Back to Journals » Journal of Inflammation Research » Volume 19
Renal Complement C3 Deposition is Associated with Glomerular Prothrombotic Milieu in Patients with IgA Nephropathy
Authors Guo Y, Zheng S ![]() , Li S, Ye Z
, Li S, Ye Z ![]() , Luo M, Liu H
, Luo M, Liu H
Received 10 April 2026
Accepted for publication 25 June 2026
Published 3 July 2026 Volume 2026:19 611287
DOI https://doi.org/10.2147/JIR.S611287
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wenjian Li
Yun Guo, Siqi Zheng, Shangmei Li, Zhennan Ye, Mianna Luo,* Huafeng Liu*
Department of Nephrology, National Clinical Key Specialty Construction Program (2023); Institute of Nephrology; Guangdong Provincial Key Laboratory of Autophagy and Major Chronic Non-Communicable Diseases; Key Laboratory of Prevention and Management of Chronic Kidney Disease of Zhanjiang City; Affiliated Hospital of Guangdong Medical University, Zhanjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mianna Luo, Department of Nephrology, Affiliated Hospital of Guangdong Medical University, No. 57, Renmin Avenue South, Xiashan District, Zhanjiang, Guangdong Province, 524001, People’s Republic of China, Tel +860759 2387583, Email [email protected]; Huafeng Liu, Department of Nephrology, Affiliated Hospital of Guangdong Medical University, No. 57, Renmin Avenue South, Xiashan District, Zhanjiang, Guangdong Province, 524001, People’s Republic of China, Tel +860759 2387583, Email [email protected]
Introduction: Complement activation plays a central role in the pathogenesis of IgA nephropathy (IgAN); however, not all patients exhibit renal C3 deposition. Accumulating evidence suggests that complement activation is closely linked to coagulation activation and prothrombotic cellular responses.
Methods: This retrospective study was conducted using clinical and laboratory data obtained from the institutional clinical database of the Affiliated Hospital of Guangdong Medical University. This study investigated the association between renal C3 deposition and an intraglomerular prothrombotic milieu in 890 biopsy-proven IgAN patients categorized by C3 deposition status. Histological glomerular prothrombotic lesions reflecting a prothrombotic milieu were defined by pathological features, including intraglomerular erythrocyte aggregation and/or glomerular capillary microthrombus-like lesions. The primary outcome was a composite of a ≥ 30% decline in eGFR from baseline or kidney failure, defined as initiation of maintenance dialysis, kidney transplantation, or eGFR ≤ 15 mL/min/1.73 m2. Firth’s penalized logistic regression was used to assess associations with histological glomerular prothrombotic lesions, and Cox proportional hazards regression was used to evaluate renal outcomes; cumulative incidence curves were generated using the survival and survminer packages in R.
Results: Among 890 patients, 852 (95.7%) exhibited C3 deposition and 38 (4.3%) did not; 324 patients experienced histological glomerular prothrombotic lesions indicative of an intraglomerular prothrombotic milieu. In multivariable analyses, glomerular C3 deposition remained independently associated with histological glomerular prothrombotic lesions (OR 8.22, 95% CI 2.01– 75.72, P = 0.001). During follow-up, 110 patients reached the primary outcome. In unadjusted Cox analysis, renal C3 deposition was associated with a lower risk of the composite outcome (HR 0.53, 95% CI 0.28– 0.99, P = 0.048); however, this association was attenuated and no longer significant after sequential adjustment for clinical variables, pathological lesions, and treatment (fully adjusted HR 0.86, 95% CI 0.35– 2.11, P = 0.74).
Conclusion: Renal C3 deposition is associated with intraglomerular coagulation abnormalities and a heightened prothrombotic milieu in IgAN. Although an apparent association with better renal outcomes was observed in unadjusted analysis, renal C3 deposition was not independently associated with long-term renal prognosis after adjustment for potential confounders.
Keywords: IgA nephropathy, complement C3, prothrombotic milieu, prognosis
Introduction
IgAN is the most common primary glomerulonephritis worldwide and is characterized by mesangial IgA deposition with heterogeneous clinical presentation and prognosis.1 Several advances in IgAN research have elucidated the underlying disease pathogenesis, which is commonly conceptualized as a four-hit model. This model involves the gut microbiota exerts an excessive stimulatory effect on mucosal innate immune cells, which in turn hyperactivates mucosal B cells. This excessive activation prompts mucosal B cells to produce substantial quantities of galactose-deficient IgA1 (Gd-IgA1), a key pathogenic molecule that subsequently enters the systemic circulation. Within the bone marrow, the immune system generates IgG, IgA, and IgM antibodies that target Gd-IgA1, laying the groundwork for subsequent pathogenic events. Anti-Gd-IgA1 autoantibodies bind Gd-IgA1 to form immune complexes. These immune complexes are then transported through the vascular system to the kidneys. These complexes deposit preferentially in the renal mesangium, where Gd-IgA1 immune complex accumulation triggers mesangial cell activation and proliferation, with subsequent release of pro-inflammatory and pro-fibrotic cytokines.2,3
Complement activation plays a central role in the pathogenesis of IgAN. C1q is seldom detected in IgAN, involvement of the classical complement pathway is considered minimal. In contrast, multiple lines of evidence support a prominent role for activation of the alternative and/or lectin complement pathways.4 Despite distinct initiating mechanisms, the classical, alternative, and lectin pathways all converge at the proteolytic activation of C3, the most abundant complement component in circulation.5 As a result, C3 serves as the central effector of the complement system, exerting its diverse functions through distinct binding sites and their corresponding receptors.6 Not all patients with IgA nephropathy exhibit C3 deposition, although previous studies have reported its presence in over 90% of cases.7
Growing evidence indicates that complement activation and coagulation are closely interconnected.8 C3 activation products can promote platelet activation and fibrin formation, thereby contributing to a prothrombotic microvascular environment.9,10 In kidney diseases, terminal complement activation may promote a prothrombotic endothelial environment in membranous nephropathy.11 Histological glomerular prothrombotic lesions may reflect local microcirculatory disturbance. Within the glomerular microcirculation, these prothrombotic lesions changes could potentially contribute to microvascular obstruction and glomerular injury. However, a critical knowledge gap remains: whether glomerular C3 deposition is linked to intraglomerular prothrombotic milieu in IgAN has not been systematically explored. Therefore, the primary objective of this study was to investigate the association between renal C3 deposition and intraglomerular prothrombotic milieu in patients with IgAN.
Methods
Study Population
Clinical and laboratory data were retrospectively obtained from the institutional clinical database. The investigators had access to de-identified clinical and laboratory data from the institutional clinical database used to identify eligible patients and extract study variables. This study was conducted and reported in accordance with the RECORD (Reporting of studies Conducted using Observational Routinely-collected Data) guidelines. A total of 1077 patients with biopsy-proven IgAN who underwent renal biopsy at the Department of Nephrology, Affiliated Hospital of Guangdong Medical University between January 2009 and June 2025 were retrospectively screened. Exclusion criteria included age <14 years, eGFR ≤ 30 mL/min/1.73 m2 at the time of biopsy, missing serum creatinine or renal C3 deposition data, and the presence of other glomerulonephritis. Based on these criteria, 187 patients were excluded. The selection process is illustrated in Figure 1. The remaining patients were classified into a renal C3 deposition-positive group (n = 852) and a renal C3 deposition-negative group (n = 38).
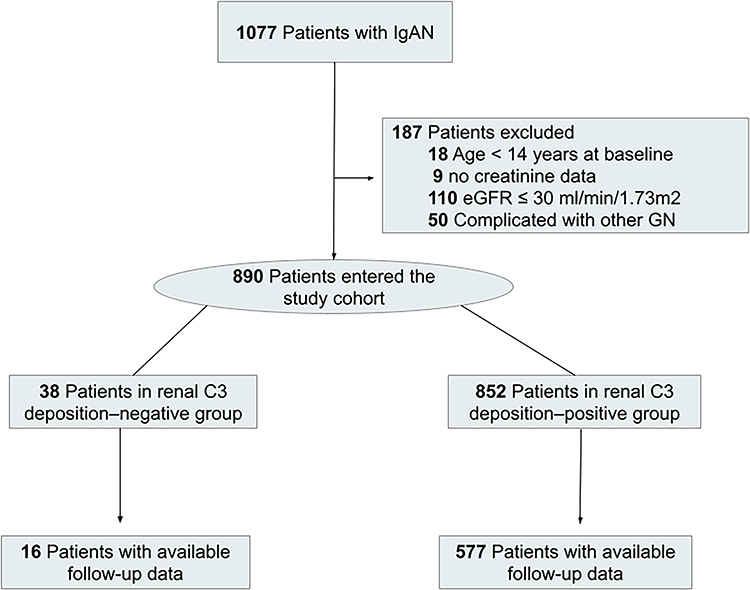 |
Figure 1 Flow charts of the study. |
This retrospective study was conducted in accordance with the Declaration of Helsinki. The study protocol was reviewed and approved by the Ethics Committee of the Affiliated Hospital of Guangdong Medical University (Approval Number: PJKT2026-111; Acceptance Number: KT2026-111-01).
Baseline Clinical and Pathological Characteristics
Baseline clinical and laboratory data were retrospectively retrieved from the institutional clinical database at the time of renal biopsy. The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation.12 Renal pathological features were evaluated according to the Oxford MEST classification for IgA nephropathy, including mesangial hypercellularity (M), endocapillary hypercellularity (E), segmental sclerosis (S), and interstitial fibrosis/tubular atrophy (T), based on renal biopsy findings.13 Analyses of individual MEST components were based on available pathological data, and the corresponding denominators are reported in Table 1. The crescent score (C) was not included in the analyses because it was unavailable for a substantial proportion of patients, many of whom underwent renal biopsy before the 2017 update of the Oxford MEST-C classification.14 Renal complement C3 deposition was evaluated using immunofluorescence analysis on frozen tissue sections, and representative histopathological images are shown in Figure 2. Mesangial C3 staining intensity was semi-quantitatively graded as negative, weak positive, 1+, 2+, 3+, or 4+ according to routine pathological evaluation. Any detectable mesangial C3 staining, including weak positive staining, was classified as C3-positive, whereas the absence of detectable mesangial C3 staining was classified as C3-negative. In this study, the classification was based on mesangial C3 deposition, and glomerular capillary wall staining patterns were not analyzed separately.
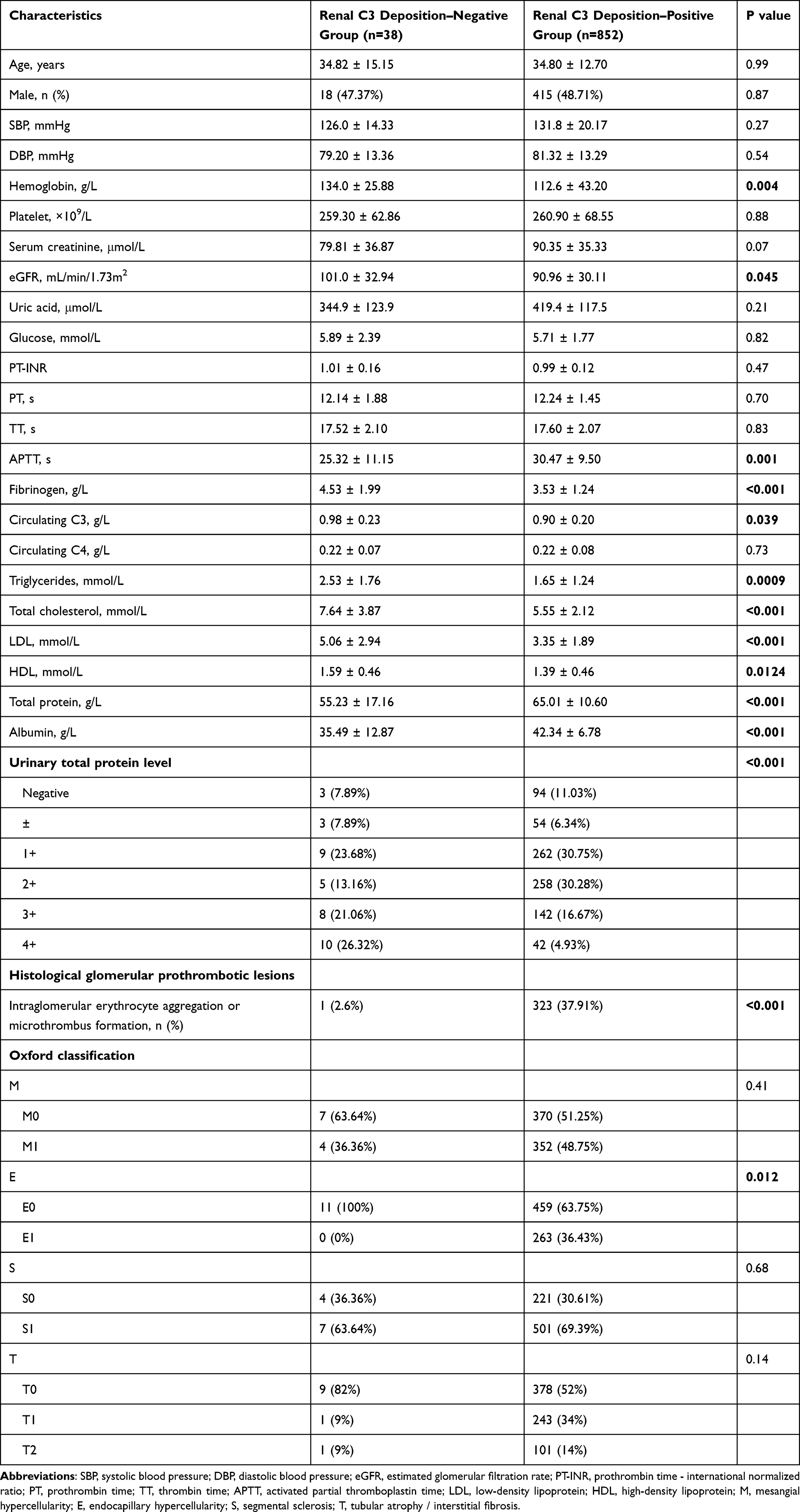 |
Table 1 Baseline Characteristics of Patients with Immunoglobulin A Nephropathy Stratified by Renal Complement C3 Deposition |
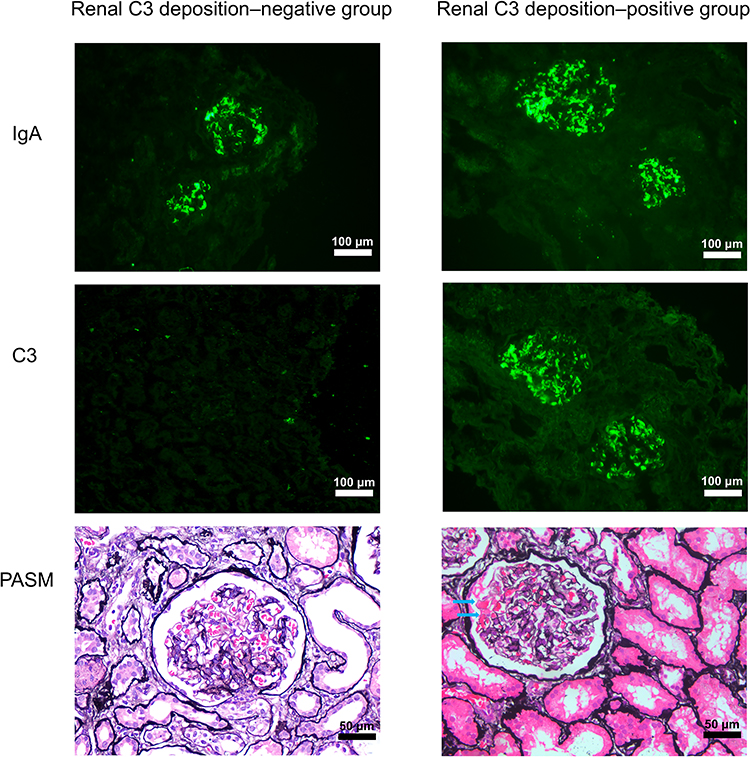 |
Figure 2 Representative renal pathological features in IgA nephropathy stratified by C3 deposition status. Immunofluorescence images demonstrate glomerular IgA deposition (upper panels) in both the renal C3 deposition-negative and C3 deposition-positive groups, whereas glomerular C3 deposition (middle panels) is observed only in the C3-positive group. The lower PASM-stained panels show representative erythrocyte-rich microthrombus-like lesions within glomerular capillary loops, as indicated by the arrows. The immunofluorescence images were acquired at ×200 magnification (scale bars = 100 μm), whereas the PASM-stained images were acquired at ×400 magnification (scale bars = 50 μm). |
Histological Glomerular Prothrombotic Lesions Evaluation
Histological glomerular prothrombotic lesions of interest were defined as pathological features reflective of a prothrombotic milieu, including intraglomerular erythrocyte aggregation and/or glomerular capillary microthrombus-like lesions. Glomerular prothrombotic lesions were evaluated independently by two experienced renal pathologists who were blinded to clinical information. Intraglomerular erythrocyte aggregation was defined as dense clustering of erythrocytes within glomerular capillary lumina involving one or more capillary loops. Microthrombus-like lesions were defined as compact intraluminal erythrocyte-rich partial or complete occlusion of glomerular capillary lumina. These lesions were distinguished from simple capillary congestion by the presence of dense erythrocyte accumulation with luminal narrowing or occlusion, rather than passive capillary engorgement. Cases showing only scattered erythrocytes within capillary lumina without aggregation or luminal obstruction were not considered positive. Erythrocytes located outside the capillary lumina or changes compatible with nonspecific hematuria-related leakage were also not classified as glomerular prothrombotic lesions. Potential tissue-processing artifacts were excluded by assessing the overall glomerular architecture and excluding lesions associated with section distortion, folding artifacts, or tissue disruption. Representative pathological images are presented in Figure 2. Renal C3 deposition was treated as a binary variable (positive vs. negative) based on renal biopsy findings. These features were evaluated primarily by light microscopy. All samples were independently reviewed by experienced renal pathologists blinded to clinical information. Discrepant cases were resolved by joint review and consensus.
Renal Outcomes
The primary outcome was a composite of a ≥30% decline in eGFR from baseline or kidney failure, defined as initiation of maintenance dialysis, kidney transplantation, or eGFR ≤15 mL/min/1.73 m2. Follow-up data were obtained from outpatient visits, inpatient records, and laboratory databases. The follow-up period was calculated from the date of renal biopsy to the occurrence of the primary composite renal outcome or the last available clinical assessment. Patients without an endpoint event were censored at their last recorded follow-up visit. Missing data were handled using complete-case analysis because the proportion of missing values was minimal.
Statistical Methods and Analysis
Prior to analysis, the data was screened for completeness and consistency, and data cleaning procedures were performed to identify missing values, outliers, and potential data entry errors. Continuous variables are presented as mean (standard deviation, SD) or median (interquartile range, IQR), whereas categorical variables are expressed as counts and percentages. Differences between groups were assessed using the t test or Mann–Whitney U-test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables, as appropriate.
Given the low frequency of histological glomerular prothrombotic lesions, Firth’s penalized logistic regression was applied to minimize small-sample bias in the estimation of odds ratios.15 Subgroup analyses were additionally performed to assess potential effect modification, stratified by age, serum albumin, and baseline eGFR. These variables were selected a priori based on their clinical relevance and potential influence on coagulation status and renal microvascular injury. Time-to-event analyses were performed, and cumulative incidence curves for the composite outcome were generated using the survival and survminer packages in R (version 4.3.3). The association between renal C3 deposition and the primary composite outcome was further evaluated using Cox proportional hazards regression models. Sequential Cox models were constructed, including an unadjusted model, a clinical model adjusted for baseline eGFR, proteinuria, systolic blood pressure, and diastolic blood pressure, a clinical plus pathology model additionally adjusted for Oxford MEST lesions, and a fully adjusted model additionally adjusted for treatment. Treatment variables included kidney-protective therapy, defined as the use of a renin-angiotensin system inhibitor, mineralocorticoid receptor antagonist, or sodium-glucose cotransporter 2 inhibitor, as well as corticosteroid or immunosuppressive therapy. All Cox regression analyses were performed using the survival package in R (version 4.3.3). All statistical tests were two-sided, and a P value < 0.05 was considered statistically significant.
Results
Baseline Characteristics of the Study Population
A total of 1077 patients with IgAN were identified during the study period. After applying the predefined exclusion criteria, 890 patients were included in the final analysis, of whom 852 showed renal complement C3 deposition and 38 had no evidence of renal C3 deposition (Figure 1). Among the 852 C3-positive patients, staining intensity was weakly positive in 29 (3.4%), 1+ in 244 (28.6%), 2+ in 409 (48.0%), 3+ in 154 (18.1%), and 4+ in 16 (1.9%). The mean (SD) age of the study population was 3513 years, and the mean (SD) eGFR was 91.39 (30.28) mL/min/1.73 m2. Baseline characteristics stratified by renal C3 deposition status are presented in Table 1. Compared with patients without renal C3 deposition, those with C3 deposition had significantly lower hemoglobin levels and lower eGFR. Furthermore, the C3-positive group exhibited prolonged activated partial thromboplastin time (APTT), reduced fibrinogen levels, and lower serum C3 concentrations.
Histological Glomerular Prothrombotic Lesions
Histological glomerular prothrombotic lesions were identified in 324 patients overall. The prevalence of histological glomerular prothrombotic lesions was significantly higher in patients with C3 deposition than in those without C3 deposition (37.91% vs. 2.6%, P < 0.0001). In addition, endocapillary hypercellularity was more frequently observed in patients with positive renal C3 deposition (36.4%).
Impact of Glomerular C3 Deposition on Histological Glomerular Prothrombotic Lesions
Among the 852 patients with positive glomerular C3 deposition, 323 (37.91%) patients presented with glomerular RBC aggregation or glomerular capillary microthrombus-like lesions on renal biopsy. In contrast, 1 of the 38 patients (2.6%) without glomerular C3 deposition exhibited RBC aggregation or microthrombus in kidney.
Given the low event frequency in the C3 deposition–negative group, Firth’s penalized logistic regression was applied. Univariable Firth logistic regression analysis was performed to identify factors associated with histological glomerular prothrombotic lesions (Table 2). Glomerular C3 deposition was strongly associated with histological glomerular prothrombotic lesions (odds ratio [OR], 15.27; 95% confidence interval [CI], 4.06–136.01; P < 0.001). In addition, male sex was associated with a higher risk of histological glomerular prothrombotic lesions (OR, 1.40; 95% CI, 1.07–1.84; P = 0.02). Several hematologic and coagulation-related parameters were also significantly associated with histological glomerular prothrombotic lesions, including hemoglobin level, platelet count, prothrombin time, activated partial thromboplastin time, fibrinogen level, and serum albumin (all P < 0.05).
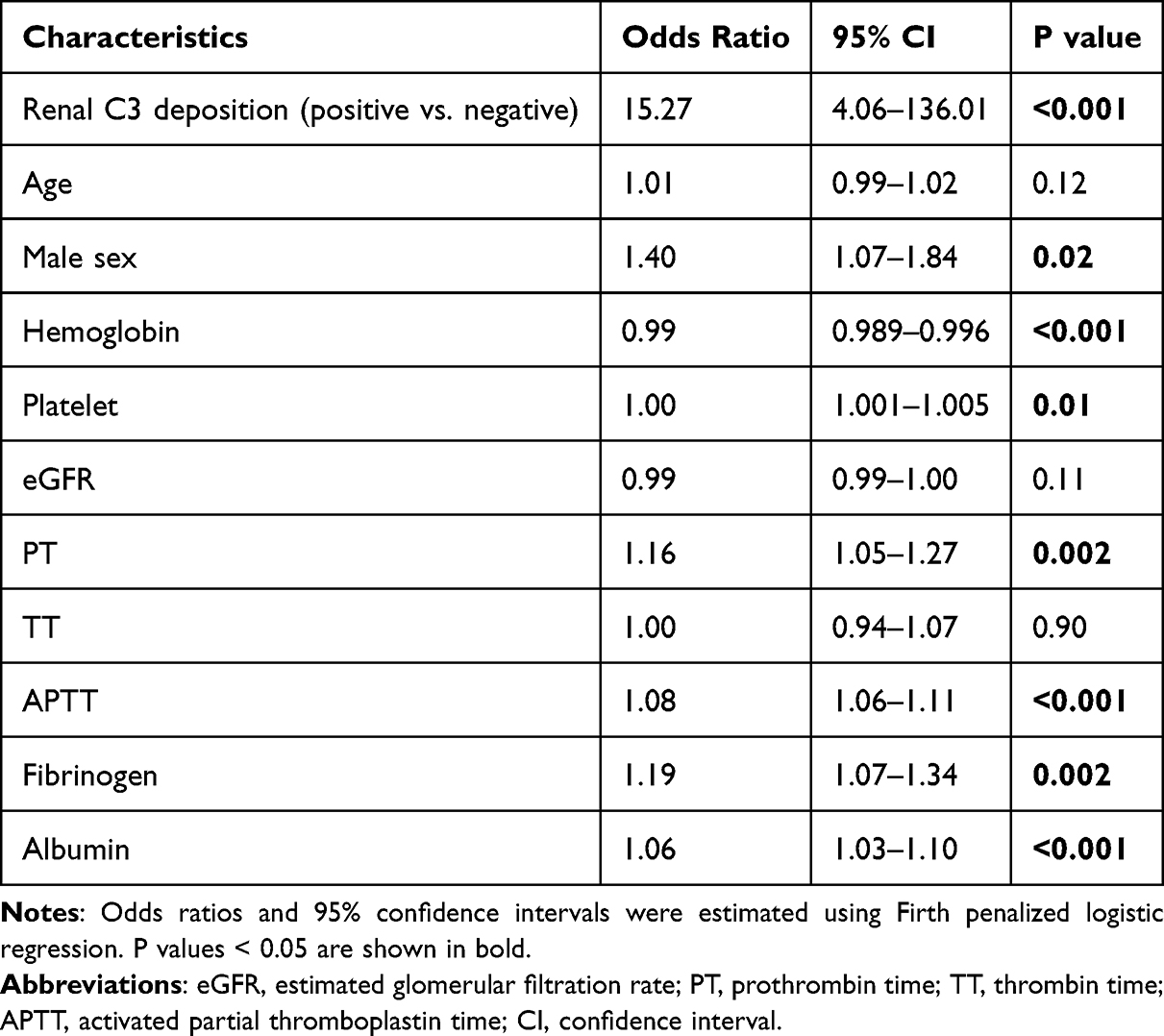 |
Table 2 Univariable Firth Logistic Regression Analysis for Histological Glomerular Prothrombotic Lesions |
To further determine whether glomerular C3 deposition was independently associated with histological glomerular prothrombotic lesions, a multivariable Firth logistic regression model was constructed adjusting for clinically relevant demographic, hematological, and coagulation-related variables (Table 3). In the multivariable analysis, glomerular C3 deposition remained independently and significantly associated with histological glomerular prothrombotic lesions (OR 7.07, 95% CI 1.74–64.79, P = 0.003).
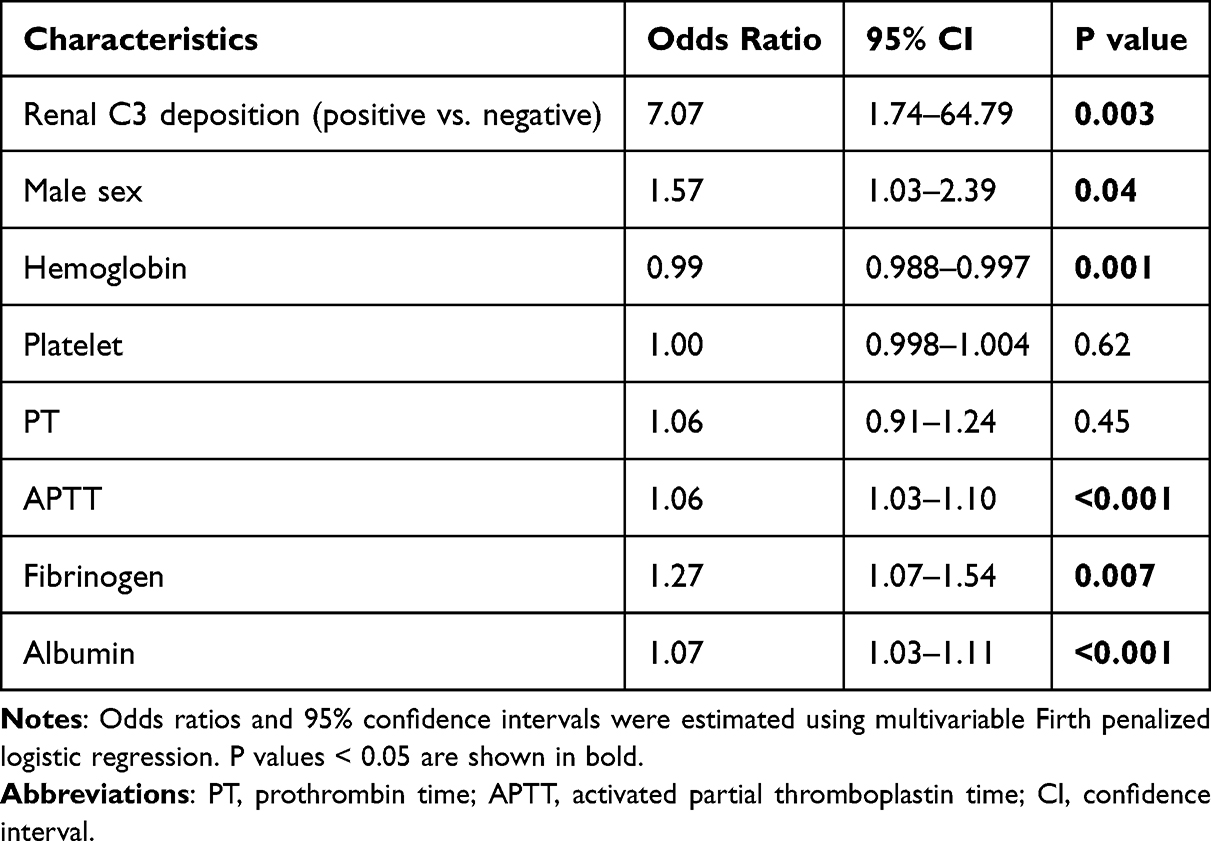 |
Table 3 Multivariable Firth Logistic Regression Analysis for Histological Glomerular Prothrombotic Lesions |
Subgroup Analyses
To assess whether the association between glomerular C3 deposition and histological glomerular prothrombotic lesions differed across clinical strata, subgroup analyses were performed according to age, serum albumin, and baseline eGFR (Figure 3). Glomerular C3 deposition was associated with histological glomerular prothrombotic lesions in both younger (<35 years, OR 10.42, 95% CI 1.31–1347.11, P = 0.021) and older patients (≥35 years, OR 6.48, 95% CI 1.54–59.90, P = 0.008), with no significant interaction by age (P for interaction = 0.786). Similarly, patients with higher albumin levels (≥30 g/L, OR 9.97, 95% CI 2.52–90.44, P = 0.0002) and those with lower albumin (<30 g/L, OR 4.14, 95% CI 0.38–572.01, P = 0.283) both showed associations, with no significant interaction (P = 0.653). Stratification by renal function indicated a stronger association in patients with eGFR ≥60 mL/min/1.73 m2 (OR 27.58, 95% CI 3.70–3526.70, P < 0.001) than in those with eGFR <60 (OR 1.62, 95% CI 0.25–17.31, P = 0.623), and the interaction was non-significant (P = 0.071).
 |
Figure 3 Subgroup analysis of the association between glomerular C3 deposition and histological glomerular prothrombotic lesions. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated using Firth’s penalized logistic regression within predefined subgroups according to age, serum albumin (Alb), and baseline estimated glomerular filtration rate (eGFR). The vertical dashed line indicates an OR of 1, and the horizontal lines represent the corresponding 95% CIs. ns, P ≥ 0.05; *P < 0.05; **P < 0.01; ***P < 0.001. |
The Effect of Glomerular C3 Deposition on the Primary Composite Outcome
During a median follow-up time of 55 months (IQR: 26–85 months), the cohort observed 110 primary composite outcome events. Among these, 99 (90%) occurred in the renal C3 deposition positive group, while 11 (10%) were observed in the renal C3 deposition negative group (Figures 4 and 5). When the C3 deposition–negative group was used as the reference, renal C3 deposition was significantly associated with the primary composite outcome (HR 0.53, 95% confidence interval 0.28–0.99, P = 0.048). Consistently, renal C3 deposition was associated with a reduced hazard of ≥30% decline in eGFR (HR 0.51, 95% CI 0.27–0.97, P = 0.039). Sensitivity analyses were then performed using sequential Cox regression models with increasing levels of adjustment (Table 4). The association was attenuated and became non-significant after adjustment for baseline clinical variables (HR 0.85, 95% CI 0.39–1.82, P = 0.67), pathological variables including Oxford MEST lesions (HR 0.84, 95% CI 0.34–2.07, P = 0.70), and treatment information (HR 0.86, 95% CI 0.35–2.11, P = 0.74).
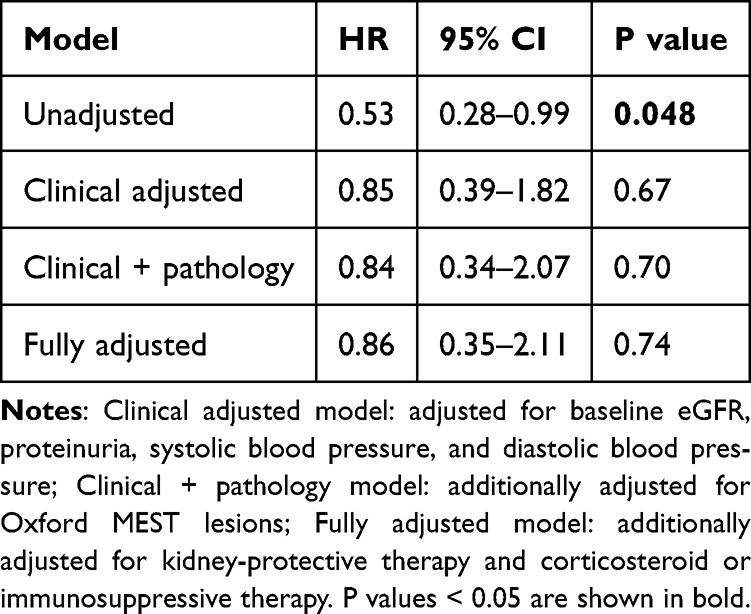 |
Table 4 Sequential Multivariable Cox Regression Analyses of the Association Between Renal C3 Deposition and the Primary Composite Outcome |
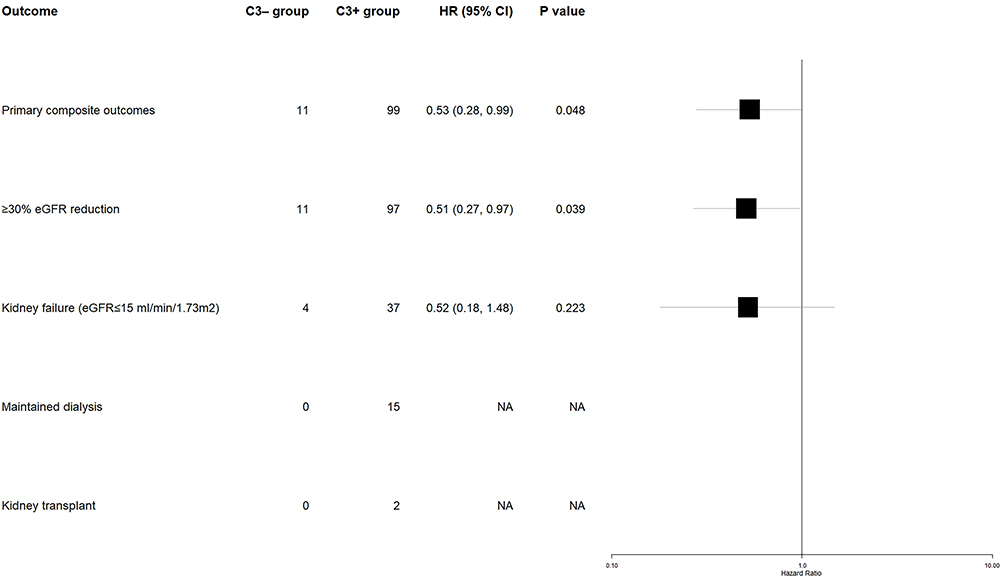 |
Figure 4 Comparison of renal outcomes between IgAN patients without renal complement C3 deposition group (C3- group) and with renal complement C3 deposition group (C3+ group). The forest plot presents the hazard ratios for renal outcomes. Boxes denote the hazard ratios, and horizontal lines represent the corresponding 95% confidence intervals. |
 |
Figure 5 The cumulative incidence of the primary composite outcome. The median follow-up was 55 months. The hazard ratio for the primary outcome in the C3+ group compared to the C3- group was 0.53 (95% CI:0.28–0.99), with a p value of 0.048; C3+ group, IgAN patients with renal complement C3 deposition group; C3- group, IgAN patients without renal complement C3 deposition group. |
Discussion
In a previous study, we reported that hepatitis B virus (HBV) antigen deposition in the kidney was associated with renal prognosis in patients with IgA nephropathy.16 However, that study primarily focused on HBV antigen deposition status. The present study investigates a distinct biological pathway by examining the relationship between renal complement C3 deposition, intraglomerular prothrombotic features, and renal outcomes in a larger cohort of biopsy-proven IgAN patients. Although both studies were derived from the same institutional database, the research questions and exposures examined are different. In this study of patients with biopsy-proven IgA nephropathy, renal C3 deposition was detected in 95.73% of patients, which is consistent with the prevalence reported in prior literature.17,18 Compared with the renal C3 deposition–negative group, patients with positive C3 deposition exhibited a markedly higher prevalence of histological glomerular prothrombotic lesions. In addition, circulating C3 levels were significantly reduced, accompanied by prolonged APTT and decreased fibrinogen levels. In a vivo study, the C3a/C3aR axis on platelet were identified to regulate distinct steps of thrombus formation such as platelet adhesion, spreading, and Ca2+ influx.9 Previous studies found that C3−/− mice displayed reduced thrombus burden and platelet activation, which indicated that C3 activation independently contributes to platelet activation and fibrin formation.10 Collectively, these observations support a potential link between renal C3 deposition and histological glomerular prothrombotic lesions, which in this study was defined by the presence of intraglomerular erythrocyte aggregation or microthrombus formation on renal pathology.
To further explore the relationship between glomerular C3 deposition and histological glomerular prothrombotic lesions, Firth’s penalized logistic regression was applied, which reduces potential small-sample bias associated with low event rates. C3 deposition showed the strongest association in univariable analysis and remained significantly associated after adjustment for other relevant variables. These findings suggest that glomerular C3 deposition may represent an independent factor associated with histological glomerular prothrombotic lesions in IgA nephropathy. To assess whether the association between glomerular C3 deposition and histological glomerular prothrombotic lesions differed across clinical subgroups, stratified analyses were performed according to age, eGFR, and serum albumin levels. Sex was not included in the subgroup analysis because histological glomerular prothrombotic lesions were extremely imbalanced between sexes. The association between C3 deposition and histological glomerular prothrombotic lesions was consistently observed across all subgroups, suggesting that this relationship was not substantially modified by these clinical characteristics. Increasing evidence supports a close interplay between complement activation and thrombosis in kidney diseases. In membranous nephropathy, terminal complement activation leads to excessive C5b-9 deposition, which not only mediates tissue injury but also promotes a prothrombotic environment by inducing platelet microparticle formation and endothelial vesiculation, thereby facilitating prothrombinase assembly.11,19 In parallel, C5b-9–mediated calcium influx may further enhance platelet activation and coagulation activity.20 In IgA nephropathy, a previous study reported that patients with arteriolar microangiopathic lesions exhibited extensive deposition of complement activation products on arterioles, with more than 90% of patients showing C3d and C5b-9 positivity.21 Collectively, these findings support the concept that complement C3 deposition may contributes to intraglomerular microvascular injury in IgAN. Consistent with this hypothesis, patients with glomerular C3 deposition exhibited a higher proportion of endocapillary hypercellularity, a pathological feature indicative of glomerular endothelial activation and injury.22 This finding supports the involvement of complement-mediated endothelial dysfunction within the glomerulus. We therefore speculate that complement-mediated endothelial activation may promote histological glomerular prothrombotic lesions by facilitating intraglomerular thrombotic processes, leading to impaired capillary perfusion, localized ischemia. In this setting, the observed prolongation of APTT and reduction in fibrinogen levels are more plausibly interpreted as secondary consequences of ongoing coagulation factor consumption, rather than markers of a primary systemic anticoagulant state.
In our study, patients with renal C3 deposition had lower baseline eGFR and reduced circulating C3 levels than those without C3 deposition, which is consistent with findings from previous studies.17 The cumulative incidence curve showed an apparently lower incidence of the primary composite renal outcome among patients with renal C3 deposition, which was consistent with the unadjusted Cox model. This finding appears to differ from previous studies in which mesangial C3 deposition was associated with worse renal outcomes. However, this apparent discrepancy should be interpreted cautiously. As shown in Supplementary Table 1, treatment allocation differed substantially between the two groups. Kidney-protective therapy was used in 5 of 16 patients (31.3%) in the C3-negative group and 358 of 577 patients (62.0%) in the C3-positive group, while corticosteroid or immunosuppressive therapy was used in 6 of 16 patients (37.5%) and 351 of 577 patients (60.8%), respectively. Patients with renal C3 deposition may have been more likely to receive active treatment because of greater baseline disease activity, and these treatment differences may have modified subsequent renal outcomes. Consistent with this interpretation, the association between renal C3 deposition and primary composite renal outcome was substantially attenuated and became non-significant after adjustment for clinical, pathological, and treatment-related factors.
Several factors may explain the apparent discrepancy between our unadjusted findings and previous reports linking mesangial C3 deposition to worse renal outcomes. First, the comparison strategy differed across studies: prior studies stratified patients according to the intensity of mesangial C3 deposition, whereas our control group consisted exclusively of patients without renal C3 deposition. Second, as shown in Supplementary Table 1, the median follow-up duration was longer in the C3-negative group than in the C3-positive group (100 months [IQR, 27.0–134.3] vs 54 months [IQR, 26.0–85.0]), potentially providing a longer opportunity to detect renal outcome events. Although follow-up time and censoring were incorporated into the Cox models, only 16 C3-negative patients had available follow-up data, which may have reduced statistical stability and introduced selection bias. Differences in population characteristics and potential geographic heterogeneity may also have contributed. Third, the renal C3 deposition-negative group was small, which may have increased the instability of unadjusted estimates. Therefore, the prognostic significance of renal C3 deposition in IgAN warrants further investigation in larger prospective cohorts.
This study has several limitations, including its retrospective, single-center design, which limits causal inference and generalizability. In addition, specific staining for fibrin or platelet-rich thrombi was not routinely available; therefore, histological glomerular prothrombotic lesions were identified based on morphological features observed on routine renal biopsy sections. The marked imbalance in group size may have introduced selection bias. Moreover, dynamic assessment of circulating complement activity was unavailable, and residual confounding cannot be excluded.
Conclusion
In patients with IgA nephropathy, renal C3 deposition is associated with coagulation abnormalities, increased glomerular prothrombotic milieu, and distinct biochemical profiles. However, renal C3 deposition is not independently associated with long-term renal outcome after adjustment for clinical, pathological, and treatment-related factors. These findings highlight the potential importance of complement–coagulation interactions in IgAN and suggest that renal C3 deposition may help characterize a complement-related prothrombotic phenotype. Further validation in independent prospective cohorts is needed to clarify its prognostic significance.
Abbreviations
IgAN, immunoglobulin A nephropathy; C3, complement 3; eGFR, estimated glomerular filtration rate; OR, odds ratio; HR, hazard ratio; Gd-IgA1, galactose-deficient IgA1; SD, standard deviation; IQR, interquartile range; APTT, a prolonged activated partial thromboplastin time; PLA2R, phospholipase A2 receptor; MASP, mannan-binding lectin-associated serine protease; MBL, mannose-binding lectin.
Data Sharing Statement
The data are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Review Committee of The Affiliated Hospital of Guangdong Medical University (Approval Number: PJKT2026-111; Acceptance Number: KT2026-111-01). The patients were provided with a clear explanation of the relevant details of the project, and written informed consent was obtained from all participants or their legal guardians prior to renal biopsy and data collection. All participants or their guardians were informed about the purpose of the study prior to providing consent. All participants were free to choose whether to participate in the study and could withdraw at any time for any reason without incurring any personal or professional penalties, and without any impact on their subsequent medical treatment.
Acknowledgments
The authors wish to acknowledge the staff of the Institute of Renal Diseases, The Affiliated Hospital of Guangdong Medical University.
Author Contributions
Yun Guo: Conceptualization, Methodology, Software, Formal analysis, Writing – original draft;
Siqi Zheng: Methodology, Software, Validation, Data curation, Writing – review & editing; Shangmei Li: Visualization, Data curation, Writing – review & editing; Zhennan Ye: Software, Validation, Writing – review & editing; Mianna Luo: Methodology, Writing – review & editing, Funding acquisition; Huafeng Liu: Conceptualization, Writing – review & editing, Funding acquisition. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from National Natural Science Foundation of China (82370705); Guangdong Provincial Key Laboratory of Autophagy and Major Chronic Non-Communicable Diseases (2022B1212030003); Affiliated Hospital of Guangdong Medical University Clinical Research Program (LCYJ2023B006); Special Project for Clinical and Basic Sci&Tech Innovation of Guangdong Medical University (GDMULCJC2025048). This study was supported by the Big Data Platform of Affiliated Hospital of Guangdong Medical University.
Disclosure
The authors report no conflicts of interest for this study.
References
1. Cheung CK, Alexander S, Reich HN, Selvaskandan H, Zhang H, Barratt J. The pathogenesis of IgA nephropathy and implications for treatment. Nat Rev Nephrol. 2025;21(1):9–14.
2. Stamellou E, Seikrit C, Tang SC, et al. IgA nephropathy. Nat Rev Dis Primers. 2023;9(1).
3. Stoneman S, Teh JW, O’Shaughnessy MM. IgA nephropathy in adults: a review. JAMA. 2026;2026:1.
4. Barratt J, Lafayette RA, Zhang H, et al. IgA nephropathy: the lectin pathway and implications for targeted therapy. Kidney Int. 2023;104(2):254–264. doi:10.1016/j.kint.2023.04.029
5. Mastellos DC, Hajishengallis G, Lambris JD. A guide to complement biology, pathology and therapeutic opportunity. Nat Rev Immunol. 2024;24(2):118–141. doi:10.1038/s41577-023-00926-1
6. Zarantonello A, Revel M, Grunenwald A, Roumenina LT. C3-dependent effector functions of complement. Immunol Rev. 2023;313(1):120–138. doi:10.1111/imr.13147
7. Cheung CK, Dormer JP, Barratt J. The role of complement in glomerulonephritis-are novel therapies ready for prime time? Nephrol Dial Transplant. 2023;38(8):1789–1797. doi:10.1093/ndt/gfac296
8. Schmidt CQ, Schrezenmeier H, Kavanagh D. Complement and the prothrombotic state. Blood. 2022;139(13):1954–1972. doi:10.1182/blood.2020007206
9. Sauter RJ, Sauter M, Reis ES, et al. Functional relevance of the anaphylatoxin receptor C3aR for platelet function and arterial thrombus formation marks an intersection point between innate immunity and thrombosis. Circulation. 2018;138(16):1720–1735. doi:10.1161/CIRCULATIONAHA.118.034600
10. Subramaniam S, Jurk K, Hobohm L, et al. Distinct contributions of complement factors to platelet activation and fibrin formation in venous thrombus development. Blood. 2017;129(16):2291–2302.
11. Liu Z, Liang W, Pan Y. Complement-coagulation crosstalk in idiopathic membranous nephropathy: the potential pathogenesis and therapeutic perspective. Autoimmun Rev. 2025;24(5):103763.
12. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
13. Cattran DC, Coppo R, Cook HT, et al; Working Group of the International Ig ANN, the Renal Pathology S. The Oxford classification of IgA nephropathy: rationale, clinicopathological correlations, and classification. Kidney Int. 2009;76(5):534–545. doi:10.1038/ki.2009.243.
14. Trimarchi H, Barratt J, Cattran DC, et al. Oxford classification of IgA nephropathy 2016: an update from the IgA nephropathy classification working group. Kidney Int. 2017;91(5):1014–1021. doi:10.1016/j.kint.2017.02.003
15. Heinze G, Schemper M. A solution to the problem of separation in logistic regression. Stat Med. 2002;21(16):2409–2419. doi:10.1002/sim.1047
16. Guo Y, Li S, Wei J, Luo M, Liu H. The relationship between HBV antigens deposition in kidneys and renal prognosis in IgA nephropathy patients infected with HBV. Ren Fail. 2024;46(2):2417737. doi:10.1080/0886022X.2024.2417737
17. Kang Y, Xu B, Shi S, et al. Mesangial C3 deposition, complement-associated variant, and disease progression in IgA nephropathy. Clin J Am Soc Nephrol. 2023;18(12):1583–1591. doi:10.2215/CJN.0000000000000290
18. Duval A, Caillard S, Fremeaux-Bacchi V. The complement system in IgAN: mechanistic context for therapeutic opportunities. Nephrol Dial Transplant. 2023;38(12):2685–2693. doi:10.1093/ndt/gfad140
19. Hamilton KK, Hattori R, Esmon CT, Sims PJ. Complement proteins C5b-9 induce vesiculation of the endothelial plasma membrane and expose catalytic surface for assembly of the prothrombinase enzyme complex. J Biol Chem. 1990;265(7):3809–3814. doi:10.1016/S0021-9258(19)39666-8
20. Wiedmer T, Ando B, Sims PJ. Complement C5b-9-stimulated platelet secretion is associated with a Ca2+-initiated activation of cellular protein kinases. J Biol Chem. 1987;262(28):13674–13681. doi:10.1016/S0021-9258(19)76479-5
21. Li J, Guo L, Shi S, et al. The role of complement in microangiopathic lesions of IgA nephropathy. Kidney Int Rep. 2022;7(6):1219–1228. doi:10.1016/j.ekir.2022.03.028
22. Pattrapornpisut P, Avila-Casado C, Reich HN. IgA nephropathy: core curriculum 2021. Am J Kidney Dis. 2021;78(3):429–441. doi:10.1053/j.ajkd.2021.01.024
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Value of the HALP Score Compared with Other Inflammatory and Nutritional Indices in IgA Nephropathy
Benlioglu BN, Korkut G, Girtine E, Celebioglu Pekiner M, Sarsik Kumbaraci B, Şen S, Sezis M
International Journal of General Medicine 2026, 19:578963
Published Date: 20 April 2026