Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Revisiting Acute Exacerbations of Chronic Obstructive Pulmonary Disease: Insights from Applying the Rome Proposal in a North American Academic Hospital
Authors Saint-Pierre MD ![]() , Neder JA
, Neder JA
Received 3 April 2026
Accepted for publication 18 May 2026
Published 26 May 2026 Volume 2026:21 614290
DOI https://doi.org/10.2147/COPD.S614290
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Mathieu D Saint-Pierre,1 J Alberto Neder2
1Respirology, Montfort Hospital, University of Ottawa, Ottawa, ON, Canada; 2Respirology, Kingston Health Sciences Centre, Queen’s University, Kingston, ON, Canada
Correspondence: Mathieu D Saint-Pierre, Email [email protected]
Background: Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are traditionally classified by healthcare utilization, a framework that may not reflect physiologic severity. The 2021 Rome Proposal introduced objective criteria for grading AECOPD, but North American data, including emergency department (ED)–treated patients, are limited.
Research Questions: To determine the distribution of AECOPD severity using the Rome Proposal in a North American hospital cohort, characterize patients with mild events, and assess whether Rome-based grading predicts short-term readmissions among ED-treated patients.
Study Design and Methods: We conducted a retrospective cohort study of 481 patients treated for AECOPD in a large tertiary hospital in Ontario, Canada, between January 2022 and September 2024. Events were reclassified as mild, moderate, or severe as per the Rome Proposal criteria (modified Medical Research Council score ≥ 2 substituted for dyspnea visual analog scale). Clinical characteristics and 1- and 3-month hospital representation were analyzed.
Results: Overall, 49% of events were severe, 22% moderate, and 29% mild. Among hospitalized patients, 69% met criteria for severe AECOPD, whereas most ED-only events were mild (65%). Compared with moderate/severe events, mild events were associated with younger age, less home supplemental oxygen use, and higher mean forced expiratory volume in the first second. Among ED-treated patients, moderate/severe events were associated with significantly higher 3-month representation for AECOPD (31% versus 16%; mean 0.48 versus 0.18 visits per patient).
Interpretation: Application of the Rome Proposal criteria substantially reclassified AECOPD severity and demonstrated meaningful clinical and prognostic discrimination, particularly in ED-treated patients.
Keywords: chronic obstructive pulmonary disease, emergency department, hospitalization, Rome Proposal, severe acute exacerbations
Introduction
Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) represent a substantial burden on hospitals and are associated with significant morbidity and mortality.1,2 The Canadian Thoracic Society COPD pharmacotherapy guidelines and the Global Initiative for Chronic Obstructive Lung Disease recommendations both currently define AECOPD severity based on healthcare utilization, with events requiring an emergency department (ED) visit or hospitalization categorized as severe.3,4 This has major implications for overall COPD management, as experiencing at least one severe AECOPD in the preceding year places patients in the “high-risk” group, often requiring more intensive and costly therapies, more frequent follow-up with primary care providers (PCP), and referrals to specialists.
In this context, it should be acknowledged that grading AECOPD severity solely by healthcare utilization has important limitations. For instance, it does not account for differences in healthcare system structure, including variability in primary care access, emergency care models, and admission thresholds across regions and countries.5 Moreover, there may be substantial variability in patient perceptions of AECOPD, which could influence willingness to present to the ED.
In 2021, an international panel of COPD experts proposed the Rome criteria, which incorporate objectively measurable variables into the classification of AECOPD severity. Under the Rome Proposal, severe AECOPD is defined by evidence of acidotic hypercapnic respiratory failure (pH < 7.35 with PaCO2 > 45 mmHg). Moderate AECOPD necessitates the presence of at least three of the following five criteria: dyspnea visual analog scale (VAS) ≥ 5; respiratory rate ≥ 24 breaths per minute; heart rate ≥ 95 beats per minute; resting oxygen saturation < 92% and/or a decrease > 3% from baseline (when known); and C-reactive protein (CRP) ≥ 10 mg/L. Events with less than three of these criteria are classified as mild AECOPD.6 Studies from Europe and Asia have investigated how applying the Rome Proposal would impact the severity classification of AECOPD among admitted patients.7–11 Across these studies, only a minority of events—30% or fewer —met the Rome Proposal criteria for severe AECOPD. Importantly, the Rome Proposal criteria have been validated and are generally associated with worse clinical outcomes in patients with more severe AECOPD, including a higher risk of intensive care unit admission and mortality, supporting their prognostic value in clinical practice. However, it remains unclear how this reclassification would apply within a North American healthcare system. Furthermore, most prior studies have focused exclusively on inpatients, even though ED-treated AECOPD events are also categorized as severe under the current definition.
We therefore aimed to determine the proportion of patients treated for AECOPD in a Canadian hospital setting who would be classified as mild, moderate, or severe using the Rome Proposal. We hypothesized that a large proportion of patients would have non-severe AECOPD, implying that the mere criterion of ED treatment would have overestimated the severity of the event. We also sought to better characterize patients presenting to the hospital with events categorized as mild. In addition, we explored whether this novel objective grading system could help identify ED-treated patients at higher risk of AECOPD readmission after discharge.
Materials and Methods
Study Design and Setting
We conducted a retrospective cohort study of patients treated for AECOPD (ED or inpatient) at Montfort Hospital (Ottawa, Ontario, Canada) between January 2022 and September 2024. Montfort Hospital is an academic teaching hospital serving approximately 1.5 million people. Each patient’s medical record was reviewed to confirm that AECOPD was the most likely cause for presentation. The study was approved by the Montfort Hospital Research Ethics Board (file #22-23-02-052). Given the retrospective design, participant informed consent was waived. Data were anonymized and kept strictly confidential. All ethical principles set out in the Declaration of Helsinki were followed.
Data Collection and Variables
Hospital records were reviewed to extract data required for classification according to the Rome Proposal, including blood gas results, vital signs, symptoms, and CRP levels. As dyspnea VAS scores are not routinely performed in clinical practice, a modified Medical Research Council (mMRC) dyspnea scale ≥ 2 was used as a surrogate measure. Clinical variables collected included age, sex, and access to PCP. Cigarette smoking status, home supplemental oxygen use, prior spirometry results (when available), and baseline long-acting inhaled medications were also documented. Inpatient mortality and representation to the hospital for AECOPD within one and three months of discharge were charted.
Data Analysis and Statistical Methods
We first determined the proportion of AECOPD events classified as mild, moderate, or severe according to the Rome Proposal. Demographic and clinical characteristics were then compared between patients with mild events and those with moderate or severe events. Hospital representation within one and three months was subsequently reviewed according to the Rome Proposal classification. Student’s t-test was used for continuous variables and Pearson’s chi-squared test for categorical variables. Continuous results were presented as means with standard deviations, and categorical results as total numbers and percentages. Data distributions were visually assessed, and, given the large sample sizes, parametric tests were considered appropriate under the central limit theorem. Multivariate logistic regression analyses were performed to determine odds ratios with 95% confidence intervals. Covariates included in the multivariate models were age, sex, access to PCP, smoking status and history, home supplemental oxygen use, baseline inhaler therapy, and hospital representation. Statistical significance was defined as p < 0.05. Analyses were performed using IBM SPSS Statistics version 22 (Armonk, New York), and reporting followed STROBE guidelines for observational studies.
Results
Sample Characteristics
A total of 481 patients were treated for AECOPD during the study period. The mean age of the overall cohort was 70 years, and 231 patients (48%) were female. 375 individuals (78%) had access to PCP. 253 (53%) were active smokers, with a mean smoking history of 50 pack-years. 111 patients (23%) used home supplemental oxygen. Spirometry data were available for 195 subjects (41%); the mean forced expiratory volume in the first second (FEV1) was 49% predicted. At hospital presentation, 252 patients (52%) were prescribed inhaled maintenance triple therapy (Table 1). Sixteen subjects (3%) died in the hospital. Hospital representation for AECOPD occurred in 57 patients (12%) within one month of discharge and in 96 (21%) within three months.
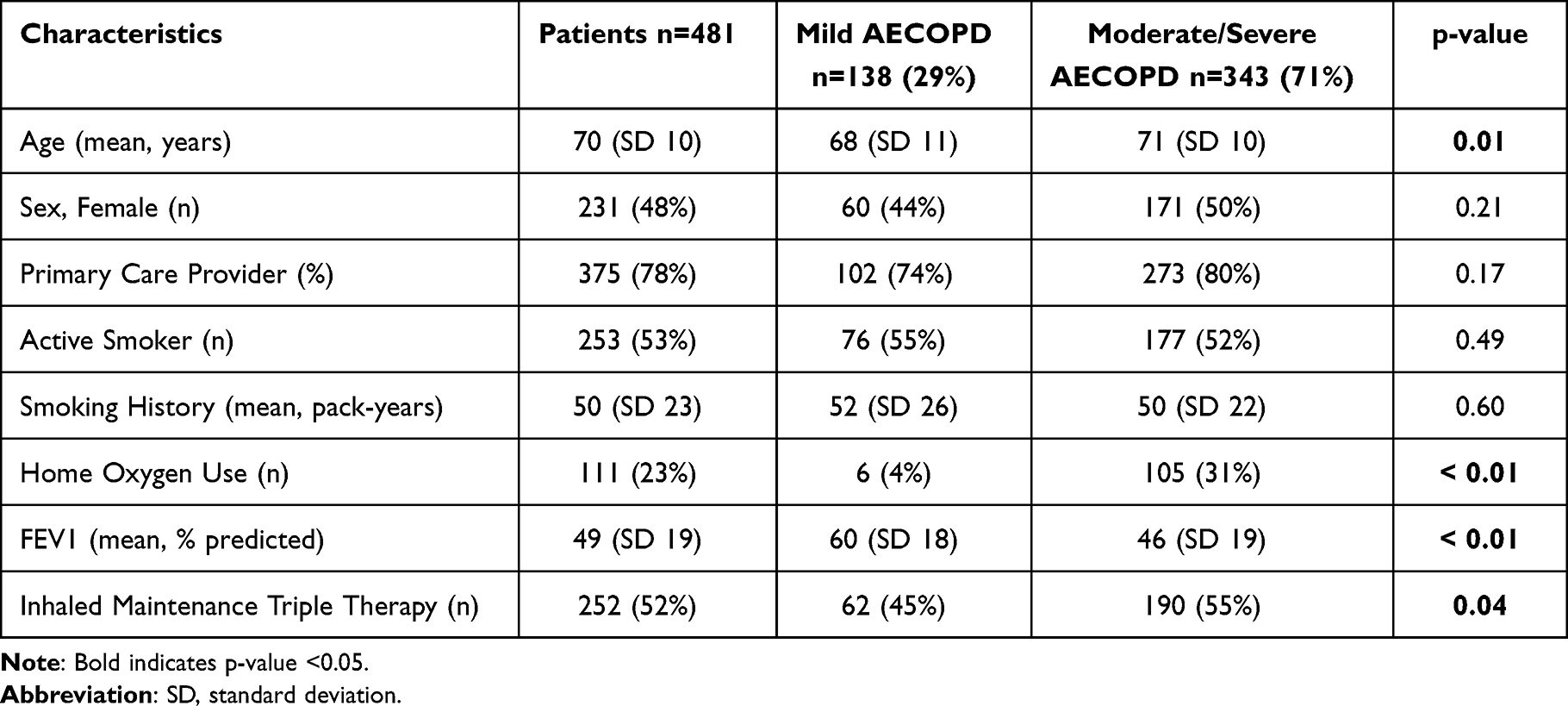 |
Table 1 Clinical Characteristics of AECOPD Patients According to Rome Proposal Criteria |
Severity of AECOPD
According to the Rome Proposal, 49% of events were classified as severe, 22% as moderate, and 29% as mild. 296 patients (62%) required inpatient admission. Among hospitalized patients, 69% met criteria for severe AECOPD. In contrast, among patients treated exclusively in the ED, most events (65%) were classified as mild (Table 2).
 |
Table 2 Distribution of AECOPD Severity According to the Rome Proposal Criteria |
Characteristics of Mild AECOPD
When stratified by Rome Proposal classification, patients with mild events differed significantly from those with moderate or severe events. Compared with the moderate/severe group, patients with mild AECOPD were younger, less likely to use home supplemental oxygen, and had higher mean % predicted FEV1 (Tables 1 and 3). Among patients treated exclusively in the ED, those with events classified as mild also had lower rates of home supplemental oxygen use and higher mean % predicted FEV1 (Tables 4 and 5).
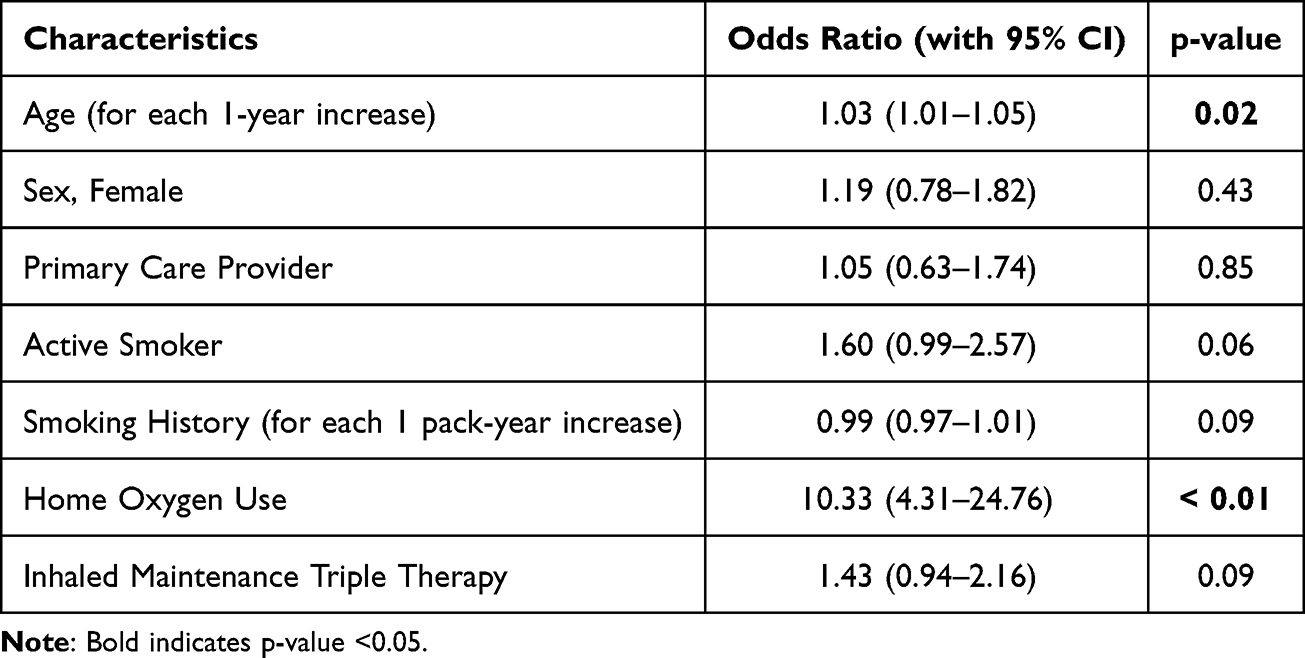 |
Table 3 Multivariate Logistic Regression Analysis of Clinical Characteristics in AECOPD Patients According to Rome Proposal Criteria (Moderate/Severe Versus Mild AECOPD) |
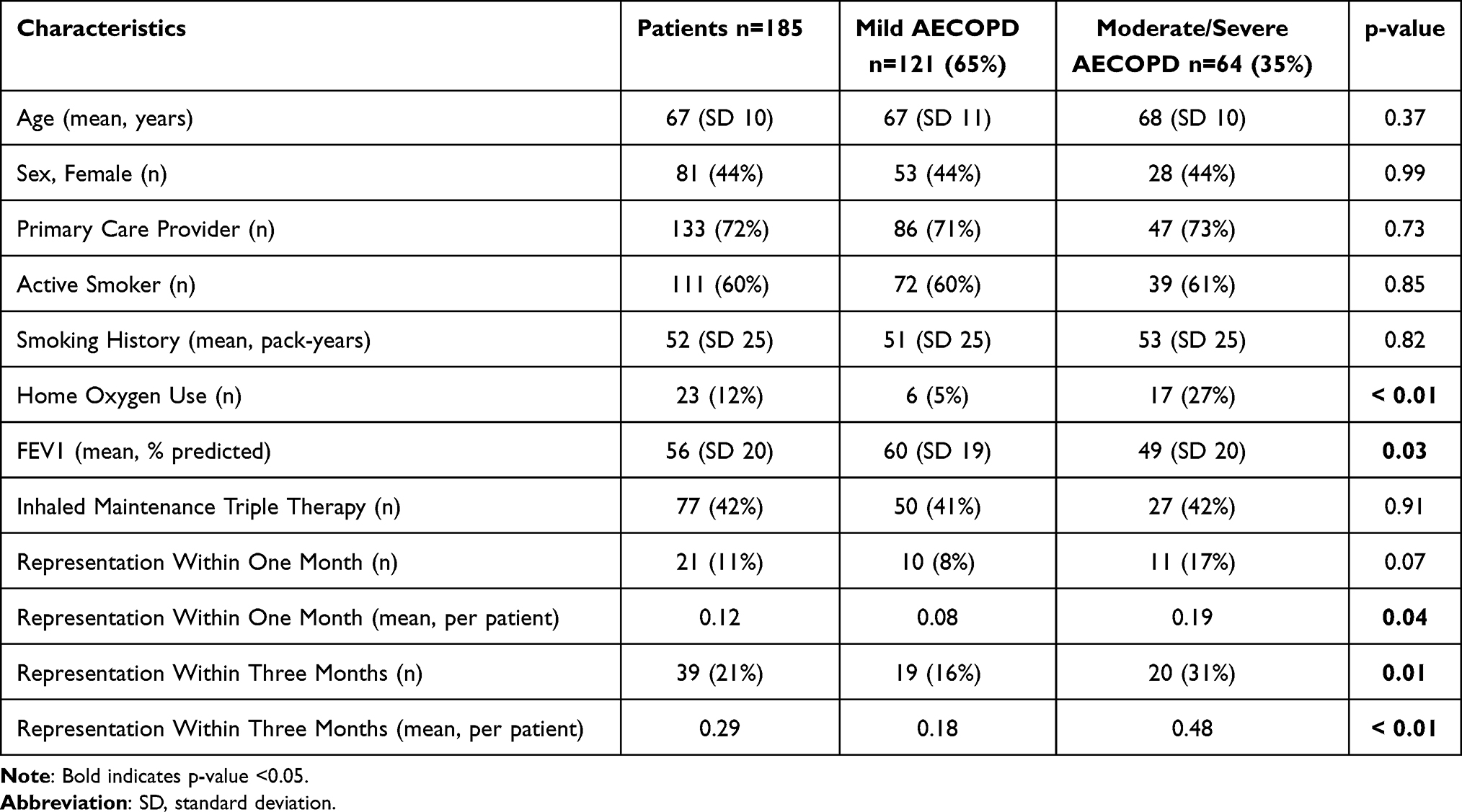 |
Table 4 Clinical Characteristics and Short-Term Hospital Representation in ED-Treated AECOPD Patients According to Rome Proposal Criteria |
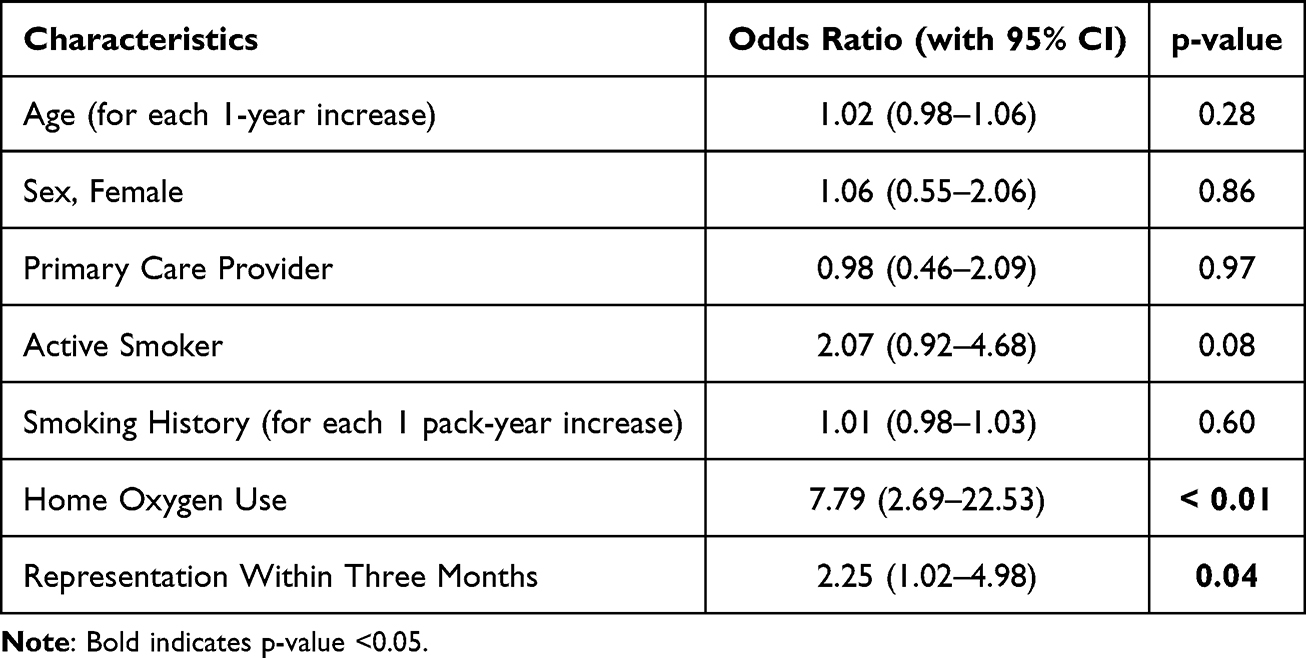 |
Table 5 Multivariate Logistic Regression Analysis of Clinical Characteristics and Short-Term Hospital Representation in ED-Treated AECOPD Patients According to Rome Proposal Criteria (Moderate/Severe Versus Mild AECOPD) |
Predicting Short-Term Readmissions in ED Patients
ED-treated subjects with moderate/severe events were more likely to present to the hospital for AECOPD within three months compared with those with mild events (31% versus 16%). A significant difference was observed in both univariate analysis and multivariate logistic regression analysis (Tables 4 and 5). They also had higher mean AECOPD visits per patient at one month and three months following discharge (Table 4).
Discussion
In this retrospective study of patients treated for AECOPD in a Canadian hospital setting, application of the Rome Proposal criteria resulted in substantial reclassification of event severity compared with the traditional healthcare utilization–based framework. Adoption of the Rome Proposal would therefore represent a major conceptual and practical shift in how AECOPD severity is defined. Transitioning from a utilization-based to a physiology-based system would significantly alter not only terminology, but also clinical decision-making and prognostication.
In our cohort, approximately half of the patients currently classified as having severe AECOPD would no longer meet criteria when the Rome Proposal was applied. This degree of reclassification is clinically meaningful. Our data showed clear clinical differences between patients with mild versus moderate/severe events according to the Rome Proposal, including age, home supplemental oxygen use, and baseline lung function. These findings suggest the Rome Proposal classification provides better clinical discrimination than a utilization-based model.
Compared with previously published cohorts, we observed a higher proportion of severe AECOPD events using the Rome Proposal.7–11 This discrepancy may reflect differences in healthcare organizations, hospital admission thresholds, and models of urgent care delivery. Variations in baseline disease burden as well as access to outpatient care may also contribute. Such geographic differences underscore a central limitation of a utilization-based definition and highlight the potential advantage of an objective, physiology-driven classification system.
An important methodological consideration relates to the dyspnea VAS, one of the Rome Proposal criteria. In routine North American practice, dyspnea VAS scoring is rarely performed. For this reason, we used a mMRC dyspnea score ≥ 2 as a more practical surrogate. While this approach increases real-world applicability, it also illustrates that some variables required for the Rome Proposal are not yet embedded in standard clinical care, including routine CRP measurement.
Our findings also revealed marked differences between admitted patients and those treated exclusively in the ED. Among hospitalized patients, most events met criteria for severe AECOPD under the Rome Proposal, whereas the majority of ED-only cases were classified as mild. Notably, ED-treated patients have not been systematically evaluated in prior Rome-based studies.7–11 Because the current Canadian Thoracic Society guidelines and Global Initiative for Chronic Obstructive Lung Disease recommendations define any ED visit as a severe event, our results raise an important question: should ED utilization alone continue to serve as a defining criterion of severe AECOPD?3,4 In healthcare systems with varying models of primary and urgent care, ED presentation may reflect structural factors rather than disease severity. A physiology-based grading system may therefore provide a more consistent framework across jurisdictions.
The subgroup of ED-only treated patients is particularly noteworthy. Within this population, moderate and severe events according to the Rome Proposal were associated with higher rates of short-term representation and greater mean AECOPD visits per patient following discharge. These findings suggest that objective grading may help identify ED patients at increased risk of treatment failure or early relapse. In this setting, the Rome Proposal could serve not only as a descriptor of event severity, but also as a risk stratification tool to guide ED management and discharge planning. While our findings are retrospective, they support the rationale for prospective studies assessing whether the Rome Proposal classification can guide targeted ED interventions. Importantly, objective severity grading should complement other key elements of high-quality ED care, including systematic optimization of maintenance inhaler therapy at the time of AECOPD.12,13
The Rome Proposal does not address the suspected mechanisms or drivers of AECOPD. In contrast, the recently proposed Baseline, Acuity, and trigger (BAt) model incorporates underlying disease severity alongside potential exacerbation triggers, which may improve the prediction of clinical outcomes. However, this model remains investigational and requires further validation and prospective evaluation before it can be adopted in routine clinical practice.14
This study has several limitations. Some patients may have sought care for subsequent AECOPD at other institutions after their initial presentation to Montfort Hospital. The study methodology prevented assessing for a history of AECOPD treated outside of the hospital setting. A minority of subjects had spirometry data on file, which prevented inclusion in the multivariate analyses. Lastly, this was a single-centre Canadian review, and the findings may not be generalizable to other North American hospitals.
Conclusion
Application of the Rome Proposal in a North American hospital cohort resulted in substantial reclassification of AECOPD severity and demonstrated meaningful clinical discrimination between mild and moderate/severe events. Among ED-treated patients, physiology-based grading identified individuals at higher risk of short-term representation. These findings support the potential value of an objective, physiology-driven framework.
Abbreviations
AECOPD, acute exacerbations of chronic obstructive pulmonary disease; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; ED, emergency department; FEV1, forced expiratory volume in the first second; mMRC, modified Medical Research Council; PCP, primary care providers; VAS, visual analog scale.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Montfort Hospital and Institut du Savoir Montfort.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Canadian Institute for Health Information. Inpatient Hospitalization Report, 2023-2024. Available from: https://www.cihi.ca/en/hospital-stays-in-canada-2023-2024.
2. Amegadzie JE, Lee TY, Sadatsafavi M, Lynd LD, Sin DD, Johnson KM. Trends in hospital admissions for chronic obstructive pulmonary disease over 16 years in Canada. Can Med Assoc J. 2023;195(35):E1172–7. doi:10.1503/cmaj.221051
3. Bourbeau J, Bhutani M, Hernandez P, et al. 2023 Canadian Thoracic Society guideline on pharmacotherapy in patients with stable COPD. Can J Respir Crit Care Sleep Med. 2023;7(4):173–191. doi:10.1080/24745332.2023.2231451
4. Global Initiative for Chronic Obstructive Lung Disease 2026 report. Available from: https://goldcopd.org/2026-gold-report-and-pocket-guide/.
5. Saint-Pierre MD. Severe acute exacerbations of chronic obstructive pulmonary disease: are there significant differences between hospitalized and emergency department patients?. Int J Chronic Obstruct Pulmon Dis. 2024;19:133–138.
6. Celli BR, Fabbri LM, Aaron SD, et al. An Updated Definition and Severity Classification of Chronic Obstructive Pulmonary Disease Exacerbations. Am J Respir Crit Care Med. 2021;204(11):1251–1258.
7. Amado Diago CA, Figueira Goncalves JM, Golpe R, et al. Classification of the severity of COPD exacerbations in hospitalized patients according to rome vs GesEPOC criteria. Archivos de Bronconeumología. 2023;59(1):57–58. doi:10.1016/j.arbres.2022.06.009
8. Crisafulli E, Sartori G, Huerta A, et al. Association between Rome classification among hospitalized patients with COPD exacerbations and short-term and intermediate-term outcomes. Chest. 2023;164(6):1422–1433. doi:10.1016/j.chest.2023.07.021
9. Reumkens C, Endres A, Simons SO, Savelkoul PHM, Sprooten RTM, Franssen FME. Application of the Rome severity classification of COPD exacerbations in a real-world cohort of hospitalised patients. ERJ Open Res. 2023;9(3):569. doi:10.1183/23120541.00569-2022
10. Zeng J, Zhou C, Yi Q, et al. Validation of the Rome severity classification of chronic obstructive pulmonary disease exacerbation: a multicenter cohort study. Int J Chronic Obstr. 2024;19:193–204. doi:10.2147/COPD.S442382
11. Baha A, Baysan C, Nayci SA, et al. Validation study of Rome criteria for assessing COPD exacerbation severity and predicting clinical outcomes: Turkish Thoracic Society COPD assembly. Int J Chronic Obstr. 2025;20:3993–4003. doi:10.2147/COPD.S554744
12. Saint-Pierre MD. Evaluating adherence to the 2023 Canadian Thoracic Society chronic obstructive pulmonary disease pharmacotherapy guidelines: a hospital-based study. Therap Adv Pulmon Crit Care Med. 2025;20. doi:10.1177/29768675251336660
13. Saint-Pierre MD, Chagnon N, Neder JA. Just the facts: management of patients with an acute exacerbation of chronic obstructive pulmonary disease in the emergency department. CJEM. 2026;28(3):179–182. doi:10.1007/s43678-025-01050-w
14. Aung HWW, Vermeersch K, McAuley HJC, et al. Multidimensional prognostic risk stratification of COPD exacerbations: the baseline, acuity, and trigger (BAt) model. Lancet Respir Med. 2026;14:174–186. doi:10.1016/S2213-2600(25)00362-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Emergency Department Visits Due to Dyspnea: Association with Inhalation Therapy in COPD and Cases with Adverse Drug Reactions
Bergs I, Just KS, Müller A, Stingl JC, Dreher M
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1827-1834
Published Date: 11 August 2022
Comorbid Heart Disease in Patients with COPD is Associated with Increased Hospitalization and Mortality – A 15-Year Follow-Up
Giezeman M, Sundh J, Athlin Å, Lisspers K, Ställberg B, Janson C, Montgomery S, Kisiel MA, Nager A, Sandelowsky H, Hasselgren M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:11-21
Published Date: 9 January 2023
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:881-893
Published Date: 15 May 2023
Clinical Characteristics and Medical Utilization of Smokers with Preserved Ratio Impaired Spirometry
Shin YY, Park S, Kim KJ, Rhee CK, Yoo KH, Jung KS, Lee JH
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2187-2194
Published Date: 6 October 2023