Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Exogenous Insulin Antibody Syndrome in Patients with Type 2 Diabetes
Authors Han CY, Ye XM, Lu JP, Jin HY, Xu WW, Wang P, Zhang M
Received 7 March 2023
Accepted for publication 3 June 2023
Published 26 June 2023 Volume 2023:16 Pages 1895—1902
DOI https://doi.org/10.2147/DMSO.S410349
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Chen-Yu Han, Xiao-Mei Ye, Jia-Ping Lu, Hai-Ying Jin, Wei-Wei Xu, Ping Wang, Min Zhang
Department of Endocrinology, Qingpu Branch of Zhongshan Hospital Affiliated to Fudan University, Shanghai, 201700, People’s Republic of China
Correspondence: Min Zhang, Department of Endocrinology, Qingpu Branch of Zhongshan Hospital Affiliated to Fudan University, No. 1158 of Gongyuan Road, Qingpu District, Shanghai, 201700, People’s Republic of China, Tel +86 18116016187, Fax +86 021-69719190, Email [email protected]
Background: Exogenous insulin antibody syndrome (EIAS) is an immunological disorder caused by circulating insulin antibodies (IAs), featuring hypersensitivity to exogenous insulin and insulin resistance. With the wide use of recombinant human insulin and insulin analogs, there has been a significant proliferation of EIAS.
Case Report: We describe two cases of diabetes mellitus (DM) with hyperinsulinemia and high serum levels of IAs. They had never been exposed to methimazole, glutathione, lipoic acid, and other sulfhydryl drugs, but they all received insulin treatment. The patient in case 1 had recurrent hypoglycemia before hospitalization. A prolonged oral glucose tolerance test (OGTT) showed hypoglycemia with inappropriately high insulin levels. The patient in case 2 was hospitalized for diabetic ketosis. An OGTT indicated hyperglycemia with hyperinsulinemia and low levels of C-peptide. IAs induced by exogenous insulin in the two patients with DM were positive at high titers, prompting a diagnosis of another condition—EIAS.
Conclusion: We discussed the differences between these two cases of EIAS in clinical manifestations and treatment and summarized all patients of EIAS treated in our department to date.
Keywords: diabetes mellitus, exogenous insulin, hyperinsulinemia, insulin antibodies, IAs
Introduction
Classical insulin autoimmune syndrome (IAS) is a rare autoimmune condition caused by the presence of endogenous antibodies that bind insulin and/or proinsulin.1 It features high serum levels of insulin autoantibody (IAA), hyperinsulinemia, hypoglycemia, and no history of exposure to exogenous insulin.2 Hypoglycemia usually develops 2–6 h after meals, following an early postprandial hyperglycemia. In the peripheral blood, a large amount of insulin and/or proinsulin was bound to IAA, just like a reservoir. When insulin and/or proinsulin were separated from IAA, bioactive insulin was released into the blood and continued to cause hypoglycemia of varying severity, usually within 2 h to 6 h or longer.3 In recent years, glycemic dysregulation and hypoglycemia cases in individuals receiving exogenous insulin therapy have accumulated in patients with diabetes mellitus (DM). These patients have been labeled as having IAS, but more recently, the term exogenous insulin antibody syndrome (EIAS) has been used to distinguish this group of patients from those with IAS.4–6 EIAS is an immunological disorder caused by circulating insulin antibodies (IAs), featuring hypersensitivity to exogenous insulin and insulin resistance. With the wide use of recombinant human insulin and insulin analogs, there has been a significant proliferation of EIAS. The essential characteristics of this condition are glycemic dysregulation manifesting as episodes of hyperglycemia and unpredictable hyperinsulinemic hypoglycemia associated with high titers of IAs.7 EIAS is determined by genetic instability, immunogenicity, formulation, and injection mode of insulin.8 Previous studies indicated that the presence of histocompatibility leukocyte antigen (HLA)-DR4 and HLA-DR7 may increase the titers of IAA.9 Recombinant human insulin and insulin analogs are generally used at present. Although the amino acid sequence of recombinant human insulin is consistent with human insulin, it can induce IAs.10 There is no significant difference in the production of IAs between insulin analogs in which amino acid sequences have been slightly modified by the recombinant human insulin.11 However, levels of IAs may increase following the delivery of recombinant human insulin with implantable insulin pumps (IIPs), prompting the need for applying surfactants or polyethylene glycol on the surface of pump reservoirs.12 Nevertheless, evidence of EIAS is limited. The exact incidence, clinical features, and genetic susceptibility of EIAS are still unclear. In this study, we collected clinical cases to summarize the manifestation, genetic susceptibility, and treatment of EIAS.
Case Report 1
A 49-year-old male came to our hospital to seek medical advice in May 2020 with frequent episodes of hypoglycemia. Since January 2020, he had experienced recurrent attacks of dizziness, palpitations, tremors, and sweating, both when fasting and after meals, with a documented hypoglycemia (peripheral blood glucose levels were approximately 2.8–3.5 mmol/L). The symptoms were relieved after food intake. He had a history of type 2 diabetes (T2D) for 10 years. His glucose concentration was well controlled initially after diagnosis with metformin. One year ago, metformin was changed to Novolin 30R for weight loss. He denied suffering from hyperthyroidism and other autoimmune diseases, and using glutathione and lipoic acid. Then, he was hospitalized for frequent hypoglycemia. On physical examination, he was healthy, with a Body Mass Index(BMI) of 19.1 kg/m2. A tentative diagnosis of insulinoma prompted a negative abdominal computed tomography (CT) scan. The laboratory findings, the level of growth hormones, thyroid, and adrenal function were all normal except for slightly increased antibodies to a cyclic citrullinated peptide (ACCP) at 17.36 u/mL (average value: < 1 u/mL). The IA test revealed that the class of immunoglobulins was 35.43 U/mL [average value: 0.00–0.40 U/mL, radioligand-binding assay (RBA)]. The HLA allele of this patient was DRB1*0405.
A 300-min oral glucose tolerance test (OGTT) of 82.5g anhydrous glucose was carried out on 07:00 07/06/2020 to investigate reactive hypoglycemia: the basal glucose level was 5.60 mmol/L, with a maximum level of 17.20 mmol/L at 120 min and a nadir of 3.20 mmol/L at 300 min. The plasma insulin ranged from a basal level of 732.10 mIU/L to a peak of 1420.00 mIU/L at 120 min. C-peptide levels (average value: 0.37–1.47mmol/L) were 1.43 nmol/L at the baseline and 3.16 nmol/L at the peak. The islet function of the patient exists, but C-peptide secretion was insufficient after glucose stimulation. The patient underwent 54.9 hours of continuous glucose monitoring (CGM) after admission, which revealed: time in range (TIR) (3.9 mmol/L < PT < 10 mmol/L) of 41.30% (22 h 40 min), time above range (TAR) (PT > 13.9 mmol/L) of 21.67% (11 h 53 min), time below range TBR (PT <3.9 mmol/L) of 6.76% (3 h 42 min). Hypoglycemia occurred between 12 a.m. to 4 a.m. He was treated with acarbose (100 mg three times a day) instead of insulin injections and prescribed to take leflunomide for rheumatoid arthritis. During the subsequent follow-up, the hypoglycemic episodes became less frequent and ceased altogether after a few months. The IAs assay and a 180-min OGTT were repeated at 8 and 15 months after the diagnosis of EIAS (see Table 1 and Figure 1).
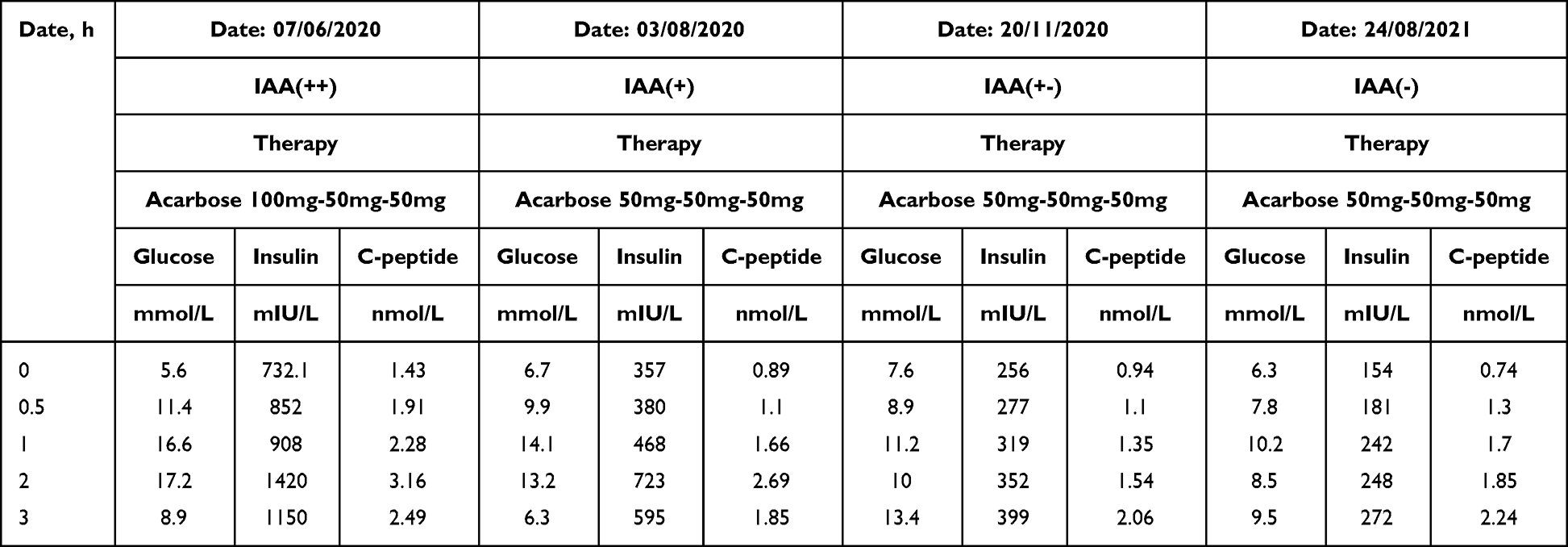 |
Table 1 Laboratory Investigations of Case 1 |
 |
Figure 1 Glucose, insulin, and C-peptide in the OGTT of case 1 before and after treatment. |
Case Report 2
A 65-year-old female was admitted in September 2020 for diabetic ketosis. She had a history of T2D for 16 years. Acarbose and metformin were initially prescribed but were switched to insulin Aspart 30 (20–15 units twice a day) because of poor glucose control since November 2019. She denied a history of using lipoic acid and any drug containing sulfur/sulfhydryl groups (eg, thiols with -SH) such as methimazole, captopril, D-penicillamine, hydralazine, glutathione, methionine, mercaptans, clopidogrel, aurothioglucose, imipenem, penicillin G, and diltiazem.12–14 Since June 2020, she had experienced polydipsia and a 10 kg weight loss without any symptoms of hypoglycemia. Her peripheral blood sugar concentrations increased to 20 mmol/L. The patient sought medical advice from our Endocrine Unit. Laboratory tests showed positive ketone body, hyperinsulinemia, and positive IAs. After being admitted to our hospital, her physical examination found her to be very thin, with a BMI of 17.71 kg/m2. Laboratory findings, the level of growth hormone, thyroid and adrenal function, and indexes of autoimmune antibodies were all normal except for hyperlipidemia. Thyroid B-ultrasound and abdominal CT scan were negative. The IAs test revealed that the class of immunoglobulins were strongly positive (3+): > 50 U/mL (average value: 0.00–0.40 U/mL, RBA). The HLA allele of this patient was DRB1*0403.
A 300-min OGTT 82.5g anhydrous glucose was carried out on 07:00 11/09/2020: the basal glucose level was 13.60 mmol/L, with a maximum level of 22.30 mmol/L at 180 min. The plasma insulin ranged from a basal level of 531.50 mIU/L to a peak of 973.00 mIU/L at 240 min, and C-peptide levels (average value: 0.37–1.47mmol/L) were 0.41 nmol/L at the baseline and 0.87 nmol/L at the peak. CGM was performed for 72 hours after admission, which revealed: TIR (3.9 mmol/L <PT <10 mmol/L) of 4.15% (2 h 59 min), TAR (PT > 13.9 mmol/L) of 95.85% (69 h 1 min), TBR (PT <3.9 mmol/L) of 0% (0 min). The patient was hospitalized due to an acute complication of diabetes (diabetic ketosis), and her pancreatic islet function was inferior. After hospitalization, she was continuously monitored for hyperglycemia instead of hypoglycemia. After an intravenous infusion of a small dose of insulin and a large amount of liquid supplement, the ketosis of the patient was relieved. Intensive insulin treatment was given to her after she turned negative for ketone bodies; however, the glucose did not drop significantly compared with that before treatment. Her treatment regimen was changed to acarbose (50 mg three times a day), metformin (0.5 g twice a day), and glargine (18 units once a day). In addition, prednisone was added (5 mg three times a day) for five days. Following this treatment, her glucose level improved gradually. The laboratory tests during follow-ups are shown in Table 2 and Figure 2.
 |
Table 2 Laboratory Investigations of Case 2 |
 |
Figure 2 Glucose, insulin, and C-peptide in the OGTT of case 2 before and after treatment. |
Discussion
The two cases described here had a definite history of diabetes and exogenous insulin therapy before admission. Both patients denied using drugs containing sulfur/sulfhydryl groups or viral infections/reinfections. The condition featured hyperinsulinemia, high serum levels of IAs, and an overt history of exposure to exogenous insulin. The levels of insulin and IAs decreased gradually after withdrawal or changed to another type of exogenous insulin. Therefore, we temporarily identified these cases as EIAS.
The patient in case 1 was admitted for frequent hypoglycemia. The C-peptide levels in the OGTT showed that the islet function of the patient exists, hence he was treated with acarbose (100 mg three times a day) instead of insulin injections. It has been reported that α-glucosidase inhibitors can lower plasma IAs concentrations significantly.13 After stopping exogenous insulin, hypoglycemia gradually improved, and titers of IAs dropped. However, the patient in case 2 never experienced hypoglycemia. It goes to show that patients with EIAS may paradoxically manifest hyperglycemia. During the treatment of this patient, combination of multiple oral hypoglycemic drugs were used successively, but blood glucose of this patient has not been ideal. Considering the poor pancreatic function of this patient, insulin therapy was added. Asparagus 30 was replaced with insulin glargine, with a combination of metformin and acarbose capsules. Besides, prednisone was added (5 mg three times a day) for five days. Following this treatment, her glucose levels improved gradually.
We have treated 17 patients with EIAS since January 2020 (see Table 3 and Table 4 for details). All of them were diabetic patients and had received exogenous insulin therapy. Among the 17 patients, 16 were adults (median age, 58.47±15.79 years; range, 44–77 years) and 1 was a juvenile (16 years old) with type 1 diabetes (T1D). Seven patients developed EIAS after exposure to Aspart 30; two were exposed to Humulin 70/30, one was exposed to Novolin 30R, two were exposed to Lispro 25, and one was exposed to Aspart and Detemir. Two of them had other autoimmune conditions (1 with chronic thyroiditis and 1 with high ANA titers) (see Table 2). None of these cases in our hospital were associated with Graves’ disease, probably because patients with EIAS tend to be associated with DRB1*0405, which differs from the HLA DRB1*0406 found in Japanese patients with IAS.14 HLA results were available for the 16 patients with EIAS: six were DRB1*0405, four were DRB1*0301, four were DRB1*1202, and two were DRB1*0901. In the current case series, all patients with EIAS were lean, with a mean BMI of 19 kg/m2. Although none of these patients were overweight or obese, 9 out of the 17 patients suffered from dyslipidemia. In the patient in case 2, the highest cholesterol was 9.65 mmol/L, and the highest triglyceride was 10.45 mmol/L (see Table 3 for details). Whether there is a direct relationship between dyslipidemia and EIAS needs further discussion in future research.
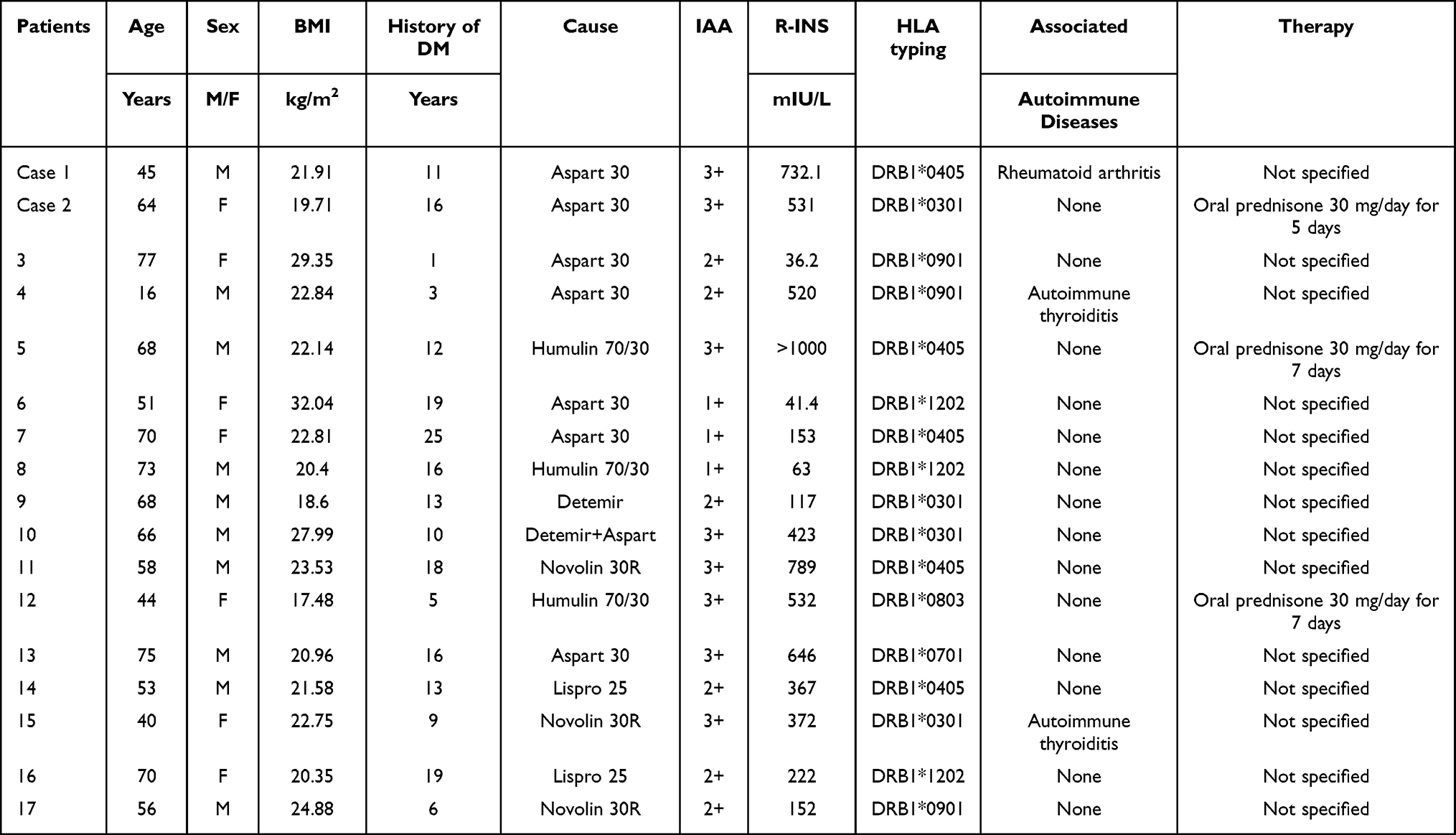 |
Table 3 List of Medications and HLA Typing of Patients Reported in Case Series |
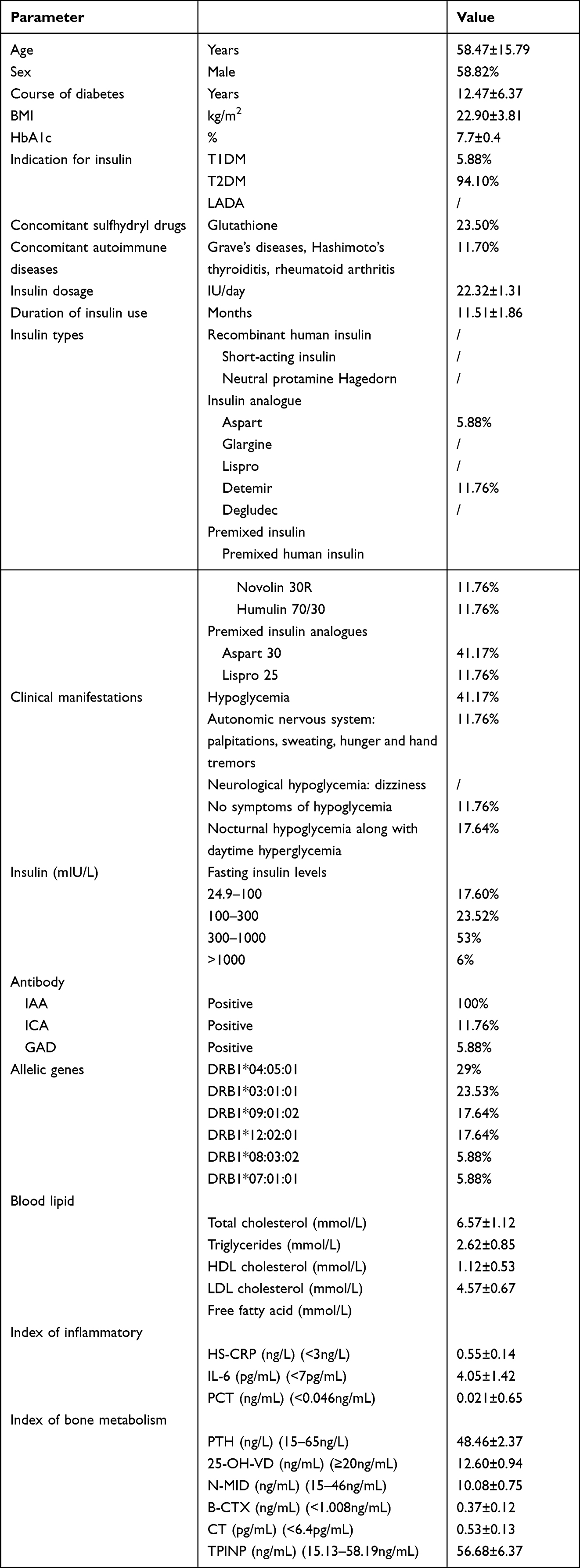 |
Table 4 General Data and Clinical Information of Patients Reported in Case Series |
The main symptom of EIAS is the fluctuation of blood glucose instead of severe spontaneous hypoglycemia. Most EIAS patients tend to have nocturnal hypoglycemia and postprandial hyperglycemia, as it was with the patient in case 1. A suggested mechanism of postprandial hyperglycemia is insufficient endogenous insulin secretion after meals and ineffective action of exogenous insulin bound to IAs. This results in prolonged pancreatic secretion of insulin and C-peptide in equimolar amounts until the IAs binding capacity is exceeded. However, this combination is reversible—when insulin dissociates continuously according to the intrinsic dissociation rate constant, a large amount of free insulin appears in the blood, resulting in hypoglycemia.15
The treatment of EIAS is the same as that of IAS, aiming at eliminating antibodies and stabilizing blood glucose. Based on the islet function of the patient, either the use of insulin should be stopped or another type of insulin used, to reduce the production of antibodies. The function of the pancreatic islet of the patient in case 1 was good, but hypoglycemia frequently occurred, so he was treated with acarbose (100 mg three times a day) instead of insulin injections. However, in the patient in case 2, due to the poor islet function, the type of insulin was changed. We prefer to switch to a different kind of insulin if the islet function appears poor. If the patient’s islet function is good, we prefer gradually reducing the insulin dose and adding oral drugs. A small prospective research study demonstrated that IAs have a long half-life in the body, which decreases gradually within one month after insulin withdrawal.16 However, it will take 1–2 years for antibodies to disappear completely.17 From January 2020, only 3 out of the 17 patients with EIAS that we followed up were negative for IAs. It has been reported that glucocorticoids may inhibit insulin antibody production or promote insulin antibody immune complex dissociation.18 So, steroids were used to treat patients with IAS and EIAS in clinical practice, although they may aggravate hyperglycemia. In the study, IAs titers and insulin levels of the patient in case 2 decreased after steroid treatment, and her blood glucose stabilized gradually. However, discontinuing the previous insulin treatment and switching to steroid treatment may worsen glucose control in some patients.19 Due to technical limitations, we did not classify IAs and did not conduct a PEG test to determine the generation of the complex. This is the limitation of the study.
Conclusion
EIAS is an immunological disorder caused by circulating IAs, featuring hypersensitivity to exogenous insulin and insulin resistance. With the wide use of recombinant human insulin and insulin analogs, there has been a significant proliferation of EIAS. We discussed the differences between these two cases of EIAS in clinical manifestations and treatment and summarized all patients of EIAS treated in our department to date. The main symptom of EIAS is the fluctuation of blood glucose instead of severe spontaneous hypoglycemia. Changing insulin formulations or discontinuing insulin and switching to oral antidiabetic agents are effective treatments for EIAS. Glucocorticoids are generally part of empirical treatments, though the mechanism behind their therapeutic effect is yet to be clarified.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Qingpu Branch of Zhongshan Hospital affiliated to Fudan University. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for Publication
All participants signed a document of informed consent.
Funding
Shanghai Municipal Health Commission (No. 20204Y0060); Science and Technology Development Fund Project of Qingpu District in Shanghai (No. QKY2021-03).
Disclosure
The authors declare that they have no competing interests.
References
1. Ismail AA. The insulin autoimmune syndrome (IAS) as a cause of hypoglycaemia: an update on the pathophysiology, biochemical investigations and diagnosis. Clin Chem Labor Med. 2016;54(11):1715–1724. doi:10.1515/cclm-2015-1255
2. Censi S, Albergoni MP, Gallo N, et al. Insulin autoimmune syndrome (Hirata’s disease) in an Italian patient: a case report and review of the literature. Clin Chem Labor Med. 2018;56(6):889–895. doi:10.1515/cclm-2017-0392
3. Lin MX, Chen Y, Ning J, et al. Insulin autoimmune syndrome: a systematic review. Int J Endocrinol. 2023;2023:1225676. doi:10.1155/2023/1225676
4. Hu X, Chen F. Exogenous insulin antibody syndrome (EIAS): a clinical syndrome associated with insulin antibodies induced by exogenous insulin in diabetic patients. Endocr Connect. 2018;7(1):R47–R55. doi:10.1530/EC-17-0309
5. Robbins DJ, Taylor NE, Narayanan D, et al. Therapeutic plasma exchange for exogenous insulin antibody syndrome in combined variable immunodeficiency: a case report. J Clin Apher. 2020;35(2):128–130. doi:10.1002/jca.21769
6. Fineberg SE, Kawabata TT, Finco-Kent D, et al. Immunological responses to exogenous insulin. Endocr Rev. 2007;6(6):625–652. doi:10.1210/er.2007-0002
7. Saleem M, Martin H, Coates P, et al. Prolactin biology and laboratory measurement: an update on physiology and current analytical issues. Clin Biochem. 2018;39(1):3–16. doi:10.1210/jc.2010-1692
8. Li Z, Yi D, Zheng L, et al. Analysis of the clinical characteristics of insulin autoimmune syndrome induced by exogenous insulin in diabetic patients. Diabetol Metab Syndr. 2021;13:138. doi:10.1186/s13098-021-00658-z
9. Cappellani D, Macchia E, Falorni A, et al. Insulin autoimmune syndrome (Hirata Disease): a comprehensive review fifty years after its first description. Diabetes Metabol Syndr Obesity. 2020;13:963–978. doi:10.2147/DMSO.S219438
10. Sauerborn M, Brinks V, Jiskoot W, et al. Immunological mechanism underlying the immune response to recombinant human protein therapeutics. Trends Pharmacol Sci. 2010;31(2):53–59. doi:10.1016/j.tips.2009.11.001
11. Lindholm A, Jensen LB, Home PD, et al. Immune responses to insulin aspart and biphasic insulin aspart in people with type 1 and type 2 diabetes. Diabetes Care. 2002;25(5):876–882. doi:10.2337/diacare.25.5.876
12. Olsen CL, Chan E, Turner DS, et al. Insulin antibody responses after long-term intraperitoneal insulin administration via implantable programmable insulin delivery systems. Diabetes Care. 1994;17(3):169–176. doi:10.2337/diacare.17.3.169
13. Feingold KR. Atypical forms of diabetes. In: Feingold KR, editor. Endotext. MDText.com, Inc.; 2022.
14. Patel M, Shah R, Ramteke‐Jadhav S, et al. Management of insulin autoimmune hypoglycaemia: single-centre experience from Western India with systematic review of world literature. Clin Endocrinol (Oxf). 2020;92(5):409–420. doi:10.1111/cen.14174
15. Boro H, Gupta U, Singh C, et al. Insulin autoimmune syndrome - a case series. Eur Endocrinol. 2020;16(2):168–171. doi:10.17925/EE.2020.16.2.168
16. Sutkowska E, Ostrowska M, Sutkowska M, et al. Insulin autoimmune syndrome as part of pre-clinical LADA. Diabetes Metabol Syndr Obesity. 2021;14:1557–1561. doi:10.2147/DMSO.S302874
17. Douillard C, Jannin A, Vantyghem M-C, et al. Rare causes of hypoglycemia in adults. Annales d’endocrinologie. 2020;81(2–3):110–117. doi:10.1016/j.ando.2020.04.003
18. Okuroglu N, Sertbas M, Akkoz C, et al. Insulin autoimmune syndrome - time to remember. Endokrynol Pol. 2020;71(2):204–205. doi:10.5603/EP.a2019.0065
19. Sima A, Vlad AR, Timar B, et al. Insulin autoimmune syndrome in a young caucasian woman. Acta Endocrinol. 2021;17(2):248–250. doi:10.4183/aeb.2021.248
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treating Alpelisib-Induced Hyperinsulinemia in Patients with Advanced Breast Cancer – A Real-Life Experience
Percik R, Oedegaard Smith C, Leibovici A, Shai A
Biologics: Targets and Therapy 2023, 17:61-67
Published Date: 3 May 2023
Relationship Between Hyperinsulinemia and Coronary Microvascular Disease
Tan Q, Zu C, Zhang W, Hao J, Li Y, Lu Q, Li Z, Guo Y
Diabetes, Metabolic Syndrome and Obesity 2025, 18:3931-3940
Published Date: 25 October 2025