Back to Journals » Cancer Management and Research » Volume 14
Risk Factors for Colorectal Adenocarcinoma in an Indigenous Population in East Africa
Authors Wismayer R, Kiwanuka J ![]() , Wabinga H, Odida M
, Wabinga H, Odida M
Received 7 July 2022
Accepted for publication 31 August 2022
Published 6 September 2022 Volume 2022:14 Pages 2657—2669
DOI https://doi.org/10.2147/CMAR.S381479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Richard Wismayer,1– 3 Julius Kiwanuka,4 Henry Wabinga,3 Michael Odida3,5
1Department of Surgery, Masaka Regional Referral Hospital, Masaka, Uganda; 2Department of Surgery, Faculty of Health Sciences, Habib Medical School, IUIU University, Kampala, Uganda; 3Department of Pathology, School of Biomedical Sciences, College of Health Sciences, Makerere University, Kampala, Uganda; 4Department of Epidemiology and Biostatistics, School of Public Health, College of Health Sciences, Makerere University, Kampala, Uganda; 5Department of Pathology, Faculty of Medicine, Gulu University, Gulu, Uganda
Correspondence: Richard Wismayer, Department of Surgery, Masaka Regional Referral Hospital, Masaka, Uganda, Email [email protected]
Introduction: The incidence of colorectal cancer (CRC) is increasing in East Africa. Changes in lifestyle and dietary changes, particularly alcohol consumption, smoking, and consumption of cooked meats with a reduction in fibre in the diet may be responsible. The objective of our study was to determine the risk factors responsible for CRC in Uganda.
Methods: We recruited 129 participants with histologically proven colorectal adenocarcinoma and 258 control participants from four specialized hospitals in central Uganda from 2019 to 2021. Controls were block matched for age (± 5 years) and sex of the case participants. The risk factor variables included; area of residence, tribe, body mass index (BMI), smoking, alcohol consumption and family history of gastrointestinal cancer. We used conditional or ordinal logistic regression to obtain crude and adjusted odds ratios for risk factors associated with CRC.
Results: In bivariate analysis, case participants were more likely to be associated with urban residence (cOR:62.11; p< 0.001); family history of GI cancer (cOR: 14.34; p=0.001); past smokers (cOR: 2.10; p=0.080); past alcohol drinkers (cOR: 2.35; p=0.012); current alcohol drinkers (cOR: 3.55; p< 0.001); high BMI 25– 29.9 kg/m2 (cOR: 2.49; p< 0.001); and high BMI ≥ 30kg/m2 (cOR: 2.37; p=0.012). In the multivariate analysis, urban residence (aOR: 82.79; p< 0.001), family history of GI cancer (aOR: 61.09; p< 0.001) and past smoking (aOR: 4.73; p=0.036) were independently associated with a higher risk of developing CRC.
Conclusion: A family history of gastrointestinal cancer was a risk factor for CRC. While population-based CRC screening may not be feasible in low income-countries, targeted CRC screening for first-degree relatives with CRC should be considered in East Africa. Molecular genetic studies need to be carried out to determine the role of hereditary factors in our population. Prevention strategies should be adopted to avoid smoking in our population which was associated with an increased risk of CRC.
Keywords: colorectal cancer, East Africa, risk factors, urban, family history, CRC screening
Introduction
In East Africa, colorectal cancer (CRC) has high morbidity and mortality as it presents at an advanced stage in the affected population.1 As the sixth most common cancer in Sub-Saharan Africa, it contributes significantly to the cancer burden in this part of the world.2,3
Over the last two decades, there has been a steady increase in Ugandan patients presenting with CRC.4 Between the years 1991 and 2010 there has been a 4.1% per year percentage change in the incidence rate for Ugandan female patients. For all patients, during the period 1991–1995, the age-standardized incidence rate was 6.8 per 100,000 and increased to 11.0 per 100,000 for the period 2011–2015. For this time period, there was a 2.2% annual percentage change in the incidence rate of CRC.4,5
In Uganda, although the burden from CRC remains low compared to high-income developed countries, the increase in CRC may be due to an improvement in the diagnosis of this disease. However, an increase in the prevalence of risk factors may also account for the steady increase in CRC.6
In high-incidence countries, five percent of CRC cases are caused by genetic disorders such as familial adenomatous polyposis and hereditary nonpolyposis colorectal carcinoma, and sixty-five per cent are sporadic colorectal cancers caused by lifestyle and dietary factors.7 In Uganda, 40% of CRC patients are under 49 years of age,8 and therefore hereditary factors may also play an important role. However, only 12.4% of colorectal cancers in Uganda exhibit features of signet ring or mucinous histology, which are histological subtypes associated with Lynch syndrome.8 Furthermore, other parts of the world, have also reported an increase in the number of young adults presenting with CRC.9
Changes in lifestyle, in particular smoking and alcohol consumption, and dietary changes such as an increase in the consumption of cooked meats and a reduction in fibre in the diet, may be responsible for the steady increase in CRC in this part of the world. In the USA, alcohol consumption and smoking result in a one in five probability of CRC.10 The risk increases with an increase in BMI with obese individuals having a higher risk. Compared to individuals with a BMI of 23, elderly individuals tend to have a 5–100% higher risk of CRC with a BMI of 30.10
It has been postulated that individuals living in urban areas in Uganda, have a higher risk of certain health behaviours such as decreased physical activity, smoking, alcohol consumption and adoption of a Western diet.11 Furthermore, compared to rural parts of the country, there is also an increased rate of obesity and diabetes. In East Africa, the interplay between environmental and hereditary factors responsible for the aetiology of CRC remains poorly understood.
Therefore, to clarify the uncertainties in the East African context, the objective of our study was to determine the risk factors responsible for CRC in Ugandan patients.
Methodology
Study Design
This was a case-control study.
Study Setting
The study sites were four specialized hospitals, which included Masaka Regional Referral Hospital, Mulago National Referral Hospital, Uganda Martyrs’ Hospital Lubaga and Mengo Hospital. Together, these four sites receive over 100 incident cases of CRC per year. All the health facilities that participated in the study are located in central Uganda and receive patients from all regions of Uganda.
Recruitment of Participants
Consecutive case participants with a histologically proven diagnosis of colorectal adenocarcinoma were recruited prospectively during the study period from September 2019 to September 2021. Controls were randomly selected male or female participants who were recruited from patients with other conditions in the same surgery wards and non-relatives of case participants accompanying or visiting the case participants in the respective hospitals. The participants were socioeconomically and ethnically diverse, representing the patient population that came to the four specialized hospitals in central Uganda and the diversity of the Ugandan population.
Controls came from the same catchment as the cases, and there were two control participants for every case participant recruited to increase the power of this study. Controls were block matched for age (±5 years) and sex of the case participants. To minimize misclassification of undiagnosed cases, controls had a negative faecal occult blood test before final enrolment. The choice of non-relative controls, was to minimize the genetic, environmental and dietary exposure correlation between cases and controls which would have inflated the sample size.
Selection Criteria for Participants
Case participants who had incident histologically proven colorectal adenocarcinoma and were able to provide written informed consent were included. Case participants in poor general health were excluded due to interference with the established patterns of clinical care.
The inclusion criteria for controls included participants with a negative faecal occult blood test who were able to provide written informed consent. Controls did not have any type of cancer as determined from their general physical examination and medical history. Relatives of case participants and participants testing positive for faecal occult blood were excluded as controls. Participants not willing to provide faecal samples for faecal occult blood testing were also excluded as controls.
Those control participants who tested positive for faecal occult blood, were referred for a colonoscopy to the endoscopy units in the respective hospital sites. The two matched controls were delineated as control A and control B. During the matching, the first control to be identified was delineated as “A” and the second as “B”.
Study Variables
The study variables were obtained through the history taken from all the study participants using a pre-coded and pretested interview administered questionnaire. The same interview-administered questionnaire was used for case and control participants. The variables included age, sex, area of residence (urban or rural), tribe, body mass index (BMI), alcohol consumption, smoking, diabetes, use of hormone replacement therapy, family history of colorectal cancer and family history of gastrointestinal cancer.
Age was block matched (±5 years) for case and control participants, while sex was matched for case and control participants. BMI was determined by measuring weight in kilograms per height in metres squared. Smoking use was determined through history taking with a response of “yes” or “no”, including the type, amount and duration of smoking. Alcohol consumption was determined from the history by responding to “yes” or “no”, including the type, amount and duration of alcohol consumption.
Urban residence included participants residing in gazetted urban centres and ungazetted trading centres having a population exceeding 1000 persons according to the 1991 Population and Housing Census (National Population and Housing Census, 2014). Rural residence included all localities and excluding areas of urban residence.88
Quality Assurance and Laboratory Methods
The diagnosis of invasive colorectal adenocarcinoma was confirmed on hematoxylin and eosin staining of the tissue slides. The histopathological type and grade were determined on all the tissue slides. Two experienced consultant pathologists read all the tissue slides for each case participant.
Data Analysis
Data were statistically analyzed using STATA version 14.0. Categorical variables were summarized as percentages, and continuous variables were summarized as the means (standard deviation). In the bivariate analysis, the relationship between CRC status and categorical exposure variables was assessed by using Pearson’s or Fischer’s exact chi-square tests as appropriate. Secondary, crude and adjusted odds ratios of having a given risk factor and their associated 95% confidence intervals were estimated via two forms of logistic regression models depending on model convergence. Thus, we used matched analysis using conditional logistic regression and unmatched analysis using ordinary logistic regression.
Variables in the multivariable models were included in a stepwise fashion and were based on biological plausibility, literature review and a bivariate p-value of up to 0.2. Candidate variables for multivariable modelling were first assessed for collinearity and in all instances, two or more variables with a correlation of at least 40% were not included into the same multivariable model. In the final model, only variables with a p-value <0.05 were considered statistically significant.
Results
A total of 387 participants were included in this study. The study groups were composed of 129 case participants and 258 control participants. The mean age (SD) of the case participants was 54 (16.2) years. The mean age of control A participants was 53.4 (16.1) years and of control B participants was 53.3 (16.3) years. The 129 case participants included 67 (51.9%) colon cases and 61 (46.7%) rectal cases (Table 1).
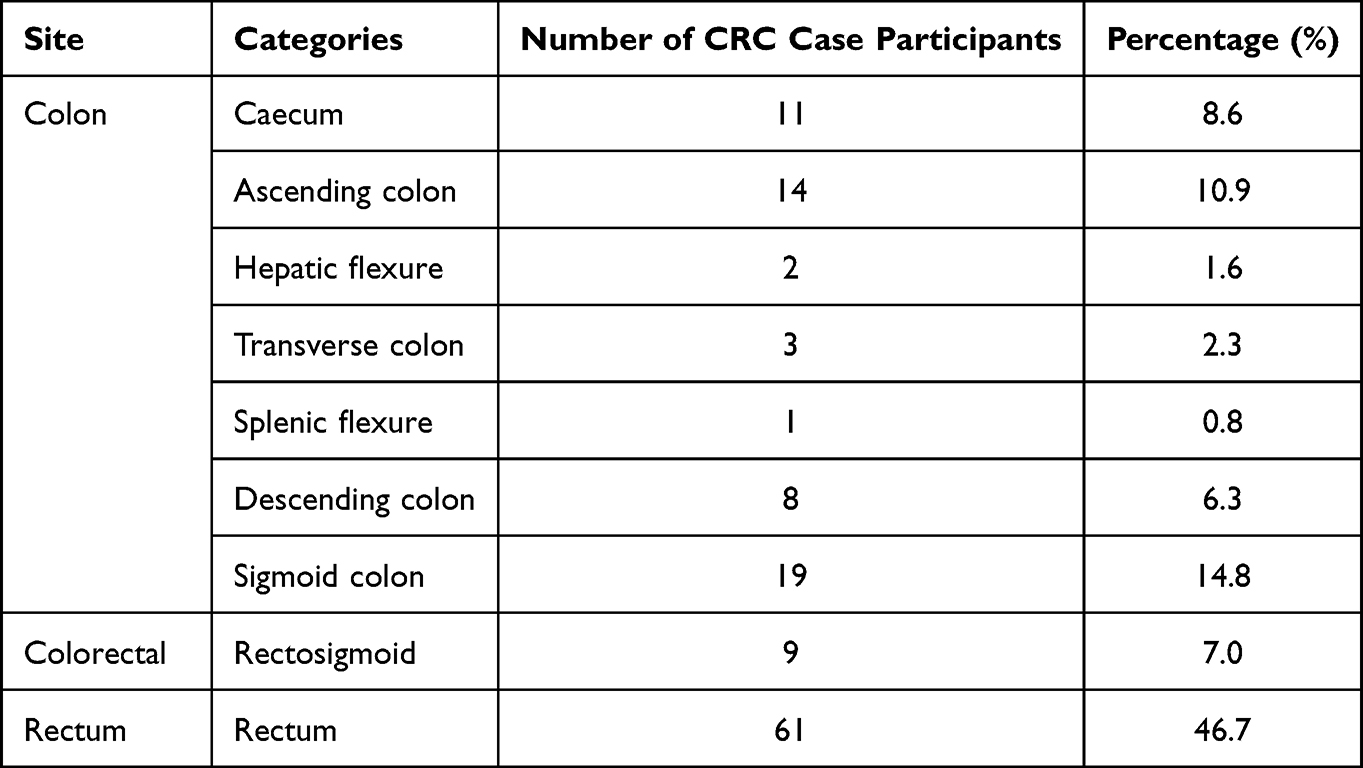 |
Table 1 Distribution of Colorectal Cancer Case Participants |
In Table 2, 61.2% of cases resided in an urban setting compared to 48.5% of controls (p=0.018). Approximately 5% of cases compared to no controls had a family history of CRC (p=0.001) and 10.1% of cases compared to 0.8% of controls had a family history of GI cancer (p<0.001).
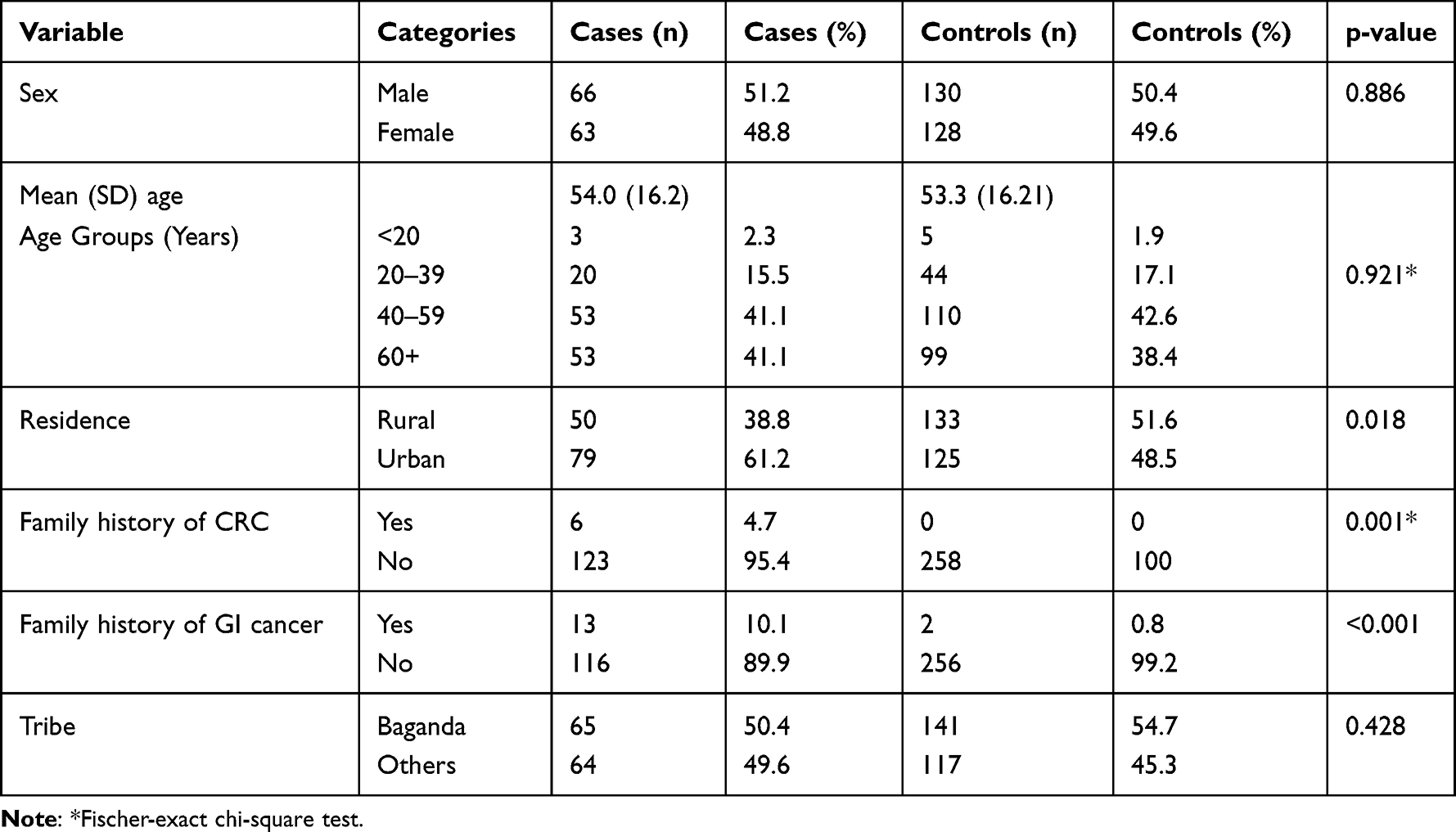 |
Table 2 Descriptive Statistics of Demographics and Family History for Participant Groups |
Demographics and Family History of Colorectal Cancer and Gastrointestinal Cancer
In bivariate analysis, the odds of being a CRC case were higher among patients who resided in an urban setting than among those in a rural setting (cOR=62.11, 95% CI, 30.62–125.99) and among patients with a family history of GI cancer (cOR=14.34, 95% CI, 3.19–64.60). Compared to patients who had never smoked, past smokers were twice as likely to have CRC (cOR=2.10, 95% CI, 0.91–4.82. With alcohol intake, compared to patients who were never drinkers, the odds of having CRC were 2.35 (95% CI, 1.20–4.59) and 3.55 times (95% CI, 1.87–6.75) in patients who were past and current drinkers, respectively. Compared to patients with a BMI of <25, the odds of being a CRC case were more than two times (cOR=2.49, 95% CI, 1.50–4.14) and 2.37 times (95% CI, 1.21–4.64) in patients who had a BMI of 25–29.9 and ≥30, respectively.
Body Mass Index
Case participants having a BMI ≥30kg/m2 were 14.7%. There were 8.5% of control A participants and 8.5% of control B participants who had a BMI ≥30kg/m2. An increased risk of CRC was associated with increasing BMI (p=0.001) (Table 3). The risk of developing CRC in obese patients was 2.37 (cOR:2.37; 95% CI: 1.21–4.64), and in the multivariate analysis, it was 1.23 (aOR:1.23; 95% CI: 0.44–3.41) (Table 4).
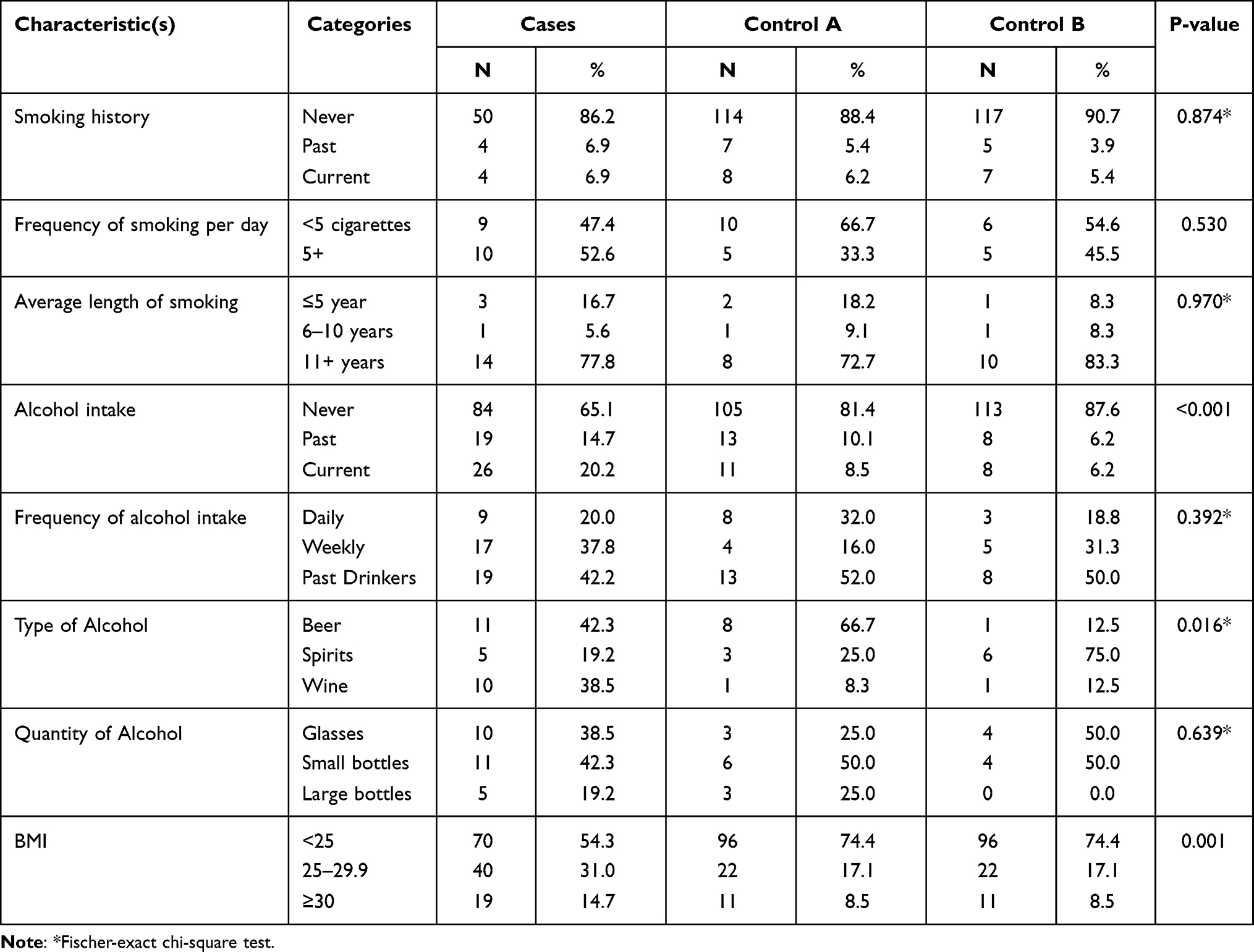 |
Table 3 Descriptive Statistics of Lifestyle Factors for the Participant Groups |
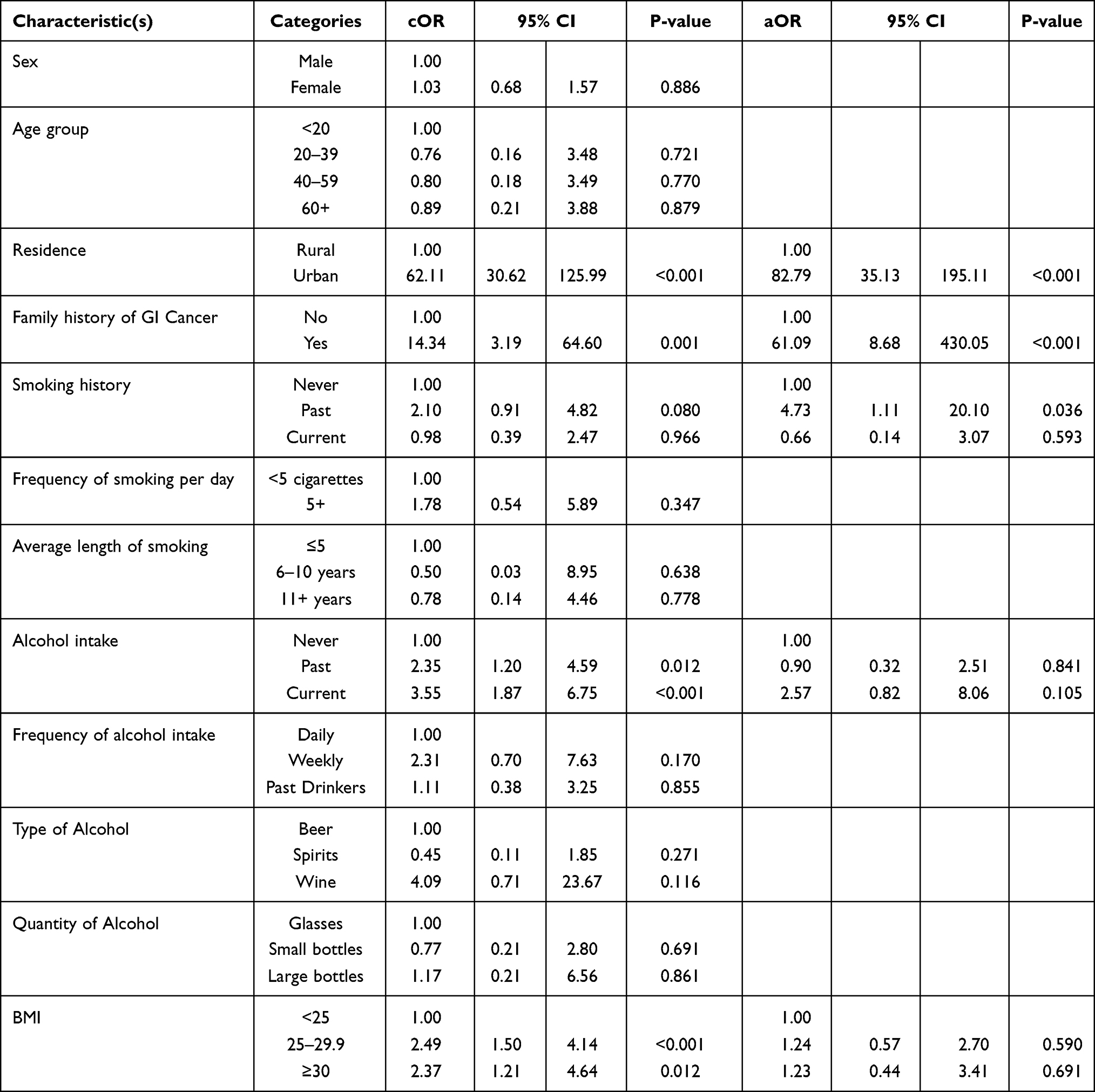 |
Table 4 Multivariate Analysis of Risk Factors Associated with Colorectal Cancer in Ugandan Patients |
Smoking
A total of 6.9% of case participants were past smokers, while 5.4% of control A participants and 3.9% of control B participants were past smokers. A total of 6.9% of case participants were current smokers, while 6.2% of control A participants and 5.4% of control B participants were current smokers. A total of 52.6% of case participants smoked more than 5 cigarettes daily, while 33.3% of control A participants and 45.5% of control B participants smoked more than 5 cigarettes daily. Past smokers had a higher risk of developing CRC at 4.73 (aOR:4.73; p=0.036) (Table 4).
Alcohol Consumption
A total of 14.7% of the case participants drank alcohol in the past, while 10.1% of control A participants and 6.2% of control B participants drank alcohol in the past. A total of 20.2% of case participants currently drank alcohol, while 8.5% of control A participants and 6.2% of control B participants currently drank alcohol. Case participants had a risk of 3.55 if they were currently drinking (cOR:3.55; 95% CI: 1.87–6.75) and a risk of 2.35 when they were past drinkers (cOR: 2.35; 95% CI: 1.20–4.59). In the multivariate analysis, current alcohol drinkers had a 2.57 risk of CRC; however, this did not reach statistical significance (aOR: 2.57; 95% CI: 0.82–8.06) (Table 4).
Tribe
There were 50.4% of case participants from the Baganda tribe and 49.6% from other tribes. The risk of CRC with other tribes was 1.26 (cOR: 1.26; 95% CI: 0.83–1.93), and this did not reach statistical significance (Table 3).
After adjusting for potential confounding factors, urban residence (aOR=82.79, 95% CI, 35.13–195), family history of GI cancer (aOR=61.09, 95% CI, 8.68–430.05) and past smoking (aOR=4.73, 95% CI, 1.11–20.10) were associated with the likelihood of developing CRC (Table 4).
Discussion
This study investigated the risk factors related to CRC in an East African population. In our population, the results show that an urban domicile, family history of gastrointestinal cancer and smoking are associated with CRC. The association between age and sex and CRC could not be determined in our study, as these variables were matched.
An association between colorectal cancer and individuals who lived in urban areas within the country was found in our study. In Sub-Saharan Africa, dietary changes have been associated with urbanization, particularly with a reduction in the consumption of plant-based foods and staple starches and an increased intake of meat and fat energy-dense foods.12 A well-known risk factor for CRC in urban settings is a westernized diet with high consumption of processed meat.13
A higher incidence of CRC in urban areas than in rural areas has also been found in studies from the USA and the Middle East.13–15 Paquette et al showed that there is a significant difference in the incidence of CRC between urban and rural areas.16 In Sub-Saharan Africa, an urban residence has also been found to be associated with a higher incidence of colorectal cancer, which is in keeping with the findings in our study.17 Urbanization is associated with obesity due to a sedentary lifestyle, noncommunicable diseases such as diabetes and behavioural risk factors, in particular smoking and alcohol consumption, which are associated with CRC. However, this difference in the incidence of CRC between rural and urban areas may be due to a difference in access to diagnostic colonoscopy services and health care facilities.18
Urbanization has been found to be associated with high levels of tobacco smoking, and a study has shown a 1.8 times increased incidence of CRC in the urban area of the Ardabil Province of Iran.19 Studies have also shown that urbanization is associated with physical inactivity resulting in a high BMI.15 The prevalence of obesity has been found to be higher in urbanized areas and significantly lower in rural areas.20–22 This increased prevalence of obesity due to physical inactivity increases the incidence of colorectal cancer.15,20 Industrialization may explain the physical inactivity in individuals from urban communities leading to obesity.15 Apart from urban individuals having adopted a westernised diet, they also have a higher prevalence of noncommunicable diseases such as diabetes, smoking and alcohol consumption, which results in a more frequent predisposition to the risk factors associated with CRC.
The presentation of many of our CRC study participants was at an age younger than 40 years. The mean age in our study was 54 years for CRC participants; 17.8% of CRC patients were below the age of 40 years, and 58.9% were below 60 years of age. This is in contrast to findings from the USA whereby only 17.4% of CRC patients present under 54 years of age and in the UK only 16% of CRC patients were diagnosed under the age of 60 years.23–25 Compared to developed countries, Africa reports a lower median age and a higher proportion of individuals presenting with CRC under 50 years of age.23 The reason for the younger age may be due to a shorter life expectancy in a younger population or it may be due to a different CRC tumour biology.23
Globally, the majority of CRC cases occur in individuals with no predisposing disease or familial history. Given the high frequency of CRC presenting at a younger age in Uganda, the role of hereditary factors as a risk factor needs to be explored.26 Compared to Western developed countries, it has been postulated that there is a higher frequency of Lynch syndrome in Uganda. This may be consistent with studies from Sub-Saharan Africa, which have shown a high frequency of mismatch repair protein deficiency in colorectal cancers.27
In our study, the risk was higher for having a history of colon or rectal cancer in the family. Individuals having relatives with CRC have been shown to have a higher predominance of adenomas with two or more adenomas in the colon.28–31 A difference in the location of these adenomas has not been reported in these individuals.28–32 Molecular genetic studies are currently being performed on the colorectal cancer tissues of our patient cohort to determine the frequency of hereditary nonpolyposis colorectal carcinoma in our population and to determine whether adenomas are actually predisposing to CRC in our familial CRC patients. Since the cost of population screening for CRC is high, targeting these individuals with a positive family history of CRC for screening may be feasible in the East African context.
Lack of exercise and obesity have been shown in studies to be important lifestyle factors that are associated with CRC.33,34 A sedentary lifestyle has been found to be an independent risk factor for CRC.33 A sedentary lifestyle leads to obesity, and unequivocally, our study showed a positive correlation of a risk of CRC with increasing BMI. However, our study did not independently examine the effect of a lack of exercise. A recent study showed a fifty percent increased risk of CRC with a sedentary lifestyle.33,34
In obese men, it has been shown that the risk of rectal and colon cancer is twenty percent and fifty percent, respectively.35 A meta-analysis has shown that for every five kilograms increase in body weight, there is a three percent increase in the tendency to develop CRC.10 A high BMI is associated with a fifteen percent risk of developing rectal cancer and a forty-seven percent risk of developing colon cancer.36,37 An increased tendency to develop colon cancer has been found in individuals up to middle age with an increase in weight. However, a lower tendency of developing colon cancer with an increase in weight in middle- and older-aged individuals was reported in the same study.38,39
Due to the small number of diabetic patients recruited in our study we could not report on the relationship between diabetes and CRC. However, independent of a lack of physical exercise and obesity, diabetes has been found in other studies to be a risk factor for CRC.40,41 Diabetic patients tend to have high levels of insulin and insulin-like growth factors. Insulin-like growth factors inhibit the apoptosis of colonic epithelial cells, while hyperinsulinaemia causes activation of the Ras pathway, which stimulates carcinogenesis.42,43
Studies in diabetic individuals have shown that colonic tumours may develop when insulin activates aberrant foci in the crypts of the colonic epithelium.44–47 Obesity is an independent risk factor for CRC, which has been increasing in the affluent population of Sub-Saharan Africa. Obesity may also be responsible for the steady increase in noncommunicable diseases such as diabetes which in turn may also increase the risk of CRC.
Several studies support the association between alcohol consumption and rectal cancer,48–51 while other studies found no association between rectal cancer and alcohol intake.52–54 Studies have also reported a significant relationship between alcohol consumption and colon cancer.50,51,55–57 From seven studies that confirmed an association between rectal cancer and alcohol, six studies showed that beer intake increased the risk, three studies showed spirits increasing the risk, two studies showed that wine intake increased the risk and one study showed no association between rectal cancer and the intake of wine.48–51,58,59 A meta-analysis has shown a forty percent risk of CRC developing in individuals who drink three alcoholic drinks a day, while there is a twenty percent risk of CRC if they drink two to three alcoholic drinks daily.72
In our study, the type of beverage consumed in the form of beer, spirits or wine and the frequency and quantity of alcohol consumed had no association with the development of CRC. An association with CRC was seen even with a small amount of alcohol intake with past and current alcohol drinkers, although this did not reach statistical significance in the multivariable model, possibly because other confounding variables, such as smoking, BMI and area of residence, were also considered in our study. A study observed that biopsies taken from chronic alcoholics showed rectal mucosal hyperproliferation, which is associated with an increased risk of cancer compared to rectal biopsies from controls.58
There is sparse evidence regarding the type of beverage effects on CRC, with studies generally showing a strong association with the intake of beer;49,58,59 however, there is also an increased risk with wine and spirits.59 Some studies have shown no risk of CRC with wine, which suggests that this beverage has anticarcinogenic effects compared to other beverages.60
Several biological mechanisms have been postulated regarding the role of alcohol in colorectal carcinogenesis. The contamination of beer with nitrosamine carcinogens from breweries may explain the consistent finding of an association between beer and colorectal cancer in several studies.56 Another mechanism is that alcohol consumption damages the liver, resulting in the inhibition of the detoxification of nitrosamines and other carcinogens.61 Low aldehyde dehydrogenase activity in the colonic mucosa results in the accumulation of acetaldehyde in the colon and rectum, which is carcinogenic.60,62 A Japanese study showed an increased risk of colon cancer in individuals who drink alcohol and have a mutant aldehyde dehydrogenase-2-allele.63 The intake of methionine and folate micronutrients is required for the methylation of DNA, which is responsible for gene regulation. A low level of folate and methionine in the diet has been found in men who drink alcohol to increase the risk of colon cancer.64
In our study wine was not significantly associated with an increased risk of CRC. This is in keeping with other studies from Italy that showed no increased risk of wine with CRC.65,66 Other studies have observed an anticarcinogenic effect in wine.60 The cellular events of CRC initiation, promotion and progression are inhibited by phytoalexin called resveratrol found in wine and grapes.67 In rats, resveratrol has been found to suppress the growth of human colon cancer cells by suppressing the growth of aberrant colorectal crypt foci.68 The growth of human cancer cells has also been shown to be suppressed by methanol extracts in white and red wine, which contain flavonoids, particularly anthocyanin.69
We found that current cigarette smokers had a negative correlation with CRC; however, with past smoking had a positive correlation. This is consistent with results from previous studies.70,71 Possible pathophysiological mechanisms behind the decreased risk in current smokers is that peristalsis of the colon may be stimulated by the nicotine in cigarette smoke. Nicotine increases the motor activity and tone of the colon, resulting in a decreased faecal transit time and hence decreasing the tendency to develop colon cancer.72
However, cigarette smoking has also been shown to increase the risk of adenomatous polyps in the colon and rectum, which eventually lead to colorectal cancer. A recent meta-analysis conducted in Europe, the USA and Asia showed that past smokers and ever smokers were strongly associated with CRC; however, for current smokers, the association with CRC was weak.73 Proximal colon cancers were associated with past smokers and ever smokers, while rectal cancers were associated with past, current and ever smokers.73,74 In another meta-analysis, it was found that compared to nonsmokers, the risk of rectal and colon cancer was greater for current and past cigarette smokers. Passive smokers are exposed to higher levels of carcinogenic compounds than active smokers.75 These high levels of carcinogenic compounds in passive smokers include nitrosamines, carbon monoxide and ammonia.76 Carcinogenic compounds generally found in tobacco smoke mainly include arylamines, N-nitosonornicotine, polycyclic and aromatic hydrocarbons.76 Our study did not examine the effect of passive smoking on the risk of CRC.
In rectal and colon cancer patients, epigenetic and mutational changes in the BRAF and KRAS genes have been identified. However, heavier smokers tend to have CRC molecular subtypes that are a combination of MSI high and CIMP positive. Therefore, the serrated pathway is commonly involved in the development of CRC in smokers.77 In rats, heterocyclic amines in cigarette smoke have been found to mutate the APC (adenomatous polyposis coli) gene causing colon cancer. This mutation in the APC gene has also been found in human colon cancer.76–79
Earlier studies in Sub-Saharan Africa have examined the relative frequency of cancers and outlined possible differences in the risk between different tribes.80 In Uganda, the different traditional ethnic groups have been residing in different parts of the country. Although the case participants in our study were recruited from hospitals in central Uganda whose catchment is representative of all of the country, the majority were currently living in different residential areas in Uganda and not in their native home tribal district. Furthermore, there are socioeconomic differences between individuals in the same tribe that were not assessed in this study. This may possibly explain the findings in our study and those of another study in Uganda where the difference in the tribe was not found to be a risk factor for CRC.81
Limitations
Early undiagnosed colorectal cancers possibly could have been left out due to the lack of population screening, resulting in a selection error. Given the low prevalence of CRC at 9.3% from patients reported to our National Referral Hospital in Central Uganda,81 the general population at risk of CRC is low; therefore, the effect of this selection error is likely to be small. The relation between age and sex on CRC could not be determined in our case-control study, as they were matched variables.
Recall bias was another limitation in our study as the CRC disease history was self-reported however reliable histories were obtained for smoking and alcohol consumption. The lack of data on socioeconomic factors, such as the individuals’ level of education, and neighbourhood residential factors, which have been found to be risk factors for CRC in other studies82 is a limitation. Data were also lacking on the duration, quantity of alcohol intake and physical activity, which is a potential limitation of our study. However, further follow-up studies will address these risk factors in our East African environment.
While inflammatory bowel disease is a risk factor for CRC, none of our histologically proven adenocarcinomas from our patient cohort in Uganda had features of ulcerative colitis or Crohn’s disease on histological examination. This is in keeping with the generally very low incidence of ulcerative colitis in Africa which is currently 5.12/per 100,000 population.83–88
Hospital-based studies may result in selection bias, as they may not be representative of the entire population. The patients who tend to come to these centres are the ones who can afford to come very long distances, so generalization needs to be done with caution. However, our patients were recruited from four major specialized hospitals in central Uganda that receive patients from all four major regions of the country, giving a high level of confidence about the generalizability of the study findings.
Conclusions
Our study determined the risk factors associated with CRC in an indigenous population in East Africa. A positive family history of gastrointestinal cancer is a risk factor; therefore, it is imperative that molecular genetic studies be carried out to determine the role of genetic susceptibility in our population. Although in low-income developing countries it may not be feasible to carry out population-based CRC screening, our findings show that the feasibility of targeted CRC screening, particularly for first-degree family members, should be considered in our East African population. Lifestyle factors, particularly smoking, were associated with an increased risk of CRC. Urbanization in East Africa has resulted in this urban population changing to a sedentary lifestyle, which leads to obesity, adoption of health-risk behaviours and a westernized type of diet that tends to be associated with CRC. Hence, these findings highlight the importance of adopting prevention strategies to help the population avoid these health-risk behaviours.
Data Sharing Statement
The dataset generated and/or analyzed during this PhD study is available as an Excel supplementary file titled: “Risk factors for CRC in an indigenous East African population”.
Ethical Considerations
This work was part of the PhD study, which was approved by the Higher Degrees Research and Ethics Committee, School of Biomedical Sciences, College of Health Sciences, Makerere University (reference number: SBS-HDREC-630) and Uganda National Council for Science and Technology (reference number: HS-2574). Written informed consent was obtained from all participants included in the study before completing the questionnaire form. Written informed consent was obtained before obtaining a biopsy confirming colorectal adenocarcinoma on the case participants and before obtaining a faecal occult blood sample in control participants. Those control participants who tested positive for faecal occult blood were referred for screening investigations, particularly a colonoscopy, to rule out or confirm colorectal malignancy. All data pertaining to the research were kept as confidential as possible and did not identify any particular individual. The conduct of this study was in accordance with the principles outlined in the Declaration of Helsinki.
Consent for Publication
Written informed consent was obtained from all participants included in the study before completing the questionnaire form. Written informed consent was obtained before obtaining a biopsy confirming colorectal adenocarcinoma in the case participants. For control participants, written informed consent was obtained before obtaining a faecal occult blood sample.
Acknowledgments
This study was part of the PhD work, which was approved by the Doctoral Committee and Higher Degrees Research and Ethics Committee of the School of Biomedical Sciences, College of Health Sciences, Makerere University for the corresponding author. Final approval of this research study was obtained from the Uganda National Council for Science and Technology. The authors wish to thank the clinical staff and research assistants, particularly Dr. Sulaiman Ishaq Mahmud and Dr. Justus Atuhaire who recruited the participants from the Department of Surgery of Masaka Regional Referral Hospital, Mulago National Referral Hospital, Uganda Martyrs’ Hospital Lubaga and Mengo Hospital for their support in this research project.
Funding
The authors declare that they received no specific funding for this work. However, the corresponding author personally funded this part of his PhD research study. No payment was received by the authors to write and publish this part of the study.
Disclosure
The authors declare that they have no competing interests.
References
1. Chalya P, Mchembe M, Mabula J, et al. Clinicopathological patterns and challenges of management of colorectal cancer in a resource-limited setting: a Tanzanian experience. World J Surg Oncol. 2013;11:88. doi:10.1186/1477-7819-11-88
2. Katsidzira L, Gangaidzo I, Thomson S, Rusakaniko S, Matenga J, Ramesar R. The shifting epidemiology of colorectal cancer in sub-Saharan Africa. Lancet Gastroenterol Hepatol. 2017;2:377–383. doi:10.1016/S2468-1253(16)30183-2
3. Parkin DM, Bray F, Ferlay J, Jemal A. Cancer in Africa 2012. Cancer Epidemiol Biomarkers Prev. 2014;23:953–966. doi:10.1158/1055-9965.EPI-14-0281
4. Wabinga H, Nambooze S, Phoebe MA, Okello C, Mbus L, Parkin DM. Trends in the incidence of cancer in Kampala, Uganda 1991–2010. Int J Cancer. 2014;135(2):432–439. doi:10.1002/ijc.28661
5. Bukirwa P, Wabinga H, Nambooze S, et al. Trends in the incidence of cancer in Kampala, Uganda, 1999 to 2015. Int J Cancer. 2021;148(9):2129–3138. doi:10.1002/ijc.33373
6. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. GLOBOCAN 2008, cancer incidence and mortality Wordwide: IARC CancerBase No. 10; 2010.
7. Lichtenstein P, Holm N, Verkasalo P, et al. Enviromental and heritable factors in the causation of cancer. Analyses of cohorts from Sweden, Denmark and Finland. N Engl J Med. 2000;343:78–85. doi:10.1056/NEJM200007133430201
8. Wismayer R, Kiwanuka J, Wabinga H, Odida M. Clincopathological features and sujrvival outcomes of histopathological subtypes of colorectal adenocarcinoma in Ugandan patients. IJSCP. 2022;4(1):1–13.
9. Connell LC, Mota JM, Braghiroli MI, et al. The rising incidence of younger patients with colorectal cancer: questions about screening, biology and treatment. Curr Treat Options Oncol. 2017;18(4). doi:10.1007/s11864-017-0463-3
10. Lewandowska A, Rudzki G, Lewandowski T, Stryjkowska-Gora A, Rudzki S. Risk factors for the diagnosis of Colorectal cancer. Cancer Control. 2021;29:1–15.
11. Walker ARP, Segal I. Colorectal cancer in an African city population in transition. Eur J Cancer Prev. 2002;11(2):187–191. doi:10.1097/00008469-200204000-00012
12. Vorster H, Kruger A, Margetts B. The nutrition transition in Africa: can it be steered into a more positive direction. Nutrients. 2011;3:429–441. doi:10.3390/nu3040429
13. Bouvard V, Loomis D, Guyton KZ, et al. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015;16(16):1599–1600. doi:10.1016/S1470-2045(15)00444-1
14. Coughlin SS, Richards TB, Thompson T, et al. Rural/nonrural differences in colorectal cancer incidence in the United States, 1998–2001. Cancer. 2006;107:1181–1188. doi:10.1002/cncr.22015
15. Enayatrad M, Yavari P, Vahedi H, Mahdaui S, Etemad K, Khodakarim S. Urbanization levels and its association with the prevalence of risk factors and colorectal cancer incidence. Iran J Public Health. 2021;50(11):2317–2325. doi:10.18502/ijph.v50i11.7588
16. Pacquette I, Finlayson SR. Rural versus urban colorectal and lung cancer patients: differences in stage at presentation. J Am Coll Surg. 2007;205:636–641. doi:10.1016/j.jamcollsurg.2007.04.043
17. Katsidzira L, Gangaidzo IT, Makunike-Mutasa R, et al. A case-control study of risk factors for colorectal cancer in an African population. Eur J Cancer Prev. 2019;28(3):145–150. doi:10.1097/CEJ.0000000000000439
18. Singh GK, Miller BA, Hankey BR, et al. Area socioeconomic variations in USA cancer incidence, mortality, stage, treatment and survival, 1975–1999. NCI Cancer Surveill Monogr Series. 2003;4(3):5417.
19. Pourfarzi F, Yazdanbod A, Daneshvar R, Saberi SH. Evaluation of effective factors in incidence of colorectal cancer. J Ardabil Univ Med Sci. 2012;12:56–64.
20. Mohan V, Mathur P, Deepa R, et al. Urban rural differences in prevalence of self-reported diabetes in India – the WHO-ICMR Indian NCD risk factor surveillance. Diabetes Res Clin Pract. 2008;80:159–168. doi:10.1016/j.diabres.2007.11.018
21. Ramachandran A, Mary S, Yamuna A, Murugeson N, Snehalatha C. High prevalence of diabetes and cardiovascular risk factors associated with urbanization in India. Diabetes Conc. 2008;31:893–898.
22. Liu S, Wang W, Yang X, et al. Prevalence of diabetes and impaired fasting glucose in Chinese adults, China National Nutrition and Health Survey. Prev Chronic Dis. 2002;8(1):A13.
23. Dijxhoorn DN, Boutall A, Mulder CJ, et al. Colorectal cancer in patients from Uganda: a histopathological study. East Cent Afr J Surg. 2014;19(1):112–119.
24. Altekruse SF, Kosary CL, Krapcho M, et al. SEER cancer statistics review, 1975–2007. Bethesda, MD: National Cancer Institute; 2010. Available from: http://seer.cancer.gov/csr/1975_2007/.
25. Barrett J, Jiwa M, Rose P, Hamilton W. Pathways to the diagnosis of colorectal cancer: an observational study in three UK cities. Fam Pract. 2006;23(1):15–19. doi:10.1093/fampra/cmi093
26. Daly M, Paquette I, Daly MC, Paquette IM. Surveillance, Epidemiology and End Results (SEER) and SEER-medicine databases: use in clinical research for improving colorectal cancer outcomes. Clin Colon Rectal Surg. 2019;32(1):61–68. doi:10.1055/s-0038-1673355
27. Fairley TL, Cardinez CJ, Martin J, et al. Colorectal cancer in US adults younger than 50 years of age, 1998–2001. Cancer. 2006;107(5):1153–1161. doi:10.1002/cncr.22012
28. O’Connell JB, Maggard MA, Liu JH, Etzioni DA, Livingston EH, Ko CY. Rates of colon and rectal cancers are increasing in young adults. Am Surg. 2003;69(10):866–872.
29. Cronje L, Paterson A, Becker P. Colorectal cancer in South Africa: a heritable cause suspected in many young black patients. S Afr Med J. 2009;99(2):103–106.
30. Vergouwe F, Boutall A, Stupart D, et al. Mismatch repair deficiency in colorectal cancer patients in a low-incidence area. SAJS. 2013;51(1):16–21.
31. Wark PA, Wu K, Van’t Veer P, Fuchs CF, Giovanucci EL. Family history of colorectal cancer: a determinant of advanced adenoma stage or adenoma multiplicity?. Int J Cancer. 2009;125:413–420.
32. Lynch KL, Ahnen DJ, Byers T, Weiss DG, Liebeman DA. First-degree relatives of patients with advanced colorectal adenomas have an increased prevalence of colorectal cancer. Clin Gastroenterol Hepatol. 2003;1:96–102. doi:10.1053/cgh.2003.50018
33. Bass AJ, Meyerhardt JA, Chan JA, Giovanucci EL, Fuchs CS. Family history and survival after colorectal cancer diagnosis. Cancer. 2008;112:1222–1229. doi:10.1002/cncr.23294
34. Kao PS, Lin JK, Wang HS, et al. The impact of family history on the outcome of patients with colorectal cancer in a veterans’ hospital. Int J Colorectal Dis. 2009;24:1249–1254. doi:10.1007/s00384-009-0774-3
35. Henrikson NB, Webber EM, Goddard KA, et al. Family history and natural history of colorectal cancer: systematic review. Genet Med. 2015;17(9):702–712. doi:10.1038/gim.2014.188
36. Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet. 2008;371(9612):569–578. doi:10.1016/S0140-6736(08)60269-X
37. Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: incidence, mortality, survival and risk factors. Gastroenterol Rev. 2019;14(2):89–103. doi:10.5114/pg.2018.81072
38. Karahalios A, Simpson JA, Baglietto L, et al. Change in weight and waist circumference and risk of colorectal cancer: results from the Melbourne collaborative cohort study. BMC Cancer. 2016;16:157. doi:10.1186/s12885-016-2144-1
39. Ma Y, Yang Y, Wang F, et al. Obesity and risk of colorectal cancer: a systematic review of prospective studies. PLoS One. 2013;8(1):e53916. doi:10.1371/journal.ponc.0053916
40. Lauby-Secretan B, Scoccianti C, Loomis D, Grosse Y, Bianchini F, Straif K. Body fatness and cancer-viewpoint of the IARC working group. N Engl J Med. 2016;375(8):794–798. doi:10.1056/NEJMsr1606602
41. Nunez C, Nair-Shalliker V, Egger S, Sitas F, Bauman A. Physical activity, obesity and sedentary behaviour and the risks of colon and rectal cancers in the 45 and up study. BMC Public Health. 2018;18:325. doi:10.1186/s12889-018-5225-z
42. Karahalios A, English DR, Simpson JA. Weight change and risk of colorectal cancer: a systematic review and meta-analysis. Am J Epidemiol. 2015;181(11):832–845. doi:10.1093/aje/kwu357
43. Jarvandi S, Davidson NO, Schootman M, Bermano G. Increased risk of colorectal cancer in type 2 diabetes is independent of diet quality. PLoS One. 2013;8(9):e74616. doi:10.1371/journal.pone.0074616
44. Yuhara H, Steinmans C, Cohen SE, Corley DA, Teiy Buffer PA. Is diabetes mellitus an independent risk factor for colon cancer and rectal cancer?. Am J Gastroenterol. 2011;106:1911–1921.
45. Leitner JW, Kine T, Carel K, Goalstone M, Draznin B. Hyperinsulinaemia potentiates activation of p21RAS by growth factors. Endocrinology. 1997;138:2211–2214. doi:10.1210/endo.138.5.5240
46. Guo YS, Narayan S, Yallampalli C, Singh P. Characterisation of insulin like growth factor 1 receptors in human colon cancer. Gastroenterology. 1992;102:1101–1108. doi:10.1016/0016-5085(92)90744-J
47. Corpet DE, Jacquinet C, Peiffer G, Tache S. Insulin injections promote the growth of aberrant crypt foci in the colon of rats. Nutr Cancer. 1997;27:316–320. doi:10.1080/01635589709514543
48. Stemmermann G, Nomura A, Chyou P, et al. Prospective study of alcohol intake and large bowel cancer. Dig Dis Sci. 1990;11:1414–1420. doi:10.1007/BF01536750
49. Freudenheim JL, Graham S, Marshall JR, et al. Lifetime alcohol intake and risk of rectal cancer in western New York. Nutr Cancer. 1990;13:101–109. doi:10.1080/01635589009514050
50. Hirayama T. Association between alcohol and cancer of the sigmoid colon: observations from a Japanese cohort study. Lancet. 1989;23:725–727. doi:10.1016/S0140-6736(89)90782-4
51. Longnecker M, Orza M, Adams M, et al. A metaanalysis of alcoholic beverages in relation to risk of colorectal cancer. Cancer Causes Control. 1990;1:59–68. doi:10.1007/BF00053184
52. Adami HO, McLaughlin JK, Hsing AW, et al. Alcoholism and cancer risk: a population-based cohort study. Cancer Causes Control. 1992;3:419–425. doi:10.1007/BF00051354
53. Gapstur S, Potter J, Folsom A. Alcohol consumption and colon and rectal cancer in postmenopausal women. Int J Epidemiol. 1994;23:50–57. doi:10.1093/ije/23.1.50
54. Riboli E, Cornee J, Macquart-Moulin G, et al. Cancer and polyps of the colorectum and lifetime consumption of beer and other alcoholic beverages. Am J Epidemiol. 1991;134:157–166. doi:10.1093/oxfordjournals.aje.a116068
55. Giovanucci E, Rimm EB, Acherio A, et al. Alcohol, low-methionine-low-folate diets, and risk of colon cancer in men. J Natl Cancer Inst. 1995;87:265–273. doi:10.1093/jnci/87.4.265
56. Glynn S, Albanes D, Pietinen P, et al. Alcohol consumption and risk of colorectal cancer in a cohort of Finnish men. Cancer Causes Control. 1996;7:214–223. doi:10.1007/BF00051297
57. Meyer F, White E. Alcohol and nutients in relation to colon cancer in middle-aged adults. Am J Epidemiol. 1993;138:225–236. doi:10.1093/oxfordjournals.aje.a116851
58. Newcomb P, Storer B, Marcus P. Cancer of the large bowel in relation to alcohol consumption: a case-control study in Wisconsin (United States). Cancer Causes Control. 1993;4:405–411. doi:10.1007/BF00050858
59. Goldbohm R, Van den Brandt P, Veer P, et al. Prospective study on alcohol consumption and the risk of the colon and rectum in the Netherlands. Cancer Causes Control. 1994;5:95–104. doi:10.1007/BF01830255
60. Penderson A, Johansen C, Gronback M. Relations between amount and type of alcohol and colon and rectal cancer in a Danish population based cohort study. Gut. 2003;52(6):861–867. doi:10.1136/gut.52.6.861
61. Hakkak R, Korourian S, Ronis M, et al. Effects of diet and ethanol on the expression and localization of cytochromes P450 2E1 and P450 2C7 in the colon of male rats. Biochem Pharm. 1996;51:61–69. doi:10.1016/0006-2952(95)02154-X
62. Salaspuro M. Bacterocolonic pathway for ethanol oxidation: characteristic and implications. Ann Med. 1996;28:195–200. doi:10.3109/07853899609033120
63. Yokoyama A, Marumatsu T, Ohmori T, et al. Alcohol-related cancers and aldehyde dehydrogenase-2 in Japanese alcoholics. Carcinogenesis. 1998;8:1383–1387. doi:10.1093/carcin/19.8.1383
64. Kono S, Ikeda N, Yani F, et al. Alcoholic beverages and adenomatous polyps of the sigmoid colon: a study of male self-defence officials in Japan. Int J Epidemiol. 1990;19:848–852. doi:10.1093/ije/19.4.848
65. Barra S, Negri E, Franceschi S, et al. Alcohol and colorectal cancer: a case-control study from Northern Italy. Cancer Causes Control. 1992;3(2):153–159. doi:10.1007/BF00051655
66. Tavani A, Ferraroni M, Mezzetti M, et al. Alcohol intake and risks of cancers of the colon and rectum. Nutr Cancer. 1998;30:213–219. doi:10.1080/01635589809514666
67. Jang M, Cai L, Udeani GO, et al. Cancer chemopreventitive activity of resveratrol, a natural product derived from grapes. Science. 1997;275:218–220. doi:10.1126/science.275.5297.218
68. Tessitore L, Davit A, Sarotto I, et al. Resveratrol depress the growth of colorectal aberrant crypt foci by affecting bax and p21 (CIP) expression. Carcinognesis. 2000;21:1619–1622. doi:10.1093/carcin/21.5.619
69. Kamei H, Hashimoto Y, Tatsurou K, et al. Anti-tumor effect of methanol extracts from red and white wines. Cancer Biother Radiopharm. 1998;6:447–452. doi:10.1089/cbr.1998.13.447
70. Train TT, Medine A, Bruce WR. Insulin promotion of colon tumours in rats. Cancer Epidemiol Biomarkers. 1996;5:1013–1015.
71. Cho E, Stephanie A, Spiegelman D, et al. Dairy foods, calcium, and colorectal cancer: a pooled analysis of 10 Cohort studies, JCSI. J Natl Cancer Inst. 2004;96(13):1015–1022. doi:10.1093/jnci/djh185
72. Fedirko V, Tramacere I, Bagnardi V, et al. Alcohol drinking and colorectal cancer risk: an overall and dose-response meta-analysis of published studies. Ann Oncol. 2011;22(9):1958–1972. doi:10.1093/annonc/mdq653
73. Lutgens MW, Van Oijen MG, Van der Heijden GJ, Vlaggaar FP, Siersema PD, Oldenburg B. Declining risk of colorectal cancer in inflammatory bowel disease: an updated meta-analysis of population-based cohort studies. Inflamm Bowel Dis. 2013;19(4):789–799. doi:10.1097/MIB.0b013e31828029c0
74. Higginson J. Etiological factors in gastrointestinal cancer in man. J Natl Cancer Inst. 1966;37:527–545.
75. Hoshiyama Y, Sekine T, Sasaba T. A case-control study of colorectal cancer and its relation to diet, cigarettes and alcohol consumption in Saitama Prefecture, Japan. Tohoku J Exp Med. 1993;171:153–165. doi:10.1620/tjem.171.153
76. Taylor P. Ganglionic stimulating and blocking agents. In: Gilman AG, Goldman LS, Rall TW, Murad F, edited by. The Pharmacological Basis of Therapeutics.
77. Botteri E, Iodice S, Bagnardi V, Raimondi S, Lowengels AB, Maisonneuve P. Smoking and colorectal cancer. J Am Med Assoc. 2008;300(23):2765–2778. doi:10.1001/jama.2008.839
78. Botteri E, Iodice S, Raimondi S, Maisonneuve P, Lowenfels AB. Cigarette smoking and adenomatous polyps: a meta-analysis. Gastroenterology. 2008;134(2):388–395. doi:10.1053/j.gastro.2007.11.007
79. Ordonez-Mena JM, Walter V, Schottker B, et al. Impact of prediagnostic smoking and smoking cessation on colorectal cancer prognosis: a meta-analysis of individual patient data from cohorts within the CHANCES CONSORTIUM. Ann Oncol. 2018;29(2):472–483. doi:10.1093/annonc/mdx761
80. Hoffmann D, Djordjevic MV, Hoffmann I. The changing cigarette. Prev Med. 1997;26(4):427–434. doi:10.1006/pmed.1997.0183
81. Giovanucci E, Colditz GA, Stampfer MJ, Willett WC. Physical activity, obesity and risk of colorectal adenoma in women (United States). Cancer Causes Control. 1996;7(2):253–263. doi:10.1007/BF00051301
82. Wang X, Efrat A, Tabitha AH, et al. Association between smoking and molecular subtypes of colorectal cancer. JNCI Cancer Spectrum. 2021;5(4). doi:10.1093/jncics/pkab056
83. Huang K, Sandler SRS, Millikan RC, Shroader JC, North KE, Hu J. GSTM1 and GSTT1 polymorphisms, cigarette smoking and risk of colon cancer: a population-based case-control study in North Carolina (United States). Cancer Causes Control. 2006;17(4):385–394. doi:10.1007/s10552-005-0424-1
84. Clifford P, Linsell CA, Timms GL. Cancer in Africa. Nairobi: East African Publishing House; 1968.
85. Wekha G, Ssewante N, Iradukunda A, et al. Bongomin. Colorectal Cancer in Uganda: a 10-year, facility-based, retrospective study. Cancer Manag Res. 2021;13:7697–7707. doi:10.2147/CMAR.S334226
86. Doubeni CA, Major JM, Laiyemo AO, et al. Contribution of behavioural risk factors and obesity to socioeconomic differences in colorectal cancer incidence. J Natl Cancer Inst. 2012;104(18):1353–1362. doi:10.1093/inci/dis346
87. Hammada T, Lemdaoui M-C, Boutra F, Zoughailech D, Asselah H. Aspects epidemiologiques des maladies inflammatoires chronique de l’intestin dans une population algerienne. J Afr Hepato Gastroenterol. 2011;5:293–302. doi:10.1007/s12157-011-0327-6
88. Uganda Bureau of Statistics. The national population and housing census 2014- main report. Kampala, Uganda; 2016.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Uneven Between-Hospital Distribution of Patient-Related Risk Factors for Adverse Outcomes of Colorectal Cancer Treatment: A Population-Based Register Study
Rattenborg S, Möller S, Frostberg E, Rahr HB
Clinical Epidemiology 2023, 15:867-880
Published Date: 22 July 2023
A Prospective Nested Case-Control Study of Risk Factors for Postoperative Delirium in Elderly Patients with Colorectal Cancer

Cui X, Cao N, Tian S, Liu Y, Xiang J
Clinical Interventions in Aging 2025, 20:639-648
Published Date: 21 May 2025
Metabolic-Behavioral Risk Factors for Colorectal Adenomatous Polyps in Young Adults
Zheng Q, Li Z, Hu J, Chu Y, Shi X
Clinical and Experimental Gastroenterology 2025, 18:251-257
Published Date: 27 October 2025
Risk Factors for Severe Postoperative Complications After Laparoscopic Colorectal Cancer Surgery in Octogenarians: A Retrospective Cohort Study
Li Y, Du J, Qiu W, Tang J
Clinical Interventions in Aging 2026, 21:590287
Published Date: 27 April 2026