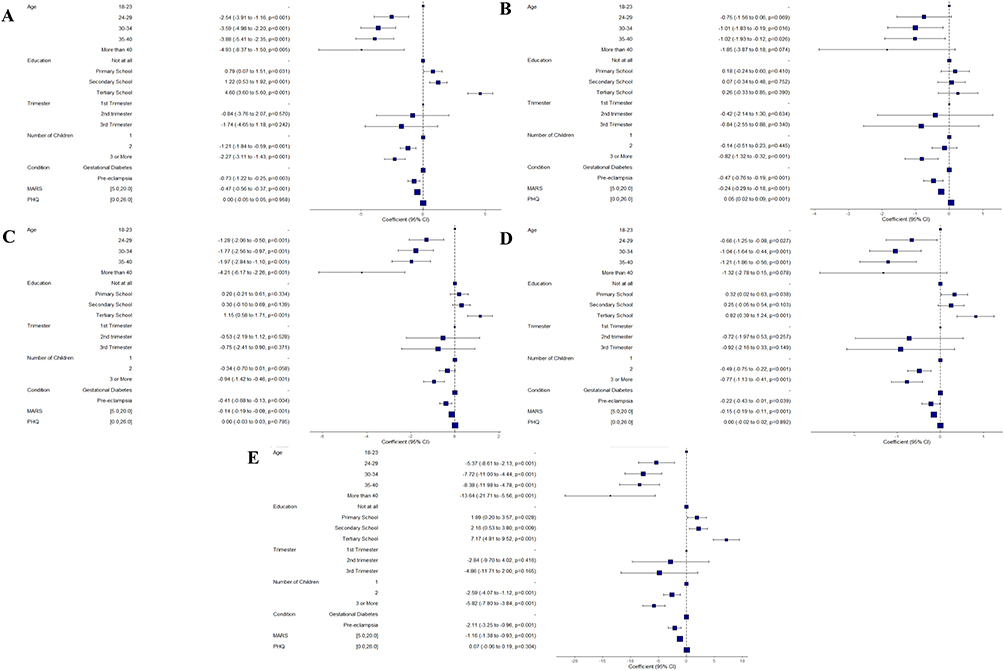 |
Figure 3 Forest plot using linear regression model of WHOQoL domains (A) Environmental, (B) Physical, (C) Psychological, (D) Social Relationships, (E) Overall WHOQOL. |
Significant correlations were identified between WHOQOL-BREF domains and several variables in the forest plot analysis. Medication adherence was notably significant across many domains, with the most pronounced negative relationship observed in the environmental domain −0.47 (−0.56 to −0.37, p<0.001). This shows that women who closely followed their treatment regimens had more environmental constraints, such as limited access to healthcare, financial pressure, transportation issues, and lack of social support. The women with tertiary level education showed the most substantial positive correlation in the same domain 4.60 (3.60 to 5.60, p<0.001), indicating that higher-educated women experienced better healthcare, financial resources, and supportive living conditions. Similarly, the clinical condition of PE demonstrated a considerable effect, exhibiting a strong negative correlation −0.73 (−1.22 to −0.25, p=0.003). This shows that women with PE reported significantly lower satisfaction with their environmental conditions (Figure 3A).
Depression (PHQ score) showed a strong association with the physical health domain 0.05 (0.02 to 0.09, p=0.001), indicating that higher depression scores were significantly linked to poorer physical health QoL in preeclamptic women (Figure 3B). All domains exhibited significance regarding age, with the most pronounced negative correlation in the psychological domain for women over 40 years old −4.21 (−6.17 to −2.26, p<0.001), which means that advancing age is associated with increased psychological health problems during pregnancy (Figure 3C). The women having more than three children exhibited a substantial negative correlation with the social relationship domain −0.77 (−1.13 to −0.41, p<0.001), indicating that women with higher parity reported lower social relationship as compared to women with fewer or no children (Figure 3D). The combined effect of all the variables influencing WHOQOL is shown in Figure 3E. This data visualization showed which factors substantially affect patient QOL. These differing patterns observed highlight the complex but important interplay of variables in women diagnosed with GDM and PE. The cofounder control age was significant in each model which can be a potentially confounder need to be controlled for the improvement of internal validity and bias whereas the education was not significant in most of the model.
Descriptive Comparison of Medication Adherence, Depression, and QoL Across Conditions and Trimesters
The substantial disparities in medication adherence, health dimensions, and QoL across medical conditions and pregnancy trimesters are shown in Table 2. Women with PE had substantially higher medication adherence (median MARS: 13 vs 14; p = 0.012) than those with GDM. Women with GDM had considerably better outcomes than those with PE in all WHOQOL areas (p < 0.001). GDM patients reported better overall WHOQOL (median: 88 vs 82; p < 0.001). From the first to the third trimester, there was a gradual reduction in overall health, psychological well-being, social connections, environmental satisfaction, and overall WHOQOL (p < 0.001).
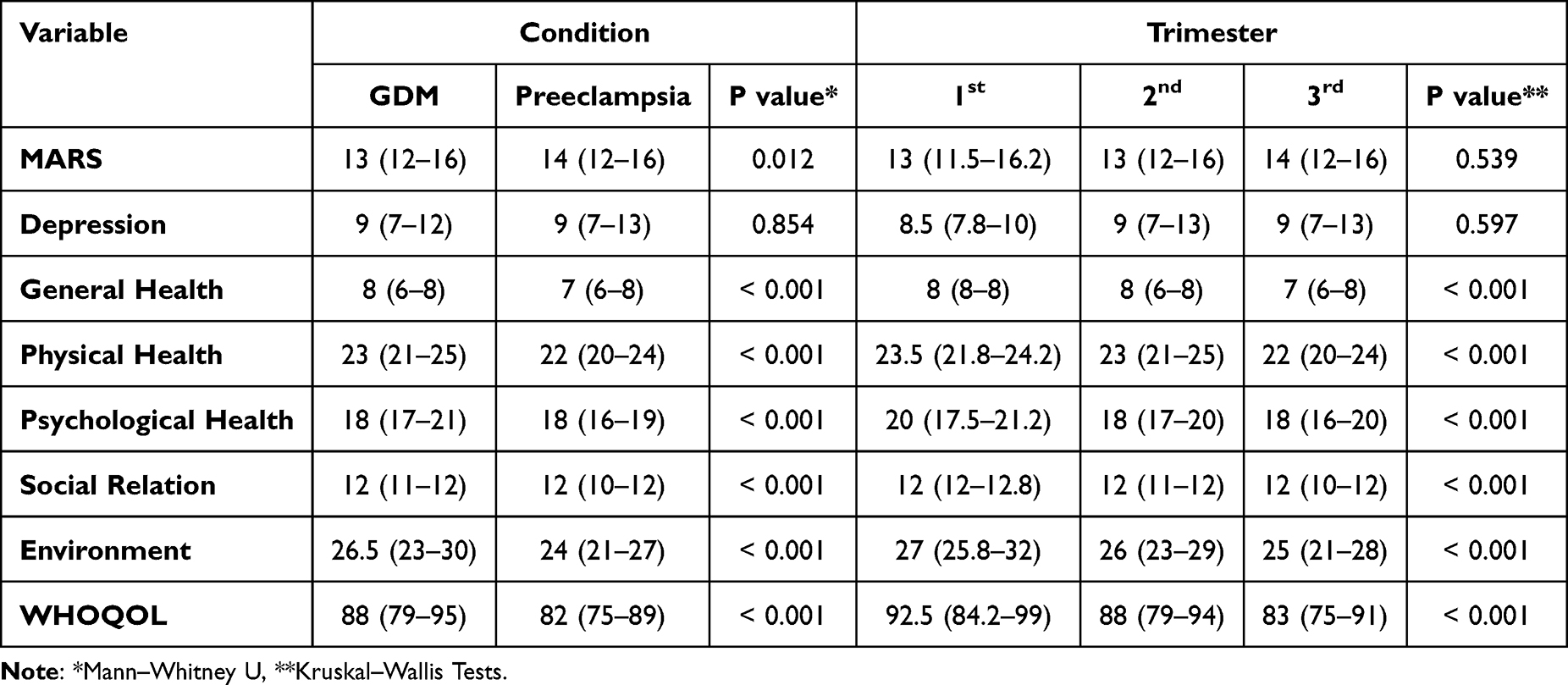 |
Table 2 Descriptive Analysis of Medication Adherence, Depression, and Quality of Life Across Conditions and Trimesters; Median (Q1–Q3) |
Discussion
Maternal health during pregnancy is an important predictor of both short- and long-term outcomes for mothers and newborns. In this cross-sectional study, we investigated the relationship among medication adherence, depression and QoL between women diagnosed with GDM and PE, two of the most common and high-risk conditions affecting pregnant women worldwide and in Pakistan.
Medication adherence during pregnancy has demonstrated a negative but significant association with different HRQoL categories, especially those evaluated by the WHOQOL-BREF, including physical health, psychological well-being, and social interactions in women diagnosed with GDM. This indicates that increased treatment adherence lead to reduced self-reported QoL. Strict regimens may increase treatment burden, lifestyle limitations, monitoring needs, or psychosocial stress. These findings are generally consistent with the study conducted by Saleem, Fahad et al reported that medication adherence in hypertensive patients was found to negatively correlate with HRQoL (EQ-5D).28
Our findings explored the pattern of medication adherence between women diagnosed with GDM and PE during pregnancy. The results showed that better medication adherence was seen in pregnant women with PE as compared to GDM. This is supported by the findings of a multi-site implementation study that observed pregnant women with PE were more likely to adhere to severe hypertension protocols in prenatal care, which included the use of antihypertensives and aspirin, than patients with other hypertensive diseases.29
Depression, an important predictor of physical health in pregnant women diagnosed with PE, showed a significant positive relation with the physical health domain of QoL. The results of our study indicate the positive correlation between depression and physical health and illustrate how emotional discomfort influences women’s perception of their physical well-being. This outcome is supported by the findings of Kelly et al, who observed that antenatal anxiety and depression may enhance the impression of physical symptoms throughout pregnancy.30
Our findings showed that women with GDM showed higher QoL on various dimensions of the WHOQOL-BREF instrument, notably the physical health, psychological health, social relations, and environment domains. The study linked to increased health awareness, more frequent clinical monitoring, and enhanced family support during the high-risk pregnancy period. Contrary to these positive trends, several reports highlight that woman with GDM still demonstrate significantly lower QoL, driven by persistent psychological and lifestyle burdens.31
Our results indicated a notable disparity in QoL across several trimesters, with the peak QoL recorded in the first trimester, followed by a progressive fall in the second and third trimesters. These results are in line with previous study that also reported a lower HRQoL, physical health, and role-physical ratings were seen in the third trimester compared to the first and second trimesters, demonstrating that gestational age is a major predictor of declining QoL.32 Our findings revealed that an increasing number of children was associated with a decline in maternal QoL, particularly in the physical and environmental domains. Our results coincide with a qualitative phenomenological study in North Jordan which reported that pregnant women with four or more children (“high parity”) experienced poorer QoL during gestation compared to lower-parity peers.33 The findings of our study showed that higher maternal education was significantly associated with better QoL, particularly in the physical and psychological domains of WHOQOL-BREF, supported by a cross-sectional study of pregnant women with GDM found a significant positive association between the educational level of the woman (and her spouse) and their GDM-specific quality of life (GDMQoL). Higher educational attainment predicted improved psychological and general health perception, leading to better QoL scores.34
The study has several limitations. The cross-sectional approach limits the capacity to demonstrate causal links between medication adherence, depression, and QoL. Furthermore, the study was performed in particular urban healthcare facilities in Punjab, which may limit the implications of the results to rural populations or other provinces. The use of self-reported measures to assess QoL and adherence may introduce recall or social desirability bias. Furthermore, the study did not evaluate long-term maternal or neonatal outcomes, which offer a more complete picture of the impact of these diseases. Despite these limitations, the study provides a strong foundation for future longitudinal and interventional studies on maternal health in lower-middle income countries.
Conclusion
When compared to women with GDM, preeclamptic women were more likely to take their medication as prescribed. The low adherence scores with WHOQOL categories in GDM patients were attributed to the presence of greater behavioral challenges during pregnancy. However, the significance of depression as a predictor of physical health was observed in preeclamptic patients with WHOQOL scores. Women with GDM frequently reported better overall QoL. Furthermore, demographic variables such as age, education level, parity, and trimester at diagnosis were discovered to impact QoL and adherence patterns, highlighting the varied nature of maternal health throughout pregnancy. These findings underscore the critical role of integrating psychological screening and adherence-focused interventions into standard antenatal care. Such strategies facilitate early detection of psychological distress, enhance treatment compliance and collectively contribute to improve maternal health outcomes and QoL in high-risk pregnancies.
Abbreviations
GDM, Gestational diabetes mellitus; GDMQoL, GDM-specific quality of life; MARS, Medication Adherence Rating Scale; PHQ-9, Patient Health Questionnaire-9; QoL, Quality of life.
Ethical Approval and Consent to Participate
The paradigm used for this study respects the participants’ ethics and dignity. With reference number GCUF/ERC/492-A, ethical permission was acquired by the Government College University, Faisalabad Ethics Review Board. Every procedure used in this study, which involved human subjects, complied with the national and/or institutional research committee’s ethical guidelines. The Declaration of Helsinki and its subsequent revisions’ requirements for confidentiality and anonymity were satisfied. Following an explanation of the study’s goals and voluntary nature, participants provided their informed consent. After that, a consent document was signed. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) research design guidelines were adhered to in this investigation.
Acknowledgments
The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through the Large Research Project under grant number RGP2/676/46.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through the Large Research Project under grant number RGP2/676/46.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Zhang Y, Ding W, Wu T, et al. Pregnancy with multiple high-risk factors: a systematic review and meta-analysis. J Global Health. 2025;15:04027. doi:10.7189/jogh.15.04027
2. Kuppusamy P, Prusty RK, Kale DP. High-risk pregnancy in India: prevalence and contributing risk factors–a national survey-based analysis. J Global Health. 2023;13:04116. doi:10.7189/jogh.13.04116
3. McIntyre HD, Fuglsang J, Kampmann U, Knorr S, Ovesen P. Hyperglycemia in pregnancy and women’s health in the 21st century. Int J Environ Res Public Health. 2022;19(24):16827. doi:10.3390/ijerph192416827
4. Karrar SA, Martingano DJ, Hong PL. Preeclampsia StatPearls [Internet]. StatPearls Publishing; 2024.
5. Paulo MS, Abdo NM, Bettencourt-Silva R, Al-Rifai RH. Gestational diabetes mellitus in Europe: a systematic review and meta-analysis of prevalence studies. Front Endocrinol. 2021;12:691033. doi:10.3389/fendo.2021.691033
6. Bidhendi Yarandi R, Vaismoradi M, Panahi MH, Gåre Kymre I, Behboudi-Gandevani S. Mild gestational diabetes and adverse pregnancy outcome: a systemic review and meta-analysis. Front Med. 2021;8:699412. doi:10.3389/fmed.2021.699412
7. Hanafee A, Suthon S, Innang S, et al. Comparison of maternal characteristics and clinical parameters in Thai pregnant women with and without gestational diabetes mellitus. Diabetes Res Clin Pract. 2025;226:112336. doi:10.1016/j.diabres.2025.112336
8. Gojnic M, Todorovic J, Stanisavljevic D, et al. Maternal and fetal outcomes among pregnant women with diabetes. Int J Environ Res Public Health. 2022;19(6):3684. doi:10.3390/ijerph19063684
9. Lai J, Syngelaki A, Nicolaides KH, von Dadelszen P, Magee LA. Impact of new definitions of preeclampsia at term on identification of adverse maternal and perinatal outcomes. Am J Clin Exp Obstet Gynecol. 2021;224(5):
10. Mou AD, Barman Z, Hasan M, et al. Prevalence of preeclampsia and the associated risk factors among pregnant women in Bangladesh. Sci Rep. 2021;11(1):21339. doi:10.1038/s41598-021-00839-w
11. Mayrink J, Reis ZSN. Pre‐eclampsia in low and middle‐income settings: what are the barriers to improving perinatal outcomes and evidence‐based recommendations? Int J Gynecol Obstet. 2024;164(1):33–10. doi:10.1002/ijgo.14913
12. Mukona D, Munjanja SP, Zvinavashe M, Stray-Pederson B. Barriers of adherence and possible solutions to nonadherence to antidiabetic therapy in women with diabetes in pregnancy: patients’ perspective. J Diabetes Res. 2017;2017(1):3578075. doi:10.1155/2017/3578075
13. Olson DN, Russell T, Ranzini AC. Assessment of adherence to aspirin for preeclampsia prophylaxis and reasons for nonadherence. Ame J Obstet Gynecol MFM. 2022;4(5):100663. doi:10.1016/j.ajogmf.2022.100663
14. Asiedu-Danso M, Kretchy IA, Sekyi JK, Koduah A, Schiattarella A. Adherence to antidiabetic medications among women with gestational diabetes. J Diabetes Res. 2021;2021(1):9941538. doi:10.1155/2021/9941538
15. Nisar A, Yin J, Waqas A, et al. Prevalence of perinatal depression and its determinants in Mainland China: a systematic review and meta-analysis. J Affective Disord. 2020;277:1022–1037. doi:10.1016/j.jad.2020.07.046
16. Arafa A, Dong J-Y. Depression and risk of gestational diabetes: a meta-analysis of cohort studies. Diabetes Res Clin Pract. 2019;156:107826. doi:10.1016/j.diabres.2019.107826
17. Rogers A, Obst S, Teague SJ, et al. Association between maternal perinatal depression and anxiety and child and adolescent development: a meta-analysis. JAMA Pediatrics. 2020;174(11):1082–1092. doi:10.1001/jamapediatrics.2020.2910
18. Jin Y, Wu C, Chen W, Li J, Jiang H. Gestational diabetes and risk of perinatal depression in low-and middle-income countries: a meta-analysis. Front Psychiatry. 2024;15:1331415. doi:10.3389/fpsyt.2024.1331415
19. Dagher RK, Bruckheim HE, Colpe LJ, Edwards E, White DB. Perinatal depression: challenges and opportunities. J Women’s Health. 2021;30(2):154–159. doi:10.1089/jwh.2020.8862
20. Ohene‐Agyei P, Gamble GD, Samuel D, et al. Is a history of gestational diabetes associated with long‐term mental health?—findings from the GEMS 5‐year follow up study. Brain Behav. 2025;15(7):e70666. doi:10.1002/brb3.70666
21. Pantzartzis KA, Manolopoulos PP, Paschou SA, Kazakos K, Kotsa K, Goulis DG. Gestational diabetes mellitus and quality of life during the third trimester of pregnancy. Qual Life Res. 2019;28(5):1349–1354. doi:10.1007/s11136-018-2090-2
22. Martínez-Galiano JM, Hernández-Martínez A, Rodríguez-Almagro J, Delgado-Rodríguez M, Rubio-Alvarez A, Gómez-Salgado J. Women’s quality of life at 6 weeks postpartum: influence of the discomfort present in the puerperium. Int J Environ Res Public Health. 2019;16(2):253. doi:10.3390/ijerph16020253
23. Dalfrà M, Nicolucci A, Bisson T, Bonsembiante B, Lapolla A. Quality of life in pregnancy and post-partum: a study in diabetic patients. Qual Life Res. 2012;21(2):291–298. doi:10.1007/s11136-011-9940-5
24. Rep A, Ganzevoort W, Bonsel GJ, Wolf H, de Vries JI. Psychosocial impact of early-onset hypertensive disorders and related complications in pregnancy. Am J Clin Exp Obstet Gynecol. 2007;197(2):
25. Stone JK, Shafer LA, Graff LA, et al. Utility of the mars-5 in assessing medication adherence in IBD. Inflamm Bowel Dis. 2021;27(3):317–324. doi:10.1093/ibd/izaa056
26. Smith ML, Sanchez SE, Rondon M, Gradus JL, Gelaye B. Validation of the patient health questionnaire-9 (PHQ-9) for detecting depression among pregnant women in Lima, Peru. Curr Psychol. 2022;41(6):3797–3805. doi:10.1007/s12144-020-00882-2
27. Skevington SM, Lotfy M, O’Connell KA. The world health organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004;13(2):299–310. doi:10.1023/B:QURE.0000018486.91360.00
28. Saleem F, Hassali MA, Shafie AA, et al. Does treatment adherence correlates with health related quality of life? Findings from a cross sectional study. BMC Public Health. 2012;12(1):318. doi:10.1186/1471-2458-12-318
29. Kachoria AG, Fatima H, Lightfoot AF, et al. Understanding barriers and facilitators to implementation of a patient safety bundle for pregnancy-related severe hypertension in 3 North Carolina outpatient clinics: a qualitative study. Implement Sci Commun. 2025;6(1):7. doi:10.1186/s43058-024-00685-7
30. Kelly RH, Russo J, Katon W. Somatic complaints among pregnant women cared for in obstetrics: normal pregnancy or depressive and anxiety symptom amplification revisited? Gen Hosp Psychiatry. 2001;23(3):107–113. doi:10.1016/s0163-8343(01)00129-3
31. Won S, Kim HJ, Park JY, et al. Quality of life in women with gestational diabetes mellitus and treatment satisfaction upon intermittently scanned continuous glucose monitoring.JKMS. 2024;40(15):e46–0. doi:10.3346/jkms.2025.40.e46
32. Pobee RA, Setorglo J, Kwashie Klevor M, Murray-Kolb LE. High levels of depressive symptoms and low quality of life are reported during pregnancy in Cape Coast, Ghana; a longitudinal study. BMC Public Health. 2022;22(1):894. doi:10.1186/s12889-022-13299-2
33. Alzboon G, Vural G. The experience of healthy pregnancy in high parity women: a phenomenological study in north Jordan. Medicina. 2021;57(8):853. doi:10.3390/medicina57080853
34. Nazarpour S, Simbar M, Kiani Z, Khalaji N, Khorrami Khargh M, Naeiji Z. The relationship between quality of life and some mental problems in women with gestational diabetes mellitus (GDM): a cross-sectional study. BMC Psychiatry. 2024;24(1):511. doi:10.1186/s12888-024-05960-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Anxiety and Depression Among HIV-Positive and HIV-Negative Pregnant Women During COVID-19 Pandemic in Ekiti State, Southwest Nigeria
Ade-Ojo IP, Dada MU, Adeyanju TB
International Journal of General Medicine 2022, 15:4123-4130
Published Date: 16 April 2022
Relation Among Anxiety, Depression, Sleep Quality and Health-Related Quality of Life Among Patients with Systemic Lupus Erythematosus: Path Analysis
Chen HJ, Wang H, Qiu LJ, Ling HY, Wu LL, Wang TR, Zhou Y, Xue Y, Ye DQ, Wang B
Patient Preference and Adherence 2022, 16:1351-1358
Published Date: 25 May 2022
Quality of Life and the Presence of Depression Among Adults with Hair Loss in the South of Saudi Arabia
Alomaish AR, Gosadi IM, Dallak FH, Darraj AI, Jaafari SM, Alshamakhy AE, Mleeh NT
Psychology Research and Behavior Management 2022, 15:1989-1996
Published Date: 4 August 2022
A Cross-Sectional Study on the Relationship Between Rosacea Severity and Quality of Life or Psychological State
Yang F, Zhang Q, Song D, Liu X, Wang L, Jiang X
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2807-2816
Published Date: 20 December 2022
Level of Depression and Anxiety on Quality of Life Among Patients Undergoing Hemodialysis
Alshelleh S, Alhawari H, Alhouri A, Abu-Hussein B, Oweis A
International Journal of General Medicine 2023, 16:1783-1795
Published Date: 10 May 2023