")
Back to Journals » Advances in Medical Education and Practice » Volume 10
“Rebuilding what has eroded”: a descriptive, survey-based study of near-peer instructors’ experiences in a critical pedagogy-based sociomedical course
Authors Logan AA , DeLisser HM
Received 24 November 2018
Accepted for publication 19 April 2019
Published 2 May 2019 Volume 2019:10 Pages 253—262
DOI https://doi.org/10.2147/AMEP.S195864
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Alexander A Logan,1 Horace M DeLisser2
1Department of Medicine, University of Washington, Seattle, DC, USA; 2Academic Programs Office, Perelman School of School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
Purpose: Near-peer assisted learning has been deployed in numerous settings within medical education with promising results. However, there is very little experience utilizing near-peers in sociomedical or cultural competency training. We recently described a novel model for sociomedical learning based on Introduction to Medicine and Society (IMS), a critical pedagogy-based course at the Perelman School of Medicine at the University of Pennsylvania (PSOM). Near-peer facilitation, by senior medical students, is central to this model. The aim of this descriptive study is to examine how facilitating within this curriculum impacts senior medical students’ self-reported attitudes toward course content, medical education, as well as self-care and medical practice.
Methods: At the conclusion of the course, near-peer facilitator attitudes were assessed in three key domains through an anonymous survey. Attitudes were rated according to a 5-point Likert scale. Data from subgroups were analyzed using standard two-tailed t-tests. Optional narrative data were also collected.
Results: Twenty six of 34 (76%) eligible facilitators completed the survey. Strong majorities of facilitators felt that their experience facilitating IMS had a favorable effect on attitudes related to course content (sociomedical issues and communication skills). A majority also endorsed favorable changes in their attitudes toward teaching and medical education. Large proportions of facilitators endorsed positive changes in a number of domains linked to trainee resilience.
Conclusions: Our descriptive data suggest that acting as a near-peer facilitator as a senior medical student within a critical pedagogy-based course could help to fill multiple important curricular gaps at the transition from medical school to residency. Moreover, we find that a sociomedical facilitation experience during this important transition may increase enthusiasm for careers in medical education and undo some of the negative impacts of clinical training during medical school.
Keywords: near-peer assisted learning, sociomedical education, cultural competency, self-care
Introduction
Near-peer assisted learning, in which more senior trainees act as instructors for learners who are one or more years behind them in training, is an increasingly popular paradigm in medical education.1 Near-peer models have been successfully employed in undergraduate medical education in a range of settings, including problem- and case-based learning,2,3 clinical skills development,4–8 and basic resuscitation training.9,10 Within these contexts, near-peer instructors have been entrusted with a range of autonomy and responsibility with favorable results.3
Near-peer instruction benefits learners by bridging experience gaps between junior students and senior clinicians, thereby enhancing the “social and cognitive congruence” of the learning experience.1,3,11,12 In randomized trials, near-peers are at least as effective as faculty preceptors in transferring knowledge and skills,9,10,13 and descriptive data suggest that they can enhance the motivations of learners while serving as effective role models.3,14
Studies of near-peer assisted learning models across different content areas have also suggested benefits for student instructors themselves. Such experiences can help them develop as effective teachers – an essential quality for senior medical students.1,15 Additionally, “learning by teaching” helps to consolidate near-peer instructor’s own knowledge and skills,5–7,16 while developing their communication skills.17 Finally, engaging in near-peer teaching can reinforce student instructors’ positive attitudes toward teaching.7,18
There is comparatively little experience in the literature deploying near-peers in sociomedical training. In this report, “sociomedical training” references what has been traditionally called “cultural competency training” in the medical education literature. We do this to avoid the limitations of the latter term19,20 and to subsume more recent pedagogical approaches in this area, such as cultural humility21 and critical pedagogy.22 In one report, Tang et al18 utilized fourth-year medical students as near-peer facilitators for second-year students in “diversity-focused” case-based discussions. Facilitators attended a training that covered health disparities broadly, the specific biomedical and sociocultural issues within their designated case, as well as basic facilitation skills. They then facilitated, along with a faculty mentor, a single 90-min discussion session for second-year students. After the discussion, senior student-teachers endorsed a high degree of openness to “learning and teaching sociocultural issues in patient care,” while pre- and post- measurements demonstrated an improvement in their awareness of sociocultural issues.
We have recently described a comprehensive model for sociomedical learning at the undergraduate medical level based on Introduction to Medicine and Society (IMS), a course at the Perelman School of Medicine at the University of Pennsylvania (PSOM).22 This model is unique in two ways within sociomedical training. First, it is grounded in the theory of critical pedagogy – a framework that emphasizes understanding how power and difference shape social structure and interaction, coupled with an orientation to pragmatic action.22 And second, it relies heavily on fourth-year near-peer instructors to deliver course content and experiences to first-year learners. The course is built around a unique dialogic space. Within this space, learners and facilitators bring their “whole selves”23 into dialog with one another around issues at the core of sociomedical disparity and power (eg, race, gender, and class) as well as their professional experience (eg, death and dying, suffering, and advocacy). The goal of this dialogic process is to build critical consciousness – a deep awareness of these issues on personal, interpersonal, and structural levels, with an orientation toward action.24,25 This dialogic process is dynamic and often challenging (for both learners and facilitators) on emotional, intellectual, and interpersonal levels. It depends on generating a high level of trust, vulnerability, and engagement within the group. Initial experiences with this IMS course have been very promising.22
Material and methods
Description of the course
IMS is a semester-long course for first-year medical students covering a broad range of sociomedical topics. The primary learning spaces are discussion groups consisting of 12–14 first-year students (“learners”); 2–4 fourth-year medical student near-peer facilitators; and 2–4 faculty facilitators. Within these groups, faculty facilitators offer context, experience, and support, while near-peer facilitators are expected to drive transformational dialog. The IMS model takes advantage of the enhanced social and cognitive congruence of near-peer facilitation to cultivate this dialogic process. Near-peer facilitators are given a high degree of autonomy and responsibility. They serve as the primary facilitators of discussion, working to manage varied communication styles and interpersonal power dynamics to generate meaningful, inclusive dialog. They are empowered to implement session guides with a high degree of flexibility, adapting them to best meet the needs of their group. They receive training to prepare them to coach group members in a common set of relational communication skills. Successful implementation of these skills is essential to mitigating interpersonal conflict and power dynamics and generating an open and productive dialogic space.
Evaluation of facilitator experience
Near-peers facilitated discussion groups and attended debriefing sessions each week during a 12-week course in Fall 2015. Based on themes that emerged during these debriefing sessions, we chose to explore the effects of this facilitation experience on near-peer instructors. First, we assessed the effect of facilitating on uptake of content and skills related to the course itself. Next, we assessed near-peer facilitators’ attitudes toward medical education. Finally, we explored attitudes toward aspects of self-care and medical practice associated with resilience against burnout, since elements of the IMS dialogic process have been linked to resilience in physicians and trainees. These include examining personal values and sources of meaning,26 managing the doctor–patient relationship,27 exploring feelings provoked by patient suffering and death,28 and considering professional responsibility to patients who are victimized by sociomedical disparity.29
We designed a multiple-choice questionnaire examining instructors’ attitudes in the three domains described above: course content and related skills (Table 1), medical education and training (Table 2), and self-care and medical practice (Table 3). This questionnaire was administered electronically to student instructors at the conclusion of the course. We also collected basic demographic data (Table 4) concurrently. Participation was voluntary and responses were anonymous. Respondents reported the effects of their facilitation experience by indicating agreement with a number of statements on a 5-point Likert scale (1= strongly disagree, 5= strongly agree). Each statement was preceded by the phrase “As a result of my experience facilitating the [IMS] course…”. We considered a selection of either “agree” or “strongly agree” to represent a positive response to any given statement. Results from different subgroups were analyzed for differences using standard two-tailed t-tests.30
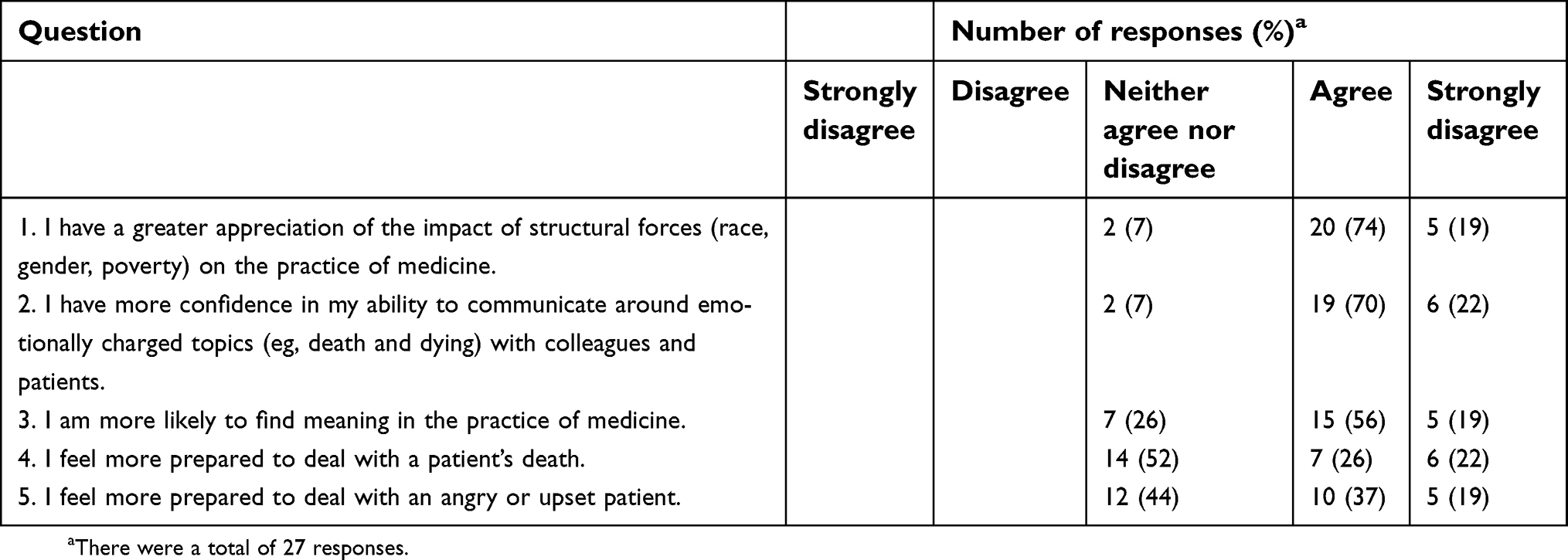 | Table 1 Facilitator responses regarding course content and related skills |
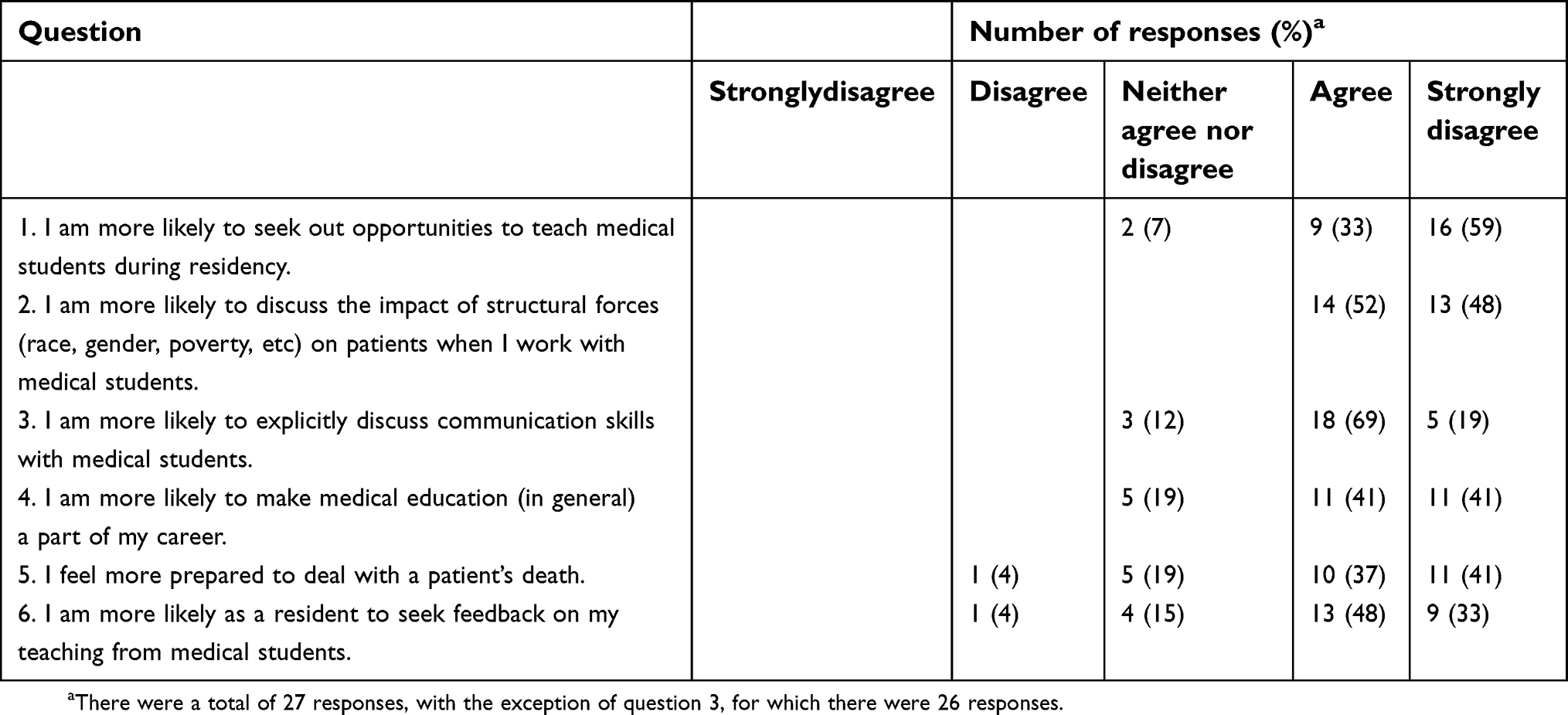 | Table 2 Facilitator responses regarding medical education and teaching |
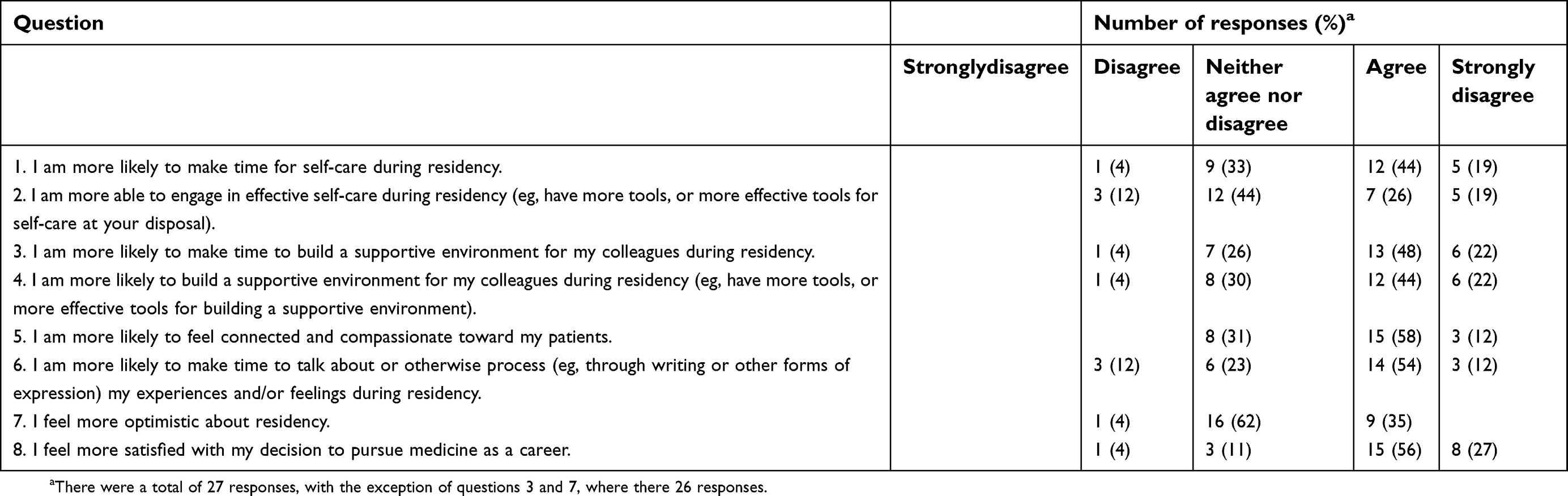 | Table 3 Facilitator responses regarding self-care and medical practice |
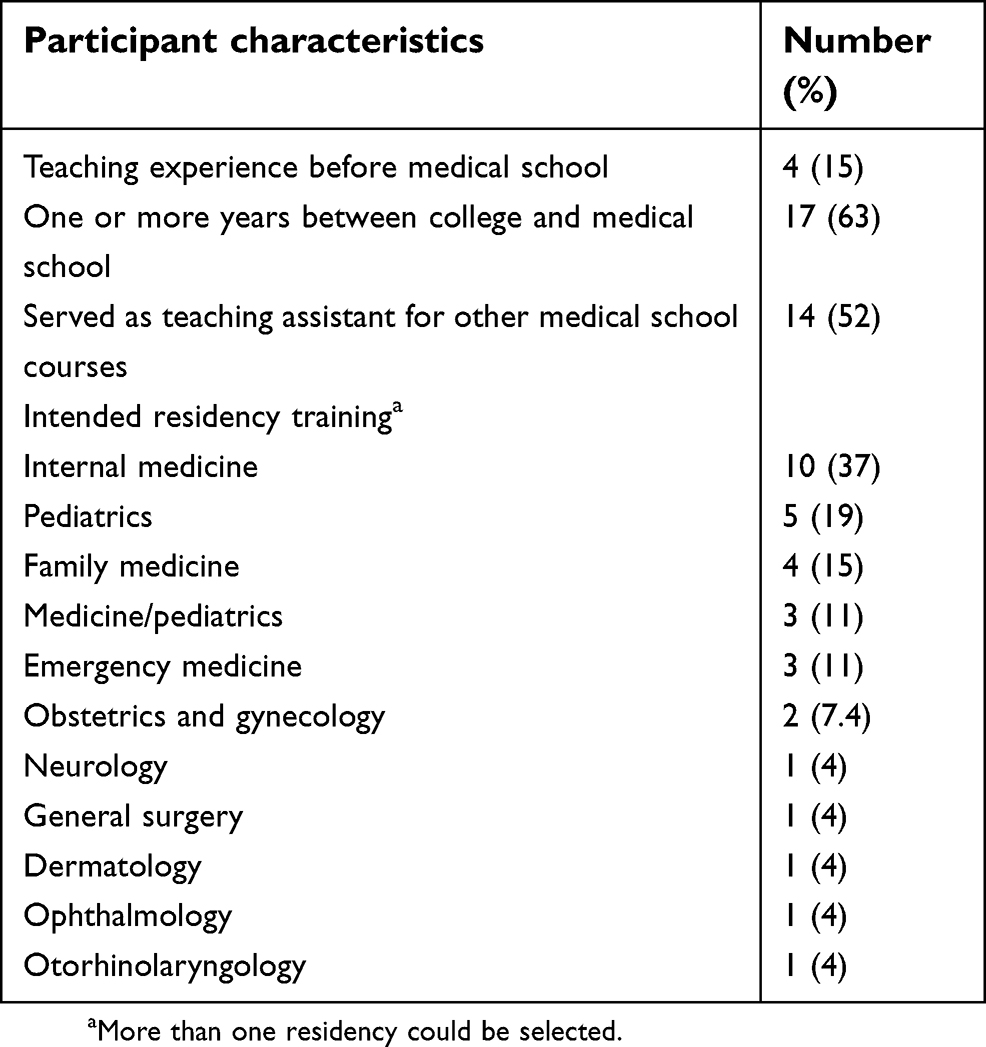 | Table 4 Baseline characteristics of the 27 study participants |
The questionnaire included three qualitative open-ended prompts (“Please elaborate on the impact this course has had (if any) on your feelings toward practicing medicine during residency and beyond”; “Please elaborate on the impact this course has had (if any) on your feelings toward working with medical students during residency and beyond”; and “Please elaborate on the impact this course has had (if any) on your attitudes toward self-care or supporting your colleagues during residency and beyond”). The authors reviewed respondents’ narrative comments for common themes and mapped these to the three domains examined by the quantitative survey.
Informed consent was obtained from all respondents. This study was approved by the Institutional Review Board at the University of Pennsylvania.
Results
Demographic characteristics of facilitators
Of 34 eligible student facilitators, 26 (76%) completed the survey. One respondent completed 85% of the survey and this response was included in the analysis. Characteristics of respondents are shown in Table 4. Four (15%) had formal teaching experience before medical school (informal experience, such as tutoring, was excluded), but over half (52%) had served as teaching assistants in other PSOM courses (none of which were sociomedical courses). Seven (26%) respondents were returning from a year-out at the beginning of the course, compared to 47% of the PSOM graduating class of 2016 (P>0.05). Interest in nonprimary care residencies (residencies other than internal medicine, pediatrics, family medicine, and combined medicine-pediatrics) was under-represented in our sample compared to the PSOM graduating class of 2016 (P< 0.05).
Course content and related skills
Strong majorities of respondents “agreed” or “strongly agreed” that facilitating IMS increased their awareness of the impact of structural forces on the practice of medicine.
A similar number reported increased confidence communicating around emotionally charged topics in a clinical setting (Table 1). About half of the respondents agreed that their experience helped prepare them to deal with an angry or upset patient or with a patient’s death.
In their narrative comments, five respondents commented on the educational value of the experience with respect to sociomedical topics. Five wrote that they believed the experience filled an undermet curricular need in medical training. For example:
"I really value being able to work with students on topics like humanism and social justice to help [first-year students] maintain those priorities that are often otherwise lost in medical school".
"I think getting to work with pre-clinical students as an MS4 helped .. re-focus me [on] ideals of patient care and patient communication that I may have lost a bit after a year on the wards".
Teaching and medical education
Strong majorities of respondents felt that their experience facilitating IMS made them more likely to seek out teaching opportunities in residency, and to incorporate medical education in general, and medical humanism or social medicine-oriented education specifically, into their careers (Table 2). Large proportions agreed that their experience made it more likely that, when working with medical students, they would discuss the impact of structural forces on patients, explicitly discuss clinical communication skills, and seek feedback on their teaching.
In narrative responses, 12 respondents commented on the positive impact of their experience on their enthusiasm for teaching.
For example:
"[I] was interested in medical education previously but now would be interested not only in clinical teaching on the wards but also working on humanism in medicine courses or the like".
"This course made me appreciate how difficult it is to teach communication skills and gave me a greater appreciation for their importance."
Self-care and medical practice
Large proportions of respondents reported that, as a result of their experience facilitating IMS, they felt more satisfied with their decision to pursue medicine, were more likely to feel connected and compassionate toward patients, and were more likely to find meaning in the practice of medicine, although fewer than half agreed that they felt more optimistic about residency as a result of the course (Table 3). A majority agreed that they were more likely to make time for self-care during residency, although fewer felt that they were more able to pursue effective self-care as a result of their experience. A similar number reported that they were more likely to make time to process their experiences and/or feelings during residency. Majorities agreed that they were more likely to make time to build a supportive environment for their co-residents and that they were more able to do so.
Eleven respondents mentioned in their narrative responses that the facilitation experience deepened their self-understanding or was emotionally restorative. For example:
"The biggest impact this course has had on me is rebuilding … part of me that eroded during clerkship year. By serving as a mentor and [helping] prepare other students to have healthy, satisfying medical trainings and careers, I feel better about myself overall and my ability to have a positive impact on my environment. It has also been a nice reminder that practicing medicine is a beautiful privilege and there are many likeminded doctors and future doctors out there who care deeply about caring for their patients and each other".
"Working with first years showed me how much I’ve changed, how much med school has changed me, in good and bad ways. Working with them forced me to confront those changes and figure out which were positive coping strategies and which were bad habits that I should work on getting rid of … Furthermore, the exercise of reflecting on good and bad experiences in clerkships re-affirmed my decision to pursue my chosen specialty".
"I believe that I am a better and more supportive listener after precepting and helping some MS1s through tough experiences. Hopefully this will mean that I can be a better support to my co-interns next year".
Because our sample included a large proportion (52%) of respondents who served as teaching assistants in other PSOM courses, we tested the hypothesis that this experience might result in a differential effect on facilitator attitudes. No significant difference (P> 0.05) was found between the two groups (those that had other teaching experience at PSOM versus those that did not) for any of the survey questions (Table S1).
Discussion
Course content and skills
The IMS model was designed to develop consciousness in first-year students. As we have previously described,22 this model has achieved early success in terms of learner satisfaction. The results of this study suggest that instructing in a critical pedagogy-based course can also develop cognitive and communicational learning around sociomedical topics in near-peer facilitators. This mirrors previous observations of benefits to near-peer instructors in nonsociomedical settings.5–7,16,18 Previous studies have found that residents across specialties have poor knowledge in areas related to vulnerable populations31 and that medical students’ attitudes toward caring for these patients worsen throughout medical school.32–35 Although we did not directly measure knowledge acquisition or attitudes toward vulnerable patients, nearly all respondents endorsed greater awareness of the impacts of structural forces on medical practice. This suggests that near-peer facilitation experiences within comprehensive critical pedagogy-based curricula could help fill this curricular gap, a notion that was mirrored in the qualitative comments we collected. Furthermore, our finding that 100% of respondents felt they were more likely in the future to discuss the impacts of structural forces on patients with medical students suggests that such experiences could prime facilitators to continue building consciousness of sociomedical disparities in their future trainees.
It is also possible that facilitating within an IMS-like course can help senior students develop important skills for functioning as a resident physician. Within the IMS model, relational communication skills serve two primary purposes: to enhance the dialogic space by improving interpersonal communication and to prepare first-year students to be effective communicators in the clinical environment. Our results suggest that near-peer facilitators also benefit from this kind of skill building. We hypothesize that, in addition to formal relational communication skills, near-peer facilitators also hone interpersonal skills informally by navigating challenging group discussions. This effect has been noted in problem-based curricula17 and is likely enhanced in the IMS dialogic space, where there is often a high degree of vulnerability and emotional charge. Taken together, these data further support the notion that serving as a facilitator in an IMS-like course can help to fill some of the gaps36 in trainees’ preparation to navigate psychosocial issues in residency.
Attitudes toward teaching and medical education
Facilitating within the IMS model had a striking impact on near-peer facilitators’ attitudes toward teaching medical students. Our results surpass previous findings that near-peer experiences can reinforce preexisting enthusiasm for teaching and make senior students more “open to learning and teaching sociocultural issues in patient care.”7,18 We posit that the longitudinal aspect of this facilitation experience and the high degree of ownership and autonomy expected of facilitators in our model may contribute to this effect.
In their narrative responses, multiple facilitators commented on benefits or insights they had gained with regard to specific aspects of medical education. This is reflected in our findings that large numbers felt they were more likely to engage in specific teaching behaviors as residents (Table 2). Clinical communication represents a substantial proportion of what medical students learn informally from residents,37 but there is an unmet need for explicit teaching of communication skills to medical students on the wards.38 Our finding that near-peer facilitators felt they were more likely to explicitly discuss communication as part of their clinical teaching as residents again suggests that this type of facilitation experience could fill a curricular gap. Additionally, many facilitators reported being more likely to seek out opportunities to teach medical students in residency and to seek feedback on their teaching.
Attitudes toward self-care and medical practice
Because IMS discussions often delve into questions of self-care and the emotional dynamics of medical practice, we chose to assess facilitators’ attitudes in these domains. We found that many facilitators felt they were more likely to engage in self-care during residency and that about half felt better able to do so. We hypothesize that these attitudes are related to exposure to varied reflective practices within the IMS small groups, as well as experiencing a close-knit group of colleagues with whom there is a shared sense of solidarity and trust.
Recent studies have found an alarming prevalence of burnout and emotional distress in entering interns39,40 and medical students,41,42 suggesting that, for many trainees, burnout is a process that begins at the undergraduate level. In response, there have been calls for proactive interventions that build resilience in trainees during medical school and at the transition to residency.26,27,41–45 We hypothesize that this intensive near-peer facilitation experience during the last year or medical school may be protective against burnout, and indeed found self-rated improvements in numerous attitudes that have been inversely correlated with burnout in prior studies (Table 3). These include satisfaction with career choice,46,47 actively processing feelings and experiences,47,48 and feeling connected and compassionate toward patients.47–49 In narrative comments, multiple facilitators described their IMS experience as emotionally restorative, with some explicitly referencing the need to recover from the clerkship experience, which is consistent with observations that identify the clerkship year as an important source of empathy decline and distress.50
Of particular interest is our finding that many facilitators felt they were more likely to find meaning in medical practice. There is a growing body of evidence suggesting that finding meaning in one’s career can be protective against burnout.26,51,52 Based on our quantitative and qualitative data, as well as informal conversations with student facilitators, we hypothesize that certain aspects of the IMS near-peer experience contribute to this effect. Acting as a role model for and nurturing younger trainees appears to deepen facilitators’ process of self-discovery and self-definition. This experience may also reveal to some near-peer facilitators that teaching and mentoring can be a source of meaning, as is true for many practicing physicians.51
Taken together, these data raise the possibility that interventions involving intensive near-peer facilitation in critical pedagogy curricula could be both restorative and protective vis-a-vis burnout and distress. Additionally, we found self-rated improvements in both readiness and ability to create supportive environments for colleagues. Evidence suggests that supportive team environments may protect against burnout for both residents and medical students.47,48,53–55
Our study has a number of important limitations. It is small and from a single center, and we performed post-measurement only. This study is descriptive in nature, relying on study respondents’ self-reported attitudes, so it would be inappropriate to draw causal conclusions from these data. Concise, validated instruments assessing the attitudes of interest were not available at the time of this study, so we used a nonvalidated ad hoc instrument. Narrative comments were not formally analyzed and are included to lend subjective richness to this descriptive data only. Importantly, the student facilitators in IMS were self-selected, so it is possible that the effects of this intervention would not be generalizable to an entire medical school cohort. Notably, students interested in nonprimary care residencies were under-represented in our cohort of facilitators. Many of the students who apply for this position are already interested in medical education generally, which may account for some of the benefits they reported. However, we found no difference in responses between facilitators who had previously acted as teaching assistants and those who had not.
Conclusions
This descriptive study suggests that participation in an intensive near-peer facilitation model within a critical pedagogy-based course benefits senior medical students in multiple ways. Facilitators endorsed educational benefit in sociomedical content and communications skills, as well as improvements in attitudes toward teaching, self-care, and medical practice. Similar curricular interventions at the transition between medical school and residency could represent one component of broader efforts to train more compassionate, resilient, and effective physician-educators.
Acknowledgments
At the time of the work described herein, Dr. Logan was a medical student at the Perelman School of Medicine. The authors would like to acknowledge Diane Dao, Adeline Goss, Andrew Hoekzema, Lauren Kelly, Sanjiv Mehta, Michelle Munyikwa, and Uptal Sandesara for designing and implementing the course upon which this study is based. The authors also appreciate the support provided by the Academic Programs Office of the Perelman School of Medicine.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bulte C, Betts A, Garner K, Durning S. Student teaching: views of student near-peer teachers and learners. Med Teach. 2007;29(6):583–590. doi:10.1080/01421590701583824
2. Sobral DT. Peer tutoring and student outcomes in a problem-based course. Med Educ. 1994;28(4):284–289.
3. Nelson AJ, Nelson SV, Linn AMJ, Raw LE, Kildea HB, Tonkin AL. Tomorrow’s educators… today? Implementing near-peer teaching for medical students. Med Teach. 2013;35(2):156–159. doi:10.3109/0142159X.2012.737961
4. Field M, Burke J, Lloyd D, McAllister D. Peer-assisted learning in clinical examination. Lancet. 2004;363(9407):490–491. doi:10.1016/S0140-6736(04)15501-3
5. Field M, Burke JM, McAllister D, Lloyd DM. Peer-assisted learning: a novel approach to clinical skills learning for medical students. Med Educ. 2007;41(4):411–418. doi:10.1111/j.1365-2929.2007.02713.x
6. Kim JE, Schickedanz AD, Chou CL. Near-peer workshops for pre-clerkship physical examination skills. Med Educ. 2010;44(5):499–500. doi:10.1111/j.1365-2923.2010.03661.x
7. Buckley S, Zamora J. Effects of participation in a cross year peer tutoring programme in clinical examination skills on volunteer tutors’ skills and attitudes towards teachers and teaching. BMC Med Educ. 2007;7:20. doi:10.1186/1472-6920-7-20
8. Nestel D, Kidd J. Peer tutoring in patient-centred interviewing skills: experience of a project for first-year students. Med Teach. 2003;25(4):398–403. doi:10.1080/0142159031000136752
9. Perkins GD, Hulme J, Bion JF. Peer-led resuscitation training for healthcare students: a randomised controlled study. Intensive Care Med. 2002;28(6):698–700. doi:10.1007/s00134-002-1291-9
10. Hughes TC, Jiwaji Z, Lally K, et al. Advanced cardiac resuscitation evaluation (ACRE): a randomised single-blind controlled trial of peer-led vs. expert-led advanced resuscitation training. Scand J Trauma Resusc Emerg Med. 2010;18:3. doi:10.1186/1757-7241-18-3
11. Lockspeiser TM, O’Sullivan P, Teherani A, Muller J. Understanding the experience of being taught by peers: the value of social and cognitive congruence. Adv Health Sci Educ Theory Pract. 2008;13(3):361–372. doi:10.1007/s10459-006-9049-8
12. Schmidt HG, Moust JH. What makes a tutor effective? A structural-equations modeling approach to learning in problem-based curricula. Acad Med. 1995;70(8):708–714.
13. Tolsgaard MG, Gustafsson A, Rasmussen MB, Høiby P, Müller CG, Ringsted C. Student teachers can be as good as associate professors in teaching clinical skills. Med Teach. 2007;29(6):553–557. doi:10.1080/01421590701682550
14. Ten Cate O, Durning S. Peer teaching in medical education: twelve reasons to move from theory to practice. Med Teach. 2007;29(6):591–599. doi:10.1080/01421590701606799
15. Dandavino M, Snell L, Wiseman J. Why medical students should learn how to teach. Med Teach. 2007;29(6):558–565. doi:10.1080/01421590701477449
16. Liew S-C, Sow C-F, Sidhu J, Nadarajah VD. The near-peer tutoring programme: embracing the “doctors-to-teach” philosophy–a comparison of the effects of participation between the senior and junior near-peer tutors. Med Educ Online. 2015;20:27959. doi:10.3402/meo.v20.27959
17. Crowe JPS. Perceptions of student peer tutors in a problem-based learning programme. Med Teach. 2001;23(2):181–186. doi:10.1080/01421590020031101
18. Tang TS, Hernandez EJ, Adams BS. Learning by teaching”: a peer-teaching model for diversity training in medical school. Teach Learn Med. 2004;16(1):60–63. doi:10.1207/s15328015tlm1601_12
19. Weissman S. When and how do we teach cultural awareness? Acad Med. 2017;92(12):1653. doi:10.1097/acm.0000000000001985
20. DeLisser HM. In reply to Weissman. Acad Med. 2017;92(12):1653. doi:10.1097/ACM.0000000000001990
21. Tervalon M, Murray-García J. Cultural humility versus cultural competence: a critical distinction in defining physician training outcomes in multicultural education. J Health Care Poor Underserved. 1998;9(2):117–125.
22. Dao DK, Goss AL, Hoekzema AS, et al. Integrating theory, content, and method to foster critical consciousness in medical students: a comprehensive model for cultural competence training. Acad Med. 2017;92(3):335–344. doi:10.1097/ACM.0000000000001390
23. Kumagai AK, Naidu T. Reflection, dialogue, and the possibilities of space. Acad Med. 2015;90(3):283–288. doi:10.1097/ACM.0000000000000582
24. Kumagai AK, Lypson ML. Beyond cultural competence: critical consciousness, social justice, and multicultural education. Acad Med. 2009;84(6):782–787. doi:10.1097/ACM.0b013e3181a42398
25. Freire P. Pedagogy of the Oppressed. New York: The Continum International Publishing Group;1970.
26. Dyrbye L, Shanafelt T. Nurturing resiliency in medical trainees. Med Educ. 2012;46(4):343. doi:10.1111/j.1365-2923.2011.04206.x
27. Howe A, Smajdor A, Stöckl A. Towards an understanding of resilience and its relevance to medical training. Med Educ. 2012;46(4):349–356. doi:10.1111/j.1365-2923.2011.04188.x
28. Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. JAMA. 2001;286(23):3007–3014.
29. Dyrbye LN, Massie FS
30. De Winter JCF, Dodou D. Five-point likert items: t test versus Mann-Whitney-Wilcoxon. Pract Assess Res Eval. 2010;15(11):1–12.
31. Wieland ML, Beckman TJ, Cha SS, Beebe TJ, McDonald FS. Underserved care curriculum collaborative. Resident physicians’ knowledge of underserved patients: a multi-institutional survey. Mayo Clin Proc. 2010;85(8):728–733. doi:10.4065/mcp.2009.0703
32. Crandall SJ, Volk RJ, Cacy D. A longitudinal investigation of medical student attitudes toward the medically indigent. Teach Learn Med. 1997;9(4):254–260. doi:10.1207/s15328015tlm0904_2
33. Crandall SJS, Volk RJ, Loemker V. Medical students’ attitudes toward providing care for the underserved: are we training socially responsible physicians? JAMA. 1993;269(19):2519–2523.
34. Crandall SJS, Reboussin BA, Michielutte R, Anthony JE, Naughton MJ. Medical students’ attitudes toward underserved patients: a longitudinal comparison of problem-based and traditional medical curricula. Adv Health Sci Educ Theory Pract. 2007;12(1):71–86. doi:10.1007/s10459-005-2297-1
35. Stephens MB, Landers G, Davis SW, Durning SJ, Crandall SJ. Medical student attitudes toward the medically underserved: the USU perspective. Mil Med. 2015;180(4S):61–63. doi:10.7205/MILMED-D-14-00558
36. Chen CA, Kotliar D, Drolet BC. Medical education in the United States: do residents feel prepared? Perspect Med Educ. 2015;4(4):181–185. doi:10.1007/s40037-015-0194-8
37. Karani R, Fromme HB, Cayea D, Muller D, Schwartz A, Harris IB. How medical students learn from residents in the workplace: a qualitative study. Acad Med. 2014;89(3):490–496. doi:10.1097/ACM.0000000000000141
38. Rosenbaum ME, Axelson R. Curricular disconnects in learning communication skills: what and how students learn about communication during clinical clerkships. Patient Educ Couns. 2013;91(1):85–90. doi:10.1016/j.pec.2012.10.011
39. Ripp J, Babyatsky M, Fallar R, et al. The incidence and predictors of job burnout in first-year internal medicine residents: a five-institution study. Acad Med. 2011;86(10):1304–1310. doi:10.1097/ACM.0b013e31822c1236
40. Ripp J, Fallar R, Babyatsky M, David R, Reich L, Korenstein D. Prevalence of resident burnout at the start of training. Teach Learn Med. 2010;22(3):172–175. doi:10.1080/10401334.2010.488194
41. Ishak W, Nikravesh R, Lederer S, Perry R, Ogunyemi D, Bernstein C. Burnout in medical students: a systematic review. Clin Teach. 2013;10(4):242–245. doi:10.1111/tct.12014
42. Dyrbye LN, Shanafelt TD. Commentary: medical student distress: a call to action. Acad Med. 2011;86(7):801–803. doi:10.1097/ACM.0b013e31821da481
43. Tempski P, Martins MA, Paro HBMS. Teaching and learning resilience: a new agenda in medical education. Med Educ. 2012;46(4):345–346. doi:10.1111/j.1365-2923.2011.04207.x
44. Campbell J, Prochazka AV, Yamashita T, Gopal R. Predictors of persistent burnout in internal medicine residents: a prospective cohort study. Acad Med. 2010;85(10):1630–1634. doi:10.1097/ACM.0b013e3181f0c4e7
45. Eckleberry-Hunt J, Van Dyke A, Lick D, Tucciarone J. Changing the conversation from burnout to wellness: physician well-being in residency training programs. J Grad Med Educ. 2009;1(2):225–230. doi:10.4300/JGME-D-09-00026.1
46. Agarwal G, Karpouzian T. An exploratory analysis of work engagement, satisfaction, and depression in psychiatry residents. Acad Psychiatry. 2016;40(1):85–88. doi:10.1007/s40596-015-0459-x
47. Eckleberry-Hunt J, Lick D, Boura J, et al. An exploratory study of resident burnout and wellness. Acad Med. 2009;84(2):269–277. doi:10.1097/ACM.0b013e3181938a45
48. Zwack J, Schweitzer J. If every fifth physician is affected by burnout, what about the other four? Resilience strategies of experienced physicians. Acad Med. 2013;88(3):382–389. doi:10.1097/ACM.0b013e318281696b
49. Lamothe M, Boujut E, Zenasni F, Sultan S. To be or not to be empathic: the combined role of empathic concern and perspective taking in understanding burnout in general practice. BMC Fam Pract. 2014;15:15. doi:10.1186/1471-2296-15-15
50. Hojat M, Vergare MJ, Maxwell K, et al. The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Acad Med. 2009;84(9):1182–1191. doi:10.1097/ACM.0b013e3181b17e55
51. Shanafelt TD. Enhancing meaning in work: a prescription for preventing physician burnout and promoting patient-centered care. JAMA. 2009;302(12):1338–1340. doi:10.1001/jama.2009.1385
52. Shanafelt TD, West CP, Sloan JA, et al. Career fit and burnout among academic faculty. Arch Intern Med. 2009;169(10):990–995. doi:10.1001/archinternmed.2009.70
53. Doolittle BR, Windish DM, Seelig CB. Burnout, coping, and spirituality among internal medicine resident physicians. J Grad Med Educ. 2013;5(2):257–261. doi:10.4300/JGME-D-12-00136.1
54. Thomas NK. Resident burnout. JAMA. 2004;292(23):2880–2889. doi:10.1001/jama.292.23.2880
55. Haglund MEM, Aan Het Rot M, Cooper NS, et al. Resilience in the third year of medical school: a prospective study of the associations between stressful events occurring during clinical rotations and student well-being. Acad Med. 2009;84(2):258–268. doi:10.1097/ACM.0b013e31819381b1
Supplementary material
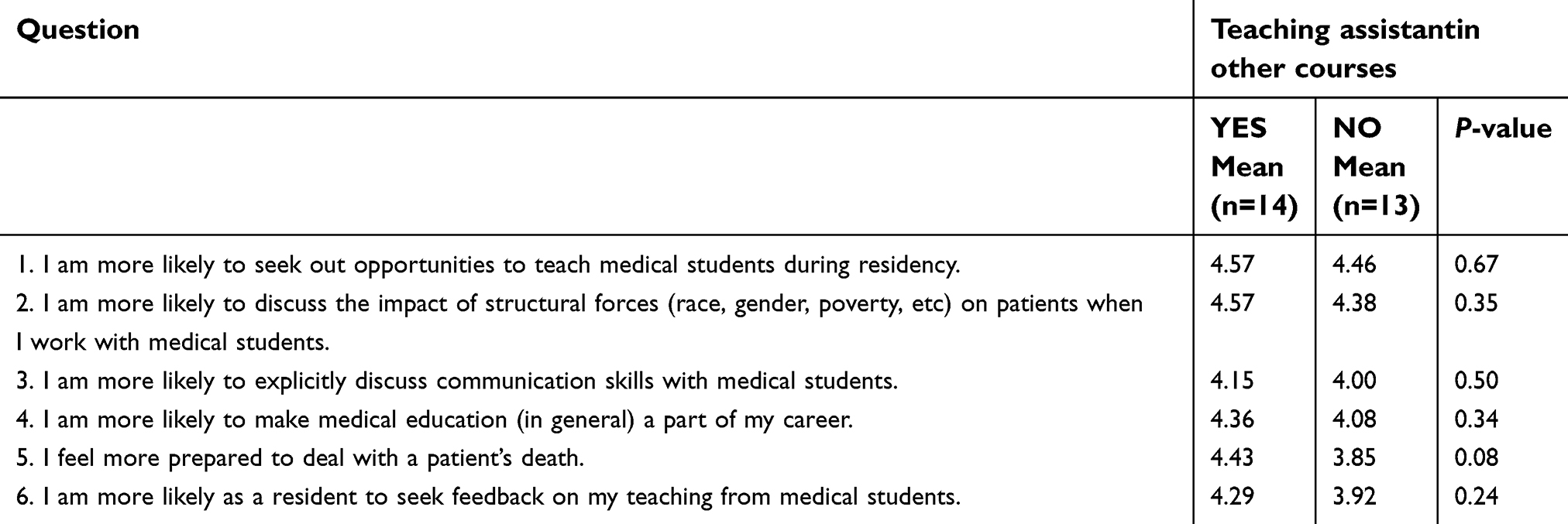 | Table S1 Educational responses by teaching assistant experience |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.