Back to Journals » Clinical Interventions in Aging » Volume 20
Risk Factors for Chronic Post-Surgical Pain in the Elderly: A Single-Center Retrospective Study
Authors Li LH ![]() , Guo H
, Guo H ![]() , Su FZ, Chen J, Xie YB
, Su FZ, Chen J, Xie YB ![]()
Received 4 September 2025
Accepted for publication 25 November 2025
Published 3 December 2025 Volume 2025:20 Pages 2363—2376
DOI https://doi.org/10.2147/CIA.S562458
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Zhi-Ying Wu
Li-Heng Li,1,* Hao Guo,2,* Feng-Zhi Su,3 Jie Chen,4 Yu-Bo Xie1,5
1Department of Anesthesiology, The First Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China; 2Department of Anesthesiology, Renmin Hospital, Hubei University of Medicine, Shiyan, People’s Republic of China; 3Department of Anesthesiology, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, People’s Republic of China; 4Department of Anesthesiology, The Second Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China; 5Department of Anesthesiology, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu-Bo Xie, Department of Anesthesiology, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China, Email [email protected]
Purpose: Chronic Post-Surgical Pain (CPSP) is a common surgical complication, but the association between perioperative complications, patients’ intrinsic mental status, and 3-month CPSP remains unclear in elderly surgical populations. This study thus aims to identify perioperative risk factors for 3-month CPSP in elderly patients after non-cardiac surgery, with CPSP here defined as pain intensity ≥ 3 on the Numerical Rating Scale at 3-month follow-up.
Patients and Methods: This retrospective study included 367 elderly patients. We first analyzed variables with descriptive statistics, then conducted all subsequent analyses separately for each of the three surgical subgroups, allowing for potential nuances in the contributory patterns of key factors across groups. To predict 3-month CPSP, we used 10 machine learning algorithms. Model performance was assessed via repeated 5-fold cross-validation, and top-performing models were interpreted using SHapley Additive exPlanations (SHAP) to clarify how key factors contribute.
Results: Of 367 patients, the overall prevalence of 3-month CPSP was 25.07%, with significant variation across surgical subgroups: 48.05% in orthopedic surgery, 10.34% in urinary tumor surgery, and 7.14% in abdominal tumor surgery. The Random Forest model showed strong, consistent predictive ability across the three subgroups. Frailty was a key shared risk factor for CPSP across all surgical types, and further analyses identified surgery-specific risk factors.
Conclusion: These findings demonstrate that data-driven models can reliably predict CPSP across studied surgical types, with frailty state as a universal risk factor and distinct surgery-specific profiles supporting tailored perioperative risk assessment and prevention strategies.
Keywords: elderly patients, chronic post-surgical pain, risk factors, machine learning algorithms
Introduction
Chronic post-surgical pain (CPSP) refers to pain in and around the surgical area that lasts longer than 3 months, excluding pain due to disease recurrence, inflammation, and other factors. In contrast, acute postoperative pain is defined as pain occurring within the first 72 hours after surgery, typically resolving as tissue heals. The incidence rates vary significantly among different surgical procedures. For limb amputation, it ranges from 30% to 85%; for knee joint replacement, it is between 13% and 44%. Moreover, the incidence rate is influenced by the patient’s own factors, such as being young, being female and having preoperative chronic pain, and surgical-related factors, such as long surgical duration and intraoperative nerve injury.1 Despite growing awareness of the impact of CPSP, healthcare providers frequently prioritize acute postoperative pain management, leading to inadequate intervention for CPSP.2,3 A prevalent misconception persists that postoperative pain should resolve spontaneously, neglecting the complex interplay of biological, psychological, and social determinants.4–6 Hypoactive manifestations of CPSP, characterized by absent overt pain behaviors, often evade clinical detection, resulting in delayed interventions and poorer outcomes. Recent studies,7 particularly those focusing on elderly populations, have highlighted that this subtle presentation contributes to significant underdiagnosis in older adults.
CPSP consequences in elderly patients are profound, encompassing prolonged functional disability, elevated healthcare utilization, and reduced survival rates.8–10 Epidemiological data indicate that elderly individuals have a notably higher CPSP incidence compared to younger adults across various surgical specialties.11 Nevertheless, the pathophysiological mechanisms underlying CPSP remain incompletely elucidated. Although CPSP arises from interactions between patient-specific vulnerabilities such as preexisting pain disorders and psychological distress, and surgery-induced factors including tissue trauma and neuroinflammation, the precise mechanisms perpetuating chronicity are undefined. Age-related physiological decline, multimorbidity, and diminished pain tolerance collectively exacerbate vulnerability in this population. Frailty, for instance, impacts neuroinflammatory responses and impairs neural repair capacity, while comorbidities like diabetes or cardiovascular disease amplify systemic inflammation, both of which directly influence CPSP development.12–14 CPSP imposes a substantial burden through mobility restrictions, heightened dependency, and aggravated mental health comorbidities, ultimately compromising independence and overall well-being.
To address these gaps, we designed a retrospective study to investigate multifactorial relationships between clinically relevant confounders and CPSP development in elderly surgical patients. We focused on orthopedic, urologic oncology, and abdominal oncology surgeries, as these specialties exhibit distinct clinical CPSP incidence rates and risk profiles. In the context of pain prediction, machine learning approaches have emerged as a promising tool in the field, offering advantages over traditional regression analysis such as robust handling of multivariable interactions and improved predictive accuracy. Among these machine learning-driven pain prediction frameworks, SHapley Additive exPlanations (SHAP) further enhances practical utility by quantifying the contribution of each input feature to individual pain predictions, addressing the “black box” limitation of complex models and enabling clinicians to interpret and trust the model’s outputs.15,16 This study situates itself within the growing body of research applying machine learning to CPSP prediction, aiming to refine risk stratification in elderly populations.
Materials and Methods
Study Design and Patient Selection
This single-center retrospective study analyzed data from the electronic health records and follow-up system of the First Affiliated Hospital of Guangxi Medical University. We included patients aged 65 years or older who underwent elective surgery under general anesthesia between September 2020 and August 2022. The primary outcome was CPSP, defined as a pain intensity≥3 on the NRS at 3-month follow-up despite analgesic therapy. This threshold aligns with elderly pain assessment needs and prior elderly CPSP studies, as older adults often exhibit altered pain perception that makes milder pain (NRS 3–4) clinically meaningful; this choice is consistent with established literature in the field, mitigating concerns about potential overestimation of incidence. This study approved by the Medical Ethics Committee of the First Affiliated Hospital of Guangxi Medical University (NO.2019 (KY-E-115)) and registered at the Chinese Clinical Trial Registry (ChiCTR2000032008), adhered to the STROBE guidelines and the principles of the Helsinki Declaration. When conducting the study, we relied on the hospital’s electronic medical records and ensured strict confidentiality of patient data. Before the study data was analyzed, informed consent to participate in the study had been obtained from all participants or their legal guardian(s), and the follow-up data had been obtained with verbal consent from the patients or their guardians. 3-month follow-up was used because longer-term follow-up (6–12 months) data would face the common challenge of incomplete records in elderly postoperative studies; given the relatively small sample size, this choice allowed us to use complete real data for analysis without data imputation.
Inclusion Criteria: (1) Aged ≥65 years; (2) American Society of Anesthesiologists (ASA) physical status classification I–IV; (3) Scheduled for elective surgery under general anesthesia.
Exclusion Criteria: (1) Cardiac or neurosurgical procedures; (2) Preoperative history of dementia or psychiatric disorders; (3) Incomplete medical records.
Clinical Data Collection
The data of this study were obtained from reviewing postoperative follow-up records and the medical record information system.
Preoperative variables encompassed demographic parameters (gender, age, body mass index [BMI]) and documented preoperative medical history, including conditions such as cardiovascular diseases, chronic kidney disease, infections occurring within 30 days prior to surgery, and surgical history—among which the surgical history does not include the site of the current surgery, as the surgery undergone by the patient during follow-up was the first surgery on that site. Psychosocial evaluations comprised: assessment of pain-related catastrophic thinking using the Pain Catastrophizing Scale (PCS);17 screening for anxiety and depressive disorders with the 7-item Generalized Anxiety Disorder (GAD-7)18 and 9-item Patient Health Questionnaire (PHQ-9),19 where scores ≥4 indicated clinically relevant symptoms; Frailty was defined as the FRAIL Score>2.13,20 Evaluation of preoperative sleep patterns over the preceding month via the Sleep Numerical Rating Scale (Sleep-NRS),21–23 with scores ≤6 denoting impaired sleep quality; and systematic recording of pre-existing pain conditions.
Intraoperative metrics included total operative time, estimated blood loss, intraoperative opioid administration (expressed as morphine milligram equivalents [MME]), Due to the short duration of remifentanil-induced analgesia and variation in surgical duration among patients, the opioid statistics here only include medium- or long-acting opioids, and utilization of patient-controlled analgesia (PCA) devices. This study’s three subgroups all involved complex surgeries: the Orthopedic subgroup included major joint replacement and spinal fusion with large incisions, extensive dissection and long operative time, the Urinary tumor subgroup focused on radical resection of urinary system tumors requiring precise dissection around major blood vessels and nerves, and the Abdominal tumor subgroup comprised radical resection of abdominal solid tumors involving multi-organ mobilization and complex anastomosis; for such surgeries, key intraoperative factors are standardized or reflected in recorded metrics—surgical trauma is uniformly moderate to severe per STS and shown by total operative time and estimated blood loss, anesthesia is general anesthesia with consistent use of common drugs so no extra recording is needed, and nerve monitoring and protection are mandatory for nerve-rich surgeries so no separate documentation is needed—with no need for additional variable collection to ensure data sufficiency for relevant risk analysis.
Postoperative outcomes: Acute pain trajectory quantified using the Revised American Pain Society Patient Outcome Questionnaire (APS-POQ-R)24 on postoperative days (POD) 1, 3, and 5. Pain burden was stratified by cumulative weighted scores: 0–10 (minimal), 11–35 (moderate), and 36–70 (severe). Sleep architecture disruption was assessed using Sleep-NRS thresholds on POD 1, 3, and 7, where a single score of ≤6 at any of these time points indicated a postoperative sleep disorder. Postoperative neurocognitive disorder (PND) diagnosed according to DSM-III-R criteria using the Confusion Assessment Method (CAM)25 protocol at standardized intervals (POD 1, 3, 7). CPSP operationalized as persistent pain (NRS≥3 at 3-month follow-up despite guideline-directed analgesic therapy. Healthcare-associated infections identified through structured review of electronic medical records for new-onset infection-related ICD-10 codes documented during the index hospitalization.
Sample Size Rationale
A total of 367 patients with 100% complete data (no missing values in key variables, including demographics, perioperative metrics, and 3-month follow-up outcomes for CPSP) were finally included. Analyses were conducted separately for three subgroups: Orthopedic (n = 154), Urinary tumor (n = 87), and Abdominal tumor (n = 126). The sample size of the overall cohort and each subgroup was determined based on the availability of complete historical follow-up data, with statistical adequacy validated for both the overall study and individual subgroups as follows:
Statistical Adequacy of the Overall Cohort
For the core CPSP-related association analyses, GPower 3.1 was used to verify sample size sufficiency. With a preset moderate effect size (odds ratio [OR] = 1.8, consistent with the reported association between preoperative pain and CPSP in relevant literature), significance level (α) = 0.05, and statistical power (1-β) = 80%, the minimum required sample size was calculated as 92 cases. The overall cohort of 367 cases far exceeded this threshold, ensuring sufficient foundational power for cross-subgroup trend comparisons.
Statistical Adequacy of Individual Subgroups
Orthopedic subgroup (n = 154): During follow-up, 48.05% (n = 74) of patients developed CPSP. GPower 3.1 calculations showed the minimum sample size required to detect an OR = 1.8 (α = 0.05, 80% power) for CPSP-associated factors was 95 cases. Both the total case count (154) and CPSP event count (74) in this subgroup exceeded the threshold, confirming sufficient power for independent inferential analyses. Urinary tumor subgroup (n = 87): CPSP incidence was 10.34% (n = 9). Due to the small number of CPSP events, the minimum sample size required to detect an OR = 1.8 (α = 0.05, 80% power) was 110 cases—exceeding the subgroup’s total case count (87). Thus, this subgroup had limited statistical power for standalone inferential analyses and was only included to explore preliminary CPSP-related trends. Abdominal tumor subgroup (n = 126): CPSP incidence was 7.14% (n = 9). Similarly, the small number of CPSP events meant the subgroup’s total case count (126) fell short of the 128-case threshold required to detect an OR = 1.8 (α = 0.05, 80% power). This subgroup was also analyzed for preliminary trend exploration rather than independent inference. For the Urinary tumor subgroup (9 CPSP cases) and Abdominal tumor subgroup (9 CPSP cases) with small sample sizes, Bayesian correction was adopted for bias correction, and the corrected results are presented in Supplementary Table 1. It should be clearly stated that the conclusions of these two subgroups are only for trend exploration and need to be verified by studies with larger sample sizes or multi-center designs.
Statistical Analysis
Statistical Description and Preliminary Analyses
SPSS 27 software was used to perform statistical analyses, with descriptive statistics reported as mean (standard deviation) for normally distributed continuous variables, median (interquartile range) for non-normally distributed continuous variables, and frequencies (percentages) for categorical variables. For intergroup comparisons of continuous variables, independent-samples t-tests were applied to normally distributed data, while the Mann–Whitney U-test was used for non-normally distributed data.
Data Preprocessing and Modeling Analysis
All modeling analyses were conducted in R Studio (Version 4.5.0) with key packages including caret, pROC, xgboost, glmnet, kernelshap, shapviz, ggplot2, and ggpubr. Consistent preprocessing procedures were applied across all three surgical subgroups:
Missing values: All core variables had a missing proportion of 0%, so no missing value imputation was performed; Continuous variables were standardized; Categorical variables were converted to factor variables with original levels retained; Variables with zero or near-zero variance were excluded.
An identical analytical framework was employed to independently predict 3-month CPSP for each surgical subgroup, utilizing the same panel of machine learning algorithms: random forest, XGBoost, support vector machine, logistic regression, k-nearest neighbors, partial least squares, generalized boosting models, neural networks, linear discriminant analysis, and lasso regression. Rationale for comparing multiple algorithms: 1) To avoid “single-model bias” by including both non-linear and linear models for comprehensive performance verification; 2) To adapt to the small number of CPSP events in partial subgroups, algorithms with different robustness were included to validate model stability across subgroups; 3) Naive Bayes and AdaBoost were not included in the presented analytical models. Both algorithms are less suitable for small-sample model calculations—Naive Bayes relies on strong independence assumptions that easily fail with limited data, leading to biased predictions, while AdaBoost tends to overfit with small sample sizes and cannot ensure reliable generalization across subgroups. Bayesian methods were employed for small-sample correction. Model performance was evaluated using 5-fold repeated cross-validation (three repetitions) via the trainControl function, which saved final predictions and class probabilities to estimate generalization error. The twoClassSummary function was used as the summary metric to focus on ROC curve performance.
Hyperparameter tuning was implemented for all algorithms to maximize model performance, with cross-validation integrated into the optimization process and the highest cross-validated AUC adopted as the criterion for determining the final hyperparameter combination. For the XGBoost algorithm, grid search was employed to optimize hyperparameters including nrounds (set to 50 and 100) and max_depth (set to 3 and 5), while other parameters were fixed as eta = 0.1, gamma = 0, colsample_bytree = 0.7, min_child_weight = 1, and subsample = 0.7. For the Neural Network, grid search focused on two hyperparameters—size (with values of 1 and 2) and decay (with values of 0.01 and 0.1)—and the training process was restricted to a maximum of 500 iterations. For Lasso Regression, the grid search covered alpha = 1 and lambda (which was set to 10 levels within the range of 0.01 to 0.5). For the remaining algorithms, including Random Forest, Support Vector Machine, and Generalized Boosting Models, hyperparameter optimization was carried out using a tune length of 5.
Model performance metrics: For each algorithm, 5 performance metrics were calculated based on a prediction probability threshold of 0.5: AUC (via the roc function), accuracy, sensitivity, specificity, and F1 score.
For each surgical subgroup, the best-performing model (defined by the highest cross-validated AUC) underwent in-depth interpretation using SHAP. Derived from game theory, SHAP values quantified individual feature contributions to predictions, clarifying how specific features influenced predicted CPSP risk within each subgroup. Subgroup-predictor interaction effects were assessed via likelihood ratio tests. For small-event subgroups, Bayesian correction with weakly informative priors was used to reduce bias.
Results
Baseline Characteristics
A total of 367 patients were included, with 92 (25.07%) developing CPSP during follow-up. Table 1 presents baseline data of 367 patients, grouped as Orthopedic (n = 154), Urinary tumor (n = 87), and Abdominal tumor (n = 126). Patients had a mean age of 71.66 ± 5.77 years, with varying frail state proportions (highest in Orthopedic). ASA classification, intraoperative blood loss, GAD - 7 (≥4), PHQ - 9 (≥4), and preoperative sleep disorder rates differed across groups. Notably, CPSP prevalence showed significant variation: 25.07% overall, with 48.05% in Orthopedic, 10.34% in Urinary tumor, and 7.14% in Abdominal tumor. Notably, CPSP prevalence showed significant variation. This discrepancy likely stems from orthopedic surgeries involving more musculoskeletal manipulation and higher peripheral nerve injury risk—key triggers for persistent pain linked to CPSP—while urinary and abdominal tumor surgeries focus on visceral/soft-tissue resection with less nerve impact. The orthopedic cohort also has the highest proportion of frail patients, whose weaker pain modulation, higher inflammation, and poorer tissue repair, when combined with the greater trauma of orthopedic surgeries, further elevate CPSP risk.
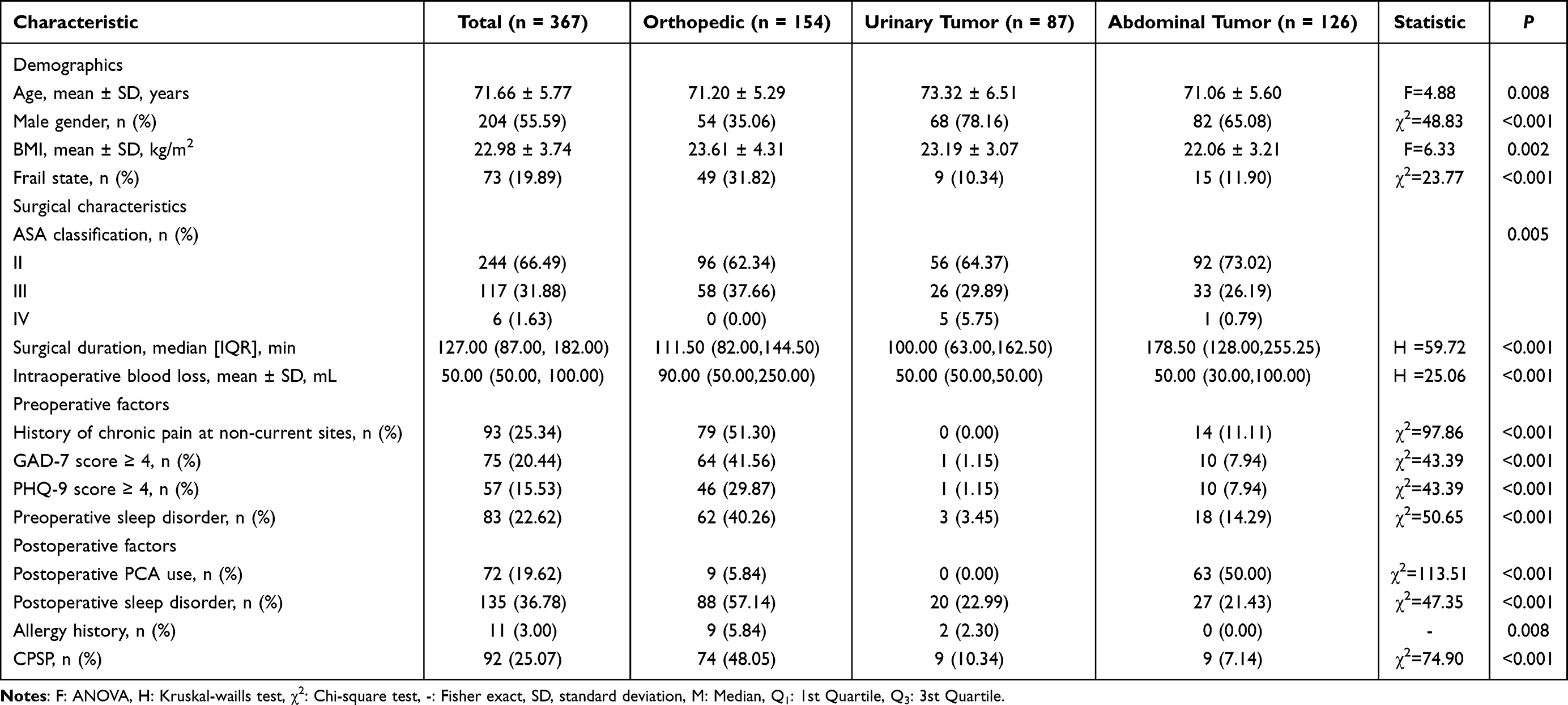 |
Table 1 Baseline Data |
Predictive Model Performance
Among machine learning prediction methods, the Random Forest model consistently demonstrated the best performance in predicting the incidence of CPSP across three surgical types. As shown in Figure 1, the AUC of the Random Forest model was 0.958 in orthopedic surgery (Figure 1A), 0.937 in urinary system tumor surgery (Figure 1B), and 0.859 in abdominal tumor surgery (Figure 1C), outperforming other models. Table 2 presents the incidence of CPSP in each surgical group and the corresponding parameters of the machine learning models. The model parameters indicate that the CPSP prediction for elderly patients undergoing orthopedic surgery exhibits stability and high applicability. However, the Sensitivity of the CPSP prediction for abdominal tumor surgeries is not very good and requires further optimization.
 |
Table 2 Best Model of Surgery Types |
 |
Figure 1 Comparison of Model ROC Curves for three types of surgery. ROC curves of predictive models for Orthopedic (A), Urinary tumor (B), and Abdominal tumor surgery (C), illustrating the true positive rate vs false positive rate across machine learning algorithms. |
To determine whether the model analysis is biased due to small sample size and verify the presence of interaction effects among the analyzed factors, this study used the likelihood ratio test to examine interaction effects and employed Bayesian methods to refine parameter estimation (to address potential small-sample bias). Subgroup-predictor interaction effects were not statistically significant (p=0.66; α=0.05, Supplementary Table 1), indicating that the association between each shared predictor and postoperative pain does not differ significantly across subgroups. Meanwhile, Bayesian parameter estimation adjusted the effects of core variables across subgroups, with changes in odds ratios and AUC values reported in Supplementary Table 2. This adjustment refines the effect estimates of core variables within each subgroup to enhance the reliability of statistical inferences.
Key Risk Factors for CPSP
Feature importance analysis (Figure 2) identified frailty state as the most critical risk factor for CPSP across all three surgical types. Beyond this shared factor, distinct risk profiles emerged by surgical type, the importance of these features is represented by the absolute values of SHAP.
 |
Figure 2 SHAP-Based Feature Importance for Predictive Models of Different Surgery Types. Panels (A) (Orthopedic surgery), (B) (Urinary tumor surgery) and (C) (Abdominal tumor surgery) present the absolute SHAP values, which are used to indicate the extent of the influence of the corresponding features on the prediction results (without distinguishing whether the influence is positive or negative). |
In orthopedic surgery (Figure 2A), additional important factors included age, postoperative sleep disorder, history of chronic pain at non-current sites, and intraoperative blood loss. In urinary tumor surgery (Figure 2B), notable factors were postoperative AST/ALT, MME, postoperative monocyte percentage, and surgery duration. In abdominal tumor surgery (Figure 2C), relevant factors included GAD-7 score, postoperative PCA use, respiratory tract infection in the past month, and preoperative sleep disorder.
To enhance transparency of the results, the summary plots of SHAP value distributions for the top 5 features across the three surgical subgroups have been uploaded as Supplementary Figure 1. Additionally, the plots of SHAP absolute values with confidence intervals estimated via Bootstrap resampling for the three surgical subgroups have been uploaded as Supplementary Figure 2.
Patterns of Feature Impact on CPSP Risk
SHAP dependence analysis showed that for orthopedic surgery, categorical features (such as frailty state, postoperative sleep disorder) had distinct impact patterns on CPSP risk across different levels, while continuous features (age, intraoperative blood loss) exhibited nonlinear relationships, reflecting complex CPSP associations (Figure 3A–3E).
 |
Figure 3 SHAP Dependence Plots for Key Features in Orthopedic Surgery Predictive Models. Panels (A)–(E) show SHAP-derived feature impacts on orthopedic surgery model predictions: (A) (“Frail state”, 0=non-frail, 1=frail) uses yellow/blue boxplots for positive/negative impacts; (B) (“Age”) has a red curve (with CI) showing a non-linear trend that rises first and drops after 75–80 years; (C) (“Postop sleep disorder”, 0=no, 1=yes) and (D) (“Chronic pain history (non-current sites)”, 0=no, 1=yes) both use yellow boxplots to indicate disorder/history increases predictions; (E) (“Intraoperative blood loss”) has a red curve showing a non-linear pattern that rises to ~1000 mL then drops. SHAP values clarify feature importance/interactions and how clinical factors shape predictions. |
In urinary tumor surgery, categorical feature (Frail state) showed divergent risk distributions, and continuous features (Postoperative AST/ALT, MME, Postoperative monocyte percentage, Surgery duration) displayed diverse nonlinear patterns, underlining complexity in their CPSP links (Figure 4A–4E).
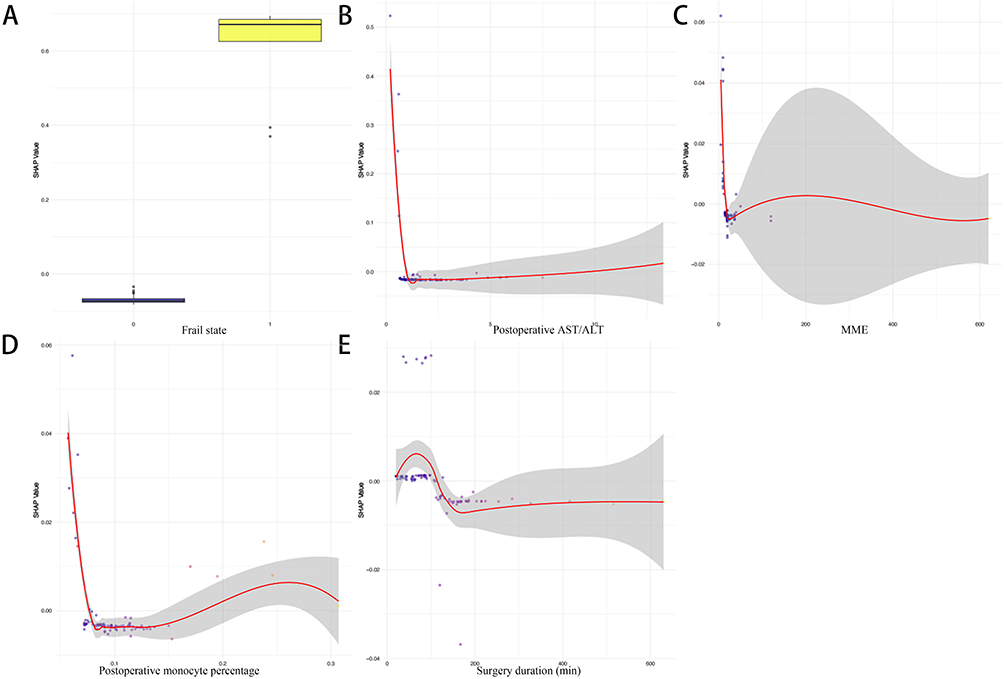 |
Figure 4 SHAP Dependence Plots for Key Features in Urinary Tumor Surgery Predictive Models. Panels (A–E) use SHAP to show how features influence urinary tumor surgery model predictions: (A) (“Frail state”, 0=non-frail, 1=frail) uses yellow/blue boxplots for distinct output impact patterns; Postoperative AST/ALT (B), Postoperative monocyte percentage (C), Postoperative monocyte percentage (D), Surgery duration (C, min) with CI depicting its non-linear relationship with predictions. |
For abdominal tumor surgery, different levels of categorical features (Frail state, GAD-7≥4, Preoperative PCA use, Respiratory tract infections in the past month, Preoperative sleep disorder) connected to distinct risk profiles, showing varied CPSP effects (Figure 5A–5E).
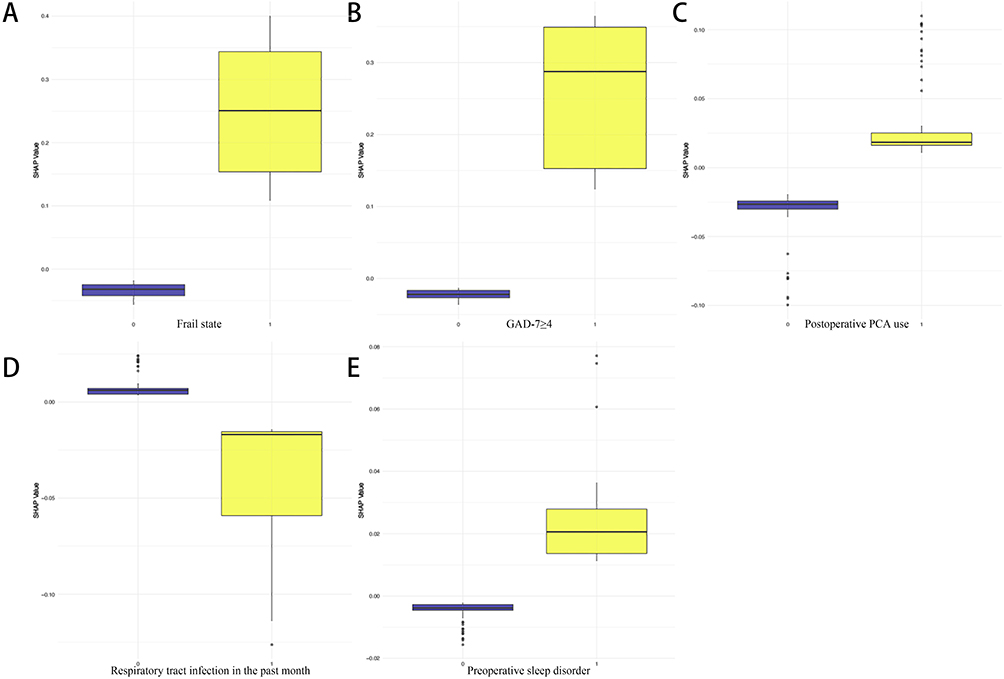 |
Figure 5 SHAP Dependence Plots for Key Features in Abdominal Tumor Surgery Predictive Models. Panels (A–E) use the SHAP to demonstrate how clinical features influence the predictions of machine learning models for abdominal tumor surgery (all features: 0 = no, 1 = yes), which helps clarify the contribution of clinical factors to the predictive model. These features include frailty status (A), GAD-7 ≥ 4 (B), postoperative PCA use (C), recent respiratory tract infection (D), and preoperative sleep disorder (E). |
Individual Sample Risk Contributions
Figure 6 consists of three subplots, with each subplot illustrating the SHAP interpretation for a random patient within one of three distinct surgical types. In orthopedic surgery samples, frailty state, postoperative sleep disorder, and history of chronic pain at non-current surgical sites were associated with an increased risk, while postoperative neutrophil percentage had a protective effect (Figure 6A). In urinary tumor surgery samples, preoperative lymphocyte percentage was associated with an elevated risk, whereas frailty state and postoperative AST/ALT were associated with a reduced risk (Figure 6B). In abdominal tumor surgery samples, postoperative PCA device use and frailty state were associated with a lowered risk, while respiratory tract infection in the past month was associated with a slightly increased risk (Figure 6C).
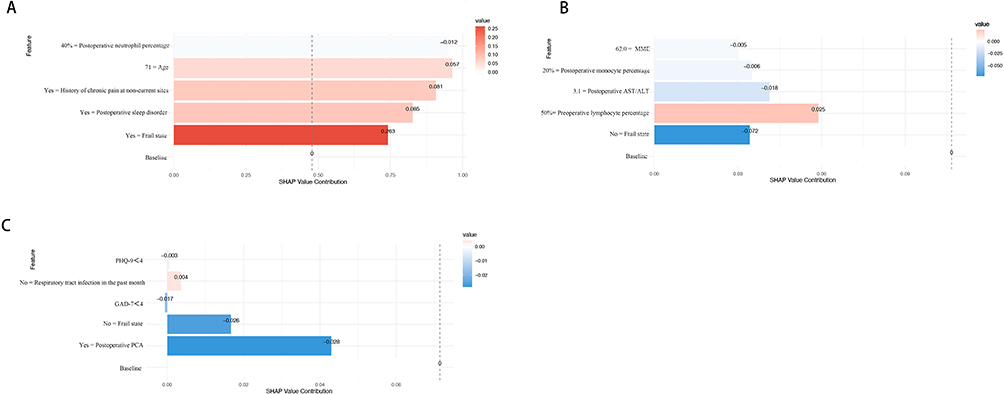 |
Figure 6 SHAP Waterfall Plots Illustrating Feature Contributions for Random Samples Across Models. This figure presents SHAP waterfall plot, analyzing feature contributions in orthopedics (A), urological tumor (B), and abdominal tumor (C) models by randomly selecting one sample from each. Features like orthopedic frailty state, urological preoperative lymphocyte percentage, and general surgical postoperative PCA usage have their SHAP values successively superimposed, illustrating the specific contribution direction and degree of each random single sample’s features to prediction results. Note that these SHAP values only represent the feature contribution of the corresponding random single sample, not the overall population’s feature importance. |
The findings demonstrate that the Random Forest model reliably predicts CPSP across orthopedic, urinary tumor, and abdominal tumor surgeries, with strong performance across all types. A key universal insight is the consistent importance of frailty state as a core risk factor, underscoring its role in CPSP development regardless of surgical context. However, distinct risk profiles emerged by surgical type, reflecting the influence of procedure-specific factors (e.g., intraoperative factors in orthopedics, metabolic markers in urinary tumor surgery, and psychological/analgesic factors in abdominal surgery). SHAP analyses further revealed that these factors exert nonlinear and heterogeneous effects on risk, with both risk-enhancing and protective contributions observed at the individual level. Collectively, these results highlight the value of tailored risk assessment and intervention strategies aligned with surgical type, while emphasizing frailty state as a cross-cutting target for CPSP prevention.
Discussion
CPSP remains a complex and multifactorial challenge in elderly patients. Our retrospective study provides support for understanding this issue through analyses on three different surgical types in the elderly population, with preliminary analyses frameworks developed based on clinical data of limited sample size. We found that preoperative frailty status was closely related to the occurrence of CPSP. Frailty may drive CPSP development by directly interacting with CPSP’s core pathological mechanisms: it enhances persistent inflammation via impaired immune homeostasis in frail elderly, weakens central pain regulation, due to age-related decline in descending inhibitory pathways, and accelerates neural sensitization by prolonging nociceptive input from delayed tissue repair. However, the occurrence of chronic pain after each type of surgery is also related to factors such as sleep status, immune cells, intraoperative opioid dosage, and postoperative use of PCA. Notably, the role of postoperative PCA use in CPSP may be mediated by its effect on acute pain control: adequate PCA-delivered analgesia can reduce acute pain to prevent central sensitization, while excessive PCA use might potentially increase CPSP risk via opioid-induced hyperalgesia—this mechanism requires further clarification with more targeted data. Beyond these considerations, among the top 5 risk factors for each type of surgery, preoperative frailty is the most prominent factor shared across all types; other factors differ by surgical type, and these differences are closely related to surgical type and patients’ underlying diseases.
Intraoperative bleeding in orthopedic surgery, linked to CPSP risk, resonates with the recognized role of tissue injury and inflammation in chronic pain development. Recent research25,26 demonstrated that trauma activates pro-inflammatory pathways, which can persistently alter neural plasticity. Our data further emphasize the importance of minimizing blood loss during surgery, potentially through advanced hemostatic techniques, cell-sparing procedures, or correction of preoperative anemia. Beyond surgical bleeding, age also emerges as a notable contributor to CPSP risk among older adults undergoing orthopedic procedures, with its influence warranting careful consideration in risk assessment and management.
Anxiety status as a risk factor for CPSP in patients undergoing abdominal tumor surgery may align with extensive prior research, and this finding—given the limited number of CPSP cases in the subgroup—should be regarded as a hypothesis to be validated in larger, multicenter cohorts. Psychological factors such as anxiety modulate pain perception through the limbic system, as supported by recent studies.27,28 Patients facing abdominal tumor surgeries are often consumed by anxiety, constantly fretting over the malignancy degree of the tumor, the intricacies of the surgical procedure, and the prospects of recovery. This anxious state can disrupt the body’s normal stress-regulating mechanisms. For example, it may lead to overactivation of the sympathetic nervous system, resulting in elevated heart rates and blood pressures during the operation, which not only increases the complexity of anesthesia management but also has the potential to impact the surgical field, further contributing to the development of CPSP. Enhanced Recovery After Surgery (ERAS) might have a role to play in the rehabilitation of these patients, with effective postoperative analgesia also showing promise in inhibiting the development of CPSP in this population.
In patients with urological tumors, MME use shows a notable association with the development of CPSP, which may align with emerging theories that effective acute pain control may mitigate central sensitization; due to the small number of CPSP cases in the urological tumor subgroup, this association should be considered a hypothesis to be further verified. For this patient population, emphasis should be placed on intraoperative pain management.29–32
Through comparisons between our research and real-world observations, a potential bidirectional association may exist between sleep and pain. While the exact mechanisms remain unclear, potential pathways include cytokine dysregulation and neurotransmitter imbalance, which may contribute to central sensitization—this directly links sleep disorders to CPSP’s core pathological processes. Additionally, cytokine dysregulation also amplifies persistent inflammation, another key driver of CPSP and neural sensitization.33,34 Clinical evidence suggests that disrupted sleep architecture post-surgery, characterized by reduced slow-wave sleep and increased awakenings, correlates positively with persistent pain.35–37 Notably, sleep disturbances and pain may form a vicious cycle: pain fragments sleep, and sleep deprivation exacerbates pain perception, especially in patients with pre-existing sleep issues. Future research should focus on evaluating the efficacy of sleep interventions in preventing CPSP and elucidating the neural mechanisms underlying this interaction.
Notably, perioperative pain management holds significant importance for the occurrence and development of postoperative chronic pain; yet, relying solely on opioid medications may not adequately address this issue, and thus requires the exploration of multimodal analgesia. For instance, Archana O’Neill and Philipp Lirk38 proposed that adequate early analgesia can reduce opioid use, thereby breaking the cycle leading to chronic pain development. This underscores the need for personalized opioid management strategies. Future research could integrate genetic factors, such as opioid receptor polymorphisms, to better understand this complex association.39
Our study has limitations despite its valuable data. As a single-center retrospective analysis, it has potential selection bias and limited generalizability. The overall sample size is small due to follow-up data constraints; urinary tumor and abdominal tumor subgroups have only 9 CPSP cases each and remain underpowered, though small-sample bias correction was performed to mitigate inaccurate estimation. Self-reported pain and sleep data may cause reporting bias. While our machine learning models were validated via K-fold cross-validation and showed no overt overfitting, they still face potential overfitting risk due to the number of predictors relative to outcome events, and lack external validation, limiting applicability. CPSP follow-up of 3 months is short, potentially missing late cases.
Future research should use objective tools, expand to multi-center cohorts, add external validation, explore missing data mechanisms, extend follow-up, incorporate metabolic analysis, integrate genetic testing, and design randomized controlled trials.
Conclusion
This study explored the prediction of CPSP across three distinct surgical subgroups using a retrospective design, yielding preliminary key insights for clinical practice and hypothesis generation. Consistent with the strong performance of the Random Forest model, our findings confirm that data-driven risk assessment can effectively identify patients at risk of CPSP. A critical universal observation is the central role of frailty state in CPSP development, emphasizing its potential as a cross-surgical target for preventive interventions. However, the identification of distinct surgical type-specific risk profiles highlights the necessity of tailored risk evaluation strategies aligned with procedure characteristics. These findings bridge the gap between empirical observation and personalized risk management, supporting the integration of targeted assessment tools into perioperative care. Future research should focus on validating these risk profiles in larger, diverse cohorts and developing intervention protocols that address both universal and surgery-specific risk factors, ultimately aiming to reduce the burden of CPSP and improve postoperative quality of life.
Ethics Approval and Consent to Participate
The study was performed in strict accordance with the Declaration of Helsinki. The study protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital of Guangxi Medical University, China (Identifier: NO.2019 (KY-E-115)). The informed consents to participate in the study had been obtained from all participants or their legal guardian(s). Where all data were collected from existing medical records (with follow-up data obtained with verbal consent from patients or their guardians) and were completely de-identified (ie, no personal identifiers could be linked to individual participants). The study was registered at the Chinese Clinical Trial Registry (www.chictr.org.cn, Registration number: ChiCTR2000032008).
Funding
This work was supported by Guangxi Science and Technology Base and Talent Special Project (No. AD25069060) and Guangxi Key Research and Development Program (No. AB24010066).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/S0140-6736(19)30352-6
2. Geneen LJ, Moore RA, Clarke C, Martin D, Colvin LA, Smith BH. Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2017;4(4):CD011279. doi:10.1002/14651858.CD011279.pub3
3. Ehde DM, Dillworth TM, Turner JA. Cognitive-behavioral therapy for individuals with chronic pain: efficacy, innovations, and directions for research. Am Psychol. 2014;69(2):153–166. doi:10.1037/a0035747
4. Edwards RR, Dworkin RH, Sullivan MD, Turk DC, Wasan AD. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J Pain. 2016;17(9 Suppl):T70–92. doi:10.1016/j.jpain.2016.01.001
5. Kohrt BA, Griffith JL, Patel V. Chronic pain and mental health: integrated solutions for global problems. Pain. 2018;159(1):S85–S90. doi:10.1097/j.pain.0000000000001296
6. Leung DKY, Fong APC, Wong FHC. Nonpharmacological Interventions for Chronic Pain in Older Adults: a Systematic Review and Meta-Analysis. Gerontologist. 2024;64(6). doi:10.1093/geront/gnae010
7. Sluka KA, Wager TD, Sutherland SP, et al. Predicting chronic postsurgical pain: current evidence and a novel program to develop predictive biomarker signatures. Pain. 2023;164(9):1912–1926. doi:10.1097/j.pain.0000000000002938
8. Schwan J, Sclafani J, Tawfik VL. Chronic Pain Management in the Elderly. Anesthesiol Clin. 2019;37(3):547–560. doi:10.1016/j.anclin.2019.04.012
9. Zis P, Daskalaki A, Bountouni I, Sykioti P, Varrassi G, Paladini A. Depression and chronic pain in the elderly: links and management challenges. Clin Interv Aging. 2017;12:709–720. doi:10.2147/CIA.S113576
10. Domenichiello AF, Ramsden CE. The silent epidemic of chronic pain in older adults. Prog Neuropsychopharmacol Biol Psychiatry. 2019;93:284–290. doi:10.1016/j.pnpbp.2019.04.006
11. Tinnirello A, Mazzoleni S, Santi C. Chronic Pain in the Elderly: mechanisms and Distinctive Features. Biomolecules. 2021;11(8):1256. doi:10.3390/biom11081256
12. Honda H, Ashizawa R, Kiriyama K. Chronic pain in the frail elderly mediates sleep disorders and influences falls. Arch Gerontol Geriatr. 2022;99:104582. doi:10.1016/j.archger.2021.104582
13. Dai Z, Wu Y, Chen J, Huang S, Zheng H. Assessment of relationships between frailty and chronic pain: a bidirectional two-sample Mendelian randomisation study. Age Ageing. 2024;53(1). doi:10.1093/ageing/afad256
14. Esses G, Deiner S, Ko F, Khelemsky Y. Chronic Post-Surgical Pain in the Frail Older Adult. Drugs Aging. 2020;37(5):321–329. doi:10.1007/s40266-020-00761-2
15. Wang Y, Zhu Y, Xue Q, et al. Predicting chronic pain in postoperative breast cancer patients with multiple machine learning and deep learning models. J Clin Anesth. 2021;74:110423. doi:10.1016/j.jclinane.2021.110423
16. Langford DJ, Reichel JF, Zhong H, et al. Machine learning research methods to predict postoperative pain and opioid use: a narrative review. Reg Anesth Pain Med. 2025;50(2):102–109. doi:10.1136/rapm-2024-105603
17. Darnall BD, Sturgeon JA, Cook KF. Development and Validation of a Daily Pain Catastrophizing Scale. J Pain. 2017;18(9):1139–1149. doi:10.1016/j.jpain.2017.05.003
18. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
19. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
20. Abellan van Kan G, Rolland Y, Bergman H, Morley JE, Kritchevsky SB, Vellas B. The I.A.N.A Task Force on frailty assessment of older people in clinical practice. J Nutr Health Aging. 2008;12(1):29–37. doi:10.1007/BF02982161
21. Qiu D, Wang X-M, Yang -J-J. Effect of Intraoperative Esketamine Infusion on Postoperative Sleep Disturbance After Gynecological Laparoscopy: a Randomized Clinical Trial. JAMA Network Open. 2022;5(12):e2244514. doi:10.1001/jamanetworkopen.2022.44514
22. Duan G, Wang K, Peng T, Wu Z, Li H. The Effects of Intraoperative Dexmedetomidine Use and Its Different Dose on Postoperative Sleep Disturbance in Patients Who Have Undergone Non-Cardiac Major Surgery: a Real-World Cohort Study. Nat Sci Sleep. 2020;12:209–219. doi:10.2147/NSS.S239706
23. Cai J, Chen Y, Hao X. Effect of Intraoperative Dexmedetomidine Dose on Postoperative First Night Sleep Quality in Elderly Surgery Patients: a Retrospective Study With Propensity Score-Matched Analysis. Front Med Lausanne. 2020;7:528. doi:10.3389/fmed.2020.00528
24. Gordon DB, Polomano RC, Pellino TA. Revised American Pain Society Patient Outcome Questionnaire (APS-POQ-R) for quality improvement of pain management in hospitalized adults: preliminary psychometric evaluation. J Pain. 2010;11(11):1172–1186. doi:10.1016/j.jpain.2010.02.012
25. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948. doi:10.7326/0003-4819-113-12-941
26. Groven RVM, Kuik C, Greven J. Fracture haematoma proteomics. Bone Joint Res. 2024;13(5):214–225. doi:10.1302/2046-3758.135.BJR-2023-0323.R1
27. Zhang X, Song W, Liu Y. Healthy Tendon Stem Cell-Derived Exosomes Promote Tendon-To-Bone Healing of Aged Chronic Rotator Cuff Tears by Breaking the Positive-Feedback Cross-Talk between Senescent Tendon Stem Cells and Macrophages through the Modulation of Macrophage Polarization. Small. 2024;20(31):e2311033. doi:10.1002/smll.202311033
28. Stegemann A, Liu S, Retana Romero OA. Prefrontal engrams of long-term fear memory perpetuate pain perception. Nat Neurosci. 2023;26(5):820–829. doi:10.1038/s41593-023-01291-x
29. Ding W, Yang L, Shi E. The endocannabinoid N-arachidonoyl dopamine is critical for hyperalgesia induced by chronic sleep disruption. Nat Commun. 2023;14(1):6696. doi:10.1038/s41467-023-42283-6
30. Chen YK, Boden KA, Schreiber KL. The role of regional anaesthesia and multimodal analgesia in the prevention of chronic postoperative pain: a narrative review. Anaesthesia. 2021;76(Suppl 1):8–17. doi:10.1111/anae.15256
31. Leemans L, Elma Ö, Nijs J. Transcutaneous electrical nerve stimulation and heat to reduce pain in a chronic low back pain population: a randomized controlled clinical trial. Braz J Phys Ther. 2021;25(1):86–96. doi:10.1016/j.bjpt.2020.04.001
32. Lovich-Sapola J, Smith CE, Brandt CP. Postoperative pain control. Surg Clin North Am. 2015;95(2):301–318. doi:10.1016/j.suc.2014.10.002
33. Ji YW, Shen Z-L, Zhang X. Plasticity in ventral pallidal cholinergic neuron-derived circuits contributes to comorbid chronic pain-like and depression-like behaviour in male mice. Nat Commun. 2023;14(1):2182. doi:10.1038/s41467-023-37968-x
34. Zhao J, Huh Y, Bortsov A, Diatchenko L, Ji -R-R. Immunotherapies in chronic pain through modulation of neuroimmune interactions. Pharmacol Ther. 2023;248:108476. doi:10.1016/j.pharmthera.2023.108476
35. Rosenstrom AHC, Konsman JP, Kosek E. Cytokines in Cerebrospinal Fluid and Chronic Pain in Humans: past, Present, and Future. Neuroimmunomodulation. 2024;31(1):157–172. doi:10.1159/000540324
36. Zhou H, Li M, Zhao R, Sun L, Yang G. A sleep-active basalocortical pathway crucial for generation and maintenance of chronic pain. Nat Neurosci. 2023;26(3):458–469. doi:10.1038/s41593-022-01250-y
37. Irwin MR, Olmstead R, Bjurstrom MF, Finan PH, Smith MT. Sleep disruption and activation of cellular inflammation mediate heightened pain sensitivity: a randomized clinical trial. Pain. 2023;164(5):1128–1137. doi:10.1097/j.pain.0000000000002811
38. O’Neill A, Lirk P. Multimodal Analgesia. Anesthesiol Clin. 2022;40(3):455–468. doi:10.1016/j.anclin.2022.04.002
39. Chuan A, Zhou JJ, Hou RM, Stevens CJ, Bogdanovych A. Virtual reality for acute and chronic pain management in adult patients: a narrative review. Anaesthesia. 2021;76(5):695–704. doi:10.1111/anae.15202
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics and Risk Factors for in-Hospital Mortality in 240 Cases of Infective Endocarditis in a Tertiary Hospital in China: A Retrospective Study
Zhang X, Jin F, Lu Y, Ni F, Xu Y, Xia W
Infection and Drug Resistance 2022, 15:3179-3189
Published Date: 18 June 2022
Risk Factors and Annual Rates of Cognitive Decline in Elderly Mild Cognitive Impairment: A Retrospective Cohort Study
Liu M, Hao Z, Chen J
Neuropsychiatric Disease and Treatment 2026, 22:600786
Published Date: 13 April 2026