Back to Journals » Infection and Drug Resistance » Volume 19
Risk Factors for Subtherapeutic Exposure and Hepatotoxicity Threshold of Posaconazole: A Real-World Study in Chinese Patients with Invasive Pulmonary Fungal Infection
Authors Wang B ![]() , Li S
, Li S ![]() , Wang J, Zhang J, Liu H, Jin L
, Wang J, Zhang J, Liu H, Jin L ![]()
Received 11 February 2026
Accepted for publication 30 May 2026
Published 15 June 2026 Volume 2026:19 602958
DOI https://doi.org/10.2147/IDR.S602958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Bingqing Wang,1,* Shuting Li,1,* Jing Wang,2 Jing Zhang,2 Hang Liu,1,2 Lu Jin1,2
1Department of Pharmacy, Nanjing Drum Tower Hospital, Nanjing Drum Tower Hospital Clinical College, Nanjing University of Chinese Medicine, Nanjing, 210008, People’s Republic of China; 2Department of Pharmacy, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, 210008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lu Jin, Department of Pharmacy, Nanjing Drum Tower Hospital, Nanjing Drum Tower Hospital Clinical College, Nanjing University of Chinese Medicine, Nanjing, 210008, People’s Republic of China, Email [email protected] Hang Liu, Department of Pharmacy, Nanjing Drum Tower Hospital,Nanjing Drum Tower Hospital Clinical College, Nanjing University of Chinese Medicine, Nanjing, 210008, People’s Republic of China, Email [email protected]
Background: Posaconazole exhibits substantial pharmacokinetic variability, particularly with oral formulations. Real-world data on target attainment across formulations and on specific toxicity thresholds remain limited. This study aimed to evaluate posaconazole target attainment rates, identify independent predictors of subtherapeutic exposure, and explore potential hepatotoxicity exposure thresholds in a real-world Chinese cohort.
Methods: This single-centre, retrospective observational study conducted at Nanjing Drum Tower Hospital, China, between January 2023 and August 2025 enrolled 148 patients with IPFI. Posaconazole was administered for prophylaxis with a target trough concentration of ≥ 0.5 mg/L, or for treatment with a target of ≥ 1.0 mg/L. Multivariable logistic regression was utilised to identify independent predictors of subtherapeutic exposure.
Results: Subtherapeutic trough concentrations were observed in 24.0% of the prophylaxis group and 23.3% of the treatment group. Concomitant proton pump inhibitor (PPI) use was the dominant independent risk factor for subtherapeutic exposure in both prophylaxis (OR 17.97, 95% CI 4.22– 76.53, P< 0.001) and treatment (OR 3.60, 95% CI 1.10– 11.75, P=0.034) groups. Regarding regimen optimisation, switching to the intravenous formulation proved more effective than oral dose escalation for correcting subtherapeutic levels. Furthermore, an exposure–safety analysis revealed that hepatotoxicity rates increased significantly when trough concentrations exceeded 1.95 mg/L (P=0.015).
Conclusion: Subtherapeutic posaconazole exposure remains common. PPI use is a critical risk factor that may not be fully overcome by delayed-release or intravenous formulations. Our findings suggest a potential exposure-hepatotoxicity relationship around 1.95 mg/L for Chinese patients, highlighting the need for individualised TDM.
Keywords: posaconazole, therapeutic drug monitoring, proton pump inhibitors, hepatotoxicity
Introduction
In recent years, with the increasing use of broad-spectrum antimicrobial agents, corticosteroids, and immunosuppressants, along with the growing number of solid organ and allogeneic haematopoietic stem cell transplant recipients, the incidence and mortality rates of invasive pulmonary fungal infections (IPFIs) have been rising.1 Despite the introduction of novel antifungal agents, mortality rates remain high.2,3
Posaconazole, a second-generation triazole antifungal, is widely used for the prevention and treatment of IPFIs because of its broad-spectrum antifungal activity and favourable safety profile. However, it exhibits significant interpatient pharmacokinetic variability, particularly with oral formulations. Multiple factors, including formulation differences, gastrointestinal function, concomitant medications, and specific patient pathophysiological conditions, can substantially affect drug exposure. Existing evidence has established a clear association between subtherapeutic concentrations and the occurrence of breakthrough invasive fungal infections or treatment failure.4 Consequently, therapeutic drug monitoring (TDM) is recommended to optimise clinical outcomes.
Although numerous studies have evaluated posaconazole TDM, most are confined to patients with haematological malignancies. Data on target attainment rates and influencing factors remain scarce in real-world clinical practice in China, particularly among patients with pulmonary fungal infections secondary to other diseases, and especially for those receiving different formulations, including oral suspension, delayed-release tablets, and intravenous formulation. Furthermore, current TDM guidelines primarily focus on defining minimum effective concentrations, while robust real-world evidence supporting a toxicity threshold for posaconazole is lacking.
Materials and Methods
Study Design and Population
This was a single-centre, retrospective observational study conducted at Nanjing Drum Tower Hospital (Nanjing, China). Inclusion criteria were patients who received posaconazole oral suspension, delayed-release tablets, or intravenous infusion between January 2023 and August 2025 and who underwent at least one therapeutic drug monitoring (TDM) measurement of posaconazole during therapy. Patients were excluded if their medical records were incomplete or if the infection was not pulmonary.
Therapeutic Drug Monitoring of Posaconazole
Throughout the course of posaconazole therapy, blood concentration measurements were performed at the discretion of the treating clinicians, based on clinical need. To assess steady-state concentrations, the initial Cmin measurement is consistently scheduled on Day 5 post-initiation. Subsequent follow-up measurements are typically conducted in cycles of approximately 5 days to monitor the impact of clinical changes or dosage adjustments. Plasma trough concentrations (Cmin) were determined using a validated two-dimensional liquid chromatography method established in our Centre (LC1 column: SC2 (3.5×25 mm, 5 μm); intermediate column: SCB (4.6×10 mm, 3.5 μm); LC2 column: SCB (4.6×125 mm, 5 μm)). The linear range of this analytical method was 0.30 to 25.00 mg/L. In accordance with the 2020 European Society of Intensive Care Medicine (ESICM) position paper “Antimicrobial therapeutic drug monitoring in critically ill adult patients”, the target trough concentration for posaconazole prophylaxis was set at ≥0.5 mg/L, and for treatment at ≥1.0 mg/L. When the Cmin failed to reach the target, clinical pharmacists provided dose adjustment recommendations, with the final decision made by the attending physician.
Data Collection
Patient data were extracted from the hospital electronic medical record system and included: (1) Demographic characteristics: age, sex, weight, and BMI; (2) Primary diagnosis, treatment outcomes, and adverse events; (3) Posaconazole medication details: formulation, dose, dosing frequency, and duration of therapy; (4) Laboratory parameters: C-reactive protein (CRP), albumin, alkaline phosphatase (ALP), aspartate aminotransferase (AST), alanine aminotransferase (ALT), estimated glomerular filtration rate (eGFR), and total bilirubin; (5) Concomitant medications with potential for interaction: proton pump inhibitors (PPIs), H2-receptor antagonists, antacids, immunosuppressants, and CYP3A4 inducers/inhibitors. Laboratory values were those collected on the day of plasma concentration testing. All other clinical information and concomitant medication data were collected within the 5 days preceding the plasma concentration measurement. The estimated glomerular filtration rate (eGFR) in our study was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.
Definition of Invasive Fungal Infection and Treatment Outcomes
Breakthrough invasive fungal infection (IFI) was defined as an IFI diagnosed during posaconazole prophylaxis or within 7 days of its discontinuation. The classification of proven, probable, and possible IFI was based on the criteria established by the European Organization for Research and Treatment of Cancer (EORTC) and the Mycoses Study Group Education and Research Consortium (MSGERC).5 For patients receiving posaconazole (PCZ) for the treatment of a fungal infection, therapeutic success was assessed based on partial or complete resolution of clinical signs of infection (e.g., infectious symptoms or fever) and radiological findings (on computed tomography [CT], high-resolution CT, or magnetic resonance imaging). Treatment failure was defined as persistent or progressive IFI according to clinical and radiological evidence, persistently positive cultures, or death due to IFI after at least 7 days of PCZ therapy. The absence of breakthrough infection in patients receiving PCZ for prophylaxis was considered a successful outcome.
Safety Assessment
Elevations in hepatic function parameters (including alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, and bilirubin concentrations) and renal function parameters (serum creatinine concentration) were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE version 5.0). Specifically, hepatotoxicity was categorised based on the following thresholds: Grade 1 (ALT/AST >ULN to 3.0×ULN; or Bilirubin >ULN to 1.5×ULN), Grade 2 (ALT/AST >3.0 to 5.0×ULN; or Bilirubin >1.5 to 3.0×ULN), Grade 3 (ALT/AST >5.0 to 20.0×ULN; or Bilirubin >3.0 to 10.0×ULN), and Grade 4 (ALT/AST >20.0×ULN; or Bilirubin >10.0×ULN). Renal impairment was graded based on serum creatinine elevations: Grade 1 (>1.0 to 1.5×baseline, or >ULN to 1.5×ULN), Grade 2 (>1.5 to 3.0×baseline, or >1.5 to 3.0×ULN), Grade 3 (>3.0×baseline, or >3.0 to 6.0×ULN), and Grade 4 (>6.0×ULN). Furthermore, posaconazole use has been associated with the occurrence of hypokalaemia in previous studies. The diagnosis of hypokalaemia was primarily based on serum potassium levels, typically defined as a serum potassium concentration below 3.5 mmol/L.6 The causality assessment between adverse events and posaconazole was evaluated using the Naranjo algorithm and categorised as follows: definitely related, probably related, possibly related, unlikely related, and unrelated. For this analysis, only adverse events classified as “definitely related” or “probably related” were included.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics (version 25.0; IBM Corp., Armonk, NY, USA). Continuous variables are expressed as median (interquartile range, IQR) and were compared using the Mann–Whitney U-test or Kruskal–Wallis H-test, as appropriate. Categorical variables are presented as frequency (percentage) and were analysed using the χ2 test or Fisher’s exact test. Kaplan–Meier curves were plotted to illustrate the cumulative probability of achieving target concentrations within 30 days of treatment across different formulations, and the log-rank test was used for between-group comparisons. Variables with P<0.05 in univariate analysis were included in a multivariable logistic regression model to identify independent predictors of subtherapeutic exposure. Odds ratios (OR) and 95% confidence intervals (CI) were calculated. The exposure-safety relationship was evaluated by comparing the incidence of adverse events across quartile groups of Cmin using the χ2 test. A two-sided P<0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 322 patients were screened, and 148 were ultimately included in the analysis based on the inclusion and exclusion criteria (Figure 1). Of these, 96 patients (64.9%) received PCZ for prophylaxis and 52 (35.1%) for treatment. The median age was 55 years (IQR 40–63), and 48% were female. The primary diagnoses included acute myeloid leukaemia (20.9%), pneumonia (16.2%), and pulmonary fungal infection (12.2%). Notably, up to 61.5% (n=91) of patients were co-administered proton pump inhibitors, and 45.3% received other medications with potential interactions. Posaconazole formulations comprised oral suspension (60.8%), delayed-release tablets (4.7%), and intravenous infusion (34.5%) (Table 1).
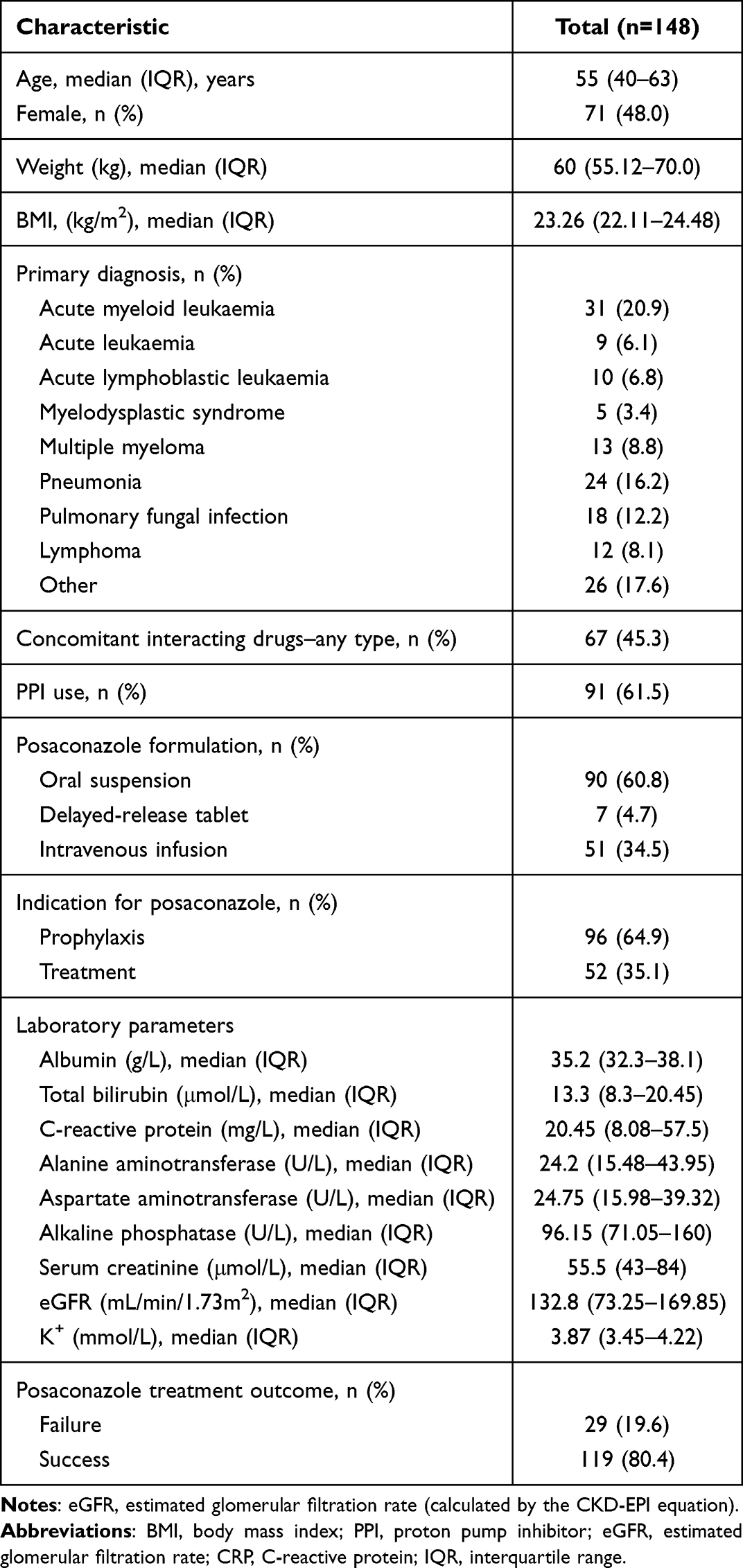 |
Table 1 Demographic and Clinical Baseline Characteristics of the Study |
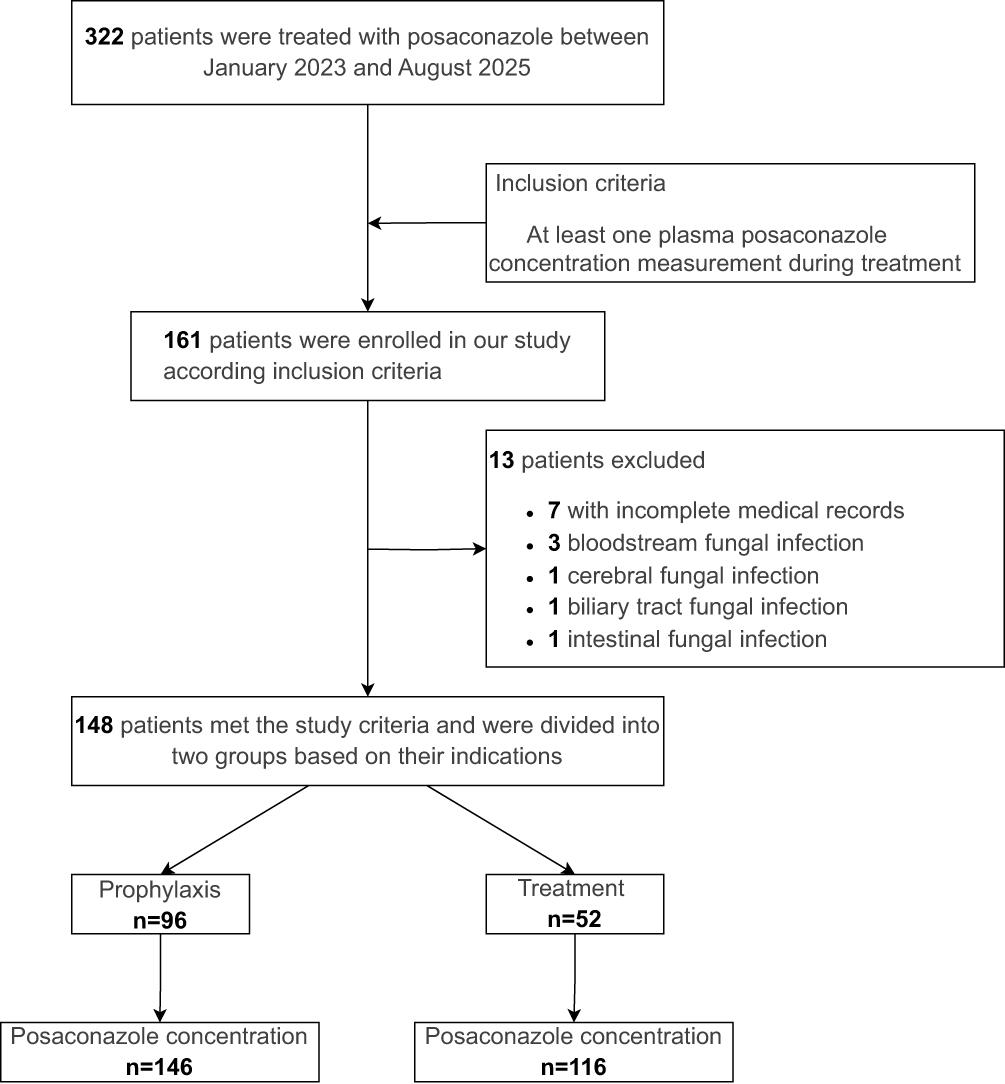 |
Figure 1 Flowchart of patient study with posaconazole treatment and inclusion criteria. |
Target Concentration Attainment
A total of 262 trough concentration (Cmin) measurements were analysed. The overall median Cmin was 1.2 mg/L (IQR 0.6–1.94). Subtherapeutic levels were observed in 24.0% (35/146) of the prophylaxis group (<0.5 mg/L) and 23.3% (27/116) of the treatment group (<1.0 mg/L). The exposure profile of posaconazole over time in the entire cohort is shown in Figure 2. All monitored plasma concentrations reached the prophylactic target (≥0.5 mg/L) by day 30 of prophylaxis. In subgroup analyses, Kaplan–Meier curves depicting the cumulative target attainment rate at 30 days across different formulations are presented in Figure 3. A significant difference in the probability of target attainment was observed among the three groups (Log-Rank P=0.0041). The intravenous formulation group showed the highest attainment rate, while the oral suspension group had the lowest.
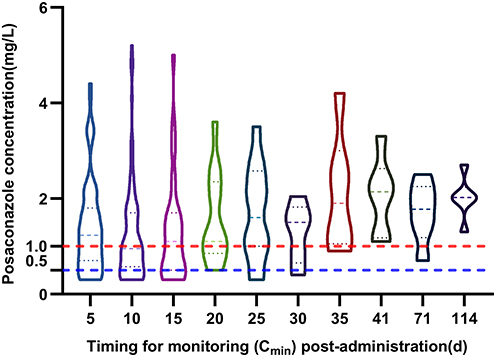 |
Figure 2 A violin plot of posaconazole concentration over post-administration monitoring days, with target lines. Notes: Boxplot elements are superimposed on the violin plot. Values are presented as medians with interquartile ranges. The dashed lines at the upper and lower edges of the box represent the third quartile (Q3) and the first quartile (Q1), respectively, and the dashed line inside the box represents the median. The horizontal lines indicate the target thresholds (prophylaxis: blue line=0.5 mg/L; therapy: red line=1.0 mg/L). |
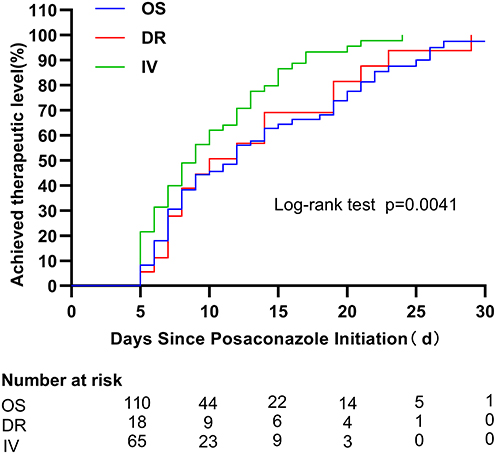 |
Figure 3 Kaplan–Meier estimates of the cumulative probability of target attainment within 30 days (stratified by formulation), and therapeutic levels over days since posaconazole start. Abbreviations: OS, oral suspension; DR, delayed-release tablet; IV, intravenous formulation. |
Risk Factors for Subtherapeutic
In the prophylaxis cohort, gastrointestinal function and concomitant medications played a decisive role (Table 2). Multivariable logistic regression identified concomitant use of proton pump inhibitors (PPIs) as the strongest independent predictor of failure to achieve the target concentration (OR 17.97; 95% CI 4.22–76.53; P<0.001) followed by active diarrhoea (OR 7.69; 95% CI 2.70–21.93; P<0.001) and vomiting (OR 6.00; 95% CI 1.20–29.91; P=0.029). Notably, in the treatment cohort, PPI use remained a significant independent risk factor for inadequate exposure (OR 3.60; 95% CI 1.10–11.75; P=0.034) (Table 3). Although this cohort included patients receiving intravenous formulations, this association is consistent with the known pH-dependent absorption mechanism of oral posaconazole and is likely driven by the substantial proportion of patients receiving the oral suspension. This finding underscores that reliance on oral formulations—even delayed-release tablets—might be suboptimal for patients requiring concomitant PPI therapy.
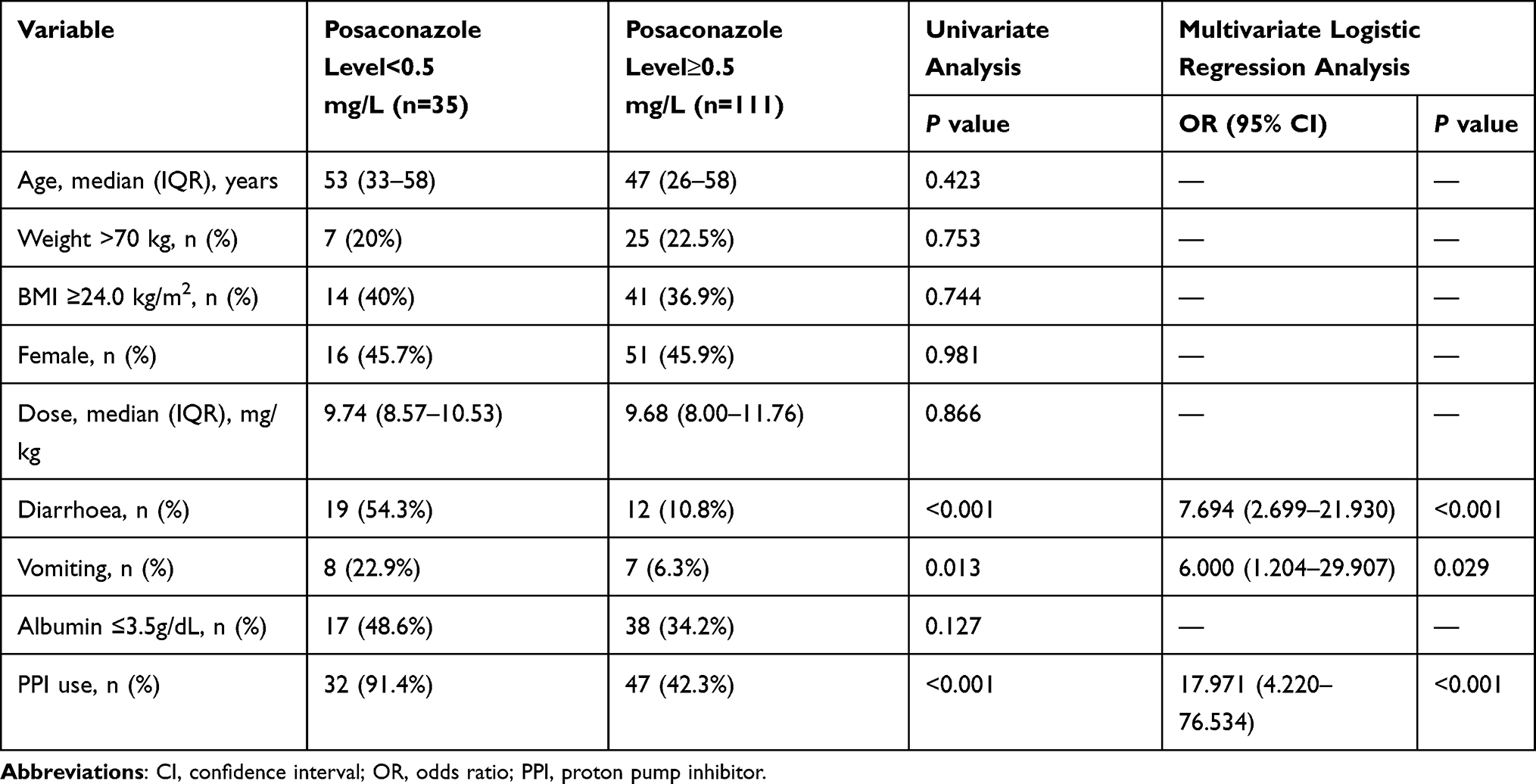 |
Table 2 Multivariate Logistic Regression Analysis of Risk Factors for Subtherapeutic Exposure in the Prophylaxis Cohort |
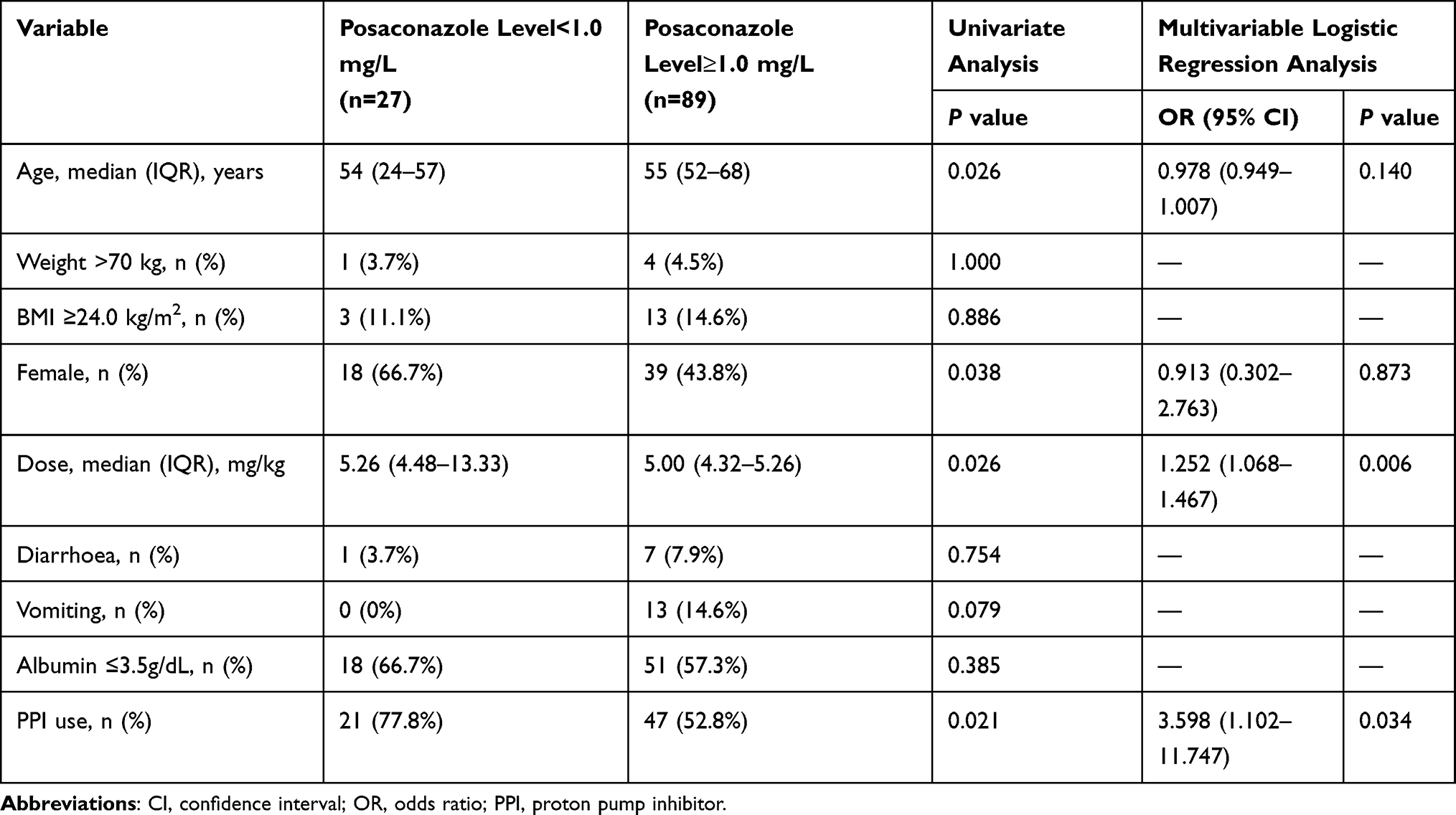 |
Table 3 Multivariate Logistic Regression Analysis of Risk Factors for Subtherapeutic Exposure in the Treatment Cohort |
Association Between Posaconazole Exposure and Clinical Outcomes
Among 96 patients receiving prophylactic therapy, breakthrough invasive fungal infections (IFIs) occurred in 15 (15.6%). Although the median Cmin was comparable between the two groups, a trend was observed in target attainment: the proportion of patients with subtherapeutic exposure (<0.50 mg/L) was nearly twice as high in the breakthrough infection group as in the non-infection group (40.0% vs. 25.9%). Although limited by the small sample size of infection events, this difference did not reach statistical significance (P=0.423). However, the data suggest a preliminary trend between low trough concentrations and prophylactic failure. In the treatment cohort (n=52), disease progression occurred in 14 (26.9%) patients. A difference in exposure was observed: patients who responded to treatment maintained a numerically higher median Cmin of 2.06 mg/L (IQR 0.98–2.45 mg/L), while those with disease progression had a lower median Cmin of 1.55 mg/L (IQR 0.50–2.52 mg/L). However, likely due to the small sample size in the non-responder subgroup, the difference was not statistically significant (P=1.000).
Exposure-Safety Response Relationship
The most common treatment-related (possible or probable) adverse events associated with posaconazole included hypokalaemia and elevations in liver enzymes (aspartate aminotransferase and alanine aminotransferase). Based on the Naranjo algorithm, among the included treatment-related adverse events, 35 events were classified as “definitely related” and 114 events were classified as “probably related” to posaconazole. Regarding liver injury, a total of 60 patients developed hepatotoxicity: 36 (60.0%) patients were CTCAE grade 1, 15 (25.0%) were grade 2, and 9 (15.0%) were grade 3. Compared with the first to third quartile groups (trough concentration range 0.30–1.94 mg/L), the incidence of most treatment-related adverse events showed an increasing trend in the fourth quartile group (range 1.95–5.20 mg/L). This finding suggests a potential exposure–toxicity relationship, with a higher incidence of hepatotoxicity observed when posaconazole trough concentrations exceeded approximately 1.95 mg/L in this real-world population. In contrast, no significant correlation across concentration ranges was observed for hypokalaemia or renal impairment (Table 4). In addition, the liver function parameters (AST, ALT, total bilirubin, and ALP) in patients with and without hepatotoxicity, as well as the detailed distribution of patients by grade of hepatotoxicity, are presented in Supplementary Tables 1 and 2.
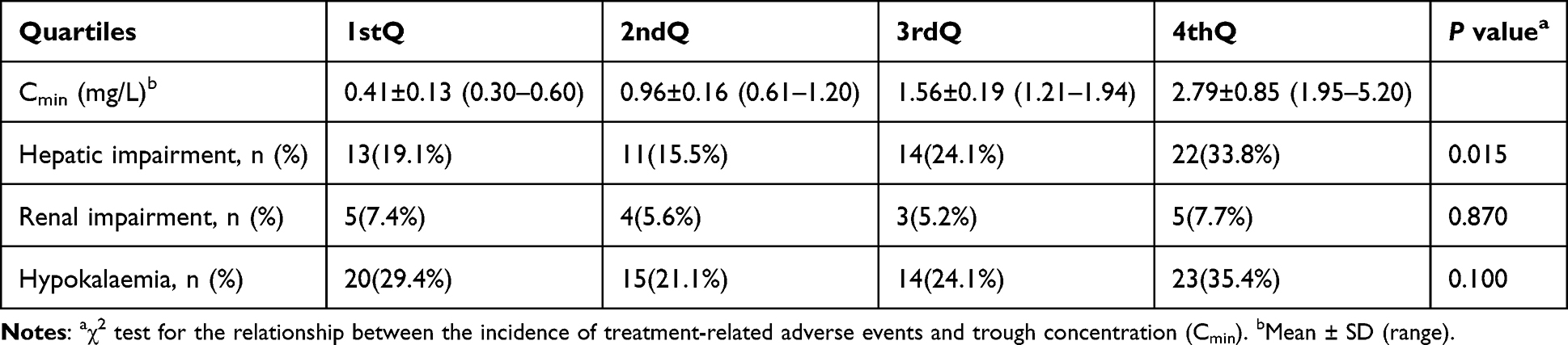 |
Table 4 Association Between Posaconazole Trough Concentration Quartiles and the Incidence of Treatment-Related Adverse Events |
Regimen Adjustment in Patients with Subtherapeutic Concentrations
Of the 43 patients (29.1%) who did not achieve the target trough concentration at baseline, 15 underwent regimen modification. Among these, 8 were switched to other antifungal agents. In the 7 patients who continued posaconazole with regimen adjustment, the outcomes in terms of target attainment varied (Table 5). Among the 3 patients who received dose escalation of the oral suspension only, only one (Patient 3) reached the therapeutic target (1.1 mg/L) after the dose was increased to 1600 mg/day, while the other two remained subtherapeutic despite dose increases up to 800 mg/day. In contrast, among the 4 patients who underwent formulation switching, 3 (75%) successfully achieved the target concentration. Only one patient (Patient 1), after switching from the suspension to the intravenous formulation, showed an increase in plasma concentration from 0.3 mg/L to 0.7 mg/L but remained slightly below the treatment target of 1.0 mg/L.
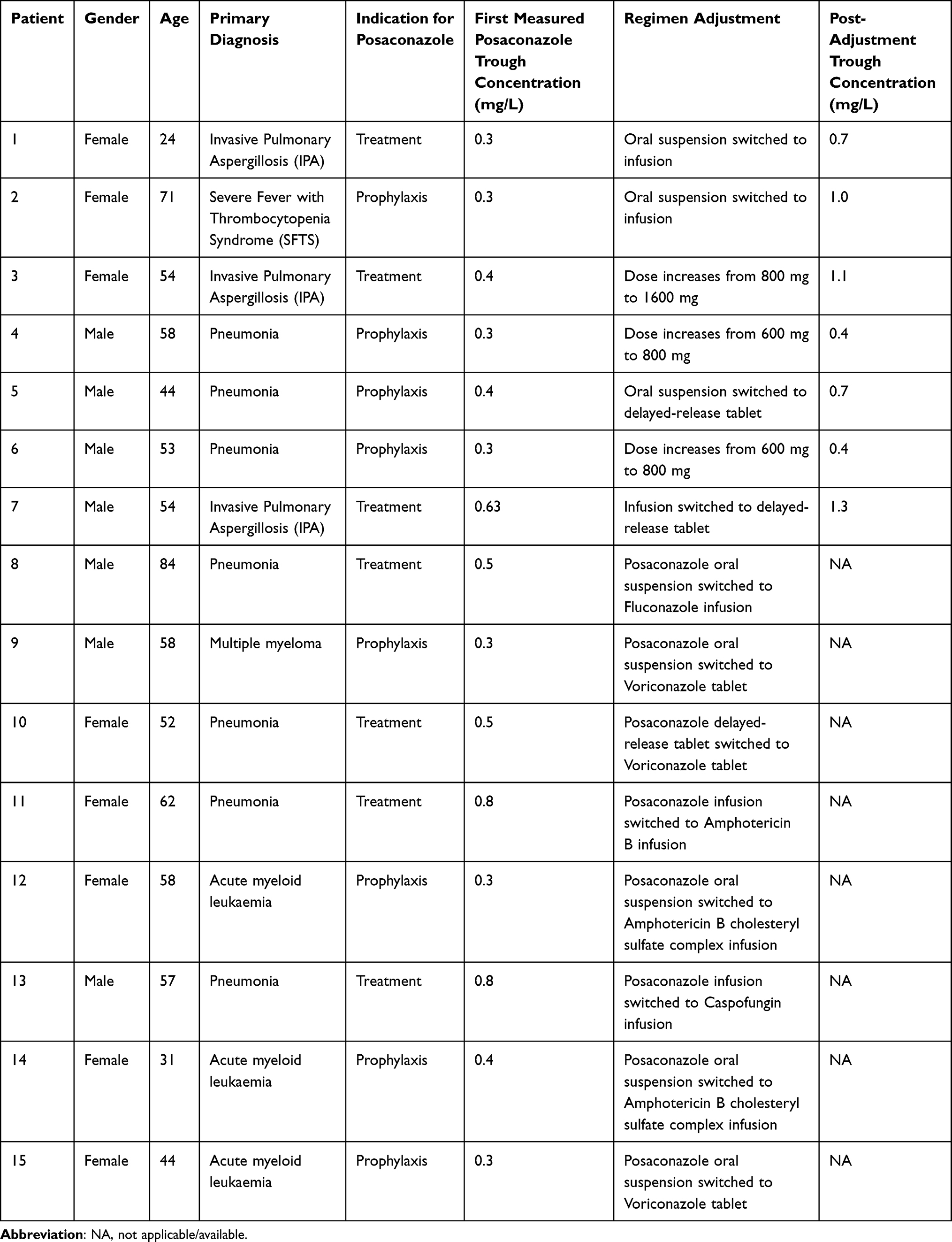 |
Table 5 Clinical Outcomes Following Regimen Adjustments in Patients with Initial Subtherapeutic Exposure |
Discussion
Through a retrospective analysis of 148 patients with invasive pulmonary fungal infections in a real-world clinical setting, this study comprehensively evaluated the target attainment rates of posaconazole trough concentrations and identified critical independent predictors of inadequate exposure, alongside defining a potential exposure-safety relationship.
In the therapeutic cohort, where the target Cmin was set at ≥1.0 mg/L, the observed target attainment rate was 76.7%. This finding closely aligns with recent real-world literature; for instance, Krekel et al7 reported that 71.8% of patients receiving delayed-release tablets or intravenous formulations achieved this therapeutic target, a trend further supported by data from Kraljevic et al.8 Conversely, the target attainment rate of 76.0% in our prophylactic cohort was notably higher than the 43.0%–59.5% reported in previous studies.4,9,10 This discrepancy is primarily driven by target threshold selection. While prior cohorts followed the conservative ≥0.7 mg/L target recommended by the 2017 ECIL-6 and ESCMID-ECMM-ERS guidelines,11,12 our study adopted the ≥0.5 mg/L threshold proposed by the 2020 ESICM position paper.13 This choice is strongly supported by a meta-analysis by Chen et al,14 which demonstrated that achieving 0.5 mg/L doubles the odds of successful prophylaxis, whereas escalating the target to 0.7 mg/L yields no incremental statistical benefit.
Mechanistically, the identified independent risk factors including concomitant PPI use, active diarrhoea, and vomiting collectively impair gastrointestinal drug disposition, highly congruent with findings by Tang et al,15 Lin et al16 and Miceli et al.17 PPIs elevate gastric pH, which substantially hinders the dissolution and absorption of the oral suspension, and potentially disrupts the complex gastrointestinal transit and disintegration of delayed-release tablets. Concurrently, diarrhoea accelerates gastrointestinal transit time, limiting mucosal drug contact, while vomiting directly reduces the active drug payload before systemic absorption. These gastrointestinal factors can significantly reduce oral bioavailability. Consequently, clinicians should meticulously evaluate the necessity of long-term PPIs, consider weaker acid-suppressive alternatives, maintain a high index of suspicion in patients with gastrointestinal disturbances, and prioritise early TDM or a transition to the intravenous formulation to bypass these physiological barriers. Intriguingly, neither elevated body mass index (BMI ≥24 kg/m2) nor hypoalbuminaemia significantly predicted subtherapeutic exposure, contrasting with observations in haematologic malignancy cohorts.15,17,18 This discrepancy likely stems from patient heterogeneity, as our study enrolled a substantial proportion of patients with non-haematologic pneumonia whose nutritional status and fluid dynamics differ markedly from typical haematology cohorts, coupled with variations in statistical power across sample sizes.
Regarding clinical efficacy, the breakthrough infection group exhibited a numerically higher proportion of subtherapeutic exposure compared to the non-infected group, with rates of 40.0% and 25.9% respectively. This observation echoes the concentration-efficacy trends described by Sengar et al.4 Similarly, the disease progression subgroup demonstrated a lower median trough concentration of 1.55 mg/L compared to 2.06 mg/L in responders. Although these differences did not achieve statistical significance (P=0.423) due to the limited number of clinical endpoint events, the observed preliminary trends strongly imply that certain refractory infections might require targets exceeding the conventional 1.0 mg/L threshold to ensure success.
In terms of safety, our quartile analysis identified a potential hepatotoxicity threshold of 1.95 mg/L, which is notably lower than the 3.75 mg/L limit reported by Schauwvlieghe et al.19 This discrepancy suggests that Chinese patients may possess a lower tolerance for posaconazole-induced liver injury, potentially driven by inter-ethnic metabolic variations or higher baseline rates of hepatic conditions.20,21 However, as this relationship is derived from a univariate analysis without adjusting for baseline liver function, concurrent hepatotoxic drugs, or disease severity, this threshold remains associative rather than predictive, and must be interpreted with caution. Importantly, our analysis of regimen optimisation demonstrates that switching from the oral suspension to an intravenous formulation or delayed-release tablets is significantly more effective for rescuing subtherapeutic levels than oral dose escalation alone, echoing the successful implementation of tablets by Patel et al22 in complex real-world settings. Simple dose escalation of the oral suspension often fails to overcome concurrent gastrointestinal risk factors, making formulation switching a preferred clinical strategy.
This study has several inherent limitations. First, its single-centre, retrospective design may introduce selection bias, information bias, patient heterogeneity, and indication bias; additionally, the resulting data are interval-censored. Second, reliance on electronic medical records precluded precise quantification of the severity and duration of gastrointestinal symptoms, such as diarrhoea and vomiting, potentially resulting in residual confounding in the risk factor analysis. Third, although the inclusion of three different posaconazole formulations reflects real-world clinical practice, the imbalanced sample sizes across formulation groups precluded a robust stratified analysis of the impact of PPI use within each specific formulation. Thus, interpretation of formulation-based comparisons should be approached with caution due to the unequal sizes of the groups. Finally, the diagnosis of invasive fungal infections and the assessment of treatment outcomes are inherently complex and, despite the application of internationally recognised criteria, some degree of subjective variation in clinical assessment may still exist.
Conclusion
In conclusion, subtherapeutic posaconazole exposure remains common despite new formulations. PPI use is a key risk factor, especially for oral therapy. Our findings suggest a potential exposure-hepatotoxicity relationship that warrants further validation. Consequently, for patients with GI dysfunction or unavoidable PPI use, intravenous administration should be prioritised over dose escalation, supported by routine TDM to balance efficacy and safety.
Data Sharing Statement
The datasets generated and analysed during the current study are available from the corresponding author, Lu Jin, upon reasonable request.
Ethical Approval
This study was granted approval by the Ethics Committee of Drum Tower Hospital affiliated with the Medical School of Nanjing University (NO. 2025-0273-02) and registered on Chinese Clinical Trial Registry (ChiCTR2500101166) (http://www.chictr.org.cn). The requirement for obtaining informed consent was waived by the relevant ethics committee because of the retrospective nature of the study and the anonymisation of data. This study complies with the Declaration of Helsinki.
Acknowledgments
We gratefully acknowledge the staff of the therapeutic drug monitoring laboratory at Nanjing Drum Tower Hospital for their technical assistance in the quantification of posaconazole plasma concentrations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the 2025 Yao Yan Xin Sheng Pharmaceutical Research Project of the Jiangsu Pharmaceutical Association (No. 202564121).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jaggi TK, Agarwal R, Tiew PY, et al. Fungal lung disease. Eur Respir J. 2024;64(5):2400803. doi:10.1183/13993003.00803-2024
2. Gaffney S, Kelly DM, Rameli PM, et al. Invasive pulmonary aspergillosis in the intensive care unit: current challenges and best practices. APMIS. 2023;131(11):654–12. doi:10.1111/apm.13316
3. Schauwvlieghe AFAD, Rijnders BJA, Philips N, et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med. 2018;6(10):782–792. doi:10.1016/S2213-2600(18)30274-1
4. Sengar M, Jain H, D’souza S, et al. Exposure-response relationship of posaconazole suspension in theprophylaxis of invasive fungal infections in patients with acute myeloid leukemia. Indian J Hematol Blood Transfus. 2023;39(2):200–207. doi:10.1007/s12288-022-01568-4
5. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
6. Gupta G, Teo AED, Swee DS, et al. Prolonged hypokalemia and delayed diagnosis of primary aldosteronism: clinical course and risk factors. J Clin Endocrinol Metab. 2024;109(8):e1574–e1581. doi:10.1210/clinem/dgad752
7. Krekel T, Miller J, Catalano A, et al. Evaluation of therapeutic target attainment with various posaconazole formulations. Transpl Infect Dis. 2025;27(6):e70105. doi:10.1111/tid.70105
8. Kraljevic M, Khanna N, Medinger M, et al. Clinical considerations on posaconazole administration and therapeutic drug monitoring in allogeneic hematopoietic cell transplant recipients. Med Mycol. 2021;59(7):701–711. doi:10.1093/mmy/myaa106
9. Du X, Yan Y, Li F, et al. Therapeutic drug monitoring of posaconazole oral suspension in paediatric hematology patients under 13 years of age. Transl Pediatr. 2025;14(1):4–13. doi:10.21037/tp-24-400
10. Lai T, Alffenaar J-W, Kesson A, et al. Evaluation of target attainment of oral posaconazole suspension in immunocompromised children. J Antimicrob Chemother. 2020;75(3):726–729. doi:10.1093/jac/dkz481
11. Tissot F, Agrawal S, Pagano L, et al. ECIL-6 guidelines for the treatment of invasive candidiasis, aspergillosis and mucormycosis in leukemia and hematopoietic stem cell transplant patients. Haematologica. 2017;102(3):433–444. doi:10.3324/haematol.2016.152900
12. Ullmann AJ, Aguado JM, Arikan-Akdagli S, et al. Diagnosis and management of Aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin Microbiol Infect. 2018;24:e1–e38. doi:10.1016/j.cmi.2018.01.002
13. Abdul-Aziz MH, Alffenaar J-WC, Bassetti M, et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: a position paper. Intensive Care Med. 2020;46(6):1127–1153. doi:10.1007/s00134-020-06050-1
14. Chen L, Wang Y, Zhang T, et al. Utility of posaconazole therapeutic drug monitoring and assessment of plasma concentration threshold for effective prophylaxis of invasive fungal infections: a meta-analysis with trial sequential analysis. BMC Infect Dis. 2018;18:155. doi:10.1186/s12879-018-3055-3
15. Tang LA, Marini BL, Benitez L, et al. Risk factors for subtherapeutic levels of posaconazole tablet. J Antimicrob Chemother. 2017;72(10):2902–2905. doi:10.1093/jac/dkx228
16. Lin H-Y, Hu S-C, Pai T-Y, et al. Plasma concentrations of prophylactic posaconazole and risk factors for subtherapeutic exposure in taiwanese patients with hematologic malignancies. Drug Des Devel Ther. 2025;19:11941–11949. doi:10.2147/DDDT.S557802
17. Miceli MH, Perissinotti AJ, Kauffman CA, et al. Serum posaconazole levels among haematological cancer patients taking extended release tablets is affected by body weight and diarrhoea: single centre retrospective analysis. Mycoses. 2015;58(7):432–436. doi:10.1111/myc.12339
18. Wasmann RE, Smit C, Van Donselaar MH, et al. Implications for IV posaconazole dosing in the era of obesity. J Antimicrob Chemother. 2020;75(4):1006–1013. doi:10.1093/jac/dkz546
19. Schauwvlieghe AFAD, Buil JB, Verweij PE, et al. High-dose posaconazole for azole-resistant aspergillosis and other difficult-to-treat mould infections. Mycoses. 2020;63(2):122–130. doi:10.1111/myc.13028
20. Ashbee HR, Barnes RA, Johnson EM, et al. Therapeutic drug monitoring (TDM) of antifungal agents: guidelines from the British Society for Medical Mycology. J Antimicrob Chemother. 2014;69(5):1162–1176. doi:10.1093/jac/dkt508
21. Cornely OA, Duarte RF, Haider S, et al. Phase 3 pharmacokinetics and safety study of a posaconazole tablet formulation in patients at risk for invasive fungal disease. J Antimicrob Chemother. 2016;71(3):718–726. doi:10.1093/jac/dkv380
22. Patel A, Patel K, Patel K, et al. Therapeutic drug monitoring of posaconazole delayed release tablet while managing COVID-19-associated mucormycosis in a real-life setting. Mycoses. 2022;65(3):312–316. doi:10.1111/myc.13420
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Voriconazole-Induced Hepatotoxicity in a Patient with Pulmonary Aspergillosis: A Case Report
Gu L, Ai T, Pang L, Xu D, Wang H
Infection and Drug Resistance 2023, 16:5405-5411
Published Date: 18 August 2023
Plasma Concentrations of Prophylactic Posaconazole and Risk Factors for Subtherapeutic Exposure in Taiwanese Patients with Hematologic Malignancies
Lin HY, Hu SC, Pai TY, Lin FJ, Wu CC
Drug Design, Development and Therapy 2025, 19:11941-11949
Published Date: 30 December 2025