Back to Journals » Clinical Ophthalmology » Volume 16
A Real-World, Multicenter, 6-Month Prospective Study in Greece of the Effectiveness and Safety of Ranibizumab in Patients with Age-Related Macular Degeneration Who Have Inadequately Responded to Aflibercept: The “ELEVATE” Study
Authors Rouvas A, Datseris I, Androudi S, Tsilimbaris M, Kabanarou SA ![]() , Pharmakakis N, Koutsandrea C, Charonis A, Kousidou O
, Pharmakakis N, Koutsandrea C, Charonis A, Kousidou O ![]() , Pantelopoulou G
, Pantelopoulou G ![]()
Received 27 April 2022
Accepted for publication 1 August 2022
Published 12 August 2022 Volume 2022:16 Pages 2579—2593
DOI https://doi.org/10.2147/OPTH.S371036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alexandros Rouvas,1 Ioannis Datseris,2 Sofia Androudi,3 Miltiadis Tsilimbaris,4 Stamatina A Kabanarou,5 Nikolaos Pharmakakis,6 Chryssanthi Koutsandrea,7 Alexander Charonis,8 Olga Kousidou,9 Georgia Pantelopoulou9
1 2nd Department of Ophthalmology, Attikon Hospital, National and Kapodistrian University of Athens, Athens, Greece; 2OMMA Ophthalmological Institute of Athens, Athens, Greece; 3Ophthalmology Clinic, University of Thessaly, Larissa, Greece; 4Ophthalmological Clinic, University of Crete Medical School, Heraklion, Greece; 5Department of Ophthalmology, General Hospital of Athens ‘korgialenio-Benakio’, Athens, Greece; 6Department of Ophthalmology, University of Patras, Patras, Greece; 7Department of Ophthalmology, National and Kapodistrian University of Athens, Athens, Greece; 8Retina Service, Athens Vision Eye Institute, Athens, Greece; 9Medical Department, Novartis (Hellas), Athens, Greece
Correspondence: Olga Kousidou, Medical Department, Novartis (Hellas), National Road No. 1 12th Km, Metamorphosis, Athens, GR-144 51, Greece, Tel +30 210 289 7189, Fax +302102835053, Email [email protected]
Purpose: Real-world evidence on short-term outcomes of ranibizumab in wet age-related macular degeneration (wAMD) following inadequate response to aflibercept is scarce. This study aimed to evaluate the functional and anatomic effects of switching to ranibizumab in cases of wAMD previously treated with aflibercept with inadequate response.
Patients and Methods: Prospective, observational study performed in eight ophthalmology hospital/private clinics in Greece, enrolling consented patients with active wAMD, ≥ 50 years-old, who had initiated ranibizumab ≥ 28 days and < 2 months after their last aflibercept injection. Data were collected at enrollment, and at 1, 3 and 6 months post-treatment onset (post-baseline).
Results: Between September-2015 and November-2017, 103 eligible patients (56.3% females; mean age: 74.8± 8.6 years) were consecutively enrolled. The age at AMD diagnosis in the study eye was 71.3± 8.8 years. Aflibercept (median of 5 injections received over 11.3 months) had been discontinued for anatomical (in 69.9%) and/or functional (38.8%) reasons. At baseline (median: 24.3 months after wAMD diagnosis), choroidal neovascularization was occult in 69.1% of evaluable study eyes; 60.2% of the study eyes had pigment epithelial detachment (PED); 42.7% cysts; 21.4% fibrosis; 66.0% subretinal, and 59.2% intraretinal fluid. At 6 months post-baseline: a median of 3 ranibizumab injections (range: 1– 6) had been received; the best-corrected visual acuity (BCVA)≥ 0 letter gain rate was 81.8%; the BCVA ≥ 15 letter gain rate was 17.0%; BCVA gain was 3.2 letters [mean increase: 3.2± 10.0 letters; median: 0.0; p = 0.002]; PED greatest basal diameter (GBD; median: 1470.5 μm) also decreased (median decrease: 114.0 μm; p = 0.019). Baseline central retinal thickness (CRT; median: 312.0 μm) remained unchanged. One patient permanently discontinued ranibizumab due to adverse event occurrence, assessed as not causally related to ranibizumab. There were no ranibizumab-related adverse reactions.
Conclusion: Six-month treatment with ranibizumab in aflibercept inadequate responders led to visual acuity and PED GBD improvements, with no statistically significant CRT change.
Keywords: best corrected visual acuity, central retinal thickness, pigment epithelial detachment
Introduction
Age-related macular degeneration (AMD) is a progressive, degenerative disease of the retina, and a leading cause of vision loss worldwide.1 It is estimated that in 2020, 196 million people worldwide will be suffering from AMD, with this figure rising to 288 million by 2040.2 Neovascular or wet AMD (wAMD) accounts for 10% of all AMD cases; nevertheless, it contributes to 90% of all severe vision loss cases associated with AMD.3 wAMD is characterized by choroidal neovascularization (CNV), ie, growth of abnormal blood vessels from the choroid layer into the subretinal space.4
Vascular endothelial growth factor (VEGF) plays a pivotal role in the pathogenesis of CNV. As a result, the introduction of anti-VEGF agents for the treatment of wAMD has drastically altered the standard of care in retinal medicine, substantially lowering the rates of legal blindness and visual impairment.5,6 Four anti-VEGF agents have been evaluated for the treatment of wAMD: pegaptanib, bevacizumab, ranibizumab, and aflibercept, of which ranibizumab and aflibercept are those most commonly used in routine care.7,8
The clinical efficacy and safety profile of ranibizumab in the treatment of subfoveal wAMD were established in two randomized clinical trials, ANCHOR and MARINA,9,10 and further validated in long-term studies11–13 and a 1-year retrospective analysis of real-world data from four European registries.14 Real-world evidence on the effectiveness of ranibizumab in the treatment of wAMD mainly stems from reports in treatment-naïve patients.15 However, reports in patients who have switched from another anti-VEGF are also needed, since due to the observed inadequate response of some patients to anti-VEGF agents or to their acquired resistance to treatment, following an initial good response, switching between agents has become common place in routine care. Despite the wealth of studies in eyes switched from ranibizumab to aflibercept,16–23 reports on patients who switched from aflibercept to ranibizumab are rather limited,24–27 mainly including retrospective studies involving eyes that were switched back to ranibizumab following inadequate response to aflibercept.28–30
In light of the above, this non-interventional, prospective study mainly aimed to provide real-world data on the six-month effects of ranibizumab on anatomical and visual acuity outcomes in eyes with active neovascular AMD, that were previously treated with aflibercept and showed inadequate response, in a representative sample of patients treated in the routine care of Greece.
Materials and Methods
Study Design, Setting, and Population
This was a multicenter, observational, 6-month prospective study conducted by retina specialists practicing in hospitals/private clinics in Greece. The study was performed in accordance with the Guidelines for Good Pharmacoepidemiology Practice of the International Society for Pharmacoepidemiology, the ethical principles laid down in the Declaration of Helsinki, and all applicable national regulatory requirements. The study protocol and informed consent form were approved by the Institutional Review Boards of the participating hospital sites before the enrollment of any patient in the study and performance of any study-related procedures. Signed written informed consent was obtained from all patients.
The study included male and female patients aged ≥50 years with active CNV secondary to AMD in the study eye and an inadequate response (according to the physician’s judgment) to aflibercept, after at least one injection prior to switching to ranibizumab. The reason(s) for aflibercept discontinuation were anatomical and/or functional; aflibercept could not have been discontinued for safety reasons, in order for the patient to be included in the study. The last aflibercept injection was received between 28 days and 2 months prior to ranibizumab treatment onset. Patients were required to have available optical coherence tomography (OCT) and visual acuity assessments in the study eye during the period elapsed between the last injection of aflibercept and the first injection of ranibizumab. Patients were treated with ranibizumab (Lucentis®) according to the summary of product characteristics. The decision to prescribe ranibizumab was taken prior to the patients’ enrollment and was separated from the physician’s decision to include the patient in the study. If both eyes were eligible, the eye with the greater central retinal thickness (CRT) at ranibizumab treatment onset (baseline) was selected for entry into the study. Patients were excluded from study participation if they had initiated treatment with ranibizumab more than 28 days prior to enrollment as well as in case they had received concurrent treatment with any investigational drug/device/intervention in either eye for any ocular condition. Data were collected using a web-based data capture system during four visits: at study enrollment and at approximately 1, 3, and 6 months post-baseline. A diagram of the study design is shown in Figure 1A.
 |
Figure 1 (A) Study design. (B) Study patient flow chart displaying number of patients enrolled, eligible and who completed study participation. Adverse event occurrence corresponds to deterioration of macular edema and increase of intraretinal fluid. |
Study Objectives and Outcomes
The study’s primary objective was to evaluate anatomical improvements after six months of treatment with ranibizumab in patients with an inadequate response to aflibercept. The relevant outcomes were the mean change in CRT (μm) and pigment epithelial detachment (PED) dimensions [maximal PED height (MH, μm) and greatest basal diameter (GBD, μm)] from baseline at 6 months post-baseline. Secondary outcomes included changes in CRT and PED dimensions at 1 and 3 months post-baseline, and changes in BCVA measurements from baseline at 1, 3 and 6 months post-baseline, including the percentages of patients with a gain of ≥15 letters, loss or gain of <15 letters and loss of ≥15 letters at 6 months post-baseline; the number of ranibizumab injections over the 6-month study observation period; and the incidence of ocular and systemic adverse events over the 6-month study observation period.
Assessments
OCT was used for measuring CRT (μm) and PED MH (μm) and GBD (μm). Early Treatment Diabetic Retinopathy Study (ETDRS) charts and Snellen charts were used to assess the BCVA, according to the physicians’ routine practice. Snellen scores were converted to ETDRS scores using the following formula: ETDRS = 85 + 50 x log (Snellen fraction).31 Physicians were strongly encouraged to use the same rater and same OCT instrument and visual acuity charts for all study-related measurements throughout the study to avoid inter-instrument and inter-rater variability.
Statistical Analysis
The normality of distribution of continuous variables was assessed using the Shapiro–Wilk test. The statistical significance of changes of CRT, PED dimensions and BCVA between baseline and post-baseline timepoints was evaluated using the Wilcoxon signed-rank test. Due to the large number of missing/non-evaluable observations (>20%) in regard to the study’s primary endpoint, the Last Observation Carried Forward (LOCF) imputation method has been applied. More specifically, in case of a missing CRT, PED MH and PED GBD measurements at 6 months (± 3 weeks) among patients with at least one post-baseline assessment, the last recorded CRT/PED measurement prior to 6 months has been carried forward. The impact of various patient, disease, and treatment characteristics on CRT changes between baseline and the 6-month post-baseline timepoint was examined using multivariable linear regression analysis. The final multivariable model was selected using a stepwise method based on the minimization of the Akaike information criterion. All statistical tests were two-sided and performed at a 0.05 significance level. Statistical analyses were performed using SAS® statistical analysis software (v.9.4; SAS Institute, Cary, NC).
Sample Size Estimation
In light of the heterogeneity of CRT changes (study’s primary outcome) among studies in patients with wAMD switching between different anti-VEGF therapies,32–37 the highest reported SD of the change in CRT (SD: 93 μm), and the smallest reported mean change (−27 μm) were used for sample size calculation. Accordingly, 96 to 130 evaluable patients were estimated to be required to detect a mean CRT change of 27.0 μm, with an SD of 93.0, at a power ranging from 80% to 90%, respectively, using a paired t-test with a 0.05 two-sided significance level. Furthermore, this sample was considered sufficient to estimate an adequately powered change in PED dimensions (study’s co-primary endpoint) based on published data; in particular, assuming the lowest reported change of 46 μm with an SD of 87.0 μm,18,33,35,38 31 to 40 patients are required to detect the aforementioned difference with a power ranging from 80% to 90%. Therefore, the study originally sought to enroll a minimum of 96 evaluable patients. Nonetheless, a total of 72 patients were finally evaluable for the study primary endpoint of change in CRT (restricting the initially assumed power), while the target sample size of 31–40 patients was met for the co-primary endpoint.
Results
Patient Disposition
Between 09-September-2015 and 30-November-2017, a total of 103 eligible patients were enrolled in the study by eight ophthalmology hospital and private clinics located in four of the 13 administrative regions in Greece; 71.8% of the patients were enrolled by five clinics in Attica. The median [interquartile range (IQR)] duration of follow-up was 5.8 (5.6, 6.1) months, with 97 patients attending the 6-month visit and six patients withdrawing (Figure 1B) after a mean (standard deviation; SD) period of 3.4 (2.9) months post-enrollment.
Patients’ Characteristics at Enrollment
At enrollment, the patients’ mean age was 74.8 years, and 97.1% had at least one medical condition/surgery/comorbidity. The patients’ characteristics at enrollment and the medical conditions/surgeries/comorbidities reported for ≥10% of the patients are presented in Table 1.
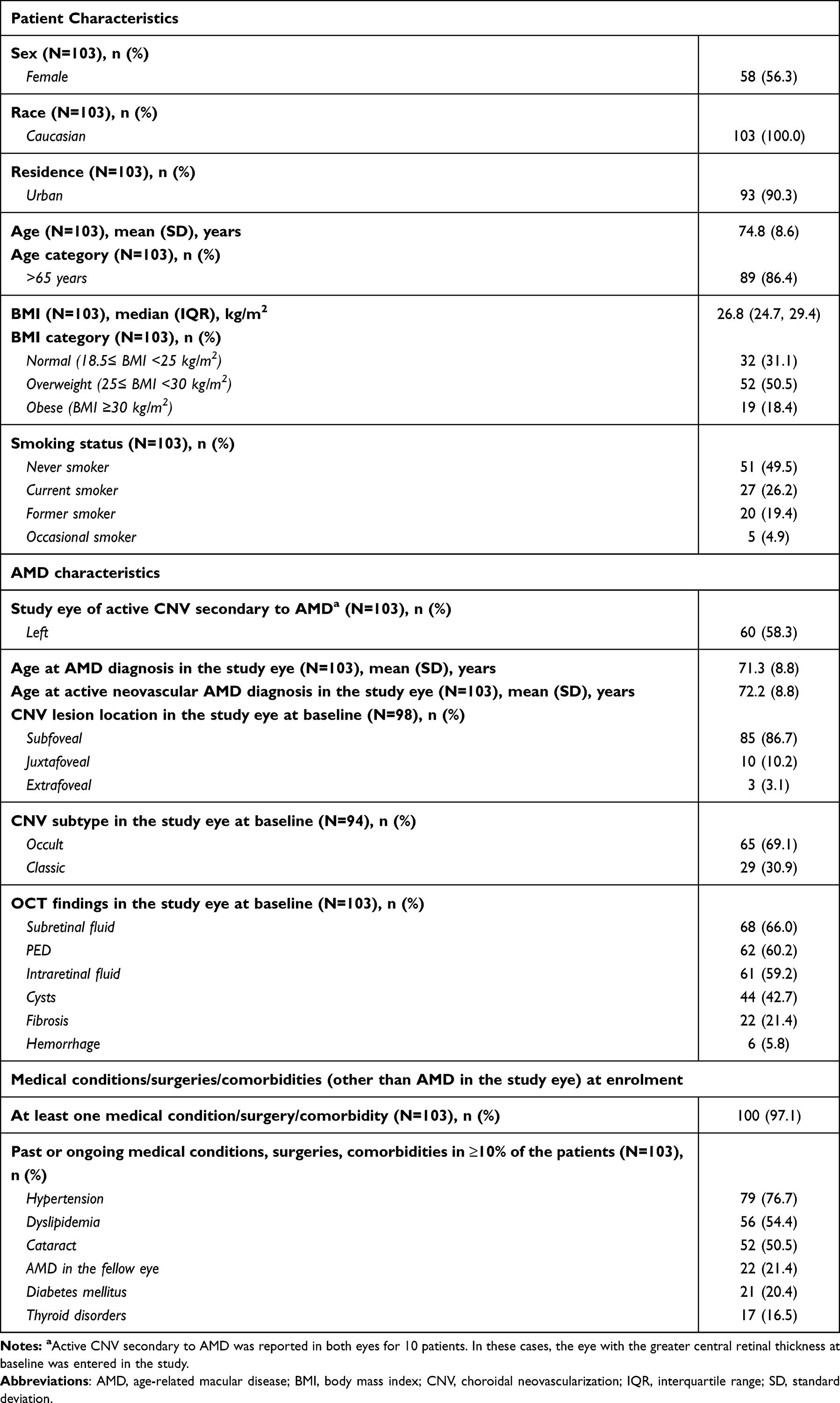 |
Table 1 Patient and Disease Characteristics at Enrollment |
wAMD Diagnosis and Treatment
Patients had been diagnosed with AMD in the study eye at a mean (SD) age of 71.3 (8.8) years. At baseline, occult CNV was reported for 69.1% (65/94) of the evaluable study eyes. In addition, 60.2% (62/103) of the study eyes had PED, with a median (IQR) MH and GBD of 262.5 (149.0, 408.0) μm and 1470.5 (918.0, 2977.0) μm, respectively. The baseline median (IQR) BCVA (ETDRS) was 50.0 (35.0, 65.0) letters (assessed by Snellen charts), while the median (IQR) CRT was 312.0 (251.0, 401.0) μm [assessed with a spectral-domain OCT in 98.1% of the cases]. Based on baseline OCT, subretinal fluid was present in 66.0% of the study eyes, intraretinal fluid in 59.2%, cysts in 42.7%, fibrosis in 21.4%, and hemorrhage in 5.8% (Table 1).
The immediately prior aflibercept treatment had been initiated a median of 6.3 months after wAMD diagnosis and discontinued a median of 49.0 days prior to ranibizumab onset, with a median (IQR) of 5 (3, 7) aflibercept injections received over a median period of 11.3 months (Table 2). The reasons for aflibercept discontinuation were exclusively anatomical in 61.2%, exclusively functional in 30.1%, and both anatomical and functional in 8.7% of the study eyes.
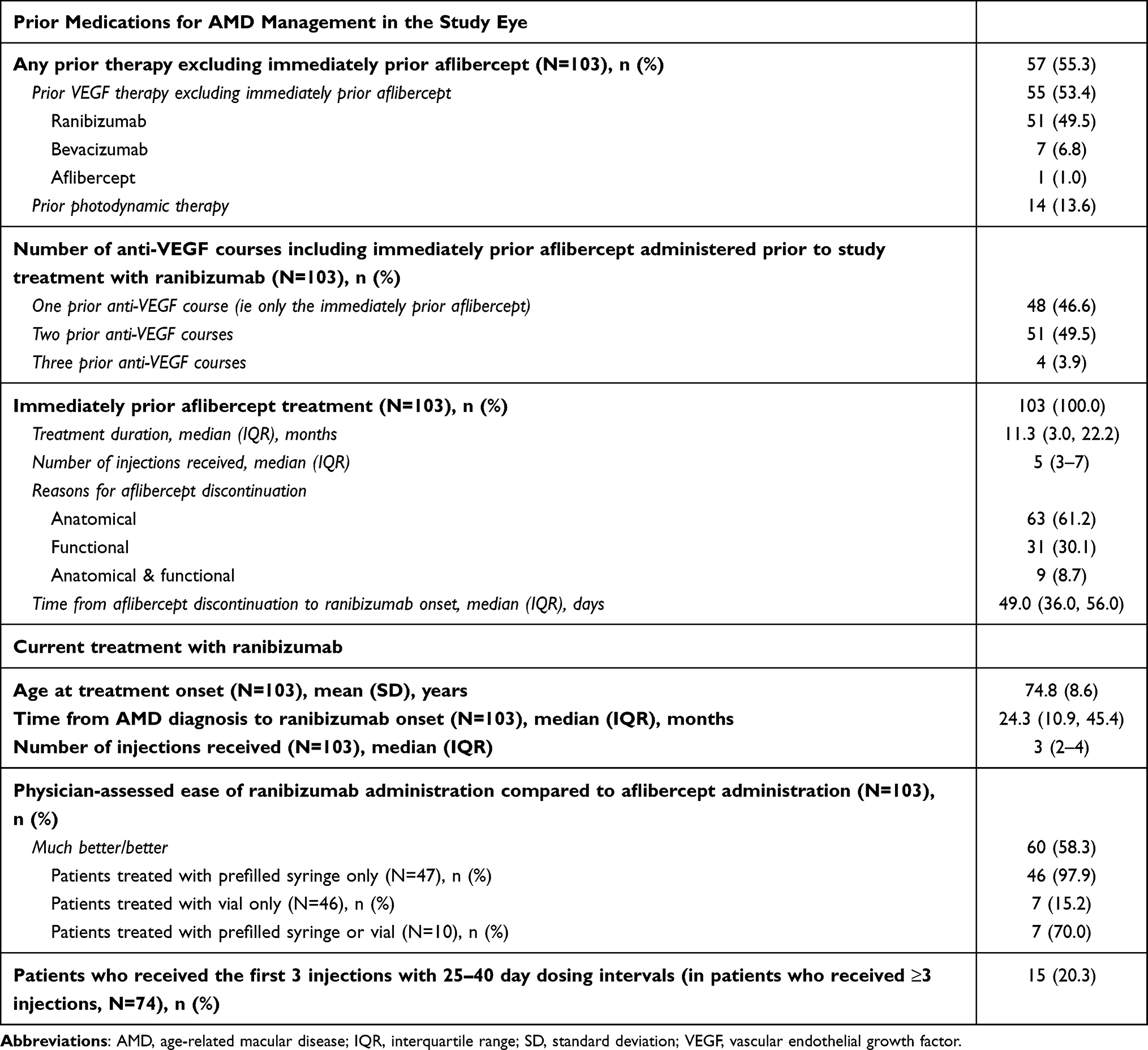 |
Table 2 Prior Medications for AMD Management in the Study Eye |
In addition, 55.3% of the patients had received prior treatment in the study eye other than the immediately prior aflibercept, including anti-VEGF therapy in 53.4% and photodynamic therapy in 13.6% (Table 2). Ranibizumab had been previously received in the study eyes of 51 (49.5%) patients (Table 2); treatment had been discontinued due to lack of efficacy in 35 cases, treatment completion in 14 cases, and disease relapse in two cases. Aflibercept had been administered a second time in the past in the study eye of one patient (1.0%) (Table 2), and had been discontinued due to disease relapse.
Ranibizumab was initiated a median of 24.3 months after wAMD diagnosis in the study eye, with all patients having received their first ranibizumab injection prior to (N = 19) or on the day of enrollment (N = 84). A median of 3 injections were received during the course of the study. In particular, 28.2% received <3 injections, 24.3% received 3, 26.2% received 4, and 21.4% received 5 or 6 injections. At the end of the study observation period, treatment with ranibizumab had been permanently discontinued in a single case due to deterioration of macular edema and increase of intraretinal fluid. Physicians ranked the ease of ranibizumab administration as “much better” or “better” than that of aflibercept for 58.3% of the patients, as “similar” in 38.8%, and as “worse” in 2.9%. Patients treated with ranibizumab using pre-filled syringe had higher rankings for much better/better ease of administration (Table 2). During the course of the study, only one patient received concomitant treatment for wAMD in the study eye, which consisted of a single course of photodynamic therapy.
Effects of Ranibizumab Treatment on CRT and PED Dimensions
At baseline, 47.2% (34/72) of the study eyes with paired baseline and 6-month post-baseline assessments had CRT <300 μm. This proportion was 45.8% (33/72) at 6 months post-baseline, while 15.3% (11/72) of the study eyes shifted from CRT ≥300 μm at baseline to CRT <300 μm at 6 months post-baseline. Baseline CRT did not statistically significantly change at any of the post-baseline timepoints based on as-observed data (Tables 3 and 4). Similarly, no statistically significant change at 6 months post-baseline was noted when applying the LOCF imputation method (Table 4).
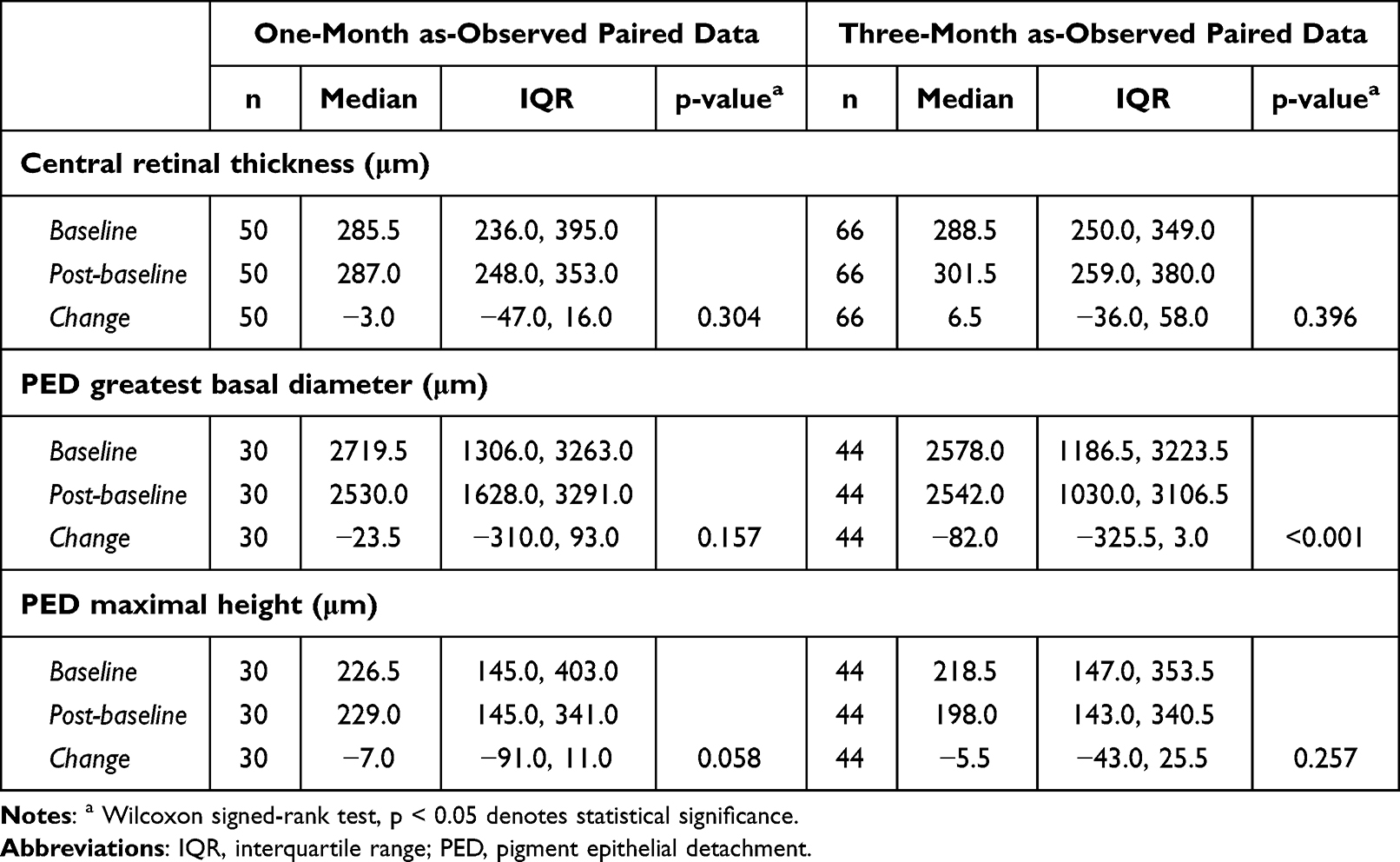 |
Table 3 Changes in Anatomical Measures at One Month and Three Months Post-Ranibizumab Treatment Onset in Study Eyes with Available Paired Assessments |
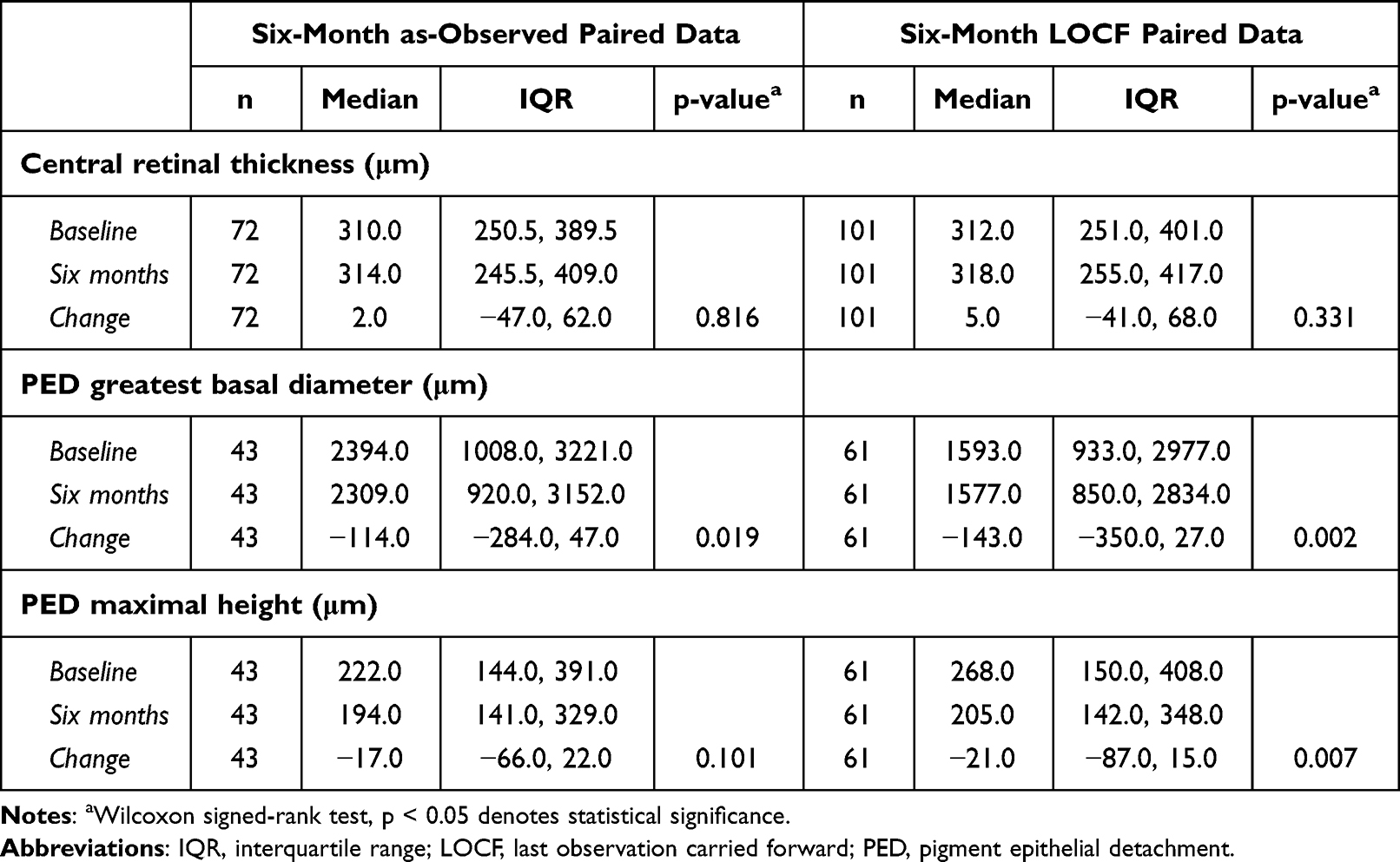 |
Table 4 Changes in Anatomical Measures at Six Months Post-Ranibizumab Treatment Onset in Study Eyes with Available Paired Assessments |
Among evaluable study eyes with PED at baseline and with paired baseline and 6-month post-baseline assessments (N = 43), the baseline PED MH did not significantly change at any post-baseline timepoint based on as-observed data (Tables 3 and 4). However, using LOCF a statistically significant median decrease of 21.0 μm (p = 0.007) was observed at 6 months post-baseline (Table 4). In addition, a statistically significant decrease in GBD was noted at 3 months (median decrease: 82.0 μm, p < 0.001; Table 3) and at 6 months (median decrease: 114.0 μm, p = 0.019; Table 4) post-baseline based on as-observed data. A significant decrease (median: 143.0 μm, p = 0.002; Table 4) was also observed at 6 months using LOCF.
Effects of Ranibizumab Treatment on BCVA
Among study eyes with paired BCVA assessments, statistically significant visual acuity gains from baseline were demonstrated at all post-baseline timepoints. In particular, the mean (SD) BCVA increased from 50.4 (15.2) letters at baseline to 52.9 (15.5) letters at 1 month (p = 0.002); from 52.3 (15.4) letters at baseline to 55.6 (15.7) letters at 3 months (p < 0.001); and from 52.0 (15.2) letters at baseline to 55.2 (16.2) letters at 6 months (p = 0.002) (Figure 2A). Moreover, at 6 months post-baseline, 81.8% (72/88) of the study eyes had a stable or improved ETDRS letter score (≥0-letter gain), while visual acuity gains of ≥15 letters from baseline was achieved by 17.0% (15/88) of the evaluable study eyes (Figure 2B).
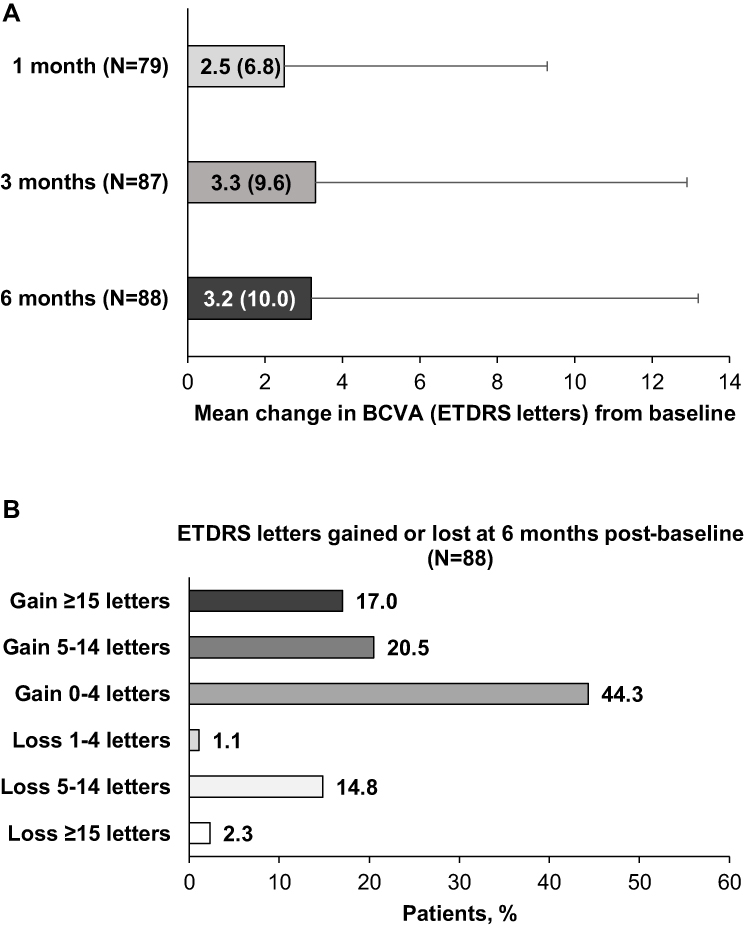 |
Figure 2 Best corrected visual acuity (BCVA) outcomes after ranibizumab treatment. (A) Mean changes in BCVA [ETDRS (Early Treatment Diabetic Retinopathy Study) letters] after 1, 3, and 6 months of ranibizumab treatment. Error bars and numbers in parentheses represent standard deviation. Statistically significant changes at 1 month (p = 0.002), 3 months (p < 0.001) and 6 months (p = 0.002) post-baseline (Wilcoxon signed-rank test). (B) Distribution of patients according to ETDRS letters gained or lost at 6 months post-baseline compared to baseline values. |
Impact of Patient, Disease, and Treatment Characteristics on CRT Changes from Baseline at 6 Months Post-Baseline
Multivariable linear regression analysis identified CNV subtype and baseline CRT to be associated with change in CRT from baseline at 6 months. Specifically, the estimated mean CRT change between baseline and 6 months post-baseline was −49.595 μm for eyes with classic CNV and 17.777 μm for those with occult CNV, corresponding to a significant difference between the groups (p = 0.021), when adjusted for sex and baseline BCVA and CRT. Moreover, the estimated mean CRT change between baseline and 6 months post-baseline was −53.751 μm for eyes with baseline CRT >300 μm and 21.932 μm for those with baseline CRT ≤300 μm, corresponding to a significant difference between the two groups (p = 0.008), when adjusted for sex, baseline BCVA and CNV subtype (Table 5).
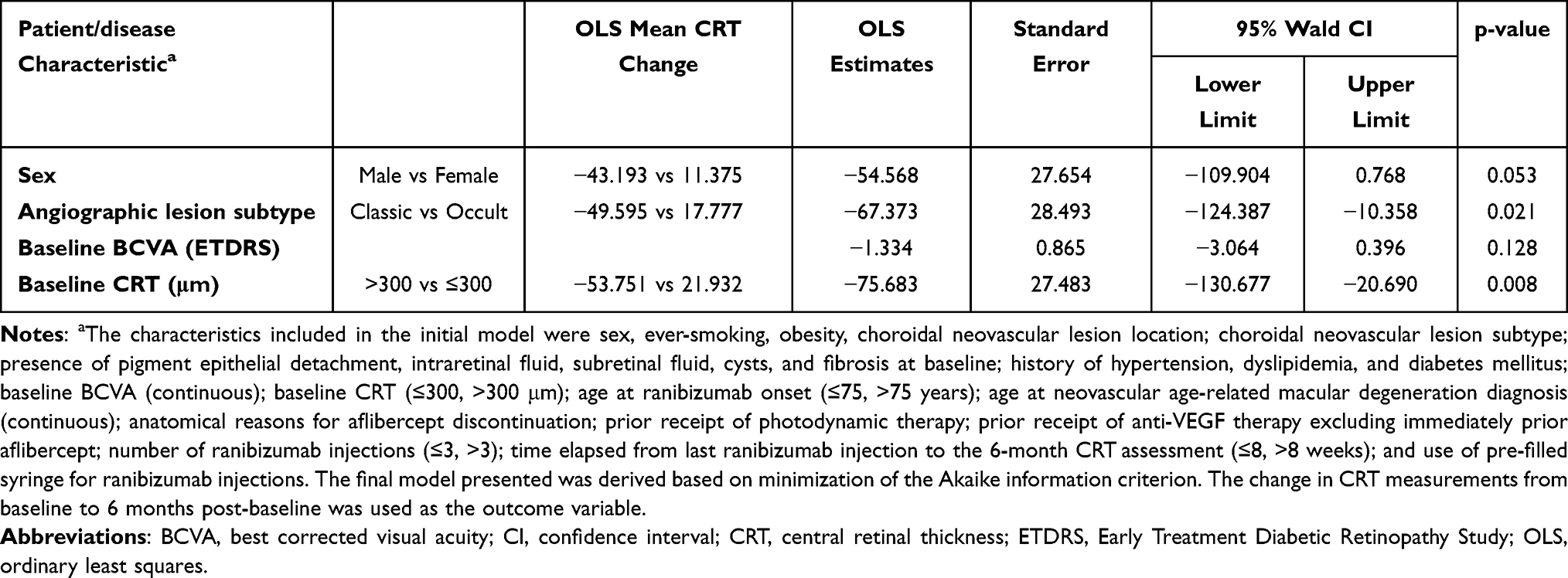 |
Table 5 Multivariable Linear Regression Analysis of the Association of CRT Changes Between Baseline and 6 Months Post-Baseline with Various Patient and Disease Characteristics |
Safety
Overall, 62.1% of the patients experienced a total of 195 AEs, none of which was assessed as causally related to ranibizumab. The 95.4% of these events (186 reports) were ocular, including 179 serious ocular events. Systemic AEs were reported for 2.9% of the patients (serious in 1.9%). The AEs reported at a frequency ≥10% included: subretinal fluid (in 37.9% of the patients), retinal edema (in 34.0%), macular edema (in 27.2%), retinal cyst (in 25.2%), detachment of retinal pigment epithelium (in 14.6%), and condition aggravated (in 12.6%). One patient (1.0%) experienced 2 AEs (“Macular oedema” and “Retinal oedema”) which led to permanent discontinuation of treatment with ranibizumab.
Discussion
To date, “ELEVATE” constitutes one of the few real-world prospective studies to have examined the effectiveness of ranibizumab in eyes pre-treated with aflibercept. The study indicates that ranibizumab improves visual acuity and certain anatomic outcomes after only 6 months of treatment, even when fewer than the recommended injections are administered. Additionally, physicians ranked the ease of administration of ranibizumab as better (58%) or the same (39%) as that of aflibercept in the vast majority of the patients.
Regarding anatomic outcomes, CRT remained stable throughout the observation period, whereas a statistically significant mean decrease of 46.5 μm in PED height from baseline to 6 months (using LOCF imputation) was noted (matching the 46-μm mean change assumed for sample size estimation),35 while significant mean decreases were also observed in PED GBD of 114.0 μm based on as-observed data and of 143.0 μm using LOCF imputation. Previous reports on anatomical outcomes in eyes switched to ranibizumab from a previous anti-VEGF agent in routine care settings are limited. To the best of our knowledge, the real-world SAFARI study represents the only prospective study on a population switched from aflibercept to ranibizumab, which examined the short-term impact of ranibizumab on functional and anatomic outcomes.25 In SAFARI, after 6 months of treatment including a median of 6 injections (as per study design all patients were to receive the first 3 monthly injections followed by a pro re nata schedule), no decrease in PED GBD was observed at 6 months (median increase from baseline: 59.5 μm). In addition, in SAFARI, PED height slightly decreased by a median of 2.5 μm, compared to a significant median decrease of 21.0 μm (LOCF imputation) observed in our study (with a median of three ranibizumab injections).25 Moreover, in a retrospective study of patients switched to ranibizumab after induction treatment with bevacizumab, a mean CRT decrease of 61.4 μm after a mean of 5.8 ranibizumab injections and over the course of 39 weeks was reported.32 It is worth mentioning that in the mentioned study the switch from bevacizumab to ranibizumab was not prompted by an inadequate response, but by the availability of licensed ranibizumab, hindering comparability to ELEVATE. Moreover, in a small case series of patients switched back to ranibizumab after one injection with aflibercept, central macular thickness decreased from 414.5 after the single aflibercept injection to 327.1 μm one month after returning to ranibizumab, while at 3 months it had returned to values observed one month prior to switching to aflibercept.39 Partial reporting of baseline characteristics in the previously mentioned study does not allow appraisal of whether disparity in the outcomes between this study and ELEVATE could be attributed to differences in confounding baseline factors. Notably, in ELEVATE, greater decreases in CRT were found to be associated with the presence of classic versus occult CNV and greater baseline CRT (>300 μm), with the latter reported as a predictor of anatomical outcomes in other studies as well.40,41 Specifically, both in patients with classic CNV and in those with baseline CRT >300 μm, the CRT decrease from baseline to 6 months post-baseline nearly reached (49.59 μm for the classic CNV subgroup) or exceeded (53.75 μm for those with baseline CRT >300 μm) the 50 μm cut-off used to define a clinically relevant significant reduction in a previous study.41
Regarding visual acuity assessments, a statistically significant median gain of 3.2 letters was found in ELEVATE at 6 months post-baseline, with 17% of the eyes experiencing clinically meaningful increases of ≥15 letters, 37.5% gaining ≥5 letters, and 82% having stable or improved BCVA. The SAFARI study reported median gains of 1 letter after 6 months of treatment in eyes switched to ranibizumab after poor response to aflibercept, with 11% of the study eyes gaining ≥15 letters.25 Moreover, in a comprehensive analysis of 20 real-world studies of ranibizumab, a mean BCVA gain of about 2.9 letters at 12 months was reported, while a mean of 19% of the patients in the 11 studies with available data were reported to have gained ≥15 letters at 12 months.15 These findings are not different from those observed in ELEVATE. Of note, lower BCVA scores and lower visual improvement rates post-ranibizumab treatment onset have been associated with the presence of intraretinal fluid,42,43 and presence of PED,42,44 which were present in 59% and 60% of the study eyes, respectively, and may have thus restricted the size of the observed ranibizumab effect.
Moreover, it is widely documented that in real-world practice retina specialists utilize pro re nata and “treat-and-extend” (T&E) protocols in terms of injection frequency, which result in patients receiving fewer injections that those recommended by ranibizumab’s label. Unfortunately, many studies have implicated this lower number of injections in worse anatomical and functional outcomes.12,15,45–50 There is one report in which utilization of a T&E regimen yielded similar BCVA outcomes to that of randomized trials when a mean of 8.6 injections were given in one year.51 Nonetheless, the median of 3 injections administered in ELEVATE over the 5.8-month study period is not only lower from that recommended in the product’s label, but also from the aforementioned 8.6 per year. Additionally, in ELEVATE only 15 of the 103 patients had received their first 3 injections within intervals ranging between 25 and 40 days (ie, approximately one month), which would match the induction phase recommended by the product’s approved label. This undertreatment of the patient population, which is likely linked to the rigid and time consuming system of injection approval that has been implemented following the economic crisis in Greece for “high-cost” pharmaceutical products, may have contributed to the absence of greater improvements in CRT and may have restricted the observed effect on other effectiveness outcomes. The observed lack of correlation between BCVA and CRT outcomes at 6 months in ELEVATE has also been reported elsewhere among patients treated with ranibizumab on a regular monthly schedule.43 Notably, this lack of correlation was not shown when ranibizumab was administered quarterly nor at the 3- and 9-month timepoints with a regular schedule. It is also of interest to mention that in the study of Simader et al,43 the effect of ranibizumab on the presence of intraretinal and subretinal fluid during the course of therapy, displayed a “spike and wave” effect, which was more pronounced in patients not treated with ranibizumab on a regular monthly schedule, further implicating pathophysiological mechanisms behind the reason why in ELEVATE, CRT change did not significantly improve despite improvements in BCVA and PED. Furthermore, in ELEVATE, nearly half of the patients were difficult-to-treat cases,52 had received more than two prior anti-VEGF treatment courses, and the majority had been switched back to ranibizumab from aflibercept.
Certain limitations of the study need to be considered, mainly arising from its observational design, including patient selection bias and information bias. Consecutive sampling was utilized to minimize patient selection bias. Regarding information bias, the missing data rate in regard to the change in CRT at 6 months was nearly 30%; the LOCF imputation method was used to assess the impact of the missing data on the primary study outcomes. It needs to be mentioned however that, although LOCF is a commonly used imputation method to handle missing data, it cannot be considered unbiased, unless the imputed values are randomly missing, which is, of course, unknown.53 This is particularly critical to keep in mind in studies like the present, as LOCF could lead to overestimation of the effectiveness of the treatment under study, if missing values mainly derive from subjects who respond poorly or are intolerant to the study drug, and for whom the last observation may be their best observation. Moreover, as data have been collected as per the physicians’ treatment practice, variation in the type of instruments employed, eg, for OCT, and the charts used for visual acuity assessments, and the instrument/chart assessors may have led to inter-instrument and inter-rater variability.54 This was accounted for by encouraging each participating study site to use the same assessor, OCT instrument, and visual acuity charts for all study-related measurements throughout the study. It should be noted that the conversion of Snellen scores to ETDRS scores may have introduced substantial errors, due to the wide range of baseline BCVA in the present study, since Snellen charts do not have regular geometrical progression of letter sizes between each line. Though discrepancies between Snellen and ETDRS measurements have been described,55 at the time of study design this conversion was selected as an acceptable approach to harmonize data obtained through different real-world practices. Lastly, the evaluable study size with regard to changes in CRT was lower than the target size derived during sample size estimation, with a total of 72 patients being finally evaluable for this endpoint, ie, 25% lower than the initially proposed minimum sample size of 96 evaluable patients. Although this deviation compromises the initially assumed power, it is not expected to adversely impact the meaningfulness of the study outcomes, taking into account the real-world nature of the study that primarily aimed to capture data generated in the routine care rather than prove or reject a formal statistical hypothesis. Moreover, the evaluable sample size for the co-primary endpoint was 43, thus meeting the target sample size of 31–40 patients. Moreover, it should be mentioned that there was no uniform definition for “inadequate response” to aflibercept, rather this was based on the physician’s judgment and could have been derived even after administration of a single aflibercept injection. Despite the lack of such a definition, it was required by the protocol that the reasons for aflibercept discontinuation be solely anatomical and/or functional, and therefore, response-related, rather than due to safety reasons or physician’s preference. In regard to the generalizability of the study results, the study population was enrolled by eight retinal specialists practicing in public/university hospitals or private eye centers distributed across administrative regions of Greece which are home to approximately two-thirds (65%) of the overall Greek population.
Conclusion
Overall, the study demonstrates that in the routine care of Greece, patients with wAMD receive fewer ranibizumab injections than those that would be administered under the approved dosage schedule. Under these conditions, after approximately 6 months of treatment, the patients’ visual acuity improved, modest improvements in PED dimensions were noted, and CRT remained stable Further real-world evidence is needed from studies more closely matching the approved dosage scheme, in order to identify predictors of early response, aiming to enhance outcomes in patients with wAMD who have inadequately responded to prior aflibercept treatment and to further delay the progression of the disease.
Abbreviations
AE, adverse event; AMD, age-related macular degeneration; BCVA, best-corrected visual acuity; BMI, body mass index; CI, confidence interval; CNV, choroidal neovascularization; CRT, central retinal thickness; ETDRS, Early Treatment Diabetic Retinopathy Study; GBD, greatest basal diameter, IQR, interquartile range; LOCF, Last Observation Carried Forward; MH, maximal height; OCT, optical coherence tomography; OLS, ordinary least squares; PED, pigment epithelial detachment; SD, standard deviation; VEGF, vascular endothelial growth factor; wAMD, wet age-related macular degeneration.
Data Sharing Statement
The data presented in this study are included in the article. The data are not publicly available due to restrictions that apply to the availability of the data (eg, privacy or ethical). Datasets from this study may be available upon request from the corresponding author and provided upon approval from the sponsor and in accordance with data privacy and ethical provisions.
Ethics Approval and Informed Consent
The study was conducted according to the guidelines of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Boards of the participating hospital sites. Participating hospital sites and approval dates for each hospital Institutional Review Board are listed below: Athens Vision Private Eye Care Center, 07-May-2015; General Hospital of Athens “Korgialenio – Benakio”, 01-Oct-2015; OMMA Private Eye Care Center, 04-May-2015; Interbalkan Center of Thessaloniki, 01-July-2015; General University Hospital of Heraklion, 09-Sep-2015; Regional General Hospital “G. Gennimatas”, 19-Feb-2016; “Attikon” University Hospital, 25-May-2016; and General University Hospital of Patras, 09-Nov-2015. All patients have given their written informed consent for participation in the study.
Acknowledgments
The authors would like to express their appreciation to the Investigators (in alphabetical order) E. Anastasiadis, A. Androu, R. A. Diamanti, Ch. Exarchou, M. Kanakis, Z. Kapsala, A. Kotsolis, A. Koutsmpi, G. Koutsocheras, A. Mani, V. Maniadi, V. Toumanidou, and Ch. Zoitsaki, for their participation in the study. In addition, they would like to thank V. Maniadi and V. Toumanidou ophthalmic photographers, and Iordanis Datseris, technician. Special thanks are extended to Novartis Field Medical Advisor Periandros Kritsiligkos, the study CRAs E. Kokkou, E-I. Patista, and D. Kokkinou and the CRA CSM I. Skarmoutsou for their valuable assistance. Finally, the authors wish to thank Qualitis Ltd. for medical writing support, which was funded by Novartis Hellas.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Novartis Hellas. Novartis Hellas was involved in the study design, data collection, interpretation and analysis, preparation of the manuscript and decision to publish.
Disclosure
AR reports receiving honoraria from Bayer Hellas; ID reports receiving honoraria from Novartis, Alcon, and Bayer; SA discloses having received research support and honoraria from Abbvie, Alcon, Bayer, Boehringer-Ingelheim, Innovis, and Novartis Hellas; MT has received support in the form of grants and/or consultancies from Novartis Hellas, Bayer Hellas, Mavrogenis, Allergan Hellas, Alcon Hellas, and Johnson and Johnson; SAK reports having received honoraria and having participated as an Investigator in clinical studies of Novartis, Bayer, and Allergan; NP reports receiving honoraria from Novartis; CK has no conflicts of interest to disclose; AC has received consultancy fees and honoraria from Bayer and Innovis, and honoraria from Optovue and Allergan Hellas; OK is an employee of Novartis Hellas, Medical Department; GP is an ex Novartis Hellas employee. The authors report no other conflicts of interest in this work.
References
1. Jonas JB, Cheung CMG, Panda-Jonas S. Updates on the epidemiology of age-related macular degeneration. Asia Pac J Ophthalmol. 2017;6:493–497.
2. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2:e106–116.
3. Vinores SA. Pegaptanib in the treatment of wet, age-related macular degeneration. Int J Nanomedicine. 2006;1:263–268.
4. Aiello LP, Pierce EA, Foley ED, et al. Suppression of retinal neovascularization in vivo by inhibition of vascular endothelial growth factor (VEGF) using soluble VEGF-receptor chimeric proteins. Proc Natl Acad Sci U S A. 1995;92:10457–10461.
5. Schmidt-Erfurth U, Chong V, Loewenstein A, et al. Guidelines for the management of neovascular age-related macular degeneration by the European Society of Retina Specialists (EURETINA). Br J Ophthalmol. 2014;98:1144–1167.
6. Borooah S, Jeganathan VS, Ambrecht AM, et al. Long-term visual outcomes of intravitreal ranibizumab treatment for wet age-related macular degeneration and effect on blindness rates in south-east Scotland. Eye (Lond). 2015;29:1156–1161.
7. Bakri SJ, Thorne JE, Ho AC, et al. Safety and efficacy of anti-vascular endothelial growth factor therapies for neovascular age-related macular degeneration: a report by the American Academy of Ophthalmology. Ophthalmology. 2019;126:55–63.
8. Mitchell P, Liew G, Gopinath B, Wong TY. Age-related macular degeneration. Lancet. 2018;392:1147–1159.
9. Rosenfeld PJ, Brown DM, Heier JS, et al.; MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355:1419–1431.
10. Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP, Ianchulev T, ANCHOR Study Group. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116:57–65.e5.
11. Silva R, Axer-Siegel R, Eldem B, et al. The SECURE study: long-term safety of ranibizumab 0.5 mg in neovascular age-related macular degeneration. Ophthalmology. 2013;120:130–139.
12. Singer MA, Awh CC, Sadda S, et al. HORIZON: an open-label extension trial of ranibizumab for choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology. 2012;119:1175–1183.
13. Rofagha S, Bhisitkul RB, Boyer DS, Sadda SR, Zhang K, SEVEN-UP Study Group. Seven-year outcomes in ranibizumab-treated patients in ANCHOR, MARINA, and HORIZON: a multicenter cohort study (SEVEN-UP). Ophthalmology. 2013;120:2292–2299.
14. Holz FG, Bandello F, Gillies M, et al.; LUMINOUS Steering Committee. Safety of ranibizumab in routine clinical practice: 1-year retrospective pooled analysis of four European neovascular AMD registries within the LUMINOUS programme. Br J Ophthalmol. 2013;97:1161–1167.
15. Chong V. Ranibizumab for the treatment of wet AMD: a summary of real-world studies. Eye (Lond). 2016;30:270–286.
16. Heussen FM, Shao Q, Ouyang Y, Joussen AM, Müller B. Clinical outcomes after switching treatment from intravitreal ranibizumab to aflibercept in neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2014;252:909–915.
17. Barthelmes D, Campain A, Nguyen P, et al. Effects of switching from ranibizumab to aflibercept in eyes with exudative age-related macular degeneration. Br J Ophthalmol. 2016;100:1640–1645.
18. Kumar N, Marsiglia M, Mrejen S, et al. Visual and anatomical outcomes of intravitreal aflibercept in eyes with persistent subfoveal fluid despite previous treatments with ranibizumab in patients with neovascular age-related macular degeneration. Retina. 2013;33:1605–1612.
19. Batioglu F, Demirel S, Özmert E, Abdullayev A, Bilici S. Short-term outcomes of switching anti-VEGF agents in eyes with treatment-resistant wet AMD. BMC Ophthalmol. 2015;15:40.
20. Chatziralli I, Nicholson L, Vrizidou E, et al. Predictors of outcome in patients with neovascular age-related macular degeneration switched from ranibizumab to 8-weekly aflibercept. Ophthalmology. 2016;123:1762–1770.
21. Narayan DS, Muecke J. Intravitreal aflibercept treatment in eyes with exudative age-related macular degeneration following prior treatment with intravitreal ranibizumab. Indian J Ophthalmol. 2015;63:832–836.
22. Sarao V, Parravano M, Veritti D, Arias L, Varano M, Lanzetta P. Intravitreal aflibercept for choroidal neovascularization due to age-related macular degeneration unresponsive to ranibizumab therapy. Retina. 2016;36:770–777.
23. Van Lancker L, Petrarca R, Moutsouris K, Masaoutis P, Kampougeris G. Clinical experience of switching anti-VEGF therapy from ranibizumab to aflibercept in age-related choroidal neovascularization. Eur J Ophthalmol. 2017;27:342–345.
24. Dugel PU, Griner R, Ferreira A, Milnes F, Lotery AJ. Clinical effectiveness of switching between ranibizumab and aflibercept in treatment of neovascular AMD: US real-world outcomes. J Vitreoretin Dis. 2019;3:127–134.
25. Gale RP, Pearce I, Eter N, et al. Anatomical and functional outcomes following switching from aflibercept to ranibizumab in neovascular age-related macular degeneration in Europe: SAFARI study. Br J Ophthalmol. 2020;104:493–499.
26. Kim JH, Kim JW, Kim CG, Lee DW. Long-term switching between ranibizumab and aflibercept in neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol. 2020;258:1677–1685.
27. Marquis LM, Mantel I. Beneficial switch from aflibercept to ranibizumab for the treatment of refractory neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2020;258:1591–1596.
28. Despreaux R, Cohen SY, Semoun O, et al. Short-term results of switchback from aflibercept to ranibizumab in neovascular age-related macular degeneration in clinical practice. Graefes Arch Clin Exp Ophthalmol. 2016;254:639–644.
29. Slean GR, Hemarat K, Khurana RN, Stewart JM. Conversion back to bevacizumab or ranibizumab for recurrent neovascular activity with aflibercept in age-related macular degeneration: a case series. Int J Retina Vitreous. 2016;2:2.
30. Waibel S, Matthé E, Sandner D. [Results of re-switch from intravitreal aflibercept to ranibizumab in patients with exudative age-related macular degeneration]. Klin Monbl Augenheilkd. 2018;235:616–621. German.
31. Gregori NZ, Feuer W, Rosenfeld PJ. Novel method for analyzing Snellen visual acuity measurements. Retina. 2010;30:1046–1050.
32. Kent JS, Iordanous Y, Mao A, Powell AM, Kent SS, Sheidow TG. Comparison of outcomes after switching treatment from intravitreal bevacizumab to ranibizumab in neovascular age-related macular degeneration. Can J Ophthalmol. 2012;47:159–164.
33. Kaiser RS, Gupta OP, Regillo CD, et al. Ranibizumab for eyes previously treated with pegaptanib or bevacizumab without clinical response. Ophthalmic Surg Lasers Imaging. 2012;43:13–19.
34. Chang AA, Li H, Broadhead GK, et al. Intravitreal aflibercept for treatment-resistant neovascular age-related macular degeneration. Ophthalmology. 2014;121:188–192.
35. Fassnacht-Riederle H, Becker M, Graf N, Michels S. Effect of aflibercept in insufficient responders to prior anti-VEGF therapy in neovascular AMD. Graefes Arch Clin Exp Ophthalmol. 2014;252:1705–1709.
36. Bakall B, Folk JC, Boldt HC, et al. Aflibercept therapy for exudative age-related macular degeneration resistant to bevacizumab and ranibizumab. Am J Ophthalmol. 2013;156:15–22.
37. Wykoff CC, Brown DM, Maldonado ME, Croft DE. Aflibercept treatment for patients with exudative age-related macular degeneration who were incomplete responders to multiple ranibizumab injections (TURF trial). Br J Ophthalmol. 2014;98:951–955.
38. Panos GD, Gatzioufas Z, Petropoulos IK, Dardabounis D, Thumann G, Hafezi F. Effect of ranibizumab on serous and vascular pigment epithelial detachments associated with exudative age-related macular degeneration. Drug Des Devel Ther. 2013;7:565–569.
39. Nudleman E, Wolf JD. Worsening anatomic outcomes following aflibercept for neovascular age-related macular degeneration in eyes previously well controlled with ranibizumab. Clin Ophthalmol. 2016;10:1053–1057.
40. Bek T, Klug SE. Age, sex, and type of medication predict the effect of anti-VEGF treatment on central retinal thickness in wet age-related macular degeneration. Clin Ophthalmol. 2018;12:473–479.
41. Ma C, Bai L, Lei C, et al. Predictors of visual and anatomical outcomes for neovascular age-related macular degeneration treated with bevacizumab. Biomed Rep. 2015;3:503–508.
42. Kodjikian L, Decullier E, Souied EH, et al. Predictors of one-year visual outcomes after anti-vascular endothelial growth factor treatment for neovascular age-related macular degeneration. Retina. 2018;38:1492–1499.
43. Simader C, Ritter M, Bolz M, et al. Morphologic parameters relevant for visual outcome during anti-angiogenic therapy of neovascular age-related macular degeneration. Ophthalmology. 2014;121:1237–1245.
44. Lotery A, Griner R, Ferreira A, Milnes F, Dugel P. Real-world visual acuity outcomes between ranibizumab and aflibercept in treatment of neovascular AMD in a large US data set. Eye (Lond). 2017;31:1697–1706.
45. Cohen SY, Mimoun G, Oubraham H, et al. Changes in visual acuity in patients with wet age-related macular degeneration treated with intravitreal ranibizumab in daily clinical practice: the LUMIERE study. Retina. 2013;33:474–481.
46. Souied EH, Oubraham H, Mimoun G, et al. Changes in visual acuity in patients with wet age-related macular degeneration treated with intravitreal ranibizumab in daily clinical practice: the TWIN study. Retina. 2015;35:1743–1749.
47. Hjelmqvist L, Lindberg C, Kanulf P, Dahlgren H, Johansson I, Siewert A. One-year outcomes using ranibizumab for neovascular age-related macular degeneration: results of a prospective and retrospective observational multicentre study. J Ophthalmol. 2011;2011:405724.
48. Dadgostar H, Ventura AA, Chung JY, Sharma S, Kaiser PK. Evaluation of injection frequency and visual acuity outcomes for ranibizumab monotherapy in exudative age-related macular degeneration. Ophthalmology. 2009;116:1740–1747.
49. Martin DF, Maguire MG, Fine SL, et al.; Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119:1388–1398.
50. Maguire MG, Martin DF, Ying GS, et al.; Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group. Five-year outcomes with anti-vascular endothelial growth factor treatment of neovascular age-related macular degeneration: the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2016;123:1751–1761.
51. Rufai SR, Almuhtaseb H, Paul RM, et al. A systematic review to assess the ‘treat-and-extend’ dosing regimen for neovascular age-related macular degeneration using ranibizumab. Eye (Lond). 2017;31:1337–1344.
52. Spooner K, Hong T, Wijeyakumar W, Chang AA. Switching to aflibercept among patients with treatment-resistant neovascular age-related macular degeneration: a systematic review with meta-analysis. Clin Ophthalmol. 2017;11:161–177.
53. Lachin JM. Fallacies of last observation carried forward analyses. Clin Trials. 2016;13:161–168.
54. Grover S, Murthy RK, Brar VS, Chalam KV. Comparison of retinal thickness in normal eyes using Stratus and Spectralis optical coherence tomography. Invest Ophthalmol Vis Sci. 2010;51:2644–2647.
55. Yu HJ, Kaiser PK, Zamora D, et al. Visual acuity variability: comparing discrepancies between Snellen and ETDRS measurements among subjects entering prospective trials. Ophthalmol Retina. 2021;5:224–233.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Real-World Evidence in the Management of Diabetic Macular Edema with Intravitreal Anti-VEGFs in Asia: A Systematic Literature Review
Yuen YS, Tan GSW, Gan NY, Too IHK, Mothe RK, Basa P, Shaikh J
Clinical Ophthalmology 2022, 16:3503-3526
Published Date: 19 October 2022
Real-World Experience Using Intravitreal Brolucizumab Alone or in Combination with Aflibercept in the Management of Neovascular Age-Related Macular Degeneration
Mehta N, Fong RD, Wilson M, Moussa K, Emami-Naeini P, Moshiri A, Yiu G, Park SS
Clinical Ophthalmology 2023, 17:657-665
Published Date: 27 February 2023
Transitioning from Aflibercept to Biosimilar Ranibizumab in Diabetic Macular Edema (DME): (The TRANSFORM-DME Trial) a Multicenter Observational Study
Chakraborty D, Sinha TK, Maiti A, Boral SK, Das A, Mondal S, Nandi K, Bhattacharya R
Clinical Ophthalmology 2024, 18:3449-3456
Published Date: 25 November 2024