Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Relationship Between Hyperinsulinemia and Coronary Microvascular Disease
Authors Tan Q ![]() , Zu C, Zhang W, Hao J, Li Y, Lu Q
, Zu C, Zhang W, Hao J, Li Y, Lu Q ![]() , Li Z, Guo Y
, Li Z, Guo Y
Received 30 May 2025
Accepted for publication 18 October 2025
Published 25 October 2025 Volume 2025:18 Pages 3931—3940
DOI https://doi.org/10.2147/DMSO.S534270
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Qiang Tan,1 Chenhong Zu,2 Wenli Zhang,1 Jia Hao,2 Yang Li,2 Qiang Lu,3 Zhimeng Li,2 Yao Guo2
1Department of Cardiology, Peking University Third Hospital Qinhuangdao Hospital, Qinhuangdao, Hebei, People’s Republic of China; 2Department of Cardiology, the First Hospital of Qinhuangdao, Qinhuangdao, Hebei, People’s Republic of China; 3Department of Endocrine, the First Hospital of Qinhuangdao, Qinhuangdao, Hebei, People’s Republic of China
Correspondence: Qiang Tan, Department of Cardiology, Peking University Third Hospital of Qinhuangdao Hospital, Qinhuangdao, Hebei, 066000, People’s Republic of China, Email [email protected]
Background and Objectives: Coronary microvascular disease (CMVD) is commonly observed among individuals presenting with chest pain, though its underlying pathological mechanisms remain incompletely elucidated. Emerging evidence suggests that hyperinsulinemia serves as a critical factor in cardiovascular dysfunction development, potentially contributing to CMVD pathogenesis. This investigation aims to examine the potential link between hyperinsulinemia and CMVD manifestation in clinical populations.
Methods: This study enrolled 347 patients presenting with ischemic chest pain but without obstructive coronary artery disease. All participants underwent coronary flow reserve (CFR) assessment through transthoracic Doppler echocardiography. Patients demonstrating CFR values below 2.0 were classified into the CMVD group (n=105), while those with CFR≥ 2 constituted the non-CMVD group (n=245). Biochemical parameters including fasting insulin (FINS), fasting blood glucose (FBS), and glycosylated hemoglobin (HbA1c) were quantitatively analyzed. Based on FINS concentration tertiles, participants were stratified into low-insulin (n=118), medium-insulin (n=114), and high-insulin (n=115) subgroups. Multivariate logistic regression analysis was employed to calculate adjusted odds ratios (OR) with corresponding 95% confidence intervals (CI) for CMVD risk assessment.
Results: CMVD patients exhibited elevated concentrations of FINS, FBS, HOMA-IR, and HbA1c compared to non-CMVD counterparts. CMVD cases demonstrated greater prevalence of female gender, diabetes mellitus, and hypertension (P < 0.05). Stratification by FINS tertiles revealed progressively diminishing CFR levels from low to high insulin groups. Multivariate analysis identified hyperinsulinemia (third tertile, FINS > 12.4 μIU/mL) as an independent predictor for CMVD (OR 2.279, 95% CI 1.046– 4.967). Additional independent risk factors included diabetes (OR 1.920, 95% CI 1.049– 3.513), female sex (OR 3.218, 95% CI 1.858– 5.572), hypertension (OR 1.746, 95% CI 1.013– 3.007), and advancing age (OR 1.036, 95% CI 1.005– 1.069) (P < 0.05).
Conclusion: Hyperinsulinemia is associated with impaired coronary microvascular function. Hyperinsulinemia serves as a significant independent contributor to the development of CMVD, demonstrating a clear pathological relationship beyond conventional risk factors.
Keywords: coronary microvascular disease, hyperinsulinemia, diabetes mellitus, coronary flow reserve
Introduction
Emerging evidence indicates that a substantial percentage of individuals experiencing ischemic chest pain present with non-obstructive coronary artery pathology upon diagnostic evaluation.1,2 Such clinical cases are increasingly recognized as manifestations of ischemia stemming from coronary microvascular dysfunction (CMVD). Contemporary research has established connections between CMVD and multiple adverse outcomes, including compromised life quality metrics, elevated risk of major adverse cardiac events, and greater frequencies of repeat hospital admissions.3,4
As we know, the most important characteristic of CMVD is coronary microvascular dysfunction, which starts with declined coronary flow reserve (CFR).5 Transthoracic Doppler echocardiography serves as a clinically valuable technique for quantifying CFR, providing non-invasive assessment of microvascular functionality through hemodynamic parameter measurement.
The pathophysiological mechanisms of CMVD are intricate and involve multiple contributing factors. Existing research has identified diabetes, hypertension, and metabolic syndrome as potential disruptors of coronary microvascular performance.6,7 Elevated concentrations of blood glucose and insulin have been linked to detrimental effects on cardiovascular health.8 Prior investigation by our team revealed that hyperinsulinemia impairs the functionality of endothelial progenitor cells, crucial mediators in maintaining vascular endothelial integrity.9 Nevertheless, the potential connection between hyperinsulinemia and coronary microvascular pathology remains poorly understood. Notably, no previous studies have explored the impact of hyperinsulinemia on coronary microvascular function. This investigation seeks to examine the potential correlation between hyperinsulinemia and the development of CMVD.
Methods
Study Population
This retrospective observational analysis examined data from patients diagnosed with coronary microvascular disease between May 2019 and January 2024. The inclusion criteria were: 1) presence of chest pain symptoms; 2) documented coronary angiography showing <50% arterial stenosis; 3) completed coronary flow reserve (CFR) assessment; and 4) available fasting insulin level measurements. The exclusion criteria were: 1) Patients with obstructive coronary artery disease, defined as coronary artery stenosis ≥50%; 2) history of acute myocardial infarction in the preceding three months; 3) recent use (within 3 months) of insulin or insulin-sensitizing agents; 4) patients with cardiomyopathy (dilated cardiomyopathy, hypertrophic cardiomyopathy, restrictive cardiomyopathy, and myocarditis).
Sample size was calculated by Pass 11 software. Based on preliminary data, we assumed CFR average value with a standard deviation. For a required power of 0.9 (90%), using an F-test for comparisons, a sample size of at least 35 cases for each group was required. The total sample size was 105 cases.
This study was approved by the ethics committee of Qinhuangdao First Hospital, and written consent documentation obtained from every participant prior to their involvement in the investigation. This study complies with the Declaration of Helsinki.
Diagnosis of Coronary Microvascular Disease
As depicted in the diagnostic flowchart (Figure 1), 5,163 patients presenting with angina pectoris as their primary complaint underwent coronary angiography. Among these, 1,547 individuals exhibited normal epicardial coronary artery morphology (coronary angiography showing <50% arterial stenosis). Following this preliminary screening, CMVD diagnosis was established through evaluation of coronary flow reserve (CFR). The diagnostic criteria required fulfillment of four conditions: symptoms of myocardial ischemia, absence of obstructive coronary artery disease, evidence of myocardial ischemia, and absence of epicardial spasm combined with a CFR measurement below 2.0, as outlined in established clinical guidelines.10
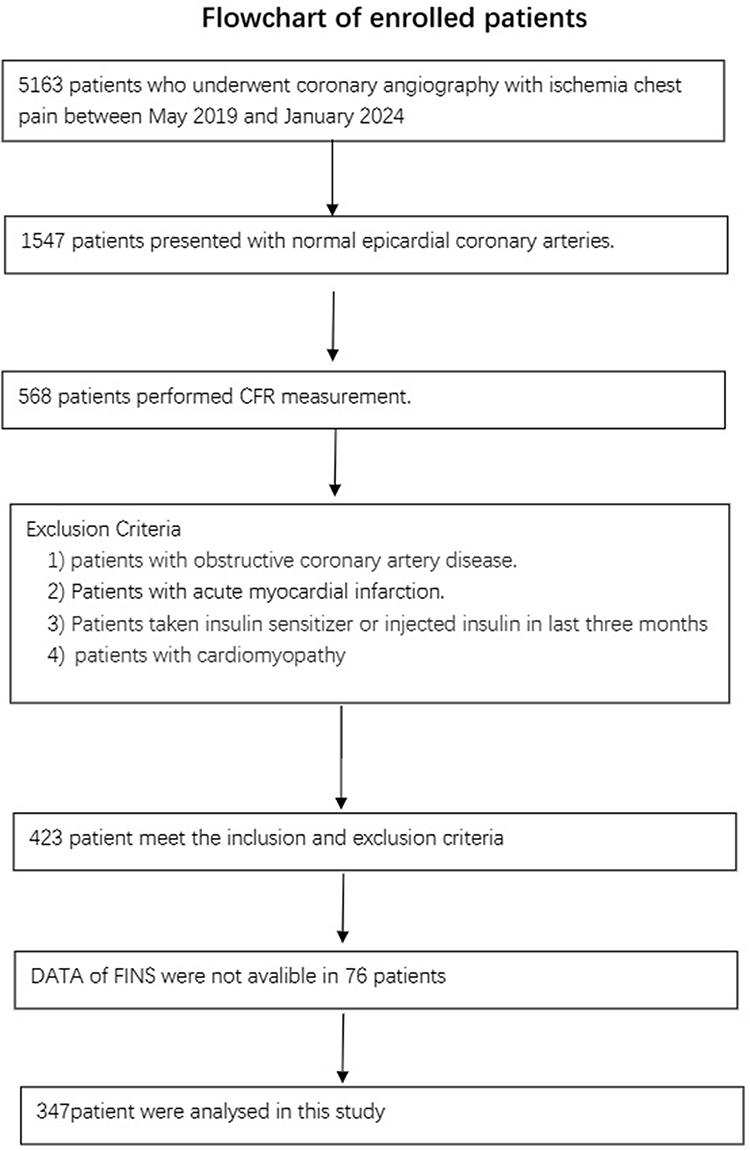 |
Figure 1 Flowchart of enrolled patients. |
Clinical data were collected, such as hypertension history, diabetes history, smoking history and history of medications.
Assessment of Coronary Flow Reserve
Coronary flow reserve assessment was conducted utilizing transthoracic Doppler echocardiographic techniques (VIVID 9 Ultrasound System, GE), adhering to protocols outlined in our prior research.11 All procedures were administered by a certified echocardiographer. Participants were instructed to abstain from caffeine and nitroglycerin consumption for 24 hours preceding the evaluation. Cardiac dimensional analysis included documentation of left ventricular chamber dimensions (LVD) and left atrial size (LAD), with left ventricular systolic function quantified through biplane Simpson’s volumetric analysis to determine LVEF values.
Coronary flow in the left anterior descending artery (LAD) was detected using color Doppler and an apical five-chamber view (distal of LAD) or by a modified low short-axis view (mid-distal of LAD).11 Baseline coronary flow velocity was measured. Adenosine was infused via the median cubital vein (140 µg/kg/min for 2 minutes), and the hyperemic peak diastolic velocity was measured. The CFR was calculated as the ratio of the hyperemic peak diastolic velocity divided by the baseline peak diastolic velocity.
Coronary blood flow within the left anterior descending artery (LAD) was assessed through color Doppler imaging, employing either an apical five-chamber view for distal LAD evaluation or a modified low short-axis approach for mid-distal LAD visualization.11 Initial hemodynamic parameters were established by recording baseline coronary flow velocities. Following intravenous administration of adenosine through the median cubital vein (140 µg/kg/min over two minutes), researchers captured hyperemic peak diastolic velocity measurements. The CFR was subsequently calculated as the ratio of the hyperemic peak diastolic velocity divided by the baseline peak diastolic velocity.
Laboratory Measurements
Fasting venous blood samples were obtained from participants following an 8-hour overnight fast. Biochemical analyses included total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), fasting blood sugar (FBS), and fasting insulin (FINS) levels. FINS concentrations were quantified using a dual-antibody sandwich immunoassay technique in accordance with standardized protocols. Insulin resistance was evaluated using the homeostasis model assessment formula [HOMA-IR (mmol/L×µU/mL) = FBS (mmol/L)×FINS (µU/mL)/22.5].12
Statistics Analysis
Statistical analyses were conducted with SPSS19 (SPSS, Chicago, IL, USA). For continuous variables, data were reported as mean ± standard deviation when data followed a normal distribution, while non-normally distributed variables were summarized using median values with interquartile ranges. Categorical data were presented numerically with corresponding percentages. Group comparisons for continuous measures employed either one-way ANOVA or the Kruskal–Wallis H-test based on distribution characteristics. Differences in categorical variables between groups were analyzed using χ2 tests or Fisher’s exact probability method as appropriate.
A multivariate logistic regression analysis was conducted to calculate adjusted odds ratios (ORs) along with corresponding 95% confidence intervals (CIs) for coronary microvascular disease risk factors. Statistical significance was defined as a two-tailed p-value below 0.05 based on conventional hypothesis testing criteria.
Results
Comparison of Clinical Data Between CMVD Patients and Non-CMVD Patients
As illustrated in Figure 1, the study recruited 347 participants, with 105 fulfilling diagnostic criteria for CMVD. The remaining 242 subjects demonstrating CFR values ≥2.0 comprised the non-CMVD cohort. No statistically significant differences were observed in smoking history between the two groups. However, the CMVD cohort demonstrated higher prevalence rates of female participants, diabetes mellitus, and hypertension compared to the non-CMVD group (P < 0.05, Table 1). Biochemical analysis revealed the CMVD group showed elevated fasting blood glucose, fasting insulin, HOMA-IR, and HbA1c levels relative to non-CMVD group. Lipid profiles (TC, TG, LDL-C, HDL-C) along with creatinine and homocysteine measurements showed comparable values across both cohorts. Echocardiographic parameters including left ventricular dimensions, atrial diameter, and ejection fraction exhibited no intergroup variations.
 |
Table 1 Comparison of Clinical Characteristics of CMVD and Non-CMVD Patients |
Hyperinsulinemia and Declined CFR Value
To investigate the association between insulin concentrations and CFR, participants were stratified into tertiles based on fasting insulin measurements (T1: ≤9.03 μIU/mL; T2: 9.04–12.40 μIU/mL; T3: >12.40 μIU/mL). Comparative analysis of baseline parameters revealed comparable distributions across age, gender prevalence, hypertension incidence, and smoking status among the three cohorts (Table 2). Lipid profiles (total cholesterol, triglycerides, LDL-C, HDL-C) along with renal function markers (creatinine, uric acid) showed no notable disparities. The T3 cohort demonstrated elevated HbA1c values, heightened insulin resistance (HOMA-IR), and increased homocysteine levels compared to lower insulin groups (Table 2). Echocardiographic measurements including left ventricular dimensions, atrial diameter, and ejection fraction remained comparable across all tertiles.
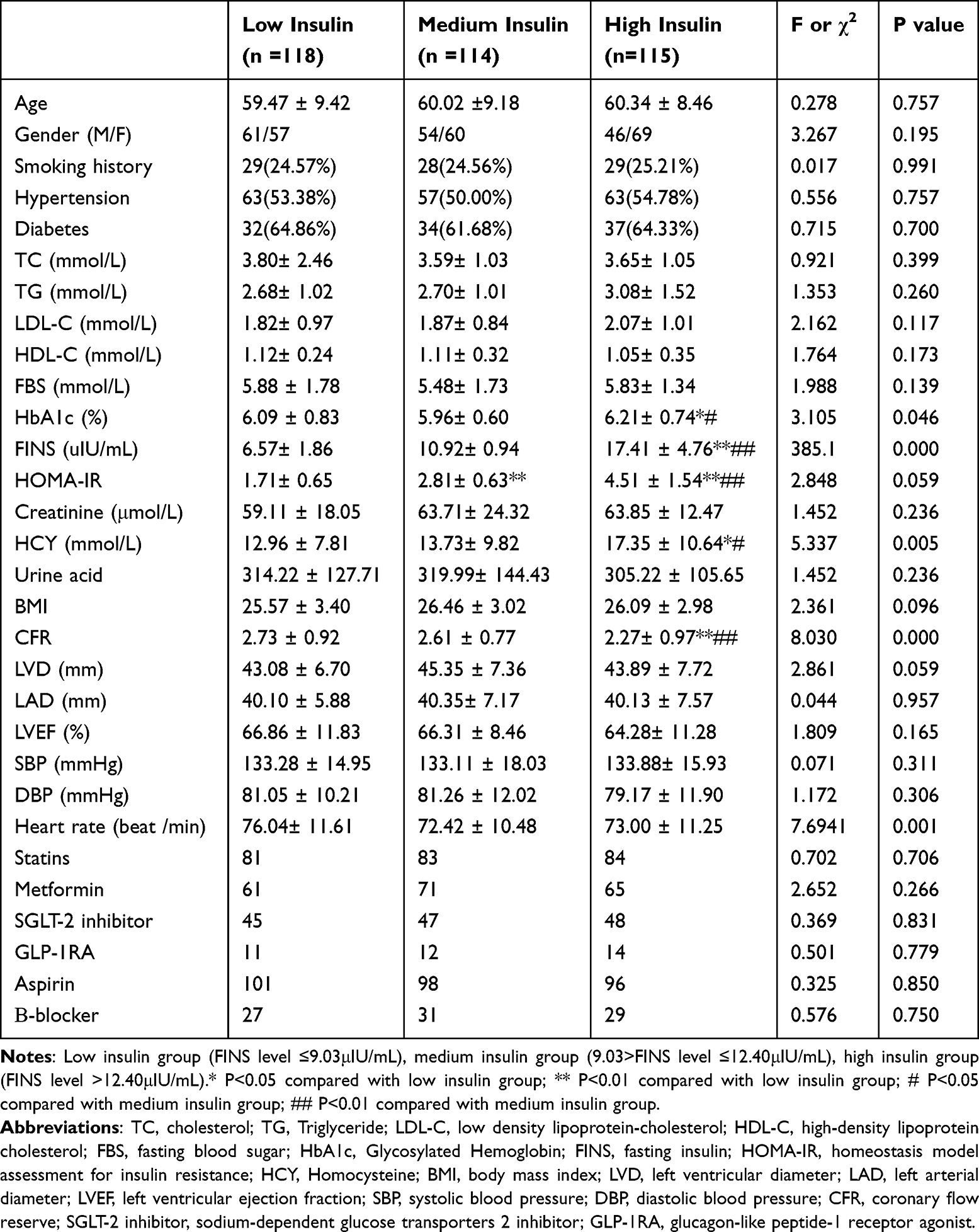 |
Table 2 Comparison of Clinical Characteristics According to FINS Status |
As shown in Figure 2, level of CFR was lower in high insulin group than in low insulin group and medium insulin group. There was no statistical difference of CFR between low insulin group and medium insulin group.
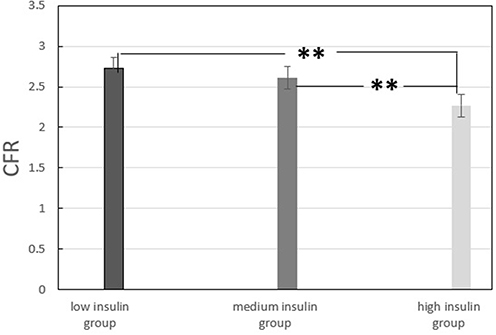 |
Figure 2 Comparison of CFR in different groups. Note: ** P<0.01 compared with high insulin group. |
Multivariate Logistic Regression Analysis
Table 3 presents the findings from multivariable logistic regression models. To investigate the relationship between insulin levels and CMVD, both categorical parameters (FINS tertiles) and continuous measurements (FINS concentrations) were examined. When evaluating categorical data, the highest FINS tertile (>12.4 μIU/mL) demonstrated a significant association with CMVD risk in adjusted models (adjusted OR 2.279, 95% CI 1.046–4.967). For continuous parameter evaluation, unadjusted analysis revealed a positive correlation between FINS concentrations and CMVD occurrence (OR 1.092, 95% CI 1.044–1.142, p<0.05). However, this relationship became statistically non-significant after comprehensive adjustment for covariates (adjusted OR 1.124, 95% CI 0.953–1.326, p=0.187).
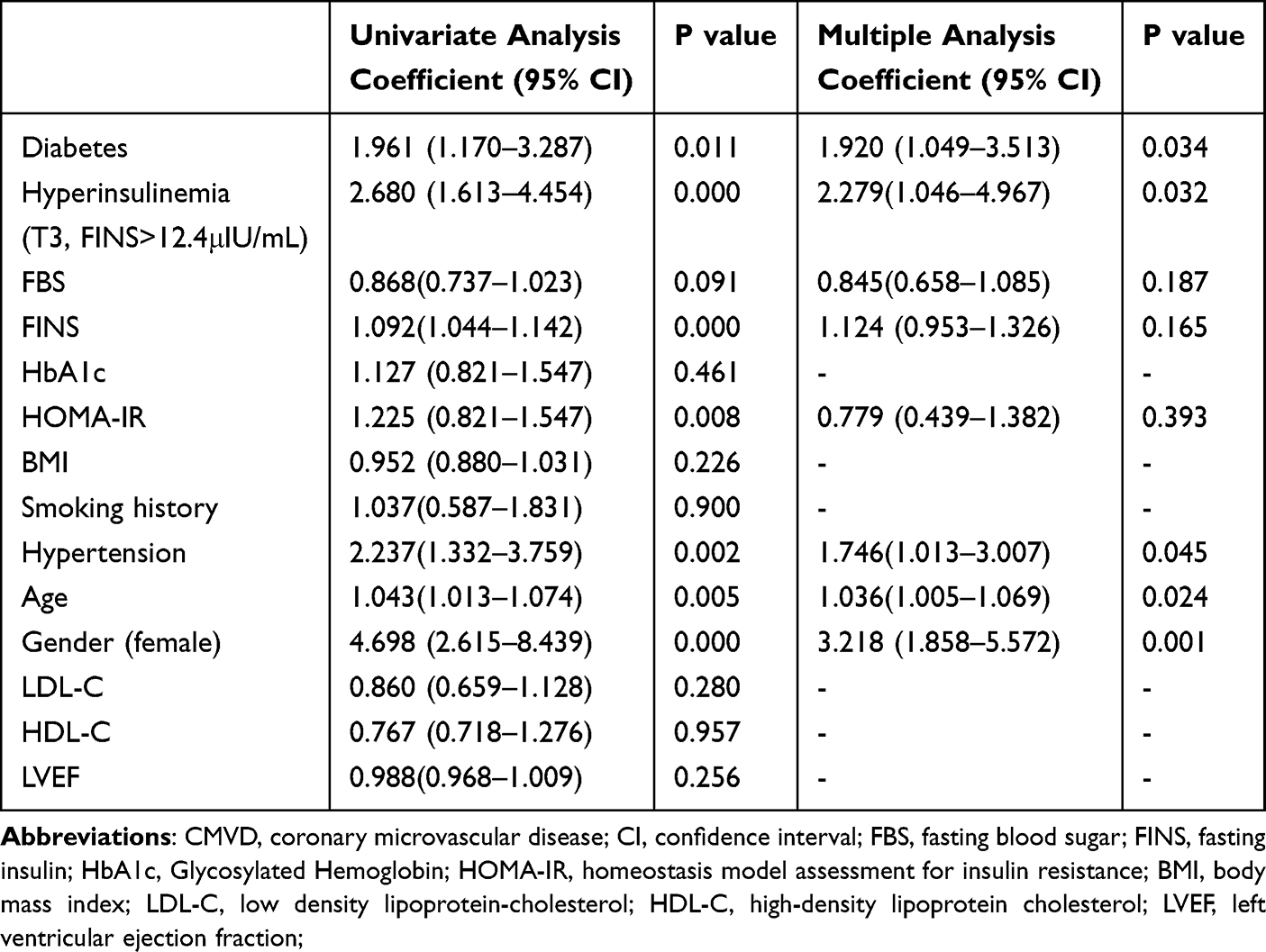 |
Table 3 Logistic Regression of Occurrence of CMVD in Patients with Chest Pain |
As Figure 3 showed, multivariate logistic regression further identified diabetes (OR 1.920,95% CI 1.049–3.513), female gender (OR 3.218, 95% CI 1.858–5.572), hypertension status (OR 1.746, 95% CI 1.013–3.007) and advancing age (OR 1.036, 95% CI 1.005–1.069) were independent factors of CMVD (all P < 0.05).
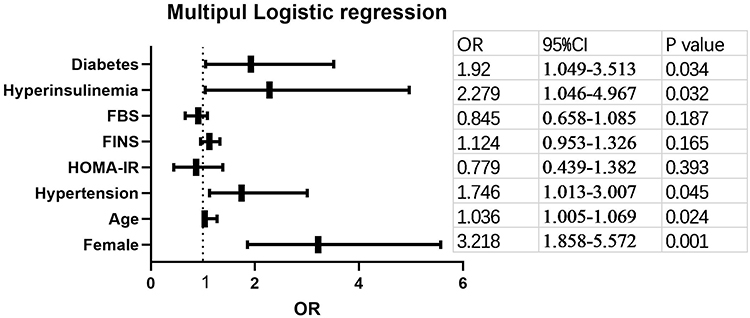 |
Figure 3 Multivariate logistic regression analysis for coronary microvascular disease. |
When evaluated as continuous parameters within multivariable regression models following comprehensive adjustment for confounding variables, FBS and HOMA-IR concentrations failed to demonstrate independent associations with CMVD.
Discussion
The main finding of this study reveals an association between elevated insulin levels and reduced coronary flow reserve. Hyperinsulinemia is an independent risk factor of coronary microvascular disease.
Myocardial ischemia stems not only from obstructive coronary artery disorders but also originates from coronary microvascular dysfunction.13 While atherosclerotic plaque deposition and blockage of major coronary arteries define occlusive coronary disease, CMVD arises from abnormalities in both structural integrity and functional capacity within coronary microvessels. Emerging research suggests that microvascular impairment might represent an initial phase in cardiovascular pathology development, with evidence indicating its potential emergence before or alongside atherosclerotic processes.14
Metabolic disorders including diabetes and prediabetes remain globally prevalent health concerns. Existing research has established that diabetes contributes to impaired microvascular function. In a clinical investigation utilizing dobutamine stress echocardiography for CFR measurement, Ahmari’s team observed significantly diminished CFR levels in diabetic patients compared to non-diabetic individuals.15 Takei et al’s research demonstrated that OGTT-triggered transient hyperglycemia significantly reduced CFR in individuals without preexisting diabetes mellitus or cardiovascular disorders.16 Recent evidence demonstrates that obesity is associated with coronary micovascular disease, which is mediated by viscarel adipose tissue and inflammation.17
Hyperinsulinemia represents a prevalent condition among individuals with diabetes and prediabetic states. While certain researchers propose insulin resistance as the triggering mechanism for hyperinsulinemia, alternative perspectives posit it as an underlying pathology.18 Previous investigations have documented elevated MACE incidence in hyperinsulinemic patients with obstructive coronary artery disease, though no prior studies specifically examined its microvascular implications in CMVD populations.19 Our investigation revealed significantly greater CMVD prevalence among hyperinsulinemic subjects compared to those with normal insulin levels. To our knowledge, this constitutes the inaugural exploration of hyperinsulinemia-CMVD correlations. The findings indicate a robust association between hyperinsulinemia and reduced coronary flow reserve, suggesting this metabolic abnormality may serve as an independent contributor to microvascular endothelial dysfunction.
While the precise mechanisms linking CMVD with hyperinsulinemia remain partially unclear, emerging evidence suggests endothelial dysfunction plays a mediating role. Elevated insulin levels have been shown to induce oxidative stress and inflammatory responses within both macrophages and vascular endothelial cells.20 This pathological process stimulates the release of pro-inflammatory mediators including various cytokines and interleukins, which collectively contribute to endothelial impairment.21 Furthermore, hyperinsulinemic conditions impair nitric oxide (NO) synthesis - a critical regulator of endothelium-dependent vasomotor function. Prior research from our team demonstrated that hyperinsulinemia downregulated phosphorylation of eNOS, PI3-K and Akt in endothelial progenitor cells.9 As a result, hyperinsulinemia reduced NO paracrine ability of endothelial progenitor cells.
Insulin-stimulated excessive growth of vascular smooth muscle cells (VSMCs) could represent a potential contributing factor to coronary microvascular impairment.22 Research has demonstrated that coronary microvessels may exhibit inward hypertrophic remodeling patterns during the development of coronary microvascular disease in type 2 diabetes and metabolic syndrome. Furthermore, these structural alterations in microvascular architecture might progressively compromise blood flow regulation within myocardial tissue.
Jin et al investigated the pathological mechanisms of vascular intimal thickening through a type 2 diabetic murine model. Their research demonstrated that insulin administration significantly enhanced aortic smooth muscle cell proliferation and migratory capacity via CDKN2B-AS1 overexpression.23 This finding suggests that elevated insulin levels potentially exacerbate post-traumatic neointimal formation and contribute to arterial wall rigidity following vascular endothelial damage.
Limitations
The current study presents several limitations. The primary limitation arises from its retrospective design, which introduced potential selection bias due to incomplete medical records, ultimately restricting participant numbers. The interpretations of this study need more cautious given its retrospective design. A second methodological gap concerns the absence of follow-up for CMVD patients. Existing evidence identifies compromised coronary microvascular function as a robust predictor of adverse clinical outcomes, yet our study did not assess potential correlations between hyperinsulinemia and prognostic trajectories in CMVD populations. The third limitation arises from its single-center setting and absence of external validation. Future prospective and multi-center studies should prioritize extended observation periods to clarify insulin resistance’s role in determining clinical progression for these patients.
Conclusions
The investigation revealed an association between elevated insulin concentrations and occurrence of coronary microvascular disease. Hyperinsulinemia may serve as a critical contributing element in the development of coronary microvascular pathophysiology, suggesting potential metabolic mechanisms underlying vascular endothelial impairment.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by ethics committee of Qinhuangdao First Hospital. And all patients provided their written informed consent.
Funding
This manuscript was supported by Hebei medical technology project (20231399), S&T program of Qinhuangdao (202201B016), S&T program of Qinhuangdao (201805A031).
Disclosure
The authors declare that they have no competing interests.
References
1. Bradley C, Berry C. Definition and epidemiology of coronary microvascular disease. J Nucl Cardiol. 2022;29(4):1763–1775. doi:10.1007/s12350-022-02974-x
2. Taqueti VR, Di Carli MF. Coronary microvascular disease pathogenic mechanisms and therapeutic options: JACC state-of-the-art review. J Am Coll Cardiol. 2018;72(21):2625–2641. doi:10.1016/j.jacc.2018.09.042
3. Pepine CJ, Ferdinand KC, Shaw LJ, et al. Emergence of nonobstructive coronary artery disease: a woman’s problem and need for change in definition on angiography. J Am Coll Cardiol. 2015;66(17):1918–1933. doi:10.1016/j.jacc.2015.08.876
4. Thakker RA, Rodriguez LJ, Rodriguez LP, et al. Coronary microvascular disease. Cardiol Ther. 2022;11(1):23–31. doi:10.1007/s40119-021-00250-6
5. Tagliamonte E, Cirillo T, Rigo F, et al. Ivabradine and bisoprolol on doppler-derived coronary flow velocity reserve in patients with stable coronary artery disease: beyond the heart rate. Adv Ther. 2015;32(8):757–767. doi:10.1007/s12325-015-0237-x
6. Zdravkovic M, Popadic V, Klasnja S, et al. coronary microvascular dysfunction and hypertension: a bond more important than we think. Medicina. 2023;59(12):2149. doi:10.3390/medicina59122149
7. Salvatore T, Galiero R, Caturano A, et al. Coronary microvascular dysfunction in diabetes mellitus: pathogenetic mechanisms and potential therapeutic options. Biomedicines. 2022;10(9):2274. doi:10.3390/biomedicines10092274
8. Zou X, Chen M, Sun L, Tan Q. Hyperinsulinemia impaired coronary collateral circulation in patients with chronic total coronary occlusion. Diabetes Metab Syndr Obes. 2023;16:1425–1433. doi:10.2147/DMSO.S402849
9. Tan Q, Li Y, Li X, Zhang S. Hyperinsulinemia impairs functions of circulating endothelial progenitor cells. Acta Diabetol. 2019;56(7):785–795. doi:10.1007/s00592-019-01314-9
10. Ong P, Camici PG, Beltrame JF, et al. International standardization of diagnostic criteria for microvascular angina. Int J Cardiol. 2018;250:16–20. doi:10.1016/j.ijcard.2017.08.068
11. Wang Q, Hao J, Jiang W, Tan Q. Enhanced external counterpulsation increases coronary flow reserve in coronary microvascular disease. Saudi Med J. 2023;44(12):1277–1282. doi:10.15537/smj.2023.44.12.20230427
12. Li Y, Tan Q, Guo Y, et al. The influence of exercise training on endothelial function, serum irisin and inflammatory markers in the elderly with metabolic syndrome. Clin Lab. 2021;67(3):689–696. doi:10.7754/Clin.Lab.2020.200446
13. Del Buono MG, Montone RA, Camilli M, et al. Coronary microvascular dysfunction across the spectrum of cardiovascular diseases: JACC state-of-the-art review. J Am Coll Cardiol. 2021;78(13):1352–1371. doi:10.1016/j.jacc.2021.07.042
14. Bairey Merz CN, Pepine CJ, Shimokawa H, Berry C. Treatment of coronary microvascular dysfunction. Cardiovasc Res. 2020;116(4):856–870. doi:10.1093/cvr/cvaa006
15. Ahmari SA, Bunch TJ, Modesto K, et al. Impact of individual and cumulative coronary risk factors on coronary flow reserve assessed by dobutamine stress echocardiography. Am J Cardiol. 2008;101(12):1694–1699. doi:10.1016/j.amjcard.2008.02.055
16. Takei Y, Tomiyama H, Tanaka N, Yamashina A, Chikamori T. Association between insulin resistance, oxidative stress, sympathetic activity and coronary microvascular function in patients with early stage impaired glucose metabolism. Circ J. 2022;86(5):866–873. doi:10.1253/circj.CJ-21-0549
17. Cesaro A, De Michele G, Fimiani F, et al. Visceral adipose tissue and residual cardiovascular risk: a pathological link and new therapeutic options. Front Cardiovasc Med. 2023;10:1187735. doi:10.3389/fcvm.2023.1187735
18. Erion KA, Corkey BE. Hyperinsulinemia: a cause of obesity? Curr Obes Rep. 2017;6:178–186. doi:10.1007/s13679-017-0261-z
19. Tan Q, Chen M, Hao J, Wei K. Impact of hyperinsulinemia on long-term clinical outcomes of percutaneous coronary intervention in patients without diabetes who have acute myocardial syndrome. Diabetes Metab Syndr Obes. 2021;14:3949–3957. doi:10.2147/DMSO.S318852
20. Mahmoud AM, Szczurek MR, Blackburn BK, et al. Hyperinsulinemia augments endothelin-1 protein expression and impairs vasodilation of human skeletal muscle arterioles. Physiol Rep. 2016;4(16):e12895. doi:10.14814/phy2.12895
21. Incalza MA, D’Oria R, Natalicchio A, Perrini S, Laviola L, Giorgino F. Oxidative stress and reactive oxygen species in endothelial dysfunction associated with cardiovascular and metabolic diseases. Vascul Pharmacol. 2018;100:1–19. doi:10.1016/j.vph.2017.05.005
22. Mackesy DZ, Goalstone ML. Insulin augments tumor necrosis factor-alpha stimulated expression of vascular cell adhesionmolecule-1 in vascular endothelial cells. J Inflam. 2011;8:34–38. doi:10.1186/1476-9255-8-34
23. Sehgel NL, Vatner SF, Meininger GA. “smooth muscle cell stiffness syndrome”-revisiting the structural basis of arterial stiffness. Front Physiol. 2015;6:335. doi:10.3389/fphys.2015.00335
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treating Alpelisib-Induced Hyperinsulinemia in Patients with Advanced Breast Cancer – A Real-Life Experience
Percik R, Oedegaard Smith C, Leibovici A, Shai A
Biologics: Targets and Therapy 2023, 17:61-67
Published Date: 3 May 2023
Exogenous Insulin Antibody Syndrome in Patients with Type 2 Diabetes
Han CY, Ye XM, Lu JP, Jin HY, Xu WW, Wang P, Zhang M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1895-1902
Published Date: 26 June 2023