Back to Journals » Advances in Medical Education and Practice » Volume 12
Roses and Balances: A Paradigm for Constructive Ethical Review of Health Professions Education Research
Authors Schutte T, Scheele F ![]() , van Luijk S
, van Luijk S
Received 3 February 2021
Accepted for publication 30 April 2021
Published 25 May 2021 Volume 2021:12 Pages 529—535
DOI https://doi.org/10.2147/AMEP.S305094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Tim Schutte,1,2 Fedde Scheele,3,4 Scheltus van Luijk5
1Department of Internal Medicine, Amsterdam UMC, Amsterdam, The Netherlands; 2Department of Internal Medicine, Zaans Medisch Centrum, Zaandam, The Netherlands; 3Athena Institute for Transdisciplinary Research, VU University, Amsterdam, The Netherlands; 4Department of Healthcare Education, OLVG Hospital, Amsterdam, The Netherlands; 5Institute for Post Graduate Education MUMC+, Medical University Hospital, Maastricht, The Netherlands
Correspondence: Tim Schutte Email [email protected]
Abstract: Recently, the balance between value and necessity of ethical review of health professions education research has been debated. At present, there are large differences in how ethical review of research proposals for health professions education is organized. We present a framework that describes the organization of ethical review in health professions education research, based on the interpersonal circumplex model, also known as Leary’s Rose. The framework is based on the two main balances in ethical review of health professions education research, being the protectiveness for the subjects and how ethical review is organized and responsibilities are shared. The axis/balance of protectiveness ranges between the extremes “paternalistic protective” to “liberal permissive”. The axis/balance of organization and responsibility ranges between the extremes of “centralized” to “local/decentralized”. This model offers insight in the position of an ethical review board and shows the dynamics of the decisions for ethical approval and the consequences of the different approaches to the organization of ethical review of health professions education research.
Keywords: ethical review, health professions education research, ethical approval of health professions education research
Background
Recently, the balance between value and necessity of ethical review of health professions education research (HPE-R) has been debated.1,2 Schuwirth and Durning started a discussion by implying that the benefits of ethical reviewing are minimal compared to the effort.1 Although everyone would agree that (ethical) reviewing takes time, the benefits should not be underestimated. A recent reaction underlined the value of ethical reviewing and described how an ethical review board could mitigate harm and improve research proposals.2 Still, the balance between effort and benefits depends on the organization and process of a review board.
There are large differences in how ethical review of research proposals for health professions education is organized. For instance, in the Netherlands, a dedicated national committee, as part of the national association for medical education assesses a great deal of HPE-R proposals.3,4 In the United States of America and the United Kingdom HPE-R is organized locally in universities and in more general ethical review boards (Institutional Review Boards (IRBs)).1,5 Other HPE-R proposals are not externally reviewed or assessed by local (senior) colleagues.6 All systems have benefits and disadvantages.
A (more) centralized and dedicated organized review board has the benefits of experienced and focused expertise in education research.3,7 Disadvantages of such a centralized system include the decoupling and externalization of responsibility for all ethical issues from the local researchers to the ethical board. For decentralized organized review, benefits include approachability and proximity. Disadvantages of a decentralized system include difficulties in approval for multicenter studies and limited expertise on ethical issues concerning educational research in local IRBs.
Internationally, ethical review for HPE-R has the challenges to prevent an unnecessarily onerous and lengthy review process and search for a procedure to facilitate efficient and reasonable review of HPE-R.1
Altogether, the international differences and challenges in the organization of ethical review practice made us question how ethical reviewing for HPE-R can be organized.
Therefore, this article aims to present a framework that describes the challenges of the organization of ethical review in health professions education research, inspired by the interpersonal circumplex model (Leary’s Rose).
A Paradigm for Constructive Ethical Review of Health Professions Education Research
We were inspired by the interpersonal circumplex model, also known as Leary’s Rose, as a theoretical framework8–10 (see Figure 1). This model has been validated scientifically and has paradigm status.8,11,12 Originally, this model describes interpersonal interaction and is used in medical communication and psychology. The basis of the interpersonal circumplex model consists of two (and later more) orthogonal axes and concentric circles indicating the level of intensity. The two original main axes are power and love. The opposing sides for the love-axis were love and hate; and of the power-axis dominance and submission.8,9 A position (on one of the axes) in the center of the rose is considered moderate, and the more off-center one is positioned, the extremer the position is.
 |
Figure 1 A sketch of the interpersonal circumplex model, also known as Leary’s Rose, with the two original main axes; “power” and “love”. |
We choose this model as a framework as our present model is based on both the concept of the interpersonal circumplex model (two dimensions and concentric circles of strength) and the analogy with the original axis’ themes, which are discussed in the following sections.
The individual concepts within our framework (see Figure 2) are inspired by previous publications on the design, organization and evaluation of ethical reviewing.1–4,7,13–19 The framework describes the dimensions that relate to the two main balances in ethical review of HPE-R, being the protectiveness for the subjects and the organization with its corresponding responsibility (see Figure 2).
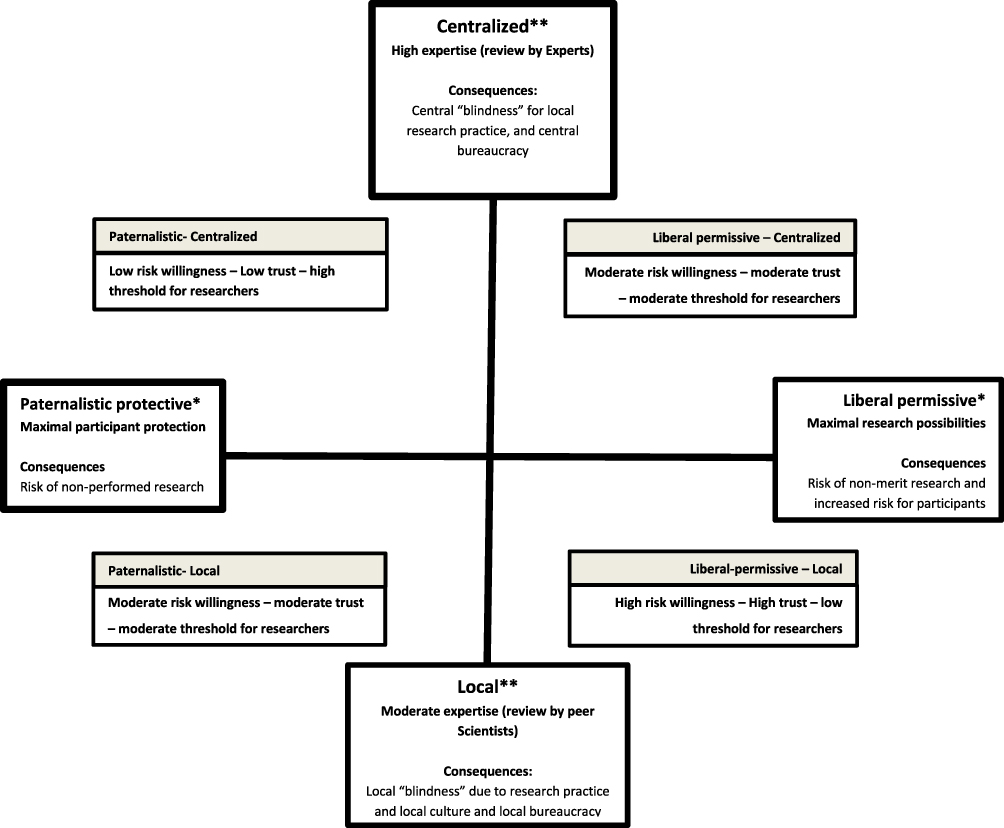 |
Figure 2 The framework of organization of ethical review in health professions education research. The two axis with its extremes being, paternalistic protective versus liberal permissive on the protectiveness axis (*), and central versus local/decentralized on the organization and responsibility axis (**). A position high on this organization and responsibility axis encompasses centralized high expertise and review by experts. This is as opposed to low on this organizational responsibility axis, encompassing review by local peer scientists with associated moderate expertise. On the protectiveness axis, a position left on this axis encompasses an attitude of maximal participant protection (at all costs) as opposed to a position on the right of this axis which encompasses a liberal and permissive viewpoint, with maximal research possibilities. Consequences include central “blindness” for research practice and a central bureaucracy for a position high on the organization and responsibility axis. As opposed to a consequential local blindness and local bureaucracy for a position low on the organization and responsibility axis. In the quadrants the core characteristics (the levels of risk willingness, trust and the threshold for researchers) and consequences (per axis) are depicted. |
Organization and responsibility
Organization and responsibility encompass how ethical review is organized and how the responsibilities of reviewing and ethical considerations are shared. A position high on this organization and responsibility axis (thus a more centralized focus of organization and responsibilities) encompasses a structured and equivalent review of research proposals in (more) centralized boards by experts. Specific standards and predefined processes with standardized documents and specific requirements regarding committee members competencies are examples of characteristics of highly organized approaches, thus high on the organization and responsibility axis. Subsequently, a position low(er) on this organizational responsibility axis (thus a more local organization and responsibility) encompasses review by local peer scientists with associated moderate expertise, less structure and more diverse assessments, all due to limited exposure to reviewing HPE-R proposals.
From a strategic/regulatory perspective, a centralized organization and responsibility structure (high on the organization and responsibility axis) with a central “power” to reject, require adjustments or approve submitted proposals, can be seen as a dominant approach (and thus towards dominance on the power axis in the original interpersonal circumplex model). This is as opposed to a local approach, where “power” is delegated and responsibilities are shared by local researchers. The latter can be interpreted as a more submissive approach from a strategic/regulatory perspective (towards submission on the interpersonal circumplex power-axis).
As mentioned before, all systems have benefits and disadvantages. When the organizational responsibility is more centralized, possible consequences are a (central) ‘blindness’ for research practice and a (central) “bureaucracy”. This is as opposed to a consequential local “blindness” and local “bureaucracy” for locally organized review. These terms are explained hereafter.
Central “blindness” can be described as the inability of a central organization (eg the ethical committee) to appreciate the daily practice (of researchers) and the consequences of their demands and procedures for local researchers. This can include demanding further specific information about research proposals that is judged by local researchers as redundant and abundant. This central committee’s practice can be perceived as “arrogance”. Good communication and explanation about the reasons to ask for such information from the central organization is essential to prevent resistance.
Local blindness can be described as the inability of local researchers to see the big picture from a certain distance and therefore the consequences of their research on the population/society. This includes the consequence of allowing certain (non-merit or even harmful) research to take place, which can create a precedent for future research.
By central bureaucracy, we mean ethical reviewing from an ivory tower, making rigid decisions based on strict rules and regulations and no or limited possibilities for tailored decisions. Thereby, the procedure is not content-specific and equal for all applicants and applications. This organization can be perceived as undue for specific proposals and can provoke resistance against a central organization.
By local bureaucracy we mean ethical reviewing from a practice perspective. Decisions are based on common (used) methods, making ad-hoc decisions. Local culture can induce a specific attitude with selective attention or a lack of attention regarding other aspects. Thereby the procedure or even decision of a researcher not to pursue ethical approval, depends on the researcher. In case of external review by a known fellow researcher, this creates the risk of favoritism. Moreover, this organization can be perceived as incomplete. Furthermore, a lack of standardization could lead to large differences in lead time; a similar protocol could take only days in one setting yet take weeks or even months in another institution or with another colleague.18
Protectiveness
The second dimension and axis in the framework is the protectiveness for the subjects. This encompasses the ability or intention to protect potential vulnerable future research participants. On the protectiveness axis, a position left on this axis (thus paternalistic protective) encompasses an attitude of maximal participant protection (at all costs) with a possible consequence of the risk of non-performed research. This is as opposed to a position on the right of this axis (thus liberal permissive) that encompasses a liberal and permissive viewpoint, with maximal research possibilities. Consequences of the latter encompass the risk of non-merit research and increased risk for participants.
From a researcher perspective, an ethical review committee with a paternalistic protective approach regarding the protectiveness of the subjects can be seen as reluctant and hostile (towards “hate” on the interpersonal circumplex love-axis). This is as opposed to a committee with a liberal permissive approach regarding the protectiveness of the subjects which can be seen as supportive and allowing (towards love on the interpersonal circumplex love-axis).
Altogether, the two axis create four quadrants. In these quadrants, the core characteristics and consequences (per axis) are depicted. The consequences of each position in the rose are foreseeable and directly linked with the core characteristics of each quadrant. These core characteristics are the levels of risk willingness, trust and the threshold for researchers. The risk willingness is a concept that describes the risk one is willing to take from a strategic/regulatory perspective. When you do not want any risks (eg for participants) the risk willingness is zero. When one accepts some or more than some risk, the risk willingness is moderate or high. The “trust” refers to the trust in the researchers’ self-assessment of expertise and decisions on the ethical aspects for the intended research. The “threshold for researchers” reflects the estimated effort for a researcher to pass the ethical review process. This effort has been described as a major disadvantage of intensive ethical review described by Schuwirth and Durning (risk of non-performed research).1 The consequences of the core characteristics are also aligned and graded, with the lowest risk willingness and trust (and highest threshold for researchers) in the left upper quadrant and the highest risk willingness and trust (and lowest threshold for researchers) in the right lower quadrant.
As with the original rose, a position in the center of the rose is considered moderate (on this axis), and the more off-center one is positioned, the extremer the position is. Using this model, one can see the possible positions for how a review board can operate and the consequences of this position.
Applicability in Large and Small Regions/Countries
Internationally there are large differences in the number of medical schools per region/country and the amount of HPE-R that is initiated and submitted for review. As a consequence, there is no simple international recipe for how to organize ethical reviewing. Nevertheless, the framework seems applicable and scalable to these different conditions. Changing towards a more local system can be accomplished by involving (more) local researchers, by establishing more local ethical review boards or to only review high stakes/high-risk proposals. Changing towards a more central system seems more context specific. In large countries with many medical schools and other HPE institutions, a (more) central approach would not necessarily mean a dedicated national HPE-R board; instead, it could also mean multicenter collaboration or a shared dedicated committee for multiple institutions. As an example, the dedicated national committee for HPE-R in the Netherlands is in fact a multicenter collaboration of the eight medical schools and other HPE institutions, as part of the Netherlands association for medical education (NVMO).3,4 For smaller countries or countries with low numbers of initiated HPE-R international collaboration could be sought to secure higher levels of experience with ethical considerations in HPE-R when aiming for a higher level on the organization and responsibility axis. A challenge in such a situation would be that the international collaborators could be unfamiliar with the local laws and regulations.
Discussion
This model helps to understand the organization and process of a review board, describes core characteristics of approaches to the organization of ethical reviewing practice and shows blind-spots, risks and consequences. In each situation/context, a different balance would be best suitable for optimal organization of ethical review in HPE-R. The risks and consequences of each position in the rose are foreseeable and directly linked with its core characteristics regarding risk willingness, trust and the threshold for researchers.
Recently, Schuwirth and Durning advocated for a limited and liberal approach for ethical review of HPE-R based on a utilitarian view of ethical reviewing.1 Based on our model, the core characteristics of their approach are high-risk willingness, high trust and low threshold for researchers. It would make performing research easy, trusting the researchers to “do good”; however, it does have some possible risks for participants and therefore tolerates this risk (high-risk willingness). Based on the model, the consequence/risks would be local “blindness” due to research practice and local culture, with higher risks for participants. Recognizing the core characteristics and mitigating these risks and consequences could help in implementing such an approach, or lead to a new or different balance, following the discussion in literature.
As a second example of the application of the framework, one can use it to review the position of ethical review committee(s) for HPE. A central committee used to have a more paternalistic and protective conception, with a position in the left upper quadrant of the model. Using the presented model can offer insight to aim for a more intermediate level of protectiveness and shared level of centralization. This would strengthen the engagement and involvement of the local research teams and reduce the risk of non-performed or non-assessed and still performed research outside the purview of the ethical review board.
The practice of ethical reviewing of HPE-R is contextual; however, the underlying principles seem to be overarching concepts. Above all, there is no right or wrong in this model; each decision and position has beneficial and adverse consequences. Finding a (right) balance is essential. Moreover, one has to realize the position in this framework is multidimensional and dynamic in time and influenced from internal and external factors. On the macro-level, an ethical review board can determine and adjust its general position, influenced by changes in rules, laws and customs, discussions in literature and society, previous incidents, the composition of the committee and previous decisions on other submissions. On a micro-level, a board could adjusts its position for each proposal. Perceived risk in a proposal would shift a committee’s position towards a central and paternalistic protective position; supposed benefit would shift the attitude towards permissive. A conceptual description of the balancing of an ethical review board on this micro level is described in Eikelboom’s framework of the ethical review process in medical education research.4 Future research is needed to validate and support the present model and could include measuring perceived value and placement of ethical reviewing practice in a specific context/by a specific board. Such research could eventually modify the model to include additional dimensions, as with the original circumplex model.
The value of this model is to visualize the balances in ethical reviewing for HPE-R and the consequences of a chosen approach and offers perspectives for future practice and research. This model can also help to structure in a discussion on the future of ethical reviewing for HPE-R. Being aware of the current position of an ethical review board is essential to secure sufficient support to foster, continue and improve HPE-R ethical reviewing.
Conclusion
We present a framework that describes the organization of ethical review in health professions education research, based on the interpersonal circumplex model, also known as Leary’s Rose. The framework is based on the two main balances in ethical review of HPE-R, being the protectiveness for the subjects and how ethical review is organized and responsibilities are shared. The axis/balance of protectiveness ranges between the extremes “paternalistic protective” to “liberal permissive”. The axis/balance of organization and responsibility ranges between the extremes of “centralized” to “local/decentralized”. Using this model offers insight in the position of an ethical review board and shows the dynamics of the decisions for ethical approval and the consequences of the different approaches to the organization of ethical review of HPE-R.
Abbreviations
ERB, ethical review board; HPE, health professions education; HPE-R, health professions education research; IRB, Institutional Review Board.
Data Sharing Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Acknowledgments
We would like to thank the reviewers for their suggestions to improve our manuscript.
Author Contributions
All authors (TS, FS, SvL): made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
No funding was obtained.
Disclosure
T. Schutte is a resident member in the ethical review board of the Netherlands association for medical education (NVMO). F. Scheele is the former chair of Netherlands association for medical education (NVMO) and S.J. van Luijk is the former chair of the ethical review board of the Netherlands association for medical education (NVMO). The authors declare that they have no other competing interests.
References
1. Schuwirth LWT, Durning SJ. Ethics approval for health professions education research: are we going too far down the barrel? Med Educ. 2019;53(10):956–958. doi:10.1111/medu.13942
2. Schutte T, Kaushik K, Postmes L, Bremer A. Ethics approval for health professions education research: necessary and beneficial. Med Edu. 2020;54(7):672. doi:10.1111/medu.14140
3. van den Broek WES, Scheele F, Ten Cate O, van Delden JJM. A health professions education research-specific ethical review board. Acad Med. 2016;91(12):1590–1591. doi:10.1097/ACM.0000000000001430
4. Eikelboom JI, Ten Cate OT, Jaarsma D, Raat JA, Schuwirth L, van Delden JJ. A framework for the ethics review of education research. Med Educ. 2012;46(8):731–733. doi:10.1111/j.1365-2923.2012.04293.x
5. DeMeo S, Heflin MT, Nagler A. In Reply to van den Broek et al. Acad Med. 2016;91(12):1591. doi:10.1097/ACM.0000000000001462
6. Hally E, Walsh K. Research ethics and medical education. Med Teach. 2016;38(1):105–106. doi:10.3109/0142159X.2014.956068
7. van den Broek WE, Wouters RH, van Delden JJ. In response to ‘Medical Education Research: is participation fair?’. Perspect Med Educ. 2015;4(3):158–159. doi:10.1007/s40037-015-0188-6
8. Wiggins JS. An informal history of the interpersonal circumplex tradition. J Pers Assess. 1996;66(2):217–233. doi:10.1207/s15327752jpa6602_2
9. Wiggins JST. When is a Circumplex an “Interpersonal Circumplex”? The Case of Supportive Actions. Plutchik RC, H R, editor. Washington DC, USA: American Psychological Association; 1997.
10. Leary T. Interpersonal Diagnosis of Personality: A Functional Theory and Methodology for Personality Evaluation. New York, USA: Ronald Press Co; 1957.
11. Orford J. The interpersonal circumplex - a theory and method for applied-psychology. Hum Relat. 1994;47(11):1347–1375. doi:10.1177/001872679404701103
12. Moskowitz DS. Cross-situational generality and the interpersonal circumplex. Am Psychol Assoc. 1994;921–33.
13. Walsh K. Medical education research: is participation fair? Perspect Med Educ. 2014;3(5):379–382. doi:10.1007/s40037-014-0120-5
14. Brown C, Spiro J, Quinton S. The role of research ethics committees: friend or foe in educational research? An exploratory study. Brit Educ Res J. 2020;46(4):747–769. doi:10.1002/berj.3654
15. DeMeo SD, Nagler A, Heflin MT. Development of a health professions education research-specific institutional review board template. Acad Med. 2016;91(2):229–232. doi:10.1097/ACM.0000000000000987
16. Ten Cate O. Why the ethics of medical education research differs from that of medical research. Med Educ. 2009;43(7):608–610. doi:10.1111/j.1365-2923.2009.03385.x
17. McAreavey R, Muir J. Research ethics committees: values and power in higher education. Int J Soc Res Method. 2011;14(5):391–405. doi:10.1080/13645579.2011.565635
18. Dyrbye LN, Thomas MR, Mechaber AJ, et al. Medical education research and IRB review: an analysis and comparison of the IRB review process at six institutions. Acad Med. 2007;82(7):654–660. doi:10.1097/ACM.0b013e318065be1e
19. Keune JD, Brunsvold ME, Hohmann E, Korndorffer JR
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.