Back to Journals » Clinical and Experimental Gastroenterology » Volume 18
Metabolic-Behavioral Risk Factors for Colorectal Adenomatous Polyps in Young Adults
Authors Zheng Q, Li Z ![]() , Hu J, Chu Y, Shi X
, Hu J, Chu Y, Shi X
Received 1 August 2025
Accepted for publication 10 October 2025
Published 27 October 2025 Volume 2025:18 Pages 251—257
DOI https://doi.org/10.2147/CEG.S553734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Vipul Yagnik
Quan Zheng, Zaizai Li, Jiangtian Hu, Yukun Chu, Xiaolong Shi
Department of Gastroenterology, the Fifth Affiliated Hospital of Zhengzhou University, Zhengzhou City, Henan, People’s Republic of China
Correspondence: Zaizai Li, Department of Gastroenterology, the Fifth Affiliated Hospital of Zhengzhou University, Zhengzhou City, Henan, People’s Republic of China, Email [email protected]
Objective: This study aimed to identify risk factors associated with colorectal adenomatous polyps in young adults (≤ 40 years) to support early prevention and screening strategies for colorectal cancer.
Methods: We conducted a study involving 805 young patients who underwent colonoscopy at the Endoscopy Center of The Fifth Affiliated Hospital of Zhengzhou University, China, from September 2023 to January 2025. Among them, 288 patients had at least one pathologically confirmed adenomatous polyp (cases), and 517 patients with no detected polyps served as controls. Data on demographics, lifestyle habits (smoking, alcohol use), metabolic parameters, and hematological indices were collected and analyzed.
Results: Several factors were significantly associated with an increased risk of adenomatous polyps, including male sex, hypertension, diabetes, smoking, alcohol consumption, elevated body mass index, and reduced high-density lipoprotein cholesterol (HDL-C). Multivariate analysis further identified hypertension, alcohol use, and higher red blood cell count as independent risk factors. Conversely, female sex and higher HDL-C levels were found to be protective.
Conclusion: The development of colorectal adenomatous polyps in young adults is strongly linked to modifiable risk factors such as hypertension and alcohol consumption, as well as elevated red blood cell counts. These findings highlight the importance of addressing cardiovascular and metabolic health, along with lifestyle modifications, in early screening and prevention programs for high-risk young individuals.
Keywords: adenomatous, colorectal polyps, young adults, risk factors, colorectal cancer
Introduction
Colorectal cancer (CRC) remains the third most prevalent malignancy globally, presenting a significant public health burden characterized by distinct age-stratified patterns in both incidence and mortality.1 Historically associated with advanced age, there is now an alarming epidemiological shift towards earlier disease onset that fundamentally challenges established paradigms. Recent data highlight this concerning trend: the American Cancer Society’s 2023 report indicates a sustained annual increase of approximately 2% in CRC incidence among individuals under 50 years old over recent decades.2 Consequently, the proportion of new diagnoses within the 20–49 age group has surged dramatically, rising from 6% in 1995 to 12% in 2020. This phenomenon is not confined to North America; corroborating evidence from the National Cancer Center of China3 reveals an even more pronounced escalation 48% in CRC incidence among young adults aged 18–45 years over the past decade.4 Importantly, this rate of increase significantly outpaces that observed in older populations within these regions, signaling a unique and growing public health challenge specific to younger demographics.
This increasing incidence among younger individuals directly challenges the traditional screening initiation age of 45–50 years established in longstanding clinical guidelines.5 Acknowledging this urgency, the American College of Gastroenterology revised its recommendations in 2021, lowering the suggested screening age for average-risk individuals to 45 years. However, while this broad adjustment is necessary, it remains inadequate. A significant gap persists in developing and validating evidence-based strategies for effective risk stratification and targeted early intervention specifically designed for high-risk young adults. Identifying which younger individuals require intensified surveillance prior to symptomatic presentation is crucial for efficient resource allocation and impactful prevention efforts.
Adenomatous polyps are recognized as the primary precursor lesions for the majority of sporadic colorectal cancers (CRCs). The timely detection and endoscopic removal of these neoplastic growths through screening colonoscopy represent a highly effective strategy for significantly reducing future CRC incidence and mortality. However, existing research on adenomatous polyps predominantly focuses on populations aged 50 and older,6 reflecting traditional screening cohorts. As a result, there exists a substantial knowledge gap regarding the prevalence, characteristics, and underlying risk factors specifically associated with adenoma development in adults under 45 to 50 years of age. Compounding this issue is the persistently low awareness of CRC risks and symptoms among young adults themselves, which often leads to delayed presentation and diagnosis at more advanced stages that are less amenable to treatment. Furthermore, the array of risk factors predisposing young adults to adenomatous polyp formation—potentially differing in nature, magnitude, or interaction from those affecting older adults—remains poorly defined and inadequately studied.While recognized hereditary conditions—such as Lynch syndrome and familial adenomatous polyposis—confer significant risk, they explain only a fraction of cases. Broader genetic susceptibilities, including common risk alleles and family aggregation, may interact with modifiable factors to shape individual risk. In addition to alcohol and tobacco use, which are well-documented, other lifestyle elements are likely contributory. These include dietary habits rich in processed meats and low in fiber, physical inactivity, obesity, and metabolic disorders such as diabetes and dyslipidemia. Furthermore, early-life environmental exposures and shifts in gut microbiota composition are emerging as potential mediators of risk. A comprehensive approach that incorporates genetic predisposition, multifaceted lifestyle factors, and metabolic health is crucial to elucidating the etiology of adenomatous polyps in young adults and informing targeted prevention and early screening strategies.
Methods
All participants underwent complete colonoscopic examination reaching the cecum using an Olympus CF-H290Z video colonoscope (Olympus Corporation, Tokyo, Japan). Tissue specimens analyzed consisted of complete pathological biopsy samples or polyps excised during surgical procedures. Relevant clinical and laboratory data were collected for each participant, encompassing demographics (sex), anthropometrics (body mass index, BMI), lifestyle factors (smoking status, alcohol consumption), comorbidities (hypertension, diabetes mellitus), serum lipid profile [triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), liver function tests [total bilirubin, direct bilirubin, indirect bilirubin, albumin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), coagulation/hematology markers (D-dimer, platelet count), erythrocyte count, and fasting blood glucose (FBG). Cases comprised patients with ≥1 colorectal adenomatous polyp confirmed by both colonoscopy and histopathology. Controls were defined as individuals who underwent complete colonoscopy (cecal intubation confirmed) with no polyps of any histologic type identified.
Participants were classified as “smokers” if they reported current regular tobacco use (≥1 cigarette per day) for over 6 months, and “non-smokers” otherwise. “Drinkers” were defined as individuals consuming ≥30 g of ethanol per week for males or ≥20 g per week for females for at least one year.
Hypertension:7 Defined as either:
(i) Self-reported physician diagnosis with ongoing antihypertensive medication use, OR.
(ii) Systolic blood pressure ≥140 mmHg and/or diastolic ≥90 mmHg on two consecutive measurements during enrollment (using Omron HEM-7124 sphygmomanometer).
Diabetes mellitus: Defined as either:
(i) Self-reported physician diagnosis with hypoglycemic treatment, OR
(ii) Fasting plasma glucose ≥7.0 mmol/L or HbA1c ≥6.5% at enrollment.
Statistical analyses were conducted using SPSS software (version 27.0; IBM Corp., Armonk, NY, USA). Categorical variables are presented as frequencies and percentages and were compared using the Chi-square (χ²) test. Normality of continuous variables was assessed using the Shapiro–Wilk test. Variables exhibiting non-normal distribution (eg, BMI, TG, ALT, AST, FBG; all P < 0.05 on Shapiro–Wilk testing) were expressed as median (interquartile range) [M (Q1, Q3)] and compared using the Mann–Whitney U-test. Normally distributed variables (eg, RBC, HDL-C; P > 0.05) were expressed as mean ± SD and compared using the independent samples t-test. Variables demonstrating statistically significant differences (P < 0.05) in these univariate analyses were subsequently included in a binary logistic regression model to identify independent risk factors associated with colorectal adenomatous polyps. Statistical significance was defined as a two-tailed P-value < 0.05 for all analyses. Variables demonstrating statistically significant differences (P* < 0.05) in univariate analyses were included in the subsequent binary logistic regression model to identify independent risk factors. This study was conducted in accordance with the Declaration of Helsinki. The research protocol was reviewed and approved by the Institutional Review Board of the Fifth Affiliated Hospital of Zhengzhou University (Approval Number: 20230812). Written informed consent was obtained from each study participant.
Although a formal priori sample size calculation was not performed, this exploratory study aimed to enroll as many eligible consecutive patients as possible during the study period to ensure robust model fitting. With a total of 805 participants (288 cases and 517 controls), a post-hoc power analysis revealed that the achieved statistical power exceeded 99% (α=0.05, two-sided) to detect the observed effect sizes of our primary risk factors (eg, an odds ratio of 1.69 for alcohol use), indicating that the sample size was more than adequate.
Results
Univariate analysis identified significant differences between the adenomatous polyp and control groups for multiple variables (Table 1). Sex, hypertension, diabetes, smoking, alcohol consumption, BMI, TC, TG, HDL-C, LDL-C, ALT, AST, RBC, and FBG demonstrated statistically significant associations with adenomatous polyps (P < 0.05). Conversely, no significant differences (P > 0.05) were observed for age, TB, DT, ALB, ALP, IB, D-dimer, PLT, or WBC.
Significant variables from the univariate analysis were included in a multivariate binary logistic regression model (Table 2). This identified sex, hypertension, alcohol consumption, HDL-C, and RBC as independent predictors of colorectal adenomatous polyps (all P < 0.05):
 |
Table 1 Comparison of Baseline Characteristics Between Non-Adenomatous and Adenomatous Polyp Groups in Young Adults |
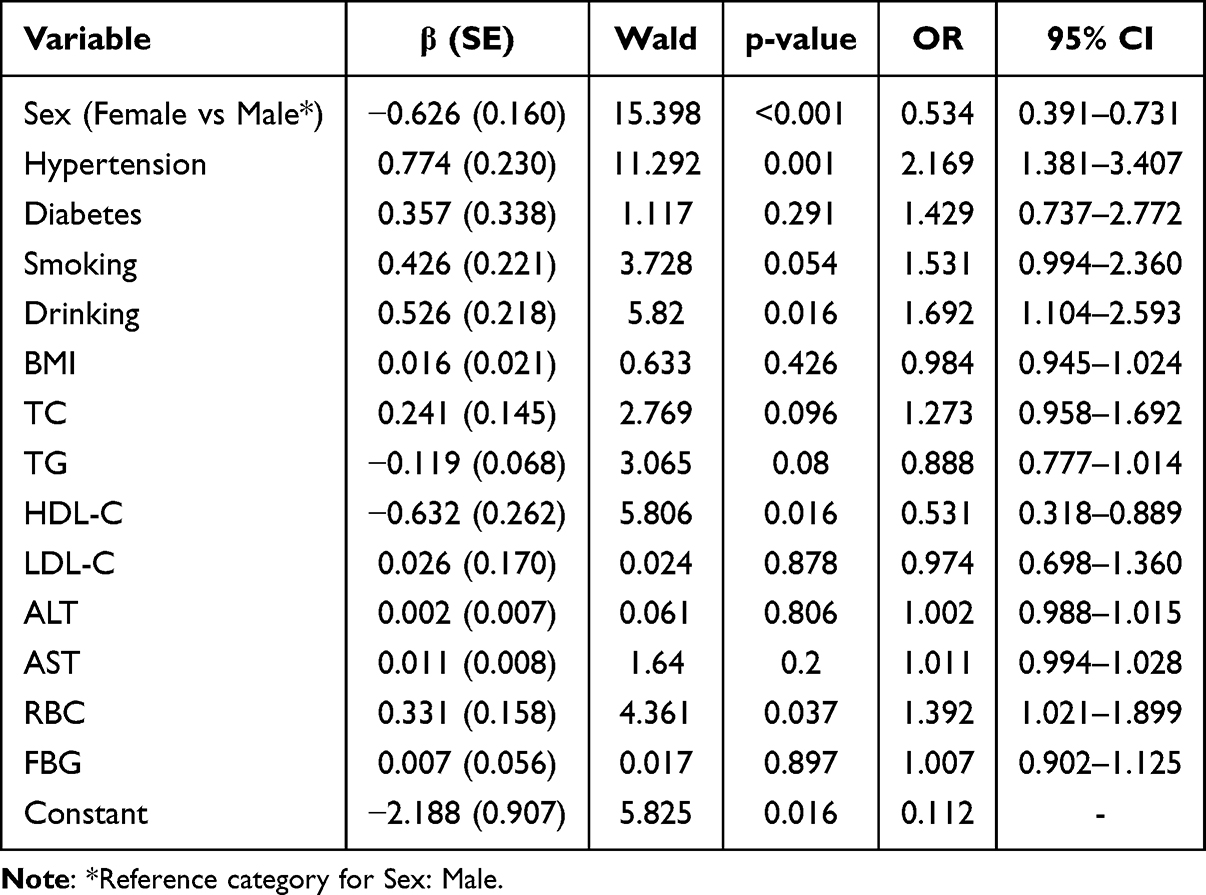 |
Table 2 Results of Binary Logistic Regression Analysis for Factors Associated with Colorectal Adenomatous Polyps in Young Adults |
- Female sex: Significantly lower risk vs males (OR = 0.534; 95% CI: 0.391–0.731; P < 0.001).
- Hypertension: 2.17-fold increased risk (OR = 2.169; 95% CI: 1.381–3.407; P = 0.001).
- Alcohol consumption: 69.2% increased risk vs non-consumers (OR = 1.692; 95% CI: 1.104–2.593; P = 0.016).
- HDL-C: Each 1 mmol/L increase associated with 46.9% risk reduction (OR = 0.531; 95% CI: 0.318–0.889; P = 0.016).
- RBC: Each 1 × 10¹²/L increase associated with 39.2% increased risk (OR = 1.392; 95% CI: 1.021–1.899; P = 0.037).
Variables including BMI, TC, smoking, and diabetes did not show independent significance (P > 0.05).
Discussion
This study identifies hypertension, alcohol consumption, and elevated red blood cell (RBC) count as independent risk factors for colorectal adenomatous polyps in young adults (≤40 years). In contrast, female sex and higher levels of HDL-C provide significant protective effects. These findings address a critical knowledge gap concerning early-onset colorectal carcinogenesis, emphasizing the synergistic roles of metabolic dysregulation and behavioral exposures within young populations. The association between hypertension and adenomatous polyps (OR=2.169) may be attributed to angiotensin II–induced oxidative stress and chronic inflammation, which contribute to endothelial dysfunction and abnormal angiogenesis in the colonic mucosa. This observation is consistent with mechanistic studies that link hypertension to advanced adenomas through mechanisms involving VEGF overexpression and impaired DNA repair pathways.8
Alcohol consumption (OR=1.692) is likely to contribute to carcinogenesis through multiple mechanisms: the metabolism of ethanol produces acetaldehyde, a direct DNA mutagen, while simultaneously depleting folate reserves that are crucial for methyl-group donation and maintaining DNA stability.9,10 Notably, the increased risk observed among young alcohol consumers may be indicative of higher rates of binge drinking within this demographic, which exacerbates mucosal injury and accelerates adenoma formation.11 This observation aligns with cohort studies indicating a 40% increase in colorectal cancer incidence among heavy drinkers under the age of 45 years.12,13
The novel association with elevated red blood cell (RBC) count (OR=1.392 per 1×10¹²/L) necessitates further mechanistic investigation. We hypothesize that erythrocytosis may indicate subclinical chronic hypoxia or undiagnosed myeloproliferative disorders, which could lead to increased luminal iron concentrations that promote the formation of reactive oxygen species (ROS) and subsequent epithelial DNA damage.14,15 Alternatively, an increase in RBC mass might serve as an early indicator of metabolic syndrome, given its correlation with visceral adiposity and insulin resistance observed within our cohort.
Regarding protective factors, female sex (OR=0.534) is likely to benefit from the anti-inflammatory effects of estrogen and the suppression of IGF-1 signaling, both of which collectively inhibit polyp development.16 Furthermore, elevated levels of HDL-C (OR=0.531 per 1 mmol/L) may provide protection through mechanisms such as reverse cholesterol transport and direct antioxidant actions. These include the neutralization of endotoxins and the inhibition of oxidized LDL uptake in colonic tissue.17 Our findings extend previous epidemiological evidence indicating a 22% reduction in colorectal cancer risk for each 0.1 mmol/L increase in HDL-C levels.18
Notably, smoking and diabetes—established risk factors in older populations—lost their statistical independence in multivariate analysis. This divergence suggests that young-onset adenomas may develop through distinct pathways, where hemodynamic stress (hypertension), hematological alterations (RBC count), and acute toxic exposures (alcohol) outweigh traditional metabolic drivers.19 This paradigm shift underscores the necessity for age-specific risk stratification models.20 Clinically, these findings advocate for enhanced colonoscopic screening in young males with hypertension or alcohol consumption habits. High-density lipoprotein cholesterol and red blood cell count should be evaluated as accessible biomarkers for risk stratification, while lifestyle interventions aimed at reducing alcohol intake and controlling blood pressure should be prioritized among high-risk youth.
The limitations of this study include its single-center design, the potential presence of unmeasured confounders (such as dietary patterns and genetic susceptibility), and its cross-sectional nature, which precludes causal inference. Future prospective studies should aim to validate these associations in multi-ethnic cohorts and further elucidate the biological interplay between elevated red blood cell counts and early colorectal carcinogenesis.
Conclusion
This case-control study establishes that young adults (≤40 years) with colorectal adenomatous polyps exhibit distinct metabolic and behavioral risk profiles. Hypertension (OR=2.169, 95% CI: 1.381–3.407), alcohol consumption (OR=1.692, 95% CI: 1.104–2.593), and elevated red blood cell count (per 1 × 10¹²/L increase; OR=1.392, 95% CI: 1.021–1.899) were identified as independent risk factors, conferring increased risks of 2.17-fold, 1.69-fold, and approximately 39.2%, respectively. Conversely, female sex (OR=0.534, 95% CI: 0.391–0.731) and higher HDL-C levels (per 1 mmol/L increase; OR=0.531, 95% CI: 0.318–0.889) were found to be protective factors that reduced the risk by approximately 46.6% and 46.9%. These findings underscore a synergistic interplay between behavioral exposures—such as alcohol use—and metabolic dysregulation—including hypertension and low HDL-C—in the pathogenesis of early-onset adenomas. To address the growing burden of young-onset colorectal lesions, clinicians may consider more vigilant colonoscopic evaluation and metabolic assessment in high-risk young adults—such as males, individuals with hypertension, and those who consume alcohol. Lipid profiles and hematological parameters could serve as potential tools for refining risk stratification in this population.
Author Information
Quan Zheng:He is the Director of the Digestive Endoscopy Center at The Fifth Affiliated Hospital of Zhengzhou University.
Zaizai Li:He is a Master’s candidate in Gastroenterology at The Fifth Affiliated Hospital of Zhengzhou University.
Jiangtian Hu:She is a Master’s candidate in Gastroenterology at The Fifth Affiliated Hospital of Zhengzhou University.
Yukun Chu:He is a Master’s candidate in Gastroenterology at The Fifth Affiliated Hospital of Zhengzhou University.
Xiaolong Shi: He is a Staff Nurse at the Digestive Endoscopy Center of The Fifth Affiliated Hospital of Zhengzhou University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no competing interests in this work.
References
1. Nierengarten MB. Global cancer statistics 2022. Cancer. 2024;130(15):2.
2. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. Ca-a Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
3. Zheng RS, Zhang SW, Zeng HM, et al. Cancer incidence and mortality in China, 2016. J Nat Cancer Center. 2022;2(1):1–9. doi:10.1016/j.jncc.2022.02.002
4. Danpanichkul P, Moolkaew P, Kanjanakot Y, et al. Rising incidence and impact of early-onset colorectal cancer in the Asia-Pacific with higher mortality in females from Southeast Asia: a global burden analysis from 2010 to 2019. J Gastroenterol Hepatol. 2023;38(12):2053–2060. doi:10.1111/jgh.16331
5. Patel SG, May FP, Anderson JC, et al. Updates on age to start and stop colorectal cancer screening: recommendations from the US multi-society task force on colorectal cancer. Gastroenterology. 2022;162(1):285–299. doi:10.1053/j.gastro.2021.10.007
6. Shaukat A, Kahi CJ, Burke CA, Rabeneck L, Sauer BG, Rex DK. ACG clinical guidelines: colorectal cancer screening 2021. Ame J Gastroenterol. 2021;116(3):458–479. doi:10.14309/ajg.0000000000001122
7. Tinawi M. New trends in the diagnosis and management of hypertension. Cureus J Med Sci. 2022;14(2):10.
8. Cheng YX, Tao W, Liu XY, et al. Hypertension remission after colorectal cancer surgery: a single-center retrospective study. Nutrit Cancer-an Inter J. 2022;74(8):2789–2795. doi:10.1080/01635581.2021.2025256
9. Fedirko V, Tramacere I, Bagnardi V, et al. Alcohol drinking and colorectal cancer risk: an overall and dose-response meta-analysis of published studies. Ann Oncol. 2011;22(9):1958–1972. doi:10.1093/annonc/mdq653
10. Li XY, Hur J, Zhang Y, et al. Drinking pattern and time lag of alcohol consumption with colorectal cancer risk in US men and women. Jnci-J Nat Cancer Instit. 2025;117(5):971–979. doi:10.1093/jnci/djae330
11. Puzzono M, Mannucci A, Granno S, et al. The role of diet and lifestyle in early-onset colorectal cancer: a systematic review. Cancers. 2021;13(23):26. doi:10.3390/cancers13235933
12. Wang G, Liu ZC. Alcohol intake associated with increased risk of early-onset colorectal cancer. J Clin Oncol. 2023;41(34):5328. doi:10.1200/JCO.23.01548
13. Lim U, Wilkens LR, Tiirikainen M, Boushey CJ, Kolonel LN, Marchand LL. Colorectal cancer risk associated with alcohol intake is modified by common genetic variants in one-carbon metabolism: the multiethnic cohort study. Cancer Res. 2014;74(19):2. doi:10.1158/1538-7445.AM2014-2193
14. Hilsden RJ, Heitman SJ, Mizrahi B, Narod SA, Goshen R. Prediction of findings at screening colonoscopy using a machine learning algorithm based on complete blood counts (ColonFlag). PLoS One. 2018;13(11):9. doi:10.1371/journal.pone.0207848
15. Tudek B, Speina E. Oxidatively damaged DNA and its repair in colon carcinogenesis. Mutation Res Fundament Mole Mechan Mutagene. 2012;736(1–2):82–92. doi:10.1016/j.mrfmmm.2012.04.003
16. Lee M, Ko HM, Kudose S, et al. High risk features in colorectal adenomatous polyps: a multi-institutional study. Ann Diagnostic Patholog. 2024;72:4. doi:10.1016/j.anndiagpath.2024.152323
17. Patel KKK, Kashfi K. Lipoproteins and cancer: the role of HDL-C, LDL-C, and cholesterol-lowering drugs. Biochem Pharmacol. 2022;196:17. doi:10.1016/j.bcp.2021.114654
18. Yuan FC, Wen WQ, Jia GC, Long JR, Shu XO, Zheng W. Serum lipid profiles and cholesterol-lowering medication use in relation to subsequent risk of colorectal cancer in the UK biobank cohort. Cancer Epidemiol Biomarkers Prev. 2023;32(4):524–530. doi:10.1158/1055-9965.EPI-22-1170
19. Pan P, Li JN, Wang B, et al. Molecular characterization of colorectal adenoma and colorectal cancer via integrated genomic transcriptomic analysis. Front Oncol. 2023;13:13. doi:10.3389/fonc.2023.1067849
20. Patel SG, Murphy CC, Lieu CH, Hampel H. Early age onset colorectal cancer. In: Berger FG, Boland CR, editors. Novel Approaches to Colorectal Cancer. San Diego: Elsevier Academic Press Inc; 2021:1–37.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors for Colorectal Adenocarcinoma in an Indigenous Population in East Africa
Wismayer R, Kiwanuka J, Wabinga H, Odida M
Cancer Management and Research 2022, 14:2657-2669
Published Date: 6 September 2022
Uneven Between-Hospital Distribution of Patient-Related Risk Factors for Adverse Outcomes of Colorectal Cancer Treatment: A Population-Based Register Study
Rattenborg S, Möller S, Frostberg E, Rahr HB
Clinical Epidemiology 2023, 15:867-880
Published Date: 22 July 2023
Improving Adherence of Young Male Patients with HBV Infection to the Regular Follow-Up via Mobile Healthcare Platform Might Be Cost-Effective to Decrease the Morbidity of Advanced Liver Cancer
Liang H, Yang M, Luo D, Wu YK
Patient Preference and Adherence 2024, 18:2581-2595
Published Date: 19 December 2024
A Prospective Nested Case-Control Study of Risk Factors for Postoperative Delirium in Elderly Patients with Colorectal Cancer

Cui X, Cao N, Tian S, Liu Y, Xiang J
Clinical Interventions in Aging 2025, 20:639-648
Published Date: 21 May 2025
Risk Factors for Severe Postoperative Complications After Laparoscopic Colorectal Cancer Surgery in Octogenarians: A Retrospective Cohort Study
Li Y, Du J, Qiu W, Tang J
Clinical Interventions in Aging 2026, 21:590287
Published Date: 27 April 2026