Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Rotavirus Prevalence in Children with Acute Gastroenteritis Admitted to a Tertiary Hospital in Somalia in 2020-2023: A Retrospective, Single-Center Study
Authors Orhan Z, Mohamud SM ![]() , Mohamud RYH
, Mohamud RYH ![]() , Doğan S
, Doğan S ![]()
Received 24 April 2024
Accepted for publication 11 November 2024
Published 27 November 2024 Volume 2024:15 Pages 365—373
DOI https://doi.org/10.2147/PHMT.S475345
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Zerife Orhan,1 Said Mohamed Mohamud,2 Rahma Yusuf Haji Mohamud,3 Serpil Doğan2
1Department of Medical Microbiology, Vocational School of Health Services, Kahramanmaraş Sütçü Imam University, Kahramanmaraş, Turkey; 2Department of Medical Microbiology, Mogadishu Somalia Turkey Recep Tayyip Erdogan Training and Research Hospital, Mogadishu, Somalia; 3Department of Nursing, Mogadishu Somali Turkiye Recep Tayyip Erdogan Training and Research Hospital, Mogadishu, Somalia
Correspondence: Rahma Yusuf Haji Mohamud, Department of Nursing, Mogadishu Somali Turkiye Recep Tayyip Erdogan Training and Research Hospital, Mogadishu, Somalia, Tel +252615216313, Email [email protected]
Purpose: Rotavirus is the leading cause of severe and fatal diarrhea in African children. The aim of this study is to investigate the prevalence of rotavirus in children with acute gastroenteritis admitted to a tertiary hospital in Somalia.
Patients and Methods: 5804 children who applied with complaints of acute gastroenteritis between January 2020 and December 2023 were examined retrospectively. Rotavirus antigens were detected in the feces of 1324 patients by qualitative immunochromatographic analysis. The frequency of rotavirus gastroenteritis was evaluated according to age, gender and seasonal distribution. Statistical analysis was done using SPSS version 22.0.
Results: In the years, an increase in the number of patients tested with suspicion of rotavirus and an increase in rotavirus positivity was observed. While the positivity rate was 8.1% (n = 107) in 2020, it increased to 41.4% (n = 548) in 2023. Viral antigens were identified in 1324 of 5804 patients (22.8%). 743 (56.1%) of the children were boys and 581 (43.9%) were girls. The incidence of rotavirus positive cases was higher in the summer and spring months and in children aged 0– 2 years (78.6%) (p< 0.001). Diarrhea due to rotavirus was seen throughout the year. The monthly rotavirus antigen positivity rate in patients admitted to the hospital due to acute gastroenteritis reached its peak in May with 17.2%.
Conclusion: The results of this study showed us that rotavirus is a common cause of acute gastroenteritis in infants. Rotavirus gastroenteritis, which causes significant mortality and morbidity all over the world, is still seen at a high rate of 22.8% in Somalia. We are of the opinion that public health education, good hygiene practices and an effective vaccination program can reduce rotavirus infection.
Keywords: children, rotavirus, prevalence, Somalia
Introduction
Rotavirus is the leading cause of severe diarrhea among infants and young children in both developed and developing countries. This virus is widespread in the population and individuals can be infected multiple times throughout their lives, usually through fecal-oral transmission.1 every year, approximately 25 million people worldwide apply to outpatient clinics, 2 million children are hospitalized 2 and 453,000 children die due to rotavirus diarrhea.2,3 According to the World Health Organization’s 2013 epidemiological data, rotavirus is shown as the main cause of acute watery diarrhea in Somalia (64%).4 85% of rotavirus deaths occur in African and Asian countries with limited resources.2,3 Rotavirus has been reported to cause more than 258,000,000 infections and approximately 128,500 deaths worldwide, in children under five years of age in 2016.1 Rotavirus infection causes approximately 3 million cases of diarrhea and an estimated 55,000 hospitalizations due to diarrhea and dehydration in children under five years of age in the United States each year; however, these infections cause relatively few deaths in the United States.5
Rotavirus diarrhea occurs at a younger age in children in developing countries than in children in developed countries. In many African and Asian countries, the average age of children hospitalized due to rotavirus diarrhea is 6–9 months, and up to 80% of them are under one year old. However, in developed countries, the average age is 13–16 months and the majority of cases occur in the second year of life.6,7
Seasonal fluctuations in infectious diseases, and especially in rotavirus infection, are a well-known phenomenon.8 A study on the burden and epidemiology of rotavirus diarrhea in selected African countries found that rotavirus infections occurred in all countries throughout the year, but the prevalence generally reached its peak in the cool, dry months.9
One of the most important reasons for the high incidence of rotavirus in Somalia is the difficulties in accessing clean water and poor water quality. Poor hygiene and contaminated water sources contribute to the spread of waterborne diseases such as rotavirus.10
Some studies have reported reductions in rotavirus infections and deaths in recent years as a result of advances in safe water, sanitation, and medical care, as well as advances in precautions and treatment, such as the use of rotavirus vaccines.11 However, the burden of rotavirus remains high and remains a significant cause of diarrhea worldwide.12,13
In 2013, WHO published a report recommending the use of rotavirus vaccines in all national immunization programs, particularly in South and Southeast Asia and Sub-Saharan Africa. However, Somalia did not include rotavirus vaccine in its routine immunization program.14
There is only one study on the prevalence of rotavirus in children with acute gastroenteritis in Somalia. Therefore, this study aimed to investigate the prevalence of rotavirus in children with acute gastroenteritis admitted to a tertiary hospital in Somalia between 2020 and 2023.
Materials and Methods
Study Setting and Population
The place where the stool samples were collected is Mogadishu, the largest city in Somalia. Mogadishu, located in the southeastern Indian Ocean region of Somalia, is a city with an urban population of approximately 3 million and limited basic sanitation, water and sanitation services. The climate is dry and hot and rainfall is quite low.
Population and Sample
In this study, children aged 0–17 years who complained of diarrhea were targeted. A total of 5804 stool samples sent to the Medical Microbiology Laboratory of our hospital for four years were included in this study.
Sample Collection and Method
In this study, stool samples were collected in stool containers with spoons. The samples collected from the patients were studied daily with the rapid immunochromatographic method (Rotavirus antigen test; Turklab, Turkey) after they were accepted to the laboratory. The sensitivity of the test for adenovirus was reported as 100%, the specificity as 99.0%, and for rotavirus as 100% and specificity as 98.0%. After the sample was taken into collection containers in line with the company’s recommendations, approximately 50 mg of fecal samples were taken from 3 different regions for solid samples, diluted and dropped. Liquid samples were dropped directly into the sample compartment on the cassette in two drops (approximately 80 μL). Samples with a colored line in the T1 region after 10 minutes were considered positive for rotavirus. Test results, annual distributions, and demographic data of the patients were scanned retrospectively.
Ethical Consideration
Ethical approval was obtained for this study from the clinical research ethics committee of Mogadishu Somalia – Turkey Recep Tayyip Erdoğan Training and Research Hospital (date: 08.11.2023, Decision no: 879, Number: MSTH/16083) and the study was conducted in accordance with the Declaration of Helsinki. Since the hospital ethics committee approved this retrospective study, all patients were anonymous, and independent informed consent was not required.
Statistical Analysis
In the evaluation of the data, the differences in the frequency distributions of the qualitative variables according to the groups were examined with the Chi-square test and Fisher exact test. The effect of independent variables on the dependent variable was examined with logistic regression analysis. Statistical parameters are expressed as n and %. Statistical significance was accepted as p<0.05. IBM SPSS version 22 program was used to evaluate the data.
Results
Viral antigens were detected in a total of 1324 (22.8%). It was determined that both positivity and negativity rates increased in the distribution of rotavirus results over the years. The rotavirus positivity rate was found to be 43.9% (n=581) in girls and 56.1% (n=743) in boys, and there was no statistically significant relationship between girls and boys (p=0.698). A statistically significant difference was detected in the distribution of Rotavirus results according to age groups. While rotavirus positivity was observed at very high rates in the 0–2 age group (78.6%) (p<0.001), it was determined that the rates of rotavirus positivity decreased as the age level increased (2% for those aged 12 and above). Statistically significant differences were detected in the distribution of rotavirus results according to seasons (p<0.001). While rotavirus positivity reached the highest rate in the summer (32.6%), it was observed to be the lowest in the autumn (15.6%) (Table 1).
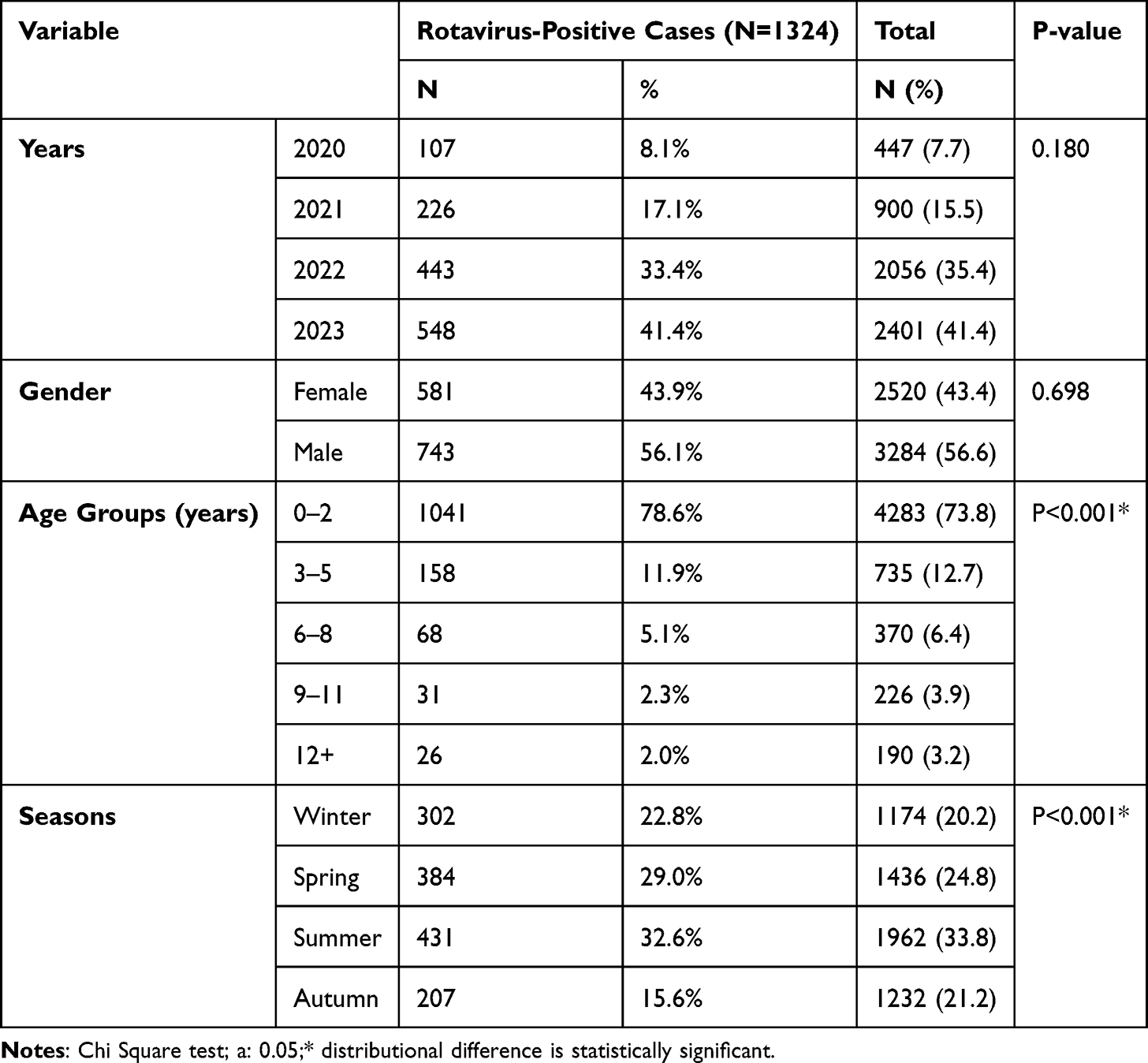 |
Table 1 Distribution of Rotavirus Test Results by Year, Gender, Age Groups, and Seasons |
According to logistic regression analysis, differences between years (2022 is significant compared to 2020), differences between seasons (spring, summer and autumn seasons are significant compared to winter) or differences between age groups (3–5 age group and 6–8 age group are significant compared to 0–2 age group) have an effect on the observation of rotavirus (Table 2).
 |
Table 2 Logistic Regression Analysis |
Discussion
Rotavirus is one of the common causes of viral gastroenteritis in infants and young children.15 In Somalia, 9000 children under the age of five die every year due to diarrhea. Inequality in access to clean water and sanitation is a major cause of diarrhea in Somalia and other low-income countries.16
One of the important findings of this study is that rotavirus has increased significantly in children over the years. The positivity rate, which was 8.1% in 2020, increased to 41.4% in 2023 (Figure 1, Table 1). Consistent with our study, Tanaka et al17 reported in their study in Bangladesh that the rate of diarrheal cases attributable to rotavirus almost doubled in the 2002–2004 period compared to 1993–1995 (42% versus 22%, P<0.001). Sarker et al18 reported ın their study that while the general isolation rate of rotavirus was approximately 25% in 1993–1997, this rate increased to 42% in 2008–2012.
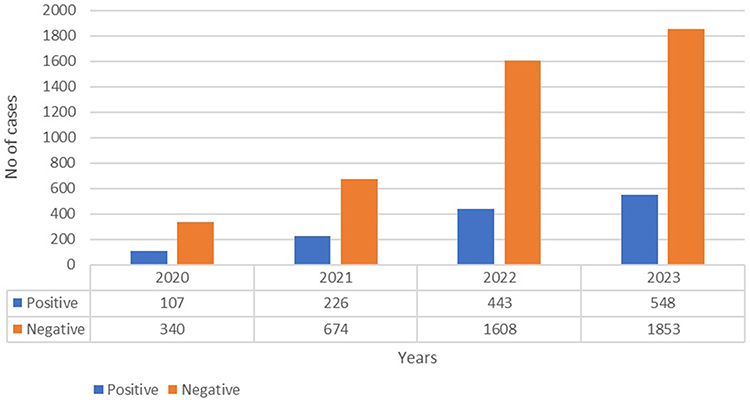 |
Figure 1 Annual distribution of rotavirus antigen positivity and negativity numbers. The annual distribution of rotavirus antigen positivity and negativity numbers. Of the 5804 children tested during the four-year period, 1324 (22.8%) were found to be positive for the rotavirus antigen, while 4480 (77.2%) were negative. Over the years, an increase has been observed in the number of patients tested with suspicion of rotavirus and their positivity for and rotavirus. The positivity rate was seen as 8.1% (n=107), 17.1% (n=226), 33.4% (n=443), 41.4% (n=548) between 2020 and 2023, respectively. |
Osman et al19 reported a rotavirus positivity rate of 17.8% in a similar study conducted in Somalia. The frequency of rotavirus positivity in acute gastroenteritis cases varies from country to country and even from region to region within the same country. In the global rotavirus surveillance system bulletin, the average rotavirus positivity rate in 2008 was reported as 21–44% in Africa, 16–42% in America, 23–57% in Asia and 13–57% in Europe.20 CDC worldwide surveillance data revealed that 40% of 62,584 hospitalizations for diarrhea were due to rotavirus infection.21 In this study, the four-year prevalence of rotavirus antigen in Somalia was determined to be 22.8% (Figure 1). In similar studies conducted in India and Venezuela, rotavirus antigen positivity was detected at rates similar to our study (24%, 21.3%).22,23 Our results are lower than those reported in India (36.9%)24 Denmark (39%)25 and Bangladesh (40%).26
In this study, it was observed that there was no significant difference between girls and boys in terms of rotavirus positivity. However, the incidence of the disease was higher in boys (56.1%) (Table 1). This situation is similar to the findings of previous studies. While some studies reported higher but insignificant rates of rotavirus in boys than girls,27,28 other studies reported significantly higher infections in boys than girls.29,30 However, the reasons for the difference in detection rates between men and women are unknown.28
In this study, two-fifths (40.1%) of the rotavirus gastroenteritis cases within the diarrhea group occurred in babies younger than one year old (Figure 2). This younger age distribution contrasts with the older age distribution of children with rotavirus gastroenteritis observed in more developed countries.31,32
 |
Figure 2 Distribution of rotavirus positivity and negativity rates by age. The distribution of rotavirus positivity and negativity numbers by age. The age group with the highest number of patients applying to the hospital with suspicion of rotavirus and rotavirus positivity was determined as the zero age group. There was a decrease in the positivity rate as age increased. The positivity rate in children in the zero age group is 40.1%, while it is 27.6% in the one age group and 11.0% in the two age group. |
Although rotavirus infection can occur at any age, symptomatic infections are mostly seen in children under 2 years of age.33 In the current study, 1041 (78.6%) of the 1320 rotavirus positivity cases were detected in children aged 0–2 years (p<0.001) (Table 1). In studies, the rate of cases in the first 2 years of age varies between 54.9% and 72%.34,35 This may be due in part to the fact that in underdeveloped environments, the peak of rotavirus diarrhea early in life may be due to early exposure to contaminated sources, undetectable antibodies in early infancy, and overcrowding.36 Additionally, almost all children have at least one rotavirus infection by the age of 3.37
Rotavirus shows a distinct seasonality and is known as “winter diarrhea” because it is only winter seasonal in the Americas. However, at the most recent study on the global seasonality of rotavirus infections, ıt was concluded that in temperate regions globally, rotavirus is more common in the cooler months, but seasonal peaks of infections can vary widely and occur from autumn to spring.38 In the current study, rotavirus was detected throughout the year (Figure 3). Nguyenet al39 in a study conducted in Vietnam, they reported that rotavirus infection occurred throughout the year, consistent with our study. In a systematic review on rotavirus in Africa, it was reported that rotavirus was detected year-round in almost every country and generally exhibited significant peaks during the dry months. It has been stated that peaks are more common in dry periods than in rainy periods, but this is not valid for every country.40 For example, In a study compared hospital admissions for rotavirus in three Australian cities with climate factors and found that higher temperature and humidity in the previous week were associated with a decrease in rotavirus admissions.41 In a study has shown that the one-year periodic mode for rotavirus data correlates in reverse phase with meteorological data recorded from November 2007 to December 2009 in Kolkata, India. In other words, it was reported in the study that as temperature, humidity and precipitation data values decrease, rotavirus infections increase and vice versa.42
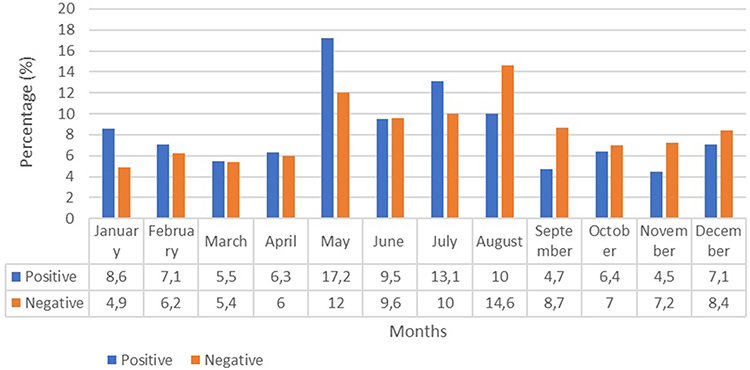 |
Figure 3 Monthly distribution of rotavirus antigen positivity and negativity rates. The Monthly distribution of rotavirus antigen positivity and negativity rates. Diarrhea due to rotavirus has been seen throughout the year. The monthly rotavirus antigen positivity rate in patients admitted to the hospital due to acute gastroenteritis reached its peak at 17.2% in May; In the one-year period, the rates were higher in July (n=173, 13.1%), August (n=132, 10.0%) and January (n=114, 8.6%); It was observed that it was more rare in November (n=60, 4.5%), September (n=62, 4.7%) and March (n=72, 5.5%). |
In our study, hospital admission due to acute gastroenteritis was most common in summer (n=1962) and spring (n=1436), and rotavirus antigen positivity was most common in summer (32.6%) and spring (29.0%)(Table 1). As for the month, the infection peaked in May (17.2%) and was followed by July (13.1%), August (10.0%) and January (8.6%). Infection was observed as month, at least in November (4.5%), followed by September (4.7%) (Figure 3), and as a season, at least in autumn (15.6%) (Table 1). In a study conducted in Saudi Arabia between 2004 and 2005, it was reported that rotavirus peaked ın the cooler months such as November and December and the lowest infection rates were observed in June,43 while another study conducted in Bahrain reported that rotavirus gastroenteritis peaked in April between 2006 and 2007.44 Konca et al45 partly consistent with our study, reported that the highest number of hospital admissions due to acute gastroenteritis was observed in the autumn or spring months, and the most frequent rotavirus antigen positivity was observed in the autumn and spring months. They detected the least number of cases in the summer season. In the tropics, low- and middle-income countries may have an alternative environmental situation (eg water) that may contribute to the temperature-related incidence of rotavirus infection. Seasonal indirect spread of rotavirus in temperate regions can be explained by large seasonal changes.8,46
It is possible to be protected from rotavirus infections with vaccination. Studies conducted abroad have reported that there is a significant decrease in both hospital admissions and hospitalizations after vaccination.47–49According to the data obtained from the Global Burden of Disease Study, rotavirus vaccine was reported to be effective and it was stated that the vaccine prevented approximately 28000 deaths in 2016 and that it would have been possible to save approximately 83200 more children if everyone had been reached that year.1
To date, 33 African countries have included rotavirus vaccines in their national vaccination programmes, but many of the countries with the highest rotavirus death rates, such as the Central African Republic, Chad, Democratic Republic of Congo, Nigeria and Somalia, have not yet introduced.50 Changes in the seasonality of rotavirus disease after rotavirus vaccines are made widely available will allow testing of various hypotheses proposed for the seasonal cycle of rotavirus disease, especially in countries with year-round disease and high rates of seasonal disease. Moreover, to accurately evaluate the effectiveness of the vaccine, a world-wide In many places, the seasonal nature of rotavirus disease should be taken into account.51 It is necessary to conduct continuous surveillance studies throughout the year to capture the seasons when rotavirus is most common. Determining the seasonal epidemiology of infections may be useful in ensuring that vaccination campaigns are carried out in seasons when relevant viral infections are most common.52
Limitation of Study
The limitations of this study are that the hospital where the data was obtained was a tertiary health care facility, so the profile of the cases going to primary or secondary health centers was not determined. Therefore, the findings of this study reflect only a limited population and a specific health institution and do not fully represent the causes of diarrhea across the country. Data on bacterial and other viral etiologies of pediatric diarrhea were not available in this study. Such data would have been useful to monitor trends in the diarrheal burden attributable to these agents following rotavirus vaccine implementation in Somalia.
Conclusion
In our study, it was found that the frequency of rotavirus gastroenteritis increased under the age of two and in the summer months. The data we present here highlight the high burden of rotavirus in Africa. Continuing rotavirus surveillance in the region will be important to provide countries with up-to-date data to guide policy-making processes for new vaccine administration and to monitor disease trends after vaccine implementation. Additionally, this surveillance platform can be used to evaluate vaccine effectiveness through specific studies. Although rotavirus vaccination was universally recommended by the World Health Organization (WHO) in 2009, it has not yet been made part of the national vaccination program in Somalia. This suggests that rotavirus continues to spread among Somali children and cause hospitalizations. Our data suggest that the inclusion of rotavirus vaccine in the national vaccination programme is an urgent public health priority, especially because of the prevalence of infection in children aged 0–2 years. Therefore, a national rotavirus vaccination programme needs to be implemented in Somalia and urgent measures need to be taken to control the infection.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Funding
There was no funding for this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Troeger C, Khalil IA, Rao PC, et al. Rotavirus vaccination and the global burden of rotavirus diarrhea among children younger than 5 years. JAMA Pediatr. 2018;172(10):958–965. doi:10.1001/jamapediatrics.2018.1960
2. Parashar UD, Hummelman EG, Bresee JS, Miller MA, Glass RI. Global illness and deaths caused by rotavirus disease in children. Emerg Infect Dis. 2003;9(5):565–572. doi:10.3201/eid0905.020562
3. Shakya P, Adhikari BNAS, Pandey P, Maheshwari A. Rotavirus infection in neonates and young infants. Newborn. 2022. doi:10.5005/jp-journals-11002-0014
4. WHO: Epidemiological Bulletin Somalia. 2013. Accessed from: https://www.emro.who.int/images/stories/somalia/documents/Epidemiological_Bulletin_Somalia_Wk_52_eDEWSCSR.pdf.Accessed.
5. Junaid SA, Umeh C, Olabode AO, Banda JM. Incidence of rotavirus infection in children with gastroenteritis attending Jos university teaching hospital, Nigeria. Virol j. 2011;8(1):1–8. doi:10.1186/1743-422X-8-233
6. Nakagomi T, Nakagomi O, Takahashi Y, Enoki M, Suzuki T, Kilgore P. Incidence, and burden of rotavirus gastroenteritis in Japan as estimated from a prospective sentinel hospital study. J Infect Dis. 2005;192(Suppl 1):106–110. doi:10.1086/431503
7. Cunliffe NA, Ngwira BM, Dove W, et al. Epidemiology of rotavirus infections in children in Blantyre, Malawi, 1997–2007. J Infect Dis. 2010;202(S1):168–174. doi:10.1086/653577
8. Levy K, Hubbard AE, Eisenberg JN. Seasonality of rotavirus disease in the tropics: a systematic review and meta-analysis. Int J Epidemiol. 2009;38(6):1487–1496. doi:10.1093/ije/dyn260
9. Mwenda JM, Ntoto KM, Abebe A. Burden and epidemiology of rotavirus diarrhea in selected African countries: preliminary results from the African Rotavirus Surveillance Network. J Infect Dis. 2010;202(S1):5–11. doi:10.1086/653557
10. UNICEF. Water, sanitation and hygiene in Somalia. 2020. Accessed from: https://www.unicef.org/somalia/water-sanitation-and-hygiene.
11. Lestari FB, Vongpunsawad S, Wanlapakorn N, Poovorawan Y. Rotavirus infection in children in Southeast Asia 2008–2018: disease burden, genotype distribution, seasonality, and vaccination. J Biomed Sci. 2020;27(1):66. doi:10.1186/s12929-020-00649-8
12. Troeger C, Blacker BF, Khalil IA, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: a systematic analysis for the global burden of disease study 2016. Lancet Infect Dis. 2018;8(11):1211–1228. doi:10.1016/S1473-3099(18)30362-1
13. Magalhães G Félix, Nogueira P Afonso, Grava A Fagundes, Penati M, Silva L Hildebrando and Orlandi P Puccinelli. (2007). Rotavirus and adenovirus in Rondônia. Mem. Inst. Oswaldo Cruz, 102(5), 555–557. doi:10.1590/S0074-02762007005000067
14. Gargano LM, Tate JE, Parashar UD, Omer SB, Cookson ST. Comparison of impact and cost-effectiveness of rotavirus supplementary and routine immunization in a complex humanitarian emergency, Somali case study. ConflHealth. 2015;9:1–10. doi:10.1186/s13031-015-0032-y
15. Kotloff KL, Nataro JP, Blackwelder WC, et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): a prospective, case-control study. Lancet. 2013;382(9888):209–222. doi:10.1016/S0140-6736(13)60844-2
16. Four more African countries commit to rotavirus and pneumococcal vaccines. Accessed from: https://www.defeatdd.org/blog/four-more-african-countries-commit-rotavirus-and-pneumococcal-vaccines.
17. Tanaka G, Faruque AS, Luby SP, Malek MA, Glass RI, Parashar UD. Deaths from rotavirus disease in Bangladeshi children: estimates from hospital-based surveillance. Pediatr Infect Dis J. 2007;26(11):1014–1018. doi:10.1097/INF.0b013e318125721c
18. Sarker MHR, Das SK, Ahmed S, et al. Changing characteristics of rotavirus diarrhea in children younger than five years in urban Bangladesh. PLoS One. 2014;9(8):e105978. doi:10.1371/journal.pone.0105978
19. Osman MM, Adan FN, Akyol T, Sümbül HE. Prevalence of rotavirus, adenovirus, and hepatitis a virus in a tertiary care hospital in Somalia. J Mol Virol Immunol. 2023;4(4):153–160. doi:10.46683/jmvi.2023.82
20. Global Rotavirus Information and Surveillance Bulletin Reporting Period: January through December 2008 Volume 1: December 2009. Available from: https://www3.paho.org/hq/dmdocuments/2010/Bulletin_Rota_Dec_09.pdf.
21. Centers for Disease Control and Prevention. Rotavirus surveillance--worldwide, 2001–2008. MMWR Morb Mortal Wkly Rep. 2008;57(46):1255–1257.
22. Vizzi E, Pineros O, Gonzalez GG, Zambrano JL, Ludert JE, Liprandi F. Genotyping of human rotaviruses circulating among children with diarrhea in Valencia, Venezuela. J Med Virol. 2011;83(12):2225–2232. doi:10.1002/jmv.22211
23. John BM, Devgan A, Mitra B. Prevalence of rotavirus infection in children below two years presenting with diarrhea. Med j Armed Forces India. 2014;70(2):116–119. doi:10.1016/j.mjafi.2014.02.008
24. Chakravarti A, Chauhan MS, Sharma A, Verma V. Distribution of human rotavirus G and P genotypes in a hospital setting from Northern India. Southeast Asian J Trop Med Public Health. 2010;41(5):1145–1152. PMID: 21073035.
25. Fischer TK, Rungoe C, Jensen CS, et al. The burden of rotavirus disease in Denmark 2009-2010. Pediatr Infect Dis J. 2011;30(7):e126–129. doi:10.1097/INF.0b013e3182145277
26. Paul SK, Hossain MA, Mahmud MC, et al. Instability of human rotavirus G genotypes circulating in a rural area of Bangladesh. Mymensingh Med J. 2011;20(1):1–8. PMID: 21240155.
27. Aminu M, Esona MD, Geyer A, Steele AD. Epidemiology of rotavirus and astrovirus infections in children in northwestern Nigeria. Ann Afr Med. 2008;7(4):168–174. doi:10.4103/1596-3519.55658
28. Ojobor CD, Olovo CV, Onah LO, Ike AC. Prevalence and associated factors to rotavirus infection in children less than 5 years in Enugu State, Nigeria. Virus Dis. 2020;31(3):316–322. doi:10.1007/s13337-020-00614-x
29. Ndze NV, Akum AE, Kamga GH, et al. Epidemiology of rotavirus diarrhea in children under 5 years in Northern Cameroon. Pan Afr Med J. 2012;11:73. PMCID: PMC3361211.
30. Tagbo BN, Chukwubuike C, Mwenda JM, et al. Molecular characterization of rotavirus strains circulating in Enugu Nigeria: 2011 to 2016. World J Vaccin. 2019;2019(9):22–36. doi:10.4236/wjv.2019.91002
31. Bresee J, Glass RI, Ivanoff B, Gentsch J. Current status and future priorities for rotavirus vaccine development, evaluation and implementation in developing countries. Vaccine. 1999;17(18):2207–2222. doi:10.1016/s0264-410x(98)00376-4
32. Bresee JS, Hummelman E, Nelson EAS, Glass RI. Rotavirus in Asia: the value of surveillance for informing decisions about the introduction of new vaccines. J Infect Dis. 2005;192(Suppl 1):1–5. doi:10.1086/431515
33. Ramsay M, Brown D. Epidemiology of group A rotaviruses. In: Gray J, Desselberger U, editors. Rotaviruses: Methods and Protocols. Totowa, NJ: Humana Press Inc; 2000:217–236.
34. Akıncı N, Ercan TE, Yalman N, Eren A, Severge B, Ercan G. Akut Gastroenteritli Çocuklarda Adenovirüsve Rotavirüs[Adenovirus and rotavirus in children with acute gastroenteritis]. Pediatr Inf. 2007;1(3):98–101. Turkish.
35. Carneiro NB, Diniz-Santos DR, Fagundes SQ, et al. Clinical and epidemiological aspects of children hospitalized with severe rotavirus-associated gastroenteritis in Salvador, BA, Brazil. Brazilian J Infect Dis. 2005;9(6):525–528. doi:10.1590/s1413-86702005000600013
36. Tagbo BN, Mwenda JM, Armah G, et al. Epidemiology of rotavirus diarrhea among children younger than 5 years in Enugu, SouthEast, Nigeria. J Pediatr Infect Dis. 2014;33(1):19–22. doi:10.1097/INF.0000000000000047
37. Parashar UD, Gibson CJ, Bresee JS, et al. Rotavirus and severe childhood diarrhea. Emerg Infect Dis. 2006;12(2):304–306. doi:10.3201/eid1202.050006
38. Cook SM, Glass RI, LeBaron CW, Ho MS. Global seasonality of rotavirus infections. Bull World Health Organ. 1990;68(2):171–177. PMCID: PMC2393128.
39. Nguyen TV, Le Van P, Le Huy C, Weintraub A. Diarrhea caused by rotavirus in children less than 5 years of age in Hanoi, Vietnam. J Clin Microbiol. 2004;42(12):5745–5750. doi:10.1128/JCM.42.12.5745-5750.2004
40. Cunliffe NA, Kilgore PE, Bresee JS, et al. Epidemiology of rotavirus diarrhoea in Africa: a review to assess the need for rotavirus immunization. Bull World Health Organ. 1998;76(5):525–537.
41. D’Souza RM, Halll G, Becker NG. Climatic factors associated with hospitalizations for rotavirus diarrhoea in children under 5 years of age. Epidemiol Infect. 2008;136(1):56–64. doi:10.1017/S0950268807008229
42. Sumi A, Rajendran K, Ramamurthy T, Krishnan T, Nair GB, Harigane K, Kobayash N. Effect of temperature, relative humidity and rainfall on rotavirus infections in Kolkata. India Epidemiol Infect. 2013;141(8):1652–1661. doi:10.1017/S0950268812002208
43. Kheyami AM, Nakagomi T, Nakagomi O, Dove W, Hart CA, Cunliffe NA. Molecular epidemiology of rotavirus diarrhea among children in Saudi Arabia: first detection of G9 and G12 strains. J Clin Microbiol. 2008;46(4):1185–1191. doi:10.1128/JCM.02244-07
44. Musawi MA, Zainaldeen H, Shafi F, Anis S, Deantonio R. Rotavirus gastroenteritis in children under 5 years in the Kingdom of Bahrain: hospital-based surveillance. Clin Epidemiol. 2013;5:269–275. doi:10.2147/CLEP.S46822
45. Konca Ç, Tekin M, Akgün S, et al. Prevalence of Rotavirus in Children with Acute Gastroenteritis, Seasonal Distribution, and Laboratory Findings in the Southeast of Turkey/Güneydogu Anadolu BölgesindekiAkutGastroenteritliÇocuklarda Rotavirus Görülmesikligi, MevsimselDagilimiveLaboratuvarBulgulari. J Pediatr Inf. 2014;8(1):7–11.
46. Kraay ANM, Brouwer AF, Lin N, Collender PA, Remais JV, Eisenberg JNS. Modeling environmentally mediated rotavirus transmission: the role of temperature and hydrologic factors. Proc Natl Acad Sci. 2018;115(12):E2782–90. doi:10.1073/pnas.1719579115
47. De Oliveira LH, Giglio N, Ciapponi A, et al. Temporal trends in diarrhea-related hospitalizations and deaths in children under age 5 before and after the introduction of the rotavirus vaccine in four Latin American countries. Vaccine. 2013;31(3):99–108. doi:10.1016/j.vaccine.2013.05.065
48. Quintanar-Solares M, Yen C, Richardson V, Esparza-Aguilar M, Parashar UD, Patel MM. Impact of rotavirus vaccination on diarrhea-related hospitalizations among children < 5 years of age in Mexico. Pediatr Infect Dis J. 2011;30(1Suppl):11–15. doi:10.1097/INF.0b013e3181fefb32
49. Fernandes EG, Sato HK, Leshem E, et al. Impact of rotavirus vaccination on diarrhea-related hospitalizations in Sao Paulo State, Brazil. Vaccine. 2014;32(27):3402–3408. doi:10.1016/j.vaccine.2014.04.015
50. Rotavirus in Africa. 2016. Available from: https://preventrotavirus.org/wp-content/uploads/2016/10/Rotavirus-Vaccine-Africa-Factsheet-Oct-2016.pdf.
51. Patel MM, Pitzer VE, Alonso WJ, et al. Global seasonality of rotavirus disease. Pediatr Infect Dis J. 2013;32(4):e134–e147. doi:10.1097/INF.0b013e31827d3b68
52. Zaraket R, Salami A, Bahmad M, et al. Prevalence, risk factors, and clinical characteristics of rotavirus and adenovirus among Lebanese hospitalized children with acute gastroenteritis. Heliyon. 2020;6(6):e04248. doi:10.1016/j.heliyon.2020.e04248
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Risk Factors of Childhood Asthma in Jazan Region, Saudi Arabia
Gohal G, Yassin A, Darraj H, Darraj A, Maghrabi R, Abutalib YB, Talebi S, Mutaen AA, Hamdi S
Journal of Asthma and Allergy 2024, 17:33-43
Published Date: 20 January 2024
Urolithiasis Burden in Somalia: Associated Factors and Regional Distribution Among Patients Undergoing CT Scan in Selected Centers in Mogadishu
Dirie NI, Ahmed MM, Olad OM, Shire IH, Mohamud AK, Garba B, Mohamoud JH, Asowe HA, Orey FAH, Hassan J, Adam MH
Research and Reports in Urology 2025, 17:105-118
Published Date: 3 April 2025
Prevalence and Risk Factors of Positional Obstructive Sleep Apnea in Chinese Children: A Retrospective Study
Tang A, Dai S, Au CT, Yu MWL, Li AM, Chan KCC
Nature and Science of Sleep 2025, 17:2933-2946
Published Date: 11 November 2025
Spatial Distribution and Determinants of Inadequate Vitamin A–Rich Food Consumption Among Children Aged 6–23 Months in Somalia: Evidence from the 2020 Somalia Demographic and Health Survey
Osman OM, Abdi HA, Abdilleh MM, Muse AH, Osman AM, Muse YH
Pediatric Health, Medicine and Therapeutics 2026, 17:587150
Published Date: 14 May 2026