Back to Journals » Patient Preference and Adherence » Volume 16
Risk of Severe COVID-19 in Non-Adherent OSA Patients
Authors Genzor S ![]() , Prasko J
, Prasko J ![]() , Mizera J
, Mizera J ![]() , Jakubec P, Sova M
, Jakubec P, Sova M ![]() , Vanek J
, Vanek J ![]() , Šurinová N
, Šurinová N ![]() , Langova K
, Langova K
Received 26 August 2022
Accepted for publication 26 October 2022
Published 9 November 2022 Volume 2022:16 Pages 3069—3079
DOI https://doi.org/10.2147/PPA.S387657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Samuel Genzor,1,* Jan Prasko,2– 4,* Jan Mizera,1,* Petr Jakubec,1,* Milan Sova,1,5,* Jakub Vanek,2,* Nikoleta Šurinová,6,* Katerina Langova7,*
1Department of Respiratory Medicine, Faculty of Medicine and Dentistry, Palacky University Olomouc and University Hospital Olomouc, Olomouc Czech Republic; 2Department of Psychiatry, University Hospital Olomouc and Faculty of Medicine and Dentistry, Palacky University Olomouc, Olomouc Czech Republic; 3Institute for Postgraduate Education in Health Care, Prague Czech Republic; 4Department of Psychology Sciences, Faculty of Social Science and Health Care, Constantine the Philosopher University in Nitra, Nitra The Slovak Republic; 5Department of Respiratory Medicine, Faculty of Medicine and Dentistry, Masaryk University Brno and University Hospital Brno, Brno Czech Republic; 6Palacky University Olomouc, Olomouc Czech Republic; 7Department of Biophysics, Palacky University Olomouc, Olomouc Czech Republic
*These authors contributed equally to this work
Correspondence: Jan Prasko, Department of Psychiatry, Faculty of Medicine and Dentistry, University Hospital Olomouc, I. P. Pavlova 6, Olomouc, 775 20, Czech Republic, Email [email protected]
Background: Patients with obstructive sleep apnoea (OSA) are at increased risk of severe course of COVID-19. Vaccination remains to be the most effective prevention of complicated courses of infection. The best contemporary conservative treatment of OSA is continuous positive airway pressure (CPAP) therapy.
Purpose: To compare vaccination acceptance and outcomes of COVID-19 infection between OSA patients adhering to the CPAP therapy and those who rejected CPAP and surgical therapy.
Patients and Methods: Subjects were divided into two groups: group A (N = 167) were individuals with sufficient CPAP adherence (more than 4 hours per night on average) over the last 10 years. Group B (N = 106) were individuals who did not use the CPAP therapy at all and had no indications to surgical therapy.
Results: Three patients in group B died, and one had a severe course of COVID-19. None of the patients in group A died or experienced a severe course of COVID-19. Group A had a significantly higher proportion of males (77.8% compared to 66% in group B) and all parameters of OSA severity. The vaccination status was similar among both groups, with a complete triple dose vaccination rate of 69.5% and 67.9% in groups A and B, respectively.
Conclusion: The results show that the patients with OSA adherent to CPAP therapy were less likely to experience a severe course of COVID-19 or death than the OSA patients non-compliant with therapy, despite the former group having more severe OSA. This result underlines the importance of adherence to CPAP therapy in OSA.
Keywords: OSA, COVID-19, vaccination, treatment with CPAP, CPAP adherence
Introduction
Sleep is a natural and important part of our lives. The average person spends approximately one-third of their life asleep. Therefore, the quality and the amount of sleep are very important.1 Sleep disordered breathing (OSA) greatly impacts the overall health condition in affected individuals. The interconnection of OSA with cardiovascular diseases is well described.2,3 OSA decreases the individual’s quality of life and decreases life expectancy. There is increasing evidence that OSA might be an independent risk factor for the complicated course of respiratory infections, including COVID-19.4,5
Vaccination is the most effective prevention of the severe course of COVID-19 (even in mutated strains of SARS-CoV-2).6,7 The acceptance of vaccination recommendations differs among various patient groups, and most developed countries reached vaccination coverage of over 70%.6 Generally, it seems reasonable to expect better vaccination acceptance in individuals with proper adherence to health care in other areas.
Left untreated, OSA carries an amplified risk of possibly life-threatening illnesses. It has been suggested that it is connected to hypertension, heart rhythm disorders, ischemic heart disease, stroke, road traffic accidents, and premature death.8–16
Positive airway pressure (PAP) therapy remains the standard treatment in OSA, especially in moderate to severe sleep apnoea syndrome patients.17 Reaching proper long-term compliance with positive airway pressure therapy is often problematic. In most studies, the average use of CPAP for more than 4 hours per night is considered sufficient. However, this amount of CPAP usage may only significantly affect symptoms of the OSA, with even better CPAP adherence (up to 6 hours per night) needed to reduce cardiovascular morbidity and mortality.18–22
The COVID pandemic has changed every part of our lives. There is clear evidence that it also changed the behaviour of the patients, including patients with CPAP. Most studies found that in persons with proper CPAP adherence, its usage improved even more, and many individuals with previously insufficient CPAP use had improved their adherence.23,24
On the other hand, the data about the acceptance of vaccination in OSA patients are not available. In addition, the impact of CPAP adherence and vaccination on the risk of severe COVID courses is also unknown.
The study aimed to compare OSA patients adherent to CPAP therapy and OSA patients who refused any kind of therapy (CPAP, surgery, or other) with regards to:
- Their acceptance of vaccination against COVID-19.
- The severity of COVID-19 illness in those with a history of the infection.
- OSA severity (apnoea-hypopnoea index, t90 – percentage time of sleep spent under 90% of peripheral blood saturation, ODI (Oxygen Desaturation Index), average blood saturation.
- OSA symptoms (sleepiness measured by Epworth sleepiness scale; presence of microsleeps).
- Body mass index, demographics (sex, age).
- Presence of comorbidities.
Hypotheses were as follows:
- Patients with better CPAP compliance will also be more compliant with vaccination.
- Patients with more severe OSA problems at the beginning will be more compliant with CPAP.
- Patients who are uncooperative with CPAP will have a worse course of coronavirus disease (COVID-19).
- Patients with worse compliance will have more severe somatic complications/comorbidities related to OSA.
Methods
This study is prospective. Patients were enrolled from 2005 to 2012 and followed up for over ten years at routine visits.
Inclusion Criteria
- AHI> 10.
- Age 18–80.
Exclusion Criteria
- Contraindications for CPAP therapy.
- Indication to other therapy methods (BPAP, oxygen therapy, surgical therapy).
- Dominantly central apnoea aetiology.
- Use of drugs or substances connected with a high incidence of central apnoea (especially alcohol abuse and opioid medication).
- Conditions connected with a high incidence of central apnoea (especially recent brain stroke history and decompensated heart failure).
The Course of Study
A sleep monitoring was performed with respiratory sleep polygraphy (Stardust, Easyscreen); each recording lasted at least 6 hours and was evaluated by sleep laboratory technicians according to the current American Academy of Sleep Medicine scoring manual.25 At the initial examination, the patient’s medical history was taken. Daytime symptoms (ie, sleepiness and microsleeps presence) have been evaluated by the patients’ statements and Epworth sleepiness scale score. The optimum therapeutic pressure was titrated using automatic CPAP for at least three consecutive nights, during which the patient was hospitalized at the sleep laboratory. Subjects who agreed to use home CPAP therapy were further followed up. The first check-up was performed after three months of CPAP use. At this check-up, the effect of the CPAP therapy (measured by the residual AHI), the average CPAP use per night, and the Epworth sleepiness scale score were evaluated. Annual follow-up was performed routinely over ten years with the same objective measures as at the first check-up. Subjects with sufficient compliance over the last ten years (with average CPAP use for more than 4 hours or more) and residual AHI below 10% of pre-therapy values or below five at the first check-up were classified into group A. The subjects with a significant change in their weight were excluded as this may change the severity of OSAS and reduce or increase their risk of the COVID-19 course.
Subjects who refused the CPAP therapy at the beginning or shortly after the home therapy initiation were longitudinally observed (group B).
The COVID-19 infection and vaccination data were obtained from the national registry on Feb 1, 2022–Feb 7, 2022.
Post-Hoc Exclusion Criteria
A significant change in the body weight of the patient (more than 10% of the body weight at the therapy beginning).
Non-effectivity of CPAP therapy (residual AHI higher than 10% of pre-therapy values or higher than 5).
Technical problems with the CPAP therapy (especially problems with data collection or mask fit).
Insufficient CPAP compliance (less than 4 hours of CPAP use per average night).
Death of the subject during the follow-up for other cause than COVID-19 until FEB 1, 2022.
Statistical Analysis
Qualitative data were described using absolute numbers and relative frequency. The Shapiro–Wilk test was used to evaluate of normality of the distribution of the values. The differences between the study groups were evaluated using Fischer’s exact test. The differences between groups in ordinal data were evaluated using Mann–Whitney U-test. Shapiro–Wilks tests of normality showed that the quantitative data, except for circumferences (neck, waist, and waist/hips ratio), had a normal distribution. The Mann–Whitney test evaluated the parameters with non-normal distribution, and a two-tailed t-test evaluated the parameters with normal distribution. To identify the significant factors impacting the overall risk of severe COVID-19 was used logistic regression analysis by the Forward Stepwise method (Likelihood Ratio).
All tests were performed on the alpha level of 0.05. The statistical software used for the calculations was IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Ethical Approval
All procedures performed in studies involving human participants followed the ethical standards of the ethics committee of the Bavarian Medical Association (approval number: 08064) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The local Ethical Committee of the University Hospital Olomouc approved the study (ruling number EK 98/21, the date of issue Jun 7, 2021).
Results
From 2005 to 2012, our sleep laboratory consecutively examined 670 subjects suspected of sleep disordered breathing. Of those, 405 were diagnosed with sleep apnoea syndrome with an indication of CPAP therapy. In 278, CPAP therapy was initiated after the standard procedures mentioned. One hundred sixty-seven patients reached an average compliance level of 4 hours per night and were classified into group A. In group A the mean number of hours of CPAP use last year was 6.98 ± 1.41 per night (min 4.14, max 11.1). One hundred eleven subjects presented one or more exclusion or post-hoc criteria defined in the methods. Of those, 24 died of other causes than COVID-19 (20 of them even before the COVID-19 pandemic started). Forty-five subjects did not reach a sufficient compliance level, and eighteen subjects had low effectiveness of the CPAP therapy. Only a small number of patients presented other causes of exclusion (together, 24 subjects – were indicated for other therapy modes, eg, BPAP, surgical therapy, or significant change in body weight). These patients were not eligible for any study group. One hundred six rejected the therapy early or shortly after the home therapy initiation. This group is designated as group B.
More males were in group A (77.8% compared to 66% in group B). The age between the study groups did not differ significantly (64.7 ± 10.6 vs 65.9 ± 12.3); similarly, BMI was comparable between the groups (33.9 ± 6.1 vs 34.08 ± 7.0). In anthropometric parameters, only differences were found in the neck circumference, which was higher in the CPAP adherent group (43.6 ± 4.1 vs 42.0 ± 4.4; p < 0.01). There were more never-smokers in group A (60% vs 50.9%). All parameters of OSA severity (AHI, ODI, t90 and average saturation) were worse/more severe in group A at the beginning of the study.
Similarly, symptoms of OSA, especially the ESS level, were significantly higher in group A. However, the total number of comorbidities was higher in the non-adherent group. Notably, the presence of pulmonary fibrosis was significantly higher in the non-adherent group. We analyzed the documentation of our patients and found that subjects with pulmonary fibrosis may have poor CPAP tolerance, especially due to an increased tendency to cough.
All subjects with severe/critical COVID-19 disease history were in group B. From that, one person had severe covid and consequently got triple dose vaccination, two died from COVID-19 and had no vaccination at all, and one died despite having shortly after the second dose of anti-COVID-19 vaccine. At least one vaccine dose had a similar number of patients in both groups (87.4% in group A vs 82.1% in group B). In a single vaccine subpopulation, subjects exclusively used Johnson & Johnson vaccine. Of non-vaccinated subjects, 42.1% and 36.8% were infected by COVID-19 in the study period in groups A and B, respectively. In vaccinated subjects (at least one dose) were COVID-19 infection found in 29.9% and 26.3% in groups A and B, respectively. The proportion of infected persons was significantly lower in the vaccinated subjects (p = 0.001). The B group presented mainly with mild symptoms; only three subjects had moderate COVID-19 illness (after the triple-dose vaccination). After the statistical analysis, no significant differences were found in the number of vaccination doses between groups A and B. Similarly, there were no significant differences between the groups in the distribution of COVID severity grades, but when we compare only more severe cases, there the difference between the groups was observed. For full results, see Tables 1 and 2. At the time of evaluation, no subjects were proven to have reinfections by COVID-19.
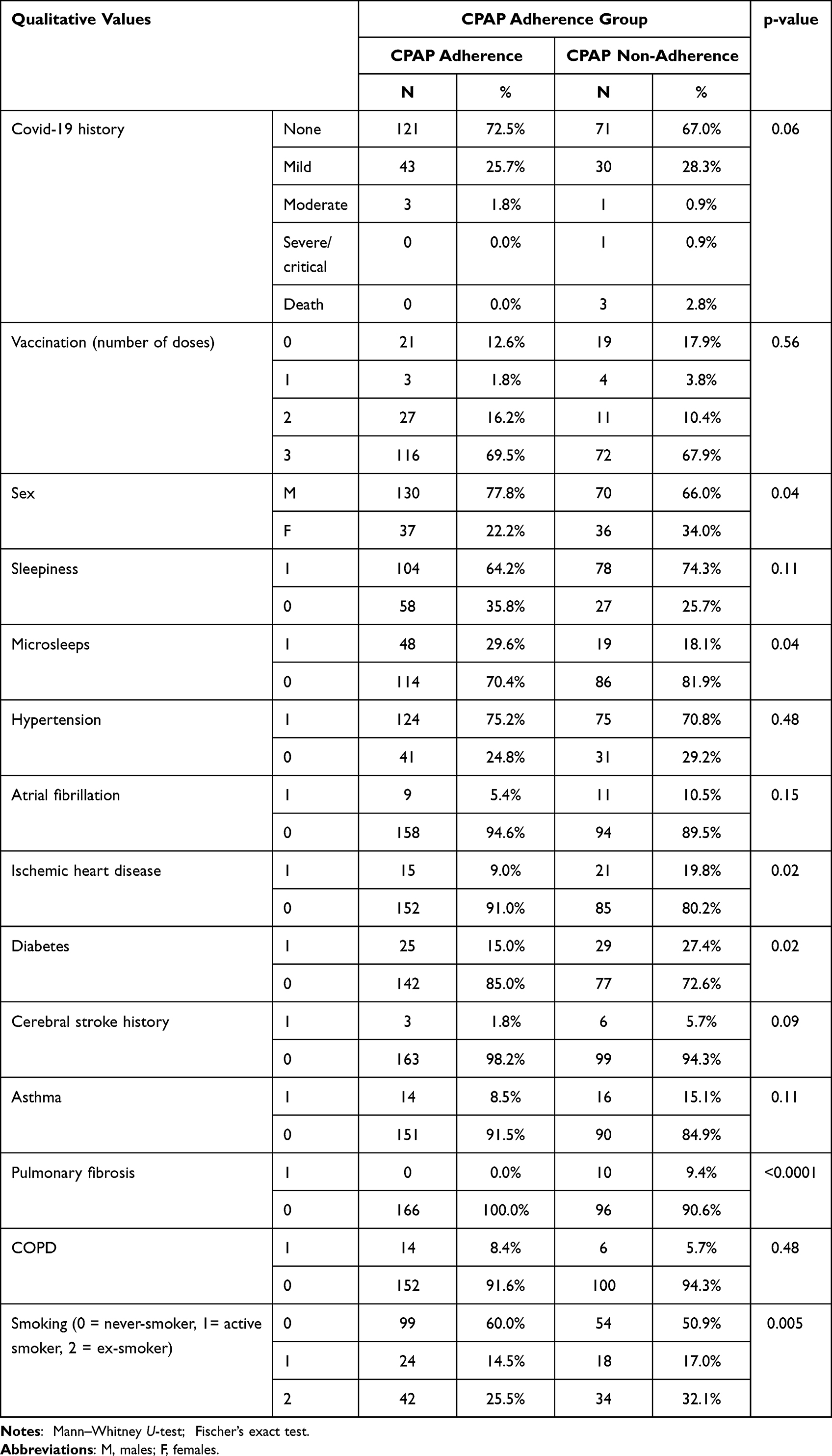 |
Table 1 Comparison of the CPAP Adherence Groups (Qualitative Parameters) |
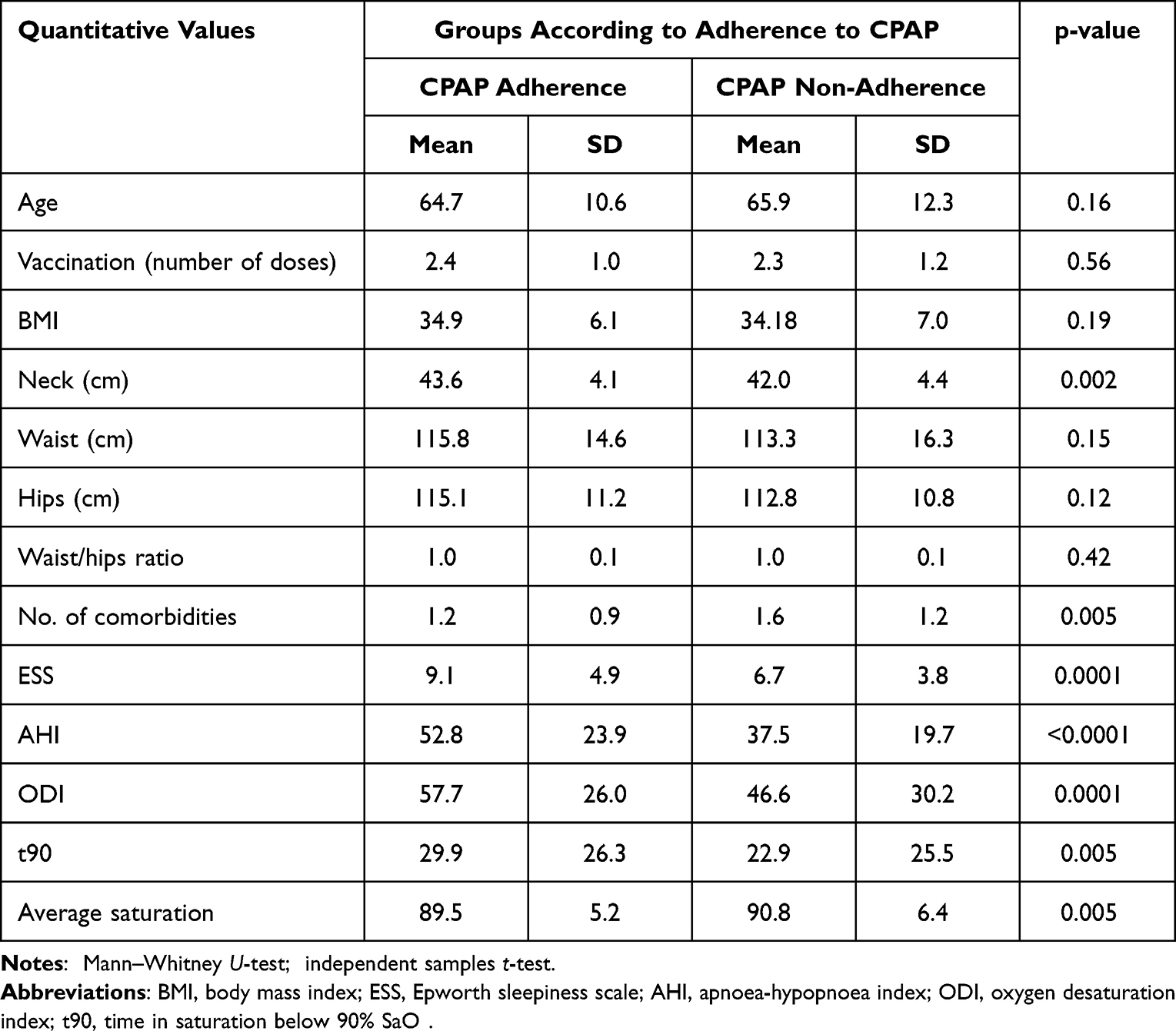 |
Table 2 Comparison of the CPAP Adherence Groups (Quantitative Parameters) |
When we compare the number of severe cases of COVID-19 between groups (in the CPAP-compliant group, no patient had a severe course, and none died, in the non-compliant CPAP group, four patients had a severe course and three of them died; Table 1), Fischer’s exact test shows a statistically significant difference between groups (p < 0.05). More exact characteristics of persons with severe or critical COVID-19 course and death are listed in Table 3.
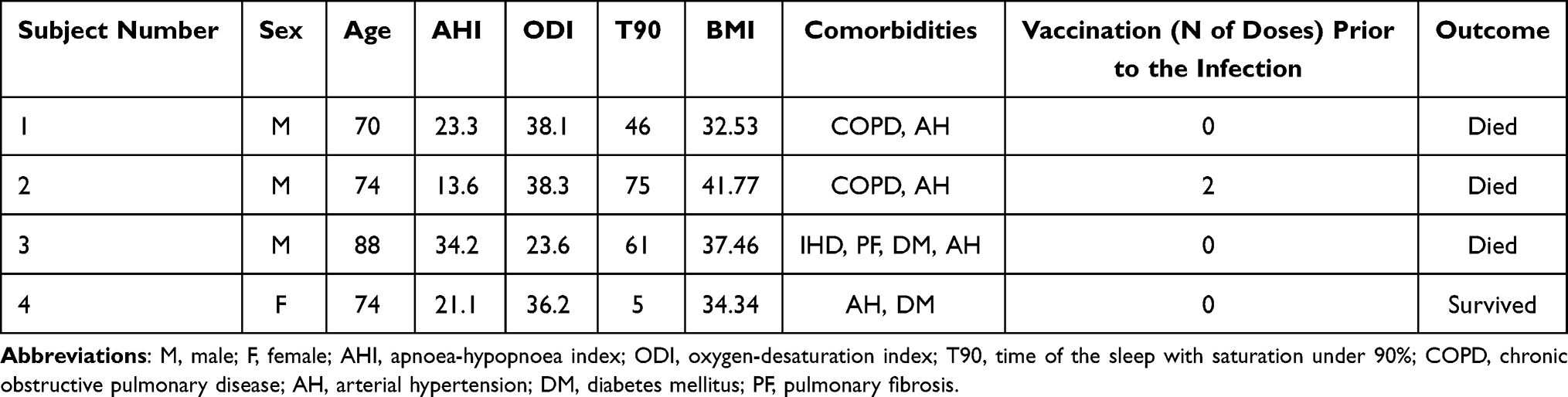 |
Table 3 Characteristics of Subjects with Severe COVID-19 Course and Death |
The adjusted odds-ratio (on BMI, age, sex, smoking status, number of vaccination doses and number of comorbidities) proved two other significant risk factors – number of vaccination doses (as a protective factor with OR of 0.454; 95% CI of 0.216–0.953) and comorbidities number (as a risk factor with OR of 2.701; 95% CI of 1.100–6.634) both with p < 0.05 (see Table 4).
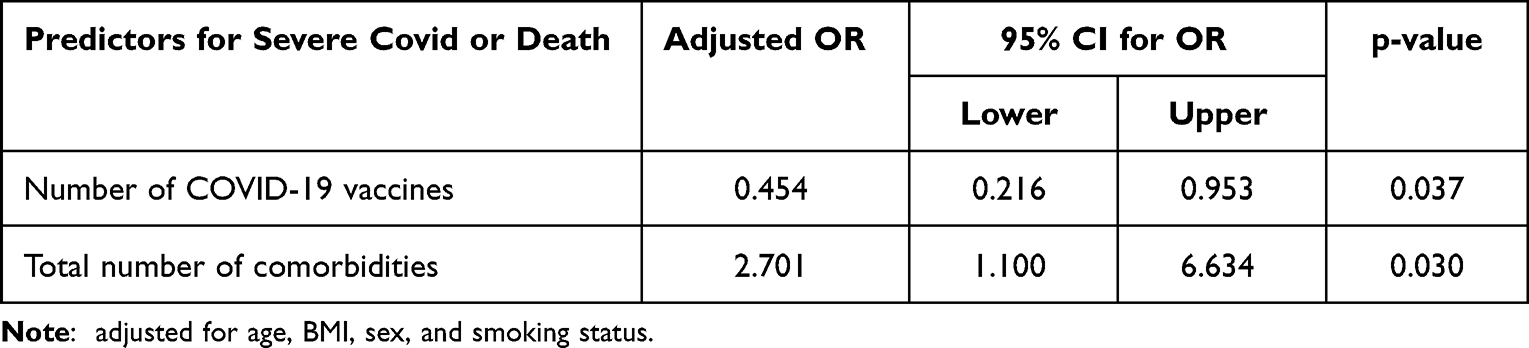 |
Table 4 Logistic Regression Analysis of Factors with Possible Impact on the COVID-19 Course |
Discussion
The first part of the discussion is divided into paragraphs answering the group differences from the Aims part.
- Are there differences between CPAP adherent and non-adherent patients’ acceptance of vaccination against COVID-19?
According to our results, it does not seem so. The acceptance of the triple-dose scheme in vaccination against COVID-19 was 69.5% in CPAP adherent subjects and 67.9% in CPAP refusing subjects. On the other side, we assume that the rate for this vaccination is better than overall adult anti-COVID-19 vaccination in the Czech Republic (64.3%) and World (61.4%). Most developed countries report a proportion of fully vaccinated persons above 70%.8 At least one dose of the vaccine was received by 87.4% and 82.1% of subjects in groups A and B, respectively. We are unaware of any study dealing with vaccination acceptance in SBD patients.
- Are there differences between CPAP adherent and non-adherent patients in the severity of COVID-19 cases in those with a history of infection?
We identified significant differences between groups A and B in COVID-19 severity when we compared the number of patients with severe clinical cases or death; there were significantly more patients with severe clinical presentation in the non-adherent group. Moreover, all severe cases were found in CPAP non-adherent group. However, the number of severe cases is not high, as only four subjects in all study groups had a severe case or died (ie, only 1.4% of all OSA subjects and 3.8% of CPAP non-adherent subjects). According to Maas et al.4 OSA relates to an increased risk of respiratory failure and severe COVID-19 in non-vaccinated persons (the odds ratio after adjusting to comorbidities and BMI was 1.98). However, our study group observed fewer severe outcomes than expected, given the high vaccination rate. After adjustment on probable risk factors (age, sex, smoking status, BMI, vaccination dose and the number of comorbidities) have been found two other factors have an impact on severe COVID-19 risk – the number of vaccination doses (as a protective factor) and the number of comorbidities (as a risk factor). As the number of patients with severe COVID-19 course was very small (and in group A none), the adjustment of the odds-ratio for adherence was not possible to perform.
- Are there differences between CPAP adherent and non-adherent patients in their OSA severity (AHI - apnoea-hypopnoea index, t90 – percentage time of sleep spent under 90% of peripheral blood saturation, ODI (Oxygen Desaturation Index), average blood saturation?
All measured OSA severity objective parameters were conclusive for more severe OSA in group A. Namely, mean AHI was 49.0 and 33.2 in group A and B, respectively (p < 0.0001); ODI was 54.90 vs 38.70 (p = 0.0001); t90 was 21.5% vs 9% (p = 0.0004) and average blood saturation was 91% in group A and 92% in group B (p = 0.005). This concurs with previous studies, which confirmed that more severe OSA patients tend to have better compliance.18,25,26 The higher severity of OSA in the CPAP adherent group observed in our study is not surprising.
- Are there differences between CPAP adherent and non-adherent patients in their OSA symptoms (sleepiness measured by Epworth sleepiness scale; presence of microsleeps)?
Similarly, as in the previous study question, we have confirmed dealing with the issue of CPAP adherence – that subjects with more profound symptoms of OSA have better compliance/adherence to the OSA. 29.9% of group A stated having microsleeps before the CPAP treatment, while only 18.1% stated the same in group B (p = 0.043). The score of the Epworth sleepiness scale was significantly higher in group A (mean of 8 points) compared to the mean of 6 points in group B (p = 0.0001). As confirmed by previous studies, sleepiness is a classical predictor of good adherence to CPAP therapy.18,26,27 On the other hand, some studies reported that sleepiness before the treatment did not influence compliance and, more importantly, an improvement of the symptoms after the therapy.28,29
- Are there differences between CPAP adherent and non-adherent patients’ body mass index (BMI) and demographics (sex, age)?
In our study, groups had no differences in BMI and age, and the proportion of males was significantly higher in group A than in group B (77.8% vs 66%; p < 0.05). Similarly, our previous study18 did not find any age and BMI predictors of adherence. However, some studies28,30 find BMI to predict better adherence to CPAP therapy. As AHI usually correlates quite strongly with BMI, this might be a bias of the mentioned studies, as the notion of better adherence to CPAP due to higher BMI seems counterintuitive.
- Are there differences between CPAP adherent and non-adherent patients in the presence of comorbidities?
A higher number of comorbidities was surprisingly found in group B. According to the recent literature, there is usually better adherence to the CPAP treatment in subjects with serious comorbidities. A post-hoc analysis of the SAVE study26 identified persons with more comorbidities as those with better adherence to the CPAP therapy (24-month follow-up of 1121 persons). The possible explanation may be the coexistence of more severe OSA parameters with higher BMI and comorbidities (ie, diabetes, hypertension, ischemic heart diseases, etc.). As our study group, A has more severe OSA and OSA symptoms, the presence of comorbidities is more common in group A. Interestingly, the presence of pulmonary fibrosis was significantly higher in a non-adherent group. The other studies focused primarily on CPAP tolerance in pulmonary fibrosis patients are unavailable. However, Papadogiannis et al31 found low PAP tolerance of the therapy in their study group of 29 OSA-IPF individuals (59% reached an acceptable level of adherence). However, the study above standardly used a humidifier to reduce the dry nocturnal cough. At the time of recruitment, our patients were humidifiers not widely available in our country. Therefore, we suppose their poor tolerance of the therapy might cause the high prevalence of fibrosis in the CPAP non-adherent group.
Limitations of the Study
The study has some limitations. Firstly, we performed only respiratory polygraphy to diagnose the obstructive sleep apnoea severity. On the other hand, this method is widely available, cheaper, and its results correlate with the findings on polysomnography. Secondly, the number of patients in both groups is quite small, which is probably why we did not find significant differences between the groups’ survival. The unicentric design of the study might also be considered a limitation. On the other side, all the patients have been consistently examined and followed up by the same study team. In future, we plan to perform a larger study with a multicentre design to confirm our findings. Additionally, the individuals with CPAP usage less than <4 hours (partially adherent) were excluded as their number was small to bring any relevant significant statistical analysis, and their involvement did not bring any new results (45 subjects did not reach a sufficient compliance level, and 18 subjects had low effectiveness of the CPAP therapy). However, this might also be considered as one of the limitations, and this subpopulation may also be interesting for further analysis.
We also did not study the subjects’ social background and education level, which may also play a role in the decision-making regarding vaccination. Sufficient compliance was evaluated as 4 hours of CPAP use or more, which is considered in the majority of studies as effective for reducing both sleepiness and cardiovascular risks in patients.32,33 However, no randomized controlled trial confirmed the mortality reduction in real life. This may be explained by the lack of matched controls in the clinical studies, as it is unethical not to treat symptomatic OSA patients.34
The main advantage of our study is a long-term observation of sufficient compliance in group A and observation of subjects refusing CPAP therapy for which they are indicated. We did not involve subjects with dominantly central aetiology of sleep apnoea.
The second part of the discussion is the responses to the hypotheses:
- Patients with better CPAP compliance will also be better compliant with vaccination.
This hypothesis is not confirmed. The percentage of vaccinated patients in both groups is not significantly different.
- Patients with more severe OSA problems will be more compliant with CPAP.
This hypothesis is confirmed. Our results agree with the outcomes of other studies.18,26,27,29
- Patients with better CPAP compliance will have a less severe course of COVID-19.
This hypothesis is confirmed. The CPAP non-adherent group has more patients with a severe and critical course of COVID-19. We did not find any study which systematically evaluates the effect of CPAP adherence and COVID-19 outcome.
- Patients with worse compliance will have more severe somatic complications/comorbidities in OSA.
This hypothesis is confirmed. The CPAP non-compliant group has significantly more comorbidities and a percentage of patients with pulmonary fibrosis, diabetes mellitus, and ischemic heart disease. We know that the presence of comorbid diseases is an important risk factor for the severe COVID-19 course. As listed in Table 3, subjects with severe course had several comorbidities – three had pulmonary disease (two had chronic obstructive pulmonary disease, and one had pulmonary fibrosis). One of them had arterial hypertension and diabetes mellitus. Also, the age of the persons with severe cases was above the average of the study group. On the other side, parameters of the OSA severity were lower, except for t90 in three of them. The subjects also had poor vaccination acceptance, as only one was vaccinated before the COVID-19 infection. Three of them were males, and one was female. We assume that all the listed factors might have added to the final unfavourable outcome – the absence of vaccination, the higher age, male sex, presence of comorbidities, and finally – sleep disordered breathing with no CPAP therapy.
Conclusion
All severe COVID-19 cases were identified in the group with poor compliance with the CPAP. Therefore, we postulate that CPAP adherence in OSA is very important in treating sleep-disordered breathing and may contribute to better outcomes in OSA patients. Our study showed that the severe and critical course of COVID-19 was more prevalent in OSA patients who were non-adherent to CPAP therapy than in OSA patients who were adherent to CPAP therapy. Achieving good acceptance of COVID-19 vaccination is extremely important in reducing the risk of severe COVID-19, especially in older patients and patients with comorbidities.
Abbreviations
AHI, apnoea-hypopnoea index; BMI, body mass index; ESS, Epworth sleepiness scale; ODI, oxygen desaturation index; OSAS, obstructive sleep apnoea; CPAP, continuous positive airway pressure.
Funding
Supported by Czech Health Research Council grant NU22-A-105.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ruan H, Xun P, Cai W, et al. Habitual sleep duration and risk of childhood obesity: systematic review and dose-response meta-analysis of prospective cohort studies. Sci Rep. 2015;2015;5:16160.
2. Garvey JF, Taylor CT, McNicholas WT. Cardiovascular disease in obstructive sleep apnoea syndrome: the role of intermittent hypoxia and inflammation. Eur Respir J. 2009;33(5):1195–1205. doi:10.1183/09031936.00111208
3. Lombardi C, Tobaldini E, Montano N, Losurdo A, Parati G. Obstructive Sleep Apnea Syndrome (OSAS) and cardiovascular system. Med Lav. 2017;108(4):276–282. doi:10.23749/mdl.v108i4.6427
4. Maas MB, Kim M, Malkani RG, et al. Obstructive sleep apnea and risk of COVID-19 infection, hospitalization and respiratory failure. Sleep Breath. 2021;25(2):1155–1157. doi:10.1007/s11325-020-02203-0
5. Mashaqi S, Lee-Iannotti J, Rangan P, et al. Obstructive sleep apnea and COVID-19 clinical outcomes during hospitalization: a cohort study. J Clin Sleep Med. 2021;17(11):2197–2204. doi:10.5664/jcsm.9424
6. Wang Q, Yang L, Jin H, Lin L. Vaccination against COVID-19: a systematic review and meta-analysis of acceptability and its predictors. Prev Med. 2021;150:106694. doi:10.1016/j.ypmed.2021
7. Fiolet T, Kherabi Y, MacDonald CJ, Ghosn J, Peiffer-Smadja N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: a narrative review. Clin Microbiol Infect. 2022;28(2):202–221. doi:10.1016/j.cmi.2021.10.005
8. Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006;3(3):34.
9. Pedrosa RP, Drager LF, Gonzaga CC, et al. Obstructive sleep apnea: the most common secondary cause of hypertension associated with resistant hypertension. Hypertension. 2011;58(5):811–817. doi:10.1161/HYPERTENSIONAHA.111.179788
10. Chami HA, Resnick HE, Quan SF, Gottlieb DJ. Association of incident cardiovascular disease with progression of sleep-disordered breathing. Circulation. 2011;123(12):1280–1286. doi:10.1161/CIRCULATIONAHA.110.974022
11. Martinez D, Klein C, Rahmeier L, et al. Sleep apnea is a stronger predictor of coronary heart disease than traditional risk factors. Sleep Breath. 2012;16(3):695–701. doi:10.1007/s11325-011-0559-0
12. Jaffe LM, Kjekshus J, Gottlieb SS. Importance and management of chronic sleep apnoea in cardiology. Eur Heart J. 2013;34(11):809–815. doi:10.1093/eurheartj/ehs046
13. Sova M, Sovova E, Hobzova M, Zapletalova J, Kamasova M, Kolek V. The effect of continuous positive airway pressure therapy on the prevalence of masked hypertension in obstructive sleep apnea patients. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015;159(2):277–282. doi:10.5507/bp.2014.063
14. Shahar E, Whitney CW, Redline S, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001;163(1):19–25. doi:10.1164/ajrccm.163.1.2001008
15. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep disordered breathing and hypertension. N Engl J Med. 2000;342(19):1178–1384. doi:10.1056/NEJM200005113421901
16. Han Q, Yeung SC, Ip MS, Mak JC. Cellular mechanisms in intermittent hypoxia-induced cardiac damage in vivo. J Physiol Biochem. 2014;70(1):201–213. doi:10.1007/s13105-013-0294-z
17. Batool-Anwar S, Goodwin JL, Kushida CA, et al. Impact of continuous positive airway pressure (CPAP) on quality of life in patients with obstructive sleep apnea (OSA). J Sleep Res. 2016;25(6):731–738. doi:10.1111/jsr.12430
18. Genzor S, Prasko J, Vanek J, Asswad AG, Nadjarpour S, Sova M. Adherence of obstructive sleep apnoea syndrome patients to positive airway pressure therapy - 10-year follow-up. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2021. doi:10.5507/bp.2021.041
19. Watach AJ, Hwang D, Sawyer AM. Personalized and patient-centered strategies to improve positive airway pressure adherence in patients with obstructive sleep apnea. Patient Prefer Adherence. 2021;15:1557–1570. doi:10.2147/PPA.S264927
20. Baratta F, Pastori D, Bucci T, et al. Long-term prediction of adherence to continuous positive air pressure therapy for the treatment of moderate/severe obstructive sleep apnea syndrome. Sleep Med. 2018;43:66–70. doi:10.1016/j.sleep.2017.09.032
21. Chai-Coetzer CL, Luo YM, Antic NA, et al. Predictors of long-term adherence to continuous positive airway pressure therapy in patients with obstructive sleep apnea and cardiovascular disease in the SAVE study. Sleep. 2013;36(12):1929–1937. doi:10.5665/sleep.3232
22. Lao M, Cheng Y, Gao X, Ou Q. The interaction among OSA, CPAP, and medications in patients with comorbid OSA and cardiovascular/cerebrovascular disease: a randomized controlled trial. BMC Pulm Med. 2022;22(1):99. doi:10.1186/s12890-022-01879-2
23. Demirovic S, Lusic Kalcina L, Pavlinac Dodig I, et al. The COVID-19 lockdown and CPAP adherence: the more vulnerable ones less likely to improve adherence? Nat Sci Sleep. 2021;13:1097–1108. doi:10.2147/NSS.S310257
24. Attias D, Pepin JL, Pathak A. Impact of COVID-19 lockdown on adherence to continuous positive airway pressure by obstructive sleep apnoea patients. Eur Respir J. 2020;56(1):2001607. doi:10.1183/13993003.01607-2020
25. AASM. American Academy of Sleep Medicine, diagnostic and scoring manual, version 2.6.; 2020.
26. Van Ryswyk E, Anderson CS, Antic NA, et al. Predictors of long-term adherence to continuous positive airway pressure in patients with obstructive sleep apnea and cardiovascular disease. Sleep. 2019;42(10):152. doi:10.1093/sleep/zsz152
27. Dzierzewski JM, Wallace DM, Wohlgemuth WK. Adherence to continuous positive airway pressure in existing users: self-efficacy enhances the association between continuous positive airway pressure and adherence. J Clin Sleep Med. 2016;12(2):169–176. doi:10.5664/jcsm.5478
28. Gagnadoux F, Le Vaillant M, Goupil F, et al. Influence of marital status and employment status on long-term adherence with continuous positive airway pressure in sleep apnea patients. PLoS One. 2011;6(8):e22503. doi:10.1371/journal.pone.0022503
29. Campbell A, Neill A, Lory R. Ethnicity and socioeconomic status predict initial continuous positive airway pressure compliance in New Zealand adults with obstructive sleep apnoea. Intern Med J. 2012;42(6):e95–101. doi:10.1111/j.1445-5994.2010.02360.x
30. Inoue A, Chiba S, Matsuura K, Osafune H, Capasso R, Wada K. Nasal function and CPAP compliance. Auris Nasus Larynx. 2019;46(4):548–558. doi:10.1016/j.anl.2018.11.006
31. Papadogiannis G, Bouloukaki I, Mermigkis C, et al. Patients with idiopathic pulmonary fibrosis with and without obstructive sleep apnea: differences in clinical characteristics, clinical outcomes, and the effect of PAP treatment. J Clin Sleep Med. 2021;17(3):533–544. doi:10.5664/jcsm.8932
32. Weaver TE, Maislin G, Dinges DF, et al. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep. 2007;30(6):711–719. doi:10.1093/sleep/30.6.711
33. Barbé F, Durán-Cantolla J, Sánchez-de-la-Torre M, et al. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: a randomized controlled trial. JAMA. 2012;307(20):2161–2168. doi:10.1001/jama.2012.4366
34. Pack AI, Magalang UJ, Singh B, Kuna ST, Keenan BT, Maislin G. Randomized clinical trials of cardiovascular disease in obstructive sleep apnea: understanding and overcoming bias. sleep. 2021;44(2):zsaa229. doi:10.1093/sleep/zsaa229
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Why Does COVID-19 Vaccine Acceptance Rate Remain Low Among Patients with Chronic Diseases? Evidences from Public Hospitals of Ethiopia
Daba C, Asefa L, Lemma H, Atamo A, Kebede E, Gebrehiwot M
Patient Preference and Adherence 2022, 16:1371-1380
Published Date: 27 May 2022
Effects of Obstructive Sleep Apnea on SARS-CoV-2 Antibody Response After Vaccination Against COVID-19 in Older Adults
Tufik S, Andersen ML, Rosa DS, Tufik SB, Pires GN
Nature and Science of Sleep 2022, 14:1203-1211
Published Date: 28 June 2022
Determinant Factors of COVID-19 Vaccine Hesitancy Among Adult and Elderly Population in Central Java, Indonesia
Utami A, Margawati A, Pramono D, Nugraheni A, Pramudo SG
Patient Preference and Adherence 2022, 16:1559-1570
Published Date: 28 June 2022
New Onset of Severe Plaque Psoriasis Following COVID-19 Vaccination: A Case Report
Hu YQ, Zhang JZ, Zhao Y
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1485-1487
Published Date: 2 August 2022
Factors Associated with the Acceptance of COVID-19 Vaccines in Citizens of Northern Peru: Cross-Sectional Study

Yupari-Azabache IL, Díaz-Ortega JL, Bardales-Aguirre LB, Barros-Sevillano S, Paredes-Díaz SE
Risk Management and Healthcare Policy 2022, 15:1705-1715
Published Date: 9 September 2022