Back to Journals » Clinical Ophthalmology » Volume 17
Real-World Experience Using Intravitreal Brolucizumab Alone or in Combination with Aflibercept in the Management of Neovascular Age-Related Macular Degeneration
Authors Mehta N, Fong RD ![]() , Wilson M, Moussa K, Emami-Naeini P, Moshiri A, Yiu G
, Wilson M, Moussa K, Emami-Naeini P, Moshiri A, Yiu G ![]() , Park SS
, Park SS ![]()
Received 1 December 2022
Accepted for publication 9 February 2023
Published 27 February 2023 Volume 2023:17 Pages 657—665
DOI https://doi.org/10.2147/OPTH.S399590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Neesurg Mehta,1 Rodney D Fong,1,2 Machelle Wilson,3 Kareem Moussa,1 Parisa Emami-Naeini,1,4 Ala Moshiri,1 Glenn Yiu,1 Susanna S Park1
1Department of Ophthalmology and Vision Science, University of California Davis Health, Sacramento, CA, USA; 2University of Nevada, Reno School of Medicine, Reno, NV, USA; 3Department of Public Health Sciences, Division of Biostatistics, University of California, Davis, CA, USA; 4Department of Ophthalmology, Veterans Administration Hospital, Mather, CA, USA
Correspondence: Susanna S Park, Department of Ophthalmology & Vision Science, University of California Davis Health, Ernest E. Tschannen Eye Institute, 4860 Y St, Sacramento, CA, 95817, USA, Tel +1 916 734 6074, Fax +1 916 703 5076, Email [email protected]
Purpose: To evaluate real-world experience using intravitreal brolucizumab (IVBr), alone or in combination with aflibercept, in eyes with neovascular age-related macular degeneration (nAMD) treated previously with other inhibitors of VEGF (anti-VEGF).
Methods: This was a retrospective study of all eyes with nAMD treated with IVBr on a treat-and-extend protocol at a single center. Best-corrected visual acuity (BCVA), optical coherence tomography (OCT) at baseline and final visit, and drug-related adverse events were analyzed. Eyes with recurrent macular fluid on IVBr every 8 weeks were treated with a combination therapy alternating between IVBr and aflibercept every month.
Results: Among 52 eyes (40 patients) on IVBr, all had been previously treated with other anti-VEGF therapy, with 73% having persistent macular fluid. After a mean follow-up of 46.2± 27.4 weeks on IVBr, the mean treatment interval for intravitreal therapy increased to 8.8± 2.1 weeks on IVBr from a baseline of 6.1± 3.1 weeks (p< 0.001). Macular fluid decreased and BCVA was stable/improved in 61.5% of eyes on IVBr. Ten eyes with increased macular fluid on IVBr monotherapy when extended to every 8 weeks were treated with combination therapy alternating between IVBr and aflibercept every 4 weeks. In these eyes, 80% had improved macular fluid on OCT and 70% stable or improved BCVA after a median follow-up of 53 weeks on combination therapy. Mild intraocular inflammation developed in four eyes, all occurring on IVBr monotherapy, and none had associated vision loss.
Conclusion: In the real world, IVBr used to treat eyes with nAMD previously treated with other anti-VEGF therapies appears to be well tolerated and associated with an improvement in macular fluid, stabilization of BCVA, and/or increase in intravitreal treatment interval. Combination therapy alternating between IVBr and aflibercept monthly appears to be well tolerated and can be considered for eyes with macular fluid on IVBr every 8 weeks.
Keywords: age-related macular degeneration, aflibercept, anti-VEGF, brolucizumab, intravitreal injection; optical coherence tomography
Introduction
Neovascular age-related macular degeneration (nAMD) is the leading cause of vision loss in people aged 65 years or older in the US.1 Intravitreal anti-VEGF therapy has become the first line therapy for nAMD.2 Currently, there are several anti-VEGF drugs available for nAMD to limit vision loss, but they require repeated injections, usually indefinitely. Therefore, newer drugs with longer duration of effect are desired.
Intravitreal brolucizumab (IVBr) is a newer drug for nAMD approved by the US Food and Drug Administration (FDA) in 2019 based on the results of two phase III clinical trials—HAWK and HARRIER. These clinical trials showed that IVBr administered every 8 or 12 weeks was noninferior to aflibercept administered every 8 weeks.3,4 However, postmarketing data and post hoc analysis revealed an increased risk for intraocular inflammation (IOI), retinal vasculitis (RV), and retinal vascular occlusion (RVO) associated with IVBr when compared to aflibercept.5 Since some cases of RV and RVO resulted in vision loss, IVBr has not been adopted as widely as other anti-VEGF drugs.
In order to assess the real-world safety and efficacy of IVBr in the treatment of nAMD, we conducted a single-center retrospective analysis of all eyes with nAMD treated with IVBr and evaluated the visual and anatomic outcomes of these eyes. Our analysis includes a subset of eyes that were refractory to IVBr monotherapy every 8 weeks and received a combination therapy consisting of alternating doses of IVBr and aflibercept every month.
Methods
This retrospective, single-center study included consecutive patients with nAMD who received 6 mg IVBr therapy between January 2020 and November 2021 at the Department of Ophthalmology and Vision Science, University of California Davis Health, Sacramento, California. This study complied with the tenets of the Declaration of Helsinki and was approved by the Office of Human Research (Institutional Review Board) at the University of California Davis Health. No informed consent was obtained since requirement for informed consent was waived by the Office of Human Research, given the retrospective study design.
In this study population, all patients had been previously treated with IV anti-VEGF therapy for nAMD and were switched to IVBr for recalcitrant fluid on spectral-domain optical coherence tomography (OCT) or new macular hemorrhage on maximum therapy, desire for extension of treatment interval, or both (See Figure 1). All patients were put on a treat-and-extend protocol. There was no prespecified loading phase of IVBr, since all eyes had been treated previously with other anti-VEGF drugs. Demographic data, including age, ethnicity, and history of any concurrent retinal or uveitic conditions in the study eye, were recorded. Prior to the switch to IVBr therapy, the number and type of anti-VEGF injections administered in the study eye and presence of macular fluid on OCT, if any, was recorded. Information collected included best-corrected visual acuity (BCVA), number of IVBr injections, central subfield thickness (CST, µm) on OCT, and presence of fluid on OCT at final visit. Safety data were collected on the number of drug-related adverse events, including IOI. IOI related to IVBr included any new iritis, vitritis, RV, and RVO noted in the study eye on clinical exam after starting IVBr therapy, A decrease in macular fluid was defined as a reduction in CST on OCT. An increase in macular fluid was defined as an increase in CST on OCT with an increase in intraretinal fluid (IRF) and/or subretinal fluid (SRF) on OCT line scans. A subset analysis was conducted for eyes that had recurrent macular fluid on IVBr every 8 weeks and were treated with a combination therapy alternating between IVBr and aflibercept every month (Figure 1). For these eyes on combination therapy, the clinical data while on IVBr monotherapy were added to the total cohort.
 |
Figure 1 Flow diagram of study eyes with neovascular age-related macular degeneration (AMD) treated with intravitreal brolucizumab (IVBr) and included in the study. All eyes had had prior treatment with other intravitreal drugs that inhibit VEGF (anti-VEGF) before starting IVBr. Abbreviation: OCT, optical coherence tomography. |
Statistical Analysis
To calculate mean BCVA, mean logMAR BCVA was calculated and converted to Snellen VA equivalent. Summary statistics calculated and tests comparing patient demographics and clinical characteristics were conducted using SPSS 28.0.1.0. Mixed-effect regression models were used to evaluate change from baseline while controlling for length of follow-up. Baseline measurements were fitted using SAS 9.4 for Windows (SAS Institute, Cary, NC). p<0.05 was considered statistically significant.
Results
Demographic Data
We identified 52 eyes (40 patients) with nAMD treated with IVBr (Table 1). Mean age was 81.3±9.5 years, and 69.2% were female. All 52 eyes had been previously treated with other IV anti-VEGF agents before starting IVBr. The anti-VEGF agents used previously were 42 (80.8%) aflibercept, nine (19.3%) ranibizumab, and one (1.9%) bevacizumab. Median duration on anti-VEGF therapy prior to starting IVBr was 27.5 (2–69) months. Median number of anti-VEGF injections prior to starting IVBr was 20 (3–64). Median and mean treatment interval of the anti-VEGF treatments just prior to starting IVBr were 5.0 (3.5–17.5) weeks and 6.1±3.1 weeks, respectively. In sum, 23 eyes (44.2%) were switched to IVBr due to recalcitrant fluid (defined as either IRF, SRF, or both on OCT on maximum every 4 weeks therapy), 18 eyes (34.6%) were switched to IVBr to extend treatment interval, and eleven eyes (21.2%) were switched to IVBr for a combination of these two reasons.
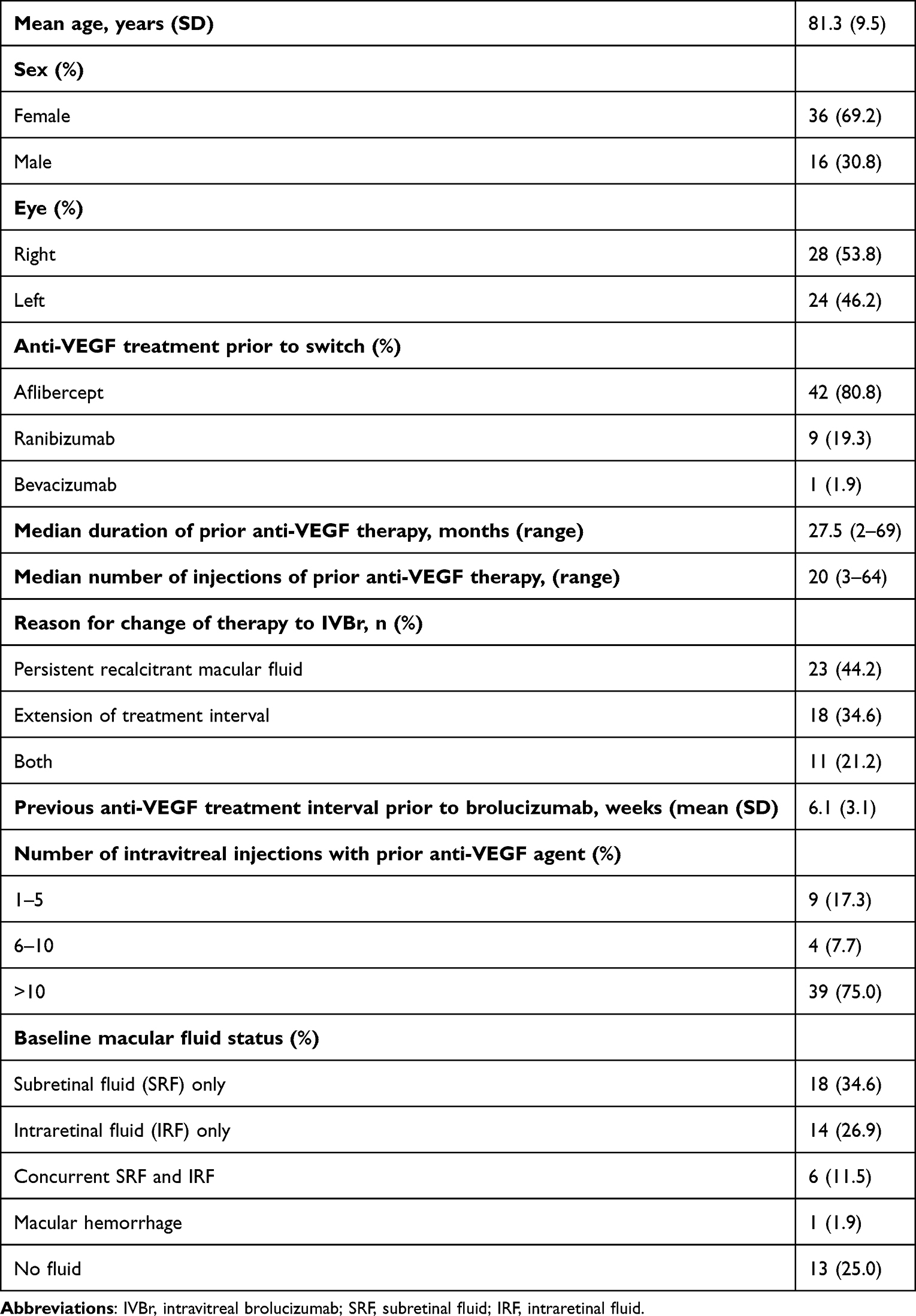 |
Table 1 Baseline characteristics of the study population |
Anatomic and Functional Outcomes—IVBr Monotherapy
At baseline prior to starting IVBr, mean logMAR BCVA was 0.599±0.544 (Snellen equivalent 20/80) and mean CST on OCT 291.5±112.9 µm. Macular OCT showed no fluid in 13 eyes (25.0%), SRF in 18 eyes (34.6%), IRF in 14 eyes (26.9%), and both IRF and SRF in six eyes (11.5%). One eye (1.9%) had a new macular hemorrhage. Median and mean duration of follow-up on IVBr were 37 (9–89) weeks and 46.2±27.4 weeks, respectively.
Table 2 summarizes the visual and anatomic changes noted in the study eyes after starting IVBr monotherapy. On IVBr, the mean number of injections was 7.1±3.3 with a median IVBr treatment interval between injections of 8 (4–15) weeks. Mean treatment interval on IVBr was 8.8±2.1 weeks, which was significantly increased from baseline of 6.1±3.1 weeks (p<0.001). At last visit on IVBr monotherapy, three eyes (5.8%) were on a 4- to 6-week treatment interval, 29 eyes (55.8%) on an 8-week interval, 15 (28.8%) on a 9- to 10- week interval, and five (9.6%) had extended to an interval of ≥12 weeks.
 |
Table 2 Visual and anatomic outcomes for intravitreal brolucizumab monotherapy and combined with intravitreal aflibercept |
At the final visit on IVBr monotherapy, 13 eyes (25%) had no fluid, 16 eyes (30.8%) had SRF, 16 eyes (30.8%) had IRF, and seven eyes (13.4%) had both SRF and IRF. Overall, macular fluid had decreased in 32 eyes (61.5%) from baseline with improvement in IRF and/or SRF on IVBr. BCVA was stable or improved in 32 eyes (61.5%) on IVBr, but the mean BCVA at final follow-up was 20/96, which was significantly worse than baseline mean BCVA of 20/80 (p=0.03) after controlling for length of follow-up and baseline BCVA (Table 2). The amount of change in BCVA from baseline was significantly associated with baseline BCVA (p=0.03). After controlling for variable length of follow-up and baseline CST, the mean CST at final follow-up was 276.8±87.1 μm, which trended lower but was not significantly different from baseline CST of 291.5±112.9 (p=0.14). Baseline CST was significantly associated with change in CST (p=0.012). For every unit increase in CST at baseline, the expected change in final CST was −0.42 after controlling for length of follow-up.
Before starting IVBr monotherapy, 14 eyes had no macular fluid (including one eye with new macular hemorrhage) and 38 (73%) eyes had residual macular fluid on OCT. Of the 14 eyes with no macular fluid at baseline, eight remained without macular fluid at last follow-up visit, and six had developed recurrent macular fluid after IVBr treatment interval was increased to every 8 weeks after the first three monthly loading doses. Of the 38 eyes with persistent macular fluid at baseline, seven (18.4%) achieved full resolution of fluid at a median 14 (4–60) weeks with an average treatment interval of 9.14±1.6 weeks, 18 (47.4%) had persistent fluid that was not worse at last follow-up, and 13 (34.2%) had initial resolution of fluid at a median 7 (4–80) weeks, but eventually had recurred macular fluid at a median 9 (7–17) weeks) after the IVBr treatment interval of was increased. The average IVBr treatment interval for these 31 eyes with persistent or recurrent macular fluid was 8.33±1.8 weeks.
Anatomic and Functional Outcomes—Combination-Therapy Subset
Ten eyes (ten patients) with recurrent or increased macular fluid after increasing IVBr treatment interval to 8 weeks were started on a combination therapy alternating between IVBr and aflibercept every month. All ten eyes in this combo group received Eylea monthly before switching to IVBr monotherapy. An alternating monthly dose of Eylea and IVBr was used in this combination-therapy group, because increased macular fluid was noted when IVBr treatment interval was increased to every 8 weeks after the first three loading doses of IVBr, as required for insurance coverage. The mean number of IVBr injections prior to the switch was 5.4±3.0. Just prior to starting combination therapy, mean BCVA and CST on OCT were 20/75 and 310±91.2 μm, respectively. The median period of follow-up on combination therapy was 53 (8–67) weeks. On this combination therapy with alternating anti-VEGF treatment every 4 weeks, macular fluid improved in 80% of eyes (eight of 10) and BCVA was stable or improved in 70% of eyes (seven of ten). Table 2 summarizes the visual and anatomic changes in these ten study eyes on combination therapy. At the final follow-up on combination therapy, mean BCVA was 20/88, which was not significantly different from baseline mean BCVA before starting combination therapy (p=0.47). Mean CST on OCT at the final visit was 257.7±110.5 μm, which trended lower than mean baseline CST before starting combination therapy (p=0.06). In all ten eyes on combination therapy, recurrence of macular fluid between anti-VEGF injections was minimized. However, OCT at 4 weeks after IVBr tended to look slightly drier than OCT at 4 weeks after Eylea.
Safety
Four eyes (7.6%) of four patients developed IOI and IVBr was stopped. None of the eyes was on combination therapy. IOI occurred after the second IVBr injection in one eye, after the third IVBr injection in two eyes, and after the fourth IVBr injection in one eye. Median time to IOI after starting IVBr was 22 (6–39 weeks). Time from last IVBr injection to development of IOI ranged from 6 to 79 days. IOI included mild iritis (three eyes) or vitritis (one eye), which resolved with topical corticosteroids in three eyes and without treatment in one. No RV or RVO was seen. No eye had vision loss associated with IOI. No serious adverse ocular events, such as endophthalmitis, retinal detachment, retinal tear, macular hole, or vitreous hemorrhage, was noted.
Discussion
IV anti-VEGF therapy for nAMD has limited duration of effect and requires frequent retreatment, often indefinitely. Therefore, newer therapy with longer duration of effect is desired. Based on the results of the HAWK and HARRIER studies, IVBr may be a newer anti-VEGF treatment for nAMD that achieves this aim. When administered every 8 and 12 weeks, IVBr was not inferior to aflibercept administered every 8 weeks in terms of BCVA and OCT. The study eyes receiving IVBr gained on average six letter on BVCA, and 76% of patients had resolution of fluid over 96 weeks.6 Furthermore, 37%–45% of patients were able to be maintained on an every-12-week treatment regimen.
However, it is well known that fixed anti-VEGF treatment regimens and well-defined inclusion and exclusion criteria used in clinical trials of anti-VEGF therapy for nAMD usually result in better functional and anatomic outcomes7,8 when compared to real-world data.9–11 Therefore, it is important to consider both clinical trials and real-world data when discussing treatment options for nAMD with patients.
In this study, we conducted a real-world analysis of the long-term anatomic and visual outcomes of eyes with nAMD treated with IVBr. None of the eyes was treatment-naïve, unlike the HAWK and HARRIER studies.6 Most of our study eyes had recalcitrant nAMD with persistent macular fluid, requiring very frequent anti-VEGF injections prior to starting IVBr. In fact, the indication for changing treatment to IVBr was persistent macular fluid on anti-VEGF therapy every 4 weeks and/or the desire to increase treatment interval due to high retreatment burden.
Despite these baseline characteristics of our study eyes, macular fluid decreased in 61.5% of eyes and BCVA was stable or improved in 61.5% of eyes after changing to IVBr. Of the 38 eyes with persistent macular fluid before starting IVBr therapy, 18.4% achieved full resolution of IRF and SRF at a median 14 weeks after starting IVBr, and 47% had improved or stable macular fluid on IVBr. Slightly more than half of the eyes on IVBr were maintained on an 8-week treatment interval, and 10% had the interval extended to 12 weeks or beyond without increase in macular fluid. Thirteen eyes initially achieved full resolution of macular fluid on IVBr, but fluid recurred as treatment interval increased to every 8 weeks. Among them, ten eyes were changed to combination therapy alternating between IVBr and aflibercept monthly to limit fluid recurrence.
VA was stable or improved in a majority of our study eyes on IVBr, but visual outcome was not as positive as the HAWK and HARRIER studies due to differences in baseline characteristics and treatment regimen protocols. In fact, our study showed a decrease in mean BCVA at the last follow-up on IVBr when compared to baseline. This decrease was statistically significant and noted after adjusting for the variable duration of follow-up of our study population. Further statistical analysis demonstrated that the amount of change in BCVA from baseline was significantly associated with baseline BCVA. Given that the mean duration of follow-up of our study was 46 weeks on IVBr and all eyes had prior anti-VEGF therapy for nAMD, a decrease in mean BCVA was not unexpected in our study population, since AMD is a progressive disease. Prior extended follow-up studies of treatment-naïve eyes with nAMD on chronic anti-VEGF therapy showed that mean BCVA improvement noted in the first 2 years on anti-VEGF therapy was lost with extended follow-up, due to progression of AMD and development of geographic atrophy involving the fovea.9,11 In our study population, which included eyes with recalcitrant nAMD with chronic macular fluid on prior anti-VEGF therapy, vision loss may have occurred sooner, since chronic macular fluid likely results in structural damage to the macula and vision decrease over time.12
Our real-world study with mean follow-up of 46 weeks on IVBr is unique, as it evaluates longer effects of IVBr therapy in eyes with nAMD with persistent activity on other anti-VEGF therapies. Several real-world studies have shown good anatomic and visual improvement at 4 weeks13,14 and 7 weeks15,16 after one IVBr injection. There is limited real-world information on the long-term effects of IVBr in nAMD.
Our study is the first to report the outcomes of eyes with nAMD refractory to IVBr monotherapy every 8 weeks that were switched to a combination therapy of IVBr and aflibercept alternating monthly. All ten eyes that received this combination therapy had increased macular fluid on OCT on IVBr every 8 weeks when compared to OCT when IVBr was administered more frequently than every 8 weeks. All ten eyes had a history of increased macular fluid on Eylea every 4 weeks before starting IVBr. We could not administer IVBr more frequently than every 8 weeks after the first three loading doses in these eyes, since more frequent IVBr dosing was not covered by insurance. Thus, these eyes were treated with alternating monthly doses of IVBr and Eylea. Of the ten eyes on this combination regimen, macular fluid improved in 80% and BCVA was stable or improved in 70% over mean follow-up of 53 weeks when maintained on every-4-week anti-VEGF injection, alternating between IVBr and Eylea. This novel combination of anti-VEGF therapy appears to be well tolerated. None of the eyes developed IOI. Therefore, in eyes that have recurrent fluid on every-8-week IVBr monotherapy, this regimen may be considered.
Following the FDA approval of IVBr in 2019,4 several cases of RV and RVO were reported.17–20 A post hoc analysis of the HAWK and HARRIER studies revealed that 4.6% of eyes had probable IOI, with 50% and 75% cases of IOI and/or RV and/or RVO occurring within the first 3 months and 6 months, respectively.5 Khanani et al reported the incidence of IOI as approximately 2.4% in the IRIS registry.21 In our study, four eyes (7.6%) developed mild IOI after a median time of 22 (6–39) weeks after starting IVBr. Our rate is somewhat higher than prior reports. Although there was no standard protocol to evaluate IOI in our study population in this retrospective study, all the authors made a point to carefully evaluate all eyes on IVBr for signs of iritis, vitritis, RV, or RVO using slit-lamp and indirect ophthalmoscopy. This was based on reports of IOI related to IVBr that became public after our study patients were started on IVBr,17–20 No angiography was done on any of the study eyes to evaluate for RV or RVO, since none was suspected on exam. Whether this latter fact underdiagnosed subclinical RV and RVO is unknown.
Although the rate of IOI was higher with IVBr than aflibercept in HAWK and HARRIER, the overall rate of vision loss was not different between the drugs.5 In our study, all cases of IOI were mild and not associated with vision loss. Given these observations, it is important to tailor the treatment of nAMD for each individual after a detailed discussion of the relative risk and benefit of the various anti-VEGF drugs for nAMD. Depending on the patient’s perspective, the benefit of potentially increasing the treatment interval using IVBr might offset the risk of IOI on IVBr. Since a majority of cases of IOI on IVBr are seen in eyes receiving initial monthly loading doses of IVBr,5 combination therapy alternating between IVBr with aflibercept is an alternative approach that can be considered to increase anti-VEGF effects in nAMD eyes without increasing IVBr dosing.
Our study has several limitations: its retrospective nature, limited sample size, and some inconsistencies in initiation and dosing of IVBr. Most eyes started IVBr after at least three doses of other anti-VEGF therapy, but one eye started IVBr after two doses of other anti-VEGF drugs due to lack of response. On initiation of IVBr, there was no preset required loading phase of IVBr, since these eyes had had prior treatment with anti-VEGF. In order to minimize the risk of IOI, the authors aimed to initiate extension of treatment interval as soon as maximum response was achieved on IVBr. Furthermore, the treat-and-extend regimens varied depending on the degree of activity of CNV and history of response to prior anti-VEGF therapy: some eyes were extended at 2-week intervals and others at 1-week intervals.
Despite these limitations, this real-world study provides longer follow-up information and new insights regarding the safety and efficacy of IVBr in treating nAMD. Although a newer anti-VEGF therapy has been FDA-approved recently, IVBr used alone or in combination with other anti-VEGF agents remains a treatment option to be considered in treating eyes with nAMD, especially when inadequate response is observed with other anti-VEGF drugs.
Conclusion
In this real-world retrospective study, IVBr was used to treat nAMD eyes that had been previously treated with other anti-VEGF drugs. In a majority of these eyes, IVBr use was associated with an improvement in macular fluid, stabilization of BCVA, and/or increase in treatment interval. Mild IOI was noted in a few eyes and not associated with vision loss. In eyes with macular fluid on IVBr monotherapy every 8 weeks, combination therapy alternating between IVBr and aflibercept monthly may be beneficial and well tolerated.
Abbreviations
nAMD, neovascular age-related macular degeneration; IVBr, intravitreal brolucizumab; FDA, Food and Drug Administration; IOI, intraocular inflammation; RV, retinal vasculitis; RVO, retinal vascular occlusion; OCT, optical coherence tomography; BCVA, best-corrected visual acuity; CST, central subfield thickness; IRF, intraretinal fluid; SRF, subretinal fluid.
Acknowledgment
This work was supported in part by the Barbara A and Alan M Roth MD Endowed Chair in Visual Science from the University of California Davis (SSP). There was no other funding support.
Disclosure
Dr Glenn Yiu reports personal fees from AbbVie, Adverum, Alimera, Bausch & Lomb, Clearside, Endogena, Genentech, Gyroscope, Intergalactic, Iridex, Janssen, Myro, NGM Biopharmaceutical, Novartis, Regeneron, Thea, Topcon, and Zeiss, outside the submitted work. Professor Dr Susanna S Park reports grants from Roche/Novartis and Ophthea outside the submitted work. The authors report no other conflicts of interest directly related to this work.
References
1. CDC. Common eye disorders and diseases; 2020. Available from: https://www.cdc.gov/visionhealth/basics/ced/index.html.
2. Flaxel CJ, Adelman RA, Bailey ST, et al. Age-related macular degeneration preferred practice pattern®. Ophthalmology. 2020;127:1–65. doi:10.1016/j.ophtha.2019.09.024
3. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127:72–84. doi:10.1016/j.ophtha.2019.04.017
4. Novartis Pharmaceuticals Corporation. BEOVU- Brolucizumab Injection, Solution, [package insert]; 2022. Available from: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=5d1dc1fa-a2d3-46ed-9e9a-c1a036590d3d.
5. Monés J, Srivastava SK, Jaffe GJ, et al. Risk of inflammation, retinal vasculitis, and retinal occlusion-related events with brolucizumab: post hoc review of HAWK and HARRIER. Ophthalmology. 2021;128:1050–1059. doi:10.1016/j.ophtha.2020.11.011
6. Dugel PU, Singh RP, Koh A, et al. HAWK and HARRIER: ninety-six-week outcomes from the phase 3 trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2021;128:89–99. doi:10.1016/j.ophtha.2020.06.028
7. Schmidt-Erfurth U, Kaiser PK, Korobelnik JF, et al. Intravitreal aflibercept injection for neovascular age-related macular degeneration: ninety-six-week results of the VIEW studies. Ophthalmology. 2014;121:193–201. doi:10.1016/j.ophtha.2013.08.011
8. Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116:57–65.e5. doi:10.1016/j.ophtha.2008.10.018
9. Maguire MG, Martin DF, Ying G-S; Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group, et al. 5-year outcomes with anti-VEGF treatment of neovascular Age-related Macular Degeneration (AMD): the comparison of AMD treatments trials. Ophthalmology. 2016;123:1751–1761. doi:10.1016/j.ophtha.2016.03.045
10. Khanani AM, Gahn GM, Koci MM, Dang JM, Brown SM, Hill LF. Five-year outcomes of intravitreal drug therapy for neovascular age-related macular degeneration in eyes with baseline vision 20/60 or better. Clin Ophthalmol Auckl NZ. 2019;13:347–351. doi:10.2147/OPTH.S191170
11. Rofagha S, Bhisitkul RB, Boyer DS, Sadda SR, Zhang K; SEVEN-UP Study Group. Seven-year outcomes in ranibizumab-treated patients in ANCHOR, MARINA, and HORIZON: a multicenter cohort study (SEVEN-UP). Ophthalmology. 2013;120:2292–2299. doi:10.1016/j.ophtha.2013.03.046
12. Metrangolo C, Donati S, Mazzola M, et al. OCT biomarkers in neovascular age-related macular degeneration: a narrative review. J Ophthalmol. 2021;2021:9994098. doi:10.1155/2021/9994098
13. Bulirsch LM, Saßmannshausen M, Nadal J, Liegl R, Thiele S, Holz FG. Short-term real-world outcomes following intravitreal brolucizumab for neovascular AMD: SHIFT study. Br J Ophthalmol. 2021;bjophthalmol-2020–318672. doi:10.1136/bjophthalmol-2020-318672
14. Avaylon J, Lee S, Gallemore RP. Case series on initial responses to intravitreal brolucizumab in patients with recalcitrant chronic wet age-related macular degeneration. Int Med Case Rep J. 2020;13:145–152. doi:10.2147/IMCRJ.S252260
15. Sharma A, Kumar N, Parachuri N, et al. Brolucizumab—early real-world experience: BREW study. Eye. 2021;35:1045–1047. doi:10.1038/s41433-020-1111-x
16. Chakraborty D, Maiti A, Sheth JU, et al. Brolucizumab in neovascular age-related macular degeneration – Indian real-world experience: the BRAILLE Study. Clin Ophthalmol. 2021;15:3787–3795. doi:10.2147/OPTH.S328160
17. Jain A, Chea S, Matsumiya W, et al. Severe vision loss secondary to retinal arteriolar occlusions after multiple intravitreal brolucizumab administrations. Am J Ophthalmol Case Rep. 2020;18:100687. doi:10.1016/j.ajoc.2020.100687
18. Haug SJ, Hien DL, Uludag G, et al. Retinal arterial occlusive vasculitis following intravitreal brolucizumab administration. Am J Ophthalmol Case Rep. 2020;18:100680. doi:10.1016/j.ajoc.2020.100680
19. Witkin AJ, Hahn P, Murray TG, et al. Occlusive retinal vasculitis following intravitreal brolucizumab. J Vitreoretin Dis. 2020;4:269–279. doi:10.1177/2474126420930863
20. Baumal CR, Spaide RF, Vajzovic L, et al. Retinal vasculitis and intraocular inflammation after intravitreal injection of brolucizumab. Ophthalmology. 2020;127:1345–1359. doi:10.1016/j.ophtha.2020.04.017
21. Khanani AM, Zarbin MA, Barakat MR, et al. Safety outcomes of brolucizumab in neovascular age-related macular degeneration: results from the IRIS registry and Komodo healthcare map. JAMA Ophthalmol. 2022;140:20–28. doi:10.1001/jamaophthalmol.2021.4585
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Morphological and Functional Assessment of the Optic Nerve Head and Retinal Ganglion Cells in Dry vs Chronically Treated Wet Age-Related Macular Degeneration
Wichrowska M, Wichrowski P, Kocięcki J
Clinical Ophthalmology 2022, 16:2373-2384
Published Date: 28 July 2022
Brolucizumab for the Treatment of Degenerative Macular Conditions: A Review of Clinical Studies
Karasavvidou EM, Tranos P, Panos GD
Drug Design, Development and Therapy 2022, 16:2659-2680
Published Date: 9 August 2022
A Real-World, Multicenter, 6-Month Prospective Study in Greece of the Effectiveness and Safety of Ranibizumab in Patients with Age-Related Macular Degeneration Who Have Inadequately Responded to Aflibercept: The “ELEVATE” Study
Rouvas A, Datseris I, Androudi S, Tsilimbaris M, Kabanarou SA, Pharmakakis N, Koutsandrea C, Charonis A, Kousidou O, Pantelopoulou G
Clinical Ophthalmology 2022, 16:2579-2593
Published Date: 12 August 2022
Efficacy, Safety, and Durability of Brolucizumab: An 8-Month Post-Marketing Surveillance Analysis
Saba NJ, Walter SD
Clinical Ophthalmology 2023, 17:2791-2802
Published Date: 20 September 2023
Brolucizumab versus Aflibercept in Patients with Diabetic Macular Edema: A Meta-Analysis of Randomized Controlled Trials
Justino LB, Justino GB, Graffunder FP, Binotti WW, Khodor A, Caranfa JT
Clinical Ophthalmology 2024, 18:3679-3690
Published Date: 10 December 2024