Back to Journals » Infection and Drug Resistance » Volume 19
Risk Factors Analysis and Nomogram Prediction Model Construction for Pulmonary Infection After Laparoscopic Cholecystectomy
Authors Huang X, Li Y, Huang X, Chen Y
Received 31 July 2025
Accepted for publication 16 January 2026
Published 22 January 2026 Volume 2026:19 557317
DOI https://doi.org/10.2147/IDR.S557317
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Xiaomei Huang, Yiping Li, Xiaoliang Huang, Yijian Chen
Department of Anesthesiology, Ganzhou People’s Hospital, Ganzhou, Jiangxi Province, 341000, People’s Republic of China
Correspondence: Yijian Chen, Department of Anesthesiology, Ganzhou People’s Hospital, 16 Meiguan Avenue, Zhanggong District, Ganzhou City, Jiangxi Province, 341000, People’s Republic of China, Email [email protected]
Objective: To explore the risk factors of pulmonary infection after laparoscopic cholecystectomy and construct a nomogram prediction model.
Methods: From July 2022 to April 2025, 594 patients who underwent laparoscopic cholecystectomy in our hospital were included and randomly separated into a modeling group of 416 cases and a validation group of 178 cases in a 7:3 ratio. The modeling group was separated into an infection group of 50 cases and a non infection group of 366 cases based on the occurrence of postoperative pulmonary infection. The operative time, preoperative albumin (Alb), preoperative WBC and other data were recorded. Single factor and multiple factor logistic regression analyses were performed to determine risk factors. R software was performed to construct nomogram prediction models. Receiver Operating Characteristic(ROC) curve was used to evaluate discrimination, the calibration curve was used to evaluate calibration, and the clinical decision curve was used to evaluate net benefit.
Results: Parameters like male sex, diabetes, long operative time, and high preoperative WBC were independent risk factors for pulmonary infection after laparoscopic cholecystectomy, while high preoperative Alb was an independent protective factor (P< 0.05). The Hosmer-Lemeshow test for the modeling and validation groups showed P=0.43,0.35; the Area Under the Curve(AUC) values of the ROC curve were 0.94 (95% CI: 0.90~0.98) and 0.93 (95% CI: 0.89~0.97). In the calibration curve results, the predicted probability was basically consistent with the actual probability. In the clinical decision curve results, the nomogram prediction model provided greater net benefits within the threshold probability ranges of 2%~83% and 3%~86%.
Conclusion: The nomogram model constructed in this study can be effectively used to evaluate the individual risk of pulmonary infection after laparoscopic cholecystectomy.
Keywords: laparoscopic cholecystectomy, pulmonary infection, risk factors, nomogram
Introduction
Laparoscopic cholecystectomy has become the primary treatment for cholecystectomy, characterized by minimal trauma, less postoperative discomfort, short hospital stay, and a fast recovery period.1 Laparoscopic cholecystectomy, compared with open surgery, causes less damage to the abdominal wall muscles and nerves, significantly reduces postoperative pain, enables early ambulation, promotes pulmonary function recovery, and may partially lower the risk of postoperative pulmonary complications.2,3 However, laparoscopic surgery requires pneumoperitoneum, and CO2 insufflation can cause diaphragmatic elevation, reduced lung compliance, and decreased functional residual capacity, all of which may increase the risk of pulmonary infections and other respiratory complications.4 Pulmonary infection can further lead to complications like respiratory failure, sepsis, empyema, and pleural effusion, worsening the patient’s condition and affecting survival outcomes and medical costs.5 Therefore, there is a clinical need to distinguish and identify patients at high risk of postoperative pulmonary infection early on, and to promote early intervention to reduce its incidence or improve postoperative outcomes. Previous studies have mostly focused on the risk factors for surgical site infections after laparoscopic cholecystectomy, while the risk factors for pulmonary infection remain unclear.6–8 Nomograms are primarily based on multivariate regression models. Their core principle is to convert regression coefficients into additive scores through linear mapping, allowing rapid calculation of the probability of a specific outcome. Currently, nomograms have been widely applied in various fields, such as postoperative complications after thoracoscopic lung cancer surgery and prolonged air leaks after minimally invasive lung resection.9,10 However, their application in pulmonary infections following laparoscopic cholecystectomy remains to be further investigated. Consequently, this study aims to investigate the risk factors for postoperative pulmonary infection following laparoscopic cholecystectomy and to construct a nomogram prediction model based on these risk factors to identify high-risk patients.
Materials and Methods
Study Subjects
This was a retrospective study involving all patients who underwent laparoscopic cholecystectomy at our hospital between July 2022 and April 2025,with patients enrolled consecutively. The inclusion criteria were: ① all patients underwent laparoscopic cholecystectomy for conditions including symptomatic gallstones with surgical indications, chronic cholecystitis, and polypoid lesions of the gallbladder; ② age 18 years or older; and ③ complete case data. The exclusion criteria were: ① concurrent neoplastic diseases; ② concurrent dysfunction of other organs; ③ concurrent autoimmune or hematological system diseases; and ④ a history of acute or chronic infection within the last 3 months. The study was approved by the hospital’s Medical Ethics Committee. The study flowchart is shown in Figure 1. Based on the inclusion and exclusion criteria, a total of 594 patients who underwent laparoscopic cholecystectomy were included and randomly divided into a development cohort (n=416) and a validation cohort (n=178) at a 7:3 ratio[A 7:3 ratio is widely used in predictive model studies, as it ensures both the stability and reliability of the modeling set (meeting the EPV principle) and provides a sufficient sample size in the validation set to assess model performance]. In the development cohort, patients were further divided into an infected group (n=50) and a non-infected group (n=366) based on the occurrence of postoperative pulmonary infection.
 |
Figure 1 Case flow chart. |
Outcomes and Data Collection
The primary endpoint was pulmonary infection. The definition of pulmonary infection was based on the criteria from the Centers for Disease Control and Prevention and the National Healthcare Safety Network surveillance definition:11 the brief assessment criteria included positive pathogen results from sputum culture; inflammatory infiltrative lesions in the lungs on imaging studies; a temperature higher than 38°C; significantly elevated WBC count and neutrophils in laboratory tests; and clinical signs such as cough, sputum production, and moist rales in the lungs. Data collected included patient gender, smoking (defined as continuous or cumulative smoking for six months or more in a lifetime), alcohol consumption (defined as an average daily pure alcohol intake of more than 60 g for men and more than 40 g for women), age, body mass index (BMI), diabetes, hypertension, prophylactic antibiotic use, American Society of Anesthesiologists (ASA) classification, operation time, intraoperative blood loss, postoperative hospital stay, insufficient cystic duct stump, gallbladder perforation, gallbladder abscess, preoperative albumin (Alb), preoperative hemoglobin (Hb), preoperative WBC, and preoperative C-reactive protein (CRP).
Statistical Analysis
SPSS 26.0 and R Studio 4.0.2 software were used for statistical analysis. Normally distributed measurement data were expressed as mean ± standard deviation (x±s) and compared between groups using the independent samples t-test. Count data were expressed as n (%) and compared between groups using the χ2 test. Included patients were randomly divided into a development cohort and a validation cohort at a 7:3 ratio. In the univariate analysis, variables with a P < 0.05 were included in a multivariate logistic regression analysis to identify the risk factors for postoperative pulmonary infection after laparoscopic cholecystectomy. Features were presented as odds ratios (OR) with 95% confidence intervals (CI). A two-tailed P < 0.05 was considered statistically significant. Internal validation was used to evaluate the predictive performance of the nomogram model. The receiver operating characteristic (ROC) curve was used to assess discrimination, the calibration curve to assess calibration, and decision curve analysis to assess the net benefit.
Results
Comparison of Data Between the Development and Validation Cohorts
There were no statistically significant differences (P=0.17,0.49,0.36,0.17,0.33,0.71,0.11,0.11,0.75,0.07,0.11,0.29,0.10,0.42,0.50,0.40,0.88,0.51,0.21) between the development cohort and the validation cohort in terms of gender, smoking, alcohol consumption, age, BMI, diabetes, hypertension, prophylactic antibiotic use, ASA classification, operation time, intraoperative blood loss, postoperative hospital stay, insufficient cystic duct stump, gallbladder perforation, gallbladder abscess, preoperative Alb, preoperative Hb, preoperative WBC, and preoperative CRP. See Table 1.
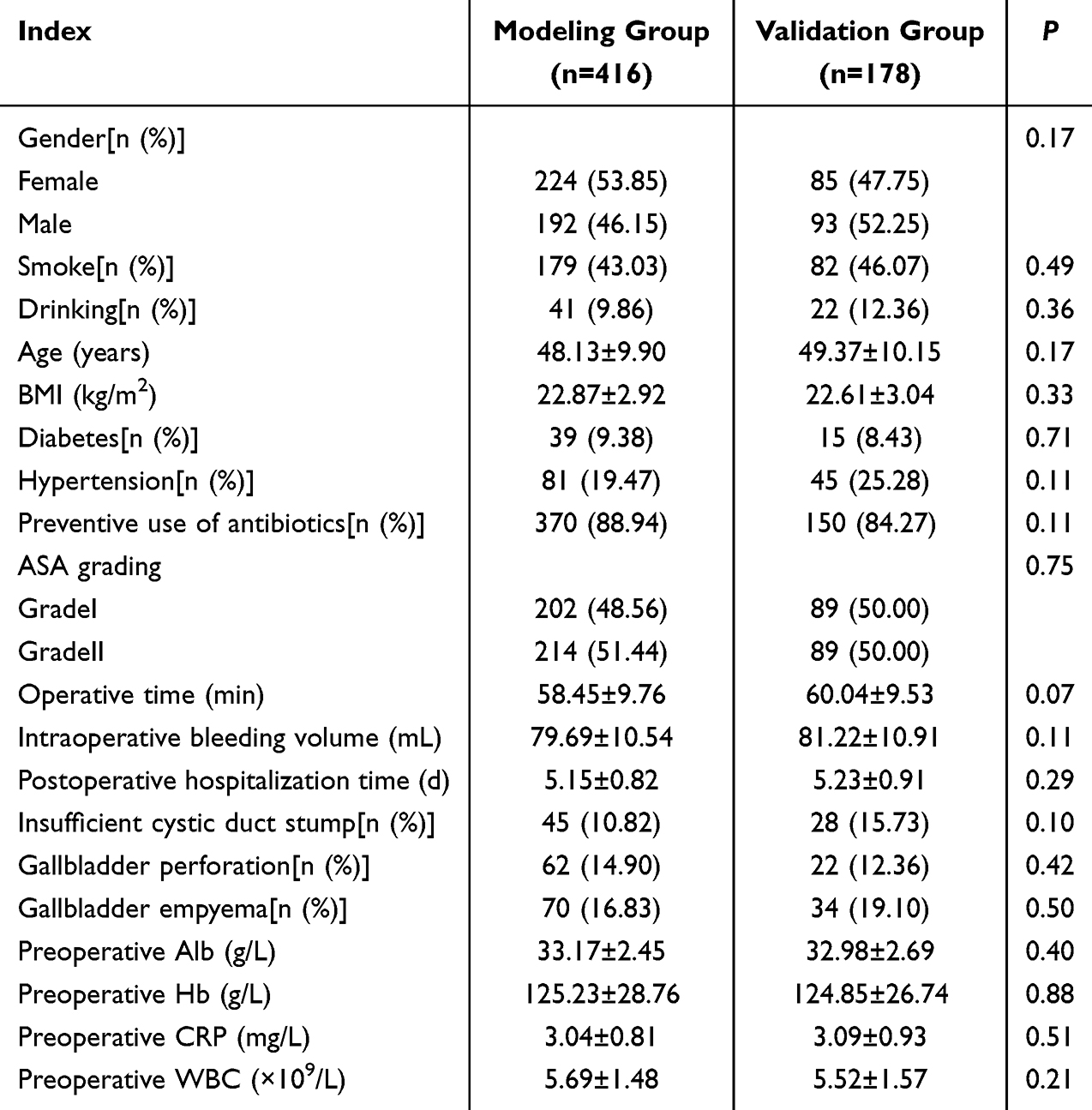 |
Table 1 Comparison of Data Between Modeling Group and Validation Group[n (%) / ( |

Univariate Analysis of Postoperative Pulmonary Infection After Laparoscopic Cholecystectomy
There were no statistically significant differences (P=0.10,0.19,0.12,0.24,0.63,0.10,0.26,0.07,0.10,0.44,0.51,0.81,0.70,0.34)) between the infected and non-infected groups in terms of smoking, alcohol consumption, age, BMI, hypertension, prophylactic antibiotic use, ASA classification, intraoperative blood loss, postoperative hospital stay, insufficient cystic duct stump, gallbladder perforation, gallbladder abscess, preoperative Hb, and preoperative CRP. The proportion of males, proportion with diabetes, operation time, and preoperative WBC were higher in the infected group, while preoperative Alb was lower, compared to the non-infected group (P < 0.05). See Table 2.
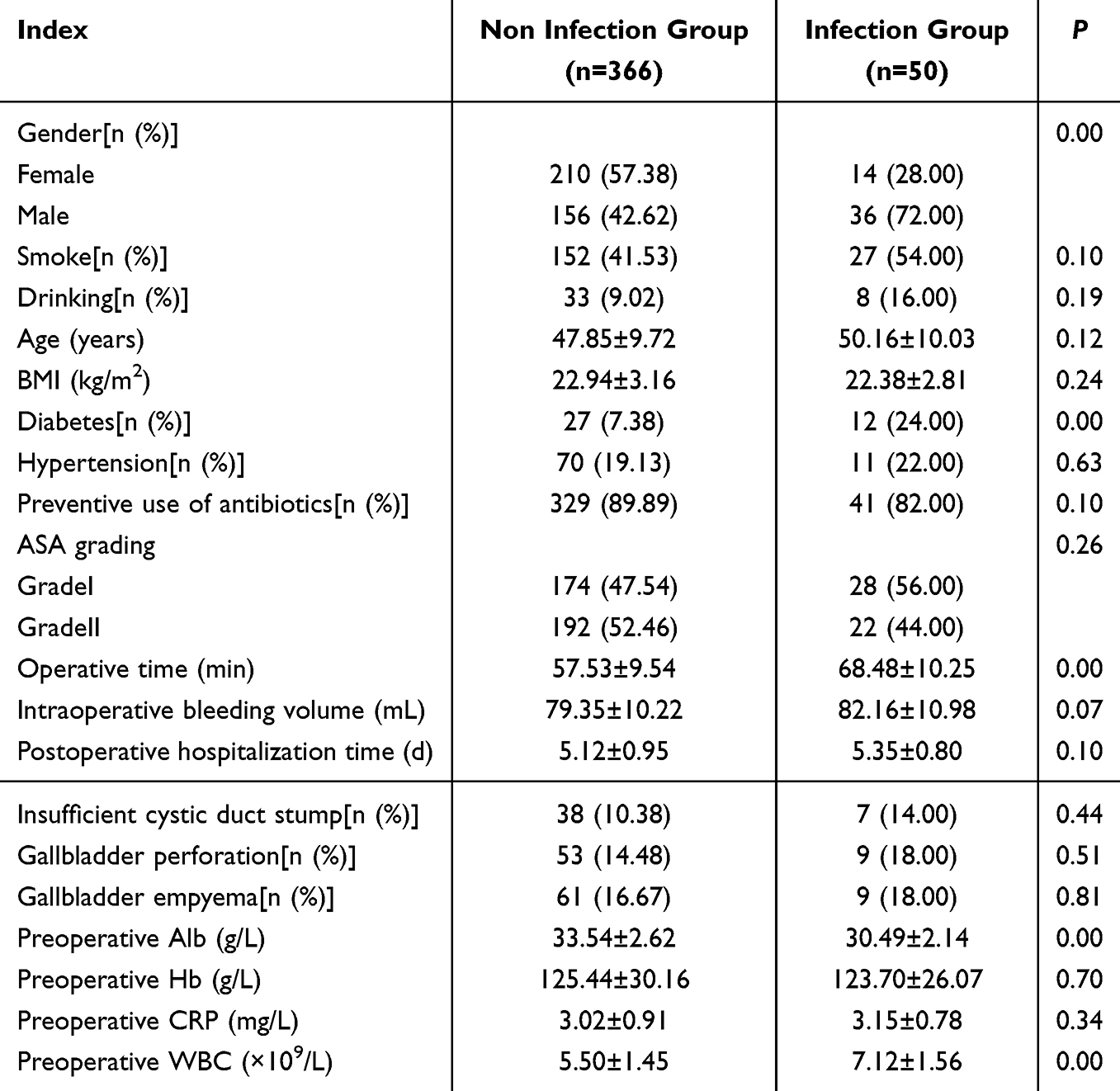 |
Table 2 Univariate Analysis of Pulmonary Infection After Laparoscopic Cholecystectomy[n (%) / ( |

Analysis of Influencing Factors for Postoperative Pulmonary Infection After Laparoscopic Cholecystectomy
Variables that showed significant differences in the univariate analysis were included as independent variables in the multivariate analysis, with the occurrence of pulmonary infection as the dependent variable. The results of the logistic regression analysis, presented in Table 3, showed that male gender, presence of diabetes, long operation time, and high preoperative WBC were independent risk factors for postoperative pulmonary infection after laparoscopic cholecystectomy, while high preoperative Alb was an independent protective factor (P < 0.05).
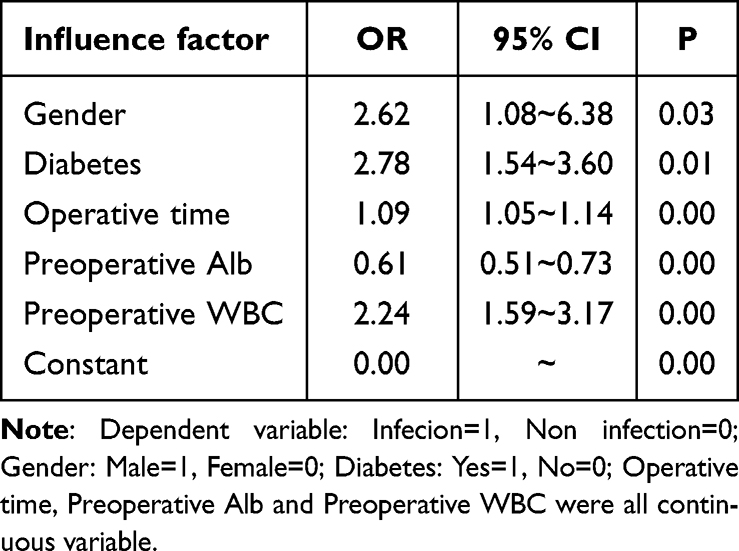 |
Table 3 Multivariate Logistic Regression Analysis of Lung Infection Following Laparoscopic Cholecystectomy |
Construction of a Nomogram Prediction Model for Postoperative Pulmonary Infection After Laparoscopic Cholecystectomy
Based on the regression analysis results from Table 3, a nomogram was constructed using R software with gender, diabetes, operation time, preoperative Alb, and preoperative WBC as predictors. The model constructed from these predictors was: logit(P) = 2.20 + 0.96 × Gender + 1.75 × Diabetes + 0.09 × Operation Time - 0.49 × Preoperative Alb + 0.81 × Preoperative WBC. The nomogram is shown in Figure 2.
 |
Figure 2 The nomogram used to predict lung infection following laparoscopic cholecystectomy. Note: Draw a vertical line up for each individual variable to obtain its “Points”, add the points together to obtain the total points, find the corresponding value on the “Total Points” axis, and draw a vertical line down to obtain the “Prediction probability” (ie the risk of postoperative lung infection). |
ROC Curve and Calibration Curve Analysis of the Nomogram Prediction Model
The Bootstrap method was used for internal validation of the nomogram prediction model. The Hosmer-Lemeshow goodness-of-fit test showed P=0.43 for the development cohort and P=0.35 for the validation cohort. ROC curves were plotted based on the nomogram prediction model. The AUC was 0.94 (95% CI: 0.90–0.98) for the development cohort and 0.93 (95% CI: 0.89–0.97) for the validation cohort, with sensitivities of 82.34% and 83.07%, and specificities of 92.16% and 94.35%, respectively.The Youden indices were 0.75 and 0.77, the positive predictive values (PPV) were 58.57% and 66.67%, and the negative predictive values (NPV) were 97.40% and 97.73%. This indicates that the nomogram prediction model can effectively distinguish between patients at high and low risk of pulmonary infection. The calibration curve results for both the development and validation cohorts showed good agreement between the predicted probabilities and the actual probabilities, with the calibration curves being close to the ideal curve. See Figure 3.
 |
Figure 3 The ROC curves and calibration curves of the nomogram used to predict lung infection following laparoscopic cholecystectomy in the modeling group and validation group (A) ROC curve in modeling group; (B) Calibration curve in modeling group; (C) ROC curve in validation group; (D) Calibration curve in validation group. |
Decision Curve Analysis of the Nomogram Prediction Model
The decision curve analysis showed that the nomogram prediction model provided a greater net benefit within the threshold probability ranges of 2%–83% and 3%–86%. See Figure 4.
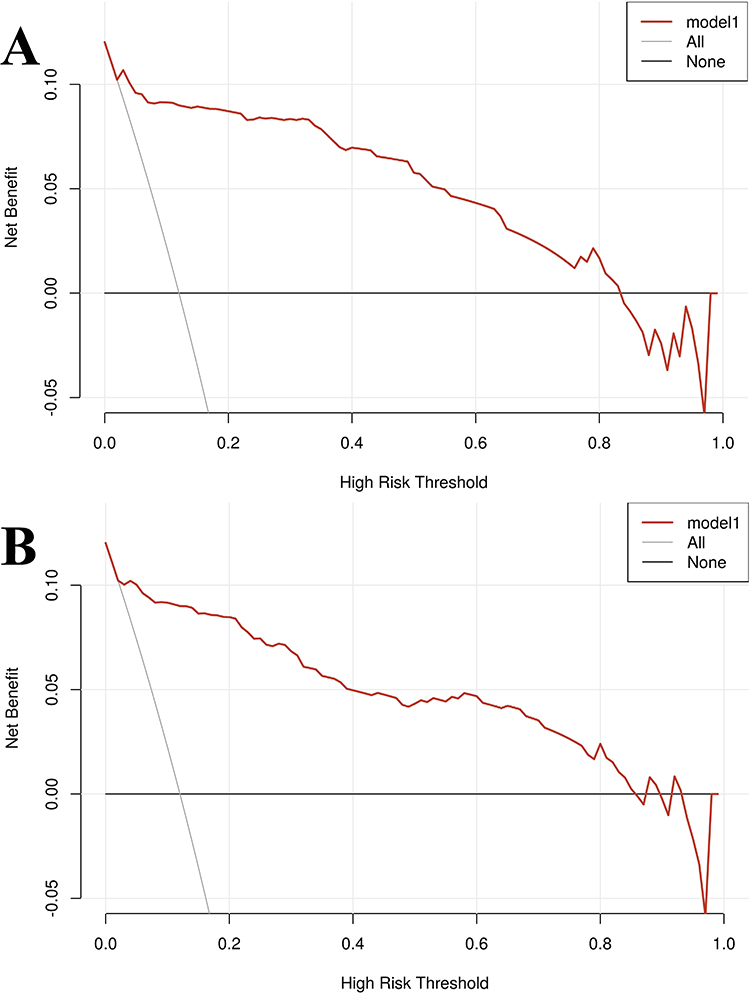 |
Figure 4 The clinical decision curves of the nomogram used to predict lung infection following laparoscopic cholecystectomy in the modeling group and validation group (A) Modeling group; (B) Validation group. Note: The model line is the nomogram for predicting the model line; The All line represents the net benefit that can be obtained by treating all patients; The None line represents the net benefit that all patients can obtain without treatment; |
Discussion
In this study, the incidence of postoperative pulmonary infection after laparoscopic cholecystectomy in the development cohort was 12.02% (50/416). This is lower than the 18.70% incidence of postoperative pulmonary infection after laparoscopic surgery reported by Liu et al12 and the 20.83% incidence after gastrointestinal surgery reported by Tang et al13 but it is generally consistent with the 12.3% incidence of viral hepatitis after hepatectomy reported by Loncar et al.14 This similarity between laparoscopic cholecystectomy and hepatectomy in the incidence of postoperative infectious complications may be related to the fact that both procedures involve upper abdominal manipulation, significantly affecting the diaphragm and respiratory function. Through univariate and multivariate analyses, five key predictors for postoperative pulmonary infection after laparoscopic cholecystectomy were identified: gender, diabetes, operation time, preoperative Alb, and preoperative WBC. The nomogram constructed based on these factors demonstrated high predictive performance and significant clinical net benefit.
Our results found that significant risk factors associated with postoperative pulmonary infection include gender. This is reflected in the literature, indicating that male patients have a higher probability of developing infections after laparoscopic cholecystectomy.15 Possible explanations for this correlation include a more intense inflammatory pattern in male cholecystitis, variations in male anatomical structures that make the surgical procedure more difficult, and the fact that male patients tend to seek medical services less frequently than female patients, thus receiving medical care at a later clinical stage. The results show that patients with diabetes are more prone to concurrent postoperative pulmonary infection, with a risk 2.78 times that of non-diabetic patients (OR = 2.78). This may be related to immune cells, particularly the subsets of dendritic cells originating from the lungs that coordinate the immune response to infection. In diabetic patients with long-term exposure to high glucose levels, these cells are severely damaged, which in turn impairs downstream immune induction and increases the risk of infection.16,17 Our findings indicate that operation time is an independent risk factor for pulmonary infection after laparoscopic cholecystectomy. After controlling for other confounding factors, for every 10-minute increase in operation time, the risk of postoperative pulmonary infection increases by 9% (OR = 1.09). A study by Wang et al18 also found that prolonged operation time was independently associated with increased incidences of surgical site infection, pneumonia, and pulmonary embolism and longer hospital stays after laparoscopic cholecystectomy for cholecystitis in 7031 patients from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database. The analysis suggests that because hepatobiliary surgery is complex, a prolonged operation increases the patient’s physiological burden and may trigger greater immunosuppression and inflammatory responses, thereby increasing the risk of infection. Therefore, reducing the duration of laparoscopic cholecystectomy and providing appropriate postoperative analgesia can reduce corresponding complications. The results from Li et al19 confirmed that low preoperative Alb levels are an influencing factor for postoperative pulmonary infections in patients with esophageal cancer. Our findings are similar to this study, showing that the lower the preoperative Alb level, the higher the risk of postoperative pulmonary infection. Previous research has found a clinical correlation between Alb levels and the occurrence of respiratory tract infections.20,21 This finding can be explained, on one hand, by the lower immunity in patients with low Alb levels, making them susceptible to pulmonary infections. On the other hand, hypoalbuminemia can lead to a decrease in plasma osmotic pressure, causing pulmonary interstitial edema, while reduced gas diffusion and an abnormal ventilation/perfusion ratio make patients more prone to pulmonary infections. Furthermore, our study identified high preoperative WBC as an independent risk factor for pulmonary infection. The results from Liu et al12 also found that WBC is a risk factor for postoperative pulmonary complications in elderly patients undergoing laparoscopic surgery, especially for postoperative pulmonary infection (which dominated the distribution of pulmonary complications). Disease and surgical trauma often trigger an inflammatory response in the body, and WBC play a crucial role in the inflammatory process. An elevated WBC level, to some extent, reflects an exacerbated inflammatory state in the patient, which may promote the occurrence of infection. Thus, it can serve as a predictive indicator of the postoperative inflammatory state.22 Moreover, since WBC can be obtained through routine preoperative blood tests, its importance warrants further evaluation.
A nomogram prediction model was constructed based on the aforementioned risk factors. The results showed that the AUC of the nomogram was 0.938 and 0.932 for the development and validation cohorts, respectively. The similar AUCs indicate that the constructed model has stable performance and high discrimination, effectively distinguishing between patients at high and low risk of postoperative pulmonary infection. The calibration curve showed good agreement between the predicted and actual probabilities, while the decision curve analysis demonstrated the high clinical utility of the nomogram model. Therefore, this nomogram prediction model, incorporating these five simple clinical factors, can help clinicians identify high-risk patients for postoperative pulmonary infection before surgery. This is conducive to improving perioperative care management, promoting the control of postoperative pulmonary infections, and consequently improving clinical outcomes and reducing medical costs.
However, this study has some limitations. First, the data were collected mainly through retrospective analysis, which may reduce the reliability of the information, potentially introduce bias, and increase the risk of misdiagnosis and missed diagnoses, thereby confounding the results. Second, as a single-center study, the sample size may be insufficient, and some risk factors may not have been included, which could weaken the robustness of the model. Third, external validation with other centers was not performed, and its application value requires further confirmation through external validation.
In conclusion, this study developed a nomogram prediction model incorporating five simple clinical factors to predict postoperative pulmonary infection after laparoscopic cholecystectomy. This model can help clinicians identify high-risk individuals early, formulate optimal surgical plans and perioperative management strategies, and reduce the incidence of postoperative pulmonary infections through strategies such as shortening operation time, avoiding anatomical structure-related difficulties, controlling blood glucose levels, and maintaining optimal preoperative indicator levels. However, larger sample sizes and multi-center studies are needed to confirm these conclusions.
Data Sharing Statement
All data generated or analysed during this study are included in this article.
Ethics Approval and Consent to Participate
Ethics approval was obtained from Ethics Committee of Ganzhou People’s Hospital (No. PJB2025-332-01;Approval date:23 September 2025). The study was conducted in accordance with the Declaration of Helsinki. Written informed consent to participate in this study was obtained from participants.
Funding
This study was supported by the Ganzhou Science and Technology Bureau (Technology + National Regional Medical Center) Joint Plan Project under the Key Research and Development Plan Key Project (Grant No. 2022-ZD1356).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rickward J, Hameed I, Ho S, et al. Day case laparoscopic cholecystectomy: a review of patient selection factors and identification of potential barriers to same-day discharge. ANZ J Surg. 2024;94(12):2119–10. doi:10.1111/ans.19241
2. Abuahmed M, Rashid R. Day-case laparoscopic cholecystectomy in the management of gallbladder disease: a literature review. Langenbecks Arch Surg. 2024;409(1):292. doi:10.1007/s00423-024-03479-6
3. Khalid A, Khalil K, Mehmood Qadri H, et al. Comparison of postoperative complications of open versus laparoscopic cholecystectomy according to the modified clavien-dindo classification system. Cureus. 2023;15(8):e43642. doi:10.7759/cureus.43642
4. Teng Y-H, Liu F-C, Liu K-H, et al. Incidence, patient-related risk factors, and outcomes of postoperative pneumonia after cholecystectomy: a population-based cohort study. Biomed Res Int. 2021;2021(1):6614885. doi:10.1155/2021/6614885
5. Sun Y, Guo K, Tang J, et al. Changes of respiratory microbiota associated with prognosis in pulmonary infection patients with invasive mechanical ventilation-supported respiratory failure. Ann Med. 2025;57(1):2514093. doi:10.1080/07853890.2025.2514093
6. Hajong R, Dhal MR, Newme K, et al. A cross sectional study of risk factors for surgical site infections after laparoscopic and open cholecystectomy in a tertiary care hospital in North East India. J Family Med Prim Care. 2021;10(1):339–342. doi:10.4103/jfmpc.jfmpc_1245_20
7. Wang S-H. Evaluating risk factors for surgical site infections and the effectiveness of prophylactic antibiotics in patients undergoing laparoscopic cholecystectomy. World J Gastrointest Surg. 2025;17(1):98567. doi:10.4240/wjgs.v17.i1.98567
8. Masaod RE, Salih MA. Prevalence and risk factors of post-cholecystectomy surgical site infections. Ann Med Surg Lond. 2023;85(11):5428–5432. doi:10.1097/MS9.0000000000001337
9. Ma S, Li F, Li J, et al. Risk factor analysis and nomogram prediction model construction of postoperative complications of thoracoscopic non-small cell lung cancer. J Thorac Dis. 2024;16(6):3655–3667. doi:10.21037/jtd-24-113
10. Li R, Xue M, Ma Z, et al. Construction and validation of a nomogram for predicting prolonged air leak after minimally invasive pulmonary resection. World J Surg Oncol. 2022;20(1):249. doi:10.1186/s12957-022-02716-w
11. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. doi:10.1016/j.ajic.2008.03.002
12. Liu D, Liu D, Jiang F, et al. A nomogram for predicting pulmonary complications following laparoscopic surgery in elderly patients after the COVID-19 pandemic. Clin Interv Aging. 2025;20:837–848. doi:10.2147/CIA.S515849
13. Tang D, Ge H, Tan Z, et al. The factors for the occurrence of pulmonary infection after gastrointestinal surgery and the construction of a predictive model using sTREM-1 and TIM-4: a retrospective study. Ann Ital Chir. 2024;95(3):299–307. doi:10.62713/aic.3362
14. Loncar Y, Tartrat N, Lastennet D, et al. Pulmonary infection after hepatic resection: associated factors and impact on outcomes. Clin Res Hepatol Gastroenterol. 2022;46(4):101733. doi:10.1016/j.clinre.2021.101733
15. Gamo GDO, Reichardt GS, Guetter CR, et al. Risk factors for surgical wound infection after elective laparoscopic cholecystectomy. Arq Bras Cir Dig. 2022;35:e1655. doi:10.1590/0102-672020210002e1655
16. Zhao C, Xiang B, Zhang J, et al. Predicting postoperative pulmonary infection risk in patients with diabetes using machine learning. Front Physiol. 2024;15:1501854. doi:10.3389/fphys.2024.1501854
17. Lan J, Liu X, Mo L, et al. Construction and validation of a risk prediction model for postoperative pulmonary infection in patients with brain tumor: a retrospective study. PeerJ. 2025;13:e18996. doi:10.7717/peerj.18996
18. Wang DE, Bakshi C, Sugiyama G, et al. Does operative time affect complication rate in laparoscopic cholecystectomy. Am Surg. 2023;89(11):4479–4484. doi:10.1177/00031348221117032
19. Li S, Su J, Sui Q, et al. A nomogram for predicting postoperative pulmonary infection in esophageal cancer patients. BMC Pulm Med. 2021;21(1):283. doi:10.1186/s12890-021-01656-7
20. Ari M, Haykir Solay A, Ozdemir T, et al. Neutrophil percentage-to-albumin ratio as a prognostic marker in pneumonia patients aged 80 and above in intensive care. J Clin Med. 2025;14(9):3033. doi:10.3390/jcm14093033
21. Aronen M, Viikari L, Langen H, et al. The long-term prognostic value of serum 25(OH)D, albumin, and LL-37 levels in acute respiratory diseases among older adults. BMC Geriatr. 2022;22(1):146. doi:10.1186/s12877-022-02836-8
22. Zhu B, Feng X, Jiang C, et al. Correlation between white blood cell count at admission and mortality in COVID-19 patients: a retrospective study. BMC Infect Dis. 2021;21(1):574. doi:10.1186/s12879-021-06277-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Model That Predicts the Risk of Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Yang J, Jiang S
International Journal of General Medicine 2022, 15:5089-5101
Published Date: 20 May 2022
Development of Risk Prediction Model for Muscular Calf Vein Thrombosis with Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Hu X, Li X, Xu H, Zheng W, Wang J, Wang W, Li S, Zhang N, Wang Y, Han K
International Journal of General Medicine 2022, 15:6549-6560
Published Date: 10 August 2022
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Wu C, Lu J, Ruan L, Yao J
Infection and Drug Resistance 2023, 16:1499-1509
Published Date: 15 March 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023