Back to Journals » Drug Design, Development and Therapy » Volume 19
Plasma Concentrations of Prophylactic Posaconazole and Risk Factors for Subtherapeutic Exposure in Taiwanese Patients with Hematologic Malignancies
Authors Lin HY, Hu SC, Pai TY, Lin FJ ![]() , Wu CC
, Wu CC ![]()
Received 2 August 2025
Accepted for publication 23 December 2025
Published 30 December 2025 Volume 2025:19 Pages 11941—11949
DOI https://doi.org/10.2147/DDDT.S557802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Leonidas D. Panos
Hsing-Yu Lin,1,* Shu-Chen Hu,2,* Tsung-Yu Pai,1 Fang-Ju Lin,1,3,4 Chien-Chih Wu1,3
1Department of Pharmacy, National Taiwan University Hospital, College of Medicine, National Taiwan University, Taipei, Taiwan; 2Department of Pharmacy, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 3School of Pharmacy, College of Medicine, National Taiwan University, Taipei, Taiwan; 4Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, Taipei, Taiwan
*These authors contributed equally to this work
Correspondence: Chien-Chih Wu, Department of Pharmacy, National Taiwan University Hospital, College of Medicine, National Taiwan University, 7 Chung Shan S. Road, Taipei, Taiwan, Email [email protected]
Background: Posaconazole is widely used for antifungal prophylaxis in patients with hematologic malignancies. However, interindividual pharmacokinetic variability may lead to subtherapeutic exposure and treatment failure. Real-world data on the pharmacokinetics of posaconazole tablets and infusion in East Asian populations remain limited. This study aims to evaluate the plasma concentration of posaconazole and risk factors for subtherapeutic exposure in Taiwanese patients.
Methods: This nested case-control study was conducted using data from the National Taiwan University Hospital database. The study cohort comprised adult patients with hematologic malignancies receiving delayed-release tablets or intravenous formulations of posaconazole and undergoing therapeutic drug monitoring. Factors associated with subtherapeutic posaconazole exposure (< 0.7 μg/mL) were identified through multivariate logistic regression. Supratherapeutic concentration was defined as a level > 1.83 μg/mL.
Results: Of a total of 221 patients, 24.9% and 24.0% exhibited subtherapeutic and supratherapeutic posaconazole concentrations, respectively. Multivariate logistic regression indicated that male sex (odds ratio [OR] = 2.31), diarrhea (OR = 2.18), and concurrent use of proton pump inhibitors (OR = 2.00) or prokinetic agents (OR = 2.17) were independently associated with subtherapeutic exposure to posaconazole.
Conclusion: Subtherapeutic and supratherapeutic exposures to posaconazole remain a concern despite standard dosing. Therapeutic drug monitoring and personalized risk assessment are essential for optimizing antifungal prophylaxis in patients with hematologic malignancies.
Keywords: posaconazole, therapeutic drug monitoring, antifungal prophylaxis, hematologic malignancies
Introduction
Posaconazole is a broad-spectrum triazole antifungal agent that is widely used for the prophylaxis and treatment of invasive fungal infections (IFIs), particularly in immunocompromised patients, such as those with hematologic malignancies and those undergoing hematopoietic stem cell transplantation.1 Evidence suggests that posaconazole effectively treats infections caused by mold species, such as Aspergillus and Mucor, by inhibiting the synthesis of ergosterol—a key component of fungal cell membranes.2 Despite the efficacy of posaconazole, its pharmacokinetics exhibits interindividual variability, attributable to factors such as drug formulation, concomitant medication use, albumin level, body weight, gastrointestinal function, and genetic polymorphisms in drug-metabolizing enzymes.3–6 This variability may lead to subtherapeutic or supratherapeutic drug concentrations in plasma, influencing treatment success and safety.7 Higher plasma concentrations of posaconazole have been associated with more favorable clinical outcomes.8 Therefore, researchers have recommended therapeutic drug monitoring (TDM) to guide dose adjustment and ensure optimal exposure.8,9 Current TDM guidelines recommend posaconazole trough concentrations of ≥0.7 μg/mL for prophylaxis and ≥1.0–1.25 μg/mL for treatment, with a suggested upper limit of 3.75 μg/mL.10 However, one study reported that a concentration of >1.83 μg/mL was associated with hepatotoxicity.11,12
Three formulations of posaconazole are currently available for clinical use: an oral suspension, a delayed-release tablet, and an intravenous injection. The oral suspension exhibits variable and food-dependent bioavailability, and its absorption is substantially compromised by gastrointestinal disturbances, mucositis, or concomitant use of acid-suppressive agents.13 Consequently, many patients, particularly those who are immunocompromised, fail to achieve target serum concentrations when using oral suspension.14 By contrast, the delayed-release tablet exhibits improved and predictable absorption, given that it dissolves in the small intestine and is less influenced by gastric pH or food intake. This tablet form facilitates the attainment of therapeutic drug levels.6,9
A fixed-dose regimen (300 mg twice on day 1, followed by 300 mg once daily) is recommended in patients receiving the delayed-release tablet or infusion of posaconazole. However, pharmacokinetic evidence indicates that body weight is an important determinant of posaconazole exposure.4 Several real-world studies have also identified body weight as a significant risk factor for failing to achieve target concentrations.15,16 Because Asian populations generally have lower body weight than Western populations, the plasma concentrations distribution of posaconazole may differ substantially between these groups.
Prior studies in East Asian populations have largely examined the oral suspension, were limited by small sample sizes, and rarely assessed protein-binding–related factors such as total bilirubin.9,17,18 Moreover, most investigations have focused exclusively on subtherapeutic concentrations, with minimal characterization of supratherapeutic exposure that may have safety implications.9,17–19 Real-world pharmacokinetic data for the delayed-release tablet and intravenous formulations in Taiwanese populations remain particularly scarce. To address these gaps, we conducted the largest real-world analysis of posaconazole plasma concentrations in Taiwanese patients with hematologic malignancies receiving antifungal prophylaxis, using both tablet and intravenous formulations. This study provides a comprehensive evaluation of the full exposure range (including both subtherapeutic and supratherapeutic levels) examines exploratory associations with breakthrough IFIs, and identifies clinically relevant factors contributing to inadequate posaconazole exposure.
Methods
Study Design and Data Source
This nested case-control study was conducted using data from the Integrated Medical Database of National Taiwan University Hospital. This database was established in 2013 to facilitate the use of extensive clinical data for medical services and research. It contains comprehensive outpatient, inpatient, and emergency department records, which are accessible to authorized researchers for investigative and academic purposes.20 The study protocol was approved by the Research Ethics Committee of National Taiwan University Hospital (approval number: 202208071RINA). Because the data were deidentified, no informed consent was required. This study was conducted in accordance with the Declaration of Helsinki.
Study Cohort and Selection Criteria
This study included individuals aged ≥18 years who received a diagnosis of a hematologic malignancy between July 1, 2016, and December 31, 2020. Hematologic malignancies were identified using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes. Patients with acute myeloid leukemia (ICD-10-CM codes: C92.XX, C93.XX, C95.0X, and C95.9X), those with myelodysplastic syndromes (ICD-10-CM code: C94.6), and those who had undergone allogeneic hematopoietic cell transplantation (ICD-10-CM codes: Z94.81 and Z94.84) were considered to have hematologic malignancies. Eligible patients were required to have received posaconazole in a delayed-release tablet or infusion for prophylaxis against IFIs during the study period. In Taiwan, posaconazole prophylaxis is reimbursed only for specific high-risk patients: those ≥13 years with grade III–IV acute graft versus host disease requiring high-dose steroids after hematopoietic stem cell transplantation, and patients with acute myeloid leukemia or high-risk myelodysplastic syndrome undergoing high-intensive induction chemotherapy regimens.
Patients who had at least one posaconazole TDM record after the achievement of steady-state concentrations, defined as at least 5 days after the initial posaconazole dose, and those who received a standard posaconazole dose of 300 mg daily were included in this study. Patients whose first posaconazole TDM results were not recorded during hospitalization were excluded from this study.
The study cohort was divided into a case group and a control group on the basis of the plasma concentration of posaconazole. Patients with posaconazole concentrations of <0.7 μg/mL were assigned to the case group, whereas those with posaconazole concentrations of ≥0.7 μg/mL were assigned to the control group.
Covariates
Statistical models used in this study were adjusted for several potential risk factors and patient characteristics. These covariates included age, sex, body weight, body mass index, poor oral intake, diarrhea, concomitant medication use, loading dose administration, posaconazole dosage form, hepatic and renal function, C-reactive protein (CRP) level, and serum albumin level. Concomitant medications of interest included proton pump inhibitors (PPIs), H2 receptor antagonists, prokinetic agents (metoclopramide, domperidone, and mosapride), posaconazole metabolic inducers (eg, lorazepam and rifampin), and metabolic inhibitors (eg, cobicistat). Poor oral intake was defined as being nil per os (NPO), receiving intravenous nutrition, or consuming less than 50% of daily nutritional requirements during the four days prior to the TDM measurement.
Clinical Outcomes
A breakthrough IFI is defined as an invasive fungal infection that occurs while the patient is receiving antifungal prophylaxis or treatment. Due to the limitations inherent in a retrospective study design, we adapted the definitions of possible IFI and probable IFI based on the criteria of the European Organization for Research and Treatment of Cancer’s Mycoses Study Group.21 In this study, possible IFI was defined as a switch from posaconazole to another antifungal agent occurring between 5 days after the initiation of posaconazole and 1 day after its discontinuation. Probable IFI was defined as possible IFI accompanied by positive microbiological findings, such as two consecutive serum Aspergillus antigen levels >0.5, a positive cryptococcal antigen test, or a positive fungal culture. Clinical outcomes were assessed until patient discharge. For patients whose posaconazole prophylaxis was discontinued before discharge, an additional follow-up period of two weeks after discontinuation was included.
Statistical Analysis
Patient characteristics were compared between the case and control groups to identify potential risk factors for subtherapeutic posaconazole exposure. Categorical variables are presented as number (percentage) values, whereas continuous variables are presented as median (first quartile, third quartile) values. The normality of continuous variables was assessed using the Shapiro–Wilk test. Variables that met the assumption of normal distribution were analyzed using the independent t-test, whereas non-normally distributed variables were evaluated using the Mann–Whitney U-test. The chi-square or Fisher exact test were used for the categorical variables.
To identify independent risk factors after covariate adjustment, multivariate logistic regression was performed using the backward selection method for variable inclusion. Adjusted odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were calculated. All variables were initially entered into a regression model, and the variable with the highest P value was sequentially removed. This process continued until all remaining variables had a P value of <0.15. Variables with a P value of <0.05 were considered statistically significant in the final model. Data were managed and analyzed using SAS (version 9.4; SAS Institute, Cary, NC, USA).
Results
We initially identified 4026 patients with hematologic malignancies. Of them, 221 patients met the eligibility criteria and were thus included in this study. The case and control groups comprised 55 and 166 patients, respectively. Figure 1 presents a flowchart depicting patient selection.
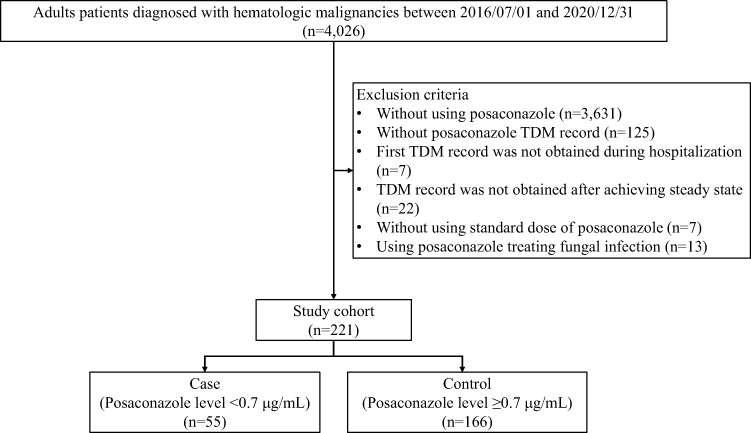 |
Figure 1 Flowchart depicting patient selection. |
Table 1 presents the baseline characteristics of the study cohort. The proportions of patients with posaconazole concentrations of <0.7, 0.7–1.83, and >1.83 μg/mL were 24.9%, 51.1%, and 24.0%, respectively. The proportion of male patients was higher in the case group than in the control group (61.8% vs 44.6%). Furthermore, the prevalence of hyperbilirubinemia, hypoalbuminemia, diarrhea, poor oral intake, and concomitant PPI or prokinetic agent use was higher in the case group than in the control group. By contrast, the level of CRP was higher in the control group than in the case group (3.61 vs 2.47 mg/dL).
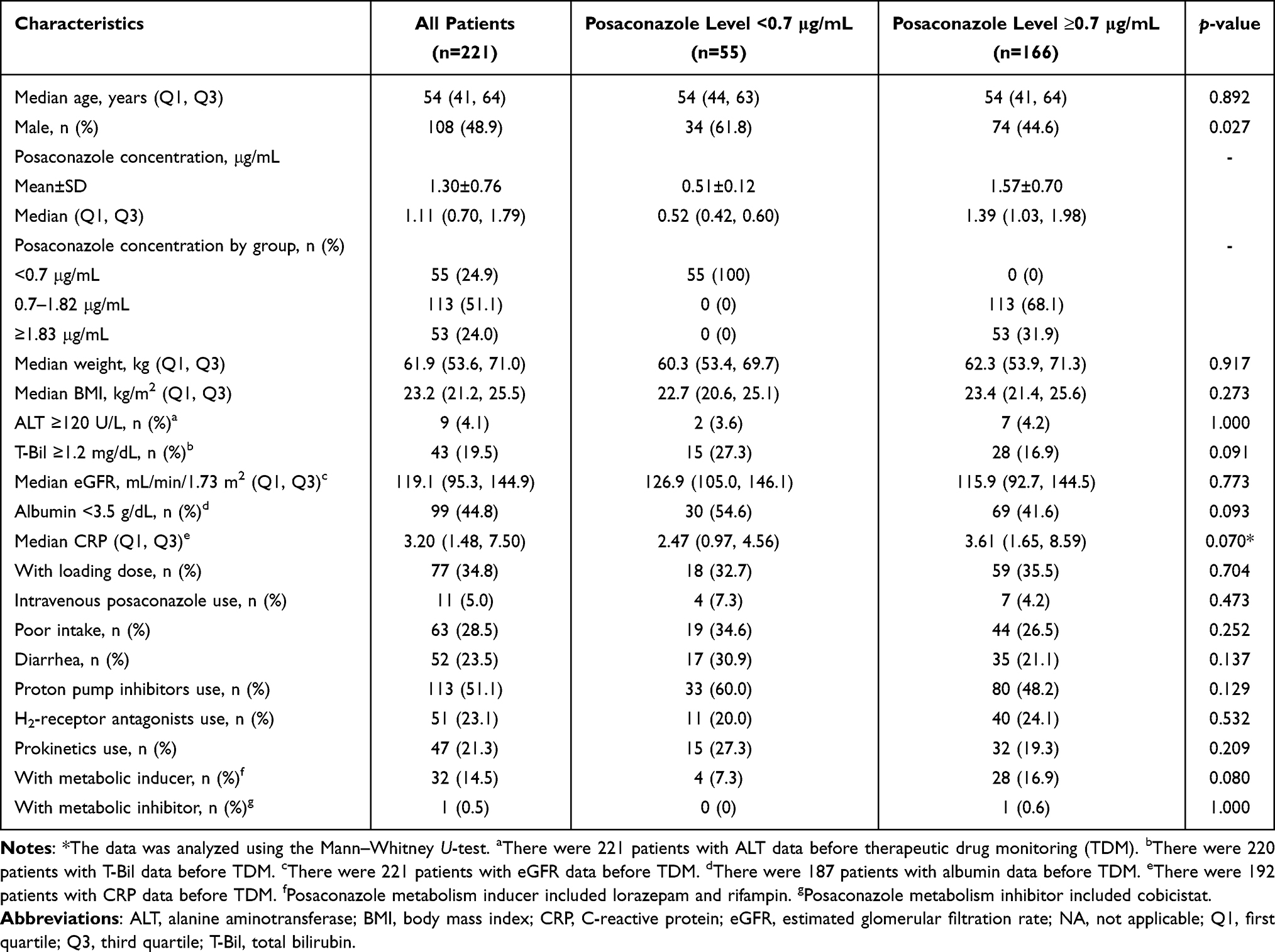 |
Table 1 Baseline Characteristics of the Overall Study Cohort, Case and Control Groups |
Table 2 presents the results of the univariate and multivariate analyses. In the univariate analysis, most potential risk factors were not significantly associated with subtherapeutic posaconazole exposure, except for male sex. After all candidate variables were included and backward selection was performed, the multivariate model retained six variables. Among these variables, male sex (OR = 2.31, 95% CI = 1.17–4.56), diarrhea (OR = 2.18, 95% CI = 1.04–4.54), PPI use (OR = 2.00, 95% CI = 1.01–4.66), and prokinetic agent use (OR = 2.17, 95% CI = 1.01–4.66) were significantly associated with an increased risk of subtherapeutic posaconazole exposure. In the analysis of fungal infection, the case group showed numerically higher rates of breakthrough invasive fungal infections (30.9% vs 20.5%) and in-hospital mortality (10.9% vs 7.2%) compared with the control group. (Table 3).
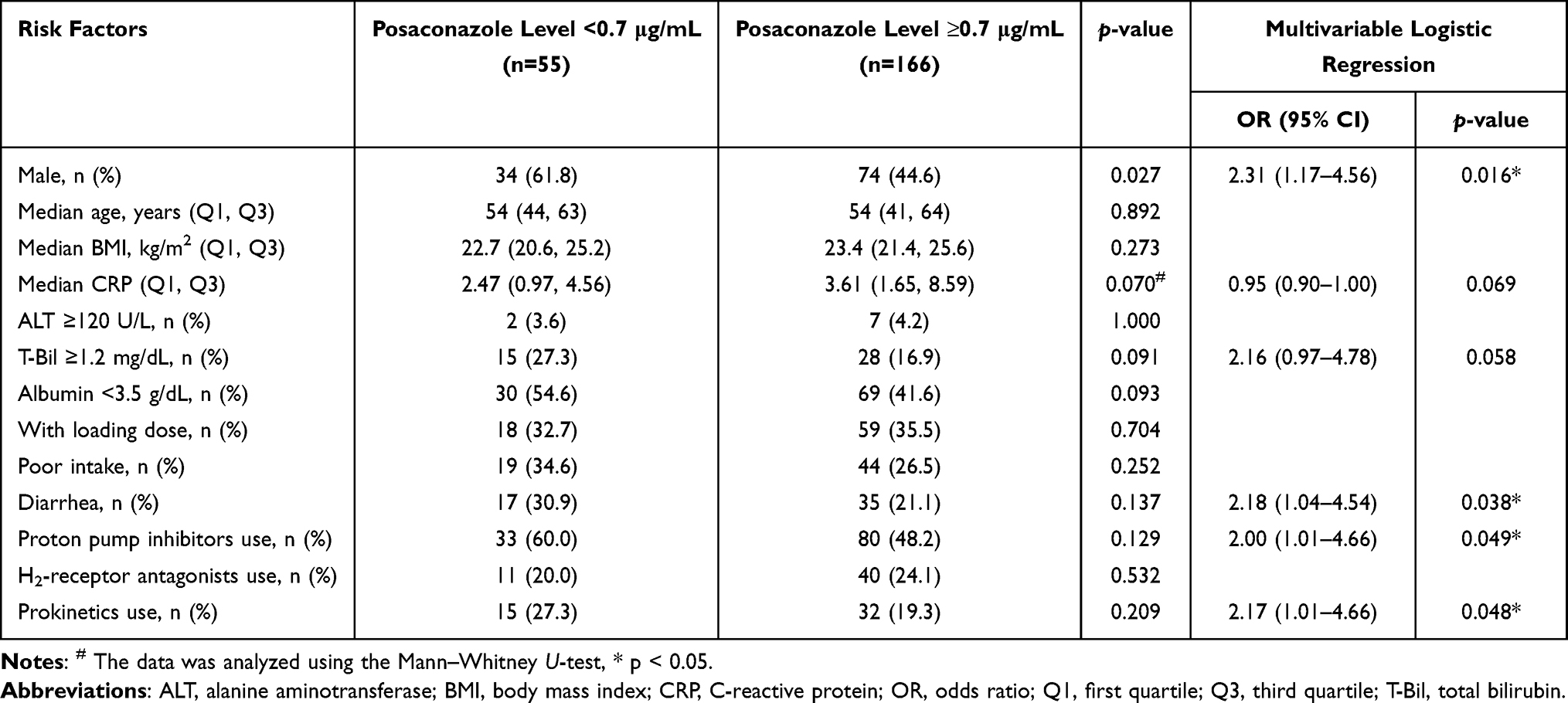 |
Table 2 Risk Factors for Subtherapeutic Posaconazole Concentrations |
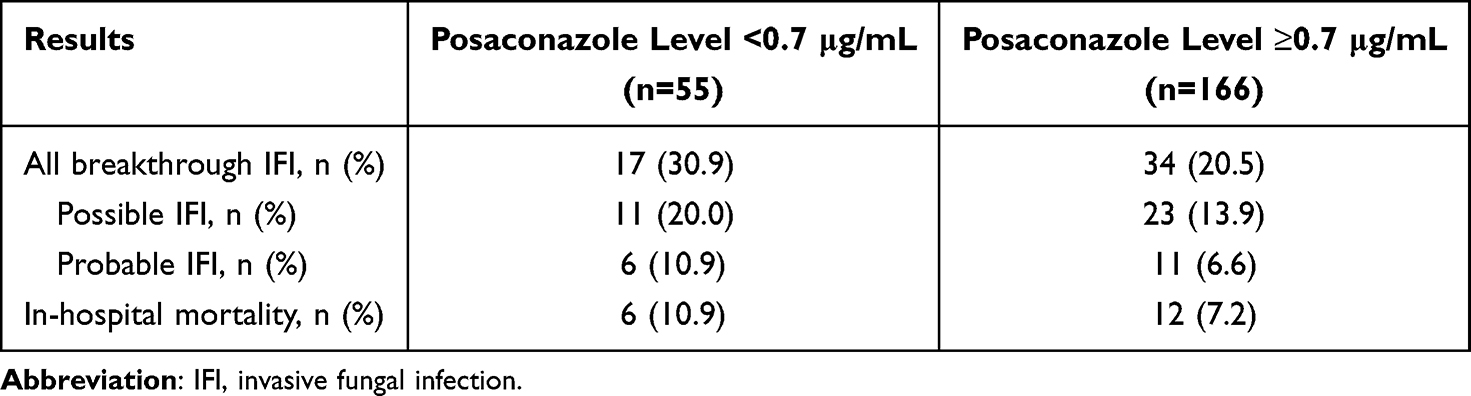 |
Table 3 Rates of Breakthrough IFIs and Mortality in the Case and Control Groups |
Discussion
In this study, we explored the real-world plasma concentrations of posaconazole in Taiwanese patients with hematologic malignancies receiving antifungal prophylaxis. We further identified key risk factors for subtherapeutic posaconazole exposure. Of the included patients, 24.9% failed to achieve the recommended prophylactic trough concentration of ≥0.7 μg/mL despite receiving a standard posaconazole dosage in a delayed-release tablet or intravenous injection form. Notably, male sex, diarrhea, and concomitant PPI or prokinetic agent use were independently associated with an increased risk of subtherapeutic posaconazole exposure. In addition, hyperbilirubinemia was associated with a trend toward reduced drug exposure, and biomarkers of inflammation tended to correlate with increased concentrations, although the between-group differences were nonsignificant.
The multivariate analysis indicated male sex, diarrhea, and concomitant PPI or prokinetic agent use as significant risk factors for subtherapeutic posaconazole exposure. This finding is consistent with those of studies indicating that PPI use increases the risk of subtherapeutic posaconazole exposure, likely by altering gastrointestinal pH, which in turn impairs the solubility and absorption of posaconazole, even in its delayed-release form.18,22 Although the tablet form of posaconazole was developed to address pH-dependent absorption problems, impaired absorption is observed with PPI use in certain patients, necessitating continued TDM. In the present study, diarrhea and concomitant use of prokinetic agents such as metoclopramide were significantly associated with reduced drug exposure. Bui et al23 reported that both diarrhea and regular metoclopramide use were significantly associated with subtherapeutic concentrations of posaconazole in the tablet form. The mechanism by which diarrhea affects absorption is likely related to reduced gastrointestinal transit time, which leads to inadequate drug dissolution and intestinal uptake.23 Prokinetic agents may accelerate gastric emptying and intestinal motility, thereby reducing the duration of posaconazole exposure to absorptive surfaces in the small intestine.24 These findings collectively highlight the need for caution and close monitoring in patients with gastrointestinal dysfunction and in those on medications affecting intestinal motility. In our cohort, male sex was identified as another independent risk factor for subtherapeutic posaconazole concentration. A study reported that male patients were more likely than female patients to exhibit low posaconazole concentrations.23 Our finding may be attributable to sex-based differences in body composition, particularly higher body weight in male individuals than in female individuals (69.0 vs 55.5 kg, p<0.001, Supplemental Table 1), which may result in a larger distribution volume and lower plasma concentrations in men than in women. Although posaconazole is a highly lipophilic drug, higher body weight in males does not necessarily reflect greater adiposity; it may instead be attributed to increased muscle and bone mass. Previous studies have also demonstrated an association between male sex and subtherapeutic posaconazole concentrations even after adjustment for body weight, suggesting that factors beyond body mass such as hepatic metabolism or gastric transit time may contribute to these differences.22,23
Our findings indicated that hypoalbuminemia and hyperbilirubinemia influenced posaconazole exposure. Posaconazole is a highly protein-bound antifungal agent (>98%) whose total plasma concentration is strongly determined by the serum level of albumin.2 In patients with hypoalbuminemia, total drug concentrations may appear deceptively low, although the pharmacologically active unbound fraction remains within the therapeutic range. Evidence suggests that relying exclusively on total concentrations for TDM can lead to inappropriate dose escalation and increased toxicity in patients with hypoalbuminemia.25 Therefore, total concentrations must be corrected using albumin-adjusted formulas (eg, Cadj = Ctotal × 4.4/Alb), similar to phenytoin correction.25 Elevated total bilirubin level may also alter protein binding by posaconazole. Bilirubin competes with posaconazole for the binding sites on albumin, potentially displacing the drug and increasing its unbound fraction.26 As in hypoalbuminemia, this increase in free drug concentration corresponds to a reduction in the measured total drug concentration, leading to the misinterpretation of subtherapeutic exposure. Moreover, because the unbound fraction is available for hepatic metabolism, the displacement may accelerate drug clearance, further reducing the total concentration. Overall, these dynamics underscore a key limitation of conventional total-level TDM and highlight the need for unbound posaconazole monitoring, particularly in patients with hepatic dysfunction or altered protein-binding profiles.
Our findings emphasize the clinical implications of subtherapeutic and supratherapeutic concentrations of posaconazole. In our cohort, approximately 25% of the patients exhibited subtherapeutic posaconazole concentrations, consistent with the findings of a real-world study, where many patients failed to achieve target exposure despite receiving the tablet form of posaconazole.27 Although baseline characteristics were not adjusted, the case group exhibited numerically higher rates of breakthrough IFIs and in-hospital mortality than did the control group, consistent with the findings of studies associating lower posaconazole concentrations with higher fungal infection risks.8,9 In the present study, high concentrations of posaconazole were observed in the cohort, with approximately 25% of the patients having concentrations exceeding 1.83 μg/mL, a threshold previously associated with an increased risk of hepatotoxicity.11 Although the current consensus indicates a posaconazole upper limit of 3.75 μg/mL, hepatotoxicity has been reported at lower thresholds in populations with hematologic malignancies, emphasizing the need to consider personalized risk assessment and avoid exclusive reliance on fixed cutoffs.10
We investigated the effect of systemic inflammation on the pharmacokinetics of posaconazole. Inflammatory states, commonly reflected by elevated CRP levels, suppress the expression and activity of hepatic drug-metabolizing enzymes and transporters, particularly cytochrome P450 enzymes such as CYP3A4.28 This inflammation-mediated downregulation has been extensively documented in the context of voriconazole, where it contributes to elevated plasma levels and increased toxicity under inflammatory conditions.29 Although posaconazole is structurally similar to voriconazole, the drugs differ substantially in terms of metabolism. Posaconazole undergoes minimal CYP-mediated metabolism and is primarily eliminated through glucuronidation by UGT enzymes, particularly UGT1A4.2 Systemic inflammation downregulates the expression and activity of UGT enzymes; consequently, glucuronidation-based metabolism is compromised.28 However, in our cohort, no significant correlation was noted between CRP level and the total posaconazole concentration. This finding may be attributable to the relatively small contribution of hepatic metabolism to the overall clearance of posaconazole, given that the drug is largely excreted without any change through the fecal route. Consistent with our study, a prospective study by Märtson et al30 revealed no significant association between CRP level and posaconazole trough concentration, confirming that systemic inflammation exerts a negligible effect on the pharmacokinetics of posaconazole. Together, the findings suggest that inflammation does not substantially affect the disposition of posaconazole in most clinical settings.
This study has several limitations. First, its retrospective and single-center design may limit the generalizability of our findings to broader populations or different clinical settings. Second, only total plasma concentrations of posaconazole were measured, without corresponding free drug concentrations. Because posaconazole is a highly protein-bound agent, the total concentration may not fully reflect the pharmacologically active fraction of this drug, particularly in patients with hypoalbuminemia or hyperbilirubinemia, which can alter drug-protein binding and may lead to TDM misinterpretation. Third, although numerical differences were observed in clinical outcomes such as breakthrough IFIs and in-hospital mortality, the definitions of possible and probable IFI in our study differed from the EORTC/MSG criteria due to data limitations. These findings were not adjusted for baseline characteristics and should therefore be interpreted with caution and considered exploratory. Finally, we did not consider the presence of genetic polymorphisms or the activity of hepatic enzyme—factors that may influence the metabolism and disposition of posaconazole. Future studies should incorporate pharmacogenomic and free drug concentration monitoring to offer comprehensive insights into interindividual variability in posaconazole pharmacokinetics.
Conclusion
Many Taiwanese patients with hematologic malignancies do not achieve the target concentration of posaconazole despite standard dosing. Our findings suggest that male sex, diarrhea, and concomitant PPI and prokinetic agent use are associated with an increased risk of subtherapeutic posaconazole exposure. Furthermore, inflammation appears to have a minimal effect on posaconazole concentration. Both subtherapeutic and supratherapeutic concentrations of posaconazole are common. Notably, patients with subtherapeutic exposure exhibited numerically higher rates of breakthrough invasive fungal infections compared with those who achieved adequate concentrations, although these exploratory findings were not adjusted for baseline differences. Collectively, these observations highlight the importance of individualized dose optimization and close monitoring to ensure adequate prophylactic coverage in this high-risk population.
Data Sharing Statement
The data used and analyzed in this study are available from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
The study protocol was approved by the Institutional Review Board of National Taiwan University Hospital (approval number: 202208071RINA). Given the retrospective nature of this study, the requirement for informed consent was waived. All patient identifiers were removed before analysis. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
Hsing-Yu Lin and Shu-Chen Hu contributed equally to this work and are co-first authors. The authors thank the staff members at the Department of Medical Research, National Taiwan University Hospital, and those at the Integrative Medical Data Center. Furthermore, the authors acknowledge the use of OpenAI’s ChatGPT-4 for revising and refining the language and structure of this manuscript. This artificial intelligence tool was used to enhance the clarity and readability of the text. The authors take full responsibility for the content, analysis, and conclusions presented in the article.
Funding
This study was supported by National Taiwan University Hospital (grant number: NTUH 113-S0036). The funding agency played no role in study design; data collection, analysis, or interpretation; manuscript preparation; or decision to submit the manuscript for publication.
Disclosure
The authors report no competing interests.
References
1. Frampton JE, Scott LJ. Posaconazole: a review of its use in the prophylaxis of invasive fungal infections. Drugs. 2008;68(7):993–1016. doi:10.2165/00003495-200868070-00008
2. Leung S, Poulakos MN, Machin J. Posaconazole: an update of its clinical use. Pharmacy. 2015;3(4):210–268. doi:10.3390/pharmacy3040210
3. Suh HJ, Yoon SH, Yu KS, et al. The genetic polymorphism UGT1A4*3 is associated with low posaconazole plasma concentrations in hematological malignancy patients receiving the oral suspension. Antimicrob Agents Chemother. 2018;62(7). doi:10.1128/AAC.02230-17
4. Ding Q, Huang S, Sun Z, Chen K, Li X, Pei Q. A review of population pharmacokinetic models of posaconazole. Drug Des Devel Ther. 2022;16:3691–3709. doi:10.2147/DDDT.S384637
5. Jia MM, Zhang QW, Qin ZF, et al. Deciphering the relationship between the trough concentration of posaconazole and its efficacy and safety in Chinese patients with hematological disorders. Front Pharmacol. 2020;11:575463. doi:10.3389/fphar.2020.575463
6. Durani U, Tosh PK, Barreto JN, Estes LL, Jannetto PJ, Tande AJ. Retrospective comparison of posaconazole levels in patients taking the delayed-release tablet versus the oral suspension. Antimicrob Agents Chemother. 2015;59(8):4914–4918. doi:10.1128/AAC.00496-15
7. Hong JY, Kang C-I, Yang J, et al. Breakthrough invasive fungal infection in patients with myeloid malignancy receiving posaconazole tablet prophylaxis: clinical features, risk factors, and posaconazole profiles. Med Mycol. 2023;61(5). doi:10.1093/mmy/myad046
8. Jang SH, Colangelo PM, Gobburu JV. Exposure-response of posaconazole used for prophylaxis against invasive fungal infections: evaluating the need to adjust doses based on drug concentrations in plasma. Clin Pharmacol Ther. 2010;88(1):115–119. doi:10.1038/clpt.2010.64
9. Oh J, Kang CI, Kim SH, et al. Antifungal prophylaxis with posaconazole tablet and oral suspension in patients with haematologic malignancy: therapeutic drug monitoring, efficacy and risk factors for the suboptimal level. Mycoses. 2020;63(1):89–94. doi:10.1111/myc.13020
10. Cornely OA, Duarte RF, Haider S, et al. Phase 3 pharmacokinetics and safety study of a posaconazole tablet formulation in patients at risk for invasive fungal disease. J Antimicrob Chemother. 2015;71(3):718–726. doi:10.1093/jac/dkv380
11. Tverdek FP, Heo ST, Aitken SL, Granwehr B, Kontoyiannis DP. Real-life assessment of the safety and effectiveness of the new tablet and intravenous formulations of posaconazole in the prophylaxis of invasive fungal infections via analysis of 343 courses. Antimicrob Agents Chemother. 2017;61(8). doi:10.1128/AAC.00188-17
12. Dekkers BGJ, Bakker M, van der Elst KCM, et al. Therapeutic drug monitoring of posaconazole: an update. Curr Fungal Infect Rep. 2016;10(2):51–61. doi:10.1007/s12281-016-0255-4
13. Pham AN, Bubalo JS, Lewis JS. Comparison of posaconazole serum concentrations from haematological cancer patients on posaconazole tablet and oral suspension for treatment and prevention of invasive fungal infections. Mycoses. 2016;59(4):226–233. doi:10.1111/myc.12452
14. Leclerc E, Combarel D, Uzunov M, Leblond V, Funck-Brentano C, Zahr N. Prevention of invasive aspergillus fungal infections with the suspension and delayed-release tablet formulations of posaconazole in patients with haematologic malignancies. Sci Rep. 2018;8(1):1681. doi:10.1038/s41598-018-20136-3
15. Krekel T, Miller J, Catalano A, Pande A, Klaus J. Evaluation of therapeutic target attainment with various posaconazole formulations. Transpl Infect Dis. 2025;e70105. doi:10.1111/tid.70105
16. Handley G, Greene J, Cannella AP, Velez AP, Shah S, Pasikhova Y. Real-world experience of posaconazole therapeutic drug monitoring in oncology patients: clinical implications of hypoalbuminemia as a predictor of subtherapeutic posaconazole levels. Open Forum Infect Dis. 2024;11(5):ofae185. doi:10.1093/ofid/ofae185
17. Li W, Xia F, Zhou H, et al. Efficacy of posaconazole prophylaxis for fungal disease in hematology patients treated with chemotherapy and transplantation: an open-label, prospective, observational study. Front Microbiol. 2020;11:349. doi:10.3389/fmicb.2020.00349
18. Chae H, Cho SY, Yi Y, et al. Evaluation of posaconazole plasma concentrations achieved with the delayed-release tablets in Korean high-risk patients with haematologic malignancy. Mycoses. 2020;63(2):131–138. doi:10.1111/myc.13031
19. Cao J, Pan P, Feng D, et al. Posaconazole gastro-resistant tablets for preventing invasive fungal disease after haematopoietic stem cell transplantation: a propensity-matched cohort study. Clin Microbiol Infect. 2024;30(12):1585–1591. doi:10.1016/j.cmi.2024.07.019
20. National taiwan university hospital integrative medical data center (2025, April, 9) introduction to medical integration database. Available from: https://wwwntuhgovtw/LARD-IMD/Fpageaction?muid=&fid=6889.
21. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
22. Tang LA, Marini BL, Benitez L, et al. Risk factors for subtherapeutic levels of posaconazole tablet. J Antimicrob Chemother. 2017;72(10):2902–2905. doi:10.1093/jac/dkx228
23. Bui J, Gellatly R, Othman J, Lindsay J. Subtherapeutic concentrations of posaconazole tablet: determining risk factors and effectiveness of a standardized dose adjustment in hematology inpatients. Leuk Lymphoma. 2022;63(14):3418–3425. doi:10.1080/10428194.2022.2126282
24. Krishna G, Moton A, Ma L, Medlock MM, McLeod J. Pharmacokinetics and absorption of posaconazole oral suspension under various gastric conditions in healthy volunteers. Antimicrob Agents Chemother. 2009;53(3):958–966. doi:10.1128/AAC.01034-08
25. Nix DE, Sime F, Roberts JA. Correction of posaconazole concentrations for hypoalbuminemia. Pharmacotherapy. 2025;45(6):324–331. doi:10.1002/phar.70021
26. Wadsworth SJ, Suh B. In vitro displacement of bilirubin by antibiotics and 2-hydroxybenzoylglycine in newborns. Antimicrob Agents Chemother. 1988;32(10):1571–1575. doi:10.1128/AAC.32.10.1571
27. Märtson AG, Veringa A, van den Heuvel ER, et al. Posaconazole therapeutic drug monitoring in clinical practice and longitudinal analysis of the effect of routine laboratory measurements on posaconazole concentrations. Mycoses. 2019;62(8):698–705. doi:10.1111/myc.12948
28. Stanke-Labesque F, Gautier-Veyret E, Chhun S, Guilhaumou R. Inflammation is a major regulator of drug metabolizing enzymes and transporters: consequences for the personalization of drug treatment. Pharmacol Ther. 2020;215:107627. doi:10.1016/j.pharmthera.2020.107627
29. Li X, Lai F, Jiang Z, et al. Effects of inflammation on voriconazole levels: a systematic review. Br J Clin Pharmacol. 2022;88(12):5166–5182. doi:10.1111/bcp.15495
30. Märtson AG, Veringa A, Bakker M, et al. Posaconazole trough concentrations are not influenced by inflammation: a prospective study. Int J Antimicrob Agents. 2019;53(3):325–329. doi:10.1016/j.ijantimicag.2019.01.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors for Subtherapeutic Exposure and Hepatotoxicity Threshold of Posaconazole: A Real-World Study in Chinese Patients with Invasive Pulmonary Fungal Infection
Wang B, Li S, Wang J, Zhang J, Liu H, Jin L
Infection and Drug Resistance 2026, 19:602958
Published Date: 15 June 2026