Back to Journals » International Journal of Women's Health » Volume 18
Longitudinal Assessment of Routine Blood–Derived Inflammatory Indices in Women with Diet-Controlled Gestational Diabetes: A Retrospective Study
Authors Jiang H, Xin W ![]() , Li Z, Gao S
, Li Z, Gao S ![]() , Wang J
, Wang J
Received 2 April 2026
Accepted for publication 6 July 2026
Published 15 July 2026 Volume 2026:18 611520
DOI https://doi.org/10.2147/IJWH.S611520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Hao Jiang,1 Wenxuan Xin,2 Zhongxian Li,3 Songkun Gao,2 Jiandong Wang2
1Department of Gynecology and Obstetrics, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Gynecologic Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, People’s Republic of China; 3Department of Pharmaceutics, School of Pharmacy, Jiamusi University, Jiamusi, Heilongjiang Province, People’s Republic of China
Correspondence: Songkun Gao, Department of Gynecologic Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Dongcheng District, Beijing, People’s Republic of China, Email [email protected] Jiandong Wang, Department of Gynecologic Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Dongcheng District, Beijing, People’s Republic of China, Email [email protected]
Purpose: To characterize longitudinal changes in routine blood count-derived inflammatory indices throughout pregnancy and the early postpartum period in women with diet-controlled gestational diabetes mellitus (GDM A1) compared with normoglycemic controls.
Methods: This retrospective cohort study included 366 pregnant women, comprising 170 women with GDM A1 and 196 normoglycemic controls, who received antenatal care at Beijing Friendship Hospital. Routine complete blood count parameters were collected at seven clinically relevant time windows: 8– 12, 16– 20, 24– 28, 28– 32, and 36 weeks of gestation, immediately before delivery, and postpartum. The aggregate index of systemic inflammation (AISI), systemic inflammation response index (SIRI), systemic immune-inflammation index (SII), lymphocyte-to-monocyte ratio (LMR), monocyte-to-lymphocyte ratio (MLR), and platelet-to-lymphocyte ratio (PLR) were calculated. Exploratory unadjusted between-group comparisons were performed using Mann–Whitney U-tests. Adjusted linear mixed-effects models were used to evaluate group-by-time interactions while accounting for within-subject correlation and baseline covariates.
Results: Women with GDM A1 were older and had higher early-pregnancy BMI than normoglycemic controls. After adjustment for maternal age, early-pregnancy BMI, gravidity, parity, and history of macrosomia, significant group-by-time interactions were observed for all six inflammatory indices, including AISI (P < 0.001), SIRI (P < 0.001), SII (P = 0.017), LMR (P = 0.011), MLR (P = 0.011), and PLR (P = 0.022). In Holm-adjusted post hoc comparisons, SIRI was higher in the GDM A1 group during the postpartum period (adjusted ratio = 1.204, 95% CI: 1.066– 1.360, P = 0.020), and PLR was higher immediately before delivery (adjusted ratio = 1.123, 95% CI: 1.036– 1.217, P = 0.032).
Conclusion: Women with GDM A1 showed altered longitudinal trajectories of CBC-derived inflammatory indices, with the most robust adjusted time-specific differences involving postpartum SIRI and pre-delivery PLR. These indices may provide accessible research markers for characterizing stage-specific inflammatory patterns in diet-controlled GDM, but prospective studies incorporating direct inflammatory and metabolic measurements are required to establish clinical utility.
Keywords: gestational diabetes mellitus, inflammatory indices, pregnancy, lymphocyte-to-monocyte ratio, platelet-to-lymphocyte ratio, systemic immune-inflammation index
Introduction
Gestational diabetes mellitus (GDM) affects approximately 7–25% of pregnancies worldwide, depending on the population and diagnostic criteria used, and is associated with increased risks of hypertensive disorders of pregnancy, cesarean delivery, fetal macrosomia, and neonatal metabolic complications.1–3 Its pathophysiology extends beyond glucose intolerance and involves insulin resistance, dyslipidemia, placental dysfunction, oxidative stress, and chronic low-grade inflammation.4–6 Pro-inflammatory cytokines, maternal adipose tissue inflammation, and altered placental immune signaling may impair insulin signaling, aggravate peripheral insulin resistance, and contribute to adverse maternal and neonatal outcomes.5–8
Pregnancy is accompanied by dynamic changes in maternal immune and inflammatory status, and in GDM this response may be amplified into pathological low-grade inflammation, accompanied by altered adipose tissue and placental inflammatory signaling.6,8 GDM can be clinically classified as diet-controlled GDM (GDM A1) or medication-treated GDM (GDM A2). Women with GDM A1 generally have more favorable maternal and neonatal outcomes than those requiring pharmacological treatment, possibly reflecting better glycemic control and a lower metabolic and inflammatory burden.9 Nevertheless, subtle inflammatory abnormalities may remain detectable even in women whose glucose levels are controlled through diet and exercise alone.
Conventional inflammatory biomarkers, including cytokines and adipokines, require specialized assays and are not routinely available in clinical practice. In contrast, inflammatory indices derived from routine complete blood count parameters are inexpensive, reproducible, and widely accessible. PLR reflects the balance between platelet activation and lymphocyte-mediated immune regulation and has been used as an inflammatory marker in several clinical conditions.10,11 LMR and its reciprocal MLR reflect the balance between lymphocyte-mediated adaptive immunity and monocyte-driven innate inflammation; altered monocyte–lymphocyte balance has been associated with insulin resistance, inflammatory diseases, and subsequent GDM development.12–14 SII integrates platelet, neutrophil, and lymphocyte counts, whereas SIRI combines neutrophil, monocyte, and lymphocyte counts, thereby reflecting overlapping but partially distinct systemic and myeloid inflammatory responses.15–18 AISI further incorporates platelets, neutrophils, monocytes, and lymphocytes and may provide a broader estimate of systemic inflammatory burden.19 GDM-specific studies have also suggested potential clinical relevance for MLR, LMR, SII, SIRI, and AISI in identifying women at increased risk of GDM or related metabolic abnormalities.12,20,21
However, most previous studies evaluated these indices at a single time point, particularly during early pregnancy or around the 24–28-week oral glucose tolerance test window. Consequently, their longitudinal trajectories from early pregnancy through delivery and the postpartum period remain poorly characterized. Moreover, systematic comparisons of multiple complete blood count–derived indices are limited, particularly in women with GDM A1, whose inflammatory abnormalities may be subtler than those observed in medication-treated GDM. Therefore, we conducted a retrospective longitudinal study comparing women with GDM A1 and normoglycemic controls at seven clinically relevant time points. Our objective was to characterize the temporal evolution of AISI, SIRI, SII, LMR, MLR, and PLR and to identify stage-specific inflammatory patterns in diet-controlled GDM.
Methods
Study Design and Participants
We conducted a retrospective cohort study of pregnant women who received antenatal care at Beijing Friendship Hospital, Capital Medical University, between January and June 2025. Women were classified into two groups: diet-controlled gestational diabetes (GDM A1) and normoglycemic control. GDM A1 was diagnosed based on 75-g oral glucose tolerance test (OGTT) results at 24–28 weeks of gestation and the absence of pharmacological therapy throughout pregnancy. Normoglycemic controls were women who delivered at the same institution and had no history of diabetes before or during pregnancy. A total of 393 potentially eligible women were initially identified; after applying the eligibility criteria and data-completeness requirements, 366 women were included in the final analysis, comprising 170 women with GDM A1 and 196 normoglycemic controls. This dataset was previously used in a study examining insulin resistance-related indices in women with GDM A1 and healthy pregnancy.22
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) singleton pregnancy; (2) complete demographic records; (3) complete blood count (CBC) data available for at least five of the seven predetermined time windows; and (4) definitive classification as GDM A1 or normoglycemic based on medical records.
The exclusion criteria were as follows: (1) pre-existing diabetes mellitus; (2) acute or chronic infectious disease; (3) autoimmune disease, hematologic disorder, malignancy, or severe hepatic or renal dysfunction; (4) exposure to systemic corticosteroids, immunosuppressants, or other medications that could substantially affect inflammatory markers during pregnancy; (5) insufficient clinical or laboratory data for analysis; and (6) insulin- or medication-treated GDM.
Diagnostic Criteria and Group Assignment
GDM was diagnosed at 24–28 weeks of gestation using a 75-g OGTT with the following thresholds: fasting glucose ≥5.1 mmol/L, 1-hour glucose ≥10.0 mmol/L, or 2-hour glucose ≥8.5 mmol/L.23 Women meeting these criteria who achieved glycemic targets through diet and exercise alone were classified as having GDM A1. Controls included women with normal OGTT results and no insulin use throughout pregnancy.
Assessment Schedule
CBC results were not collected specifically for research purposes but were obtained from routine antenatal care, GDM screening, peripartum assessment, and postpartum management. For longitudinal analysis, available CBC results were assigned to seven predefined clinical time windows according to the routine antenatal care schedule and recommended pregnancy follow-up points in China: 8–12 weeks, 16–20 weeks, 24–28 weeks, 28–32 weeks, 36 weeks, immediately before delivery, and postpartum. The 8–12-week window represented the early-pregnancy baseline and early maternal immune adaptation; 16–20 weeks represented the early-to-mid-pregnancy transition; 24–28 weeks corresponded to the routine GDM screening window and a period of increased insulin resistance; 28–32 and 36 weeks were used to evaluate inflammatory changes after GDM diagnosis and during late pregnancy; the pre-delivery window reflected peripartum physiological stress; and the postpartum window was used to assess early immune and metabolic recovery after pregnancy.
Data Collection and Inflammatory Index Calculations
Demographic and laboratory variables included maternal age, early-pregnancy body mass index (BMI), gravidity, parity, history of macrosomia, and CBC-derived parameters, including white blood cell count, platelet count, lymphocyte count, monocyte count, and neutrophil count. Six inflammation-associated indices were calculated as follows: LMR = lymphocyte count / monocyte count; MLR = monocyte count / lymphocyte count; PLR = platelet count / lymphocyte count; SII = platelet count x neutrophil count / lymphocyte count; SIRI = monocyte count x neutrophil count / lymphocyte count; and AISI = platelet count x monocyte count x neutrophil count / lymphocyte count.
Statistical Analysis
Continuous variables are presented as median (interquartile range [IQR]) unless otherwise specified, and categorical variables are presented as n (%). Baseline characteristics were compared between groups using Mann–Whitney U-tests for continuous variables and chi-square or Fisher exact tests for categorical variables, as appropriate. Exploratory unadjusted between-group comparisons of inflammatory indices at each time point were performed using Mann–Whitney U-tests.
To account for repeated measurements within participants and potential confounding, adjusted linear mixed-effects models were fitted for each CBC-derived inflammatory index. Because the inflammatory indices were right-skewed, model estimates were obtained from log-transformed outcomes and back-transformed to adjusted ratios. Fixed effects included group, time, the group-by-time interaction, maternal age, early-pregnancy BMI, gravidity, parity, and history of macrosomia. A participant-specific random intercept was included to account for within-subject correlation. Post hoc between-group comparisons at each time point were performed when the group-by-time interaction was significant, and multiplicity was controlled using the Holm method. Adjusted ratios greater than 1 indicate higher values in the GDM A1 group. Spearman correlation analyses were considered exploratory and were interpreted with caution because several indices share mathematical components. All tests were two-tailed, and statistical significance was set at P < 0.05.
Results
A total of 366 women were included in the final analysis, comprising 170 women with diet-controlled GDM (GDM A1) and 196 normoglycemic controls. Baseline characteristics are summarized in Table 1. Women with GDM A1 were older than normoglycemic controls [33.0 (31.0–36.0) vs 32.0 (30.0–34.5) years, P = 0.01] and had a higher early-pregnancy BMI [22.27 (20.70–24.89) vs 20.95 (19.71–23.33) kg/m2, P < 0.01]. Gravidity and parity were also modestly higher in the GDM A1 group (P = 0.025 and P = 0.038, respectively). A previous history of macrosomia was more frequent among women with GDM A1 than among controls [7/170 (4.1%) vs 1/196 (0.5%), P = 0.03]. These baseline differences were considered in the subsequent adjusted longitudinal analyses. Longitudinal complete blood count parameters across the seven time windows are provided in Supplementary Table S1. The unadjusted distributions of CBC-derived inflammatory indices are shown in Supplementary Table S2, and the corresponding exploratory between-group P values are summarized in Supplementary Table S9.
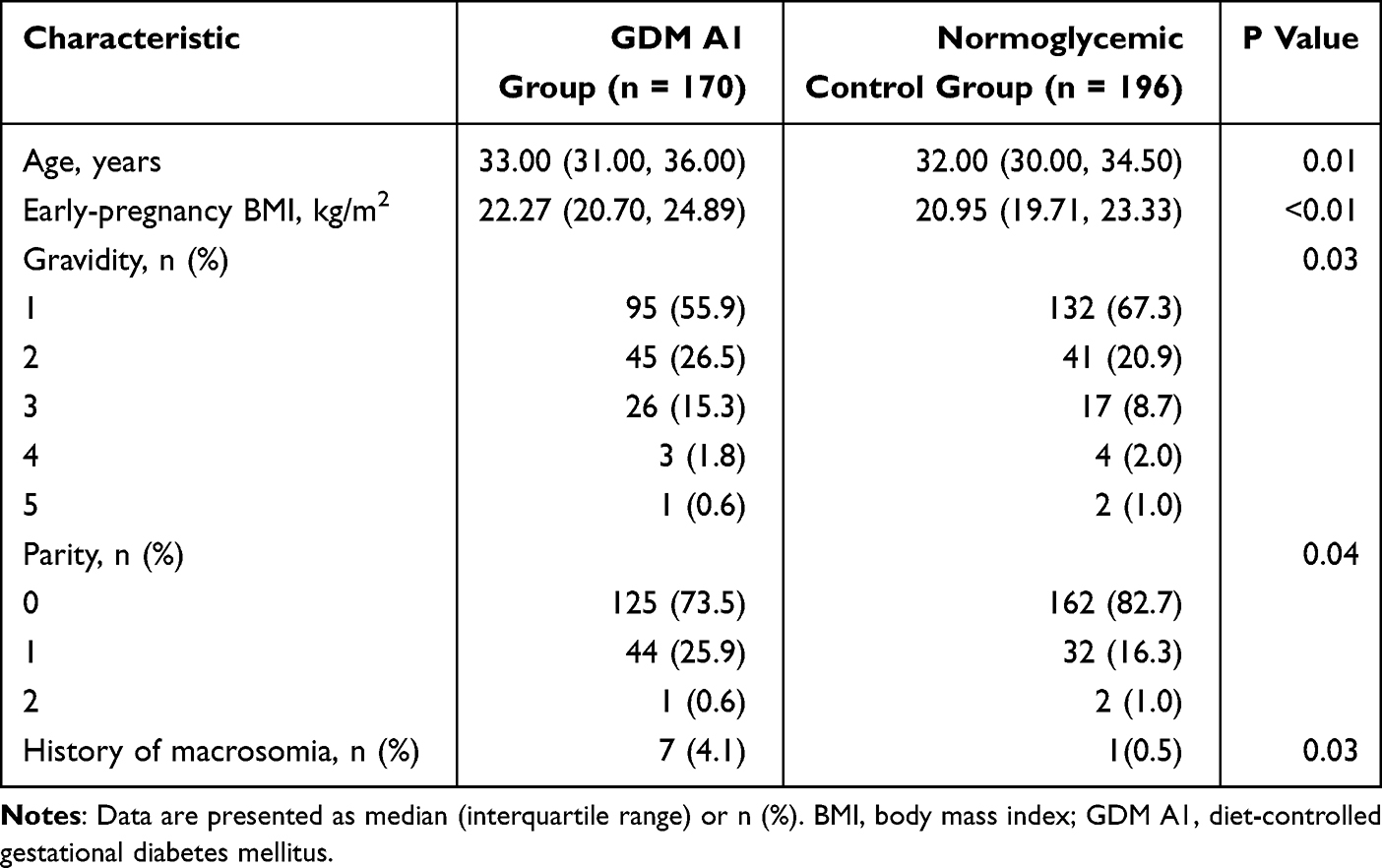 |
Table 1 Baseline Characteristics of Women with GDM A1 and Normoglycemic Controls |
Adjusted linear mixed-effects models were further used to evaluate whether the longitudinal trajectories of CBC-derived inflammatory indices differed between women with GDM A1 and normoglycemic controls after accounting for potential confounders. After adjustment for maternal age, early-pregnancy BMI, gravidity, parity, and history of macrosomia, significant group-by-time interactions were observed for AISI, SIRI, SII, LMR, MLR, and PLR (Table 2). In Holm-adjusted post hoc comparisons, SIRI remained significantly higher in the GDM A1 group during the postpartum period, whereas PLR was significantly higher immediately before delivery. Other indices showed significant overall group-by-time interaction effects, but no individual time-point comparison remained statistically significant after multiplicity correction.
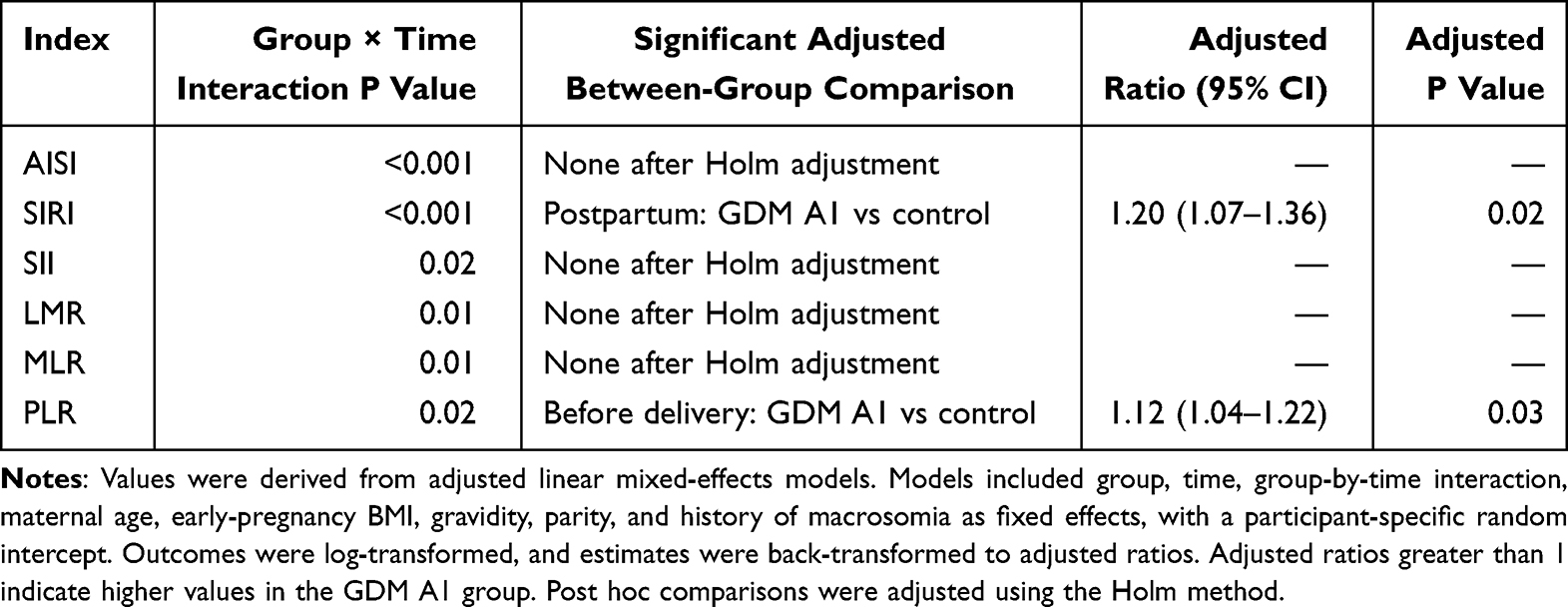 |
Table 2 Adjusted Linear Mixed-Effects Model Results for CBC-Derived Inflammatory Indices |
Descriptive longitudinal patterns are shown in Supplementary Tables 3–8. In general, composite inflammatory indices, particularly AISI, SIRI, and SII, tended to increase during mid-pregnancy, whereas LMR declined progressively and MLR increased toward the postpartum period. PLR showed a less consistent longitudinal pattern, with the clearest between-group difference observed immediately before delivery. Correlation patterns among CBC-derived inflammatory indices are provided in Supplementary Table 10. Composite indices showed moderate-to-strong positive correlations, whereas LMR and MLR were inversely correlated, consistent with their reciprocal mathematical relationship. These correlation findings were considered exploratory and were not used as the primary basis for statistical inference.
Discussion
In this retrospective longitudinal study of women with diet-controlled GDM and normoglycemic controls, we found that CBC-derived inflammatory indices followed different trajectories across pregnancy and the early postpartum period. After adjustment for maternal age, early-pregnancy BMI, gravidity, parity, and history of macrosomia, all six indices showed significant group-by-time interactions, suggesting that GDM A1 was associated with altered temporal patterns of systemic inflammatory surrogates. However, after Holm correction for post hoc comparisons, only two time-specific between-group differences remained statistically significant: higher SIRI in women with GDM A1 during the postpartum period and higher PLR immediately before delivery. These findings support the presence of stage-specific hematological differences in GDM A1, while also emphasizing the need for cautious interpretation of individual time-point comparisons.
Exploratory unadjusted analyses suggested that between-group differences were concentrated in mid-pregnancy and postpartum. Higher AISI and SIRI values at 16–20 weeks, and higher AISI and SII values at 24–28 weeks, are consistent with the concept that metabolic and inflammatory differences may become more apparent as pregnancy-related insulin resistance increases. Nevertheless, these unadjusted differences should not be interpreted as independent biomarkers after confounder adjustment and multiplicity correction. Rather, they indicate time windows in which CBC-derived inflammatory patterns may be more likely to differ between women with GDM A1 and normoglycemic controls.
The adjusted post hoc finding of higher postpartum SIRI in the GDM A1 group may reflect persistent differences in neutrophil-, monocyte-, and lymphocyte-related hematological patterns after pregnancy. Because SIRI is calculated from routine blood cell counts, it cannot directly demonstrate myeloid activation or specific inflammatory pathway involvement. However, this finding is clinically relevant because women with a history of GDM have an elevated long-term risk of type 2 diabetes,24 and postpartum inflammatory or metabolic differences may represent an important area for future follow-up studies. Prospective research incorporating direct measures of insulin resistance, cytokines, and immune cell phenotypes is required to determine whether postpartum SIRI is associated with later metabolic risk.
The adjusted pre-delivery elevation in PLR may reflect differences in platelet-lymphocyte balance during the peripartum period. Platelet activation, coagulation-inflammatory crosstalk, oxidative stress, and systemic physiological stress are all prominent near delivery.10,25,26 The fact that PLR remained significantly different after adjustment and Holm correction suggests that platelet-related inflammatory surrogates may be particularly sensitive to peripartum differences in women with GDM A1. However, platelet activation markers and coagulation parameters were not measured in this study; therefore, the biological basis of this association remains speculative.
Previous studies have evaluated CBC-derived inflammatory indices in GDM at different gestational stages, but the reported dominant markers have varied. Yildiz et al found that first-trimester SII and SIRI were higher in women who subsequently developed GDM,27 whereas Bozbay et al reported higher first-trimester SII and LMR in the GDM group, without significant differences in PLR or NLR.28 Baki Yildirim et al reported that early second-trimester MLR predicted subsequent GDM.12 Karatas et al found that first-trimester AISI and SII had predictive value for subsequent GDM and obstetric outcomes,20 and Hashemipour et al observed higher early-pregnancy NLR, SII, SIRI, and AISI among women who later developed GDM, although some associations attenuated after adjustment for insulin resistance and other confounders.21 Xie et al further reported positive associations of SII and SIRI with incident GDM in a prospective birth cohort,29 while Ergani et al suggested that SII differences may depend on gestational stage.30
Studies of platelet-related indices have also produced inconsistent results. Zhao et al reported that first-trimester PLR and NLR were elevated in women who subsequently developed GDM and were positively correlated with OGTT glucose values at 24–28 weeks.31 In contrast, Sargin et al found limited screening utility for NLR and PLR,32 and meta-analytic evidence has suggested substantial heterogeneity across studies evaluating neutrophil-to-lymphocyte ratio in GDM.33 Differences in sampling time, GDM phenotype, disease severity, participant characteristics, and statistical adjustment may explain these discrepancies. Our findings add to this literature by showing that inflammatory indices may have time-dependent associations in the specific context of diet-controlled GDM.
Several of the evaluated indices share mathematical components, and this should guide interpretation. LMR is the reciprocal of MLR; SII is mathematically related to PLR multiplied by the neutrophil count; SIRI is related to MLR multiplied by the neutrophil count; and AISI can be expressed as SII multiplied by the monocyte count or as SIRI multiplied by the platelet count. Therefore, correlations among these indices are expected and should not be interpreted as evidence of synchronized biological activation. Future studies should avoid treating these indices as independent biomarkers without assessing collinearity and should consider whether simpler component counts provide comparable information.
A strength of this study is the longitudinal assessment of multiple CBC-derived inflammatory indices across seven clinically relevant time windows from early pregnancy to postpartum. In addition, the analysis focused specifically on women with GDM A1, a group in whom inflammatory abnormalities may be subtler than in medication-treated GDM. The use of adjusted linear mixed-effects models allowed us to account for repeated measurements and important baseline differences between groups.
Limitations
This study has several limitations. First, its retrospective observational design precludes causal inference, and reverse causation cannot be excluded. Differences in CBC-derived indices may precede GDM, result from metabolic dysregulation after GDM development, or arise from shared determinants such as maternal age, adiposity, insulin resistance, and other metabolic characteristics. Although we adjusted for several baseline covariates, residual confounding remains possible. Second, CBC data were obtained from routine clinical care rather than from a prospective fixed-interval sampling protocol. Therefore, sampling density and the number of available observations differed across time windows, and missing data may have affected longitudinal estimates. Third, we did not measure C-reactive protein, IL-6, TNF-alpha, adipokines, insulin resistance indices at each time point, immune cell phenotypes, leukocyte activation states, platelet activation markers, or molecular inflammatory pathways. Consequently, the observed hematological associations cannot be interpreted as direct evidence of activation of specific immune mechanisms. Fourth, several indices share formula components, leading to expected statistical interdependence and limiting their interpretation as independent biomarkers. Finally, this was a single-center study, and the findings may not be generalizable to other populations, different diagnostic criteria, or women with medication-treated GDM. External validation in prospective multicenter cohorts is required.
Conclusions
Women with diet-controlled GDM showed altered longitudinal trajectories of CBC-derived inflammatory indices from pregnancy to the early postpartum period. After adjustment for baseline covariates and within-subject correlation, all six indices showed significant group-by-time interactions, while postpartum SIRI and pre-delivery PLR remained significant in Holm-adjusted post hoc comparisons. These findings suggest that CBC-derived indices may help characterize stage-specific inflammatory patterns in GDM A1, but their clinical utility and mechanistic significance require confirmation in prospective studies incorporating direct inflammatory and metabolic measurements.
Ethical Approval
The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and was approved by the ethics committee of Beijing Friendship Hospital, Capital Medical University (YYXSSC-2022-209). The ethics committee felt that this study could exempt patients from obtaining informed consent and that the eligibility of potential participants was established by reviewing their medical records. As this was a retrospective study and all patient treatments and outcomes had already been determined, the ethics committee waived the requirement for informed consent.All patients’ privacy is ensured by assigning anonymous codes instead of personal identifiers.
Acknowledgments
This manuscript was edited for language and style by Kimi, an artificial intelligence (AI) language model developed by Moonshot. Kimi assisted in refining the text to ensure clarity, coherence, and adherence to the scientific writing standards. The authors are responsible for the content and error.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no specific grants from any funding agency in the public, commercial, or not-for-profit sector.
Disclosure
All authors have no conflicts of interest to declare in this work.
References
1. Simmons D, Immanuel J, Hague WM, et al. TOBOGM Research Group. Regression from early gdm to normal glucose tolerance and adverse pregnancy outcomes in the treatment of booking gestational diabetes mellitus study. Diabetes Care. 2024;47(12):2079–8. PMID: 38551955. doi:10.2337/dc23-2215
2. Zhang Y, Wang D, Su J, et al. Effect of trace elements on neurodevelopment in offspring after maternal gestational diabetes mellitus, and related potential mechanisms: a narrative review. Nutr Rev. 2025;83(11):2197–2208. PMID: 40523008. doi:10.1093/nutrit/nuaf076
3. Damm P, Houshmand-Oeregaard A, Kelstrup L, Lauenborg J, Mathiesen ER, Clausen TD. Gestational diabetes mellitus and long-term consequences for mother and offspring: a view from Denmark. Diabetologia. 2016;59(7):1396–1399. Epub 2016 May 12. PMID: 27174368. doi:10.1007/s00125-016-3985-5
4. Chen W, Luo M, Guo J, et al. Metabolic pathways mediating insulin resistance and gestational diabetes mellitus discovered by high-dimensional systematic Mendelian randomization. Cardiovasc Diabetol. 2025;24(1):195. PMID: 40346526; PMCID: PMC12065323. doi:10.1186/s12933-025-02746-0
5. Mittal R, Prasad K, Lemos JRN, Arevalo G, Hirani K. Unveiling Gestational Diabetes: an Overview of Pathophysiology and Management. Int J Mol Sci. 2025;26(5):2320. PMID: 40076938; PMCID: PMC11900321. doi:10.3390/ijms26052320
6. Saucedo R, Ortega-Camarillo C, Ferreira-Hermosillo A, Díaz-Velázquez MF, Meixueiro-Calderón C, Valencia-Ortega J. Role of Oxidative Stress and Inflammation in Gestational Diabetes Mellitus. Antioxidants. 2023;12(10):1812. PMID: 37891891; PMCID: PMC10604289. doi:10.3390/antiox12101812
7. Chen B, Chen X, Li J, et al. Tunneling nanotube-mediated stem cell immunomodulation dysfunction promotes adipose inflammation and insulin resistance in GDM. Cell Rep. 2025;44(11):116505. Epub 2025 Nov 3. PMID: 41187060. doi:10.1016/j.celrep.2025.116505
8. Pinto Y, Frishman S, Turjeman S, et al. Gestational diabetes is driven by microbiota-induced inflammation months before diagnosis. Gut. 2023;72(5):918–928. Epub 2023 Jan 10. PMID: 36627187; PMCID: PMC10086485. doi:10.1136/gutjnl-2022-328406
9. Nataly F, Hadas GH, Ohad G, Letizia S, Michal K. Is there a difference in placental pathology in pregnancies complicated with gestational diabetes A2 versus gestational diabetes A1, versus one abnormal value, on 100 gr glucose tolerance test? Placenta. 2022;120:60–64. Epub 2022 Feb 16. PMID: 35217317. doi:10.1016/j.placenta.2022.02.009
10. Tao J, Huang Y, Li Y, Dai W. Platelet-to-lymphocyte ratio and serum hsCRP levels in third trimester and adverse pregnancy outcomes in women with gestational diabetes mellitus. Sci Rep. 2023;13(1):20963. doi:10.1038/s41598-023-48371-3
11. Wang R-H, Wen W-X, Jiang Z-P, et al. The clinical value of neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), platelet-to-lymphocyte ratio (PLR) and systemic inflammation response index (SIRI) for predicting the occurrence and severity of pneumonia in patients with intracerebral hemorrhage. Front Immunol. 2023;14:1115031. PMID: 36860868; PMCID: PMC9969881. doi:10.3389/fimmu.2023.1115031
12. Baki Yıldırım S, Bezirganoglu Altuntas N, Bayoglu Tekin Y. Monocyte-to-lymphocyte ratio in the early second trimester is a predictor of gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2024;37(1):2371979. Epub 2024 Jul 11. PMID: 38991941. doi:10.1080/14767058.2024.2371979
13. Torres-Torres J, Monroy-Muñoz IE, Perez-Duran J, et al. Cellular and Molecular Pathophysiology of Gestational Diabetes. Int J Mol Sci. 2024;25(21):11641. doi:10.3390/ijms252111641
14. Tan S, Yang X, Mu X, et al. The predictive role of peripheral serum inflammatory markers NLR, PLR, and LMR in ulcerative colitis and Crohn’s disease: a systematic review and meta-analysis. Front Immunol. 2025;16:1623899. Erratum in: Front Immunol. 2025;16:1676750. PMID: 40881709; PMCID: PMC12381567. doi:10.3389/fimmu.2025.1623899
15. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
16. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
17. Menyhart O, Fekete JT, Győrffy B. inflammation and colorectal cancer: a meta-analysis of the prognostic significance of the Systemic Immune-Inflammation Index (SII) and the systemic inflammation response index (SIRI). Int J Mol Sci. 2024;25(15):8441. PMID: 39126008; PMCID: PMC11312822. doi:10.3390/ijms25158441
18. Xia Y, Xia C, Wu L, Li Z, Li H, Zhang J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and Risk of All-Cause Mortality and Cardiovascular Mortality: a 20-Year Follow-Up Cohort Study of 42,875 US Adults. J Clin Med. 2023;12(3):1128. PMID: 36769776; PMCID: PMC9918056. doi:10.3390/jcm12031128
19. Zinellu A, Paliogiannis P, Carru C, Mangoni AA. The aggregate index of systemic inflammation: a novel prognostic biomarker in idiopathic pulmonary fibrosis. J Clin Med. 2021;10(18):4134. doi:10.3390/jcm10184134
20. Karatas E, Tanacan A, Ozkavak OO, et al. Predictive Value of First-Trimester Aggregate Index of Systemic Inflammation (AISI) and Other Inflammatory Indices for Gestational Diabetes Mellitus and Associated Obstetric Outcomes. Am J Reprod Immunol. 2025;93(4):e70069. PMID: 40184028. doi:10.1111/aji.70069
21. Hashemipour S, Kalantarian SS, Panahi H, et al. The association of inflammatory markers in early pregnancy with the development of gestational diabetes: qazvin maternal and neonatal metabolic study (QMNS). BMC Pregnancy Childbirth. 2025;25(1):135. PMID: 39934746; PMCID: PMC11816776. doi:10.1186/s12884-025-07267-y
22. Jiang H, Shang M, Gao S. Insulin Resistance in GDM A1 vs Healthy Pregnancy: a Comparative Study Using METS-IR and TyG Index. Int J Womens Health. 2025;17:3789–3797. doi:10.2147/IJWH.S557974
23. Obstetrics Subgroup, Chinese Society of Obstetrics and Gynecology, Chinese Medical Association; Chinese Society of Perinatal Medicine, Chinese Medical Association; Committee of Pregnancy with Diabetes Mellitus, China Maternal and Child Health Association. Guideline of diagnosis and treatment of hyperglycemia in pregnancy (2022) [Part two]. Zhonghua Fu Chan Ke Za Zhi. 2022;57(2):81–90. PMID: 35184468. doi:10.3760/cma.j.cn112141-20210917-00529
24. Bellamy L, Casas JP, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet. 2009;373(9677):1773–1779. PMID: 19465232. doi:10.1016/S0140-6736(09)60731-5
25. Hung TH, Chen SF, Hsieh TT, Lo LM, Li MJ, Yeh YL. The associations between labor and delivery mode and maternal and placental oxidative stress. Reprod Toxicol. 2011;31(2):144–150. Epub 2010 Nov 27. PMID: 21115112. doi:10.1016/j.reprotox.2010.11.009
26. Hu Y, Huang K, Sun Y, et al. Placenta response of inflammation and oxidative stress in low-risk term childbirth: the implication of delivery mode. BMC Pregnancy Childbirth. 2017;17(1):407. PMID: 29207957; PMCID: PMC5718001. doi:10.1186/s12884-017-1589-9
27. Yildiz EG, Tanacan A, Okutucu G, Bastemur AG, Ipek G, Sahin D. Can System Inflammation Response Index or Systemic Immune Inflammation Index predict gestational diabetes mellitus in the first trimester? A prospective observational study. Int J Gynaecol Obstet. 2024;166(2):837–843. Epub 2024 Mar 1. PMID: 38426227. doi:10.1002/ijgo.15442
28. Bozbay N, Medinaeva A, Akyürek F, Orgul G. The role of first-trimester systemic immune-inflammation index for the prediction of gestational diabetes mellitus. Rev Assoc Med Bras. 2024;70(10):e20240532. PMID: 39356958; PMCID: PMC11444230. doi:10.1590/1806-9282.20240532
29. Xie S, Zhang E, Gao S, et al. Associations of systemic immune-inflammation index and systemic inflammation response index with maternal gestational diabetes mellitus: evidence from a prospective birth cohort study. Chin Med J. 2025;138(6):729–737. Epub 2024 Dec 6. PMID: 39648043; PMCID: PMC11925413. doi:10.1097/CM9.0000000000003236
30. Ergani SY, Yücel KY, Şahin B, et al. The role of inflammation in cases with gestational diabetes mellitus: systemic immune inflammatory index according to trimesters. Am J Reprod Immunol. 2024;91(1):e13806. PMID: 38282603. doi:10.1111/aji.13806
31. Zhao X, Sun J, Yuan N, Zhang X. A prospective cohort study on the association between neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios and gestational diabetes mellitus in Chinese pregnant women. Front Endocrinol. 2025;16:1477092. PMID: 40297173; PMCID: PMC12034551. doi:10.3389/fendo.2025.1477092
32. Sargın MA, Yassa M, Taymur BD, Celik A, Ergun E, Tug N. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios: are they useful for predicting gestational diabetes mellitus during pregnancy? Ther Clin Risk Manag. 2016;12:657–665. PMID: 27217758; PMCID: PMC4853164. doi:10.2147/TCRM.S104247
33. Pace NP, Vassallo J. Association Between Neutrophil-Lymphocyte Ratio and Gestational Diabetes-A Systematic Review and Meta-Analysis. J Endocr Soc. 2021;5(7):bvab051. PMID: 34095691; PMCID: PMC8169042. doi:10.1210/jendso/bvab051
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Pre-Pregnancy Hemoglobin Level on the Association Between Pre-Pregnancy Body Mass Index and Gestational Diabetes Mellitus: A Retrospective Cohort Study in a Single Center in China
Wu K, Ke HH, Gong W, Hu H, Chen L
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3767-3775
Published Date: 8 December 2022
Serum Uric Acid-to-Serum Creatinine Ratio, Thyroid Function, and Gestational Diabetes Mellitus Risk during Early Pregnancy among Chinese Women
Song S, Duo Y, Zhang Y, Qiao X, Chen Y, Fu Y, Dong Y, Yuan T, Zhao W
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2235-2246
Published Date: 7 July 2025
A Comparative Cross-Sectional Study Between Gestational Diabetes Mellitus and Preeclampsia: Medication Adherence, Depression and Quality of Life
Noor R, Abbas G, Khurram H, Aslam A, Randhawa FA, Assiri A, Shah S
International Journal of Women's Health 2026, 18:565083
Published Date: 8 January 2026
Associated Factors for Cesarean Section in Pregnant Women with Gestational Diabetes Mellitus
Liu H, Fu B, Gao L, Wang F, Ji Q, Chen C, Lin C, Fan C, Chen K
International Journal of Women's Health 2026, 18:586026
Published Date: 28 May 2026