Back to Journals » Cancer Management and Research » Volume 18

Risk Stratification in Papillary Thyroid Microcarcinoma: Clinical Features Predicting Multifocality, Lymph Node Metastasis, and Recurrence – A Retrospective Cohort Study
Authors Hsu CC ![]() , Tsai CY, Lin LC, Wang SY, Yeh CN, Liou MJ, Chen ST
, Tsai CY, Lin LC, Wang SY, Yeh CN, Liou MJ, Chen ST
Received 7 October 2025
Accepted for publication 23 December 2025
Published 9 January 2026 Volume 2026:18 572526
DOI https://doi.org/10.2147/CMAR.S572526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bilikere Dwarakanath
Chih-Chieh Hsu,1 Chun-Yi Tsai,1 Li-Ching Lin,1 Shang-Yu Wang,1,2 Chun-Nan Yeh,1,2,* Miaw-Jene Liou,3,* Szu-Tah Chen3
1Division of General Surgery, Department of Surgery, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan; 2Chang Gung University, Taoyuan, Taiwan; 3Division of Endocrinology and Metabolism, Department of Internal Medicine, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan
*These authors contributed equally to this work
Correspondence: Chun-Nan Yeh, Chang Gung Memorial Hospital, Linkou Branch, No. 5, Fu-Shing Street, Kweishan District, Taoyuan City, 333, Taiwan, Tel +886 3 3281200 Ext.3219, Fax +886 3 3285818, Email [email protected]; Miaw-Jene Liou, Chang Gung Memorial Hospital, Linkou Branch, No. 5, Fu-Shing Street, Kweishan District, Taoyuan City, 333, Taiwan, Tel +886 3 3281200 Ext.3219, Fax +886 3 3285818, Email [email protected]
Purpose: Papillary thyroid microcarcinoma (PTMC, ≤ 1 cm) has risen sharply in incidence, comprising nearly half of papillary thyroid carcinoma cases. This study assessed clinical features and risk factors for multifocality, nodal metastasis, and recurrence to inform treatment and risk stratification.
Patients and Methods: We retrospectively analyzed 418 patients diagnosed with PTMC at Chang Gung Memorial Hospital between 2005 and 2015. Patients with incomplete data, initial distant metastasis, or lost to follow-up were excluded. Clinical, pathological, and treatment data were reviewed. Risk factors were identified using multivariate logistic regression analysis. Sensitivity analysis was performed on the total thyroidectomy subgroup to address potential selection bias. The study was IRB-approved and informed consent was waived due to its retrospective nature.
Results: Among 418 patients (75 males, 343 females; median age 47 years), the median tumor size was 6.0 mm. Multifocal PTMC occurred in 32.1% of patients and was significantly associated with larger tumor size (p < 0.001) and lymphovascular invasion (p < 0.001). Cervical lymph node metastasis was observed in 11.5% of patients and was linked to male sex (OR: 3.27, p = 0.006), non-incidental findings (OR: 8.38, p < 0.001), multifocality (OR: 3.13, p = 0.047), and lymphovascular invasion (OR: 709.01, p < 0.001). Sixteen patients (3.8%) experienced recurrence, which was significantly associated with prior lymph node metastasis (OR: 6.24, p = 0.011). The overall survival rate was 97.6%.
Conclusion: PTMC is usually indolent, but male gender, non-incidental findings, multifocality, and lymphovascular invasion indicate higher risk. These mainly histopathological factors can guide management and are particularly relevant when evaluating alternatives such as radiofrequency ablation.
Keywords: papillary thyroid microcarcinoma, risk stratification, clinical features, thyroidectomy, lymph node metastasis
Introduction
Papillary thyroid microcarcinoma (PTMC), defined as papillary thyroid carcinoma measuring ≤1 cm in greatest dimension, has experienced a dramatic increase in incidence over the past several decades.1,2 This increase is largely attributed to improved diagnostic imaging capabilities and increased medical surveillance, leading to the detection of previously occult lesions.3,4 PTMC now accounts for approximately 50% of all papillary thyroid carcinoma cases in many developed countries, representing a significant shift in the epidemiological landscape of thyroid cancer.
The clinical significance of PTMC remains a subject of ongoing debate in the endocrine surgery and endocrinology communities. While the majority of PTMC cases demonstrate indolent behavior with excellent long-term outcomes, a subset of patients experience adverse events including multifocal disease, cervical lymph node metastasis, and disease recurrence.5–9 This clinical heterogeneity has prompted extensive research efforts to identify predictive factors that can guide treatment decision-making and risk stratification.
Traditional management of PTMC has centered on surgical intervention, typically involving either lobectomy or total thyroidectomy depending on various clinical and pathological factors. However, the recognition that many PTMC cases may follow a benign course has led to the exploration of alternative management approaches, including active surveillance and minimally invasive treatments such as radiofrequency ablation (RFA). One recent cohort study reported that approximately one-quarter of patients who underwent thyroidectomy experienced postoperative decision regret, primarily due to scar- or psychology-related reductions in thyroid cancer–specific quality of life, whereas regret was rare among patients managed with active surveillance.10 These findings underscore the importance of accurate preoperative risk stratification and comprehensive counseling to identify patients suitable for less aggressive management strategies.
Current clinical guidelines acknowledge the importance of risk stratification in PTMC management but lack consensus on specific criteria for treatment selection. The American Thyroid Association and other professional societies have provided general recommendations, but the optimal approach to risk assessment remains an active area of investigation.7,8 Key clinical features that have been associated with adverse outcomes in various studies include male gender, younger age, multifocal disease, extrathyroidal extension, and lymphovascular invasion, though the relative importance and predictive value of these factors vary across different patient populations.
The objective of this study was to comprehensively evaluate the clinical characteristics of PTMC patients and identify independent risk factors associated with multifocality, cervical lymph node metastasis, and disease recurrence. By analyzing a large single-center cohort with extensive follow-up, we aimed to develop a practical risk stratification framework that could guide clinical decision-making and inform the evaluation of emerging treatment modalities.
Material and Methods
Study Design and Patient Selection
This retrospective cohort study was conducted at Chang Gung Memorial Hospital (CGMH), Linkou Branch, a tertiary referral center in Taiwan. The study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Chang Gung Medical Foundation Institutional Review Board (ref. 202500444B0). The requirement of informed consent was waived due to its retrospective nature with de-identified data and minimal risk to participants. From January 2005 to December 2015, all patients who underwent thyroidectomy and received a pathological diagnosis of papillary thyroid microcarcinoma were identified for potential inclusion. No a priori sample size calculation was performed due to the retrospective nature of the study.
Inclusion criteria comprised: (1) histologically confirmed papillary thyroid carcinoma ≤1 cm in greatest dimension, (2) surgical treatment at our institution, and (3) availability of complete clinicopathological data. Exclusion criteria included: (1) incomplete clinical or pathological data, (2) presence of distant metastasis at initial presentation, (3) previous history of thyroid cancer or radiation exposure, and (4) loss to follow-up within six months of surgery.
Definitions
PTMC was defined according to World Health Organization criteria as papillary thyroid carcinoma ≤1 cm in greatest dimension. Incidental PTMC was defined as microcarcinomas discovered during thyroidectomy performed for benign thyroid conditions without preoperative suspicion of malignancy based on imaging findings or fine-needle aspiration cytology results. Non-incidental PTMC referred to cases where malignancy was suspected preoperatively based on clinical, imaging, or cytological findings.
Multifocal PTMC was defined as the presence of two or more separate tumor foci within the thyroid gland, either unilateral or bilateral, as determined by histopathological examination. Lymphovascular invasion was defined as the presence of tumor cells within lymphatic or vascular spaces confirmed by histopathological examination using standard hematoxylin and eosin staining.
Cervical lymph node metastasis was classified as central neck (level VI) or lateral neck (levels II–V) based on anatomical location and confirmed by histopathological examination. Suspicious cervical lymph nodes on preoperative ultrasound were defined according to established sonographic criteria, including loss of fatty hilum, round shape, microcalcifications, cystic change, hyperechogenicity, or peripheral vascularity.11 Extrathyroidal extension was defined as tumor extension beyond the thyroid capsule into surrounding tissues.
Disease recurrence was defined as the appearance of new thyroid cancer foci detected by imaging studies (ultrasound, computed tomography, or radioiodine scanning) during follow-up, with or without tissue confirmation. Locoregional recurrence included disease in the thyroid bed, residual thyroid tissue, or cervical lymph nodes, while distant recurrence involved metastasis to organs beyond the neck.
Surgical Approach Selection
Surgical approach during the study period was determined based on institutional practice patterns and individual surgeon preferences, which generally favored more extensive resection than current guidelines recommend. Total thyroidectomy was typically performed for bilateral thyroid disease, suspected or confirmed multifocal disease, family history of thyroid cancer, patient preference for definitive treatment, or concurrent benign disease requiring bilateral intervention. Thyroid lobectomy was generally reserved for unifocal disease in patients without high-risk features or concurrent bilateral benign disease.
Central neck dissection was performed at the discretion of the operating surgeon, typically when central lymph node metastasis was suspected based on preoperative imaging or intraoperative findings. Lateral neck dissection was performed when lateral neck lymph node metastasis was confirmed preoperatively or identified intraoperatively.
Data Collection
Clinical data were extracted from electronic medical records and included patient demographics, preoperative imaging findings, laboratory results including thyroid function tests, surgical details, pathological characteristics, postoperative management including radioiodine therapy, and follow-up information. Pathological data included tumor size, histological subtype, presence of multifocal disease, extrathyroidal extension, lymphovascular invasion, and lymph node metastasis status.
Follow-up data were collected through July 2023, with a median follow-up duration of 154 months (range: 6–216 months). Follow-up protocols typically included clinical examination, neck ultrasonography, and thyroglobulin measurement at regular intervals according to institutional guidelines.
Statistical Analysis
Statistical analysis was performed using SPSS software version 20.0 (IBM Corp., Armonk, NY, USA). Given the non-normal distribution of continuous variables, non-parametric statistical methods were employed. Continuous variables were compared using the Mann–Whitney U-test, while categorical variables were analyzed using the Chi-square test or Fisher’s exact test as appropriate.
Missing data were minimal. Patients with missing data, loss to follow-up, or distant metastasis at initial presentation (n = 21) were excluded, leaving 418 patients in the final analysis; therefore, no data imputation was required. Variables with p-values < 0.05 in univariate analysis were entered into multivariate logistic regression models using backward stepwise selection to identify independent predictors of multifocality, lymph node metastasis, and recurrence. Collinearity was managed by evaluating clinically and statistically related variables; when two variables were highly correlated, only the more clinically relevant variable was retained in the multivariate model. Odds ratios (OR) with 95% confidence intervals (CI) were calculated for significant predictors. A p-value < 0.05 was considered statistically significant for all analyses.
To address potential selection bias related to the heterogeneous nature of surgical approaches in our cohort, sensitivity analyses were performed limited to patients who underwent total thyroidectomy. This subgroup analysis aimed to assess the robustness of our findings and minimize potential confounding related to surgical approach selection.
Overall survival defined as the time from surgery to death from any cause or last follow-up. Disease-free survival was defined as the time from surgery to first recurrence or last follow-up without recurrence.
Results
Patient Characteristics
A total of 418 patients met the inclusion criteria and were included in the final analysis (Figure 1). The detailed demographic and clinicopathological characteristics are summarized in Table 1. The cohort comprised 75 males (17.9%) and 343 females (82.1%), with a median age of 47 years (range: 18–82 years). The median tumor size was 6.0 mm (range: 1–10 mm), with 85% of tumors measuring ≤8 mm.
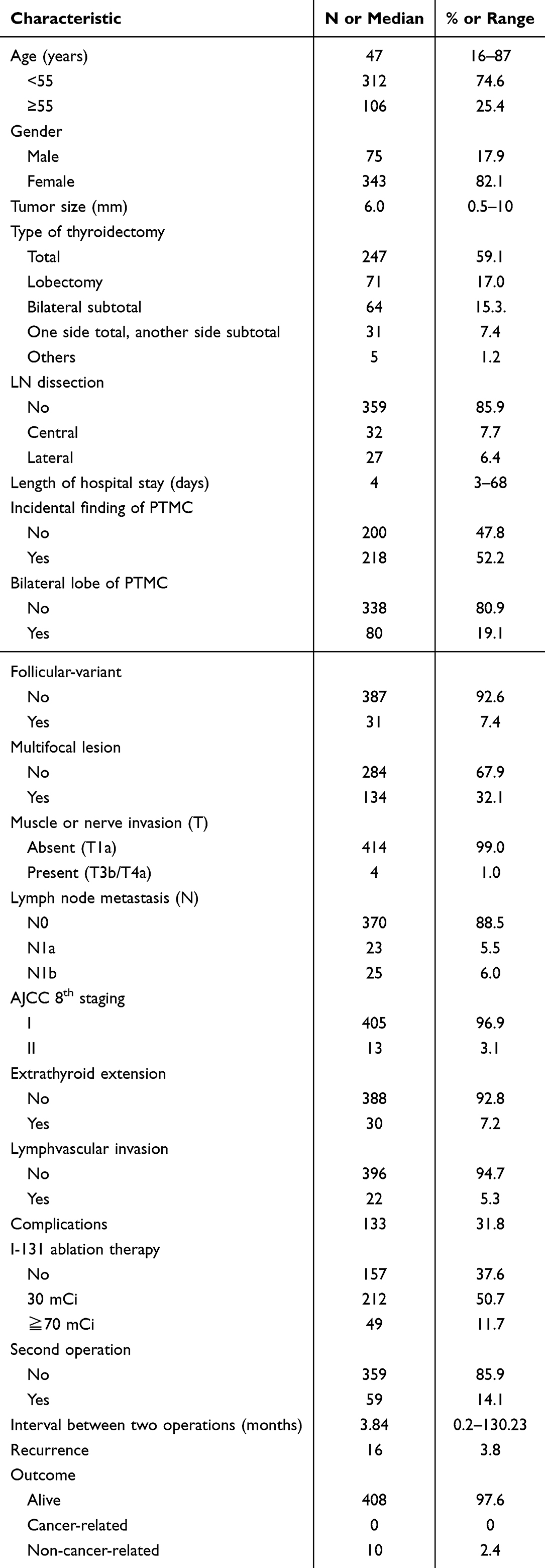 |
Table 1 Demographics and Clinicopathological Features (n=418) |
 |
Figure 1 Flowchrt of patient selection. Abbreviations: PTMC, papillary thyroid microcarcinoma; CGMH, Chang Gung Memorial Hospital; LN, lymph node. |
Regarding surgical approach, 247 patients (59.1%) underwent total thyroidectomy, while 171 patients (40.9%) underwent lobectomy. Central neck dissection was performed in 89 patients (21.3%), and lateral neck dissection was performed in 25 patients (6.0%). The higher rate of total thyroidectomy compared to current practice patterns reflects institutional preferences during the study period and likely introduces selection bias toward more extensive surgery in perceived higher-risk patients.
Incidental PTMC was identified in 218 patients (52.2%), while 200 patients (47.8%) had non-incidental findings. The most common concurrent benign conditions in the incidental group included multinodular goiter (45.3%), follicular adenoma (23.5%), and Graves’ disease (8.7%).
Multifocal Disease
Multifocal PTMC was identified in 134 patients (32.1% of the total cohort). The characteristics of the multifocal tumor group and the single tumor group are presented in Table 2. Among these, 89 patients (66.4%) had bilateral multifocal disease, while 45 patients (33.6%) had unilateral multifocal disease. The median number of tumor foci in multifocal cases was 3 (range: 2–8).
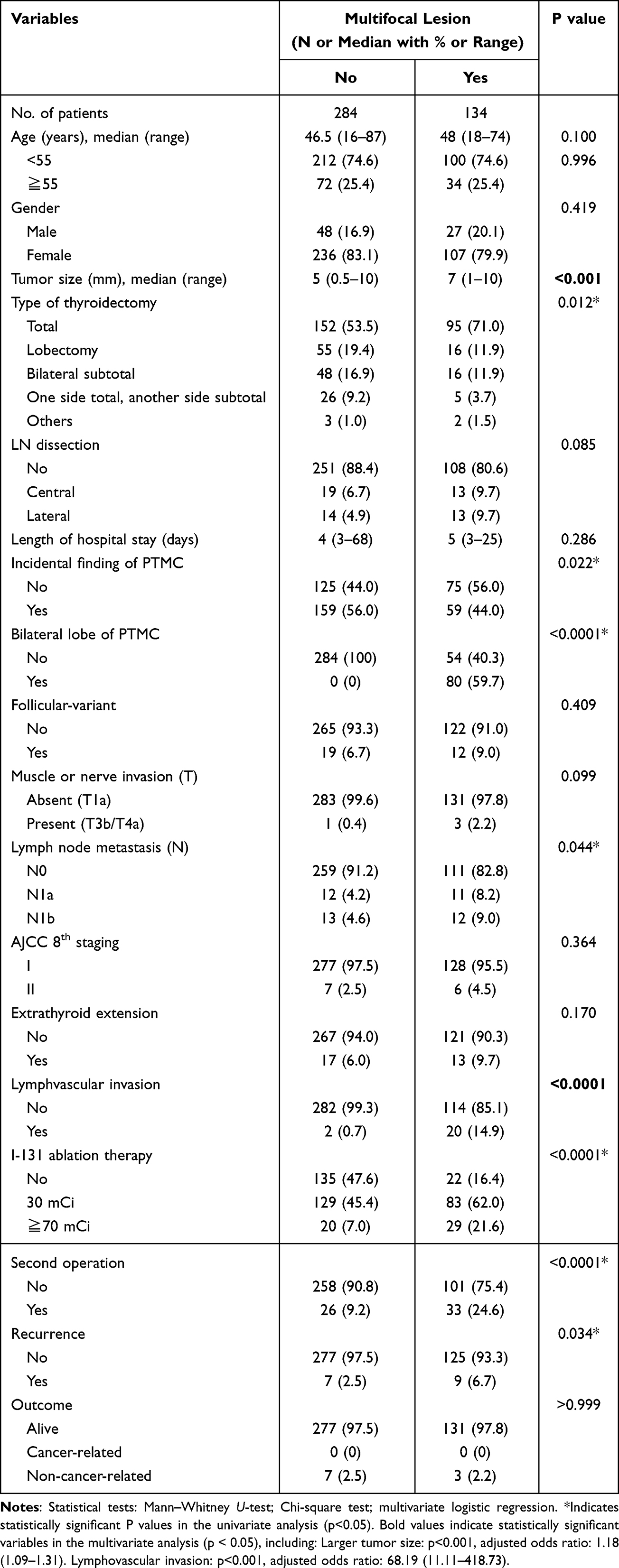 |
Table 2 Demographics and Clinicopathological Features of Multifocal Lesion |
Univariate analysis identified several factors associated with multifocal disease, including larger tumor size, incidental findings of PTMC, cervical lymph node metastasis, presence of lymphovascular invasion and recurrence. In multivariate analysis, larger tumor size (OR: 1.18 per mm increase, 95% CI: 1.09–1.31, p < 0.001) and lymphovascular invasion (OR: 68.19, 95% CI: 11.11–418.73, p < 0.001) remained significant independent predictors of multifocal disease.
Lymph Node Metastasis
Cervical lymph node metastasis was present in 48 patients (11.5% of the total cohort). Central neck metastasis was identified in 23 patients (5.5%), lateral neck metastasis in 14 patients (3.3%), and both central and lateral neck metastasis in 11 patients (2.6%). The median number of metastatic lymph nodes was 2 (range: 1–12). The characteristics of the lymph node metastasis group and the non-metastasis group are shown in Table 3.
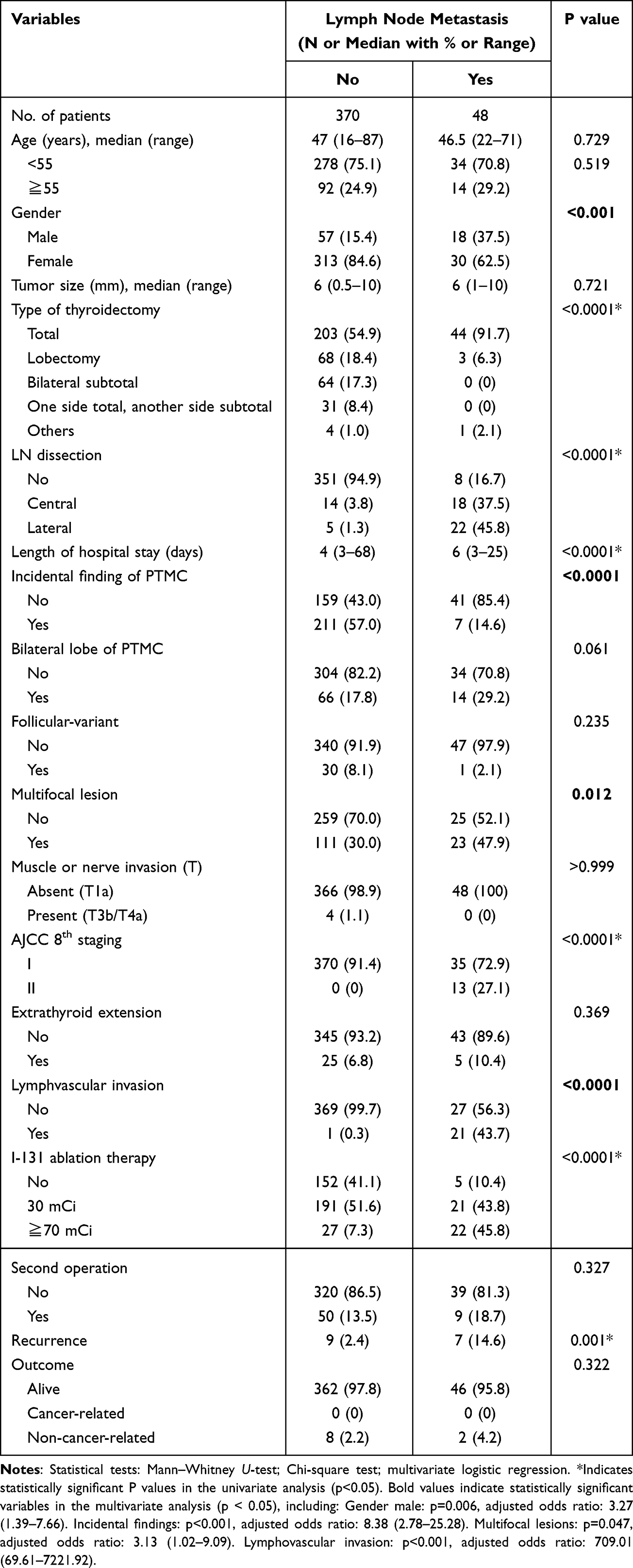 |
Table 3 Demographics and Clinicopathological Features of Lymph Node Metastasis |
Univariate analysis revealed associations between lymph node metastasis and male gender, non-incidental findings, multifocal disease, lymphovascular invasion and recurrence. Multivariate analysis confirmed male gender (OR: 3.27, 95% CI: 1.39–7.66, p = 0.006), non-incidental findings (OR: 8.38, 95% CI: 2.78–25.28, p < 0.001), multifocal disease (OR: 3.13, 95% CI: 1.02–9.09, p = 0.047), and lymphovascular invasion (OR: 709.01, 95% CI: 69.61–7221.92, p < 0.001) as independent predictors of cervical lymph node metastasis.
Recurrence and Survival Outcomes
During the median follow-up period of 154 months, recurrence occurred in 16 patients (3.8% of the total cohort). The median time to recurrence was 45 months (range: 12–128 months). Of these, three patients (18.8%) had recurrence at the thyroid bed, ten patients (62.5%) had recurrence in lymph nodes, and three patients (18.8%) had recurrence in both the thyroid bed and lymph nodes. The characteristics of the recurrence and non-recurrence groups are presented in Table 4.
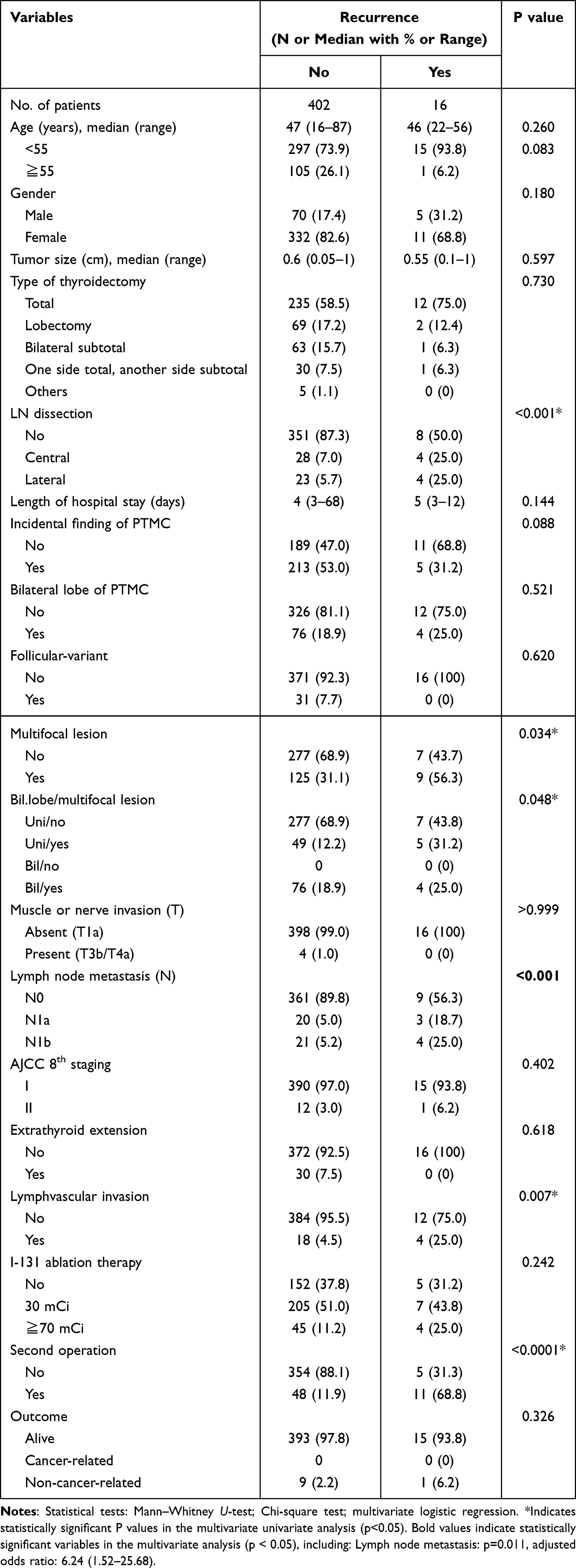 |
Table 4 Demographics and Clinicopathological Features of Recurrence |
Univariate analysis identified associations between recurrence and multifocal disease, lymphovascular invasion, and lymph node metastasis. However, in multivariate analysis, only lymph node metastasis remained a significant independent predictor of recurrence (OR: 6.24, 95% CI: 1.52–25.68, p = 0.011).
Ten deaths occurred during the study period. The overall survival rate was 97.6%, with no cancer-related mortality.
Sensitivity Analysis: Total Thyroidectomy Subgroup
To address potential selection bias, sensitivity analysis was performed on the 247 patients (59.1%) who underwent total thyroidectomy. In this subgroup, multifocal PTMC occurred in 95 patients (38.5%), cervical lymph node metastasis was present in 44 patients (17.8%), and recurrence occurred in 12 patients (4.9%). The higher prevalence of adverse features in this subgroup likely reflects selection bias toward more extensive surgery in higher-risk patients.
Multivariate analysis in the total thyroidectomy subgroup confirmed that larger tumor size (OR: 1.22, 95% CI: 1.08–1.38, p < 0.001) and lymphovascular invasion (OR: 71.23, 95% CI: 8.95–566.84, p < 0.001) remained significant predictors of multifocality. For lymph node metastasis, male gender (OR: 2.89, 95% CI: 1.26–6.63, p = 0.012), non-incidental findings (OR: 6.45, 95% CI: 1.98–21.02, p = 0.001), and lymphovascular invasion (OR: 445.67, 95% CI: 45.32–4382.15, p < 0.001) remained significant predictors. Lymph node metastasis remained the only significant predictor of recurrence (OR: 5.67, 95% CI: 1.34–23.98, p = 0.018).
Risk Stratification System
Based on our multivariate analysis results, we developed a risk stratification system incorporating the identified independent risk factors. The proposed system assigns points based on the presence of adverse features: male gender (2 points), non-incidental findings (2 points), multifocal lesions (1 point), and lymphovascular invasion (3 points).
Patients are classified into three risk categories: low risk (0–1 points), intermediate risk (2–3 points), and high risk (≥4 points or presence of lymphovascular invasion). Based on our cohort outcomes, estimated risks for lymph node metastasis are <5% for low-risk patients, 5–15% for intermediate-risk patients, and >15% for high-risk patients. Estimated recurrence risks are <2%, 2–5%, and >5% for low-, intermediate-, and high-risk patients, respectively (Figure 2).
 |
Figure 2 Study-defined risk stratification system of papillary thyroid microcarcinoma. |
Discussion
This study of 418 PTMC patients identified several clinicopathological features associated with adverse outcomes, providing important insights for risk stratification and treatment planning. Our key findings demonstrate that while PTMC generally follows an indolent course with excellent survival outcomes, specific risk factors can identify patients at increased risk for multifocal disease, lymph node metastasis, and recurrence.
The 32.1% prevalence of multifocal disease in our cohort aligns with previous reports and was independently associated with larger tumor size and lymphovascular invasion.12,13 The 11.5% rate of cervical lymph node metastasis, while lower than some published series, represents a clinically significant finding given its strong association with recurrence risk. Most importantly, our analysis identified lymph node metastasis as the only independent predictor of recurrence, emphasizing the prognostic importance of nodal status assessment.
Our findings are consistent with previous studies regarding the prevalence and risk factors for adverse outcomes in PTMC. The multifocal disease rate of 32.1% falls within the reported range of 26.8% to 34% in various series.9,12,13 Similarly, our lymph node metastasis rate of 11.5% is within the broad range reported in the literature, though lower than some series that may reflect differences in patient selection, surgical approach, or pathological assessment protocols.9
The identification of male gender as a risk factor for lymph node metastasis is consistent with multiple previous studies, though the underlying biological mechanisms remain unclear.14–16 The association between non-incidental findings and adverse outcomes likely reflects the fact that clinically apparent or imaging-detected lesions represent more aggressive tumor behavior compared to incidentally discovered microcarcinomas.
Our finding that lymphovascular invasion is the strongest predictor of both multifocal disease and lymph node metastasis is particularly noteworthy, with odds ratios exceeding 68 in our analysis. This emphasizes the importance of careful histopathological assessment for this feature, which may be underreported in routine pathological examination.
The predominantly histopathological nature of the most significant risk factors identified in our study has important implications for clinical practice. Lymphovascular invasion, the strongest predictor of adverse outcomes, can only be assessed through surgical specimen examination. Similarly, while imaging can detect some multifocal lesions, complete assessment of multifocality requires comprehensive pathological evaluation.
In our study, 16 patients (3.8%) experienced recurrence, which was associated with cervical lymph node metastasis (p = 0.011). Previous studies identified additional risk factors including age, multifocality, LN metastasis, extrathyroidal extension, capsular or vascular invasion, tumor size, BRAF V600E mutation, and sex.17–20 These findings highlight the importance of monitoring patients with these risk factors, particularly those with lymph node metastasis, for potential recurrence.
These findings support the continued importance of surgical management in PTMC, as histopathological assessment provides critical prognostic information that cannot be obtained through alternative treatment approaches. Our proposed risk stratification system provides a practical framework for treatment planning, with low-risk patients potentially suitable for less extensive surgical approaches and less intensive surveillance, while high-risk patients may benefit from more comprehensive management including total thyroidectomy with lymph node assessment.
Our findings also align with the recommendations of the American Thyroid Association (ATA) and National Comprehensive Cancer Network (NCCN) guidelines for the management of PTMC. According to the guidelines, active surveillance may be considered for carefully selected low-risk patients who show no evidence of lymph node metastasis, extrathyroidal extension, or aggressive pathological features. The risk factors identified in our cohort—particularly multifocality, lymphovascular invasion, and lymph node metastasis—correspond to guideline-defined indicators for higher-risk disease and suggest that these patients may be less suitable for active surveillance. Conversely, patients without these adverse features may fall into the low-risk category and could be considered for less extensive surgery or observation.21–23 By linking clinicopathological predictors with guideline-based risk stratification, our results help clarify which patients may benefit from more aggressive intervention versus more conservative management.
The emergence of radiofrequency ablation (RFA) as a minimally invasive alternative treatment for selected PTMC cases has generated significant interest, particularly in Asia where early clinical experience is expanding.24,25 While RFA offers potential benefits such as reduced procedural morbidity and improved cosmetic outcomes, appropriate patient selection remains a critical challenge. In our cohort, several key risk factors associated with aggressive features—such as lymphovascular invasion, multifocality, and microscopic lymph node metastasis—were primarily identified through postoperative histopathology, which t cannot be reliably assessed preoperatively.26
This gap underscores an important limitation shared by all non-surgical approaches, including RFA and active surveillance: the inability to obtain comprehensive pathological information before definitive treatment. As a result, RFA and active surveillance may be most suitable for a carefully selected subset of patients with unequivocally low-risk preoperative features, while others may still benefit from surgical intervention to allow complete pathological evaluation and more accurate risk stratification. Ultimately, treatment decisions should be individualized, integrating clinical, imaging, and—when available—molecular characteristics rather than relying on a single modality.
Several limitations should be considered when interpreting our findings. First, the retrospective single-center design introduces inherent selection and referral biases, which may limit generalizability to broader populations. The study period (2005–2015) also reflects historical practice patterns in which total thyroidectomy was more commonly performed, particularly for PTMC. This differs from contemporary guidelines that now favor less extensive surgery for appropriately selected low-risk patients, and may affect the direct applicability of our results to modern clinical practice.
Second, many of the key predictors identified in our model—such as lymphovascular invasion and multifocality—are pathological features that cannot be reliably assessed preoperatively. This highlights an important limitation for risk stratification when considering minimally invasive or non-surgical treatment modalities. Similarly, preoperative imaging has limited accuracy in detecting microscopic lymph node metastasis, further contributing to the challenge of selecting truly low-risk cases. Additionally, molecular characterization, including BRAF V600E and other markers, was not routinely performed during the study period (2005–2015). As a result, molecular data were unavailable for the majority of patients, which limits the ability to incorporate molecular risk factors into our analysis. This reflects historical practice patterns, as molecular testing was not widely adopted for PTMC during that time. The model would benefit from prospective validation and incorporation of molecular and imaging-based features.
At last, the relatively small number of recurrence events (n=16) limits statistical power for recurrence analysis and may have prevented identification of additional risk factors. Larger cohort studies with longer follow-up periods would strengthen the evidence base for recurrence risk prediction in PTMC.
Future studies should aim to validate our findings prospectively and across multiple centers. External validation of the risk stratification model, ideally incorporating molecular markers, advanced imaging characteristics, and potentially artificial intelligence–based prediction tools, would enhance its predictive accuracy and clinical utility. Further development of improved preoperative assessment methods will be essential for optimizing individualized treatment strategies, particularly as interest grows in minimally invasive approaches such as RFA and active surveillance.
Conclusion
PTMC demonstrates heterogeneous clinical behavior predictable by specific clinicopathological features. Male gender, non-incidental findings, multifocality, and lymphovascular invasion are independent risk factors for adverse outcomes, with lymphovascular invasion showing the strongest association. Cervical lymph node metastasis is the only independent predictor of recurrence. While most PTMC patients have excellent outcomes (97.6% overall survival), these findings may help guide individualized selection between surgical and minimally invasive approaches, including active surveillance, based on each patient’s clinical and pathological risk profile.
Ethics Statement
This study was approved by the Institutional Review Board of Chang Gung Medical Foundation (Approval No.: 202500444B0) and informed consent was waived due to the retrospective and anonymized nature of the data.
Acknowledgments
The authors thank Chang Gung Memorial Hospital (CGMH) for providing the research environment and institutional support. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Davies L, Welch HG. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg. 2014;140(4):317–14. doi:10.1001/jamaoto.2014.1
2. Zahan AE, Nechifor Boilă A, Pașcanu I, et al. Papillary thyroid microcarcinomas: a 25 years retrospective, institutional study of 255 cases. Acta Medica Marisiensis. 2016;62(1):41–46. doi:10.1515/amma-2015-0108
3. Grodski S, Brown T, Sidhu S, et al. Increasing incidence of thyroid cancer is due to increased pathologic detection. Surgery. 2008;144(6):1038–1043. doi:10.1016/j.surg.2008.08.023
4. Zevallos JP, Hartman CM, Kramer JR, Sturgis EM, Chiao EY. Increased thyroid cancer incidence corresponds to increased use of thyroid ultrasound and fine-needle aspiration: a study of the veterans affairs health care system. Cancer. 2015;121(5):741–746. doi:10.1002/cncr.29122
5. Heo J, Ryu HJ, Park H, et al. Mortality rate and causes of death in papillary thyroid microcarcinoma. Endocrine. 2024;83(3):671–680. doi:10.1007/s12020-023-03510-8
6. Jeon MJ, Kim WG, Choi YM, et al. Features predictive of distant metastasis in papillary thyroid microcarcinomas. Thyroid. 2016;26(1):161–168. doi:10.1089/thy.2015.0375
7. Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
8. National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Thyroid Carcinoma; 2024. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1470.
9. Song J, Yan T, Qiu W, Fan Y, Yang Z. Clinical analysis of risk factors for cervical lymph node metastasis in papillary thyroid microcarcinoma: a retrospective study of 3686 patients. Cancer Manag Res. 2020;12:2523–2530. doi:10.2147/CMAR.S250163
10. Li G, Li R, Zhong J, et al. A multicenter cohort study of thyroidectomy-related decision regret in patients with low-risk papillary thyroid microcarcinoma. Nat Commun. 2025. doi:10.1038/s41467-025-57627-7
11. Ringel MD, Sosa JA, Baloch Z, et al. 2025 American Thyroid Association Management guidelines for adult patients with differentiated thyroid cancer. Thyroid. 2025;35(8):841–985. doi:10.1177/10507256251363120
12. Zhao Q, Ming J, Liu C, et al. Multifocality and total tumor diameter predict central neck lymph node metastases in papillary thyroid microcarcinoma. Ann Surg Oncol. 2013;20(3):746–752. doi:10.1245/s10434-012-2654-2
13. Pyo JS, Sohn JH, Kang G. Detection of tumor multifocality is important for prediction of tumor recurrence in papillary thyroid microcarcinoma: a retrospective study and meta-analysis. J Pathol Transl Med. 2016;50(4):278–286. doi:10.4132/jptm.2016.03.29
14. Ruan J, Chen Z, Chen S, et al. Lateral lymph node metastasis in papillary thyroid microcarcinoma: a study of 5241 follow-up patients. Endocrine. 2024;83(2):414–421. doi:10.1007/s12020-023-03486-5
15. Zhao L, Sun X, Luo Y, Wang F, Lyu Z. Clinical and pathologic predictors of lymph node metastasis in papillary thyroid microcarcinomas. Ann Diagn Pathol. 2020;49(October):151647. doi:10.1016/j.anndiagpath.2020.151647
16. Sun J, Jiang Q, Wang X, Liu W, Wang X. Nomogram for preoperative estimation of cervical lymph node metastasis risk in papillary thyroid microcarcinoma. Front Endocrinol. 2021;12(March):1–7. doi:10.3389/fendo.2021.613974
17. de Ywata Carvalho A, Kohler HF, Gomes CC, Vartanian JG, Kowalski LP. Predictive factors of recurrence of papillary thyroid microcarcinomas: analysis of 2,538 patients. Int Arch Otorhinolaryngol. 2021;25(4):E585–E593. doi:10.1055/S-0040-1722253
18. Kaliszewski K, Diakowska D, Rzeszutko M, et al. Risk factors of papillary thyroid microcarcinoma that predispose patients to local recurrence. PLoS One. 2020;15(12 December):1–16. doi:10.1371/journal.pone.0244930
19. Huang K, Gao N, Bian D, Zhai Q, Yang P, Zhang Y. Associations of BRAF V600E, clinical pathology and imaging factors with the recurrence rate of papillary thyroid microcarcinoma. Exp Ther Med. 2020;20(6):1. doi:10.3892/etm.2020.9373
20. Chen Y, Sadow PM, Suh H, et al. BRAFV600E is correlated with recurrence of papillary thyroid microcarcinoma: a systematic review, multi-institutional primary data analysis, and meta-analysis. Thyroid. 2016;26(2):248–255. doi:10.1089/thy.2015.0391
21. Tuttle RM, Fagin JA, Minkowitz G, et al. Natural history and tumor volume kinetics of papillary thyroid cancers during active surveillance. JAMA Otolaryngol Head Neck Surg. 2017;143(10):1015–1020. doi:10.1001/jamaoto.2017.1442
22. Ito Y, Miyauchi A, Inoue H, et al. An observational trial for papillary thyroid microcarcinoma in Japanese patients. World J Surg. 2010;34(1):28–35. doi:10.1007/s00268-009-0303-0
23. Oda H, Sasai H, Masuoka H. Incidences of unfavorable events in the management of low-risk papillary microcarcinoma of the thyroid. Thyroid. 2016;26(1):150–155. doi:10.1089/thy.2015.0313
24. Yan L, Zhang M, Song Q, Luo Y. Ultrasound-guided radiofrequency ablation versus thyroid lobectomy for low-risk papillary thyroid microcarcinoma: a propensity-matched cohort study of 884 patients. Thyroid. 2021;31(11):1662–1672. doi:10.1089/thy.2021.0100
25. VanDijk SPJ, Coerts HI, Gunput STG, et al. Assessment of radiofrequency ablation for papillary microcarcinoma of the thyroid: a systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2022;148(4):317–325. doi:10.1001/jamaoto.2021.4381
26. Xing Z, Qiu Y, Yang Q, et al. Thyroid cancer neck lymph nodes metastasis: meta-analysis of US and CT diagnosis. Eur J Radiol. 2020:
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Younger Than 55 Years Old and BRAF V600E Mutation are Risk Factors for Lymph Node Metastasis in Papillary Thyroid Carcinomas ≤1.0 cm but Not in >1.0 cm
Lai Y, Gu Y, Yu M, Deng J
International Journal of General Medicine 2023, 16:1403-1414
Published Date: 19 April 2023
Preoperative Circulating Tumor Cells (CTCs) Positivity is Associated with Lymph Node Metastasis in Patients with Unifocal Papillary Thyroid Microcarcinoma (PTMC)
Zhong H, Zeng Q, Wang Y, Chen J
International Journal of General Medicine 2026, 19:569916
Published Date: 8 January 2026