Back to Journals » Journal of Pain Research » Volume 16
Relationship Between Chronic Pain Types (Nociceptive and Neuropathic-Like Symptoms) and Frailty in Community-Dwelling Japanese Older Adults: A Cross-Sectional Study
Authors Saito T ![]() , Liu X, Yatsugi H, Chu T, Yokote T, Kishimoto H
, Liu X, Yatsugi H, Chu T, Yokote T, Kishimoto H ![]()
Received 19 December 2022
Accepted for publication 30 May 2023
Published 1 August 2023 Volume 2023:16 Pages 2675—2684
DOI https://doi.org/10.2147/JPR.S402002
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Takafumi Saito,1 Xin Liu,2 Harukaze Yatsugi,3 Tianshu Chu,2 Tsubasa Yokote,2 Hiro Kishimoto2,3
1Faculty of Rehabilitation, School of Physical Therapy, Reiwa Health Sciences University, Fukuoka, Japan; 2Graduate School of Human-Environment Studies, Kyushu University, Fukuoka, Japan; 3Faculty of Arts and Science, Kyushu University, Fukuoka, Japan
Correspondence: Hiro Kishimoto, Faculty of Arts and Science, Kyushu University, IC15, 744 Motooka, Nishi-ku, Fukuoka City, Fukuoka, 819-0395, Japan, Tel +81-92-802-6071, Email [email protected]
Purpose: Chronic pain may accelerate the development of frailty in older adults through a variety of mechanisms. There are no published investigations of the influence of neuropathic-like symptoms on physical frailty. We investigated the association between chronic pain types (nociceptive and neuropathic-like symptoms) and frailty in community-dwelling Japanese older adults.
Participants and Methods: This was a population-based cross-sectional study conducted in 2017 in the city of Itoshima, Japan of 917 participants aged 65– 75 years, not in need of long-term care, who had completed the physical function tests and questionnaires administered at measurement sessions held at community centers at three sites over a 1- to 2-month period. Their chronic pain types were classified as no-chronic pain, nociceptive pain, and neuropathic-like symptoms according to their painDETECT scores. Frailty phenotypes were defined by the following five components: unintentional weight loss, low grip strength, exhaustion, slow gait speed, and low physical activity. A logistic regression model was used to compute the odds ratios (ORs) and 95% confidence interval (CIs) for frailty status outcomes.
Results: The prevalence of pre-frailty was 51.9%, and that of frailty was 5.1%. In multinomial logistic regression analyses, compared to the no-chronic pain group, the OR for the presence of pre-frailty among the participants with nociceptive pain was 1.54 (95% CI: 1.04– 2.30, p=0.03), and the OR for the presence of frailty among the participants with neuropathic-like symptoms was 4.37 (95% CI: 1.10– 17.37, p=0.04). The neuropathic sensory symptoms of burning, tingling/prickling, and numbness were each associated with frailty, but not with the risk of pre-frailty.
Conclusion: Neuropathic-like symptoms were significantly associated with the presence of frailty in community-dwelling Japanese older adults. Chronic pain types might have different effects on frailty status.
Keywords: nociceptive pain, neuropathic pain, nociceptive pain, chronic pain, frailty, community-dwelling
Introduction
Chronic pain is highly prevalent, and in older adults chronic pain is a major reason for seeking medical care.1 The economic burden of chronic pain is enormous and has been reported to be significantly associated with healthcare resource use, productivity, and costs.2 Three classifications of pain have been proposed by the International Association for the Study of Pain (IASP): nociceptive (from tissue injury), neuropathic (from nerve injury), and nociplastic (from a sensitized nervous system), and the IASP notes that the optimal management of pain could be based on the biopsychosocial model behind the pain.3
Physical frailty, a common geriatric syndrome that is characterized by decreased reserve and resistance to stressors due to cumulative declines across multiple physiologic systems, causes vulnerability to adverse outcomes.4 The frailty phenotype proposed in 2001 by Fried et al in the Cardiovascular Health Study (CHS) is one of the most widely used definitions of frailty.4 In a 2020 study of community-dwelling Japanese adults aged ≥65 years, the prevalence of pre-frailty (one or two affected components of the five Fried frailty criteria) was 40.8%, and that of frailty (three or more affected components of the five Fried frailty criteria) was 8.7%; these conditions were associated with a greater risk of adverse outcomes including hospitalization, disability, institutionalization, and death.5
Chronic pain and frailty increase with age,6,7 and they often coexist. Given the biopsychosocial factors that are common to chronic pain and frailty, chronic pain may precipitate or accelerate the development of frailty in older adults through a variety of mechanisms which may involve or be affected by severe pain, physical activity, occupation, economic status, depression, cognitive function, and loneliness.3,8–12 However, neuroinflammation has been one of the common and important mechanisms that contribute to chronic pain and frailty.13 There is evidence that chronic inflammation is a factor that contributes to aging/frailty14 and that a prolonged persistence of inflammatory stimuli is the biological background that predisposes individuals to age-related diseases or disabilities.15
Considering the contribution of neuroinflammation as a shared mechanism between chronic pain and aging/frailty,13 we speculated that individuals with neuropathic-like symptoms might be at a higher risk of developing frailty. Neuropathic pain is clinically diagnosed based on sensory abnormalities such as numbness and allodynia, more prominent pain attacks, and/or neurological and imaging findings of affected tissues.3 However, these techniques are not always available in all research settings, especially in epidemiological studies. The painDETECT Questionnaire (PD-Q) was developed as a self-administered psychometric questionnaire to identify the likelihood of a neuropathic pain component, and it is used to classify nociceptive and neuropathic-like symptoms.16,17 Since optimal pain management based on pain mechanisms is recommended, assessing the type of chronic pain may lead to optimal frailty prevention and management.
We have found no published investigations of the influence of neuropathic-like symptoms on frailty. We conducted this study to determine the association between chronic pain types (nociceptive and neuropathic-like symptoms) and frailty in a population of community-dwelling older Japanese adults, with analyses that included adjustment for a variety of covariates.
Participants and Methods
Study Population
This was a population-based cross-sectional study conducted in 2017 in the city of Itoshima, Japan (population ~96,000) as an investigation of modifiable lifestyle and social factors. The study population included independent, community-dwelling individuals aged 65–75 years who were not certified as requiring nursing care by Japan’s National Long-term Care Insurance System. The residents of Itoshima were informed about this study several times through the city’s newsletter, and we held informational meetings at each community center in order to increase the rates of participation. Of the approx. 10,000 older adults who were examined in an Itoshima Area Needs Assessment by the local government and a private company, 5000 were randomly selected by software according to their residential area, sex, and age. A set of study information sheets and questionnaires was mailed to these participants, inviting them to community centers for further assessments. Of those 5000 residents, 1589 submitted the information sheets/questionnaires, and 930 visited the local community center for a physical function test and additional questionnaires. The measurement sessions were held at community centers in three areas of Itoshima over a period of 1–2 months, respectively. All measurements were completed by nurses, public health nurses, physical therapists, and trained staff who have expertise in epidemiologic studies.
After the exclusion of 13 participants who were missing frailty-related data (n=1) or pain-related data (n=12), the final analysis included 917 participants (453 men and 464 women) with a mean ± standard deviation (SD) age of 70.8 ± 3.0 years. This study was approved by the Institutional Review Board of Kyushu University (approval no. 201708), Japan. The residents participated in this study based on their own volition. None of the participants received compensation for their participation, and they each provided written informed consent to have their data used and published. Our study complies with the Declaration of Helsinki.
Assessment of Chronic Pain Types
Chronic pain was assessed using questions ascertaining the respondent’s pain lasting ≥3 months in the previous 12-month period.18 The response options were “yes” and “no”. When answering “yes”, the respondent was asked to indicate the affected musculoskeletal sites (total of eight areas: neck, shoulders, elbows, wrists/hands, hips, knees, feet, and low back) on a body diagram. We also assessed the participants’ pain intensity during the prior 4 weeks on a numerical rating scale.
We evaluated the participants’ chronic pain types by using the PD-Q.16 The PD-Q was developed as a self-administered psychometric questionnaire to identify the likelihood of a neuropathic pain component. The Japanese version of the PD-Q has established validity and reliability.19 It comprises three items evaluating characteristics of the gradation of pain (seven sensory symptom items: burning, tingling/prickling, light touching, electric shock-type pain, cold/heat, numbness, and slight pressure), the pain course pattern, and radiating pain, which contribute to an aggregate score (range 0–38 points). In this study, to compare purely nociceptive pain (PD-Q scores ≤12) with the neuropathic component, we combined the positive components (PD-Q score ≥19) and the unclear components (PD-Q score 13–18) with neuropathic pain, which is referred to as neuropathic-like symptoms. This approach is consistent with earlier studies20,21 and ensures that participants with possible neuropathic pain characteristics are included.17 We classified chronic pain types into no-chronic pain, nociceptive pain, and neuropathic-like symptoms.
Measurement of Frailty Status
We identified physical frailty according to the CHS criteria,4 which consist of the following five components: unintentional weight loss, low grip strength, exhaustion, slow gait speed, and low physical activity. Participants with three or more affected components were considered to be frail; those with one or two affected components were considered to be pre-frailty; and those with no affected components were considered to be non-frail (or robust).
The operational definition of each component in this study was as follows (Supplemental Table S1). We identified weight loss as the self-reported unintentional loss of >2–3 kg in the previous 6 months. Grip strength was measured using a handheld dynamometer (GRIP-D, TKK 5401; Takei Scientific Instruments Co., Niigata, Japan). The measurement was performed twice for each hand, and the greater values for both hands were then averaged. Weakness was defined as scoring in the lowest 20% of grip strength and was stratified by gender and body mass index (BMI) (kg/m2). Exhaustion was indicated by a positive answer to either of two questions regarding the previous month: “Did you feel that everything you did was an effort?” and “Did you feel exhausted without any reason?”
Gait speed was measured with a 5-meter walking test at the individual’s maximum walking speed. Slowness was identified as scoring in the slowest 20% of gait speed, stratified by gender and standing height. We measured the low-energy expenditure of physical activity objectively with a tri-axial accelerometer (Active Style Pro, HJA350-IT, Omron Healthcare, Kyoto, Japan) for ≥1 week.22 Low physical activity was defined as scoring in the lowest 20% of energy expenditure of physical activity per day, stratified by gender. Data were quantified as kilocalories per kilogram of body weight expended per day (kcal/kg/day). A valid day was defined by wearing the tri-axial accelerometer for ≥10 h of wear time/day. Participants with ≥4 valid days were eligible for all analyses.
Potential Confounding Factors
Considering the biopsychosocial models of chronic pain3 and frailty,23 we investigated the following biopsychosocial factors, each of which was associated with frailty in several studies.8–12,24 Educational level was divided into two categories (<10 or ≥10 years) according to the number of years of education the participant received (a continuous variable), as compulsory education lasts a total of nine years in Japan. Employment status was assessed by the question “Do you currently have a job with income?” Respondents who answered “yes” were considered to be employed. The subjective economic status was assessed by the question “How difficult or easy is your current financial status”; the response options for this question were “very hard”, “hard”, “easy”, and “very easy”. Based on the participants’ responses, we divided the subjective economic status into low (very hard or hard) and high (easy or very easy). Comorbidities were determined by asking the participants to state whether they had any diseases currently being treated including osteoporosis, hypertension, hyperlipidemia, diabetes mellitus, stroke, and heart disease (including arrhythmia). We defined current smoking as those who responded “almost every day” or “occasionally” to the question Do you smoke cigarettes? We defined current alcohol consumption as those who responded “almost every day” or “occasionally” to the question “Do you drink alcohol? Exercise habits were assessed with the question. “How many days per week do you engage in light or regular exercise?” and were divided into two categories according to participants’ responses (≥3 times/week or not). The respondents were also asked whether they were “living alone”, “living with family”, or “other (eg, institutionalized)”. The number of communications with other people (eg, family, relatives, neighborhood, and friends) per month was divided into two categories based on the participants’ responses (none or ≥1 person). Experiences of bereavement were assessed with the question. “Have you experienced bereavement with someone in the past year?” The participants’ body height and weight with the participant in light clothing without shoes, and we calculated the BMI (kg/m2): BMI <18.5 was defined as underweight and BMI ≥25 as overweight.24 In this study, obesity (BMI ≥30) was included in the overweight category. We used the Mini-Mental State Examination (MMSE) to assess the participants’ global cognitive function.25 MMSE screenings were carried out by trained nurses and staff. The final scores were determined by two of the study coordinators. We defined cognitive impairment as an MMSE score ≤23 points.25
Statistical Analyses
Descriptive data are presented as the mean (±SD) for continuous variables and as the frequency (percentage) for categorical variables according to the status of chronic pain types. We performed Dunnett’s test for group differences with the no-chronic pain group as the reference group. We conducted a χ2-test to compare the site-specific prevalence of chronic pain between the nociceptive pain group and the neuropathic-like symptoms group. We used a direct method to calculate the age- and sex-adjusted prevalence of pre-frailty and frailty according to the status of chronic pain types.
We performed multinomial logistic regression analyses to investigate the association between the chronic pain types and the frailty status. Multivariable-adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated, and the no-chronic pain group was regarded as the reference group. The multivariable model was adjusted for age, sex, education level (<10 or ≥10 years), employment status (employed or unemployed), subjective economic status (low or high), comorbidities (yes, no), underweight (yes, no), overweight (yes, no), cognitive impairment (yes, no), current smoking (yes, no), current alcohol consumption (yes, no), regular exercise (≥3 times/week or not), living alone (yes, no), number of communications with another person per month (none or ≥1 person), experiences of bereavement (yes, no), and pain intensity (continuous).
We used a binomial logistic regression model to examine the association between chronic pain types and sub-items of frailty components (unintentional weight loss, low grip strength, exhaustion, slow gait speed, and low physical activity). We also performed multivariable-adjusted multinomial logistic regression analyses to investigate the association between the participants’ neuropathic sensory symptoms and frailty status. The data were processed using SAS software ver. 9.4 (SAS Institute, Cary, NC). The computations were carried out using the computer resources offered under General Projects by the Research Institute for Information Technology, Kyushu University. Statistical significance was defined as a two-tailed p-value <0.05.
Results
The characteristics of the study participants according to the status of chronic pain types are summarized in Table 1 Compared to the no-chronic pain group, the nociceptive pain group and neuropathic-like symptoms each had a significantly higher frequency of osteoporosis (4.3% vs 9.6% [p<0.05] vs 15.9% [p<0.01], respectively) and hyperlipidemia (24.2% vs 35.4% [p<0.01] vs 36.2% [p<0.05], respectively). Compared to the no-chronic pain group, hypertension was significantly more frequent in the nociceptive pain group (35.6% vs 44.4%, respectively; p<0.05). The overall prevalence of chronic pain was 64.5% (n=591), with a higher prevalence of chronic pain in the wrists/hands, hips, knees, and feet among the neuropathic-like symptoms group compared to the nociceptive pain group (Supplemental Table S2).
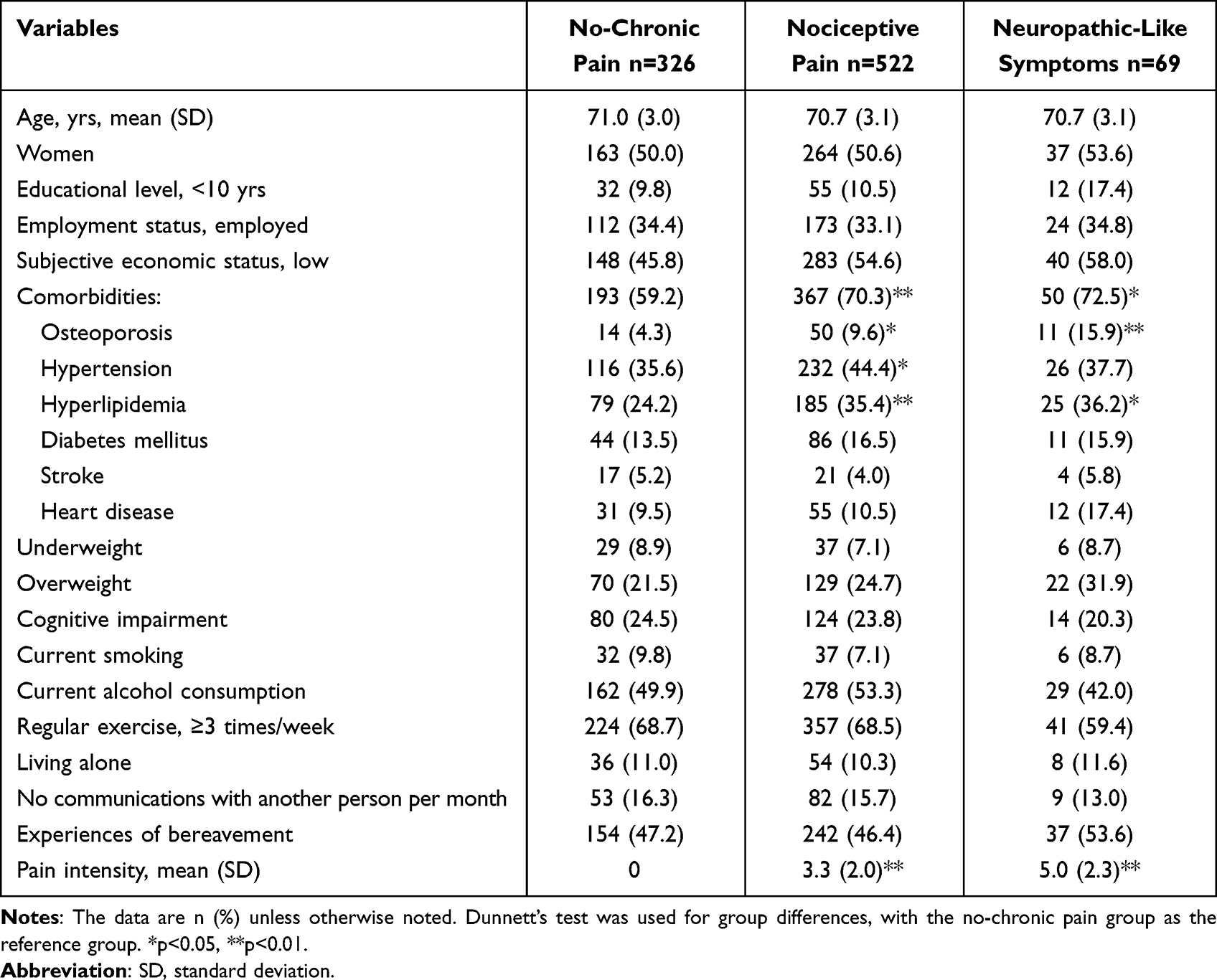 |
Table 1 Characteristics of the 917 Study Participants According to the Status of Chronic Pain Types |
Overall, 51.9% (n=476) of the participants were classified as having pre-frailty, and 5.1% (n=47) of the participants were classified as having frailty. Of the participants with chronic pain, 54.5% (n=322) were pre-frail and 6.1% (n=36) were frail. As shown in Figure 1, the age- and sex-adjusted prevalence of pre-frailty was significantly increased among the participants with nociceptive pain compared to the no-chronic pain group, whereas the age- and sex-adjusted prevalence of frailty was significantly increased among the participants with nociceptive pain and neuropathic-like symptoms compared to the no-chronic pain group.
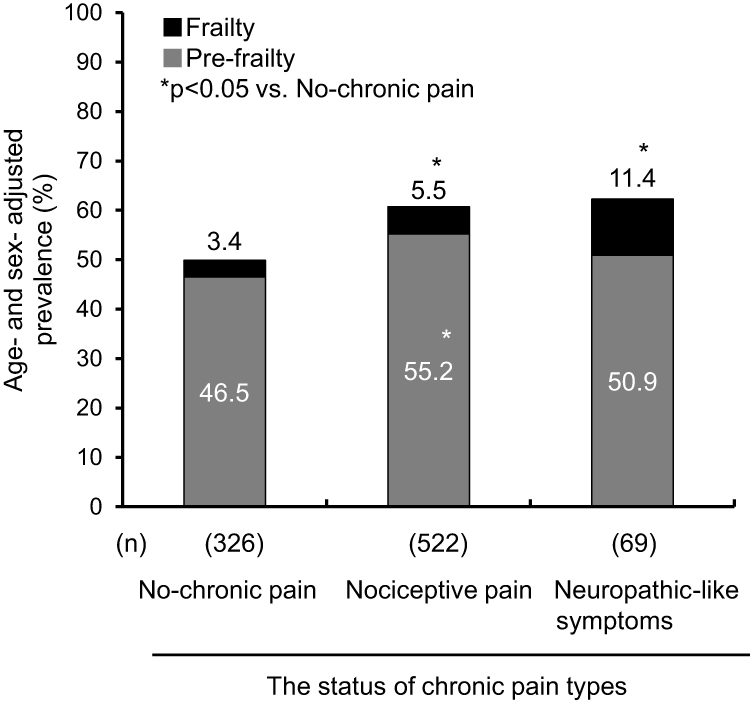 |
Figure 1 Age- and sex-adjusted prevalence of pre-frailty and frailty according to the status of chronic pain types.*p<0.05 vs No-chronic pain. |
Table 2 presents the multivariable-adjusted ORs and 95% CIs for the presence of pre-frailty and frailty according to the status of chronic pain types. In the multinomial logistic regression analyses, the following ORs and 95% CIs were revealed: for the presence of pre-frailty among the participants with nociceptive pain, 1.64 (95% CI: 1.08–2.50, p=0.02) compared to the no-chronic pain group; and for the presence of frailty among the participants with neuropathic-like symptoms, 4.68 (95% CI: 1.14–19.24, p=0.03) versus the no-chronic pain group. The binomial logistic regression analyses provided the following ORs and 95% CIs: for the presence of exhaustion in the nociceptive pain group, 2.57 (95% CI: 1.34–4.93, p<0.01) compared to the no-chronic pain group, and for the presence of slow gait speed in the neuropathic-like symptoms group, 2.29 (95% CI: 1.05–5.01, p=0.04) versus the no-chronic pain group (Supplemental Table S3).
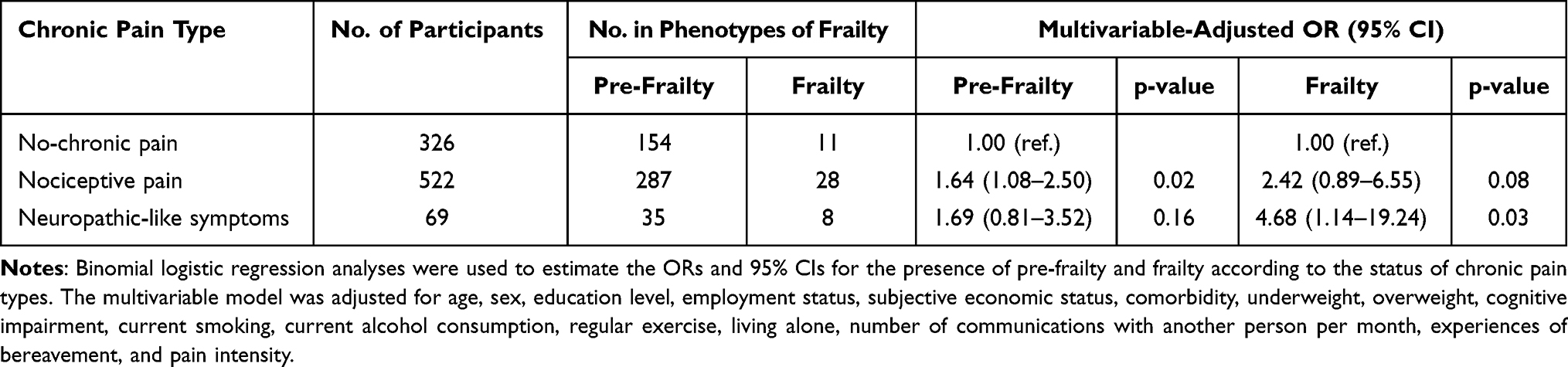 |
Table 2 Multivariable-Adjusted Odds Ratios (ORs) and 95% CIs (Confidence Intervals) for the Presence of Pre-Frailty and Frailty According to the Status of Chronic Pain Types |
Table 3 presents the multivariable-adjusted ORs and 95% CIs for the presence of pre-frailty and frailty according to the neuropathic sensory symptoms. In the multinomial logistic regression analyses, the neuropathic sensory symptoms of burning (OR 3.36, 95% CI: 1.47–7.71, p<0.01), tingling/prickling (OR 2.56, 95% CI: 1.19–5.51, p=0.02), and numbness (OR 3.60, 95% CI: 1.62–7.97, p<0.01) were significantly associated with frailty (but not pre-frailty), while light touching was significantly associated with pre-frailty (OR 1.90, 95% CI: 1.05–3.44, p=0.04), and slight pressure was significantly associated with both pre-frailty and frailty (pre-frailty, OR 1.49, 95% CI: 1.05–2.14, p=0.03; frailty, OR 2.31, 95% CI: 1.10–4.88, p=0.03).
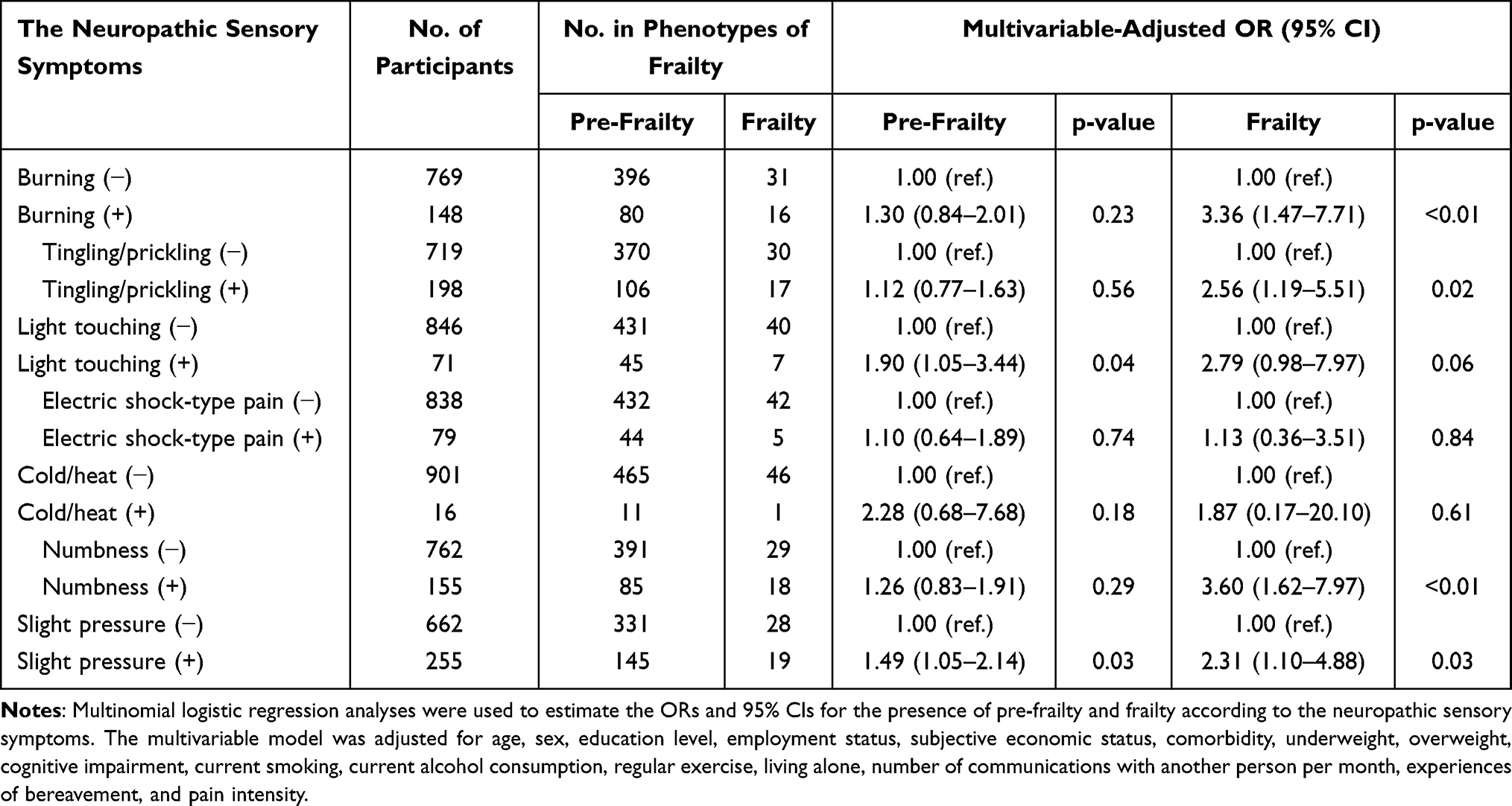 |
Table 3 Multivariable-Adjusted ORs and 95% CIs for the Presence of Pre-Frailty and Frailty According to the Neuropathic Sensory Symptoms |
Discussion
The results of our analyses demonstrated that in a population of 917 community-dwelling Japanese older adults, compared to the no-chronic pain group, (i) Nociceptive pain was significantly associated with a higher risk of the presence of pre-frailty, and (ii) Neuropathic-like symptoms were significantly associated with a higher risk of the presence of frailty. We observed that nociceptive pain was associated with exhaustion and that neuropathic-like symptoms were associated with slow gait speed. The analyses also revealed that the neuropathic sensory symptoms of burning, tingling/prickling, and numbness were each associated with frailty, but not the risk of pre-frailty.
The prevalence of frailty in this study population (5.1%) was somewhat lower than the national prevalence of frailty in Japan (8.7%),5 the United States (15.3%),26 and European Union countries (18.0%).27 This is likely due to the differences in the survey methodology, response rate, age-range, and definition of frailty. It is therefore necessary to take into account the possibility that the present study’s participants were more representative of healthy individuals.
A systematic review of the association between chronic pain and frailty among older adults indicated that frailty and pre-frailty are common in individuals with chronic pain and that chronic pain among non-frail older adults significantly predicts the incidence of frailty after an average follow-up of 5.8 years.28 Several studies have demonstrated that pain frequency, pain intensity, the number of pain sites, widespread pain, and osteoarthritis-related pain are associated with the risk of developing frailty.8–10,29,30 For example, the ENRICA prospective study of Spanish community residents aged ≥60 years without frailty reported that the association between pain characteristics (frequency, intensity, and the number of pain sites) and frailty is a dose-response relationship, with severe-type pain increasing the risk of developing frailty.8 However, since we were unable to find any study that examined the association between neuropathic pain and prefrailty and frailty in community-dwelling older adults, our present findings provide new insight into the effects of neuropathic-like symptoms that may contribute to the mechanism of frailty development. Conversely, frailty may be significantly associated with the probability of chronic pain.28 Further prospective and interventional studies may clarify the causal relationship between chronic pain types and frailty.
In a meta-analysis including 32 cross-sectional studies, frailty and pre-frailty were associated with significantly higher serum inflammatory parameters, particularly C-reactive protein (CRP) and interleukin (IL)-6, compared to robust participants.14 However, longitudinal studies did not show any association between higher inflammatory levels and the onset of frailty.14 The presence of neuropathic characteristics has been associated with central sensitization and might thus be related to the presence of nociplastic mechanisms.31 Nociplastic pain is pain that arises from the abnormal processing of pain signals without any clear evidence of tissue damage or discrete pathology involving the somatosensory system.3 An association between the PD-Q score and quantitative sensory testing (QST) has been reported.21,32,33 QST indirectly examines the possibility of the sensitization of nociceptive neurons and is increasingly used in studies of musculoskeletal pain34 as well as for patients with features of neuropathic pain.35 It has thus been speculated that moderate to severe persistent nociceptive stimulation at multiple joints may result in neuropathy-like symptoms via central sensitization,36 which may be associated with the development of frailty via the induction of vulnerability to internal and external stress.37 Moreover, fear-avoidance behaviors among individuals with chronic pain lead to the development of a sedentary lifestyle, which further decreases muscle mass and strength and contributes to the development of sarcopenia and/or slow gait speeds.38,39 In the present study, neuropathic-like symptoms were associated with slow gait speed, suggesting the need for future investigations of the possibility that catastrophic thoughts in the participants with neuropathic-like symptoms were partially involved in this association.
The strengths of our study are as follows. This is the first study to examine the relationship between chronic pain types (nociceptive and neuropathic-like symptoms) and frailty in community-dwelling older adults, and the information was obtained from a relatively large number of participants (n=917). In addition, the ORs were calculated with adjustment for potential biopsychosocial confounders. However, some limitations need to be considered when interpreting our findings. First, the study’s cross-sectional design does not allow conclusions about the direction of causality of these associations. Second, we cannot rule out the possibility that the study population was biased toward healthy individuals, since the analysis subjects (n=930) had fewer comorbidities and a lower rate of current smoking, while their regular exercise (≥3 times/week) was more frequent compared to the excluded subjects (n=659). Third, we were unable to obtain medical information on chronic inflammation and diseases that include symptoms of neuropathic pain. We used the PD-Q to identify neuropathic pain components in this study, but we cannot generalize the study’s results as pure neuropathic pain because the positive and unclear components were combined into neuropathic-like symptoms. Future research should include a precise clinical diagnosis based on physical and imaging findings of neurological symptoms including QST and a flow chart for identifying and grading nociplastic pain affecting the musculoskeletal system.40 Fourth, there is no information on nutrition that contributes to the frailty cycle,4 although it is well-known that unhealthy dietary behaviors are often observed in individuals with chronic pain.41 Fifth, although multiple covariates were considered for adjustment, the effects of residual confounding remain a concern. Finally, there are limitations in the generalizability of the findings to other populations with different cultures and lifestyles, because the study was conducted in a single region of Japan.
Conclusions
The results of our analyses demonstrated that in a population of community-dwelling Japanese older adults, compared to the no-chronic pain group, (i) nociceptive pain was significantly associated with a higher risk of the presence of pre-frailty, and (ii) neuropathic-like symptoms were significantly associated with a higher risk of the presence of frailty. In particular, the neuropathic sensory symptoms of burning, tingling/prickling, and numbness were each associated with frailty, but not the risk of pre-frailty. The results of this study suggest that chronic pain types might have different effects on frailty status. Further prospective and interventional studies are needed to incorporate assessments that enable the objective classification of chronic pain types (nociceptive, neuropathic, or nociplastic) and could be developed into a multidisciplinary approach that is based on multiple pain mechanisms.
Abbreviations
BMI, body mass index; CHS, Cardiovascular Health Study; CI, confidence interval; MMSE, Mini-Mental State Examination; OR, odds ratio; PD-Q, painDETECT questionnaire; QST, quantitative sensory testing, SD, standard deviation.
Acknowledgments
We thank Dr. Shuzo Kumagai, Dr. Tao Chen, and the Itoshima City Office for their support in designing this study and recruiting participants.
Funding
This study was supported in part by a grant from the Japan Agency for Medical Research and Development (no. JP17942839); by Grants-in-Aid for Scientific Research (B) (nos. JP 20H04016 and JP20H04030) and (C) (nos. JP20K102692, JP20K11446, and JP20K12510) and Research Activity Start-up (no. JP19K24259) from the Ministry of Education, Culture, Sports, Science and Technology of Japan; by Itoshima City (2021-0032), and by Asanohi Orthopaedic Clinic (2020-0528). None of the funding sources had any role in the study design, data analysis, data interpretation, writing of the manuscript, or decisions concerning the submission of this article.
Disclosure
The authors have no conflicts of interest to declare.
References
1. St Sauver JL, Warner DO, Yawn BP, et al. Why patients visit their doctors: assessing the most prevalent conditions in a defined American population. Mayo Clin Proc. 2013;88:56–67. doi:10.1016/j.mayocp.2012.08.020
2. Schaefer C, Sadosky A, Mann R, et al. Pain severity and the economic burden of neuropathic pain in the United States: BEAT neuropathic pain observational study. Clinicoecon Outcomes Res. 2014;6:483–496. doi:10.2147/CEOR.S63323
3. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397:2082–2097. doi:10.1016/S0140-6736(21)00393-7
4. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56:M146–M156. doi:10.1093/gerona/56.3.m146
5. Murayama H, Kobayashi E, Okamoto S, et al. National prevalence of frailty in the older Japanese population: findings from a nationally representative survey. Arch Gerontol Geriatr. 2020;91:104220. doi:10.1016/j.archger.2020.104220
6. Inoue S, Kobayashi F, Nishihara M, et al. Chronic pain in the Japanese community – prevalence, characteristics and impact on quality of life. PLoS One. 2015;10:e0129262. doi:10.1371/journal.pone.0129262
7. Collard RM, Boter H, Schoevers RA, Oude Voshaar RC. Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc. 2012;60:1487–1492. doi:10.1111/j.1532-5415.2012.04054.x
8. Rodriguez-Sanchez I, Garcia-Esquinas E, Mesas AE, Martin-Moreno JM, Rodriguez-Manas L, Rodriguez-Artalejo F. Frequency, intensity and localization of pain as risk factors for frailty in older adults. Age Ageing. 2019;48:74–80. doi:10.1093/ageing/afy163
9. Wade KF, Lee DM, McBeth J, et al. Chronic widespread pain is associated with worsening frailty in European men. Age Ageing. 2016;45:268–274. doi:10.1093/ageing/afv170
10. Wade KF, Marshall A, Vanhoutte B, Wu FC, O’Neill TW, Lee DM. Does pain predict frailty in older men and women? Findings from the English Longitudinal Study of Ageing (ELSA). J Gerontol a Biol Sci Med Sci. 2017;72:403–409. doi:10.1093/gerona/glw226
11. Robinson TL, Gogniat MA, Miller LS. Frailty and cognitive function in older adults: a systematic review and meta-analysis of cross-sectional studies. Neuropsychol Rev. 2022;32:274–293. doi:10.1007/s11065-021-09497-1
12. Sha S, Xu Y, Chen L. Loneliness as a risk factor for frailty transition among older Chinese people. BMC Geriatr. 2020;20:300. doi:10.1186/s12877-020-01714-5
13. D’Agnelli S, Amodeo G, Franchi S, et al. Frailty and pain, human studies and animal models. Ageing Res Rev. 2022;73:101515. doi:10.1016/j.arr.2021.101515
14. Soysal P, Stubbs B, Lucato P, et al. Inflammation and frailty in the elderly: a systematic review and meta-analysis. Ageing Res Rev. 2016;31:1–8. doi:10.1016/j.arr.2016.08.006
15. Franceschi C, Bonafe M, Valensin S, et al. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann NY Acad Sci. 2000;908:244–254. doi:10.1111/j.1749-6632.2000.tb06651.x
16. Freynhagen R, Baron R, Gockel U, Tolle TR. painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin. 2006;22:1911–1920. doi:10.1185/030079906X132488
17. Fernandes GS, Valdes AM, Walsh DA, Zhang W, Doherty M. Neuropathic-like knee pain and associated risk factors: a cross-sectional study in a UK community sample. Arthritis Res Ther. 2018;20:215. doi:10.1186/s13075-018-1717-6
18. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160:19–27. doi:10.1097/j.pain.0000000000001384
19. Matsubayashi Y, Takeshita K, Sumitani M, et al. Validity and reliability of the Japanese version of the painDETECT questionnaire: a multicenter observational study. PLoS One. 2013;8:e68013. doi:10.1371/journal.pone.0068013
20. Soni A, Wanigasekera V, Mezue M, et al. Central sensitization in knee osteoarthritis: relating presurgical brainstem neuroimaging and PainDETECT-based patient stratification to arthroplasty outcome. Arthritis Rheumatol. 2019;71:550–560. doi:10.1002/art.40749
21. Soni A, Batra RN, Gwilym SE, et al. Neuropathic features of joint pain: a community-based study. Arthritis Rheum. 2013;65:1942–1949. doi:10.1002/art.37962
22. Ohkawara K, Oshima Y, Hikihara Y, Ishikawa-Takata K, Tabata I, Tanaka S. Real-time estimation of daily physical activity intensity by a triaxial accelerometer and a gravity-removal classification algorithm. Br J Nutr. 2011;105:1681–1691. doi:10.1017/S0007114510005441
23. Luca VD, Femminella GD, Patalano R, et al. Assessment tools of biopsychosocial frailty dimensions in community-dwelling older adults: a narrative review. Int J Environ Res Public Health. 2022;19:16050. doi:10.3390/ijerph192316050
24. Chen C, Winterstein AG, Fillingim RB, Wei YJ. Body weight, frailty, and chronic pain in older adults: a cross-sectional study. BMC Geriatr. 2019;19:143. doi:10.1186/s12877-019-1149-4
25. Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc. 1992;40:922–935. doi:10.1111/j.1532-5415.1992.tb01992.x
26. Bandeen-Roche K, Seplaki CL, Huang J, et al. Frailty in older adults: a nationally representative profile in the United States. J Gerontol a Biol Sci Med Sci. 2015;70:1427–1434. doi:10.1093/gerona/glv133
27. O’Caoimh R, Galluzzo L, Rodríguez-Laso Á, et al. Prevalence of frailty at population level in European ADVANTAGE joint action member states: a systematic review and meta-analysis. Ann Ist Super Sanita. 2018;54:226–238. doi:10.4415/ANN_18_03_10
28. Lin T, Zhao Y, Xia X, Ge N, Yue J. Association between frailty and chronic pain among older adults: a systematic review and meta-analysis. Eur Geriatr Med. 2020;11:945–959. doi:10.1007/s41999-020-00382-3
29. Veronese N, Maggi S, Trevisan C, et al. Pain increases the risk of developing frailty in older adults with osteoarthritis. Pain Med. 2017;18:414–427. doi:10.1093/pm/pnw163
30. Bindawas SM, Vennu V, Stubbs B. Longitudinal relationship between knee pain status and incident frailty: data from the osteoarthritis initiative. Pain Med. 2018;19:2146–2153. doi:10.1093/pm/pnx296
31. Fitzcharles MA, Cohen SP, Clauw DJ, et al. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet. 2021;397:2098–2110. doi:10.1016/S0140-6736(21)00392-5
32. Graven-Nielsen T, Arendt-Nielsen L. Assessment of mechanisms in localized and widespread musculoskeletal pain. Nat Rev Rheumatol. 2010;6:599–606. doi:10.1038/nrrheum.2010.107
33. Maier C, Baron R, Tölle TR, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): somatosensory abnormalities in 1236 patients with different neuropathic pain syndromes. Pain. 2010;150:439–450. doi:10.1016/j.pain.2010.05.002
34. Attal N, Fermanian C, Fermanian J, Lanteri-Minet M, Alchaar H, Bouhassira D. Neuropathic pain: are there distinct subtypes depending on the aetiology or anatomical lesion? Pain. 2008;138:343–353. doi:10.1016/j.pain.2008.01.006
35. Amris K, Jespersen A, Bliddal H. Self-reported somatosensory symptoms of neuropathic pain in fibromyalgia and chronic widespread pain correlate with tender point count and pressure-pain thresholds. Pain. 2010;151:664–669. doi:10.1016/j.pain.2010.08.023
36. Saito T, Chen T, Yatsugi H, Chu T, Liu X, Kishimoto H. Association between the number of chronic pain sites and neuropathic-like symptoms in community-dwelling older adults with chronic pain: a cross-sectional study. BMJ Open. 2023;13:e066554. doi:10.1136/bmjopen-2022-066554
37. Saraiva MD, Suzuki GS, Lin SM, de Andrade DC, Jacob-Filho W, Suemoto CK. Persistent pain is a risk factor for frailty: a systematic review and meta-analysis from prospective longitudinal studies. Age Ageing. 2018;47:785–793. doi:10.1093/ageing/afy104
38. Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85:317–332. doi:10.1016/S0304-3959(99)00242-0
39. Leeuw M, Goossens MEJB, Linton SJ, Crombez G, Boersma K, Vlaeyen JWS. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2007;30:77–94. doi:10.1007/s10865-006-9085-0
40. Kosek E, Clauw D, Nijs J, et al. Chronic nociplastic pain affecting the musculoskeletal system: clinical criteria and grading system. Pain. 2021;162:2629–2634. doi:10.1097/j.pain.0000000000002324
41. Meleger A, Froude CK, Walker J 3rd. Nutrition and eating behavior in patients with chronic pain receiving long-term opioid therapy. PM R. 2014;6:7–12.e1. doi:10.1016/j.pmrj.2013.08.597
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.