Back to Journals » Clinical Interventions in Aging » Volume 20
Development of a Risk Prediction Model for Preoperative Pre-Frailty in Elderly Patients with Gastric Cancer
Authors Yin C, Yin M, Zhen J, Xue C, Zhu Z ![]()
Received 25 September 2025
Accepted for publication 23 December 2025
Published 28 December 2025 Volume 2025:20 Pages 2763—2772
DOI https://doi.org/10.2147/CIA.S568685
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Changxin Yin,1 Meng Yin,2 Jiang Zhen,3 Chi Xue,4 Zhi Zhu4
1The Operating Room, The First Affiliated Hospital of China Medical University, Shenyang, 110001, People’s Republic of China; 2Department of Laboratory Sciences, Shengjing Hospital of China Medical University, Shenyang, 110001, People’s Republic of China; 3Department of Cardiovascular Medicine, The Fourth People’s Hospital of Shenyang, Shenyang, 110001, People’s Republic of China; 4Depatmemt of Surgical Oncology, The First Affiliated Hospital of China Medical University, Shenyang, 110001, People’s Republic of China
Correspondence: Zhi Zhu, Department of Surgical Oncology, The First Affiliated Hospital of China Medical University, Shenyang, 110001, People’s Republic of China, Email [email protected]
Objective: Complications from surgery as well as the side effects of postoperative chemotherapy, can lead to a decline in the treatment effect of elderly cancer patients, which is closely related to pre-frailty. This study aimed to analyze the prevalence and influencing factors of preoperative pre-frailty in elderly patients with gastric cancer, explore its predictive value, and construct a risk prediction model.
Methods: 317 elderly gastric cancer patients was recruited from the 1st Hospital of China Medical University between September 1, 2022, to December 18, 2024. Fried Frailty Phenotype, Health Literacy Scale for Chronic Patients, and Quality of Life Instruments for Gastric Cancer Patients. Logistic regression analysis was employed to identify the influencing factors of pre-frailty. ROC curve was used to evaluate the predictive value of the identified factors, and RStudio software was utilized to construct a Nomogram-based risk prediction model.
Results: Among the 317 included patients, 177 (53.4%) were pre-frail. Binary Logistic regression identified age, comorbidity, hemoglobin concentration, malnutrition risk, depression status, and GI symptoms as independent influencing factors (all P< 0.05). ROC curve analysis showed that the area under the curve (AUC) was 0.986 [95% CI (0.972, 0.999)]with an optimal cutoff value of 0.452, corresponding to a sensitivity of 0.889 and a specificity of 0.945.
Conclusion: The prevalence of preoperative pre-frailty is high in elderly patients with gastric cancer. Clinicians should pay attention to elderly, patients with combidity, low hemoglobin, malnutrition risk, poor mental healthy, and obvious gastric cancer-specific symptoms. The constructed risk prediction model demonstrates good predictive accuracy and discriminative ability.
Keywords: elderly, gastric cancer, laparoscopic surgery, risk prediction, nomogram, nursing
Instruction
Gastric cancer constitutes a major global health challenge, ranking among the top five most prevalent cancers worldwide with a high mortality rate. Its incidence is particularly elevated in regions such as East Asia, Eastern Europe, and parts of South America. Notably, China accounts for nearly 40% of global gastric cancer cases, with over 350,000 new cases and more than 260,000 deaths reported annually.1 In recent years, the incidence and mortality of gastric cancer have continued to rise, posing a major threat to public life health and quality of life.
Currently, surgical interventions such as laparoscopic or robotic radical gastrectomy are commonly used for gastric cancer treatment. Through the Enhanced Recovery after Surgery (ERAS) management pathway, most patients can achieve early discharge.2 However, not all patients are suitable for ERAS management, especially the elderly.3 How to determine the weak state of the elderly in advance and carry out nursing and nutritional intervention can effectively avoid postoperative complications, complications from surgery as well as the side effects of postoperative surgery, can lead to a decline in the treatment effect of elderly cancer patients, which is closely related to pre-frailty.4
Pre-frailty is considered a reversible physical condition. Understanding the characteristics of patients in pre-frailty is crucial for addressing frailty issues.5 Implementing scientific and effective medical and nursing interventions can delay or prevent patients from transitioning from a non-frail state to pre-frailty, or even reverse from pre-frailty back to non-frailty, thereby improving patient health outcomes. Current research on pre-frailty in patients often focuses on preventing its progression to frailty,6,7 while studies on early interventions to prevent or delay non-frail patients from developing pre-frailty remain limited. This study targeted preoperative non-frail and pre-frail elderly patients with gastric cancer, investigating the prevalence of pre-frailty and its influencing factors to establish a prediction model. The goal is to provide a reference for clinical healthcare providers to implement effective measures for preventing these patients from entering the pre-frailty stage.
Materials and Methods
Inclusion and Exclusion Criteria
A convenience sampling method was used to select 317 elderly patients with gastric cancer who underwent laparoscopic distal subtotal gastrectomy or total gastrectomy at the First Hospital of China Medical University between September 1, 2022, and December 18, 2024.
Inclusion Criteria
1) Age ≥ 60 years; 2) Pathologically or cytologically diagnosed with gastric cancer; 3) Non-frail or in pre-frailty, ie, meeting ≤ 2 criteria on the Fried Frailty Phenotype assessment; 4) Have a clear understanding of the treatment plan and can actively cooperate with questionnaire surveys; 5) Clear consciousness and able to communicate well; 6) Voluntarily participate in the study and sign the informed consent form.
Exclusion Criteria
1) Suffering from severe physical or mental illness or having serious complications; 2) Have received radiotherapy or prior surgical treatment for gastric cancer; 3) Be in the acute phase of the disease or the palliative care stage after disease progression.
Sample Size Calculation
The events per variable (EPV) method was adopted. This study included 30 independent variables, and with a requirement of EPV ≥5, the minimum effective sample size was calculated to be ≥150 cases. Pre-test data (50 cases) showed that the prevalence of pre-frailty in elderly patients with gastric cancer was 66%. Based on this, the required sample size was calculated to be 278 cases. Considering a 10% follow-up loss rate, the final minimum sample size was determined to be 305 cases.
General Demographic and Clinical Data Questionnaire
Developed through literature review and team discussions, the questionnaire included variables such as age, gender, body mass index (BMI), occupation, education level, tumor location, tumor stage, histological type, comorbidities (hypertension, diabetes, cerebral infarction, coronary heart disease), malnutrition risk, depression status, neuropsychiatric symptoms, and GI symptoms. Anxiety Level and depression status adopted in this study are HADS (Hospital Anxiety and Depression Scale) A and D, GI symptoms used MDASI (Memorial Symptom Assessment Scale).
Pre-Frailty Phenotype
Developed by Fried et al,8 this scale assesses frailty based on five indicators: unexplained weight loss, self-reported fatigue, decreased grip strength, reduced walking speed, and diminished physical activity. Each indicator is scored as 0 (negative) or 1 (positive). A total score of ≥3 indicates frailty, 1–2 indicates pre-frailty, and 0 indicates a non-frail (healthy) state.
Health Literacy Scale for Chronic Disease Patients
The Health Literacy Scale for Chronic Disease Patients used in this study was compiled by Chinese scholars, which is suitable for assessing the health literacy level of Chinese chronic disease patients. The scale includes 3 dimensions (basic health knowledge and skills, health information comprehension, and health behavior practice) and a total of 22 items. Each item is scored on a 5-point Likert scale (1 = completely inconsistent to 5 = completely consistent), with a total score ranging from 22 to 110. A higher score indicates a higher level of health literacy. The Cronbach’s α coefficient of this scale is 0.82, and the split-half reliability is 0.79, showing good reliability and validity.
Quality of Life Scale for Gastric Cancer Patients
The Quality of Life Scale for Gastric Cancer Patients adopted in this study is the Chinese version of the Functional Assessment of Cancer Therapy-Gastric (FACT-Ga) scale. The scale consists of 4 general dimensions (physical well-being, social/family well-being, emotional well-being, and functional well-being) and 1 gastric cancer-specific dimension, with a total of 44 items. Each item is scored from 0 to 4, and the total score is calculated by summing the scores of all items, ranging from 0 to 176. A higher total score represents a better quality of life. The Cronbach’s α coefficient of the Chinese version of the FACT-Ga scale is 0.86, and the test-retest reliability is 0.83, indicating good reliability and validity.
Data Collection and Quality Control
Before data collection, the researchers were uniformly trained to master the use of various scales and the standard of data collection. During the data collection process, the researchers explained the purpose, content, and significance of the study to the patients in detail, and distributed the questionnaires after obtaining the patients’ informed consent. For patients who had difficulty filling out the questionnaires independently due to vision or reading ability, the researchers read the questions to the patients and recorded the answers according to the patients’ true expressions. The questionnaires were collected on the spot after filling out, and the completeness and validity of the questionnaires were checked. A total of 317 questionnaires were distributed in this study, and 304 valid questionnaires were recovered, with an effective recovery rate of 96.1%. During data collection, 8 cases (2.5%) had missing values for hemoglobin concentration and GI symptom scores. Missing data were handled using multiple imputation (5 imputed datasets) to minimize bias, as this method is robust for continuous and categorical variables in logistic regression models.
Statistical Methods
All data were analyzed using SPSS 26.0 statistical software and RStudio 4.2.0 software. Measurement data that conformed to the normal distribution were expressed as mean ± standard deviation (x ± s), and comparison between groups was performed using the t-test; measurement data that did not conform to the normal distribution were expressed as median (interquartile range) [M (Q1, Q3)], and comparison between groups was performed using the Mann–Whitney U-test. Count data were expressed as frequency (percentage) [n (%)], and comparison between groups was performed using the χ2-test.
Univariate Logistic regression analysis was used to screen the factors possibly related to pre-frailty (P<0.20 was set as the inclusion criterion). Then, the factors screened by univariate analysis were included in the binary Logistic regression analysis to determine the independent influencing factors of pre-frailty (P<0.05 was set as the statistical significance level). Before conducting multivariate logistic regression, we assessed multicollinearity among independent variables using variance inflation factors (VIF). All VIF values were <3 (range: 1.02–2.45), indicating no significant multicollinearity that would affect model stability”.
The ROC curve was drawn to evaluate the predictive value of the independent influencing factors and the constructed model for pre-frailty. The AUC was calculated, and the optimal cut-off value was determined according to the Youden index (sensitivity + specificity - 1).
The nomogram prediction model was constructed using the rms package in RStudio software. To evaluate the model’s performance, internal validation was conducted using the bootstrap method, and the C-index was calculated to assess the discriminative ability of the model. In addition, the calibration curve was drawn to evaluate the consistency between the predicted probability of the model and the actual occurrence probability of pre-frailty. It should be noted that the extremely high AUC value (0.986) obtained in this study may suggest the possibility of model overfitting, and further external validation is needed to confirm the model’s generalizability.
Results
General Characteristics and Frailty Prevalence
Among the 317 patients, 170 (53.6%) were male and 147 (46.4%) were female; the mean age was 67.14±4.37 years. A total of 177 patients (55.8%) were pre-frail, and 140 patients (44.2%) were non-frail. Univariate analysis showed that age, neoadjuvant chemotherapy, multimorbidity, disease duration, hemoglobin level, C-reactive protein (CRP) level, malnutrition risk, anxiety level, depression status, and GI symptoms were significantly associated with the prevalence of pre-frailty (all P<0.05) (Table 1).
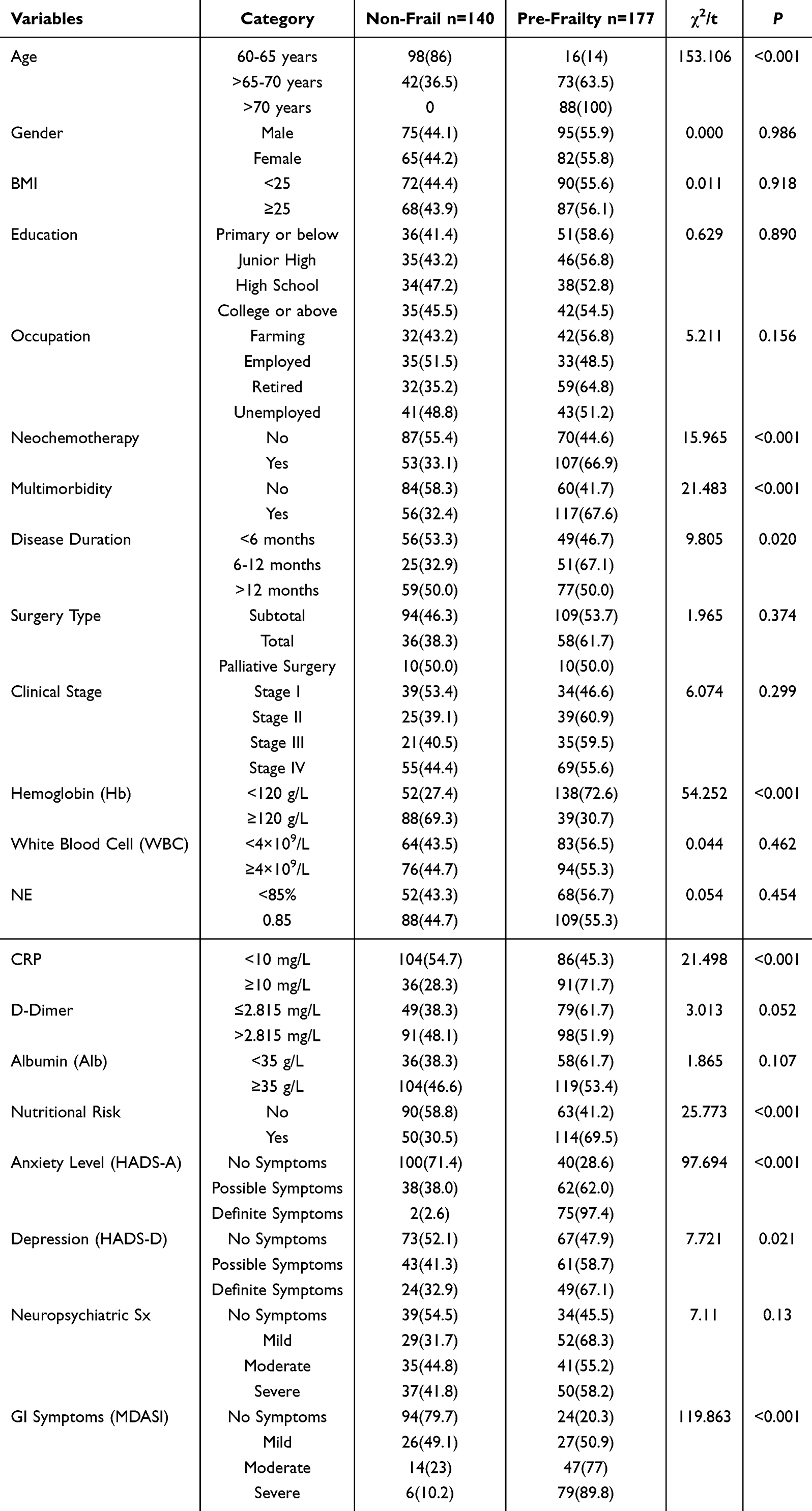 |
Table 1 Univariate Analysis of Risk Factors Associated with Pre-Frailty in Patients with Gastric Cancer |
Multivariate Analysis of Influencing Factors of Pre-Frailty
Pre-frailty status was set as the dependent variable (non-frail=0, pre-frailty=1). Variables with statistically significant differences in univariate analysis were included in the Binary Logistic regression model (entry criterion: P<0.05; removal criterion: P>0.10). The results indicated that age, comorbidity, hemoglobin concentration, malnutrition risk, depression status, and GI symptoms were independent influencing factors of preoperative pre-frailty in elderly patients with gastric cancer (all P<0.05). The variable assignment is shown in Table 2, and the results of the multivariate analysis are presented in Table 3.
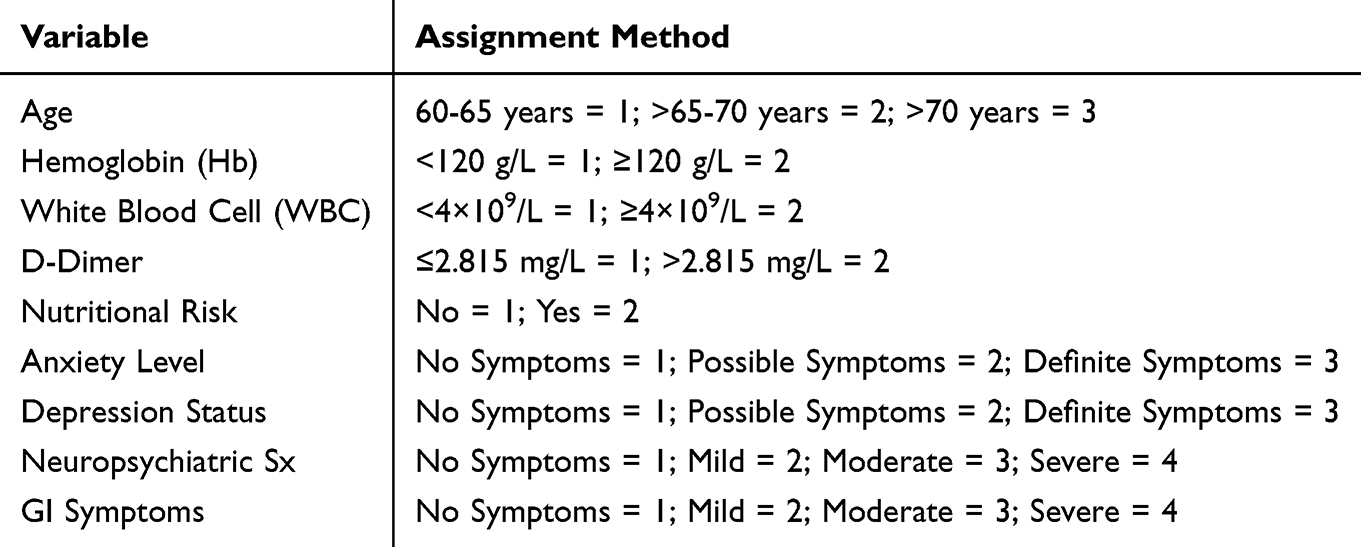 |
Table 2 Variable Assignment Methods |
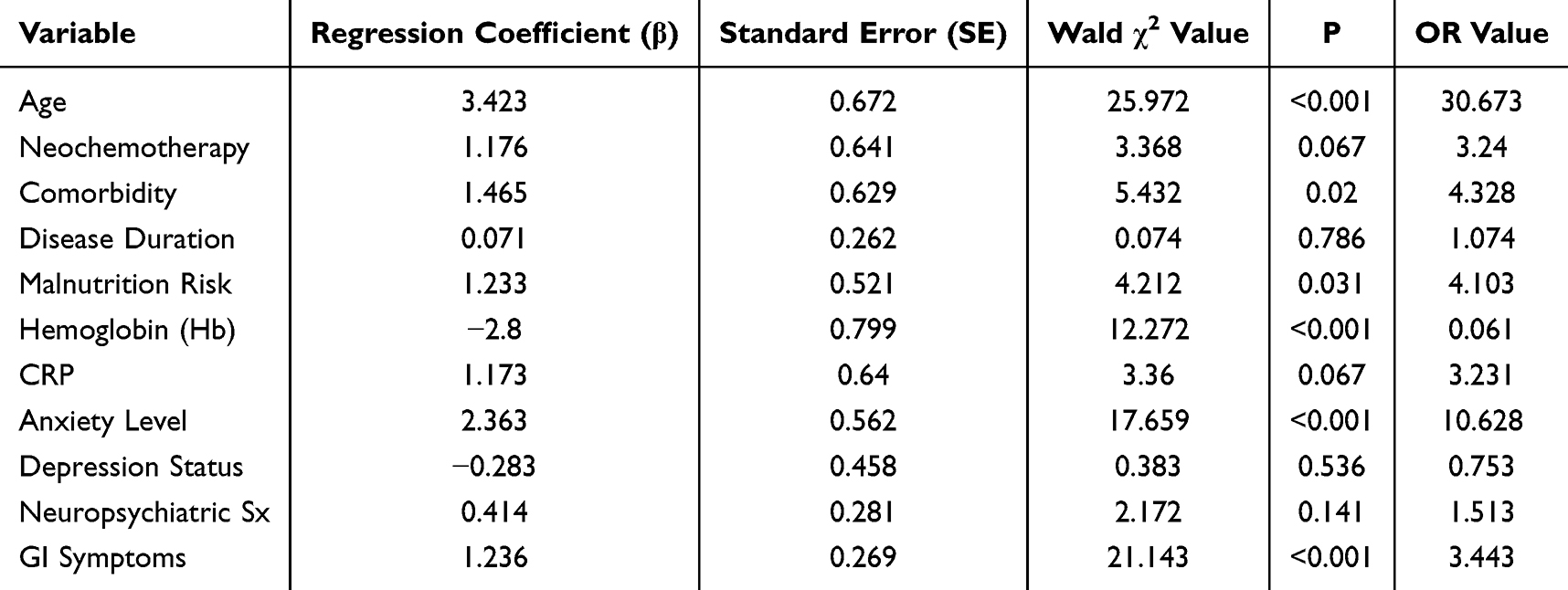 |
Table 3 Multivariate Analysis of Influencing Factors of Pre-Frailty in Elderly Patients with Gastric Cancer Undergoing Surgery |
Variables with significant univariate results were included as independent variables in Logistic regression, with pre-frailty as the dependent variable. Age, BMI, gender, NE, Hb, CRP and D-dimer were entered as original values; other variables were coded. Results showed that age, combidity, hemoglobin concentration, malnutrition risk, depression status, and GI symptoms were independent influencing factors of frailty (P<0.05).
Based on the independent influencing factors identified in the multivariate analysis, a Nomogram risk prediction model for preoperative pre-frailty in elderly patients with gastric cancer was constructed (Figure 1).
 |
Figure 1 Risk prediction model for pre-frailty in elderly patients with gastric cancer undergoing surgery. |
Performance of the Risk Prediction Model for Pre-Frailty in Elderly Gastric Cancer Patients
The Hosmer-Lemeshow goodness-of-fit test was used to evaluate the model’s calibration. The test results showed χ2=6.896, P=0.548. This indicates that the model’s predictive ability is consistent with the actual occurrence rate demonstrating good fit. The AUC was 0.986 [95% CI (0.972, 0.999)] (Figure 2). The Youden index was highest (0.568) at a model cutoff value of 0.452, corresponding to a sensitivity of 0.889 and a specificity of 0.945.
 |
Figure 2 ROC curve of the risk prediction model for pre-frailty in elderly patients with gastric cancer undergoing surgery. |
Discussion
To the best of our knowledge, this is the first study investigate the preoperative status of pre-frailty and its influencing factors to establish a prediction model in older gastric cancer patients. The results of this study show that prevalence of pre-frailty in patients with gastric cancer was 53.4%. The number of pre-frail patients was approximately 1.93 times that of non-frail patients, higher than the ratio reported in studies by Doody et al.9 Possible reasons for this discrepancy are as follows: 1) The study population consisted of elderly patients undergoing gastric cancer surgery. Both the malignant nature of cancer and the adverse effects of surgery can impair the health status of patients, increasing the detection rate of pre-frailty. 2) Differences in assessment tools may lead to variations in results. Doody et al’s study synthesized data from multiple studies that used a variety of frailty assessment scales, while this study uniformly adopted the Fried Frailty Phenotype scale. 3) Population differences may also contribute to the variation. The subjects in Doody et al’s study were elderly individuals from multiple countries, whereas this study focused on elderly patients with gastric cancer in China, whose health status may be more affected by the disease and surgery.
The health status of elderly patients undergoing gastric cancer surgery is closely related to the adverse effects of surgery. Therefore, assessing and intervening in pre-frailty is crucial for preventing the development of overt frailty in these patients. Healthcare providers should pay close attention to the decline in health status in this population, proactively take measures to delay their progression to pre-frailty, and help pre-frail patients revert to a non-frail state, thereby significantly improving their health outcomes. Preoperative pre-frailty assessment is essential for identifying high-risk patients and implementing early interventions to prevent postoperative functional decline. Based on this study, age, hemoglobin concentration, malnutrition risk, depression status, and GI symptoms were identified as the main influencing factors of preoperative pre-frailty in elderly patients with gastric cancer.
This study confirmed that age is an independent influencing factor of pre-frailty in elderly patients undergoing gastric cancer surgery, with the risk of pre-frailty increasing with age. This is consistent with the findings of previous studies.9 As age increases, the physiological functions, organ function, and immune function of the elderly gradually decline, accelerating the transition to pre-frailty. For elderly patients undergoing gastric cancer surgery, their tolerance to the adverse effects of surgery decreases with age, further increasing the risk of pre-frailty. This suggests that healthcare providers should pay special attention to elderly patients with advanced age, and develop individualized intervention measures based on their specific conditions to delay the progression to pre-frailty.
Malnutrition risk was found to be a promoting factor for pre-frailty in elderly patients undergoing gastric cancer surgery. The risk of pre-frailty in patients with malnutrition risk was 2.203 times that of patients without malnutrition risk. Surgery-induced symptoms such as anorexia, nausea, and vomiting can interfere with normal dietary intake, leading to reduced intake of dietary fiber, vitamins, and protein, and ultimately impairing the overall nutritional status of patients. Existing studies have shown that physical frailty is closely associated with malnutrition,10 and supplementation of functional nutrients and protein plays a key role in reducing the risk of frailty syndrome. Therefore, healthcare providers should strengthen nutritional support for elderly patients undergoing gastric cancer surgery, take into account both nutritional needs and individual dietary preferences, and improve the effectiveness of interventions for frailty syndrome.
Hemoglobin concentration is an influencing factor for pre-frailty in elderly gastric cancer surgery patients. Higher hemoglobin concentration is a protective factor against pre-frailty.11 Under the influence of surgery drugs, bone marrow hematopoietic function rapidly declines, red blood cells in the blood decrease rapidly, and the survival time of red blood cells shortens. Coupled with reduced production of erythropoietin in the body, this can lead to a decrease in hemoglobin concentration, thereby accelerating the patient’s entry into pre-frailty. Continuous monitoring of hemoglobin concentration is beneficial for early detection of functional decline in patients and is a relatively important indicator for determining whether a patient is in pre-frailty.
This study also found that depression status is an influencing factor of pre-frailty in elderly patients undergoing gastric cancer surgery, with patients with higher depression levels having a higher risk of developing pre-frailty.12 A cross-sectional survey by Yang Fan et al13 showed that patients with higher depressive tendencies have reduced participation in social and physical activities, which increases the risk of pre-frailty. Meanwhile, frailty can also exacerbate psychological stress in individuals. Furthermore, patients with severe depression often have elevated levels of inflammatory markers such as CRP and interleukin-6, which may lead to severe impairment of muscle mass and function. It is recommended to utilize social resources (eg, establishing patient interaction groups and peer support groups) to promote experience sharing among patients, enhance their sense of belonging, and improve their trust in healthcare providers.
Gastric cancer-related GI symptoms (diarrhea, abdominal pain, anorexia) impair digestion, cause energy metabolism disorders, and nutrient deficiency, accelerating pre-frailty. Tumor-derived proinflammatory cytokines induce systemic inflammation, enhance protein catabolism, and disrupt muscle anabolism, leading to pre-frailty.14 Patients with more severe and long-lasting GI symptoms often have impaired physical function and increased anxiety, making them more prone to pre-frailty. This suggests that healthcare providers should strengthen the management of surgery-related symptoms and explore effective interventions to delay or reverse the decline in health status.
The pre-frailty risk prediction model constructed in this study, based on the identified high-risk factors, was applied to assess the pre-frailty status of 317 elderly patients with gastric cancer during preoperative evaluation. The model exhibited excellent predictive value, with an AUC of 0.986. Nomograms can effectively quantify the odds ratio of each influencing factor and convert it into a simple scoring system, serving as an intuitive and practical risk assessment tool for surgeons. This enables surgeons to more accurately evaluate the suitability of patients for surgery. The development of this preoperative pre-frailty prediction model for elderly patients with gastric cancer represents a significant contribution of this study. As a reliable and accurate assessment tool, it helps healthcare providers identify high-risk pre-frail patients, provides a solid basis for early prevention and intervention, and facilitates more in-depth doctor-patient communication. This helps patients better understand the potential risks and benefits of surgery, thereby improving their participation in treatment decisions and satisfaction with care.
However, this study has several limitations that should be acknowledged. First, it is a single-center retrospective study with a convenience sampling method, which may limit the representativeness of the sample and fail to fully reflect the characteristics of the broader population of elderly patients with gastric cancer. To reduce selection bias, future studies should adopt a random sampling method to ensure greater diversity and representativeness of the sample. Second, due to differences in healthcare systems and cultural backgrounds across countries and regions, the applicability and generalizability of the model need to be further validated in multi-center studies with diverse populations. Third, this study did not include socioeconomic factors (eg, income level, education level), healthcare accessibility (eg, frequency of medical visits, insurance coverage), and social support in the analysis. These factors may also be associated with pre-frailty and postoperative outcomes.
To address these limitations in future research, it is recommended to collect data on socioeconomic status (eg, income, education, occupation), healthcare accessibility (eg, insurance type, frequency of medical check-ups, satisfaction with healthcare services), and social support (assessed using validated social support scales) through questionnaires and electronic health records. Incorporating these factors into the prediction model will significantly improve its predictive accuracy and clinical applicability.
Conclusion
The prevalence of preoperative pre-frailty is relatively high (53.4%) in elderly patients with gastric cancer. Age, comorbidities, low hemoglobin concentration, risk of malnutrition, depressive state, and gastrointestinal symptoms are the independent influencing factors of preoperative pre-frailty in this population. The risk prediction model constructed based on these factors (presented in the form of a nomogram) has good predictive accuracy and discriminative ability, but the possibility of overfitting should be noted, and further external validation is needed.
Clinical medical staff should pay close attention to elderly gastric cancer patients with advanced age, underlying comorbidities, low hemoglobin levels, risk of malnutrition, poor mental health status, and obvious gastrointestinal symptoms. The constructed nomogram model has potential practical value in preoperative screening for pre-frailty, which can help identify high-risk patients early and provide a basis for formulating individualized intervention plans. Future multicenter studies with larger sample sizes are recommended to validate the model’s generalizability, and intervention studies should be conducted to evaluate the effect of targeted measures on preventing pre-frailty and improving patient outcomes.
Consent to Participate Declaration
All individual participants included in this study have provided written, informed consent prior to their enrollment. The consent process strictly adhered to the ethical principles outlined in the Declaration of Helsinki (2013 revision) and the Ethics Committee of the First Hospital of China Medical University, which approved this study.
Funding
This work was supported by the Fund of Liaoning Provincial Department of Science and Technology (2023-MSLH-397). The funders had no role in considering the study design or in the collection, analysis, interpretation of data, writing of the report, or decision to submit the article for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
2. Tian Y, Lin Y, Sun C, et al. Comparison of short-term efficacy and safety between total robotic and total 3D laparoscopic distal radical gastrectomy for gastric cancer in Enhanced Recovery After Surgery (ERAS) protocol: a propensity score matching study. J Robot Surg. 2023;17:1151–1158. doi:10.1007/s11701-023-01528-8
3. You K, Han H. Application of ERAS in older patients with gastric cancer. Medicine. 2024;103:e38409. doi:10.1097/MD.0000000000038409
4. Guo Y, Miao X, Chen Y, et al. Hypothetical interventions on frailty heterogeneous trajectories of older patients with gastric cancer using parametric G-formula. Ann Surg Oncol. 2025. doi:10.1245/s10434-025-18026-w
5. Jinnouchi H, Kitamura A, Yamagishi K, et al. Associations of body mass index, lifestyle factors, and medical findings in midlife with frailty in older ages: a 15-year longitudinal study. Geriatr Gerontol Int. 2025;25:889–896. doi:10.1111/ggi.70074
6. Xia Y, He M, Guo Y, et al. Construction and validation of frailty risk prediction model in elderly patients with colorectal cancer. BMC Geriatr. 2025;25:601. doi:10.1186/s12877-025-06195-y
7. Włodarczyk J. Molecular mechanisms and clinical implications of complex prehabilitation in colorectal cancer surgery: a comprehensive review. Int J Mol Sci. 2025;26:7242. doi:10.3390/ijms26157242
8. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56:M146–156. doi:10.1093/gerona/56.3.m146
9. Doody P, Asamane EA, Aunger JA, et al. The prevalence of frailty and pre-frailty among geriatric hospital inpatients and its association with economic prosperity and healthcare expenditure: a systematic review and meta-analysis of 467,779 geriatric hospital inpatients. Ageing Res Rev. 2022;80:101666. doi:10.1016/j.arr.2022.101666
10. Coelho-Júnior HJ, Álvarez-Bustos A, Russo A, Rodriguez-Mañas L, Landi F, Marzetti E. Associations between malnutrition and physical performance, sarcopenia, and frailty in older adults. BMC Geriatr. 2025;25:612. doi:10.1186/s12877-025-06274-0
11. Wong CWY, PW Li, Doris SF, Ho BM, Chan BS. Estimated prevalence of frailty and prefrailty in patients undergoing coronary artery or valvular surgeries/procedures: a systematic review and proportional meta-analysis. Ageing Res Rev. 2024;96:102266. doi:10.1016/j.arr.2024.102266
12. Xu L, Lin X, Zhou T, Liu Y, Ge S. High cotinine levels as an associated factor with frailty status in older adults: evidence from the NHANES study. BMC Geriatr. 2024;24:894. doi:10.1186/s12877-024-05482-4
13. Hou Y, Meng Y, Wu F, Yang S, Yang F. Psychological disturbances and associated risk factors in chinese mine rescuers: a cross-sectional study. Neuropsychiatr Dis Treat. 2025;21:751–760. doi:10.2147/NDT.S504337
14. Xing S, Li X, Chen C. Association between frailty and inflammatory cytokines in patients with multiple sclerosis: a case-control study. Cytokine. 2025;191:156945. doi:10.1016/j.cyto.2025.156945
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Current Perspectives on Indications for Ileal Pouch-Anal Anastomosis in Older Patients
Shore BM, Kochar B, Herfarth HH, Barnes EL
Clinical and Experimental Gastroenterology 2022, 15:163-170
Published Date: 23 September 2022
Nomogram Based on Preoperative Fibrinogen and Systemic Immune-Inflammation Index Predicting Recurrence and Prognosis of Patients with Borrmann Type III Advanced Gastric Cancer
Wang H, Yin X, Ma K, Wang Y, Fang T, Zhang Y, Xue Y
Journal of Inflammation Research 2023, 16:1059-1075
Published Date: 12 March 2023
Factors Influencing Delayed Onset of Lactogenesis: A Scoping Review
Li S, Wupuer T, Hou R
International Journal of General Medicine 2024, 17:2311-2326
Published Date: 21 May 2024
Length of Hospital Stay in Patients with Primary Liver Cancer Undergoing Surgery: Risk Factors and Predictive Model Development
Sun B, Li X, He X, Zhang N
Journal of Hepatocellular Carcinoma 2026, 13:584645
Published Date: 17 February 2026
Mediating Role of Dyadic Coping Between Social Support and Oral Frailty Cross-Sectional Study of Elderly Ovarian Cancer Patients in China
Jin J, Zhao D, Chen Y
International Journal of Women's Health 2026, 18:594341
Published Date: 23 April 2026