Back to Journals » International Journal of General Medicine » Volume 19
Preoperative Circulating Tumor Cells (CTCs) Positivity is Associated with Lymph Node Metastasis in Patients with Unifocal Papillary Thyroid Microcarcinoma (PTMC)
Authors Zhong H, Zeng Q, Wang Y, Chen J
Received 8 October 2025
Accepted for publication 1 January 2026
Published 8 January 2026 Volume 2026:19 569916
DOI https://doi.org/10.2147/IJGM.S569916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ching-Hsien Chen
Haifeng Zhong, Qingxin Zeng, Yuedong Wang, Jiwei Chen
Department of Thyroid Surgery, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China
Correspondence: Jiwei Chen, Department of Thyroid Surgery, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China, Email [email protected]
Objective: To explore the relationship between the preoperative level of circulating tumor cells (CTCs) and lymph node metastasis in patients with unifocal papillary thyroid microcarcinoma (PTMC) (only one independent lesion, diameter ≤ 1 cm), and to clarify the value of preoperative CTCs detection in assessing the risk of lymph node metastasis in patients with unifocal PTMC.
Methods: Clinical records (age, gender, Hashimoto’s thyroiditis, thyroid function, invaded capsule, clinical stage) of 370 unifocal PTMC patients were collected retrospectively. The CTCs levels of the patients were measured. The preoperative CTCs positive rate between patients with and without lymph node metastasis were compared; logistic regression analysis was used to explore whether the preoperative CTCs positivity is an independent risk factor for lymph node metastasis.
Results: A total of 207 (55.9%) unifocal PTMC patients presented with preoperative positive CTCs (≥ 8.7 FU/3mL), whereas 163 cases (44.1%) were identified as CTCs negative (< 8.7 FU/3mL). The patients with lymph node metastasis had higher proportions of invaded capsule (35.8%% vs 25.2%, p=0.037), and preoperative CTCs positivity (64.2% vs 52.0%, p= 0.033) than patients without lymph node metastasis. Logistic regression analysis shows that preoperative CTCs positivity (odds ratio (OR): 1.654, 95% confidence interval (CI): 1.040– 2.631, p=0.033), and invaded capsule (OR: 1.652, 95% CI: 1.020– 2.677, p=0.041) were associated with lymph node metastasis in patients with unifocal PTMC.
Conclusion: Preoperative CTCs positivity (≥ 8.7 FU/3mL) and invaded capsule are associated with lymph node metastasis in unifocal PTMC. Preoperative CTCs detection can serve as an important auxiliary indicator for evaluating the lymph node metastasis potential of patients with unifocal PTMC, thereby providing valuable reference evidence for clinicians to formulate individualized surgical plans and postoperative follow-up strategies.
Keywords: circulating tumor cell, unifocal, papillary thyroid microcarcinoma, lymph node metastasis
Introduction
Thyroid carcinoma is the most common type of malignant tumor of the thyroid gland.1,2 In recent years, the incidence of thyroid carcinoma has exhibited a sustained upward trend, emerging as one of the most prevalent malignant tumors of the endocrine system.3,4 Papillary thyroid carcinoma (PTC) is the main pathological subtype of thyroid cancer, accounts for approximately 80% to 90% of all thyroid cancer cases.4–6 The overall prognosis of PTC is favorable.7 However, distinct subtypes characterized by unique clinical and pathological features show marked discrepancies in disease progression, treatment strategy selection, and prognostic evaluation.8 Adopting specific diagnostic and prognostic assessment methods for different subtypes plays a crucial role in clinical diagnosis and treatment.9
Unifocal papillary thyroid microcarcinoma (PTMC) refers to a type of PTC in which there is only one independent lesion within the thyroid gland with a maximum diameter of ≤ 1 centimeter (cm) and possessing typical pathological features of papillary carcinoma (such as papillary arrangement of tumor cells, and the cell nuclei show a frosted glass-like change).10 In recent years, the incidence of PTMC has been increasing rapidly, with unifocal PTMC accounting for 40–60% of all newly diagnosed thyroid cancer cases.11,12 Surgical treatment remains an important approach for the treatment of unifocal PTMC, and the optimal surgical approach for the primary lesion—either thyroid lobectomy or total thyroidectomy—requires careful clinical deliberation.13 The scope of cervical lymph node dissection should follow the principle of individualized treatment. The selection of surgical scope is one of the current clinical decision-making challenges.14,15 This procedure should be performed only when cervical lymph node metastasis is definitively confirmed preoperatively or intraoperatively, thereby avoiding complications such as lymphatic leakage, shoulder dysfunction, and recurrent laryngeal nerve injury that arise from unnecessary extensive dissection.16
Controversy surrounding optimal surgical strategies is far more pronounced for patients with unifocal PTMC than for those with multifocal lesions. In particular, no consensus has yet been reached regarding the role of prophylactic lymph node dissection in this patient population.17,18 The assessment of lymph node metastasis in unifocal PTMC has significant clinical value, but we still know very little about it at present. Circulating tumor cells (CTCs) refer to tumor-derived cells that detach from primary or metastatic tumor foci and enter the peripheral blood circulation.19 Their presence is closely related to the invasion and metastasis process of the tumor and has been proven to be an important biomarker for the assessment of metastasis risk, therapeutic efficacy monitoring, and prognosis judgment in various solid tumors.20–22 In the field of thyroid cancer, some studies have confirmed that CTCs were associated with tumor stage, lymph node metastasis, and distant metastasis.23–25 However, in patients with unifocal PTMC, is there any relationship between CTC and lymph node metastasis? The purpose of this study is to address this issue, and we hope to provide valuable reference data for the role of CTC in the risk assessment of lymph node metastasis in unifocal PTMC.
Materials and Methods
Subjects
The subjects of this study were all patients with unifocal PTMC who were admitted to Meizhou People’s Hospital from June 2021 to April 2023. All patients were diagnosed with unifocal PTMC via postoperative pathological examination and had complete clinical datasets, including demographic profiles, preoperative test results, surgical records, and postoperative pathological reports.
Inclusion criteria of patients were as follows: (1) the postoperative pathological diagnosis was clearly a unifocal PTMC, meaning the tumor diameter was ≤ 1 cm, and the pathological examination confirmed that there was only a single tumor lesion; (2) all patients underwent surgical treatment; (3) none of the patients had received radioiodine therapy, chemotherapy, radiotherapy, or other anti-tumor treatments targeting thyroid tumors before the surgery; (4) the clinical data of the patients were complete, and all the necessary indicators for subsequent research could be obtained, such as gender, age, tumor size, tumor location, whether it invaded the capsule, and whether it was accompanied by Hashimoto’s thyroiditis, and so on; and (5) the patients all gave informed consent, voluntarily participated in this study, and signed the informed consent form.
Exclusion criteria as follows: (1) patients with a pathological diagnosis of multifocal PTMC or other types of thyroid malignancies; (2) patients with PTC whose tumor diameter is >1 cm; (3) patients who have received anti-tumor treatments such as radioactive iodine therapy, chemotherapy, or radiotherapy before the surgery; (4) patients whose clinical data are incomplete and the key indicators required for the study cannot be obtained; (5) patients with other serious malignant tumors, severe cardiovascular and cerebrovascular diseases, liver and kidney failure, and so on, which may affect the judgment of the research results; and (6) patients who refuse to participate in this study and have not signed the informed consent form.
Data Collection
We collected the data of patients who met the inclusion criteria through the hospital’s electronic medical record system, including: age, gender, preoperative CTCs, Hashimoto’s thyroiditis, thyroid function, maximum lesion diameter, invaded capsule, clinical stage, and lymph node metastasis. Based on some previous studies, the patients included in this study were divided into two groups: <55 years old group and ≥55 years old group.26,27 Diagnosis of Hashimoto’s thyroiditis: based on the patient’s clinical symptoms (such as goiter, and fatigue), it is necessary to meet the following conditions: positive thyroid peroxidase antibody (TPOAb) and/or thyroid globulin antibody (TgAb) in thyroid function tests, as well as typical imaging features such as diffuse hypoechoic and grid-like changes shown by thyroid ultrasound; for those with negative antibodies, pathological manifestations such as lymphocyte infiltration and eosinophilic changes in follicular epithelial cells can be identified through fine-needle aspiration cytology to confirm the diagnosis.28
The diagnostic criteria of thyroid function are as follows:29 (1) normal thyroid function: 0.27mIU/L≤thyroid stimulating hormone (TSH)≤4.2mIU/L, 3.1pmol/L≤free triiodothyronine (FT3)≤6.8pmol/l, 12.0pmol/L≤free thyroxine (FT4)≤22.0pmol/L; (2) hyperthyroidism: TSH<0.27mIU/L; FT4>22pmol/L or FT3>6.8pmol/L; (3) hypothyroidism: TSH>4.2mIU/L and FT4<12pmol/L. Hyperthyroidism and hypothyroidism are both regarded as thyroid dysfunction.
Detection of CTCs
The detection of CTCs is carried out using the immunomagnetic bead sorting method (IMB) combined with real-time quantitative polymerase chain reaction (qPCR), as described in previous studies.30–32 The sample for detection is 3 mL of peripheral venous blood collected from the patient within one week before the operation, placed in an anticoagulant tube containing ethylenediaminetetraacetic acid (EDTA). The red blood cells and most white blood cells are removed by negative enrichment method to obtain folate receptor-positive cells. These cells are labeled with specific small molecule probes, and finally, through polymerase chain reaction (PCR), the oligonucleotides bound to the small molecule probes are quantitatively amplified and detected. The level of CTCs is calculated based on the Ct value. All detection operations are strictly carried out in accordance with the name and instructions of the test kit (CytoploRare Kit, Genosaber Biotech, Shanghai, China) and the laboratory standard operating procedure (SOP). Folate receptor Unit (FU) per 3mL (FU/3mL) as defined in the manufacturer’s manual, was used to represent the level of FR+CTC in 3 mL of peripheral blood. Based on the cutoff value specified in the instructions for the CTCs detection kit, a CTCs concentration of ≥8.7 FU/3mL (defined as the unit of folate receptor-positive CTCs per 3mL of blood sample) is classified as a positive result, whereas values below this threshold are regarded as negative.
Statistical Analysis
SPSS statistical software (version 26.0, IBM Inc., USA) was used for data analysis. χ2 test was used to evaluate the relationship between CTCs levels and clinical features of unifocal PTMC patients. Logistic regression analysis was used to evaluate the relationship between CTCs and lymph node metastasis in patients with unifocal PTMC adjusting for confounding factors such as age, gender, Hashimoto’s thyroiditis, thyroid function, invaded capsule, and clinical stage. Calculate the odds ratio (OR) and its 95% confidence interval (95% CI) for each independent risk factor. An OR value >1 indicates that the factor is a risk factor, while an OR value <1 indicates that the factor is a protective factor p<0.05.
Results
Clinicopathological Features of Patients with Unifocal PTMC
In the 370 patients with unifocal PTMC, 308 cases (83.2%) were aged ≤55 years and 62 cases (16.8%) were aged >55 years; the cohort comprised 67 males (18.1%) and 303 females (81.9%). Additionally, 86 patients (23.2%) had Hashimoto’s thyroiditis, 36 (9.7%) presented with abnormal thyroid function, and 106 (28.6%) had capsular invasion. With respect to T stage, 364 patients (98.4%) were classified as T1-T2 and 6 patients (1.6%) as T3-T4. A total of 207 (55.9%) unifocal PTMC patients presented with preoperative positive CTCs (≥8.7 FU/3mL), whereas 163 cases (44.1%) were identified as CTCs negative (<8.7 FU/3mL) (Table 1).
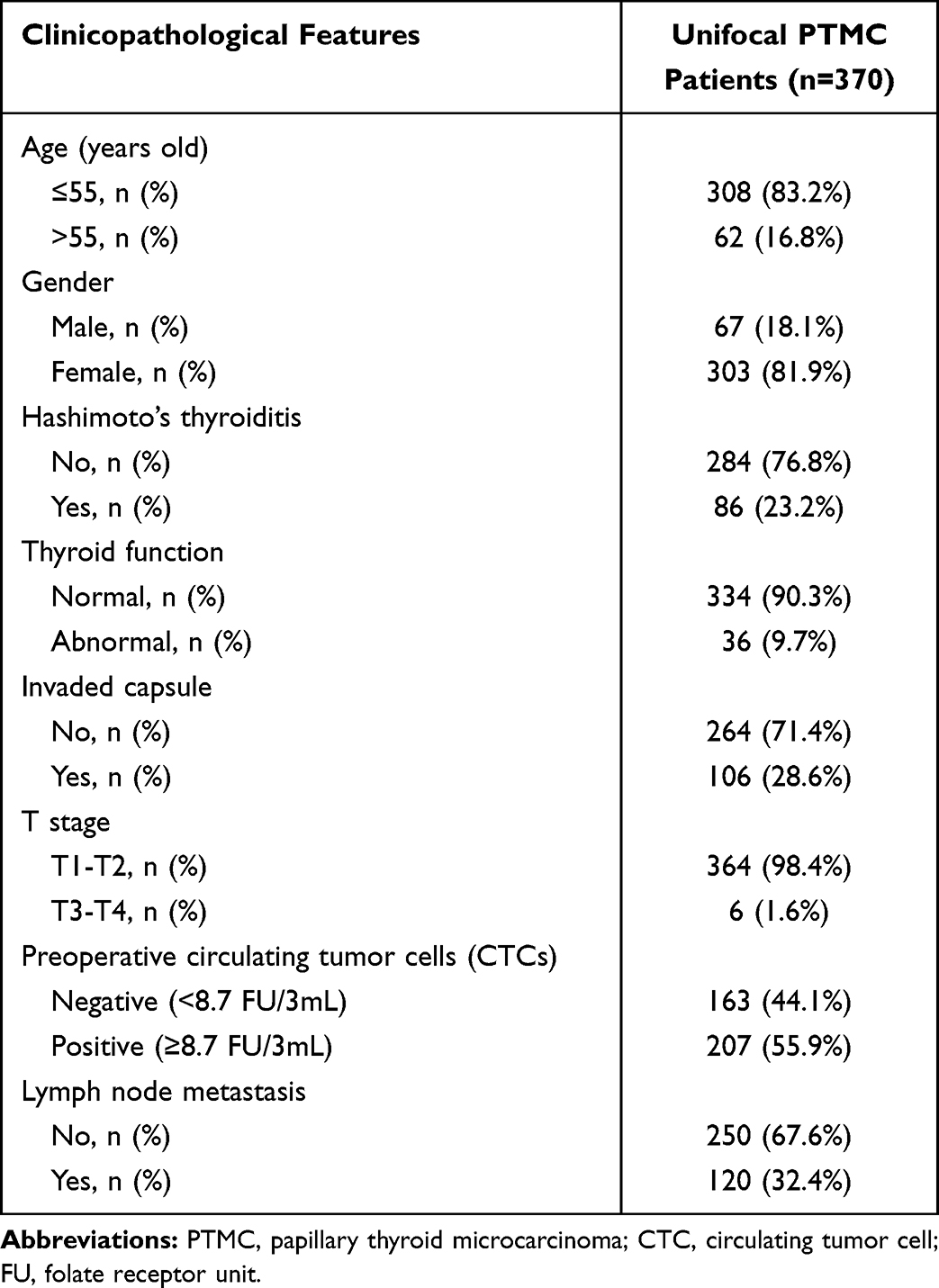 |
Table 1 The Clinicopathological Features of Patients with Unifocal PTMC |
Comparison of Clinicopathological Features Among Unifocal PTMC Patients with and without Lymph Node Metastasis
The unifocal PTMC patients with lymph node metastasis had higher proportions of invaded capsule (35.8%% vs 25.2%, p=0.037), and preoperative CTCs positivity (64.2% vs 52.0%, p=0.033) compared with those without lymph node metastasis. By contrast, no statistically significant differences were observed between the two groups in terms of age and gender distributions, or the proportions of Hashimoto’s thyroiditis, thyroid function abnormalities, and pathological T stage (Table 2).
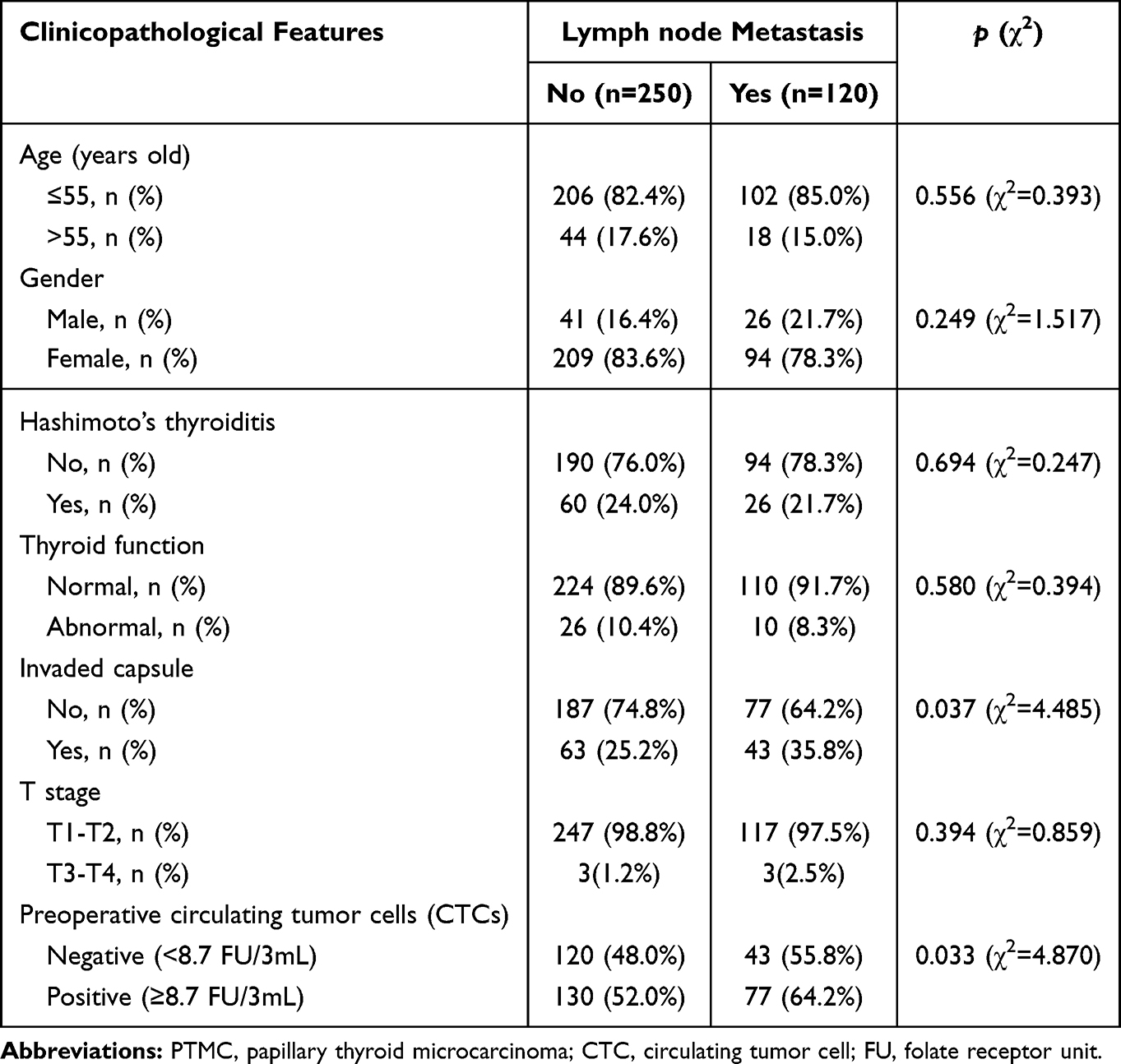 |
Table 2 Comparison of Clinicopathological Features Among Unifocal PTMC Patients with and Without Lymph Node Metastasis |
Comparison of Clinical Features According to Different CTCs Levels in Unifocal PTC Patients with and without Lymph Node Metastasis, Respectively
Among unifocal PTMC patients without lymph node metastasis, no statistically significant differences were detected between CTC-negative and CTC-positive subgroups with respect to age, gender, prevalence of Hashimoto’s thyroiditis, capsular invasion status, and pathological T stage. In unifocal PTMC patients with lymph node metastasis, there were no significant difference of clinical features between patients with negative and positive CTCs (Table 3).
 |
Table 3 Comparison of Clinical Features According to Different CTCs Levels in Unifocal PTC Patients with and Without Lymph Node Metastasis, Respectively |
Logistic Regression Analysis of Risk Factors of Lymph Node Metastasis in Unifocal PTMC
In univariate logistic regression analysis, preoperative CTCs positivity (≥8.7 vs <8.7 FU/3mL, odds ratio (OR): 1.653, 95% confidence interval (CI): 1.056–2.587, p=0.028), and invaded capsule (OR: 1.658, 95% CI: 1.036–2.652, p=0.035) were identified as factors associated with lymph node metastasis among unifocal PTMC. Consistently, multivariate logistic regression analysis confirmed that preoperative CTCs positivity (≥8.7 vs <8.7 FU/3mL, OR: 1.654, 95% CI: 1.040–2.631, p=0.033), and invaded capsule (OR: 1.652, 95% CI: 1.020–2.677, p=0.041) remained independently associated with lymph node metastasis in this cohort (Table 4).
 |
Table 4 Logistic Regression Analysis of Risk Factors of Lymph Node Metastasis in Unifocal PTMC |
Discussion
This study found that a preoperative CTCs positivity was significantly associated with cervical lymph node metastasis in patients with unifocal PTMC. This result not only provides valuable reference for the preoperative assessment of lymph node metastasis in unifocal PTMC, but also further reveals the potential mechanism of invasion and metastasis of unifocal PTMC at the molecular level, and has important clinical implications and scientific value for optimizing the individualized treatment strategy of unifocal PTMC.
In this study, the unifocal PTMC patients with lymph node metastasis had higher proportion of preoperative CTCs positivity (64.2%) than patients without lymph node metastasis (52.0%). Moreover, the multivariate logistic regression analysis showed that the preoperative CTCs positivity was an independent risk factor for lymph node metastasis in unifocal PTMC (OR: 1.654, 95% CI: 1.040–2.631, p=0.033). This result is highly consistent with the previous research results in the field of thyroid cancer.23,31–33 Some studies have found that the preoperative level of CTCs was associated with lymph node metastasis in patients with PTC.23,33 The research conducted by Yu et al revealed that in patients with PTC accompanied by capsule invasion, the preoperative level of CTCs was a risk factor for lymph node metastasis.31 However, another study suggested that the diagnostic efficacy of CTCs in thyroid cancer is limited, and their diagnostic value still requires further exploration.30
Based on the biological mechanism of tumor invasion and metastasis and the results of this study, the association between CTCs positivity before surgery and lymph node metastasis in unifocal PTMC can be explained from the following aspects. Firstly, CTCs represent a molecular marker reflective of tumor invasive potential. The development of lymph node metastasis in unifocal PTMC entails a series of critical steps, including tumor cell penetration of the thyroid basement membrane, lymphatic vessel invasion, and subsequent colony formation within regional lymph nodes.34 The generation of CTCs is a direct manifestation of the invasive nature of tumor cells. PTMC cells with high metastatic potential can acquire stronger motility and anti-apoptotic ability through the epithelial-mesenchymal transition (EMT) process, enabling them to leave the primary site and enter the bloodstream.35,36 A preoperative CTCs positivity may not only be an indication of the tumor’s invasive potential, but may also be related to the molecular driving mechanism of unifocal PTMC. The changes in gene functions and activation of signaling pathways underlying this process collectively form the molecular basis for lymph node metastasis.
Secondly, the issue of the temporal correlation between CTCs and lymph node metastasis. The traditional view holds that the path of tumor metastasis is “primary tumor → lymphatic vessels → lymph nodes → blood circulation”, meaning that lymph node metastasis occurs before the generation of CTCs.37 However, recent studies have proposed a new viewpoint that CTCs may exist before lymph node metastasis, that is, some tumor cells directly enter the blood circulation from the primary tumor to form CTCs,38,39 and can form metastatic foci more easily in the lymph nodes in the form of “circulating tumor cell clusters” (CTCs clusters).40 CTCs may be the “precursor cells” of lymph node metastases. The presence of high CTCs levels means that more CTCs are likely to invade the lymphatic system.41–45 CTCs positivity indicates the presence of more tumor cells with colonization ability, thereby increasing the risk of lymph node metastasis. This viewpoint provides a theoretical basis for the early prediction of lymph node metastasis in unifocal PTMC. The preoperative CTCs positivity can serve as a “pre-metastasis signal”, alerting to potential metastasis risks before the presence of metastatic foci is detected by imaging or pathology.
The results of this study provided optimized strategies for the preoperative risk stratification management of patients with unifocal PTMC. Currently, the preoperative risk stratification of unifocal PTMC mainly relies on clinical and pathological indicators such as tumor size, location, and ultrasound features (such as hypoechoic appearance, irregular margins), lacking molecular-level assessment indicators.46 The findings of this study suggest that preoperative CTCs levels can be incorporated into the risk stratification system for unifocal PTMC, and a combined stratification model integrating “clinicopathological indicators + CTCs” can be established. Specifically, patients with preoperative CTCs negativity and no other high-risk factors may be categorized as “extremely low-risk”; such individuals are suitable for active surveillance or thyroid lobectomy as the first-line management strategy, and routine cervical lymph node dissection is not warranted. Conversely, patients with preoperative CTCs positivity or concurrent high-risk factors may be stratified as “moderate-risk”. For this subgroup, preoperative cervical contrast-enhanced computed tomography (CT) and ultrasound-guided fine-needle aspiration cytology (US-FNAC) should be performed. Intraoperatively, careful exploration of the central lymph node compartment is recommended, with selective lymph node dissection considered when clinically indicated. In addition, although CTCs detection has advantages such as real-time monitoring and minimally invasive sampling in tumor prognosis assessment, due to technical limitations, biological characteristics, and clinical application conditions, the value of CTC detection in the diagnosis and treatment of thyroid cancer still requires more research to be confirmed. In clinical practice, CTCs can together with other markers (such as programmed death-ligand 1 (PD-L1),47 AXL level,48 and rosette-like clusters (RLC) of follicular cells49), provide a comprehensive assessment for the diagnosis and prognosis of thyroid cancer.
This study has several limitations when exploring the relationship between preoperative CTCs positivity and lymph node metastasis in patients with unifocal PTMC. Firstly, a primary constraint is the lack of well-accepted detection methods characterized by both high sensitivity and specificity, as different CTCs detection platforms differ considerably in terms of these two core performance indicators. With a wide array of CTCs detection technologies at disposal, the employment of varying methodologies for CTCs separation, enrichment and quantitative analysis is prone to produce inconsistent data, leading to the likelihood that differential detection techniques could induce variability in the outcomes of relevant research. The method used in this study to detect the number of folate receptor-positive cells by RT-PCR has yet to be further evaluated in terms of its detection efficacy. Secondly, as a single-center retrospective study, this study has selection and information bias, which affects the generalizability of the results. Thirdly, this study used postoperative pathology as the gold standard for metastasis, as the scope of dissection is not uniform and routine sectioning fails to detect small metastatic foci, resulting in inaccurate assessment and lacking comprehensive evaluation and CTCs dynamic changes, as well as long-term prognosis correlation data. Finally, this study only confirmed the correlation between CTCs and lymph node metastasis, without excluding reverse causality, lacking intervention evidence and dose-response relationship analysis, weakening the causal inference ability and clinical application accuracy.
Based on the results and limitations of this study, future research can be conducted in the following three aspects. First, highly sensitive CTCs detection technologies tailored specifically for unifocal PTMC should be developed, and combined with techniques such as single-cell sequencing and spatial transcriptomics to analyze the molecular characteristics and clonal evolution patterns of CTCs, thereby clarifying their causal relationship with lymph node metastasis. Second, large-scale multicenter, prospective randomized controlled trials are warranted to evaluate the prognostic impacts of CTCs-driven personalized treatment strategies relative to standard-of-care regimens in the unifocal PTMC population, which will further corroborate the clinical application value of CTCs detection. Third, investigations should be conducted into the combined application of CTCs with other biomarkers (eg, circulating tumor DNA (ctDNA), non-coding RNAs) to develop a multidimensional prediction model, which would further enhance the accuracy of lymph node metastasis and prognostic assessment in patients with unifocal PTMC.
Conclusions
Preoperative CTCs positivity (≥8.7 FU/3mL) and invaded capsule are associated with lymph node metastasis in unifocal PTMC. Preoperative CTCs detection can serve as an important auxiliary indicator for evaluating the lymph node metastasis potential of patients with unifocal PTMC, thereby providing valuable reference evidence for clinicians to formulate individualized surgical plans and postoperative follow-up strategies. It provides new references and evidence support for the precise diagnosis and treatment of solitary PTMC. In the future, large-sample, multicenter prospective studies are still needed to further verify the clinical application value of CTCs in predicting lymph node metastasis in unifocal PTMC and clarify the correlation between CTCs and the long-term prognosis of patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All participants were informed of the research procedures and objectives, and this study obtained the informed consent of all participants. The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital (Clearance No.: 2024-C-282).
Acknowledgments
The authors would like to thank other colleagues whom were not listed in the authorship for their helpful comments on the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program for Social Development of Meizhou (Grant No.: 2024C0301072 and 2025C0301031).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Houten PV, Netea-Maier RT, Smit JW. Differentiated thyroid carcinoma: an update. Best Pract Res Clin Endocrinol Metab. 2023;37(1):101687. doi:10.1016/j.beem.2022.101687
2. Yan K, Liu QZ, Huang RR, et al. Spatial transcriptomics reveals prognosis-associated cellular heterogeneity in the papillary thyroid carcinoma microenvironment. Clin Transl Med. 2024;14(3):e1594. doi:10.1002/ctm2.1594
3. Seib CD, Sosa JA. Evolving understanding of the epidemiology of thyroid cancer. Endocrinol Metab Clin North Am. 2019;48(1):23–10. doi:10.1016/j.ecl.2018.10.002
4. Carnazza M, Quaranto D, DeSouza N, et al. The current understanding of the molecular pathogenesis of papillary thyroid cancer. Int J Mol Sci. 2025;26(10):4646. doi:10.3390/ijms26104646
5. Zhang YH, Cheng YH, Cai G, Zhang YJ. Expression and significance of aquaporin-4 in thyroid carcinoma. Mult Scler Relat Disord. 2021;48:102726. doi:10.1016/j.msard.2020.102726
6. Al-Qurayshi Z, Sullivan CB, Pagedar N, Lee GS, Tufano R, Kandil E. Prevalence and risk of metastatic thyroid cancers and management outcomes: a national perspective. Laryngoscope. 2021;131(1):237–244. doi:10.1002/lary.28722
7. Wang Y, Xiao Y, Pan Y, et al. The effectiveness and safety of prophylactic central neck dissection in clinically node-negative papillary thyroid carcinoma patients: a meta-analysis. Front Endocrinol. 2022;13:1094012. doi:10.3389/fendo.2022.1094012
8. Zhao J, Zhang W, Lu D, et al. Clinical prognostic risk assessment of different pathological subtypes of papillary thyroid cancer: a systematic review and network meta-analysis. Langenbecks Arch Surg. 2025;410(1):251. doi:10.1007/s00423-025-03841-2
9. Li Z, Wang N, Li X, et al. Thyroid cancer: from molecular insights to therapy (Review). Oncol Lett. 2025;30(5):520. doi:10.3892/ol.2025.15266
10. Cakir E, Saygin I, Kisioglu S. A comparison between unifocal papillary thyroid microcarcinoma with noninvasive follicular thyroid neoplasm with papillary-like nuclear features and other patterns: a retrospective clinicopathological study. Indian J Pathol Microbiol. 2020;63(2):188–193. doi:10.4103/IJPM.IJPM_586_19
11. Li Q, Feng T, Zhu T, et al. Multi-omics profiling of papillary thyroid microcarcinoma reveals different somatic mutations and a unique transcriptomic signature. J Transl Med. 2023;21(1):206. doi:10.1186/s12967-023-04045-2
12. Alqaryan S, Almousa H, Almutairi R, et al. Papillary thyroid microcarcinoma with and without nodal metastasis: a comparative analysis. Saudi Med J. 2024;45(3):267–272. doi:10.15537/smj.2024.45.3.20230638
13. Ruggiero R, Pirozzi R, Gualtieri G, et al. Overview on surgical management of papillary thyroid microcarcinoma. G Chir. 2019;40(2):81–87. PMID: 31131805.
14. Su H, Li Y. Prophylactic central neck dissection and local recurrence in papillary thyroid microcarcinoma: a meta-analysis. Braz J Otorhinolaryngol. 2019;85(2):237–243. doi:10.1016/j.bjorl.2018.05.004
15. Kim BY, Choi N, Kim SW, Jeong HS, Chung MK, Son YI. Randomized trial of prophylactic ipsilateral central lymph node dissection in patients with clinically node negative papillary thyroid microcarcinoma. Eur Arch Otorhinolaryngol. 2020;277(2):569–576. doi:10.1007/s00405-019-05702-3
16. Lo CY. Lymph node dissection for papillary thyroid carcinoma. Methods Mol Biol. 2022;2534:57–78. doi:10.1007/978-1-0716-2505-7_5
17. Kaliszewski K, Diakowska D, Wojtczak B, et al. Which papillary thyroid microcarcinoma should be treated as “true cancer” and which as “precancer”? World J Surg Oncol. 2019;17(1):91. doi:10.1186/s12957-019-1638-0
18. Feng JW, Pan H, Wang L, Ye J, Jiang Y, Qu Z. Total tumor diameter: the neglected value in papillary thyroid microcarcinoma. J Endocrinol Invest. 2020;43(5):601–613. doi:10.1007/s40618-019-01147-x
19. Dai CS, Mishra A, Edd J, Toner M, Maheswaran S, Haber DA. Circulating tumor cells: blood-based detection, molecular biology, and clinical applications. Cancer Cell. 2025;43(8):1399–1422. doi:10.1016/j.ccell.2025.07.008
20. Deng Z, Wu S, Wang Y, Shi D. Circulating tumor cell isolation for cancer diagnosis and prognosis. EBioMedicine. 2022;83:104237. doi:10.1016/j.ebiom.2022.104237
21. Lin D, Shen L, Luo M, et al. Circulating tumor cells: biology and clinical significance. Signal Transduct Target Ther. 2021;6(1):404. doi:10.1038/s41392-021-00817-8
22. Pereira-Veiga T, Schneegans S, Pantel K, Wikman H. Circulating tumor cell-blood cell crosstalk: biology and clinical relevance. Cell Rep. 2022;40(9):111298. doi:10.1016/j.celrep.2022.111298
23. Gu Y, Yu M, Deng J, Lai Y. Preoperative circulating tumor cells level is associated with lymph node metastasis in patients with unifocal papillary thyroid carcinoma. World J Surg Oncol. 2025;23(1):47. doi:10.1186/s12957-025-03702-8
24. Qiu ZL, Wei WJ, Sun ZK, et al. Circulating tumor cells correlate with clinicopathological features and outcomes in differentiated thyroid cancer. Cell Physiol Biochem. 2018;48(2):718–730. doi:10.1159/000491898
25. Weng X, YangYang, Cai Y. Clinical significance of circulating tumor cells (CTCs) and survivin on predicting prognosis in thyroid cancer patients. Dis Markers. 2022;2022:5188006. doi:10.1155/2022/5188006
26. Gong J, Zhu B, Liu W, et al. Risk factors for lymph node metastasis in papillary thyroid carcinoma: a retrospective study. Horm Metab Res. 2023;55(5):315–322. doi:10.1055/a-2057-8358
27. Zhong H, Zeng Q, Long X, Lai Y, Chen J, Wang Y. Risk factors analysis of lateral cervical lymph node metastasis in papillary thyroid carcinoma: a retrospective study of 830 patients. World J Surg Oncol. 2024;22(1):162. doi:10.1186/s12957-024-03455-w
28. Ralli M, Angeletti D, Fiore M, et al. Hashimoto’s thyroiditis: an update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential malignant transformation. Autoimmun Rev. 2020;19(10):102649. doi:10.1016/j.autrev.2020.102649
29. Huang Y, Lou P, Li H, Li Y, Ma L, Wang K. Risk nomogram for papillary thyroid microcarcinoma with central lymph node metastasis and postoperative thyroid function follow-up. Front Endocrinol. 2024;15:1395900. doi:10.3389/fendo.2024.1395900
30. Zeng Q, Zhong H, Rao H, Wang Y. Diagnostic value of circulating tumor cells in patients with thyroid cancer: a retrospective study of 1478 patients. Discov Oncol. 2024;15(1):114. doi:10.1007/s12672-024-00976-4
31. Yu M, Deng J, Gu Y, Lai Y, Zheng Z. Positive preoperative circulating tumor cells level associated with lymph node metastasis in papillary thyroid carcinoma patients with capsular invasion. World J Surg Oncol. 2025;23(1):190. doi:10.1186/s12957-025-03842-x
32. Yu M, Deng J, Gu Y, Lai Y. Preoperative high level of circulating tumor cells is an independent risk factor for central lymph node metastasis in papillary thyroid carcinoma with maximum lesion diameter ≤1.0 cm. Int J Gen Med. 2024;17:4907–4916. doi:10.2147/IJGM.S487992
33. Yu M, Deng J, Gu Y, Lai Y, Wang Y. Pretreatment level of circulating tumor cells is associated with lymph node metastasis in papillary thyroid carcinoma patients with ≤ 55 years old. World J Surg Oncol. 2025;23(1):29. doi:10.1186/s12957-025-03670-z
34. Liu Y, Yin Z, Wang Y, Chen H. Exploration and validation of key genes associated with early lymph node metastasis in thyroid carcinoma using weighted gene co-expression network analysis and machine learning. Front Endocrinol. 2023;14:1247709. doi:10.3389/fendo.2023.1247709
35. Li Z, Li F, Jiang X, et al. Hypoxia upregulate TPM4 expression to strengthen epithelial-mesenchymal transition that promotes lymph node metastasis of papillary thyroid cancer. J Cancer. 2025;16(10):3216–3234. doi:10.7150/jca.116524
36. Hu Y, Xu Z, Zhou D, et al. CXCR4 promotes migration, invasion, and epithelial-mesenchymal transition of papillary thyroid carcinoma by activating STAT3 signaling pathway. J Cancer Res Ther. 2024;20(4):1241–1250. doi:10.4103/jcrt.jcrt_2395_22
37. Leong SP, Witte MH. Cancer metastasis through the lymphatic versus blood vessels. Clin Exp Metastasis. 2024;41(4):387–402. doi:10.1007/s10585-024-10288-0
38. Yu HW, Park E, Lee JK, et al. Analyzing circulating tumor cells and epithelial-mesenchymal transition status of papillary thyroid carcinoma patients following thyroidectomy: a prospective cohort study. Int J Surg. 2024;110(6):3357–3364. doi:10.1097/JS9.000000000000128
39. Li D, Li N, Ding Y. Epithelial-to-mesenchymal transition of circulating tumor cells and CD133 expression on predicting prognosis of thyroid cancer patients. Mol Clin Oncol. 2022;17(3):141. doi:10.3892/mco.2022.2574
40. Aceto N, Bardia A, Miyamoto DT, et al. Circulating tumor cell clusters are oligoclonal precursors of breast cancer metastasis. Cell. 2014;158(5):1110–1122. doi:10.1016/j.cell.2014.07.013
41. Wang XJ, Zheng HT, Xu J, et al. LINC00106 prevents against metastasis of thyroid cancer by inhibiting epithelial-mesenchymal transition. Eur Rev Med Pharmacol Sci. 2020;24(19):10015–10021. doi:10.26355/eurrev_202010_23215
42. Ye D, Jiang Y, Sun Y, et al. METTL7B promotes migration and invasion in thyroid cancer through epithelial-mesenchymal transition. J Mol Endocrinol. 2019;63(1):51–61. doi:10.1530/JME-18-0261
43. Xu S, Mo C, Lin J, et al. Loss of ID3 drives papillary thyroid cancer metastasis by targeting E47-mediated epithelial to mesenchymal transition. Cell Death Discov. 2021;7(1):226. doi:10.1038/s41420-021-00614-w
44. Gautam D, Clarke EM, Roweth HG, Smith MR, Battinelli EM. Platelets and circulating (tumor) cells: partners in promoting metastatic cancer. Curr Opin Hematol. 2025;32(1):52–60. doi:10.1097/MOH.0000000000000852
45. Matanes E, Gotlieb WH. Pathophysiological and anatomical basis of lymphatic transit of cancer cells and role of the lymphatic system: a review of published literature. Chin Clin Oncol. 2021;10(2):14. doi:10.21037/cco-20-205
46. Zhou X, Zhang M, Jin L, et al. Quantitative analysis of contrast-enhanced ultrasound combined with ultrasound in the unifocal papillary thyroid micro-carcinoma. Med Eng Phys. 2022;110:103840. doi:10.1016/j.medengphy.2022.103840
47. Dell’Aquila M, Granitto A, Martini M, et al. PD-L1 and thyroid cytology: a possible diagnostic and prognostic marker. Cancer Cytopathol. 2020;128(3):177–189. doi:10.1002/cncy.22224
48. Pizzimenti C, Fiorentino V, Ieni A. BRAF-AXL-PD-L1 signaling axis as a possible biological marker for RAI treatment in the thyroid cancer ATA intermediate risk category. Int J Mol Sci. 2023;24(12):10024. doi:10.3390/ijms241210024
49. Dell’Aquila M, Musarra T, Fiorentino V, et al. Relevance of rosette patterns in variants of papillary thyroid carcinoma. Cytopathology. 2020;31(6):533–540. doi:10.1111/cyt.12885
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Younger Than 55 Years Old and BRAF V600E Mutation are Risk Factors for Lymph Node Metastasis in Papillary Thyroid Carcinomas ≤1.0 cm but Not in >1.0 cm
Lai Y, Gu Y, Yu M, Deng J
International Journal of General Medicine 2023, 16:1403-1414
Published Date: 19 April 2023
Preoperative High Level of Circulating Tumor Cells is an Independent Risk Factor for Central Lymph Node Metastasis in Papillary Thyroid Carcinoma with Maximum Lesion Diameter ≤1.0 cm
Yu M, Deng J, Gu Y, Lai Y
International Journal of General Medicine 2024, 17:4907-4916
Published Date: 25 October 2024
Risk Stratification in Papillary Thyroid Microcarcinoma: Clinical Features Predicting Multifocality, Lymph Node Metastasis, and Recurrence – A Retrospective Cohort Study
Hsu CC, Tsai CY, Lin LC, Wang SY, Yeh CN, Liou MJ, Chen ST
Cancer Management and Research 2026, 18:572526
Published Date: 9 January 2026