Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Risk Factors of Readmission Within 90 Days for Chronic Obstructive Pulmonary Disease Patients with Frailty and Construction of an Early Warning Model
Authors Li J, Ma X, Zeng X, Zhou C, Zhu T
Received 16 December 2022
Accepted for publication 13 May 2023
Published 23 May 2023 Volume 2023:18 Pages 975—984
DOI https://doi.org/10.2147/COPD.S400638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jiaying Li,1,* Xiuqin Ma,1,* Xuetao Zeng,1,2 Chen Zhou,1 Taofeng Zhu1
1Department of Respiratory and Critical Care Medicine, The Yixing Hospital Affiliated to Jiangsu University, Yixing, Jiangsu, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, The Affiliated Hospital to Jiangnan University, Wuxi, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Taofeng Zhu, Department of Respiratory and Critical Care Medicine, The Yixing Hospital Affiliated to Jiangsu University, No. 75 Tongzhenguan Road, Yixing, Jiangsu, 214200, People’s Republic of China, Tel +86-510-879210911, Fax +86-510-87921110, Email [email protected]
Objective: This study aimed to explore the risk factors for readmission within 90 d in Chronic Obstructive Pulmonary Disease (COPD) patients with frailty and construct a clinical warning model.
Methods: COPD patients with frailty hospitalized in the Department of Respiratory and Critical Care Medicine of Yixing Hospital, Affiliated to Jiangsu University, were retrospectively collected from January 1, 2020, to June 30, 2022. Patients were divided into readmission and control groups according to readmission within 90 d. The clinical data of the two groups were evaluated by univariate and multivariate logistic regression analyses to identify readmission risk factors within 90 d in COPD patients with frailty. Then, a risk quantitative early warning model was constructed. Finally, the model’s prediction efficiency was evaluated, and external verification was carried out.
Results: The multivariate logistic regression analysis showed that BMI, number of hospitalizations in the past year ≥ 2, CCI, REFS, and 4MGS were independent risk factors for readmission within 90 d in COPD patients with frailty. The early warning model for these patients was established as follows: Logit (p) = − 1.896 + (− 0.166 × BMI) + (0.969 × number of hospitalizations in the past year ≥ 2) + (0.265 × CCI) + (0.405 × REFS) + (− 3.209 × 4MGS), and presented an area under the ROC curve (AUC) of 0.744 [95% CI: 0.687– 0.801]. The AUC of the external validation cohort was 0.737 (95% CI: 0.648– 0.826), and the AUC of the LACE warning model was 0.657 (95% CI:0.552– 0.762).
Conclusion: The BMI, number of hospitalizations in the past year ≥ 2, CCI, REFS, and 4MGS were independent risk factors for readmission within 90 d in COPD patients with frailty. The early warning model presented a moderate predictive value for assessing the risk of readmission within 90 d in these patients.
Keywords: chronic obstructive pulmonary disease, frailty, readmission, risk factors, warning model
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is characterized by high morbidity and mortality. The incidence of COPD in people over 60 has reached 27%1,2 and has become the world’s third leading cause of death.3 The risk of frailty in COPD patients is twice as high as in non-COPD patients due to aging, smoking, neuroendocrine dysfunction, immune system dysfunction, and chronic inflammation,4,5 and has a proportion of 9–28% in COPD patients.6 Additionally, COPD patients with frailty usually have a higher risk of adverse events, such as acute exacerbation, readmission, falls, disability, and even death.4,5
Frequent acute exacerbation of COPD might promote disease progression, increase the risk of readmission and death, and severely impair the quality of life of patients.7 The readmission rate of COPD patients within 90 d is about 17.5–39%.8,9 Moreover, the in-hospital mortality is higher in COPD patients readmitted within 90 d than in those not (13.4 vs 2.3%).10 Frailty is an independent risk factor for short-term readmission in COPD patients, increasing the risk of acute exacerbation and hospitalization.7
Studies on COPD with frailty are urgently required since the risk of acute exacerbation, readmission, and death in these patients has significantly increased. However, no early warning model for readmission within 90 d in COPD patients with frailty is currently available. Therefore, in the present study, we explored the risk factors of readmission within 90 d in COPD patients with frailty through case-control studies. Then, we constructed a risk quantitative early warning model suitable for clinical practice and conducted external verification. Our current findings might help clinicians identify high-risk groups, carry out early intervention and treatment, and reduce the risk of readmission in these high-risk COPD patients.
Methods
Study Design
This study was conducted in the Department of Respiratory and Critical Care Medicine of Yixing Hospital, Affiliated to Jiangsu University, from January 1, 2020, to June 30, 2022. We enrolled COPD patients with frailty and collected demographic information, laboratory test results, modified British Medical Research Council questionnaire (mMRC), chronic obstructive pulmonary disease assessment test (CAT), Charlson Comorbidity Index (CCI), and The Reported Edmonton Frail Scale (REFS) for comparative analysis.
This study followed the Helsinki Declaration and was approved by the Ethics Committee of Yixing Hospital, Affiliated to Jiangsu University (Batch No. 2022 wen 082). All participants signed the informed consent.
Study Subjects
The development cohort included COPD patients with frailty hospitalized in the Department of Respiratory and Critical Care Medicine of Yixing Hospital, Affiliated to Jiangsu University, from January 1, 2020, to September 30, 2021. The external validation cohort included COPD patients with frailty enrolled from October 1, 2021, to June 30, 2022. Patients were divided into readmission and control groups, whether they were readmitted within 90 d.
The inclusion criteria were:
- Compliance with the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) Guidelines (2019 Revision):11 Lung function test after inhalation of bronchodilators: forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) < 0.7;
- Conform to the assessment of frailty in elderly patients under acute care [12]: REFS scale score ≥ 8 points (frailty diagnosis);
- Readmission within 90 d: patients hospitalized with worsened recurrent symptoms within 90 d, such as dyspnea, cough, and sputum, and needed to be hospitalized again with systemic steroids and/or antibiotics.12
The exclusion criteria were:
- Significant cognitive impairment, unable to answer self-reported questions;
- Combined with other lung diseases such as asthma, active pulmonary tuberculosis, pulmonary embolism, and bronchiectasis;
- Patients who have not yet reached the discharge standard and require discharge;
- Patients with missing clinical data.
Research Tools
Data Collection
We collected general clinical data of all subjects, including gender, age, smoking status, body mass index (BMI), length of hospitalization, number of hospitalizations in the past year, comorbidities (hypertension, coronary heart disease, heart failure, stroke, diabetes, and tumor), and 4-meter gait speed (4MGS). We also collected laboratory examination data: white blood cell count (WBC), lymphocyte count, high-sensitivity c-reactive protein (hs-CRP), erythrocyte sedimentation rate (ESR), serum creatinine (Scr), fasting blood glucose; and data of each rating scale: modified British Medical Research Council questionnaire (mMRC),13 COPD assessment test (CAT) score,14 Charlson Comorbidity Index (CCI),15 and the Reported Edmonton Frailty Scale (REFS).16
REFS
Within 24 h before discharge, patients were assessed for frailty using the REFS. The REFS comprises nine parts: cognitive ability, general health status, social support, functional independence, drug use, emotional status, nutritional status, restraint, and self-reported performance. The highest score is 18 points; the higher the score, the more severe the weakness.
4MGS
The 4MGS test was conducted as follows: a flat route (4 m long) in the diseased area was selected and taped. The patient was required to walk in a straight line at normal speed, and a stopwatch was used to record the time to walk 4 m. Patients were asked to repeat the 4MGS test without rest. The fastest of the two times was recorded, and the 4MGS was calculated. Results are expressed as m/s. Patients could use their normal walkers, such as a cane or frame, and oxygen during measurements.
Blood Sample Collection and Testing
We collected 10–15 mL fasting venous blood within 24 h before discharge from all subjects and detected relevant serum indicators. White blood cell count (WBC) and lymphocyte, neutrophil, platelet, and eosinophil counts were detected using an automatic five-blood analyzer (Sysmex, Japan). The hs-CRP was detected using the immune turbidimetric method with a C-reactive protein detection kit (immune turbidimetric method) (Orion Diagnostica Oy). Serum creatinine (Scr), urea, total bilirubin, serum albumin (ALB), and fasting blood glucose were determined with an automatic biochemical analyzer (Siemens ADVIA 1200).
Readmission
The readmission data were obtained by summarizing the patient’s electronic case file. The researcher was unaware of the data during the previous hospitalization of subjects.
Statistical Analysis
The statistical analyses were performed using SPSS 27.0. Measurement data conforming to normal distribution are expressed as  and were compared using the t-test. Measurement data with non-normal distribution are expressed as medians and quartiles, and the Mann–Whitney U rank sum test was used to compare groups. Count data is expressed as cases (%) and were compared using the χ² or Fisher’s exact probability tests.
and were compared using the t-test. Measurement data with non-normal distribution are expressed as medians and quartiles, and the Mann–Whitney U rank sum test was used to compare groups. Count data is expressed as cases (%) and were compared using the χ² or Fisher’s exact probability tests.
The multivariate logistic regression analysis included variables with statistically significant differences in the univariate analysis. Selected risk factors were fitted to construct a readmission warning model, and the receiver operating characteristic (ROC) curve was used to evaluate the predictive efficacy of the model. Subjects were divided into high and low-risk groups according to the incidence cut-off p-value. Kaplan-Meier curves were used to compare the readmission rates of the two groups. Next, the external validation cohort data were substituted into the early warning model. The readmission within 90 d was the outcome variable, and the prediction probability was the test variable for ROC curve analysis. Then, we compared it with the ROC curve of LACE score.17
All curves were plotted using GraphPad Prism. A p < 0.05 was considered statistically significant.
Results
Subjects’ General Clinical Features
First, 323 COPD patients with frailty were included. However, 10 patients were excluded due to other lung diseases such as asthma, active pulmonary tuberculosis, interstitial lung disease, and pulmonary embolism, two due to significant cognitive deficits, and eight due to lack of clinical data. Finally, 303 patients were included in the development cohort. Patients were divided into readmission (104) and control (199) groups whether they were readmitted within 90 d of discharge (Figure 1).
 |
Figure 1 Flow diagram of patient selection. |
The clinical characteristics of COPD patients with frailty are shown in Table 1. The average age in the readmission and control groups was 78.04 ± 8.04 and 79.76 ± 7.50, and the proportion of males was 81.7% (85/104) and 77.9% (155/199), respectively. Smokers accounted for 11.5% (12/104) in the readmission group and 18.1% (36/199) in the control group.
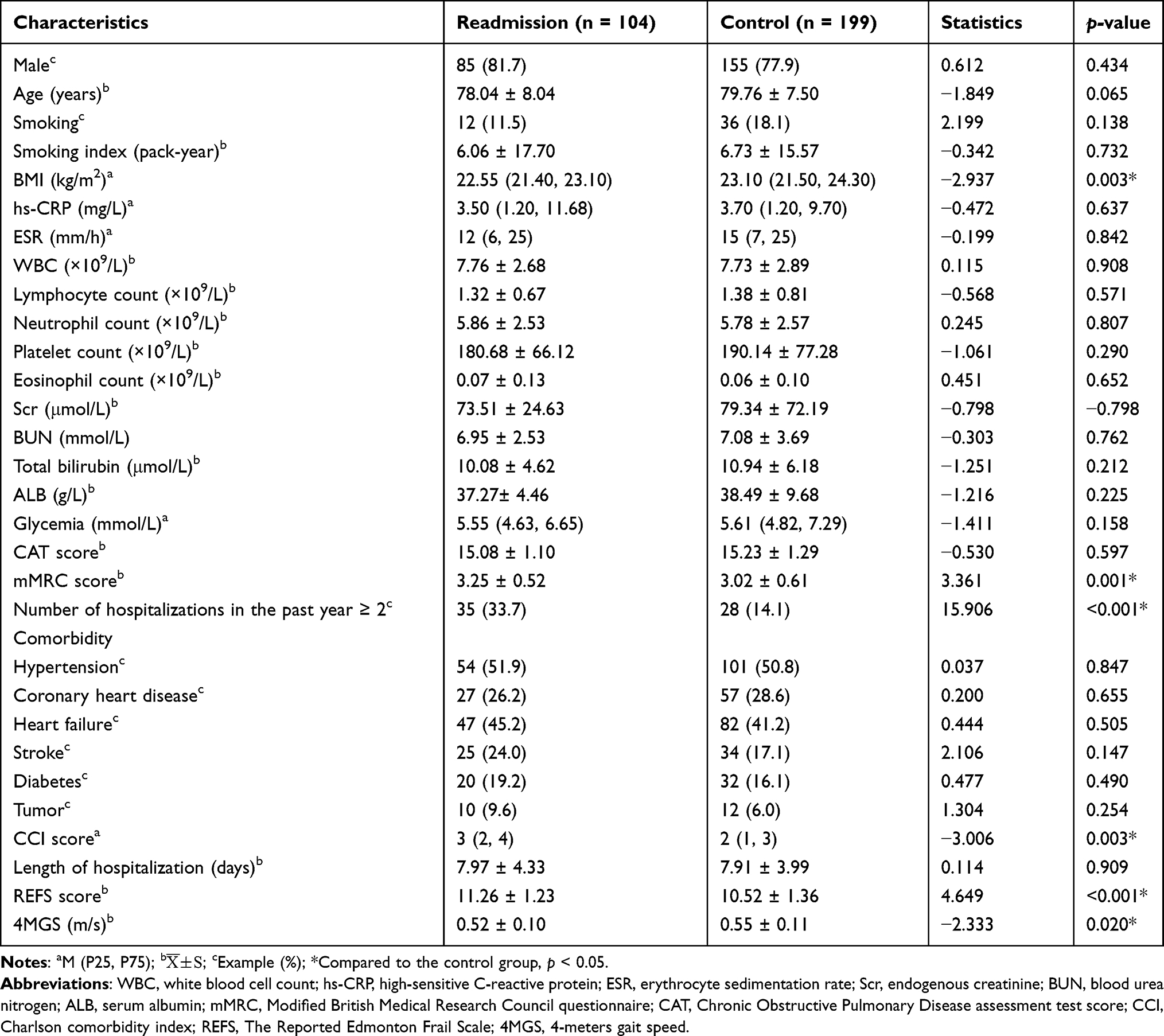 |
Table 1 General Data Comparisons Between Readmission and Control Groups |
Comparative Analysis of Clinical Data
The general clinical characteristics of the two groups are presented in Table 1. The readmission group presented higher mMRC and REFS, slower 4MGS, and a higher proportion of patients with more than two hospitalizations in the past year than the control group, as well as higher CCI and lower BMI (all p < 0.05). The other factors did not differ between the two groups (p > 0.05) (Table 1).
Multivariate Logistic Regression Analysis
The BMI, mMRC, number of hospitalizations in the past year ≥ 2, CCI, REFS score, and 4MGS were candidate predictors according to the univariate analysis. Then, the multivariate logistic regression analysis was performed, and the BMI [OR = 0.847, 95% confidence interval (CI): 0.737–0.973, p < 0.05], number of hospitalizations in the past year ≥ 2 (OR = 2.635, 95% CI: 1.422–4.884, p < 0.05), CCI (OR = 1.304, 95% CI: 1.069–1.589, p < 0.05), REFS score (OR = 1.500, 95% CI: 1.224–1.839, p < 0.05), and 4MGS (OR = 0.040, 95% CI: 0.003–0.564, p < 0.05) were identified as independent risk factors for readmission within 90 d in COPD patients with frailty (Table 2).
 |
Table 2 Multivariate Logistic Regression Analysis of Readmission Within 90 d in COPD Patients with Frailty |
Establishment of an Early Warning Model for Readmission Within 90 d in COPD Patients with Frailty
Based on the multivariate logistic regression analysis (Table 2), we constructed an early warning model for readmission within 90 d in COPD patients with frailty: Logit (p) = −1.896 + (−0.166 × BMI) + (0.969 × number of hospitalizations in the past year ≥ 2) + (0.265 × CCI) + (0.405 × REFS) + (−3.209 × 4MGS). This formula was then transformed to: p = 1/(1 + e − x); e: natural logarithm (~ 2.718); x = −1.896 + (−0.166 × BMI) + (0.969 × number of hospitalizations in the past year ≥ 2) + (0.265 × CCI) + (0.405 × REFS score) + (−3.209 × 4MGS). The AUC of this early warning model was 0.744 (95% CI: 0.687–0.801) (Figure 2). When the cut-off point was p = 0.335, the model sensitivity and specificity were 70.2 and 68.3%, respectively.
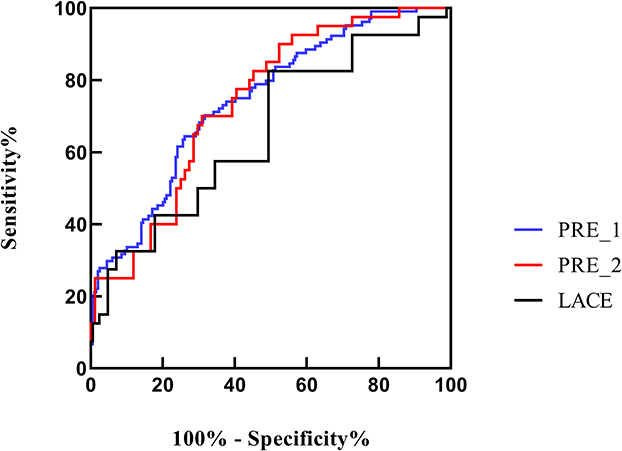 |
Figure 2 ROC curve of the early warning model (PRE_1), external validation cohort (PRE_2) and LACE warning model for predicting the readmission within 90 d in COPD patients with frailty. |
Furthermore, we determined the AUC of five variables (BMI, number of hospitalizations in the past year ≥ 2, CCI, REFS, and 4MGS) and the early warning model (PRE_1) to test their predictive value. The AUCs were: 0.603 [95% CI (0.540–0.666)], 0.598 [95% CI (0.528–0.667)], 0.602 [95% CI (0.535–0.669)], 0.648 [95% CI (0.585–0.710)], 0.577 [95% CI (0.511–0.643)], and 0.744 [95% CI (0.687–0.801)], respectively. Hence, the effectiveness of the early warning model was better than univariate diagnoses (Figures 2 and 3).
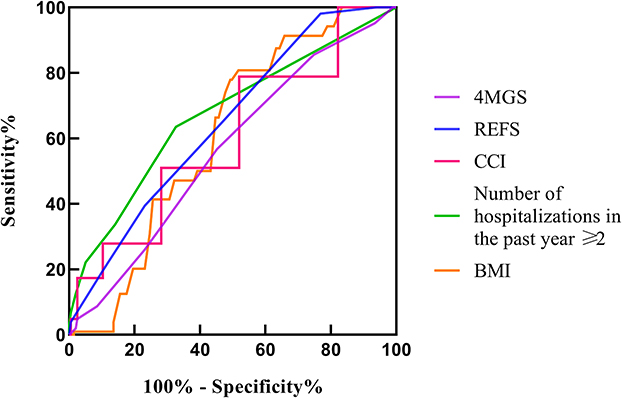 |
Figure 3 ROC curve of BMI, number of hospitalizations in the last year, CCI, REFS score, and 4MGS for predicting readmission within 90 d in COPD patients with frailty. |
Risk Stratification of Readmission Within 90 d
Next, we used the early warning model (PRE_1) to stratify patients based on the risk of readmission. Using a readmission rate cut-off p-value of 0.335, the 303 subjects were divided into high (n = 136) and low-risk (n = 167) groups. The median readmission time within 90 d in the high-risk group was 62.213 d (95% CI: 56.869–67.558), significantly shorter than the low-risk group [80.503 d (95% CI: 77.103–83.903)] (χ2 = 42.210, p < 0.01) (Figure 4).
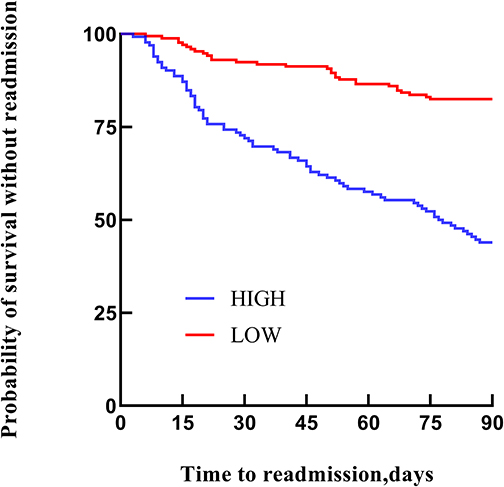 |
Figure 4 Comparison of readmission time within 90 d between high and low-risk groups. |
External Validation
The minimum sample size for external validation was 96 cases, according to Medcalc. A total of 124 cases were included in the external validation cohort, and their data were incorporated into the early warning model (PRE_1). The readmission within 90 d of COPD patients with frailty was the outcome variable, and the prediction probability was the test variable in the ROC curve analysis (PRE_2) (Figure 2). The AUC for the external validation cohort was 0.737 (95% CI: 0.648–0.826). When the cut-off point was 0.335, the sensitivity and specificity were 70% and 69%, respectively.
We substituted the external validation cohort data into the LACE warning model. The AUC for the LACE warning model was 0.657 (95% CI: 0.552–0.762), and the sensitivity and specificity were 32.5% and 91.7%, respectively (Figure 2). The predictive value of the early warning model (PRE_1) for the risk of readmission within 90 days in COPD patients with frailty was better than that of the traditional LACE warning model.
Discussion
Herein, we conducted a case-control study and found that the BMI, number of hospitalizations in the past year ≥ 2, CCI, REFS, and 4MGS were independent risk factors for readmission within 90 d in COPD patients with frailty. Then, we established an early warning model with moderate value for assessing this readmission risk. Current studies have shown that the readmission rate of COPD patients within 90 d is about 17.5–39%,8,9 consistent with our findings (34.32%).
The BMI indicates the nutritional status and has been closely related to the risk of acute exacerbation and death in COPD patients.18,19 Patients with low BMI have a higher probability of diaphragmatic weakness, decreased lung function, and other comorbidities (cardiovascular disease, osteoporosis, and depression). Meanwhile, malnutrition might also lead to poor exercise capacity in COPD patients, impairing skeletal muscle capacity.12 Patients with low BMI have poor nutritional status and are more susceptible to infections, which might lead to frequent acute exacerbation of COPD.20 Hence, the combined effects of these factors can increase the risk of readmission within 90 d in patients with low BMI.
Zhang et al found that COPD patients with acute exacerbation had a 3.891 times more chance of readmission if they had more than two hospitalizations in the past year compared to those with less than two.21 Our current results showed that the risk of readmission within 90 d increased by 2.635 times in COPD patients with frailty hospitalized more than two times in the past year. This result might be because frequent acute exacerbation of COPD patients puts the body in a chronic inflammatory state for a long time, resulting in rapid deterioration of lung function and reducing the quality of life, which increases the risk of acute exacerbation readmission and leads to increased mortality.
A large-scale epidemiological study in Europe showed that the CCI is closely related to acute exacerbation and death of COPD patients. When the CCI was > 4 points, the mortality rate of COPD patients increased by 2.89 times.22 P Luu et al also found that the risk of acute exacerbation significantly increased in COPD patients with higher CCI.23 These results are consistent with our findings that the risk of readmission will increase by 1.304 times for every CCI point increase. COPD patients with frailty usually have other comorbidities and are in a high-burden state, increasing the risk of acute exacerbation, hospitalization, and death.24
Various studies have shown that frailty is an independent predictor of short-term readmission in COPD patients. The readmission rate increases with frailty severity. The possibility of readmission in patients with severe frailty is about five times more than in patients with mild to moderate frailty.8,25 This result is consistent with our findings that for every REFS score point increase, the risk of readmission increases by 1.5 times. Additionally, the 4MGS is an alternative marker of frailty and can independently predict short-term readmission risk in hospitalized COPD patients,26,27 which was supported by our current findings.
Studies have shown that the C-statistic of LACE index predicting 90-day readmission is 0.65, which is similar to our research.28 Compared with the conventional LACE warning model, the prediction accuracy of our prediction model is higher. Probably because our warning model adds the REFS score, which is more suitable for patients with COPD and frailty, and can provide a new method for screening patients with COPD and frailty at high risk of 90-day readmission.
Furthermore, we successfully constructed a new early warning model, presenting an AUC of 0.744, a sensitivity of 70.2%, and a specificity of 68.3%. The external validation showed that the model had moderate clinical predictive value. Then, we used the early warning model to stratify patients into high and low-risk groups. The median readmission time of patients in the high-risk group was significantly shorter than that in the low-risk group. Thus, we believe this model provides a basis for the early identification of COPD patients at high risk of readmission.
Study Limitations
Our current research also has some limitations. First, we conducted a single-center retrospective case-control study with a small sample size. Second, limited by retrospective design, some important clinical data (such as 6-minute walk test, home non-invasive oxygen therapy use, pneumonia vaccination status, and socioeconomic status) were not collected. Third, because some patients had severe frailty and could not cooperate with lung function tests, this early warning model does not include lung function data, which might affect the results. Fourth, some other confounding factors of frequent acute exacerbations were not included in the analysis, such as type, dose, and duration of combined antibiotics and anti-asthmatic drugs, which might also impact the accuracy of our results. Therefore, further prospective studies with large sample sizes are needed to improve our findings.
Conclusion
The BMI, number of hospitalizations in the past year ≥ 2, CCI, REFS, and 4MGS were risk factors for readmission within 90 d in COPD patients with frailty. The early warning model presented moderate predictive value for the risk of readmission within 90 d in these patients. All indicators in the early warning model are readily available in the clinic. Therefore, this model might help clinicians identify patients at high risk of readmission for early intervention and treatment.
Abbreviations
COPD, Chronic Obstructive Pulmonary Disease; mMRC, Modified British Medical Research Council questionnaire; CAT, Chronic Obstructive Pulmonary Disease assessment test score; CCI, Charlson comorbidity index; REFS, The Reported Edmonton Frail Scale; FEV1, first second forced expiratory volume; FVC, forced vital capacity; BMI, Body mass index; 4MGS, 4 meters gait speed; WBC, white blood cell count; hs-CRP, high-sensitive C-reactive protein; ESR, erythrocyte sedimentation rate; Scr: endogenous creatinine; BUN, blood urea nitrogen; ALB, serum albumin; ROC curve, receiver operating characteristic curve; AUC, area under the curve.
Data Sharing Statement
The dataset in this study can be obtained with the corresponding author under reasonable requirements. However, these data cannot be disclosed due to privacy and moral constraints.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the People’s Hospital of Yixing City, Jiangsu Province (batch number: 2022 Wen 082), and all the subjects signed the informed consent form.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was partially supported by the National Natural Science Foundation of China (81802102) and the Young Top Talents of Wuxi Health Commission (grant no. BJ2020107).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Riley CM, Sciurba FC. Diagnosis and outpatient management of chronic obstructive pulmonary disease: a review. JAMA. 2019;321(8):786–797. doi:10.1001/jama.2019.0131
2. Alqahtani JS, Aquilina J, Bafadhel M, et al. Research priorities for exacerbations of COPD. Lancet Respir Med. 2021;9(8):824–826. doi:10.1016/S2213-2600(21)00227-7
3. Ushida K, Shimizu A, Hori S, et al. Hospital frailty risk score predicts outcomes in chronic obstructive pulmonary disease exacerbations. Arch Gerontol Geriatr. 2022;100:104658. doi:10.1016/j.archger.2022.104658
4. Kagiali S, Inal-Ince D, Cakmak A, et al. Daily living activities, exercise capacity, cognition, and balance in COPD patients with and without frailty. Ir J Med Sci. 2022;191(2):817–824. doi:10.1007/s11845-021-02654-8
5. Marengoni A, Vetrano DL, Manes-Gravina E, et al. The relationship between COPD and frailty: a systematic review and meta-analysis of observational studies. Chest. 2018;154(1):21–40. doi:10.1016/j.chest.2018.02.014
6. Yee N, Locke ER, Pike KC, et al. Frailty in chronic obstructive pulmonary disease and risk of exacerbations and hospitalizations. Int J Chron Obstruct Pulmon Dis. 2020;15:1967–1976. doi:10.2147/COPD.S245505
7. Naval E, González MC, Giraldós S, et al. Frailty assessment in a stable COPD cohort: is there a COPD-frail phenotype? COPD. 2021;18(5):525–532. doi:10.1080/15412555.2021.1975670
8. Alqahtani JS, Aldabayan YS, Aldhahir AM, et al. Predictors of 30- and 90-Day COPD exacerbation readmission: a prospective cohort study. Int J Chron Obstruct Pulmon Dis. 2021;16:2769–2781. doi:10.2147/COPD.S328030
9. Alqahtani JS, Njoku CM, Bereznicki B, et al. Risk factors for all-cause hospital readmission following exacerbation of COPD: a systematic review and meta-analysis. Eur Respir Rev. 2020;29(156):190166. doi:10.1183/16000617.0166-2019
10. Hartl S, Lopez-Campos JL, Pozo-Rodriguez F, et al. Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD Audit. Eur Respir J. 2016;47(1):113–121. doi:10.1183/13993003.01391-2014
11. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
12. Kim EK, Singh D, Park JH, et al. Impact of body mass index change on the prognosis of chronic obstructive pulmonary disease. Respiration. 2020;99(11):943–953. doi:10.1159/000511022
13. Bestall JC, Paul EA, Garrod R, et al. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
14. Cheng SL, Lin CH, Wang CC, et al. Comparison between COPD Assessment Test (CAT) and modified medical research council (mMRC) dyspnea scores for evaluation of clinical symptoms, comorbidities and medical resources utilization in COPD patients. J Formos Med Assoc. 2019;118(1 Pt 3):429–435. doi:10.1016/j.jfma.2018.06.018
15. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
16. Hilmer SN, Perera V, Mitchell S, et al. The assessment of frailty in older people in acute care. Australas J Ageing. 2009;28(4):182–188. doi:10.1111/j.1741-6612.2009.00367.x
17. Walraven CV, Dhalla IA, Bell C, et al. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. Can Med Assoc J. 2010;182(6):551–557. doi:10.1503/cmaj.091117
18. Putcha N, Anzueto AR, Calverley PMA, et al. Mortality and exacerbation risk by body mass index in patients with COPD in TIOSPIR and UPLIFT. Ann Am Thorac Soc. 2022;19(2):204–213. doi:10.1513/AnnalsATS.202006-722OC
19. Shin SH, Kwon SO, Kim V, et al. Association of body mass index and COPD exacerbation among patients with chronic bronchitis. Respir Res. 2022;23(1):52. doi:10.1186/s12931-022-01957-3
20. Wada H, Ikeda A, Maruyama K, et al. Low BMI and weight loss aggravate COPD mortality in men, findings from a large prospective cohort: the JACC study. Sci Rep. 2021;11(1):1531. doi:10.1038/s41598-020-79860-4
21. Zhang R, Lu H, Chang Y, et al. Prediction of 30-day risk of acute exacerbation of readmission in elderly patients with COPD based on support vector machine model. BMC Pulm Med. 2022;22(1):292. doi:10.1186/s12890-022-02085-w
22. Montagnani A, Mathieu G, Pomero F, et al. Hospitalization and mortality for acute exacerbation of chronic obstructive pulmonary disease (COPD): an Italian population-based study. Eur Rev Med Pharmacol Sci. 2020;24(12):6899–6907. doi:10.26355/eurrev_202006_21681
23. Luu P, Tulka S, Knippschild S, et al. Risikoabschätzung einer akuten Exazerbation bei COPD-Patienten im Rahmen einer pneumologischen Anschluss-Rehabilitation anhand der Prävalenz und Schwergradausprägung von Komorbiditäten [Risk Assessment of Acute Exacerbation in COPD patients in the context of pulmonary follow-up rehabilitation based on the prevalence and severity of comorbidities]. Pneumologie. 2021;75(7):516–525. German. doi:10.1055/a-1346-5504
24. Cheng SL, Li YR, Huang N, et al. Effectiveness of Nationwide COPD pay-for-performance program on COPD exacerbations in Taiwan. Int J Chron Obstruct Pulmon Dis. 2021;16:2869–2881. doi:10.2147/COPD.S329454
25. Bernabeu-Mora R, García-Guillamón G, Valera-Novella E, et al. Frailty is a predictive factor of readmission within 90 days of hospitalization for acute exacerbations of chronic obstructive pulmonary disease: a longitudinal study. Ther Adv Respir Dis. 2017;11(10):383–392. doi:10.1177/1753465817726314
26. Kon SS, Jones SE, Schofield SJ, et al. Gait speed and readmission following hospitalisation for acute exacerbations of COPD: a prospective study. Thorax. 2015;70(12):1131–1137. doi:10.1136/thoraxjnl-2015-207046
27. Walsh JA, Barker RE, Kon SSC, et al. Gait speed and adverse outcomes following hospitalised exacerbation of COPD. Eur Respir J. 2021;58(5):2004047. doi:10.1183/13993003.04047-2020
28. Hakim MA, Garden FL, Jennings MD, et al. Performance of the LACE index to predict 30-day hospital readmissions in patients with chronic obstructive pulmonary disease. Clin Epidemiol. 2017;10:51–59. doi:10.2147/CLEP.S149574
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
Frailty and Mortality Risk in COPD: A Cohort Study Comparing the Fried Frailty Phenotype and Short Physical Performance Battery
Brighton LJ, Nolan CM, Barker RE, Patel S, Walsh JA, Polgar O, Kon SSC, Gao W, Evans CJ, Maddocks M, Man WDC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:57-67
Published Date: 20 January 2023
Prevalence and Risk Factors for COPD in an Urbanizing Rural Area in Western China: A Cross-Sectional Study
Zhang X, Lei Z, Wu Y, Song Y, Wu X, Yang B, Fan J, Feng S, Wu L, Li L, Dai Q, Zeng Z, Feng M, Zhang T
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:459-468
Published Date: 4 April 2023
β2-Adrenoceptor Agonists in Asthma or Chronic Obstructive Pulmonary Disease and Risk of Parkinson’s Disease: Nested Case-Control Study
Paakinaho A, Tiihonen M, Koskela H, Koponen M, Tiihonen J, Hartikainen S, Tolppanen AM
Clinical Epidemiology 2023, 15:695-705
Published Date: 12 June 2023
Extrapulmonary Comorbidities Associated with Chronic Obstructive Pulmonary Disease: A Review
Xiang Y, Luo X
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:567-578
Published Date: 29 February 2024