Back to Journals » International Journal of General Medicine » Volume 19
Prognostic Value of the HALP Score Compared with Other Inflammatory and Nutritional Indices in IgA Nephropathy
Authors Benlioglu BN, Korkut G, Girtine E, Celebioglu Pekiner M, Sarsik Kumbaraci B, Şen S ![]() , Sezis M
, Sezis M
Received 4 November 2025
Accepted for publication 17 March 2026
Published 20 April 2026 Volume 2026:19 578963
DOI https://doi.org/10.2147/IJGM.S578963
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David E. Stec
Beyza Nur Benlioglu,1,* Gizem Korkut,2,* Ege Girtine,1 Manolya Celebioglu Pekiner,2 Banu Sarsik Kumbaraci,3 Sait Şen,3 Meltem Sezis2
1Department of Internal Medicine, Ege University Faculty of Medicine, Izmir, Türkiye; 2Department of Internal Medicine, Division of Nephrology, Ege University Faculty of Medicine, Izmir, Türkiye; 3Department of Pathology, Ege University Faculty of Medicine, Izmir, Türkiye
*These authors contributed equally to this work
Correspondence: Meltem Sezis, Department of Internal Medicine, Division of Nephrology, Ege University Faculty of Medicine, Izmir, Türkiye, Email [email protected]
Purpose: IgA nephropathy (IgAN) is the most common primary glomerulonephritis and is characterized by highly variable renal outcomes. Conventional prognostic factors, including proteinuria, hypertension, estimated glomerular filtration rate (eGFR), and the MEST-C classification, provide limited predictive accuracy. This study aimed to evaluate the prognostic value of inflammatory and nutritional indices, particularly the Hemoglobin–Albumin–Lymphocyte–Platelet (HALP) score, in patients with IgAN.
Patients and methods: This retrospective cohort included 204 patients with biopsy-proven IgAN. Baseline demographic, clinical, laboratory, and histopathological data were collected. Inflammatory and nutritional indices (HALP, Systemic Immune-Inflammation Index [SII], Neutrophil-to-Lymphocyte Ratio [NLR], Platelet-to-Lymphocyte Ratio [PLR], Glasgow Prognostic Score [GPS/mGPS], and Controlling Nutritional Status [CONUT]) were calculated from routine laboratory parameters. Associations with renal outcomes, particularly progression to end-stage kidney disease (ESKD), were analyzed using Cox regression, Kaplan–Meier survival, and receiver operating characteristic (ROC) analyses.
Results: During a median follow-up of 39.5 months, 17.1% of patients progressed to ESKD. Higher HALP scores were significantly associated with better renal survival, whereas other indices showed no consistent prognostic value. In multivariate analysis, HALP remained an independent predictor of renal outcome (hazard ratio = 0.13; p < 0.001). ROC analysis confirmed its prognostic performance (AUC = 0.65; 95% CI: 0.56– 0.74; p < 0.001) with an optimal cut-off value of 42.4 (sensitivity: 72.7%; specificity: 55.0%).
Conclusion: The HALP score is a strong and independent prognostic biomarker in IgAN, outperforming other inflammatory and nutritional indices. Incorporating HALP into current risk-stratification models may enhance prognostic assessment and guide clinical management.
Plain Language Summary: IgA nephropathy (IgAN) is the most common kidney disease caused by the body’s immune system attacking its own tissues. The disease can lead to kidney failure in some people, but predicting who will experience this outcome has been difficult.
In this study, researchers looked at several simple blood test scores that reflect inflammation and nutrition in the body. Among them, the HALP score—which combines levels of hemoglobin, albumin, lymphocytes, and platelets—was found to be the most useful.
The study included 204 adults with biopsy-proven IgAN who were followed for an average of about three years. People with lower HALP scores had a much higher chance of developing kidney failure compared to those with higher scores. Other scores, such as SII, NLR, PLR, GPS, and CONUT, did not show the same reliability.
This finding suggests that a single routine blood test can provide helpful information about how a patient’s disease may progress. Doctors could use the HALP score to identify patients who need closer monitoring or earlier treatment to protect their kidneys.
Keywords: IgA nephropathy, HALP score, nutritional biomarkers, inflammatory indices, prognosis
Introduction
IgA nephropathy (IgAN) is the most common primary glomerulonephritis worldwide, exhibiting marked heterogeneity in its clinical manifestations and outcomes.1 While some patients experience an indolent course, 5–15% progress to end-stage kidney disease (ESKD) within the first five years after diagnosis, and this rate increases to 10–50% after 20 years, with approximately 30–40% ultimately requiring renal replacement therapy (RRT).1,2
The prognostic evaluation of IgAN primarily relies on conventional clinical and pathological parameters, including proteinuria, hematuria, hypertension, estimated glomerular filtration rate (eGFR) at diagnosis, and the MEST-C classification (mesangial hypercellularity [M], endocapillary proliferation [E], segmental glomerulosclerosis [S], tubular atrophy/interstitial fibrosis [T], and presence of crescents [C]).3–6 However, several studies have demonstrated that these parameters alone may not adequately predict disease progression.3,6–8
The pathogenesis of IgAN involves chronic inflammation triggered by the overproduction of galactose-deficient IgA1 (Gd-IgA1) molecules and the subsequent formation of immune complexes with anti-glycan antibodies, which deposit within the glomerular mesangium.9–11 Inflammatory and nutritional indices have emerged as valuable tools for assessing systemic inflammation and the contribution of nutritional status to disease progression. These scores, derived from routine laboratory parameters, offer a practical and cost-effective means to monitor inflammatory burden and its impact on renal outcomes. When integrated with classical clinical and histopathological predictors, such indices may provide a more comprehensive assessment of prognosis. However, evidence regarding their clinical significance in IgAN remains limited.
Beyond conventional clinical and histopathological predictors, systemic inflammatory and nutritional status plays an important role in the progression of IgA nephropathy (IgAN). The Hemoglobin–Albumin–Lymphocyte–Platelet (HALP) score integrates key biological factors involved in chronic kidney disease. Anemia and hypoalbuminemia, common in IgAN, reflect chronic inflammation, protein loss, and poor nutritional status and are associated with renal hypoxia, tubular injury, and interstitial fibrosis.12,13 Lymphocyte and platelet counts further capture immune dysregulation and inflammatory activation, linking HALP to the malnutrition–inflammation–atherosclerosis (MIA) syndrome and disease progression in IgAN.14,15
Although several inflammatory and nutritional indices, including SII, NLR, PLR, CONUT, and GPS, have been evaluated in IgAN, existing evidence remains limited by small sample sizes, short follow-up periods, and a lack of direct comparison between multiple indices.15,16 Moreover, few studies have examined the association between these systemic biomarkers and histopathological features such as MEST-C components or crescent formation, which are central to disease activity and prognosis in IgAN.8,17 These gaps support the need for integrated analyses combining clinical outcomes, pathology, and multiple biomarker scores.
Recent studies published have highlighted the potential prognostic relevance of inflammatory and nutritional indices, including the Systemic Immune-Inflammation Index (SII), Hemoglobin–Albumin–Lymphocyte–Platelet (HALP) score, Glasgow Prognostic Score (GPS/mGPS), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Controlling Nutritional Status (CONUT) score, in patients with IgA nephropathy.11–13,15,16,18–20
These studies reported heterogeneous findings: while some demonstrated associations between individual indices (such as NLR, PLR, or albumin-based scores) and renal outcomes, others found limited or inconsistent prognostic value, often constrained by small sample sizes, short follow-up durations, or the evaluation of single indices without direct comparison.11–13,15,16,18–20
The present study aimed to retrospectively evaluate the prognostic impact of these inflammatory and nutritional indices (SII, HALP, GPS/mGPS, NLR, PLR, and CONUT) on renal outcomes and survival in patients with IgAN. Additionally, we assessed the relationships between these indices and conventional prognostic factors, including histopathological features defined by the MEST-C classification.
Methods
Patient Selection
A total of 280 patients diagnosed with IgA nephropathy (IgAN) by kidney biopsy at Ege University Faculty of Medicine between 2012 and 2023 were retrospectively reviewed. Among them, 204 patients with available baseline and follow-up data between January 1, 2012, and October 31, 2024, and with a minimum follow-up duration of six months were included in the study.
Inclusion Criteria
Age ≥18 years, biopsy-proven primary IgAN, and follow-up of at least six months.
Exclusion Criteria
Secondary IgAN (Henoch–Schönlein purpura, spondyloarthropathies, chronic liver disease, celiac/gluten enteropathy, or malignancy) and follow-up shorter than six months.
Clinical Data
The following variables were retrospectively obtained from patient records:
- Sociodemographic characteristics: age, sex, body mass index (BMI), follow-up duration, presence of hypertension, and blood pressure measurements.
- Biochemical parameters: hemoglobin, hematocrit, lymphocyte count, neutrophil count, platelet count, albumin, total protein, serum creatinine, serum uric acid, estimated glomerular filtration rate (eGFR), serum C3 and C4 levels, immunoglobulins (IgG, IgA), lipid profile (total cholesterol, LDL, HDL, triglycerides), ferritin, C-reactive protein (CRP), 24-hour urinary protein, hematuria, and urinary erythrocyte count.
- Histopathological data: MEST-C classification, including mesangial hypercellularity (M: M0 ≤50%, M1 >50%), endocapillary hypercellularity (E: absent E0, present E1), segmental glomerulosclerosis (S: absent S0, present S1), tubular atrophy/interstitial fibrosis (T: ≤25% T0, 26–50% T1, >50% T2), and cellular or fibrocellular crescents (C: absent C0, ≤25% C1, >25% C2).Additional variables included the degree of global glomerulosclerosis and treatments with renin–angiotensin system (RAS) inhibitors or immunosuppressive agents. Histopathological evaluation was performed by two experienced renal pathologists blinded to clinical outcomes.
Baseline laboratory parameters were obtained at the time of kidney biopsy or at first presentation.
Inflammatory and Nutritional Scores
Inflammatory and nutritional indices were calculated from baseline laboratory parameters as follows:
- SII: neutrophil (×109/L) × platelet (×109/L) / lymphocyte (×109/L)
- HALP: hemoglobin (g/L) × albumin (g/L) × lymphocyte (×109/L) / platelet (×109/L)
- GPS/mGPS: Glasgow Prognostic Score (Supplementary Table 1)
- NLR: neutrophil (×109/L) / lymphocyte (×109/L)
- PLR: platelet (×109/L) / lymphocyte (×109/L)
- CONUT: calculated based on serum albumin, lymphocyte count, and total cholesterol (Supplementary Table 2)
Outcomes
The study endpoints were defined as:
- <30% decline in eGFR compared with baseline
- ≥30% decline in eGFR compared with baseline
- End-stage renal disease (ESKD), defined as eGFR <15 mL/min/1.73 m2 or initiation of renal replacement therapy (RRT) or kidney transplantation.
The eGFR was calculated using the 2021 CKD-EPI creatinine equation:

where Scr = serum creatinine (mg/dL); κ = 0.7 for females and 0.9 for males; α = –0.241 for females and –0.302 for males.
Patients with missing key baseline or follow-up data were excluded from the analysis.
Statistical Analysis
All analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA). Categorical variables were expressed as numbers and percentages, whereas continuous variables were presented as median (interquartile range [IQR]) or mean ± standard deviation (SD), depending on distribution assessed by the Shapiro–Wilk test.
Group comparisons were conducted using the independent-samples t-test, Mann–Whitney U-test, or Kruskal–Wallis test as appropriate. Post hoc analyses after Kruskal–Wallis testing were performed with the Dunn–Bonferroni correction. The chi-square or Fisher–Freeman–Halton tests were used for categorical variables.
Multinomial and binary logistic regression analyses were employed to identify factors associated with adverse renal outcomes. Renal survival was analyzed using Kaplan–Meier survival curves.
Propensity score matching (PSM) was performed to reduce potential confounding related to RAS inhibitors use and baseline disease severity. Propensity scores were calculated using a logistic regression model including age, sex, and baseline serum creatinine level as matching variables. One-to-one nearest-neighbor matching without replacement was applied using a caliper width of 0.1. Balance between matched groups was assessed before and after matching, and subsequent analyses were conducted in the matched cohort.
Cox proportional hazards regression analysis was used to evaluate the independent association between the HALP score and progression to ESKD. Variables included in the multivariable models were selected based on clinical relevance and prior evidence and included age at diagnosis, sex, baseline estimated glomerular filtration rate, 24-hour proteinuria, presence of hypertension, use of RAS inhibitors, number of globally sclerotic glomeruli, and the tubular atrophy/interstitial fibrosis (T) component of the MEST-C classification. The proportional hazards assumption was assessed and confirmed prior to model interpretation.
Results
Baseline sociodemographic, clinical, and pathological characteristics of the study cohort according to ESKD status were presented in the Table 1. Supplementary Tables 3–8 provide detailed data on demographic, laboratory, pathological, and treatment-related variables that complement the main results presented in the manuscript. In addition, Supplementary Figure 1a–b offer further visual analyses of renal outcomes. These supplementary materials are intended to enhance transparency and allow readers to explore the extended dataset underlying the study’s findings.
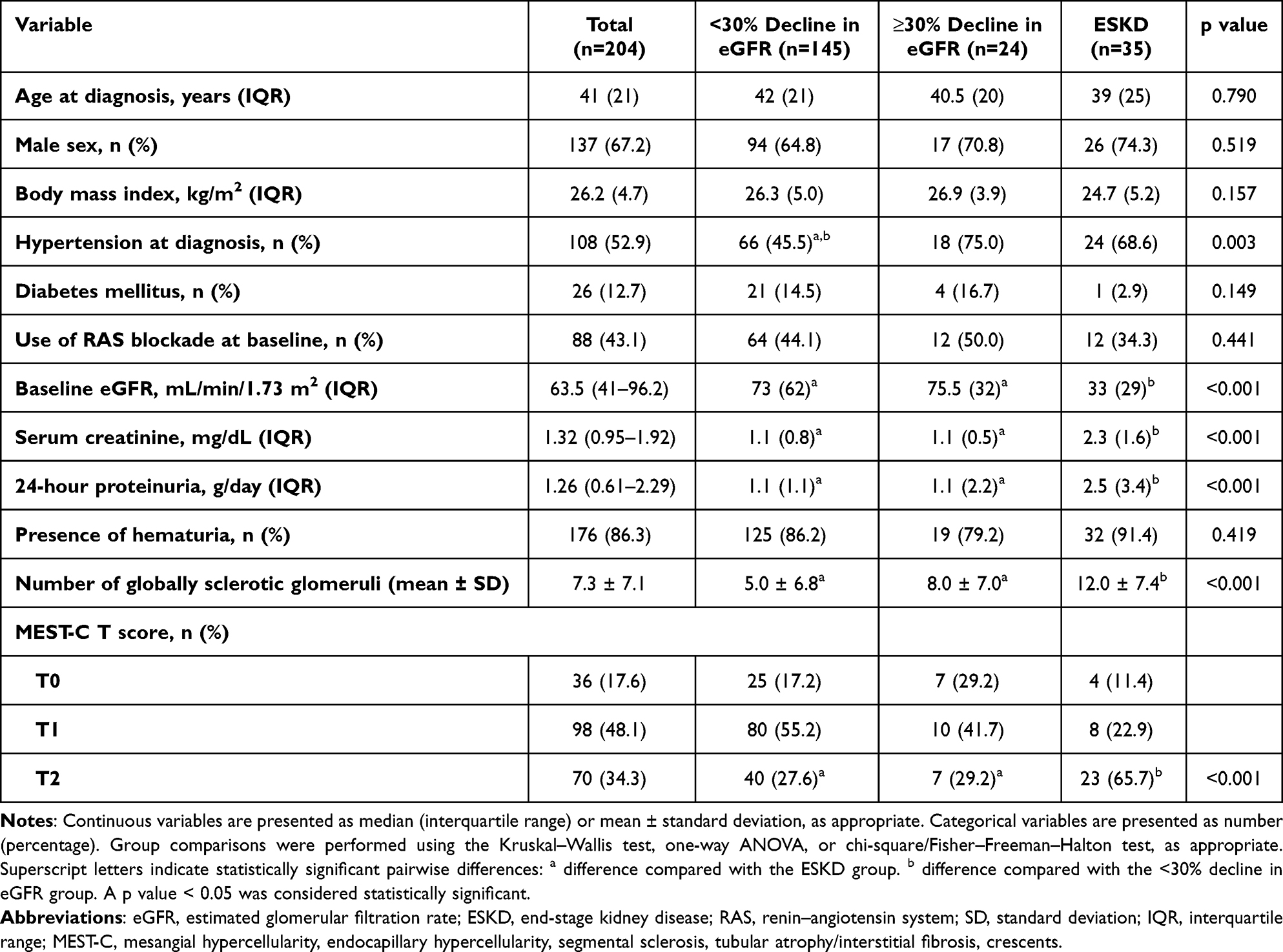 |
Table 1 Baseline Sociodemographic, Clinical, and Pathological Characteristics of the Study Cohort According to ESKD Status |
No significant differences were observed among outcome groups for SII, PLR, NLR, CONUT, GPS, or mGPS (Table 2). In contrast, HALP scores differed significantly (p = 0.035), being higher in the >30% eGFR decline group (median 45.5, IQR 25) and lower in the ESKD group (median 36.4, IQR 16.5) (Table 2).
 |
Table 2 Inflammatory and Nutritional Scores |
Patients were stratified into three groups according to baseline HALP scores: Group 1 < 36.6 (n = 68, 33.3%), Group 2 ≥ 36.6–≤ 51.4 (n = 67, 33.4%), and Group 3 > 51.4 (n = 69, 33.3%).
No differences were found among HALP groups in BMI or blood pressure. Female sex, mean age at diagnosis, and hypertension were less frequent in the high-HALP group. No significant differences were observed among HALP groups in proteinuria, hematuria count, uric acid, IgG, IgA, C3, C4, ferritin, or neutrophil counts. However, patients with higher HALP scores had significantly higher GFR, albumin, hemoglobin, and lymphocyte levels, and lower creatinine, CRP, and platelet counts. The presence of cellular crescents was also lower in the high-HALP group (Supplementary Table 9).
ESKD outcomes were significantly lower in the high-HALP group (Table 3). Patients in Group 3 were more protected against ESKD (p < 0.01) and had significantly longer renal survival (log-rank p < 0.01) (Figure 1). Conversely, patients with low HALP (Group 1) had a higher risk of ESKD.
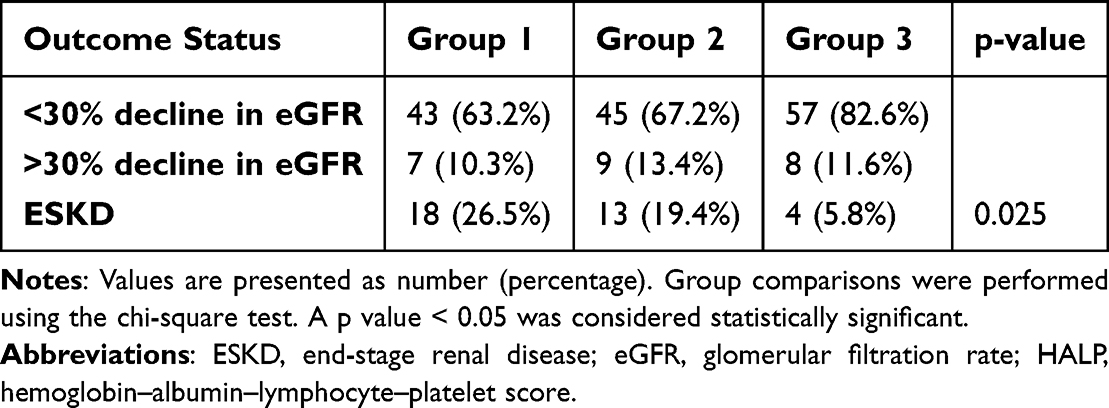 |
Table 3 Outcome Status in Different HALP Score Groups |
 |
Figure 1 Kaplan–Meier renal survival curves according to HALP tertiles. The high HALP tertile is shown in green, the intermediate tertile in red, and the low tertile in blue. Patients in the high HALP group demonstrated significantly longer renal survival compared with those in the low HALP group (log-rank p < 0.01). |
In the unadjusted model, Group 3 had an 87% lower ESKD risk compared with Group 1 (HR = 0.13, p < 0.01). This effect remained significant after adjustment in Model 1 (HR = 0.16, p < 0.01) and Model 2 (HR = 0.13, p < 0.01). No significant differences were observed between Group 2 and Group 1 (p > 0.05) (Table 4).
 |
Table 4 Effect of HALP Score Tertiles on ESKD in Unadjusted and Adjusted Cox Regression Analysis Models |
Each unit increase in proteinuria increased ESKD risk (HR = 1.27, p = 0.001; HR = 1.21, p = 0.01). Patients using RAS blockers had significantly lower risk compared with non-users (HR = 0.23–0.37, p < 0.01). Each unit increase in global sclerosis count increased ESKD risk (HR = 1.06–1.07, p < 0.001) (Table 4). After propensity score matching, the associations between HALP and renal outcomes remained consistent with the primary analyses.
ROC curve analysis for HALP demonstrated an AUC = 0.65 (p < 0.01). At a cutoff value of 42.4, HALP predicted ESKD with 72.7% sensitivity and 55.0% specificity (Table 5 and Figure 2).
 |
Table 5 Predictive Value of HALP Score for ESKD |
 |
Figure 2 Receiver operating characteristic (ROC) curve demonstrating the predictive ability of the HALP score for ESKD. The area under the curve (AUC) was 0.65 (95% CI: 0.56–0.74; p < 0.01). A cutoff value of 42.4 yielded 72.7% sensitivity and 55% specificity. |
Discussion
The HALP score emerged as the most significant prognostic biomarker in our cohort of patients with IgA nephropathy (IgAN), with lower values associated with a markedly higher risk of ESKD and shorter renal survival. While several inflammatory and nutritional indices have been proposed in recent years, evidence regarding their role in IgAN prognosis remains inconsistent. In this study, we systematically evaluated these indices and demonstrated the superior predictive performance of HALP compared with SII, NLR, PLR, CONUT, and GPS.
The systemic immune-inflammation index (SII) did not show any prognostic association in our cohort, although previous reports suggested a link with ESKD progression.16 A possible explanation for this discrepancy may be the higher rate of renin–angiotensin system (RAS) blocker use in our ESKD group, as the anti-inflammatory effects of RAS inhibition could mitigate the prognostic value of SII.21
The neutrophil-to-lymphocyte ratio (NLR) also yielded inconsistent results. Some investigations identified lower values as a risk factor,15 while others associated higher values with ESKD progression.20 In our cohort, no significant relationship was detected. It is plausible that higher NLR reflects acute neutrophil-driven inflammation, whereas lower NLR may indicate chronic immune dysregulation, both potentially influencing IgAN progression.14 The uncertainty regarding disease onset relative to the time of diagnosis may further explain the variability across studies.
The platelet-to-lymphocyte ratio (PLR) has been associated with worse renal outcomes in IgAN;18,22 however, although our ESKD group exhibited higher values, the difference did not reach statistical significance. This pattern suggests that PLR may have prognostic potential but requires validation in larger and more homogeneous populations.
The Controlling Nutritional Status (CONUT) score showed no differences across outcome groups in our analysis, despite reports of higher values in patients progressing to ESKD.12 Similarly, the Glasgow Prognostic Score (GPS) and its modification (mGPS) were not associated with outcomes, although prior studies described their role in rapidly progressive CKD or their prognostic value in univariate analyses.15,19 The lower serum albumin but higher cholesterol levels in our ESKD group may have offset the CONUT score, while methodological and population differences likely contributed to the lack of reproducibility of GPS in our study.
By contrast, the HALP score, which integrates hemoglobin, albumin, lymphocyte, and platelet values, demonstrated robust prognostic value in our cohort. Patients who progressed to ESKD had significantly lower HALP values. Prior studies have also emphasized albumin-based indices as independent prognostic factors in IgAN.23–25 Hemoglobin reflects anemia and renal hypoxia,26 lymphocyte count mirrors immune competence,13 and platelets contribute to inflammation and cytokine release.13,27 The combination of these parameters into a single score enables HALP to serve as a comprehensive indicator of both inflammatory and nutritional status, which may explain its superiority over other indices.
Sex-related differences in HALP have been reported, with males typically showing higher values,13,28 largely attributable to baseline hemoglobin levels.29,30 Consistent with previous findings, our study showed that higher HALP scores were associated with better renal function parameters, including higher eGFR and lower creatinine, as well as more favorable albumin and lymphocyte counts.13,28 Although proteinuria was higher in low-HALP groups, the difference was not statistically significant in our dataset; however, urinary albumin loss remains a biologically plausible contributor to reduced HALP values.31,32
Histopathological evaluation revealed more frequent crescent lesions in patients with low HALP, a finding consistent with previous reports linking low HALP to severe chronic lesions such as tubular atrophy and interstitial fibrosis.13,28 Although the associations with other MEST-C components varied between studies, the overall evidence supports HALP as a marker reflecting both clinical and structural disease severity.
Survival analyses confirmed that patients with low HALP values had a markedly higher risk of ESKD. Although the discriminatory performance of HALP was moderate (AUC = 0.65), this level of accuracy is comparable to that of several single biomarkers used in IgAN prognosis and suggests that HALP should be considered a complementary tool rather than a standalone predictor, particularly when integrated with established clinical and histopathological risk factors. In our cohort, a cutoff of 42.4 yielded 72.7% sensitivity and 55% specificity, consistent with previously reported thresholds.13,28 Multivariable Cox regression demonstrated that higher HALP values were independently associated with an 87% reduction in ESKD risk (HR = 0.13, p < 0.001). These results strongly support the role of HALP as an independent biomarker for renal prognosis in IgAN.
Study Limitations
This study has inherent limitations. Its retrospective, single-center design limits the generalizability of the results, and the relatively small sample size restricted subgroup analyses. In addition, IgA nephropathy is a slowly progressive disease, and although a minimum follow-up duration of six months was required for inclusion, the relatively short and non-uniform follow-up period may have limited the number of long-term renal events and, consequently, the precision of long-term prognostic estimates. Longer and more homogeneous follow-up could increase event rates and allow more robust evaluation of late renal outcomes. Furthermore, due to the retrospective design of the study, a formal a prior power calculation was not performed. This should be considered when interpreting the results, particularly for subgroup analyses. In addition, although age and sex were included in multivariable analyses, more detailed sociodemographic factors could not be fully explored, which may influence components of the HALP score, particularly hemoglobin and nutritional parameters. Nevertheless, the sample size and number of outcome events in the present study are comparable to or exceed those reported in several previously published IgAN cohorts, supporting the overall robustness of the analyses.
Conclusion
The HALP score emerged as the most significant and independent prognostic biomarker in IgAN, with lower values predicting a higher risk of ESKD and shorter renal survival. At a cutoff value of 42.4, HALP predicted ESKD with 72.7% sensitivity and 55% specificity. Given its higher sensitivity than specificity, HALP appears to be more useful as a screening and risk-identification tool rather than a definitive diagnostic marker, enabling the early identification of patients who may require closer monitoring or timely therapeutic intervention. The superior performance of HALP compared with other inflammatory and nutritional indices may be explained by its ability to integrate key components of the malnutrition–inflammation–atherosclerosis (MIA) axis, providing a more comprehensive reflection of systemic disease burden than single-ratio markers such as NLR or PLR. Importantly, the association between low HALP values and the presence of cellular crescents suggests that HALP may also reflect active inflammatory disease, with potential implications for therapeutic decision-making, including immunosuppressive strategies in selected patients. However, given its moderate predictive accuracy, HALP should be regarded as a complementary prognostic marker and interpreted in conjunction with established clinical and pathological predictors such as proteinuria, baseline renal function, and MEST-C scores. Because HALP is derived from routinely available and low-cost laboratory parameters, it may be particularly useful in resource-limited settings. When integrated with established clinical and histopathological risk factors, the HALP score may contribute to more refined risk stratification and individualized follow-up strategies in patients with IgAN.
Practical Application
The HALP score, derived from routine laboratory tests, may help clinicians identify IgAN patients at higher risk of progression. Incorporating HALP into routine evaluation could support earlier interventions and closer monitoring.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used ChatGPT-5 to refine the English language. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the final version of the manuscript.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Requests to access these datasets should be directed to [email protected].
Ethics Approval
The studies involving humans were approved by the Institutional Ethical Review Board of Ege University Hospital (24-12T/37). The study was conducted in accordance with good clinical practice guidelines and the principles of the Declaration of Helsinki. The participants provided written informed consent to participate in this study.
Consent for Publication
Due to the retrospective design, the requirement for individual informed consent was waived by the ethics committee.
Acknowledgments
The authors thank the clinical and pathology teams of Ege University Faculty of Medicine for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no financial support was received for the research and/or publication of this article.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. D’Amico G. The commonest glomerulonephritis in the world:IgA Nephropathy. Q J Med. 1987;64(245):709–11.
2. Hassler JR. IgA nephropathy: a brief review. Semin Diagn Pathol. 2020;37(3):143–147. doi:10.1053/j.semdp.2020.03.001
3. Berthoux F, Mohey H, Laurent B, Mariat C, Afiani A, Thibaudin L. Predicting the risk for dialysis or death in IgA nephropathy. J Am Soc Nephrol. 2011;22(4):752–761. doi:10.1681/asn.2010040355
4. Goto M, Wakai K, Kawamura T, Ando M, Endoh M, Tomino Y. A scoring system to predict renal outcome in IgA nephropathy: a nationwide 10-year prospective cohort study. Nephrol Dial Transplant. 2009;24(10):3068–3074. doi:10.1093/ndt/gfp273
5. Pattrapornpisut P, Avila-Casado C, Reich HN. IgA nephropathy: core curriculum 2021. Am J Kidney Dis. 2021;78(3):429–441. doi:10.1053/j.ajkd.2021.01.024
6. Radford MG Jr, Donadio JV Jr, Bergstralh EJ, Grande JP. Predicting renal outcome in IgA nephropathy. J Am Soc Nephrol. 1997;8(2):199–207. doi:10.1681/asn.V82199
7. Rodrigues JC, Haas M, Reich HN. IgA Nephropathy. Clin J Am Soc Nephrol. 2017;12(4):677–686. doi:10.2215/cjn.07420716
8. Trimarchi H, Barratt J, Cattran DC, et al. Oxford Classification of IgA Nephropathy 2016: an update from the IgA nephropathy classification working group. Kidney Int. 2017;91(5):1014–1021. doi:10.1016/j.kint.2017.02.003
9. Maillard N, Wyatt RJ, Julian BA, et al. Current understanding of the role of complement in IgA nephropathy. J Am Soc Nephrol. 2015;26(7):1503–1512. doi:10.1681/asn.2014101000
10. Roos A, Rastaldi MP, Calvaresi N, et al. Glomerular activation of the lectin pathway of complement in IgA nephropathy is associated with more severe renal disease. J Am Soc Nephrol. 2006;17(6):1724–1734. doi:10.1681/asn.2005090923
11. Tan J, Song G, Wang S, et al. Platelet-to-albumin ratio: A novel IgA nephropathy prognosis predictor. Front Immunol. 2022;13:842362. doi:10.3389/fimmu.2022.842362
12. Qian C, Li H, Hou Y, Wang W, Sun M. Clinical implications of four different nutritional indexes in patients with IgA nephropathy. Front Nutr. 2024;11:1431910. doi:10.3389/fnut.2024.1431910
13. Yuan Y, Liang X, He M, Wu Y, Jiang X. Haemoglobin, albumin, lymphocyte, and platelet score as an independent predictor for renal prognosis in IgA nephropathy. Front Endocrinol. 2024;15:1339921. doi:10.3389/fendo.2024.1339921
14. Esteve Cols C, Graterol Torres FA, Quirant Sánchez B, et al. Immunological pattern in IgA nephropathy. Int J Mol Sci. 2020;21(4). doi:10.3390/ijms21041389
15. Pană N, Ștefan G, Popa T, Ciurea O, Stancu SH, Căpușă C. Prognostic value of inflammation scores and hematological indices in IgA and membranous nephropathies: an exploratory study. Medicina. 2024;60(8). doi:10.3390/medicina60081191
16. Zhai Y, Sun S, Zhang W, Tian H. The prognostic value of the systemic immune inflammation index in patients with IgA nephropathy. Ren Fail. 2024;46(2):2381613. doi:10.1080/0886022x.2024.2381613
17. Yi F, Li Z, Jiang J, Lan L, Bai Y. Related factors of crescents and prognosis in IgA nephropathy. Clin Nephrol. 2023;99(1):24–31. doi:10.5414/cn110918
18. Chang D, Cheng Y, Luo R, et al. The prognostic value of platelet-to-lymphocyte ratio on the long-term renal survival in patients with IgA nephropathy. Int Urol Nephrol. 2021;53(3):523–530. doi:10.1007/s11255-020-02651-3
19. Stefan G, Stancu S, Zugravu A, Capusa C. Inflammation-based modified Glasgow prognostic score and renal outcome in chronic kidney disease patients: is there a relationship? Intern Med J. 2022;52(6):968–974. doi:10.1111/imj.15251
20. Wang S, Dong L, Pei G, et al. High neutrophil-to-lymphocyte ratio is an independent risk factor for end stage renal diseases in IgA nephropathy. Front Immunol. 2021;12:700224. doi:10.3389/fimmu.2021.700224
21. Awad K, Zaki MM, Mohammed M, Lewek J, Lavie CJ, Banach M. Effect of the renin-angiotensin system inhibitors on inflammatory markers: a systematic review and meta-analysis of randomized controlled trials. Mayo Clin Proc. 2022;97(10):1808–1823. doi:10.1016/j.mayocp.2022.06.036
22. Sági B, Vas T, Csiky B, Nagy J, Kovács TJ. Are platelet-related parameters prognostic predictors of renal and cardiovascular outcomes in IgA nephropathy? J Clin Med. 2024;13(4). doi:10.3390/jcm13040991
23. Qin A, Wang S, Dong L, et al. Prognostic value of the albumin-to-fibrinogen ratio (AFR) in IgA nephropathy patients. Int Immunopharmacol. 2022;113(Pt A):109324. doi:10.1016/j.intimp.2022.109324
24. Qin A, Yang D, Wang S, et al. Uric acid-based ratios for predicting renal failure in Chinese IgA nephropathy patients. Int J Med Sci. 2023;20(12):1584–1591. doi:10.7150/ijms.85430
25. Zhang Y, Man L. Albumin-to-fibrinogen ratio is an independent predictor of corticosteroid response and prognosis in patients with IgA nephropathy. Eur J Med Res. 2023;28(1):146. doi:10.1186/s40001-023-01106-6
26. Nangaku M. Chronic hypoxia and tubulointerstitial injury: a final common pathway to end-stage renal failure. J Am Soc Nephrol. 2006;17(1):17–25. doi:10.1681/asn.2005070757
27. Molnar MZ, Streja E, Kovesdy CP, et al. High platelet count as a link between renal cachexia and cardiovascular mortality in end-stage renal disease patients. Am J Clin Nutr. 2011;94(3):945–954. doi:10.3945/ajcn.111.014639
28. Liang X, Jiang X. The hemoglobin, albumin, lymphocyte, and platelet (HALP) score is associated with severe renal tubular atrophy/interstitial fibrosis in IgA nephropathy. Eur J Med Res. 2024;29(1):542. doi:10.1186/s40001-024-02148-0
29. Antar R, Farag C, Xu V, Drouaud A, Gordon O, Whalen MJ. Evaluating the baseline hemoglobin, albumin, lymphocyte, and platelet (HALP) score in the United States adult population and comorbidities: an analysis of the NHANES. Front Nutr. 2023;10:1206958. doi:10.3389/fnut.2023.1206958
30. Beutler E, Waalen J. The definition of anemia: what is the lower limit of normal of the blood hemoglobin concentration? Blood. 2006;107(5):1747–1750. doi:10.1182/blood-2005-07-3046
31. Gorriz JL, Martinez-Castelao A. Proteinuria: detection and role in native renal disease progression. Transplant Rev. 2012;26(1):3–13. doi:10.1016/j.trre.2011.10.002
32. Macé C, Chugh SS. Nephrotic syndrome: components, connections, and angiopoietin-like 4-related therapeutics. J Am Soc Nephrol. 2014;25(11):2393–2398. doi:10.1681/asn.2014030267
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Relevance of HALP Score in Predicting Hospital Stay Duration and Outcomes in Acute Heart Failure
Aydın MZ, Abdi IA
International Journal of General Medicine 2025, 18:7095-7100
Published Date: 26 November 2025
Renal Complement C3 Deposition is Associated with Glomerular Prothrombotic Milieu in Patients with IgA Nephropathy
Guo Y, Zheng S, Li S, Ye Z, Luo M, Liu H
Journal of Inflammation Research 2026, 19:611287
Published Date: 3 July 2026