Back to Journals » Journal of Pain Research » Volume 19
Risk Factors and Nomogram-Based Risk Stratification for Moderate-to-Severe Acute Postsurgical Pain After Open Lumbar Fusion: A Prospective Cohort Study
Authors Wang W, Lv J, Zhao W, Shi X, Yu D, Chen J
Received 12 December 2025
Accepted for publication 23 March 2026
Published 30 March 2026 Volume 2026:19 588610
DOI https://doi.org/10.2147/JPR.S588610
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Wanwen Wang,* Jun Lv,* Wenyan Zhao,* Xixi Shi, Donglan Yu, Jing Chen
Department of Anesthesiology, the First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, 215006, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Chen, Email [email protected]
Objective: To identify factors associated with moderate-to-severe acute postsurgical pain (APSP) during postoperative days 1– 7 (POD1– 7) after open lumbar fusion and to develop a nomogram-based prediction model for early risk stratification.
Methods: A total of 275 patients who underwent elective open lumbar fusion surgery at a tertiary hospital in Suzhou, China, from February to September 2023 were enrolled. Demographic, clinical, and psychological data were collected preoperatively. Postoperative pain intensity was assessed daily from POD1 to POD7 using the Numeric Rating Scale (NRS). Moderate-to-severe APSP was defined as any NRS score ≥ 4 during POD1– 7, a clinically meaningful threshold for analgesic intervention. Binary logistic regression was performed to identify independent predictors and construct a nomogram. Model performance was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC) and the Hosmer-Lemeshow goodness-of-fit test.
Results: Of 275 patients, 185 (67.3%) developed moderate-to-severe APSP. Five independent predictors were identified: age ≤ 50 years (OR = 3.640, P = 0.026), educational level ≤ high school (OR = 3.278, P = 0.026), no history of pain unrelated to the primary disease (OR = 2.679, P = 0.040), Pain Catastrophizing Scale score > 12 (OR = 2.054, P = 0.014), and no planned postoperative patient-controlled intravenous analgesia (PCIA) use (OR = 1.751, P = 0.044). The model showed acceptable discrimination (AUC = 0.705), with sensitivity of 64.3% and specificity of 73.3% at the optimal cutoff (0.684). The Hosmer-Lemeshow test was non-significant (P = 0.194), indicating good calibration.
Conclusion: Moderate-to-severe APSP was common after open lumbar fusion. The nomogram, based on five readily available predictors, may support early beside risk stratification and individualized analgesic and nursing management. External validation is needed before broader clinical application.
Keywords: open lumbar fusion surgery, acute postsurgical pain, risk factors, nomogram, prediction model, nursing
Introduction
The incidence of lumbar degenerative diseases is increasing annually, with a notable trend toward affecting younger populations.1,2 Lumbar fusion surgery, a primary treatment, offers significant benefits such as stabilizing the spine, relieving nerve compression, alleviating pain, and improving quality of life, leading to its widespread application in recent years. According to the latest industry data, approximately 1.215 million spinal surgeries were performed in China in 2023, with lumbar procedures being the most common, indicating a growing clinical and economic burden associated with spinal disorders.3 Despite the established efficacy of lumbar fusion, postoperative pain management remains a major challenge due to the complexity of the procedure, long operative times, large incisions, and substantial soft tissue and bone disruption.4
Acute postsurgical pain (APSP) is pain that occurs immediately after surgery and can persist for up to 7 days.5 The first postoperative week is a key clinical window for functional recovery and analgesic escalation or adjustment decisions; therefore, pain assessment during postoperative days 1–7 (POD1–POD7) is highly relevant to perioperative management. Moderate-to-severe pain is commonly assessed using the Numeric Rating Scale (NRS), and an NRS score of ≥ 4 is a commonly accepted threshold for clinically relevant pain requiring intervention. Postoperative pain after lumbar fusion is common and often substantial. A large-scale cross-sectional study in China, involving 26,193 surgical patients from 122 hospitals, reported that nearly half of the respondents experienced moderate-to-severe pain (assessed by the NRS) on the first postoperative day.6 The severity of postoperative pain varies significantly across different surgical specialties and procedures, with the incidence of moderate-to-severe APSP (NRS 4–10) reaching as high as 73% for some surgeries.6 In a retrospective analysis of 50,525 surgical patients, Gerbershagen et al found that open lumbar fusion ranked among the three most painful procedures on postoperative day 1, with particularly severe pain after fusion of more than three lumbar segments (mean NRS 6.55).7 Inadequately managed moderate-to-severe APSP may contribute to complications such as respiratory infections, psychological distress, deep vein thrombosis, and chronic pain, while also increasing healthcare costs and societal burden.6
Importantly, patients undergoing open lumbar fusion show substantial inter-individual variability in postoperative pain.8 As a result, a one-size-fits-all analgesic strategy may not achieve optimal outcomes in all patients, and more precise perioperative risk assessment is needed to support individualized analgesic management. Traditional pain risk models often rely on single-timepoint pain metrics and may not adequately capture this heterogeneity. In addition, although postoperative pain after spine surgery has been widely studied, evidence on procedure-specific prediction of APSP after open lumbar fusion remains limited. Many existing studies have focused on chronic postsurgical pain rather than clinically significant APSP during the first postoperative week, included mixed surgical populations, or failed to incorporate psychological factors that are closely related to pain outcomes (eg., pain catastrophizing). Furthermore, few studies have translated multivariable risk estimates into practical bedside tools for early perioperative risk stratification.
Postoperative pain is multifactorial and may be influenced by surgical factors, pain-related cognitions, sleep-related problems, and perioperative analgesic planning. Nomograms, based on multivariable regression analysis, provide a practical approach for integrating multiple predictors and generating individualized risk estimates.9 In this context, a nomogram may help identify high-risk patients early and support bedside risk stratification and targeted perioperative interventions, including optimized analgesic planning and enhanced postoperative nursing surveillance.
Therefore, this study aimed to identify risk factors for moderate-to-severe APSP during POD1–POD7 after open lumbar fusion and to develop a nomogram-based risk stratification model to support individualized perioperative pain management.
Participants and Methods
Study Population
A convenience sampling method was employed to recruit patients scheduled for elective open lumbar fusion surgery at a tertiary hospital in Suzhou between February and September 2023. Inclusion criteria were: ① age ≥ 18 years; ② expected postoperative hospital stay ≥ 4 days; and ③ American Society of Anesthesiologists (ASA) physical status classification I or II.10 Exclusion criteria were: ① emergency surgery; ② severe preoperative cardiac, hepatic, or renal disease; ③ inability to communicate verbally due to conditions such as aphasia, hearing impairment, or psychiatric disorders; and ④ postoperative transfer to the intensive care unit (ICU). The study was approved by the Institutional Ethics Committee of the First Affiliated Hospital of Soochow University (Institutional Review Board Approval No. 2022505). Clinical trial number: not applicable. The sample size was initially calculated using the formula N = Zα/22 × P(1−P)/δ2, with P set at 20% based on the reported incidence of moderate-to-severe APSP in a previous study.7 With α = 0.05 (Zα/2 = 1.96) and an allowable error δ = 0.05, the required sample size was 245. To support prediction-model development and account for uncertainty in the anticipated event rate, the final sample size was increased to 275. The adequacy of the events-per-variable ratio was then evaluated based on the final number of events and predictors retained in the model.
Methods
Data Collection Instruments
General Data Questionnaire: Based on a review of existing literature,11,12 a questionnaire was designed to collect demographic and disease-related data, including age, sex, body mass index (BMI), smoking history, ASA classification, educational level, number of fusion segments, history of pain unrelated to the primary disease (eg., rheumatoid arthritis, osteoarthritis, migraine, gout), operative time, intraoperative blood loss, intraoperative opioid consumption, planned use of patient-controlled intravenous analgesia (PCIA), pain catastrophizing score, and sleep quality. To standardize opioid consumption, all intraoperative intravenous opioids were converted to oral milligram morphine equivalents (OMME).13 Perioperative analgesic management followed routine clinical practice at our institution. The planned use and configuration of postoperative PCIA were determined by the attending anesthesiologist according to patient condition, clinical judgment, and patient preference, rather than a fully standardized protocol.
Numeric Rating Scale (NRS): The NRS is a widely used tool for pain assessment.14 It scores pain from 0 (no pain) to 10 (worst imaginable pain). Scores of 1–3 represent mild pain, 4–6 moderate pain, and 7–10 severe pain.14 Pain intensity was assessed daily from postoperative day 1 to postoperative day 7 (POD1–POD7). For each postoperative day, the pain score entered into the analysis was the highest NRS score reported by the patient during the preceding 24 hours, regardless of whether it occurred at rest or during movement. Patients with any NRS score of ≥ 4 during POD1–POD7 were assigned to the moderate-to-severe APSP group, while those with all NRS scores < 4 were assigned to the non-moderate-to-severe APSP group.
Pittsburgh Sleep Quality Index (PSQI): Developed by Buysse et al in 1989, the PSQI assesses subjective sleep quality.15 It consists of 18 self-rated items grouped into 7 components, each scored from 0 to 3. The total score ranges from 0 to 21, with higher scores indicating poorer sleep quality. A score > 7 was used to define the presence of a sleep disorder.16 The Chinese version of the PSQI has demonstrated good reliability and validity, with a Cronbach’s α of 0.852 and a test-retest reliability of 0.904.16 In this study, the Cronbach’s α was 0.806.
Pain Catastrophizing Scale (PCS): Developed by Sullivan et al,17 the PCS measures the tendency of individuals with chronic pain to view pain as a catastrophe and adopt passive coping strategies. This study used the Chinese version validated by Yap et al18 in 2008. The scale includes 13 items across three dimensions: rumination, magnification, and helplessness. Each item is rated on a 5-point Likert scale from 0 (not at all) to 4 (all the time), with a total score ranging from 0 to 52. Higher scores indicate greater pain catastrophizing. The scale has shown good psychometric properties, with an overall Cronbach’s α of 0.927.18 In the current study, the overall Cronbach’s α was 0.903. As there is no universally accepted cutoff for the PCS, and scores in our sample were generally lower than those reported in Western spinal surgery populations, we adopted a cutoff of > 12. This lower threshold was chosen to better reflect the psychological risk profile of our study population and facilitate the early identification of potentially high-risk individuals.
Data Collection Procedure
After obtaining informed consent, a researcher collected the data. Demographic information, PCS scores, and PSQI scores were collected via face-to-face interviews one day before surgery. Disease- and treatment-related data were retrieved from the hospital information system. Postoperatively, the researcher assessed pain daily using the NRS for 7 days via face-to-face interviews around 10:00 am. Patients discharged within 7 days were followed up by telephone.
Statistical Analysis
Data were double-entered into Epidata 3.0 and verified for accuracy. There were no missing data for the outcome or predictor variables included in the final analysis; therefore, no imputation was performed. Statistical analysis was performed using SPSS 26.0. The Shapiro–Wilk test and Q-Q plots were used to assess the normality of continuous variables. Normally distributed data were described as mean ± standard deviation (SD), while non-normally distributed data were described as median and interquartile range (IQR; P25, P75). Categorical data were presented as frequencies and percentages (%) and compared between groups using the chi-square test or Fisher’s exact test. Variables from the univariate analysis with a P-value < 0.2 were included in a binary logistic regression analysis to identify independent predictors.19 A nomogram model was constructed using the rms package in R 4.3.1. The model’s discrimination was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC), while its calibration was assessed with the Hosmer-Lemeshow goodness-of-fit test. The model’s sensitivity and specificity were also calculated.20,21 A two-sided P-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics of Participants
Of the 314 patients initially recruited, 19 had their surgery canceled, 18 had a change in surgical procedure, and 2 were transferred to the ICU postoperatively. A final sample of 275 patients was included in the analysis. Within 7 days post-surgery, 185 patients (67.3%) developed moderate-to-severe APSP. The baseline and clinical characteristics are detailed in Table 1.
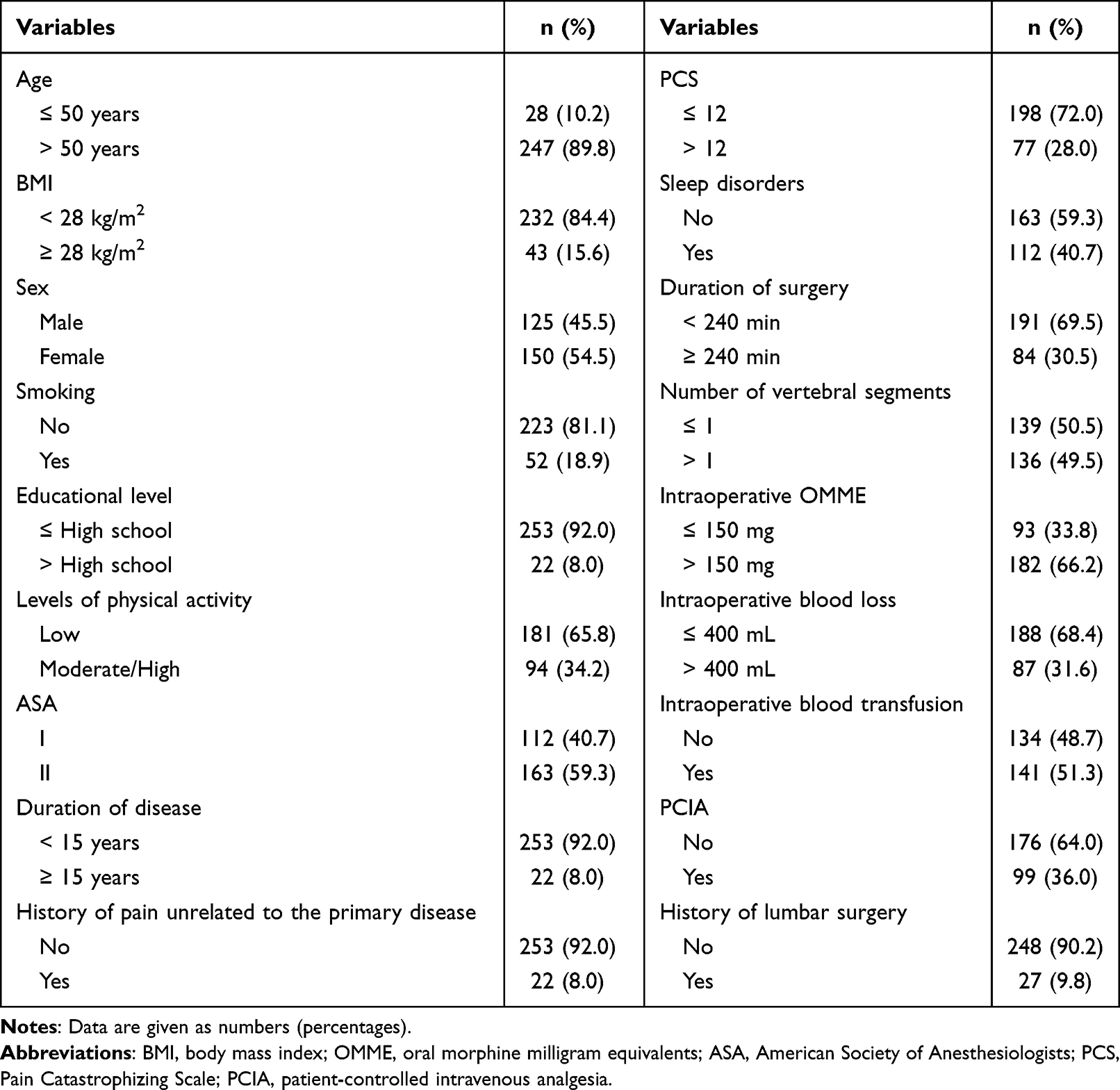 |
Table 1 Baseline and Clinical Characteristics of the Subjects (n = 275) |
Univariate Analysis of Moderate-to-Severe APSP
Patients were divided into a moderate-to-severe APSP group (n = 185) and a non-moderate-to-severe APSP group (n = 90). A comparison of demographic, clinical, and psychological variables revealed that preoperative PCS score (P = 0.006) and planned use of PCIA (P = 0.010) were significantly different between the two groups (P < 0.05), as shown in Table 2.
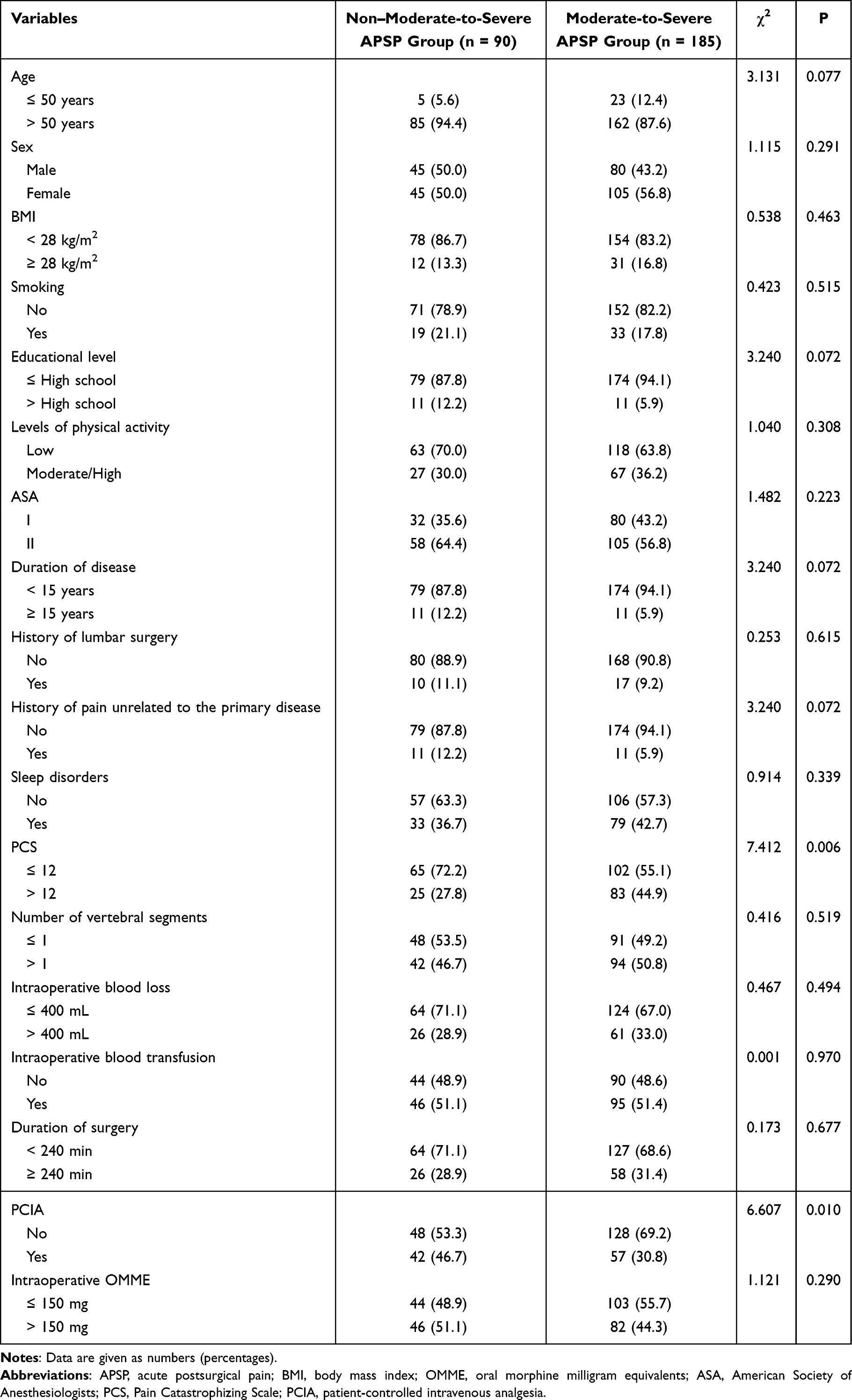 |
Table 2 Univariate Analysis of Moderate-to-Severe Acute Postsurgical Pain in Patients Undergoing Open Lumbar Fusion |
Multivariate Logistic Regression Analysis
To identify independent predictors, a binary logistic regression model was developed. The dependent variable was the occurrence of moderate-to-severe APSP (0 = No, 1 = Yes). Independent variables included those with P < 0.2 in the univariate analysis (age, educational level, history of pain unrelated to the primary disease, pain catastrophizing, disease duration, and PCIA) and gender (a known potential factor from the literature).6 The results showed that lower age (≤ 50 years), lower educational level, no planned use of PCIA, higher pain catastrophizing, and no history of pain unrelated to the primary disease were independent predictors for moderate-to-severe APSP (P < 0.05), as detailed in Table 3.
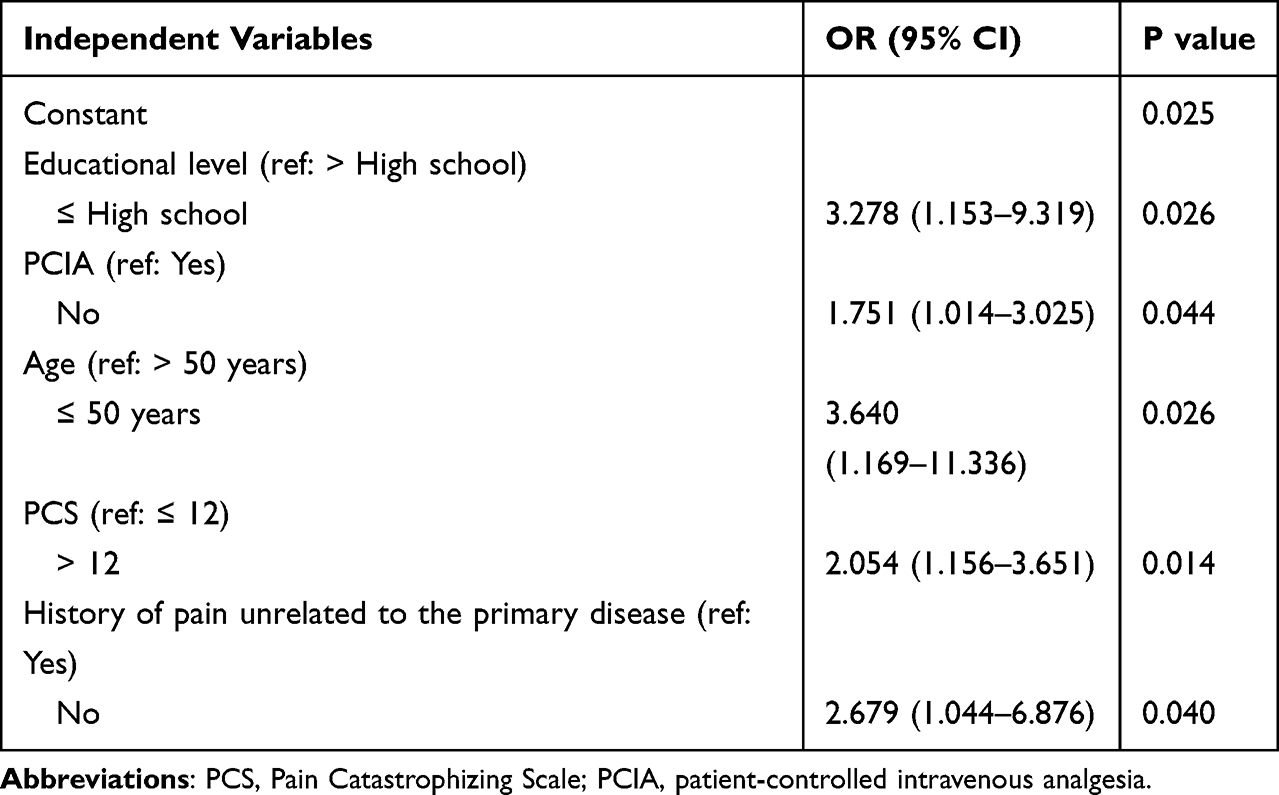 |
Table 3 Logistic Regression Analysis of Risk Factors for Moderate-to-Severe Acute Postsurgical Pain in Patients Undergoing Open Lumbar Fusion |
Development of the Risk Prediction Model
Based on the five independent risk factors (age, educational level, PCIA use, pain catastrophizing, and history of pain unrelated to the primary disease), a risk prediction model for moderate-to-severe APSP was constructed:
P = 1 / (1 + e−ʸ)
where Y = −2.204 + 1.292 × (Age ≤ 50) + 1.187 × (Low Education) + 0.985 × (No History of Pain Unrelated to the Primary Disease) + 0.720 × (High PCS) + 0.560 × (No PCIA).
A nomogram was developed based on this model (Figure 1).
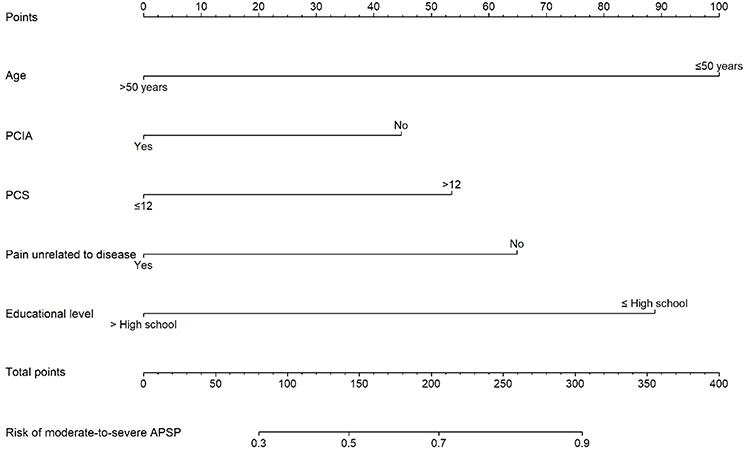 |
Figure 1 Nomogram for predicting the risk of moderate-to-severe acute postsurgical pain after open lumbar fusion. |
Evaluation of the Prediction Model
The ROC curve analysis yielded an AUC of 0.705 (95% CI: 0.638–0.771, P < 0.001), indicating acceptable discrimination of the prediction model. At the optimal cutoff value of 0.684, the Youden index was 0.377, with a sensitivity of 64.3% and a specificity of 73.3%. The Hosmer-Lemeshow test yielded a chi-square value of 9.898 (P = 0.194), suggesting good agreement between predicted and observed probabilities. Internal validation using 1000 bootstrap resamples produced a bias-corrected calibration curve that closely aligned with the ideal diagonal line, supporting the model’s calibration and robustness (Figure 2). Decision curve analysis further showed a net clinical benefit over the “treat all” and “treat none” strategies across threshold probabilities of approximately 0.40 to 0.70 (Figure 3), suggesting potential utility of the model for risk-informed perioperative pain management.
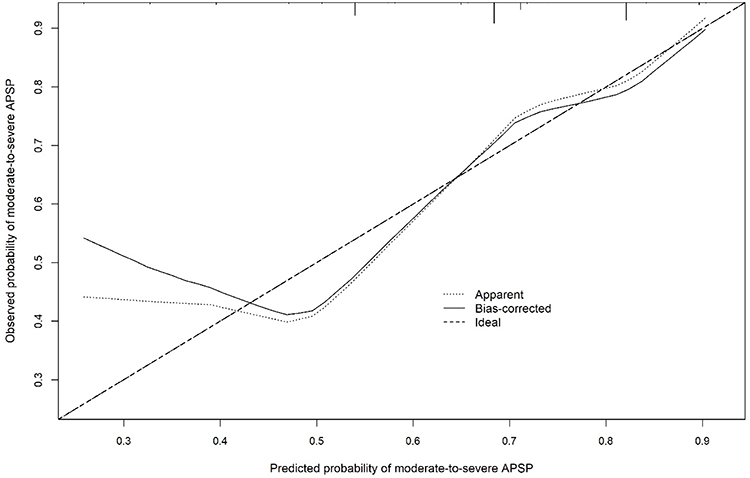 |
Figure 2 Calibration curve of the nomogram for predicting moderate-to-severe acute postsurgical pain after open lumbar fusion. |
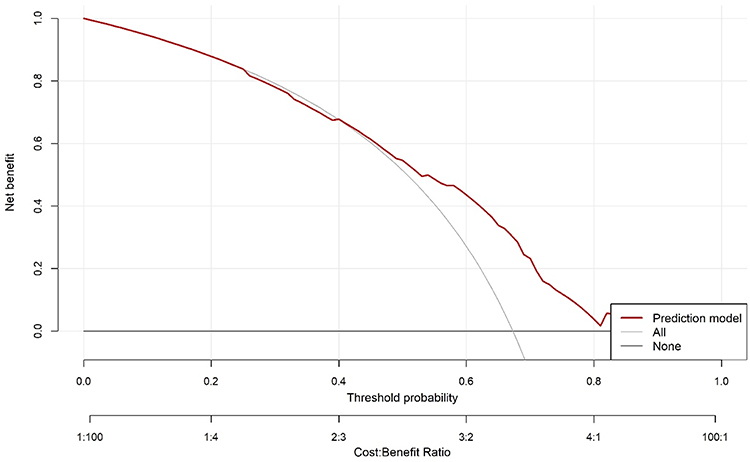 |
Figure 3 Decision curve analysis of the nomogram for predicting moderate-to-severe acute postsurgical pain after open lumbar fusion. |
Discussion
In this single-center cohort of patients undergoing open lumbar fusion, 67.3% developed moderate-to-severe APSP within the first postoperative week, confirming that APSP remains a frequent and clinically relevant problem after this highly invasive spinal procedure. This incidence is comparable to that reported in previous large-scale Chinese studies (63.3%),6 further underscoring the substantial unmet need for improved perioperative pain management in this population.
In the present study, we developed a multivariable risk prediction model incorporating five readily obtainable preoperative or perioperative factors—age, educational level, pain catastrophizing, history of pain unrelated to the primary disease, and planned use of PCIA—to estimate the probability of moderate-to-severe APSP. The model demonstrated acceptable discrimination (AUC = 0.705) and good calibration, supporting its potential utility for early perioperative risk stratification. Importantly, all predictors included in the nomogram can be assessed before or immediately after surgical planning, enhancing its feasibility for routine clinical application.
Unlike previous studies that primarily focused on chronic postsurgical pain, this work emphasizes early acute pain risk following open lumbar fusion, a procedure consistently ranked among the most painful surgical interventions. Early identification of patients at high risk of APSP may facilitate timely implementation of targeted analgesic and nursing interventions, potentially improving postoperative recovery trajectories.
Predictive Performance of the Model
The nomogram-based prediction model achieved an AUC of 0.705, indicating acceptable but modest discrimination. Although this level of performance is insufficient for precise individual-level prediction, it remains clinically useful for early risk stratification in the context of postoperative pain, which is inherently multifactorial and influenced by biological, psychological, and perioperative management factors. Accordingly, the nomogram should be interpreted as a pragmatic bedside risk stratification tool to support perioperative decision-making, rather than a deterministic predictor. The endpoint definition used in this study (any NRS score ≥ 4 during POD1–POD7) was intended to identify patients with clinically relevant pain requiring analgesic attention during the first postoperative week, a key period for recovery and perioperative pain management.
The level of discrimination is broadly comparable to that reported in other perioperative pain prediction studies.22,23 However, direct comparison should be interpreted cautiously because study populations, pain definitions, assessment windows, and modeling methods differ across studies. In addition, procedure-specific APSP prediction models for open lumbar fusion remain limited. Therefore, our nomogram is best interpreted as a practical tool for early risk stratification in this surgical population.
In addition, the model demonstrated good calibration and favorable decision-curve performance, suggesting that it may provide useful risk estimates to support perioperative decision-making. In practice, the nomogram may help identify patients at elevated risk of moderate-to-severe APSP who may benefit from intensified multimodal analgesic planning, enhanced patient education, and closer postoperative nursing surveillance.
Analysis of Risk Factors for Moderate-to-Severe APSP
Age
Patients aged ≤ 50 years had a higher risk of developing moderate-to-severe APSP. Being older (> 50 years) acted as a protective factor. This may be related to age-associated decreases in pain sensitivity, reduced natural killer cell counts, a blunted inflammatory response, and declines in neurotransmitter levels and nerve conduction velocity.24 A study by Gerbershagen et al25 found that postoperative pain intensity decreases with age, with a reduction of 0.28 points on the pain scale for every 10-year increase in age, supporting our finding that older age is associated with a lower probability of APSP.
Educational Level
Patients with a lower educational level were at higher risk for moderate-to-severe APSP. This aligns with a study by Ye et al12 on patients undergoing hysterectomy, which found a similar association. The disparity may stem from differences in health literacy and the ability to access and understand information about pain and analgesia. Patients with higher education may be more proactive in seeking knowledge, which helps them develop realistic expectations and communicate their pain effectively. In contrast, those with lower education may have limited access to such information. Therefore, providing individualized perioperative assessment and health education to this group is crucial to improve their pain-related knowledge and encourage active pain reporting.
Pain Catastrophizing
A higher level of preoperative pain catastrophizing was associated with an increased risk of moderate-to-severe APSP. Patients with lumbar degenerative diseases often experience long-term pain and functional limitations, which can lead to preoperative fear, anxiety, helplessness, and heightened concerns about the surgery, all of which contribute to catastrophizing. This cognitive style can trigger a fear-avoidance cycle, promote sympathetic nervous system activation and inflammation, and thereby intensify APSP, which in turn can reinforce catastrophic thinking. Previous research has confirmed that preoperative pain catastrophizing is a significant predictor of postoperative pain intensity and analgesic consumption,26 consistent with our results. Therefore, preoperative psychological screening and timely intervention are necessary to improve patients’ mental state and potentially reduce the incidence of APSP.
History of Pain Unrelated to the Primary Disease
A noteworthy and somewhat counterintuitive finding of this study is that patients without a history of pain unrelated to their primary condition (eg., rheumatoid arthritis, migraines) were at a higher risk of moderate-to-severe APSP. While central sensitization theory suggests that chronic pain could increase postoperative pain sensitivity, it is possible that individuals with a history of chronic pain develop stronger pain adaptation mechanisms, have more realistic expectations about postoperative pain, and experience lower preoperative anxiety. These factors could lead to lower subjective pain ratings and thus a reduced incidence of moderate-to-severe APSP.
PCIA Use
Patients who were not scheduled to use PCIA had a higher risk of developing moderate-to-severe APSP. PCIA delivers a continuous infusion of analgesics via a programmable micropump, which can be used for 48–72 hours postoperatively.27 One study found that the use of PCIA in total knee arthroplasty patients reduced the risk of APSP by 33%.11 This underscores the importance of strengthening perioperative analgesic education, ensuring patients fully understand the benefits of PCIA for pain management, and encouraging its use to alleviate discomfort and promote recovery.27
However, the association between planned PCIA use and APSP should be interpreted cautiously. In our setting, the decision to use PCIA (and its configuration) was made according to routine clinical practice based on anesthesiologist judgment, the patient’s clinical condition, and the patient’s preference, rather than a fully standardized protocol. Therefore, planned PCIA use may reflect clinical context as well as analgesic strategy. Nevertheless, planned PCIA use remains a clinically meaningful perioperative factor and may be useful for early risk stratification and analgesic planning.
For bedside usability, several predictors were dichotomized using clinically interpretable thresholds (eg., age and PCS score), although this may have reduced predictive information to some extent.
Strengths and Limitations
This study has several strengths. First, it focused on open lumbar fusion, a procedure associated with substantial pain and challenging management, and developed a procedure-specific prediction model. Second, the model incorporates multidimensional predictors, including demographic, clinical, and psychological factors, and all predictors were readily available during perioperative care, supporting bedside feasibility. Third, by focusing on APSP rather than chronic pain, this study provides a practical tool for early risk stratification and individualized perioperative pain management.
The study also has limitations. It was a single-center study and lacked external validation, which may limit generalizability. In addition, postoperative analgesic regimens (including PCIA use and configuration) were not fully standardized, and pain was assessed once daily using the highest NRS score reported over the preceding 24 hours; these factors may have introduced practice-related and measurement variability, although they reflect real-world clinical care. The endpoint definition used in this study may not distinguish transient early pain from more persistent moderate-to-severe pain trajectories. In addition, the PCS cutoff used in this study (> 12 points) is not a universally standardized threshold, which may limit comparability with other studies. Finally, dichotomization of some predictors and possible misclassification of history-based variables may have reduced predictive precision. Future multicenter studies with external validation and alternative endpoint definitions are warranted.
Conclusion
Moderate-to-severe APSP was common during the first postoperative week after open lumbar fusion. A nomogram based on five readily available perioperative factors (age, educational level, pain catastrophizing, history of pain unrelated to the primary disease, and planned PCIA use) may support early risk stratification and individualized perioperative analgesic and nursing management. However, this model should be interpreted as a pragmatic risk estimation tool rather than a deterministic predictor at the individual level. Given the single-center design and lack of external validation, further multicenter studies are needed to validate the model and to explore whether alternative outcome definitions or pain trajectory-based approaches improve predictive performance and clinical applicability.
Abbreviations
95% CI, 95% confidence interval; APSP, Acute postsurgical pain; BMI, Body mass index; ICU, Intensive care unit; IQR, Interquartile ranges; NRS, Numeric Rating Scale; OR, Odds ratio; OMME, Oral morphine milligram equivalents; PCIA, Patient-controlled intravenous analgesia; PSQI, Pittsburgh Sleep Quality Index; PCS, Pain Catastrophizing Scale; SD, Standard deviation.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Ethics Committee of the First Affiliated Hospital of Soochow University (Approval No. 2022505). All participants provided written informed consent prior to study enrollment. The research was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
We thank all participants for their time and contribution to the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive any funding.
Disclosure
The authors declare no competing interests in this work.
References
1. Fang EF, Xie C, Schenkel JA, et al. A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. 2020;64(101174). doi:10.1016/j.arr.2020.101174
2. Zhang YG, Sun Z, Zhang Z, et al. Risk factors for lumbar intervertebral disc herniation in Chinese population: a case-control study. Spine. 2009;34(25):E918–12. doi:10.1097/BRS.0b013e3181a3c2de
3. Gonyn Industry Research. Industry analysis report on spinal surgery volume in China 2023.
4. Waelkens P, Alsabbagh E, Sauter A, et al. Pain management after complex spine surgery: a systematic review and procedure-specific postoperative pain management recommendations. Eur J Anaesthesiol. 2021;38(9):985–994. doi:10.1097/EJA.0000000000001448
5. Chinese Society of Anesthesiology. Expert consensus on postoperative pain management in adults. J Clin Anesthesiol. 2017;33(9):911–917.
6. Liu Y, Xiao S, Yang H, et al. Postoperative pain-related outcomes and perioperative pain management in China: a population-based study. Lancet Reg Health West Pac. 2023;39(100822).
7. Gerbershagen HJ, Aduckathil S, van Wijck AJ, et al. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118(4):934–944. doi:10.1097/ALN.0b013e31828866b3
8. Chen J, Shi XX, Deng SY, et al. Acute pain trajectory and influencing factors in patients after lumbar fusion surgery. J Nurs Sci. 2024;39(12):10–14,19.
9. Lv J, Liu YY, Jia YT, et al. A nomogram model for predicting prognosis of obstructive colorectal cancer. World J Surg Oncol. 2021;19(1):337. doi:10.1186/s12957-021-02445-6
10. De Cassai A, Boscolo A, Tonetti T, et al. Assignment of ASA-physical status relates to anesthesiologists’ experience: a survey-based national-study. Korean J Anesthesiol. 2019;72(1):53–59. doi:10.4097/kja.d.18.00224
11. Kong WW. Study on Influencing Factors of Acute Pain After Total Knee Arthroplasty. Lanzhou: Lanzhou University; 2019.
12. Ye XX, Liu ZJ, Wang Y, et al. Predictors of acute postoperative pain and pain relief after hysterectomy. Chin J Pain Med. 2017;23(10):748–753.
13. UCSF Pain Management Education. Calculation of oral morphine equivalents (OME).
14. Eriksson K, Wikström L, Årestedt K, et al. Numeric rating scale: patients’ perceptions of its use in postoperative pain assessments. Appl Nurs Res. 2014;27(1):41–46. doi:10.1016/j.apnr.2013.10.006
15. Buysse DJ, Reynolds CF, Monk TH, et al. The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
16. Liu XC, Tang MQ, Hu L, et al. Reliability and validity of the Pittsburgh Sleep Quality Index. Chin J Psychiatry. 1996;29(2):103–107.
17. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
18. Yap JC, Lau J, Chen PP, et al. Validation of the Chinese pain catastrophizing scale (HK-PCS) in patients with chronic pain. Pain Med. 2008;9(2):186–195. doi:10.1111/j.1526-4637.2007.00307.x
19. Chen H, Li DG. Medical Statistical Methods and SPSS Implementation. Beijing: Science Press; 2016.
20. Zheng LQ, Zhang R. Research progress on goodness-of-fit evaluation methods for disease risk prediction models. Chin J Health Stat. 2015;32(3):544–546.
21. Paul P, Pennell ML, Lemeshow S. Standardizing the power of the Hosmer–Lemeshow goodness of fit test in large data sets. Stat Med. 2013;32(1):67–80. doi:10.1002/sim.5525
22. Papadomanolakis-Pakis N, Haroutounian S, Sørensen JK, et al. Predicting acute postsurgical pain in the postanesthesia care unit: risk tool development and internal validation. Pain Rep. 2025;10(5):e1329. doi:10.1097/PR9.0000000000001329
23. Shi G, Liu G, Gao Q, et al. A random forest algorithm-based prediction model for moderate to severe acute postoperative pain after orthopedic surgery under general anesthesia. BMC Anesthesiology. 2023;23(1):361. doi:10.1186/s12871-023-02328-1
24. Gagliese L. Pain and aging: the emergence of a new subfield of pain research. J Pain. 2009;10(4):343–353. doi:10.1016/j.jpain.2008.10.013
25. Gerbershagen HJ, Pogatzki-Zahn E, Aduckathil S, et al. Procedure-specific risk factor analysis for the development of severe postoperative pain. Anesthesiology. 2014;120(5):1237–1245. doi:10.1097/ALN.0000000000000108
26. Dunn LK, Durieux ME, Fernández LG, et al. Influence of catastrophizing, anxiety, and depression on in-hospital opioid consumption, pain, and quality of recovery after adult spine surgery. J Neurosurg Spine. 2018;28(1):119–126. doi:10.3171/2017.5.SPINE1734
27. Zhang JF, Cai YY, Zheng KX, et al. A systematic review of guidelines related to patient-controlled analgesia management for postoperative acute pain. Chin J Nurs. 2021;56(12):1868–1875.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Influencing Delayed Onset of Lactogenesis: A Scoping Review
Li S, Wupuer T, Hou R
International Journal of General Medicine 2024, 17:2311-2326
Published Date: 21 May 2024
Construction of a Nomogram Prediction Model for Individualized Prediction of Cervical Cancer Risk: A Retrospective Study
Zhou W, Wang Y, Long H, Wang J
International Journal of Women's Health 2025, 17:4435-4446
Published Date: 13 November 2025
Development of a Risk Prediction Model for Preoperative Pre-Frailty in Elderly Patients with Gastric Cancer
Yin C, Yin M, Zhen J, Xue C, Zhu Z
Clinical Interventions in Aging 2025, 20:2763-2772
Published Date: 28 December 2025
Influencing Factors of New-Onset Atrial Fibrillation in Sepsis Patients and Construction of a Nomogram Prediction Model: Based on LASSO Regression
Tang J, Ou W, Han B, Wen W
International Journal of General Medicine 2026, 19:565434
Published Date: 22 January 2026
Mediating Role of Dyadic Coping Between Social Support and Oral Frailty Cross-Sectional Study of Elderly Ovarian Cancer Patients in China
Jin J, Zhao D, Chen Y
International Journal of Women's Health 2026, 18:594341
Published Date: 23 April 2026